-
Instability of glenohumeral joint
-
Learning Objectives What is?Who gets?What types?How does
manifest ?How do we investigate ?How do we treat? Definition /
Anatomy Incidence Acute / Chronic Hystory / Physical exam
Investigation Treatment
-
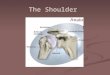
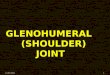
What is ? Definition Part of the shoulder joint complex 1.
Scapulo thoracic joint 2. Acromio-clavicular joint 3. Gleno humeral
joint 4. sterno-clavicular joint
-
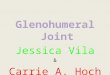
What is ? Anatomy Bony structuresAnterior view
-
What is ? Anatomy Glenoid labrum Lateral view of glenoid Torn
Labrum Bankart lesion
-
What is ? Anatomy Capsule and glenohumeral ligaments
CapsuleAnterior glenohumeral ligaments- superior- middle -
inferior
-
What is? AnatomyMuscles Dynamic stabilisation factors
-
What is ? Anatomy Other important structures
-
What is? Pathological AnatomyBankart lesion Capsule
damageHill-Sachs indentation fracture of the humeral head
-
Who gets it ? Incidence / Epidemiology
The most commonly dislocated joint
U.K. 12.3 per 100.000 people
Approximately 2% of people dislocate their shoulder at some
time
98% are anterior and inferior
-
What types? Acute dislocations
History - mechanism of injury - degree of trauma- first-time or
recurrent
Assessment - neurologic function - vascular insufficiency
-
What types? Acute dislocations Anterior inferior dislocation (
98% ) Epaulette appearance as the humeral head displaces anteriorly
and inferiorlyPatients arm :30 deg adduction Internal rotated
-
How do we investigate ? Investigation Radiography - in two
planes ( pre / post reduction ) - to confirm dislocation /
reduction - to exclude fracture humeral head
-
How do we reduce? Reduction Reduction - preferable in hospital -
patients comfortable ( analgesia / sedation ) Hippocrates
Kochers
-
What after? Post reduction treatment No consensus regarding post
reduction treatment
Young patients early immobilisation ( 7-10 days ) active
physiotherapy
Older age group no immoblisation active physiotherapy
-
What types? Recurrent dislocation Classification Degree -
subluxation ( dead arm syndrome ) - dislocation 2. Direction -
anterior ( vast majority ) - posterior - multidirectional (
inferior and ant/post ) 3.Underlying cause - traumatic -
atraumatic
4. Volition - voluntary
-
What types? Recurrent dislocation TUBSAMBRI
TraumaticUnidirectionalBankart lesion Surgery
AtraumaticMultidirectionalRehabilitation Inferior capsule
repair
-
What types? Recurrent dislocations Assessment History - more
complex - start with first episode - keep in mind TUBS -v-
AMBRI
Assessment - check general joint laxity- Apprehension test -
Drawer test ( anterior / posterior ) - Sulcus sign (
Multidirectional instab. )
-
How do we treat? Treatment Non operative treatment Most small /
medium sized chronic tears
Anti-inflamatory medication ( NSAIDs )
Strengthening exercises
Physiotherapy
-
How do we investigate ? Investigation Radiography - standard in
two planes ( ? Hill-Sachs lesion)
CT / MRI studies - beneficial with Artrography
CT - Hill-Sachs lesions - Glenoid fractures
MRI - labral lesions ( Bankart )
Arthroscopy - many centres = Gold standard
-
How do we treat ? Treatment Non-operative management Directed to
- atraumatic, - volunatry
Addressing the imbalance between internal / external
rotation
Muscle strengthening - deltoid, rotator cuff
-
How do we treat ? Treatment Operative management Aim of surgery
Return to pre-injury level of activity Indicated when
Rehabilitation has failed
Surgery correct anatomic defects ( Bankart procedure ) realign
muscle actions Arthroscopic / Open procedure
Bony architecture accounts for its tendency to dislocate It is a
ball and socket articulation with glenoid covering 1/3 of the
humeral articular surfaceThe capsule of glenohumeral joint is
attached around the margin of th ehumeral head and glenoid
articular surfacecs, except inferiorly where is attached between 1
and 2 cm below the articular margin. It is thickned anteriorly to
form the superior, middle and inferior glenohumeral ligamnetThe
contribution of girdle muscles to the joint stability is not clear.
( testing the joint under supra-scapular block paralising the supra
spinatus and infraspinatus, with no differencem implying that
muscles are not important in stability ) It has however been
sugested that the biceps tendon is important ( cadaveric studies )
Fractures associated with the acute dislocation : Hill-Sachs lesion
osteochondral fracture of the humeral head- fractures of the
greater tuberosity - fractures of the glenoid rim could give
permanent instability - fractures ofFailure to closed reduction
more likely to occur in longstanding dislocation- may occur in
fracture-dislocation , when the fragment / soft tissue
interposition between the humeral head and the glenoid- in a
Hill-Sachs lesion , the humeral head is impossible to disimpact
from the glenoid rim as a closed procedure
Sometimes need for open reduction !!!AMBRI group might be more
difficult to differentiate from the history Often people with
atraumatic dislocation childhood , check behavioral problems party
trick= Does not respond well to surgery Apprehension test - patient
seated / supine - arm 90 deg ABDuction & External rotated-
aware not to dislocate - tendency to dislocate patient becomes
apprehensive ( discomfort )
Drawer test - usefull in patients with a negative apprehension
test - supine / seated , shoulder 80-120 degrees abduction, slight
forward flexion and external rot.- examiner stabilses the scapula
with one hand and with the other lifts the humeral head forward
Sulcus sign test - described by Neer and Foster ( 1980 )- gentle
downward traction on th eupper limb , which is relaxed at the side
in neutral position - positive = visible sulcus between the
acromion and the humeral head- indicates Multidirectional
instability