-
X-Ray Rounds: (Plain) Radiographic Evaluation of the
ShoulderGarry W. K. Ho, M.D.Sports Medicine Fellow - VCU / Fairfax
Family PracticeDecember 2006
-
Anatomy3 BonesHumerusScapulaClavicle3
JointsGlenohumeralAcromioclavicularSternoclavicular1
ArticulationScapulothoracic
-
AnatomyHumerusHead *Anatomic neckSurgical neckGreater
tubercle*Lesser tubercle*Intertubercular grooveDeltoid
tuberosityShaft *
-
AnatomyScapulaBodyVentral (Costal) surfaceDorsal
surfaceBordersSuperiorLateral (Axillary)Medial
(Vertebral)AnglesSuperiorInferiorLateral (Head)
-
AnatomyScapulaGlenoidAcromionCoracoidSubscapular fossaScapular
spineSupraspinatus fossaInfraspinatus fossaGreat scapular
notchSuprascapular notch
-
AnatomyScapular Y (Lateral)
-
AnatomyClavicleFirst bone to start ossification; last to
finishThe only bony strut b/w UE and axial skeletonFlat outer
(lateral, acromial) thirdTraps, Delt, AC / CC ligamentsTubular
medial (inner, sternal) thirdStrongest in axial loadMiddle
thirdMost vulnerable to Fx
-
AnatomyGlenohumeral jointBall and socketPurpose: placement of
primary prehensile limbVery mobile; majority (0-120) of shoulder
movement (0-180)Price: instability45% of all dislocationsJoint
stability depends on multiple factors
-
AnatomyGlenohumeral jointPassive stabilityJoint conformityVacuum
effect of jt volSynovial fluid adhesion and cohesionScapular
inclinationGlenoid labrum (50%)Coracoid ligamentsCCL, CALJoint
capsuleGlenohumeral ligamentsSGHL, MGHL, IGHLCBony
restraintsGlenoid fossa, Acromion, CoracoidCoracohumeral
ligament
-
AnatomyGlenohumeral jointActive stability
Biceps (long head)
Rotator cuff
Pectoralis muscles, trapezius, serratus anterior, rhomboids,
levator scapulae, etc. (NOT deltoid)
-
AnatomyAcromioclavicular jointDiarthrodial jointThin capsuleAC
ligamentsAnterior, posterior, superior, inferiorCoracoacromial
ligamentCoracoclavicular ligamentsTrapeziod ligamentConoid
ligament
-
AnatomySternoclavicular jointDiarthrodial jointJoint
capsuleArticular diskIntraarticular disk ligamentSternoclavicular
ligamentsAnterior, posteriorInterclavicular ligament
-
AnatomyCoordinated shoulder motion
Glenohumeral motion
Acromioclavicular motion
Sternoclavicular motion
Scapulothoracic motionScapular-humeral rhythm
-
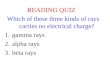
AP View of the ShoulderTransthoracic, or Routine AP ViewAP
relative to thoraxSuboptimal view of Glenohumeral jointGood view of
AC joint
Scapular, Grashey, or Glenohumeral AP ViewBetter visualize bony
relationships incl GH jointSuboptimal view of AC joint
Both have been called True AP Views
-
AP View of the ShoulderRoutine AP ViewClavicleScapulaAcromion
& scapular spineCoracoidBorders & anglesAC & SC
jointsGlenoidBoth ant & post lipsMay obscure HHHumerusHead
& necksGr & Lsr tuberosities
-
AP View of the ShoulderGlenohumeral, Grashey, or Scapular AP
View
Same structures
AC joint not visualized as well
Better visualize the glenoid & humeral head (especially with
ER view)
-
AP View of the Shoulder
-
AP View of the ShoulderAP View in External RotationGreater
tuberosity & soft tissues profiled and better visualizedBest w/
Scapular AP
AP View in Internal RotationMay demonstrate Hill-Sachs lesionsGH
instabilityBest w/ Routine AP
-
Which AP view should I get?Routine AP with humeral head in
internal rotation (IR)
Scapular / Glenohumeral AP with humeral head in external
rotation (ER)Harding WG, Nowicki KD. Plane talk about shoulder
radiographs. Phys Sportsmed 1998; 26(2)
-
Transthoracic Lateral View of the ShoulderNot usually done
Not as useful
Many obscuring over- and underlying structures
-
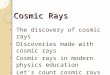
Axillary Lateral View of the ShoulderGood view of
anterior-posterior relationship of GH joint
CoracoidAcromionHumerusGlenoidGH joint
-
Axillary Lateral View of the ShoulderAlternate Axillary
views45Velpeau View magnified axillary view
-
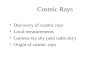
Scapular Y Lateral View of the ShoulderRelationship b/w humeral
head and glenoid
AcromionCoracoidScapular bodyScapular spine
-
Scapular Y Lateral View of the ShoulderScapular outlet viewA
variation of scapular Y viewSame projection, but with beam tilted
5-10 caudadShoulder impingement: to evaluate the subacromial space
and the supraspinatus outlet
-
Other Views of the Shoulder
-
IndicationsAmerican College of Radiology (ACR) Appropriateness
Criteria for Musculoskeletal Imaging in Shoulder Trauma
Developed in 1995, revised in 2005
AP with IR & ER, and lateral (axillary or scapular Y) views
recommended for:R/O fracture or dislocationSubacute (~3 months)
shoulder pain suspicious for:Bursitis / tendonitisRTC tear or
impingement (as initial study)
-
IndicationsStevenson and Trojian: JFP in July 2002No definitive
studies on the needs of shoulder radiographs have been
doneRecommended obtaining plain films for:Decreased ROM
(especially: abduction < 90)Severe painHistory of
traumaGlenohumeral AP, outlet & axillary lateral viewsAdd AP
with IR & ER in cases of traumaAC joint views for suspected AC
joint diseaseNeck, chest, abdominal imaging for suspected referred
painStevenson JH, Trojian T. Applied evidence: evaluation of
shoulder pain. J Fam Pract 2002; 51(7):605-611.
-
IndicationsOther indicationsSuspicion of instabilityWeakness of
shoulder motionsThe patient cannot communicate (altered mental
status, alcohol intoxication, or other)Persistent pain and
decreased ROM Anytime your history and physical dont give you
enough information
-
Normal routine AP in IRNormal routine AP in ERNormal axillary
view
-
Routine AP and axillary views
Neer classification 3-part proximal humerus fracture involving:-
Surgical neck- Lsr tuberosity
Tx: surgical eval
-
Proximal Humerus Fractures:Neer Classification2-part
fracturesMay be Txd conservatively if:Displaced < 1 cmAngulation
< 45 No dislocationsGood reductionNo intraarticular
involvementAnatomic neck intactOtherwise: surgical evaluationAll
else: surgical evaluation
-
Routine AP in ER, axillary, & scapular Y views
Anterior-inferior dislocationNo fracture
Tx: Conservative
-
Routine AP in ER, axillary, & scapular Y views
Bulb sign, rim sign, loss of parallelism
Posteriordislocation;No fracture
Tx: Conservative
-
Routine AP viewInferior GH dislocation(Luxatio erecta)- RareTx:
may attempt CRPost-reduction AP film
-
Routine AP in IR and axillary lateral views
No dislocation+ concave osseous impression in postero-lateral
aspect of humeral head
What is this lesion called?
Hill-Sachs lesion
Tx: conservative vs. operative
-
Hill-Sachs Lesions
-
Bankart Lesions
-
Type III AC separationTx: conservative mostlyType I:
conservative tx
Type II: conservative tx
Type III: conservative tx for most; may consider surgery for
active heavy laborers, frequent overhead activity, athletes 20-25
y/o
Type IV-VI: surgery
-
Clavicle FracturesMostly conservative treatmentConsider surgery
for:Group II Fxs (esp if medial to CCL)Open fracturesNeurovascular
compromiseSevere associated injuriesE.g. flail chest, mult rib fxs,
scapulothoracic dissociationNonunion / malunion
-
Scapular Fractures
Mostly conservative treatment
Surgical indications:ControversialDisplaced intraarticular fxs
involving > 25% articular surfaceScapular neck Fxs with> 1 cm
medial displacedAngulation > 40 Concomitant fxs of clavicles,
coracoid, acromion, scapular spineFracture-dislocations
-
Routine AP and Axillary Lateral Views
Advanced L shoulder osteoarthritis
Tx:Symptomatic reliefPT / Rehab exercisesInjectionsConsider
surgical eval
-
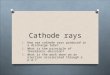
Scapular Y viewsA: normalB: Fracture / anterior dislocationC:
Posterior dislocation
-
Routine AP, True AP, and Axillary lateral views
Split fracture of humeral head with dislocated GH joint
Tx: Surgerize!
-
34 y/o M with shoulder pn and it feel like it wants to go out of
socketGlenohumeral AP & Scapular Y Lateral views of R
shoulder
Multiple radiodense loose bodies (largest infra coracoid &
infra glenoid)
Dx: Loose Bodies
Tx: Surgical consult
-
Glenohumeral AP view of shoulder and humerus
Radiolucent lesions spanning proximal third of L humerus
Enchondromas
Tx: Surgical consult (Biopsy)
-
Routine AP of R shoulder
Group 2, type 2 R clavicle fracture
Tx: Surgical repair
-
Glenohumeral AP, axillary lateral, and scapular Y views
Normal findings
Tx: as per clinical setting
-
Routine AP view
Scapular body fracture
Tx: mostly conservative
-
Routine AP view
Proximal humeral shaft fractureGlenohumeral dislocation
Tx: Orthopaedic consult
-
Axillary lateral view of L shoulder
Os acrominale; no acute fractureNormal variant; associated with
increased risk of RTC pathology
Tx: conservative
-
Routine AP view of L shoulder
Neer class 3-part comminuted, displaced proximal humerus
fracture
Tx: ORIF
-
Glenohumeral AP view of R shoulder
Humeral head collapse with loss of joint space
Tx: Ortho eval for hemi- vs. total arthroplasty
-
Routine AP view of R shoulder
Displaced group 1 clavicle fracture; risk of nonunion
Tx: ORIF (vs conservative)S/P ORIF
-
Routine AP view of L shoulder
Complete obliteration of L humeral head with heterotopic
ossification
Dx: Charcots joint
Tx: Arthroplasty
-
Routine AP and targeted AC views of R shoulder
Degenerative changes with subchondral bone cystic changes in the
AC joint
AC joint posttraumatic OA with osteolysis
Tx: conservative vs. operative
-
SummaryKnow what views to order when:
In general:Routine AP with shoulder in internal rotation
(IR)True glenohumeral AP in external rotation (ER)Axillary lateral
view
Use alternative lateral views if pt unable to tolerate axillary
lateralModified axillary lateral, Velpeau view, scapular Y
Know how to describe what you see
-
Thanks!Questions?
Ossification starts 5th wk GA laterally (acromial end); finishes
at age 22-25 y/o medially (sternal end)Intramembranous ossification
WITHOUT a cartilaginous stageAnterior acromial morphology1 (flat),
2 (curved), and 3 (hooked)
Acromial angleStryker notch view (looks like a modified axillary
view) can be used to see Hill-Sachs Lesions
West Point View (also looks like a modified axillary view) can
be used to see bony Bankart lesionsZanca Views (AP with 10 degrees
of cephalic tilt) is ideal for eval of AC jt