Embed Size (px)
Citation preview

Short Review of Chapter One’s Concepts:
1. Toxic stress which leads to adult onset disease processes and child maltreatment are large,
messy public health problems exacerbated by disciplinary fragmentation.
2. This fragmentation is fueled by different fiscal streams that fund different diagnostic
categories that follow linear research models which are reductionistic.
3. The Neurorelational Framework (NRF) aligns with the National Institute of Health and National
Institute of Mental Health shifts in the United States that support the addition of nonlinear
and dynamic systems perspectives to theory, research, and practice. Systems science models
hold complexity and the NRF is a complexity framework being evaluated with several types of
systems science models.
4. The professional and personal experiences of fragmentation (CML) became the impetus to
create a more complex theory base using the brain as a template, which was cocreated
between Drs. Lillas & Turnbull for interdisciplinary practice. From there, three clinical steps
have emerged, which are housed in this manual, further translating brain science into clinical
practice for practitioners and parents alike.
5. Due to the NRF being neurodevelopmentally sensitive, the NRF is a “valueadd” for any
existing EvidenceBased Treatment. It is designed to be used in conjunction with the term
EvidenceBased Practice (EBP). An EBP was defined by the Institute of Medicine as a decision
making process that includes the best of research, clinical wisdom and expertise, along with
family values and cultural sensitivities.
Chapter Two The NRF Green Tree Manual
Big Picture Concepts in Using the NRF’s Three Steps
A short summary and additional reading: This chapter is meant to bring to you the Big Picture and
Large, Global concepts of the NRF. The best way to get the “big picture”of the NRF is to read Chapter
12 of the NRF textbook in conjunction with this chapter in the NRF manual. The NRF is this
whole/part/whole framework and it seems wise that folks have an orientation to the whole before it’s
broken down into smaller pieces. This chapter also provides an orientation to the whole of the manual
and its structure. As this manual is being written and rewritten, this particular chapter is subject to
change. In addition, please read the FAQ on the www.nrfgc.com website along with this chapter.
Overview of the Manual
Three Steps, Early Learning Phase
We introduced the most basic of the three steps and their correlation with three key concepts in
Chapter One. The NRF is a wholetoparttowhole framework and uses the metaphor of a tree to hold
its three clinical steps. Here in this chapter, we begin with a light overview of the three components to
the tree (whole), and then will move into each part (roots, trunk, & branches) as the manual
1

progresses. However, before we begin cycling through the first three steps, you will see that the NRF
Manual begins with a global review of ourselves as practitioners and our historical roots as
professionals in Chapter #3. This reflects the philosophy of NRF practice that integrates Reflective
Practice as part of our core value system and honors the use of ourselves as well. The field of Infant
Mental Health recognizes several essential elements involved in Reflective Practice; these will be
introduced early on in Chapter Three and linked with NRF concepts as well.
The first time we cycle through the roots, trunk and branches, Phase #1, we will give you core information that allows you to get started using the NRF. These will follow in sequential order, with
chapter 4 (roots), chapter 5 (trunk), and chapter 6 (branches). We consider this the “first phase” of
the NRF’s information. Some of you are using this manual in a “selfguided” manner – learning and
practicing the concepts as you go along. Others of you are in a NRF training course with myself or a
NRF trainer. With the Early Phase beginning level of information we expect a practitioner to be able
to do a NRF Early Phase Assessment Form using Step #1 and Step #2, and aspects of Step #3. Step #3
holds the most complexity to it, so the use of Step #3 will be at a macro level in conjunction with using
the History Worksheet. Depending on how much one procedurally practices using these steps, one
will be able to use the three steps with a family in an ongoing manner at this basic level that certainly
includes the early assessment phase, and also may bring some intervention principles into the
context.
Three Steps, Intermediate Learning Phase
For those of you that want to continue learning more levels of the NRF, one can then begin a second
rotation of the three steps, the Intermediate Learning Phase, now with intermediate knowledge and
information of the three steps. Again, this will occur in linear order with chapter 7 & 8 (roots), chapter
9 (trunk), and chapter 10 to 13, a chapter for each brain system (branches). By the completion of the
Intermediate Learning Phase 2, a practitioner should have a really solid grasp of the NRF and be able
to use it not only for assessment but also for intervention. Those interested in using the NRF’s three
clinical steps on a daily basis will be able to use the NRF with enough support and reflective practice at
the end of this phase. At the same time, fidelity measures are provided for selfreflection in concert
with a mentor’s reflection on where one is in his or her learning phases so that one’s perception of his
or her use of the NRF needs to be matched with feedback from others along with his or her own
families.
Three Steps, Advanced and Research Learning Phase
The next rotation of the three steps, the Advanced Learning Phase, is the advanced and research level
of knowledge and work within the NRF. This will occur in similar fashion, rotating through the
advanced material of the three steps. These NRF practitioners will use an advanced level of Reflective
Practice and cultural awareness and integration regarding their cases. This Phase is particularly
sensitive and linked to the NRF research protocol (Chap 14, 15, 16). Thus, once these practitioners
complete their tasks for this Phase, an option for this type of practitioner is for him/her to also
2
become a part of the team collecting data for research team depending upon his or her mastery of
the NRF. Fidelity measures for the research protocol will also be integrated so that there is continuity
of how data is collected for our research studies. For those grant projects that include a Train the
Trainer component, it is hoped that this phase will be reached. However, it is not essential that
emerging NRF Trainers are all participating in data collection.
Three Steps, Synthesis Learning Phase
This Learning Phase, contains concepts that integrate and create a synthesis of the three steps. At this
point, there is enough knowledge of the three steps that one can “play” with them in in a nonlinear
fashion (Chap 17). In particular, there is enough synthesis that one can use the NRF’s three steps to
locate the strengths of any EBT to match with a parent/child dyad/family and conversely, assess
where an EBT may not be the best match (some may be able to some of this at intermediate stage!).
The ability to use hybrids of EBT’s occurs at this level, creating a clinical protocol that informs the
family of their choices and explains the strengths and compliments as to what is needed based upon
the assessment process that includes the parents’ concerns, the practitioner’s knowledge of
development, and a collaborative process between the parents and practitioner is expected.
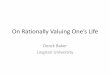
The following grid shows us the relationship of the steps and the Phases.
NRF’s 3 Steps and 4 Phases Phase 1 Early Learning Phase
Phase 2 Intermediate Learning Phase
Phase 3 Advanced/Research Learning Phase
Phase 4 Synthesis Learning Phase
NRF Informed Practitioner
NRF Practitioner NRF Research Practitioner
NRF Trainer and/or Mentor
ROOTS Step 1: Physiology, SleepAwake Cycle: Colors
ROOTS Step 1: Heart, Hand, & Head
ROOTS Step 1: Inside & Outside Cues: Physiological Sensed Data Equipment; use of MIT wristband with children and parents
Pulling the 3 Steps Together Nonlinear use of the Step 1, 2, and 3 Use with Interand Transdisciplinary Teams Can use NRF to map out any EBT and to match with parent/child dyad
TRUNK Step 2: Levels of Engagement: Pyramid
TRUNK Step 2: Levels of Engagement: SE Grid with Rating Scale of 6
TRUNK Step 2: Levels of Engagement: Grid with Rating Scale of 6, Use with any dyad
BRANCHES Step 3: Macro level of the 4 Brain Systems:
BRANCHES Step 3: Micro level of the 4 Brain Systems:
BRANCHES Step 3: Micro level of the 4 Brain Systems:
3

The Four Stories, the History Worksheet, & Purple Wheel
Early Phase Assessment form that includes the Current Functional Capacities Worksheet
Trigger & Toolkit Menu, Mapping Broadly, Mapping with Self & Coregulation. The use of the NRF phone App with children and parents.
Fidelity Measures
Fidelity measures exist for the parents to measure their NRF practitioners with and for the NRF
practitioners to measure themselves with in conjunction with learning the NRF. These are required of
a NRF Mentor/Trainer. The measures are specific to the clinical use of one’s Heart, Hand, and Head –
and the three clinical steps.
In addition, there are cultural awareness questions that are integrated into the use of the NRF that
complement an awareness of ourselves and our families. These will unfold along with the NRF’s three
steps.
Who Benefits from the NRF?
We believe that everyone, any age, can benefit from the NRF’s three steps. The fact that our NRF
research team is focusing on the birth to five year old children and their parents as a place to begin,
the NRF can often be thought of as a “birthtofive” year old treatment only. This misunderstanding
also occurred when the NRF’s original textbook was written. The confusion stems, in part, from the
fact that the neuroscience and science we included in our original book was written in particular for
the birth to five year old population. The original book's title was very much weighted towards this
age group as well. While there is no denying that this is our emphasis, what is often hard to convey is
that the NRF applies to all ages because it is specifically oriented to give you a deep picture into the
neurodevelopmental profile and relational capacities of any aged person. This is one of the very
concerns mentioned in Chapter One, that one of the traps of any particular EBT is that it has often
been geared to a particular age group or diagnostic category. We hope to gather data across age
groups and across many diagnostic profiles. This is a guide for any aged group and specifically a
treatment for parents and their children. While many parents are adults, there are those that are teen
parents as well. From our point of view, this is all the better, because this increases our age span of
those we are working with. By virtue of working with parent/child dyads, even if the child in the dyad
is a birth to five year old, we are by the very nature of the treatment, treating teens and adults at the
same time.
4

Who Can Use the NRF Professionally?
We have a wide range of professionals using the NRF in the context of the setting they work in. Most
common at this point are MA to Doctoral level providers. However, we anticipate that some of the BA
level practitioners will be involved in the prevention and promotion aspect of trainings. Some
communities are intentionally using a “Promotion to Detention” lens, in order to create a wide range
of practitioners that can work together.
Who Can Benefit From Using the NRF?
There is something for “everyone” in the use of the NRF. We believe a teen parent or high school
student can learn to use the “colors” in Step 1 and the “pyramid” in Step 2. One does not have to use
all three steps in order to find something of value and importance that one can learn and apply to
oneself, his or her relationships, and his or her community.
For those communities that want more formal practitioner training and skill with the three steps, the
NRF will lay out the Phases with their requirements. These requirements are currently being worked
on by a small group of NRF Trainers/Practitioners.
Overview of the Tree Metaphor
The tree progresses in a linear order, from the “bottomup” from the roots to the branches. Both
nature and nurture are needed to grow deep roots (healthy stress responses and stress recovery), a
strong trunk (healthy serve and return engagement with positive procedural memories) and lush
branches (healthy brain architecture).
The intersection of nature and nurture – known as epigenetics – entails how genes get expressed
through lived experiences. This interaction can be seen as occurring between the seeds (as the
genes/nature), with the quality of the soil and the amount of sun, water and wind
(environment/nurture). Of course, there are multiple ways that these variables can interact with each
other. In a simple way of viewing these intersections, at least three points on a continuum could be
viewed as markers. At one end, a healthy seed with generous amounts of healthy soil, sun, and water
would lean towards a sturdy tree. This is not to assume that challenges to the tree are not healthy. In
fact, the opposite is true. Living through storms and the four seasons are all a part of the building
sturdiness. Case example, CAH
5

In the middle of the continuum, there might be a vulnerable seed that will need a healthy surrounding
ecosystem to support it. With nourishing soil, sun, and water that matches the needs of the seed,
the seed can reach its potential as a tree. My experience with my malnourished preemie twin boy is
an example of that. His relational environment was nourishing and his access to intensive early
intervention services the first five years of his life were pivotal. I’m happy to say that at age 21, he’s a
thriving young adult whose college major is a combination of social justice with community
development and in particular, communities where child hunger and homelessness predominate. I
believe his tie with world hunger and in particular, children who are hungry, is a procedural link with
his own malnourishment. I often remark in amazement and with gratitude that my young toddler boy
who couldn’t manage a transition from the house to the car without falling apart is now a comfortable
world traveler, living for long periods of time in impoverished communities. If anyone got worried
when you read about the predictors of his being a sociopath based upon his violent behavior at age 3,
you can be relieved to know that this was not his trajectory. This is not to say that he has no struggles
and his vulnerabilities left no marks. His body height and weight is smaller than his brother’s and
always will be. His body is more vulnerable to experiencing fatigue and his paying attention to his
sleep cycle is essential. He has moments of social anxiety and he continues to work on this aspect of
his gaining comfort with this challenge.
Or, conversely, a healthy seed with mild to moderate adversity may end up thriving as well, as long as
there are sources of resilience along the way. example, CAH
6
At the other end of the continuum, the metaphors of a drought, flood, hurricane, tornado, or fire
imply a harsh and tumultuous environment that would be akin to the work described by the adverse
childhood experiences. Of course, the more vulnerable the seed is, in a harsh environment, the more
likely the “double jeopardy” of this interaction effect could lead to a tree with damage.
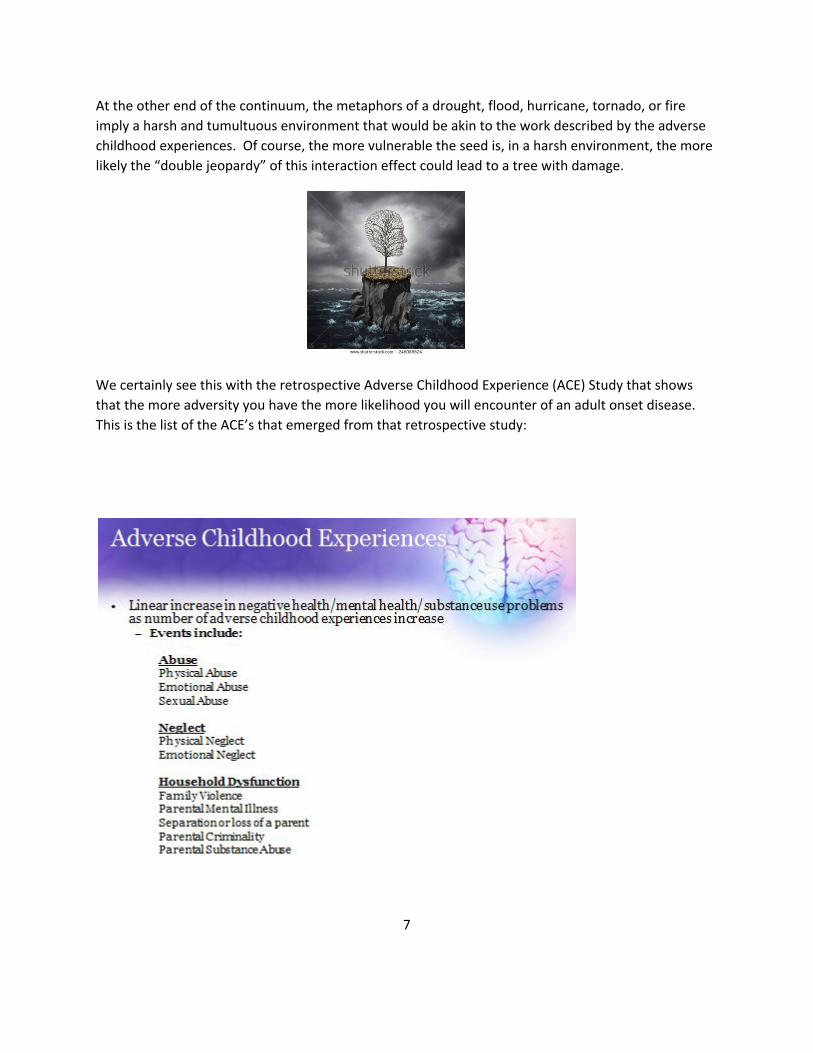
We certainly see this with the retrospective Adverse Childhood Experience (ACE) Study that shows
that the more adversity you have the more likelihood you will encounter of an adult onset disease.
This is the list of the ACE’s that emerged from that retrospective study:
7

These statistics emerge with an ACE score of 4 or more (the New Yorker, on Adrianne Burke, 2011).
For those of you more interested in longitudinal studies, Bruce McEwen’s work done on allostatic
load, known as toxic stress, leads to these similar outcomes as well. The four toxic stress patterns will
be discussed in Chapter 4 (a resource text on “allostatic load” is the original NRF textbook, especially
chapters 2 and 4/5).
8

As mentioned, all in all, my malnourished twin boy has fared fairly well, given his toxic in utero
environment. However, what would have happened if he had been raised in a hostile environment?
(maybe pull in here the link that premature boys are more likely to do poorly in homes with emotional
distress). The intensity and duration of his distress could have put him at risk for child abuse. It is
through this experience of his inconsolability that I developed respect and empathy for parents who
do harm their children under duress. I had never understood child abuse before and I don’t claim to
know it in its entirety. Yet, when I was brought to my knees as a parent, in the context of being
blessed with such internal and external resources, I understood the capacity to harm. It was
disconcerting to feel these feelings and I was taken aback by them. The feeling of, “There but for the
grace of God go I” was present. This humbled me and it is the reason why I donate a significant
amount of volunteer time to child welfare reform and the development of NRF court teams.
The Linear Progression to the Tree and the Links with the NRF’s 3 Steps
Location and health of each part of the tree and links with clinical concepts
Step #1 = deep or shallow roots = an individual’s sleepwake states of arousal
Step #2 = short or long trunk; thick or thin trunk = the back and forth “serve and return” levels of
engagement
Step #3= lush or pruned branches = an individual’s brain architecture and brain networks
9
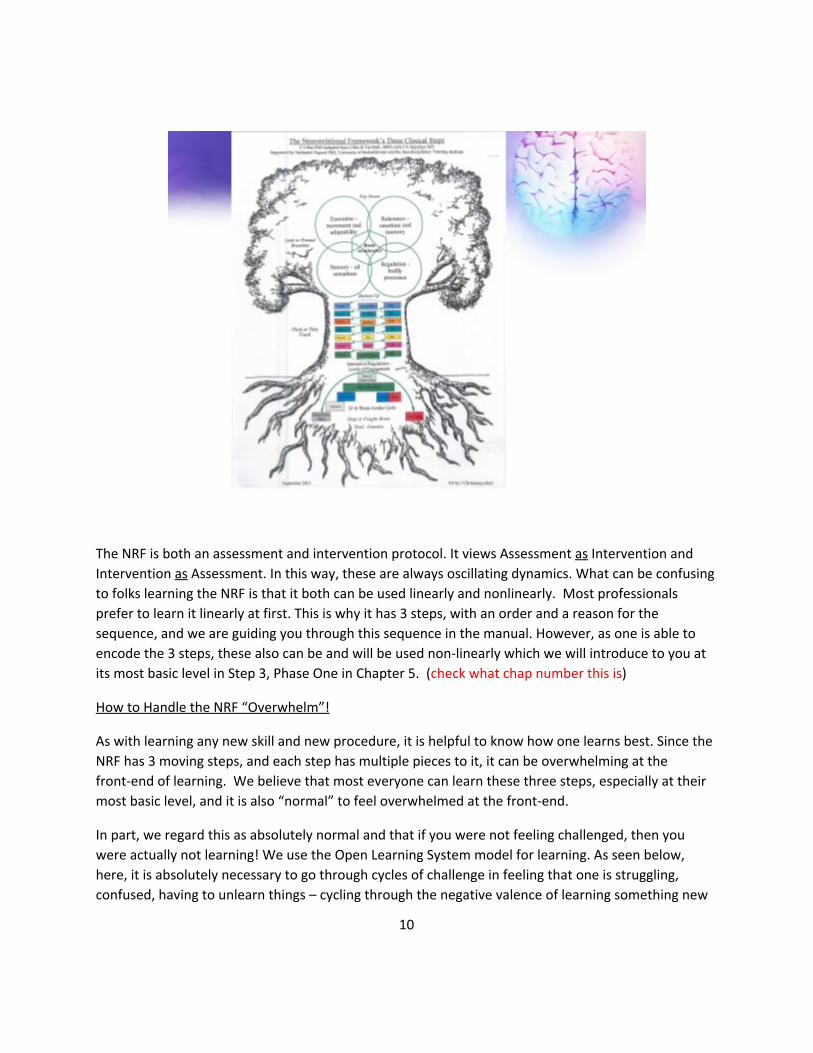
The NRF is both an assessment and intervention protocol. It views Assessment as Intervention and Intervention as Assessment. In this way, these are always oscillating dynamics. What can be confusing
to folks learning the NRF is that it both can be used linearly and nonlinearly. Most professionals
prefer to learn it linearly at first. This is why it has 3 steps, with an order and a reason for the
sequence, and we are guiding you through this sequence in the manual. However, as one is able to
encode the 3 steps, these also can be and will be used nonlinearly which we will introduce to you at
its most basic level in Step 3, Phase One in Chapter 5. (check what chap number this is)
How to Handle the NRF “Overwhelm”!
As with learning any new skill and new procedure, it is helpful to know how one learns best. Since the
NRF has 3 moving steps, and each step has multiple pieces to it, it can be overwhelming at the
frontend of learning. We believe that most everyone can learn these three steps, especially at their
most basic level, and it is also “normal” to feel overwhelmed at the frontend.
In part, we regard this as absolutely normal and that if you were not feeling challenged, then you
were actually not learning! We use the Open Learning System model for learning. As seen below,
here, it is absolutely necessary to go through cycles of challenge in feeling that one is struggling,
confused, having to unlearn things – cycling through the negative valence of learning something new
10

in order to then to get positive valence of the learning cycle wherein one “gets it” and then feels
energized and renewed with new vigor for repeating the cycle all over again! We view this as an
organic process that one will go through in terms of the phases of learning the NRF. We are hopeful
that when one gets to the “discouraged” part of the cycle that one will reach out to a colleague for
help and that one is learning the NRF in the context of some type of community – where learning
happens best!
At the same time, some practitioners have struggled mastering the NRF’s three clinical steps. We
want to pause to mention that mapping oneself will give you some clues as to why this may be more
difficult for some more than others. For example, there are some great practitioners, with great
intuition, yet the extra hard work may point to a version of ADHD, a processing speed issue, or a
working memory glitch that can make the parttowhole effort a challenge! For these practitioners,
there may be more challenge involved in encoding and following the sequence. While there are only
three steps, there is a lot of information packed into each step. For this practitioner, one might need
more repetition or tutoring support. Several folks have repeated the study groups in order to encode
more information with greater detail during the next round of repetition. As a NRF community we
recommend reflective practice as a lifelong endeavor. Getting additional support from a NRF tutor or
creating your own NRF community for peer reflection is strongly recommended for the ongoing
learning process.
For some, it may be best for you to feel you have mastery over Step #1, so you may want to learn all
the parts to Step #1. For others, they may want to learn the beginner’s level of all three Steps and
11
then rotate back for intermediate and advanced knowledge within those three steps. This way of
sequencing your learning, by rotating through the three steps, is our recommendation. This is how
the manual is laid out and organized how we recommend mastering the NRF, so that you are learning
how to hold the 3 steps in mind and you begin to see the interlocking connections between them.
The rationale behind the linear order of the three steps is this. The sleepwake cycle is the foundation
to one’s nervous system adaptive functioning. Thus, it has been given the status of the “roots” to the
tree and it carries a lot of “weight” in the NRF as Step #1. It is first in the lineup because one has to
have sound deep sleep during the sleep cycle to have robust states of arousal during the awake cycle.
With sleep as the background, then, one has to have a stable enough green zone when awake in order
to be able to engage in the “serve and return” cycles (which is Step #2). Once one has mapped out the
duration, intensity, and frequency of each of the sleepwake states of arousal in Step #1, one can
pretty quickly tell how far up the levels of engagement and how high up the trunk of the tree one
might be able to get in Step #2. In other words, if in Step #1 you find yourself looking that the odds
are that the child and/or parent are in a toxic stress pattern, you automatically know that they likely
cannot get very far up the relational trunk of the tree without much support. Even if they can go
quite a ways up the trunk of the tree, the “thickness” of their cycles of engagement may not be as
robust as we’d want them to be for optimal health or at an ageappropriate level. At the very same
time, you also immediately know that these states of arousal carry a lot of functional capacities in the
first brain system – Regulation in Step #3. Thus, once you have mapped out Step #1, you have a lot
of information that gives you hunches about Step #2 and actually quite a bit of information about
both the Regulation and the Relevance Systems in Step #3.
From a metaphorical perspective, the depth or shallowness in the roots support the growth of the
trunk of the tree becoming short or long and thick or thin, and both the roots and the trunk lead to
lush or pruned branches. A cascade effect begins to happen; one area of growth directly influences
the other. When there is toxic stress in Step #1, it can corrupt the existing branches to the tree –the
brain architecture represented in Step #3. Weak levels of engagement in the trunk of the tree, not
only lead to a “thin” trunk (Step #2), they do not provide the necessary “serve and return” levels of
engagement for the firing and the wiring of the brain networks (Step #3). Perhaps one can already
capture a sense as to how these are all mutually influencing each other, which makes this also a
nonlinear process.
Overview of Trees Via Growing Relationships and Communities
The metaphor of a “tree” implies an individual. The metaphor of “trees” can project a cluster of trees,
such as in a family system, or trees in a forest, such as in a community. A particularly powerful
metaphor is an Aspen Forest – these are all interconnected trees. (? More on this). For example, the
root system in the trees below, show the thick interconnection of the roots, with close proximity to
each other’s trunks and branches. From a family system’s perspective, we believe that trees can be
ingrown, overgrown, and too connected (enmeshed), as well as spread too far apart (disengaged).
12
NRF Communities
A NRF community is defined by its commitment to crosssectored training of at least two distinct
disciplinary boundaries in the use of the NRF’s three steps for a common language and a shared
approach. While one sector that includes multiple disciplines, such as an Early Intervention center
that work with developmental disabilities may begin using the NRF, usually there are at least two or
more funding sectors involved in the NRF training community. Some groups begin without having a
prior relationship with each other, are invited to apply, and then chosen across sectors within a close
enough zip code range, with the hope that the future connections will evolve over time.
We are learning from each NRF community how to best engage in the process of creating them. We
are still in an early phase of working with five communities, having begun several NRF communities
within last two years. We have had two primary different approaches to gathering together
communities. One approach has been to invite practitioners across all five sectors, many of them
individuals working at various agencies, centers, hospitals, or private practice sectors, not necessarily
knowing each other at the frontend. Another approach has been to work with an existing agency,
center, or hospital and to send teams from within that particular entity. We will be analyzing the
Social Network Data (see below) from these different types of communities to see which communities
are experiencing the most dynamic systems change and with which format.
At this juncture, while still too early for a definitive answer, it seems it might be best to invite a
crosssection of agencies to the table, wherein they send a team of practitioners to the training – not
just one person. It seems that there may be an advantage to inviting 3 to 4 practitioners from each
agency so that there is a team that can influence systems change back at the agency itself. If there is a
second round of funding, that first cohort can be asked to participate in sculpting the invitations to
the second group. Specific practitioners are chosen from agencies that are known to them so that the
teams grow more organically – from whom practitioners already share cases with. During this second
13

round of training, teams from agencies could be invited so that systems change can happen more
readily with a group of folks within the same agency.
The use of a Social Network Analysis Survey is how we are tracking the system’s changes over time
with each community. We are hopeful that as each community grows, that there will become either
one or two obvious formats for beginning NRF communities that becomes standardized or
recommended.
For example, the Alaska cohort has been a singular sector that includes a wide range of disciplines and
has been small in numbers. We are happy to show that even a small team, can make a big difference.
This cohort began with 15 members and at the end of the first year of training, had 10 who finished
the second year of NRF practice. The attrition was accounted for by four members who moved out of
state, accompanied by overlapping variables such as those overly committed timewise and unable to
continue. Here you see the interactions across the state of these 10 members:
With the four NRF practitioners (the four black nodes) within an agency of 31, you can see in this next
picture how those that shared cases were beginning to use the language of Step 1 with their cases.
14

The thickness of the lines communicate the degree of frequency as well as the degree of importance
folks placed on their relationship with the other practitioner. Here, you see that the thickness of Step
#2 is more prevalent, seeing the frequency of using Step #2 language is even more than Step #1.
15

This next picture shows that Step #3 is the least shared language that this community now uses. This
has inspired the NRF practitioners to really focus on Step three this coming year! With a small team
that really learns the NRF, the inspiration to share it can come rather organically and once that
happens, a whole agency can be changed in its ability to begin to share concepts, language, and goals
for families they work with. Slowly but surely, systems change begins to take place.
Node number one is a Reflective Practice supervisor. She was inspired to selforganize an open
reflective practice group for anyone at the agency that wanted to increase his or her reflective
capacities, especially with cases where the practitioner was getting triggered with a stress response.
This next picture shows her relationships with various team members and her use of Step 1, 2, and 3.
PLACE HERE
Not only is it possible to change an agency’s culture, it’s possible to have the NRF “spill over” into the
community. The second agency team in Alaska, from Sprout agency located in Homer, already had
existing relationships prior to their NRF training. One day, one of the birth mothers who had been
working with a NRF therapist, went to her child welfare meeting, telling herself to “stay green.” The
mother had a successful, albeit stressful meeting. One of the child welfare social workers overheard
this mother referring the term “staying green” and asked the NRF therapist what she was referring to.
This opened the door for the two NRF therapists from Sprout to begin to share Step One – sharing the
colors and information about adaptive versus toxic stress. This is how each NRF therapist (a mental
16

health and occupational therapist practitioner) began to share the NRF’s steps to their community
members.
SNA Outside
Before this, the NRF practitioners had also been sharing the NRF with their colleagues within their
agency. Over time, they became very confident in taking the lead in using the NRF for reflective
practice which was used on a weekly basis with all staff members. Here we see this “in action” with
this SNA.
SNA Inside
17
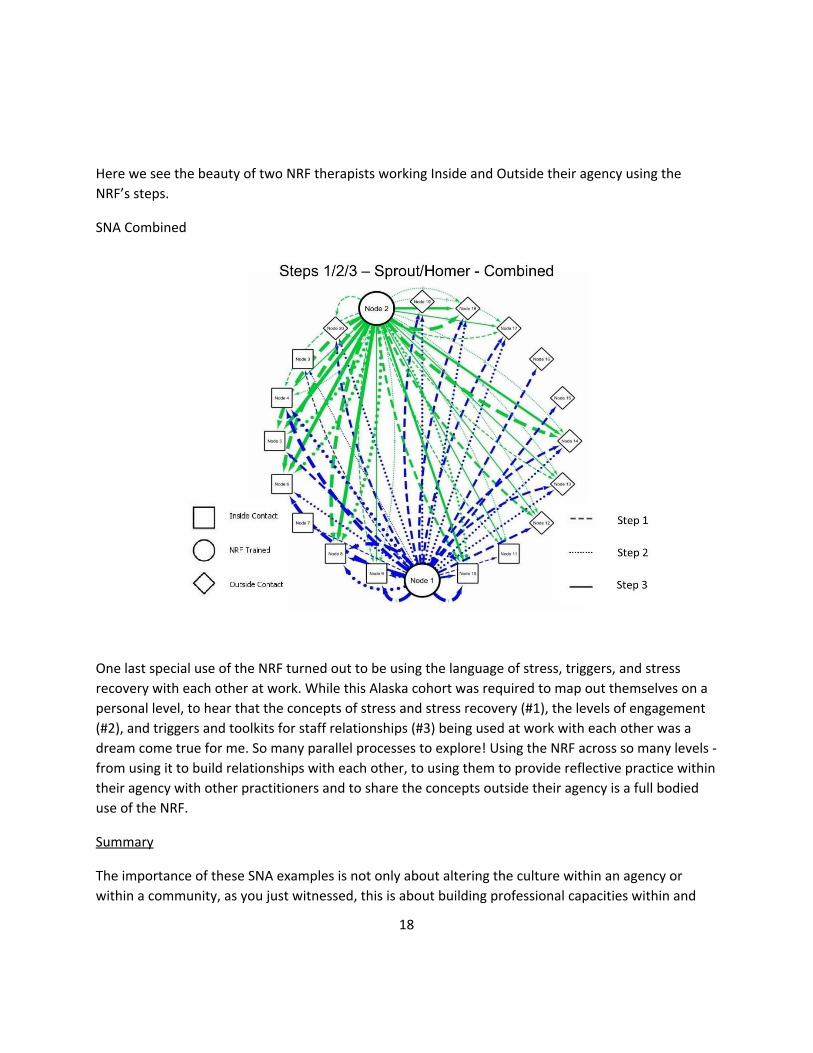
Here we see the beauty of two NRF therapists working Inside and Outside their agency using the
NRF’s steps.
SNA Combined
One last special use of the NRF turned out to be using the language of stress, triggers, and stress
recovery with each other at work. While this Alaska cohort was required to map out themselves on a
personal level, to hear that the concepts of stress and stress recovery (#1), the levels of engagement
(#2), and triggers and toolkits for staff relationships (#3) being used at work with each other was a
dream come true for me. So many parallel processes to explore! Using the NRF across so many levels
from using it to build relationships with each other, to using them to provide reflective practice within
their agency with other practitioners and to share the concepts outside their agency is a full bodied
use of the NRF.
Summary
The importance of these SNA examples is not only about altering the culture within an agency or
within a community, as you just witnessed, this is about building professional capacities within and
18
across a state or a large region. What makes Alaska’s Leadership Team unique, is a portion of the
team are involved on the state level. In addition, the NRF AK Leadership team and NRF Facilitators
were chosen specifically due to their being Alliance Endorsed Reflective Supervisors so that
professional development could be maximized. This supports their having a “big picture” view of
growing professional capacities for Infant Mental Health Specialists and Reflective Practice
Supervisors through the Endorsement Process across the state.
Future Visions
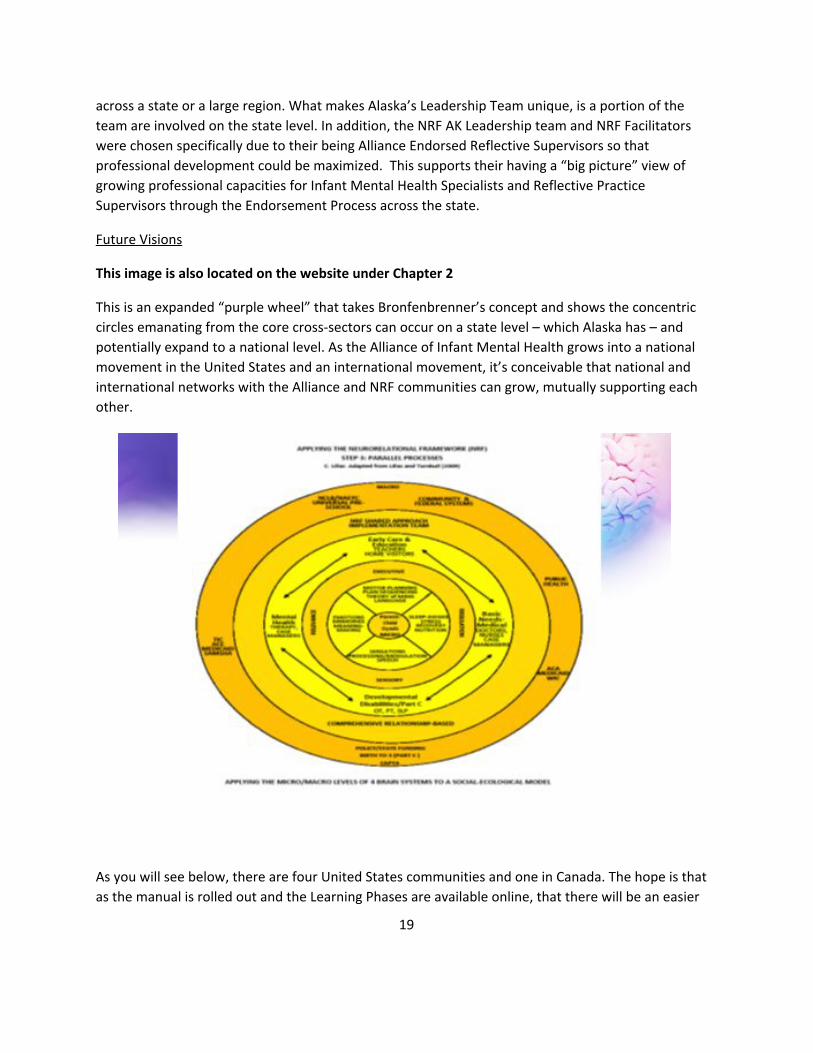
This image is also located on the website under Chapter 2
This is an expanded “purple wheel” that takes Bronfenbrenner’s concept and shows the concentric
circles emanating from the core crosssectors can occur on a state level – which Alaska has – and
potentially expand to a national level. As the Alliance of Infant Mental Health grows into a national
movement in the United States and an international movement, it’s conceivable that national and
international networks with the Alliance and NRF communities can grow, mutually supporting each
other.
As you will see below, there are four United States communities and one in Canada. The hope is that
as the manual is rolled out and the Learning Phases are available online, that there will be an easier
19

access for both grantdriven communities to arise as well as individuals or a shared team of
professionals across international communities to learn the NRF. With a dynamic systems approach
at our core, there is the possibility that a worldwide web of practitioners across disciplines will
continue to selforganize, emerge, grow, and influence each other for years to come. Each NRF
community has built into it NRF Facilitators that hold a Leadership position. As those Facilitators grow
in using the NRF, there is always the option that they will expand into transferring their knowledge
into their agency and into their community as we just saw. The goal is to always establish a NRF
Leadership team that is embedded within the community, so that the NRF training and reflective
practice continues to grow in a distributed fashion. The NRF Facilitators and Leadership teams across
each NRF community share in a Learning Collaborative call on an every other month or trimester
basis. This contributes to an ongoing and open learning system wherein we learn from our successes,
barriers, and missteps, always learning from each other and improving how we learn together.
Introducing the NRF’s five communities present at this time.
NRF Communities in 2016 Alaska Central Valley CA Canada Seattle Wisconsin PIC team in Anchorage Contact: Christy McMurren
Contact: Cassandra Joubert
Contact: Carole Anne Hapchyn
Contact: Magan Cromar Wendy Harris
Contact: Connie Lillas
Sprout team in Homer Contact: Jill Lush or Jackie Eisenberg
Fresno Team #1 Private Practice, 2 infant psychiatrists
East King Milwaukee, Prevention
Fresno Team #2 NICU MLK South Milwaukee, Detention
Merced Glenrose Rehabilitation Hospital
Waupaka County
Madera Tulare/Kings
20

For those of you interested in meeting the existing NRF communities, please go to www.nrfgc.com
and go to the NRF Communiites tab. There you will find a Poster Board on most NRF communities that
highlight aspects that are unique to each community. The NRF communities presented a poster board
workshop at the World Association for Infant Mental Health in Prague, May, 2016. The video clips of
these presentations are there for your review as well.
Overview of the Uses of the NRF
We are aware that there are folks who carry different roles in each NRF community. Thus, we have 4
groupings that we have come up with at this point that help professionals identify the work they do
and how they can use the NRF. We like to have professionals identify which group(s) they belong to.
Often one belongs to more than one group. During the course of NRF instruction, if you are a
community wherein the training is live, we hope to have folks get together that belong to a similar
group so that they can share their work, successes and barriers with others. Keep in mind that
different aspects of your professional roles may pull you towards the early, intermediate, or research
phases of the NRF.
Groups 1 to 4:
Group 1 Frontend Assessments Only
Group 2 Ongoing Assessment & Intervention
Group 3 Attend Community Group Meetings,
Group 4 Supervisor/Consultant
21

Community Leader, Trainer
22