Embed Size (px)
Citation preview
Research in Developmental Disabilities 35 (2014) 2735–2743
Contents lists available at ScienceDirect
Research in Developmental Disabilities
Short-term and long-term influences of family arguments and
gender difference on developing psychological well-being inTaiwanese adolescentsFu-Gong Lin *, Yu-Ching Chou, Cheng-Hsun Wu, Jing-Ding Lin
School of Public Health, National Defense Medical Center, Taipei, Taiwan, ROC
A R T I C L E I N F O
Article history:
Received 20 May 2014
Accepted 7 July 2014
Available online
Keywords:
Adolescent
Family argument
Psychological well-being
Gender difference
A B S T R A C T
Adolescent mental health is crucial for social competence and accomplishment in later life.
The World Health Organization (WHO) estimates that approximately 20% of adolescents
suffer from psychological symptoms. However, improving family risk and school
environments can largely promote adolescent mental health. A longitudinal survey
was conducted to investigate adolescent psychological well-being (PWB) status and
associated factors in adolescents 15–20 years of age. Family and school context variables
were interviewed and recorded. A total of 2896 participants were included from high,
middle, and less urbanized resident areas in Northern Taiwan with completed interview
data. Using multivariate regression analysis, factors associated with adolescent PWB at
various stages included quarrelsome parents, quarrels with parents, severed friendships,
and cigarette and alcohol use. In all three adolescent stages, females yielded higher
psychological symptom scores than did males, and diverse weights of risk factors on PWB
were observed between genders. Family arguments and cigarette and alcohol use were
found to have more pronounced effects on outcomes among females than males. Whereas
males are more sensitive to severed friendships than females, cigarette and alcohol use
showed more harmful effects on mental health in earlier adolescence than in later life.
Moreover, family arguments and severed friendships in earlier adolescence were found to
have lasting effects on PWB in later adolescence. In this study, gender differences were
observed in the temporal relationship on adolescent mental health. Variables of family
arguments and severed friendships exhibited short-term and long-term effects on
adolescent mental health across the early to late developmental stages. The family
argument environment and regulating cigarette and alcohol use are worthy of focus to
promote adolescent mental health.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Mental well-being is essential for adolescent development into a healthy adult with social competence (WHO, 2012). TheWorld Health Organization estimates that approximately 20% of adolescents suffer from depression or anxiety (WHO, 2012).A review of the literature shows that the onset of psychological symptoms is occurring at a younger age on average than
* Corresponding author at: School of Public Health, National Defense, Medical Center, Taipei, Taiwan, No. 161, Min-Chun E. Rd., Sec. 6, Taipei, Taiwan, ROC.
Tel.: +886 2 8792 3140x18470; fax: +886 2 87923147.
E-mail addresses: [email protected], [email protected] (F.-G. Lin).
http://dx.doi.org/10.1016/j.ridd.2014.07.018
0891-4222/� 2014 Elsevier Ltd. All rights reserved.

F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–27432736
previously (Fergusson, Boden, & Horwood, 2011; Gilman, Kawachi, Fitzmaurice, & Buka, 2002). Mehler-Wex and Kolch(2008) indicated that 80% of children and adolescents who suffer from depression will relapse into depressive adults.Depression in adults may originate from the early life family environment (Gilman et al., 2002; Gilman, Kawachi,Fitzmaurice, & Buka, 2003). Data from recent studies also suggests that depression in young people may negatively affecttheir growth and social development and may be a crucial precursor to psychopathology in later life (Bhatia & Bhatia, 2007;Chang, Zauszniewski, Heinzer, Musil, & Tsai, 2007; Chang, Chen, & Lien, 2007). Depression in early life is also found to beassociated with later mental disorders such as anxiety disorder, oppositional disorder, substance use disorder and conductdisorder, characterized by high recurrence and high social costs (Barrera, Torres, & Munoz, 2007; Fergusson et al., 2011).Suicide in depressive adolescents and youth is a common and seriously fatal complication. The evidence substantiates thatdepression can onset during adolescence, in which youth suffer from invasive depression and bear the accompanied seriousoutcome of suicide (Jellinek & Snyder, 1998).
Other studies have indicated that risk factors for mental well-being in children and adolescents involve personalcharacteristics, and family and school environments (Wu, Kao, Yen, & Lee, 2007). Personal characteristics include gender,body weight, and sleeping behavior (Erickson, Robinson, Haydel, & Killen, 2000). Among the familial components,socioeconomic status, family climate (Gilman et al., 2002), parenting style, family conflict (Gunnlaugsson, Kristjansson,Einarsdottir, & Sigfusdottir, 2011; Herrenkohl, Kosterman, Hawkins, & Mason, 2009), and a history of depression in parents(Freres, Gillham, Reivich, & Shatte, 2002; Mesman & Koot, 2000) are typically mentioned in child and adolescent mentalhealth research. Support from family and teachers has been shown to reduce the risk of psychological symptoms and anxietyin Latino youth (Potochnick & Perreira, 2010). Among the school environment factors, peer relationships, support, andacademic performance have all been shown to affect children’s mental health (Lin et al., 2008). In another study, childrenwho had relatively few friends tended to experience psychological symptoms (Schwartz, Gorman, Duong, & Nakamoto,2008).
Taiwanese adolescents also suffer from mental problems. National survey data in 1999 indicated that 30.5% ofadolescents between the ages of 12 and 18 experienced depressive symptoms (Lue, Wu, & Yen, 2010). Research on measuringdepressive symptoms conducted in 2007 revealed that nearly 24% of children were found to have depressive symptoms, and4.2% of the children were reported to have major depressive disorders (Chang, Zauszniewski, et al., 2007; Chang, Chen, et al.,2007).
Longitudinal and time-trend studies are necessary to determine the risk factors of mental disorder problems in childrenand young people (Kessler, 2000; Pelkonen, Marttunen, Kaprio, Huurre, & Aro, 2008; Sourander et al., 2012), and to explorethe critical causes of mental health problems during the various developmental stages of adolescents. The Taiwan YouthProject (TYP) conducted in 2000, investigated the psychological well-being (PWB) of the Taiwan urban/suburban/ruraladolescent cohort, and analyzed family and school-related variables related to adolescent mental health during adolescentdevelopmental stages. The primary goal of this research was to investigate the short and long-term influence of relatedfamily, school, and health behavior factors on the PWB of adolescents by analyzing the TYP cohort data during thedevelopment period.
2. Materials and methods
2.1. Study population
Participants derived from annual interviews of the TYP, conducted by the Institute of Sociology, Academia Sinica, Taiwan,from 2000 through 2007.
The study population included 1984/5-birth and 1987/8-birth cohorts living in Northern Taiwan. The presented sampleswere collected using a schooled-based, stratified design from 40 junior high schools, 16 from urbanized Taipei City, 15 fromsuburbanized Taipei County, and nine from less-urbanized Yilan County. A total of 81 classes were chosen, with two or threeclasses from each school. The two cohort samples included 2683 seventh graders (first year junior high) and 2851 ninthgraders (last year junior high). The participants were first interviewed using structured questionnaires, and the respondentswere tracked each year from adolescence to age 20 years. The participants were interviewed using a self-reported 16-itemPWB scale at 15, 18, and 20 years of age, defined as early, middle, and late adolescent stages in this study. From these twocohorts, a total of 2896 cases remained with completed interview data through the early, middle, and late adolescent stages.Data for the remaining 2896 participants were used to compare with the original 5535 participants, representing the censuspopulation comparison with gender (chi-square = 0.34, df = 1, p = .56) and residence distribution (chi-square = 1.09, df = 1,p = .29). The scores of the PWB scale of the 2896 participants were not found to significantly differ from the originalpopulation.
2.2. Measurement of psychological well-being
The PWB of participants was measured with a self-reported 16-item short version subscale extracted from the SymptomChecklist-90-revised scale (SCL-90-R) that was originally used for a broad range of psychological symptoms (Derogatis,1983). The included 16 items were among items that were typically reported by adolescent mental health-relatedinvestigations in Taiwan (Wang & Wu, 2003). In the TYP, the SCL-16 scale was measured at three time points during
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–2743 2737
adolescent developmental stages: first at their ninth grade of the 15-year old early adolescent stage, second at 3 years later intheir 18-year old middle adolescent stage, and third at 5 years later in their 20-year old late adolescent stage.
The 16 items included four dimensions as (a) somatization with six items (headaches, faintness or dizziness, musclesoreness, numbness or tingling in parts of your body, a lump in your throat, feeling weak in parts of your body), (b)depression with four items (thoughts of ending your life, feeling lonely, feeling blue, worrying too much about things), (c)hostility with three items (having urges to beat, injure, or harm someone, getting into frequent arguments, shouting orthrowing things), and (d) insomnia with three items (trouble falling asleep, awakening in the early morning, sleep that isrestless or disturbed). Each of the 16 items was rated on a 5-point scale from 1 to 5 as never, a little, average, serious, and very
serious, measuring the frequency of symptoms during the past week. Summation of the 16-item score was defined as thePWB index, with a higher score indicating worse PWB. The Cronbach’s alpha for this scale of eight waves ranged from 0.70 to0.83. (Wang & Wu, 2003; Yi, 2013).
2.3. Measurement of independent variable
Demographic variables were measured with gender, residences that were registered at the first investigation, and threeareas of Taipei City, Taipei County, and Yilan County were categorized into urban, suburban, and rural areas, respectively.Cigarette or alcohol use were asked as the frequencies of smoking or drinking behaviors during the last year as never,occasional, or frequent in adolescents younger than 18 years of age. In the late adolescent stage, the frequencies of cigaretteuse were asked as never, less than 1 pack per week, and more than 1 pack per week, and alcohol use was asked as never, 1–2
times per month, and 3+ times per month. Family related variables included family income, parent education (if> 12 years),marital status if their parents were divorced, separated, or one parent had died which defined as abnormal status. Familyarguments included two questions regarding whether parents quarrelled frequently and if participants had had frequentquarrels with parents in the past year. The school-related variable of severed friendships during the past year was examinedfor the significance on outcome.
2.4. Statistical analysis
The analysis was conducted using SPSS 20.0 software. Analysis of variance (ANOVA) tests were used for comparingcontinuous variables among the grouped data and to test for the interaction between independent variables on outcome. Forthe outcome of PWB, the summated scores of SCL-16 from adolescents were analyzed using the multiple regression method,with the independent predictive variables of family and school-related factors. The generalized estimating equation (GEE)linear model was implemented to predict the PWB score over time with three-stage repeat measuring variables from earlythrough late adolescence. In all of the tests conducted in this study, p< .05 was considered to be statistically significant.
3. Results
3.1. Description of the sample
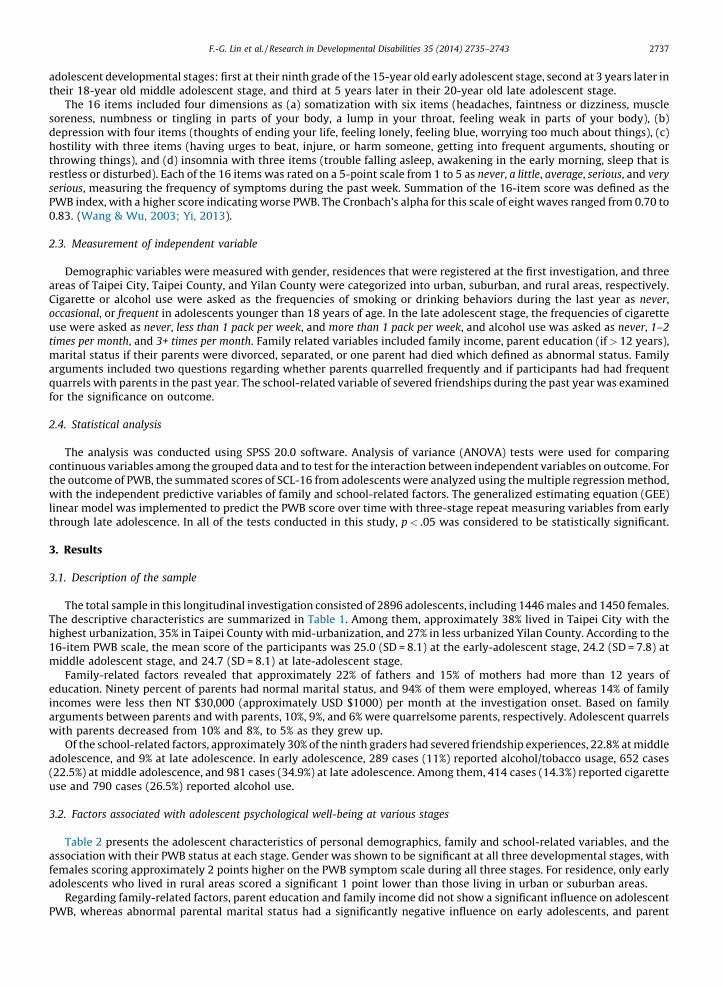
The total sample in this longitudinal investigation consisted of 2896 adolescents, including 1446 males and 1450 females.The descriptive characteristics are summarized in Table 1. Among them, approximately 38% lived in Taipei City with thehighest urbanization, 35% in Taipei County with mid-urbanization, and 27% in less urbanized Yilan County. According to the16-item PWB scale, the mean score of the participants was 25.0 (SD = 8.1) at the early-adolescent stage, 24.2 (SD = 7.8) atmiddle adolescent stage, and 24.7 (SD = 8.1) at late-adolescent stage.
Family-related factors revealed that approximately 22% of fathers and 15% of mothers had more than 12 years ofeducation. Ninety percent of parents had normal marital status, and 94% of them were employed, whereas 14% of familyincomes were less then NT $30,000 (approximately USD $1000) per month at the investigation onset. Based on familyarguments between parents and with parents, 10%, 9%, and 6% were quarrelsome parents, respectively. Adolescent quarrelswith parents decreased from 10% and 8%, to 5% as they grew up.
Of the school-related factors, approximately 30% of the ninth graders had severed friendship experiences, 22.8% at middleadolescence, and 9% at late adolescence. In early adolescence, 289 cases (11%) reported alcohol/tobacco usage, 652 cases(22.5%) at middle adolescence, and 981 cases (34.9%) at late adolescence. Among them, 414 cases (14.3%) reported cigaretteuse and 790 cases (26.5%) reported alcohol use.
3.2. Factors associated with adolescent psychological well-being at various stages
Table 2 presents the adolescent characteristics of personal demographics, family and school-related variables, and theassociation with their PWB status at each stage. Gender was shown to be significant at all three developmental stages, withfemales scoring approximately 2 points higher on the PWB symptom scale during all three stages. For residence, only earlyadolescents who lived in rural areas scored a significant 1 point lower than those living in urban or suburban areas.
Regarding family-related factors, parent education and family income did not show a significant influence on adolescentPWB, whereas abnormal parental marital status had a significantly negative influence on early adolescents, and parent
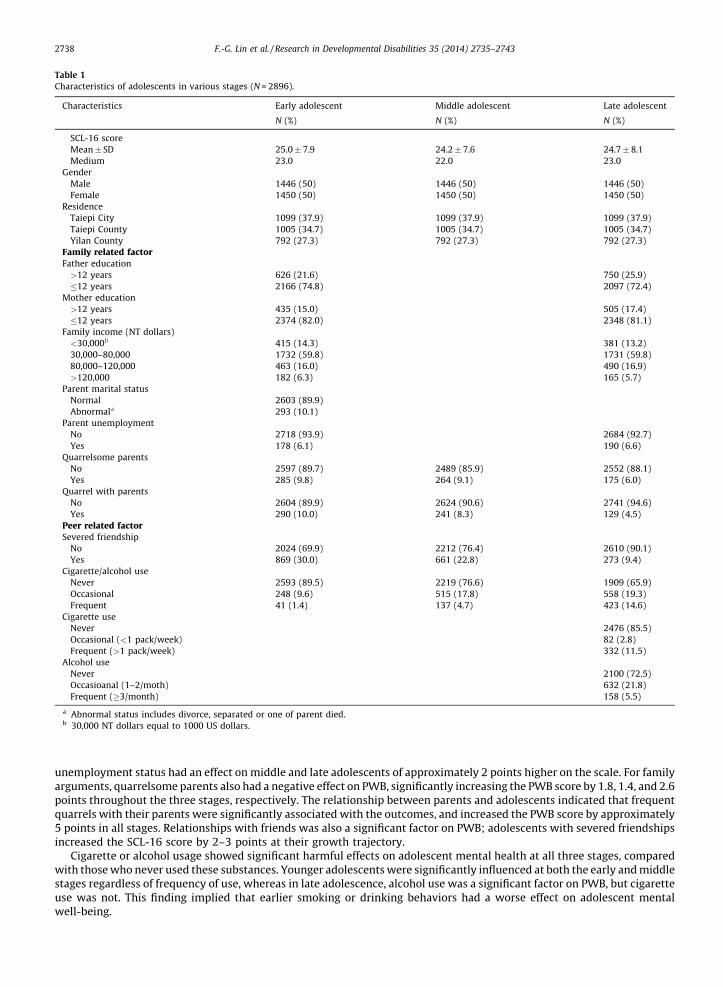
Table 1
Characteristics of adolescents in various stages (N = 2896).
Characteristics Early adolescent Middle adolescent Late adolescent
N (%) N (%) N (%)
SCL-16 score
Mean� SD 25.0� 7.9 24.2� 7.6 24.7� 8.1
Medium 23.0 22.0 23.0
Gender
Male 1446 (50) 1446 (50) 1446 (50)
Female 1450 (50) 1450 (50) 1450 (50)
Residence
Taiepi City 1099 (37.9) 1099 (37.9) 1099 (37.9)
Taiepi County 1005 (34.7) 1005 (34.7) 1005 (34.7)
Yilan County 792 (27.3) 792 (27.3) 792 (27.3)
Family related factorFather education
>12 years 626 (21.6) 750 (25.9)
�12 years 2166 (74.8) 2097 (72.4)
Mother education
>12 years 435 (15.0) 505 (17.4)
�12 years 2374 (82.0) 2348 (81.1)
Family income (NT dollars)
<30,000b 415 (14.3) 381 (13.2)
30,000–80,000 1732 (59.8) 1731 (59.8)
80,000–120,000 463 (16.0) 490 (16.9)
>120,000 182 (6.3) 165 (5.7)
Parent marital status
Normal 2603 (89.9)
Abnormala 293 (10.1)
Parent unemployment
No 2718 (93.9) 2684 (92.7)
Yes 178 (6.1) 190 (6.6)
Quarrelsome parents
No 2597 (89.7) 2489 (85.9) 2552 (88.1)
Yes 285 (9.8) 264 (9.1) 175 (6.0)
Quarrel with parents
No 2604 (89.9) 2624 (90.6) 2741 (94.6)
Yes 290 (10.0) 241 (8.3) 129 (4.5)
Peer related factorSevered friendship
No 2024 (69.9) 2212 (76.4) 2610 (90.1)
Yes 869 (30.0) 661 (22.8) 273 (9.4)
Cigarette/alcohol use
Never 2593 (89.5) 2219 (76.6) 1909 (65.9)
Occasional 248 (9.6) 515 (17.8) 558 (19.3)
Frequent 41 (1.4) 137 (4.7) 423 (14.6)
Cigarette use
Never 2476 (85.5)
Occasional (<1 pack/week) 82 (2.8)
Frequent (>1 pack/week) 332 (11.5)
Alcohol use
Never 2100 (72.5)
Occasioanal (1–2/moth) 632 (21.8)
Frequent (�3/month) 158 (5.5)
a Abnormal status includes divorce, separated or one of parent died.b 30,000 NT dollars equal to 1000 US dollars.
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–27432738
unemployment status had an effect on middle and late adolescents of approximately 2 points higher on the scale. For familyarguments, quarrelsome parents also had a negative effect on PWB, significantly increasing the PWB score by 1.8, 1.4, and 2.6points throughout the three stages, respectively. The relationship between parents and adolescents indicated that frequentquarrels with their parents were significantly associated with the outcomes, and increased the PWB score by approximately5 points in all stages. Relationships with friends was also a significant factor on PWB; adolescents with severed friendshipsincreased the SCL-16 score by 2–3 points at their growth trajectory.
Cigarette or alcohol usage showed significant harmful effects on adolescent mental health at all three stages, comparedwith those who never used these substances. Younger adolescents were significantly influenced at both the early and middlestages regardless of frequency of use, whereas in late adolescence, alcohol use was a significant factor on PWB, but cigaretteuse was not. This finding implied that earlier smoking or drinking behaviors had a worse effect on adolescent mentalwell-being.
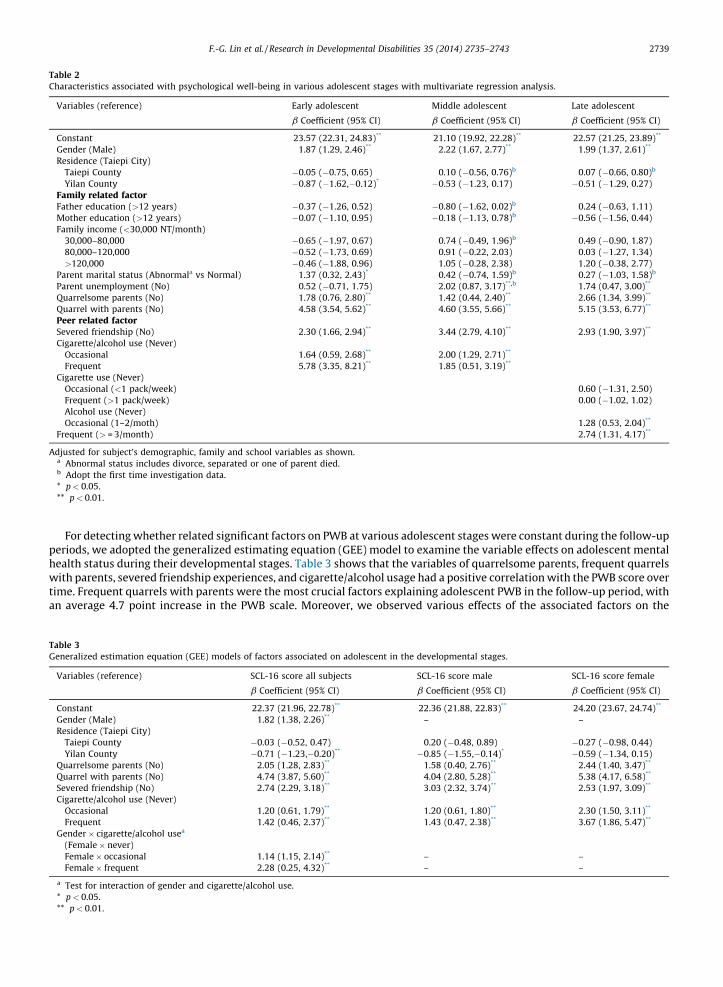
Table 2
Characteristics associated with psychological well-being in various adolescent stages with multivariate regression analysis.
Variables (reference) Early adolescent Middle adolescent Late adolescent
b Coefficient (95% CI) b Coefficient (95% CI) b Coefficient (95% CI)
Constant 23.57 (22.31, 24.83)** 21.10 (19.92, 22.28)** 22.57 (21.25, 23.89)**
Gender (Male) 1.87 (1.29, 2.46)** 2.22 (1.67, 2.77)** 1.99 (1.37, 2.61)**
Residence (Taiepi City)
Taiepi County �0.05 (�0.75, 0.65) 0.10 (�0.56, 0.76)b 0.07 (�0.66, 0.80)b
Yilan County �0.87 (�1.62,�0.12)* �0.53 (�1.23, 0.17) �0.51 (�1.29, 0.27)
Family related factorFather education (>12 years) �0.37 (�1.26, 0.52) �0.80 (�1.62, 0.02)b 0.24 (�0.63, 1.11)
Mother education (>12 years) �0.07 (�1.10, 0.95) �0.18 (�1.13, 0.78)b �0.56 (�1.56, 0.44)
Family income (<30,000 NT/month)
30,000–80,000 �0.65 (�1.97, 0.67) 0.74 (�0.49, 1.96)b 0.49 (�0.90, 1.87)
80,000–120,000 �0.52 (�1.73, 0.69) 0.91 (�0.22, 2.03) 0.03 (�1.27, 1.34)
>120,000 �0.46 (�1.88, 0.96) 1.05 (�0.28, 2.38) 1.20 (�0.38, 2.77)
Parent marital status (Abnormala vs Normal) 1.37 (0.32, 2.43)* 0.42 (�0.74, 1.59)b 0.27 (�1.03, 1.58)b
Parent unemployment (No) 0.52 (�0.71, 1.75) 2.02 (0.87, 3.17)**,b 1.74 (0.47, 3.00)**
Quarrelsome parents (No) 1.78 (0.76, 2.80)** 1.42 (0.44, 2.40)** 2.66 (1.34, 3.99)**
Quarrel with parents (No) 4.58 (3.54, 5.62)** 4.60 (3.55, 5.66)** 5.15 (3.53, 6.77)**
Peer related factorSevered friendship (No) 2.30 (1.66, 2.94)** 3.44 (2.79, 4.10)** 2.93 (1.90, 3.97)**
Cigarette/alcohol use (Never)
Occasional 1.64 (0.59, 2.68)** 2.00 (1.29, 2.71)**
Frequent 5.78 (3.35, 8.21)** 1.85 (0.51, 3.19)**
Cigarette use (Never)
Occasional (<1 pack/week) 0.60 (�1.31, 2.50)
Frequent (>1 pack/week) 0.00 (�1.02, 1.02)
Alcohol use (Never)
Occasional (1–2/moth) 1.28 (0.53, 2.04)**
Frequent (> = 3/month) 2.74 (1.31, 4.17)**
Adjusted for subject’s demographic, family and school variables as shown.a Abnormal status includes divorce, separated or one of parent died.b Adopt the first time investigation data.
* p< 0.05.
** p< 0.01.
Table 3
Generalized estimation equation (GEE) models of factors associated on adolescent in the developmental stages.
Variables (reference) SCL-16 score all subjects SCL-16 score male SCL-16 score female
b Coefficient (95% CI) b Coefficient (95% CI) b Coefficient (95% CI)
Constant 22.37 (21.96, 22.78)** 22.36 (21.88, 22.83)** 24.20 (23.67, 24.74)**
Gender (Male) 1.82 (1.38, 2.26)** – –
Residence (Taiepi City)
Taiepi County �0.03 (�0.52, 0.47) 0.20 (�0.48, 0.89) �0.27 (�0.98, 0.44)
Yilan County �0.71 (�1.23,�0.20)** �0.85 (�1.55,�0.14)* �0.59 (�1.34, 0.15)
Quarrelsome parents (No) 2.05 (1.28, 2.83)** 1.58 (0.40, 2.76)** 2.44 (1.40, 3.47)**
Quarrel with parents (No) 4.74 (3.87, 5.60)** 4.04 (2.80, 5.28)** 5.38 (4.17, 6.58)**
Severed friendship (No) 2.74 (2.29, 3.18)** 3.03 (2.32, 3.74)** 2.53 (1.97, 3.09)**
Cigarette/alcohol use (Never)
Occasional 1.20 (0.61, 1.79)** 1.20 (0.61, 1.80)** 2.30 (1.50, 3.11)**
Frequent 1.42 (0.46, 2.37)** 1.43 (0.47, 2.38)** 3.67 (1.86, 5.47)**
Gender� cigarette/alcohol usea
(Female� never)
Female� occasional 1.14 (1.15, 2.14)** – –
Female� frequent 2.28 (0.25, 4.32)** – –
a Test for interaction of gender and cigarette/alcohol use.
* p< 0.05.
** p< 0.01.
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–2743 2739
For detecting whether related significant factors on PWB at various adolescent stages were constant during the follow-upperiods, we adopted the generalized estimating equation (GEE) model to examine the variable effects on adolescent mentalhealth status during their developmental stages. Table 3 shows that the variables of quarrelsome parents, frequent quarrelswith parents, severed friendship experiences, and cigarette/alcohol usage had a positive correlation with the PWB score overtime. Frequent quarrels with parents were the most crucial factors explaining adolescent PWB in the follow-up period, withan average 4.7 point increase in the PWB scale. Moreover, we observed various effects of the associated factors on the
[(Fig._2)TD$FIG]
20
25
30
35
FrequentOccasionalNever
Cigarette/alcohol use
Psy
chol
ogic
al w
ell-b
eing
sco
re
MaleFemale
B. Middle adolescent stage
A. early adolescent stage
20
25
30
35
FrequentOccasionalNever
Cigarette/alcohol use
Psy
chol
ogic
al w
ell-b
eing
sco
re
MaleFemale
C. late adolescent stage
20
25
30
35
FrequentOccasionalNever
Cigarette/alcohol use
Psy
chol
ogic
al w
ell-b
eing
sco
re
MaleFemale
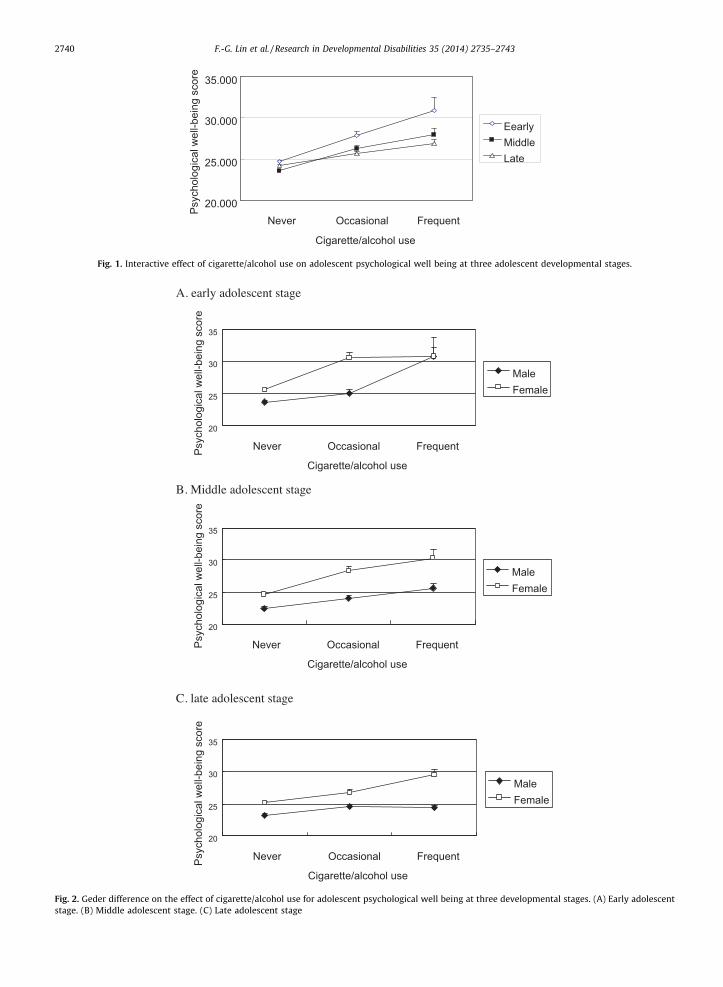
Fig. 2. Geder difference on the effect of cigarette/alcohol use for adolescent psychological well being at three developmental stages. (A) Early adolescent
stage. (B) Middle adolescent stage. (C) Late adolescent stage
[(Fig._1)TD$FIG]
20.000
25.000
30.000
35.000
FrequentOccasionalNever
Cigarette/alcohol use
Psy
chol
ogic
al w
ell-b
eing
sco
re
Eearly MiddleLate
Fig. 1. Interactive effect of cigarette/alcohol use on adolescent psychological well being at three adolescent developmental stages.
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–27432740
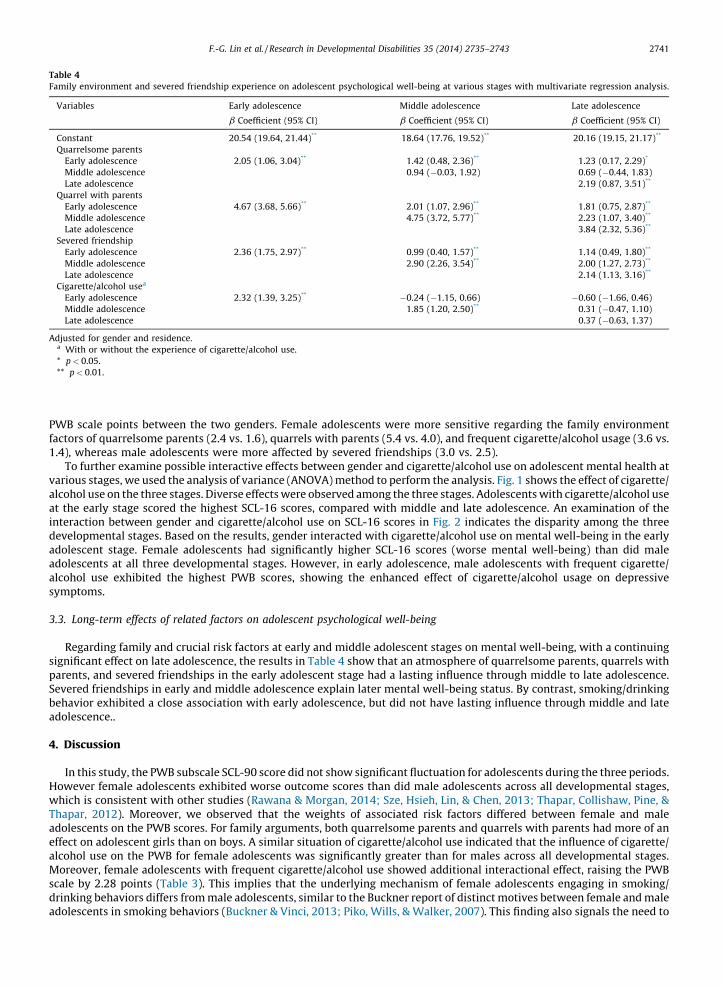
Table 4
Family environment and severed friendship experience on adolescent psychological well-being at various stages with multivariate regression analysis
Variables Early adolescence Middle adolescence Late adolescence
b Coefficient (95% CI) b Coefficient (95% CI) b Coefficient (95% CI)
Constant 20.54 (19.64, 21.44)** 18.64 (17.76, 19.52)** 20.16 (19.15, 21.17)**
Quarrelsome parents
Early adolescence 2.05 (1.06, 3.04)** 1.42 (0.48, 2.36)** 1.23 (0.17, 2.29)*
Middle adolescence 0.94 (�0.03, 1.92) 0.69 (�0.44, 1.83)
Late adolescence 2.19 (0.87, 3.51)**
Quarrel with parents
Early adolescence 4.67 (3.68, 5.66)** 2.01 (1.07, 2.96)** 1.81 (0.75, 2.87)**
Middle adolescence 4.75 (3.72, 5.77)** 2.23 (1.07, 3.40)**
Late adolescence 3.84 (2.32, 5.36)**
Severed friendship
Early adolescence 2.36 (1.75, 2.97)** 0.99 (0.40, 1.57)** 1.14 (0.49, 1.80)**
Middle adolescence 2.90 (2.26, 3.54)** 2.00 (1.27, 2.73)**
Late adolescence 2.14 (1.13, 3.16)**
Cigarette/alcohol usea
Early adolescence 2.32 (1.39, 3.25)** �0.24 (�1.15, 0.66) �0.60 (�1.66, 0.46)
Middle adolescence 1.85 (1.20, 2.50)** 0.31 (�0.47, 1.10)
Late adolescence 0.37 (�0.63, 1.37)
Adjusted for gender and residence.a With or without the experience of cigarette/alcohol use.
* p< 0.05.
** p< 0.01.
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–2743 2741
.
PWB scale points between the two genders. Female adolescents were more sensitive regarding the family environmentfactors of quarrelsome parents (2.4 vs. 1.6), quarrels with parents (5.4 vs. 4.0), and frequent cigarette/alcohol usage (3.6 vs.1.4), whereas male adolescents were more affected by severed friendships (3.0 vs. 2.5).
To further examine possible interactive effects between gender and cigarette/alcohol use on adolescent mental health atvarious stages, we used the analysis of variance (ANOVA) method to perform the analysis. Fig. 1 shows the effect of cigarette/alcohol use on the three stages. Diverse effects were observed among the three stages. Adolescents with cigarette/alcohol useat the early stage scored the highest SCL-16 scores, compared with middle and late adolescence. An examination of theinteraction between gender and cigarette/alcohol use on SCL-16 scores in Fig. 2 indicates the disparity among the threedevelopmental stages. Based on the results, gender interacted with cigarette/alcohol use on mental well-being in the earlyadolescent stage. Female adolescents had significantly higher SCL-16 scores (worse mental well-being) than did maleadolescents at all three developmental stages. However, in early adolescence, male adolescents with frequent cigarette/alcohol use exhibited the highest PWB scores, showing the enhanced effect of cigarette/alcohol usage on depressivesymptoms.
3.3. Long-term effects of related factors on adolescent psychological well-being
Regarding family and crucial risk factors at early and middle adolescent stages on mental well-being, with a continuingsignificant effect on late adolescence, the results in Table 4 show that an atmosphere of quarrelsome parents, quarrels withparents, and severed friendships in the early adolescent stage had a lasting influence through middle to late adolescence.Severed friendships in early and middle adolescence explain later mental well-being status. By contrast, smoking/drinkingbehavior exhibited a close association with early adolescence, but did not have lasting influence through middle and lateadolescence..
4. Discussion
In this study, the PWB subscale SCL-90 score did not show significant fluctuation for adolescents during the three periods.However female adolescents exhibited worse outcome scores than did male adolescents across all developmental stages,which is consistent with other studies (Rawana & Morgan, 2014; Sze, Hsieh, Lin, & Chen, 2013; Thapar, Collishaw, Pine, &Thapar, 2012). Moreover, we observed that the weights of associated risk factors differed between female and maleadolescents on the PWB scores. For family arguments, both quarrelsome parents and quarrels with parents had more of aneffect on adolescent girls than on boys. A similar situation of cigarette/alcohol use indicated that the influence of cigarette/alcohol use on the PWB for female adolescents was significantly greater than for males across all developmental stages.Moreover, female adolescents with frequent cigarette/alcohol use showed additional interactional effect, raising the PWBscale by 2.28 points (Table 3). This implies that the underlying mechanism of female adolescents engaging in smoking/drinking behaviors differs from male adolescents, similar to the Buckner report of distinct motives between female and maleadolescents in smoking behaviors (Buckner & Vinci, 2013; Piko, Wills, & Walker, 2007). This finding also signals the need to
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–27432742
focus more attention on female adolescents with cigarette/alcohol use. Regarding friendships, male adolescents were moresensitive to severed friendships than were girls.
For family environment, the frequencies of both family argument variables regarding arguments between parents andarguments with parents decreased as adolescents grew up, (from 10% to approximately 5%, Table 2), whereas the variablesshowed the continual significant importance of PWB during adolescence at all three stages. The summation of these twofamily argument variables increased adolescent scores on the PWB scales by an average of 6 points (approximately 0.8 SD),equal to adding 6 items or degrees of psychological symptoms (Table 3). Similar results also indicated that family argumentsor conflicts in early adolescence were crucial predictors of later psychopathy in adulthood. (Gunnlaugsson et al., 2011;Herrenkohl et al., 2009; Herrenkohl, Lee, Kosterman, & Hawkins, 2012) Our study further indicated the influence of familyarguments on PWB at early, middle, and late adolescence stages, and the long-term effect from early adolescence to youngadulthood. The result in Table 4 shows that the continued influence of quarrels between parents at the early adolescent stageinto the middle and late adolescent stages on PWB and experience in the middle stage also continue to significantly affectlate adolescents. This finding indicates that family arguments inversely affect adolescent mental health across thedevelopmental stages from early to late adolescence, and are worthy of focus to promote adolescent mental health. Inaddition, earlier experiences of severed friendships have a lasting effect for later PWB, indicating that adolescents valuedfriendships during their growth trajectory. The long-term effect implies that an earlier intervention prevention involving afamily and school context could take optimal advantages for promoting adolescent mental health.
Regarding adolescent smoking/drinking behavior, the rate of cigarette/alcohol use increased with age. Approximately10% of adolescents had cigarette/alcohol use experience in the early stage, 20% in the middle stage, increasing to more than30% in the late stage. The rapid rise of cigarette/alcohol use in middle to late adolescents might be because of the culturalbackground and legal rules that prohibit selling cigarette/alcohol to adolescents under 18 years of age. Although fewer earlystage adolescents exhibited cigarette/alcohol use, the effect of smoking/drinking on adolescent PWB was the most obvious atthis stage, compared with the other two stages. The results in Fig. 1 show the stage-specific influence of cigarette/alcohol usebetween the two genders. During the three developmental stages, female adolescents were more vulnerable than were maleadolescents from cigarette/alcohol use. In the early stage, the slope of cigarette/alcohol use on the PWB score was steeperthan the other two stages, whereas in the early stage, both genders showing frequent cigarette/alcohol use belonged to themost vulnerable groups, with the worst PWB outcome. This indicates that cigarette/alcohol use is harmful to mental healthas well as to physical health. From the evidence of neuroscience studies, Morales et al. observed that adolescents with even arelatively short smoking history were associated with significant brain structure change and later addiction (Morales,Ghahremani, Kohno, Hellemann, & London, 2014). Furthermore Petit, Maurage, Kornreich, Verbanck, and Campanella (2014)recently indicated the relationship between neurobiological damage and alcohol use in youths. Based on these findings,protecting adolescents from cigarette/alcohol exposure is crucial to promote their mental health. The results have importantreference value for the national cigarette/alcohol sale policy.
Although other studies have shown various risk factors on mental health for adolescents at different stages (Jaffee et al.,2002; Shanahan, Copeland, Costello, & Angold, 2011), our long-term analysis results using the GEE method reveal that familyarguments, severed friendships, and smoking/drinking behaviors continually affected the PWB status across alldevelopmental stages.
In the TYP, the measure of cigarette/alcohol use was combined for early and middle adolescents on the questionnaire,which may be because their sales to adolescents under 18 years of age is illegal, which makes it impossible to distinguish theindependent effect respectively on PWB. However, the investigation provides useful and critical messages for the long-termrepeated measurement on adolescent mental health status. Insufficient information regarding illicit drugs and othersubstance use data is limited in this study. The measurement of PWB from the simplified subscale SCL-90, the prevalence ofpsychological symptoms, and the effect of risk factors might be underestimated from the respondent self-reported surveymethod.
5. Conclusion
This research elucidated gender differences in the temporal relationships with cigarette/alcohol use and family andschool environments on adolescent PWB, and provided solid evidence of the significant influence of the earlierdevelopmental stage environment on adolescent mental health, such as family arguments, school friendships, and cigarette/alcohol use. Family arguments and severed friendships affect the mental health of contemporary adolescents and have long-term effects on adulthood. A preventive strategy to improve family and school environments at the early adolescent stage forenhancing PWB would be worthy to pursue.
Acknowledgements
Taiwan Youth Project data used in this study are available for public use and we applied for the research with the approvalof Academia Sinica in Taiwan (http://www.typ.sinica.edu.tw). We also gratefully acknowledged the instruction of Dr. Chin-Chun Yi for the TYP data.
F.-G. Lin et al. / Research in Developmental Disabilities 35 (2014) 2735–2743 2743
References
Barrera, A. Z., Torres, L. D., & Munoz, R. F. (2007). Prevention of depression: The state of the science at the beginning of the 21st Century. International Reviewof Psychiatry, 19, 655–670.
Bhatia, S. K., & Bhatia, S. C. (2007). Childhood and adolescent depression. American Family Physician, 75, 73–80.Buckner, J. D., & Vinci, C. (2013). Smoking and social anxiety: The roles of gender and smoking motives. Addictive Behaviors, 38, 2388–2391.Chang, H. J., Zauszniewski, J. A., Heinzer, M. M., Musil, C. M., & Tsai, W. C. (2007). Adaptive functioning and depressive symptoms in school-aged children. Journal
of Advanced Nursing, 60, 502–512.Chang, K., Chen, M., & Lien, T. (2007). A survey study of the prevalence of children depression in Taiwan. NTTU Educational Research Journal, 18, 29–72.Derogatis, L. R. (1983). Symptom checklist-90-R: Administration, scoring and procedures manual (second ed.). Baltimore: Clinical Psychometric Research.Erickson, S. J., Robinson, T. N., Haydel, K. F., & Killen, J. D. (2000). Are overweight children unhappy? Body mass index, depressive symptoms, and overweight
concerns in elementary school children. Archives of Pediatrics & Adolescent Medicine, 154, 931–935.Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2011). Structural models of the comorbidity of internalizing disorders and substance use disorders in a longitudinal
birth cohort. Social Psychiatry and Psychiatric Epidemiology, 46, 933–942.Freres, D. R., Gillham, J. E., Reivich, K., & Shatte, A. J. (2002). Preventing depressive symptoms in middle school students: The Penn Resiliency Program. International
Journal of Emergency Mental Health, 4, 31–40.Gilman, S. E., Kawachi, I., Fitzmaurice, G. M., & Buka, S. L. (2002). Socioeconomic status in childhood and the lifetime risk of major depression. International
Journal of Emergency Mental Health, 31, 359–367.Gilman, S. E., Kawachi, I., Fitzmaurice, G. M., & Buka, S. L. (2003). Family disruption in childhood and risk of adult depression. American Journal of Psychiatry, 160,
939–946.Gunnlaugsson, G., Kristjansson, A. L., Einarsdottir, J., & Sigfusdottir, I. D. (2011). Intrafamilial conflict and emotional well-being: A population based study among
Icelandic adolescents. Child Abuse & Neglect, 35, 372–381.Herrenkohl, T. I., Kosterman, R., Hawkins, J. D., & Mason, W. A. (2009). Effects of growth in family conflict in adolescence on adult depressive symptoms: Mediating
and moderating effects of stress and school bonding. Journal of Adolescent Health, 44, 146–152.Herrenkohl, T. I., Lee, J. O., Kosterman, R., & Hawkins, J. D. (2012). Family influences related to adult substance use and mental health problems: A developmental
analysis of child and adolescent predictors. Journal of Adolescent Health, 51, 129–135.Jaffee, S. R., Moffitt, T. E., Caspi, A., Fombonne, E., Poulton, R., & Martin, J. (2002). Differences in early childhood risk factors for juvenile-onset and adult-onset
depression. Archives of General Psychiatry, 59, 215–222.Jellinek, M. S., & Snyder, J. B. (1998). Depression and suicide in children and adolescents. Pediatrics in Review, 19, 255–264.Kessler, R. C. (2000). Psychiatric epidemiology: Selected recent advances and future directions. Bulletin of the World Health Organization, 78, 464–474.Lin, H. C., Tang, T. C., Yen, J. Y., Ko, C. H., Huang, C. F., Liu, S. C., et al. (2008). Depression and its association with self-esteem, family, peer and school factors in a
population of 9586 adolescents in southern Taiwan. Psychiatry and Clinical Neurosciences, 62, 412–420.Lue, B. H., Wu, W. C., & Yen, L. L. (2010). Expressed emotion and its relationship to adolescent depression and antisocial behavior in northern Taiwan. Journal of the
Formosan Medical Association, 109, 128–137.Mehler-Wex, C., & Kolch, M. (2008). Depression in children and adolescents. Deutsches Arzteblatt International, 105, 149–155.Mesman, J., & Koot, H. M. (2000). Child-reported depression and anxiety in preadolescence: I. Associations with parent- and teacher-reported problems. Journal of
the American Academy of Child and Adolescent Psychiatry, 39, 1371–1378.Morales, A. M., Ghahremani, D., Kohno, M., Hellemann, G. S., & London, E. D. (2014). Cigarette exposure, dependence and craving are related to insula thickness in
young adult smokers. Neuropsychopharmacology. http://dx.doi.org/10.1038/npp.2014.48 (Epub ahead of print)Pelkonen, M., Marttunen, M., Kaprio, J., Huurre, T., & Aro, H. (2008). Adolescent risk factors for episodic and persistent depression in adulthood. A 16-year
prospective follow-up study of adolescents. Journal of Affective Disorders, 106, 123–131.Petit, G., Maurage, P., Kornreich, C., Verbanck, P., & Campanella, S. (2014). Binge drinking in adolescents: A review of neurophysiological and neuroimaging
research. Alcohol and Alcoholism, 49, 198–206.Piko, B. F., Wills, T. A., & Walker, C. (2007). Motives for smoking and drinking: Country and gender differences in samples of Hungarian and US high school
students. Addictive Behaviors, 32, 2087–2098.Potochnick, S. R., & Perreira, K. M. (2010). Depression and anxiety among first-generation immigrant Latino youth: Key correlates and implications for future
research. Journal of Nervous and Mental Disease, 198, 470–477.Rawana, J. S., & Morgan, A. S. (2014). Trajectories of depressive symptoms from adolescence to young adulthood: The role of self-esteem and body-related
predictors. Journal of Youth and Adolescence, 43, 597–611.Schwartz, D., Gorman, A. H., Duong, M. T., & Nakamoto, J. (2008). Peer relationships and academic achievement as interacting predictors of depressive symptoms
during middle childhood. Journal of Abnormal Psychology, 117, 289–299.Shanahan, L., Copeland, W. E., Costello, E. J., & Angold, A. (2011). Child-, adolescent- and young adult-onset depressions: Differential risk factors in development?
Psychological Medicine, 41, 2265–2274.Sourander, A., Koskelainen, M., Niemela, S., Rihko, M., Ristkari, T., & Lindroos, J. (2012). Changes in adolescents mental health and use of alcohol and tobacco:
A 10-year time-trend study of Finnish adolescents. European Child & Adolescent Psychiatry, 21, 665–671.Sze, T. M., Hsieh, P. J., Lin, S. H., & Chen, I. J. (2013). Sex differences in the development of perceived family cohesion and depressive symptoms in Taiwanese
adolescents. Psychological Reports, 113, 1066–1084.Thapar, A., Collishaw, S., Pine, D. S., & Thapar, A. K. (2012). Depression in adolescence. Lancet, 379, 1056–1067.Wang, W. C., & Wu, C. I. (2003). Scaling issues in longitudinal studies: The symptom checklist-90-revised as an empirical example. Formosa Journal of
Mental Health, 16, 1–30.Wu, W. C., Kao, C. H., Yen, L. L., & Lee, T. S. (2007). Comparison of children’s self-reports of depressive symptoms among different family interaction types in
northern Taiwan. BMC Public Health, 7, 116.WHO (2012). Adolescent mental health. http://www.who.int/mental_health/resources/child/en/Yi, C. C. (2013). The psychological well-being of east Asian youth. New York: Springer, ISBN: 9400740808.