Embed Size (px)
Citation preview

Short Implants in Maxillaeand Mandibles: A Retrospective StudyWith 1 to 8 Years of Follow-UpEduardo Anitua*† and Gorka Orive†
Background: The aims of this study are to evaluate thelong-term survival rates of short dental implants in posteriorareas in both jaws and analyze the influence of different factorson implant survival.
Methods: A retrospective cohort study design was used. Sixhundred and sixty-one patients received 1,287 short implants(<8.5 mm) between 2001 to 2008 in Vitoria, Spain. All implantinstallations were performed by two experienced surgeonsand rehabilitations were done by three prosthodontists. Eachimplant failure was carefully analyzed. The potential influenceof demographic factors, clinical factors, surgery-dependingfactors, and prosthetic variables on implant survival was stud-ied. Implant survival was analyzed using a life table analysis(Wilcoxon [Gehan] test).
Results: The overall survival rates of short implants were99.3% and 98.8% for the implant and subject-based analysis,respectively. The mean follow-up period for the implants was47.9 – 24.46 months. A total of 9 out of 1,287 implants werelost during the observation period. None of the variables studiedresulted in statistical association with implant failure because ofthe low number of failures.
Conclusion: Results of the present retrospective study showthat treatment with short implants can be considered safe andpredictable if used under strict clinical protocols. J Periodontol2010;81:819-826.
KEY WORDS
Dental implants; growth factors.
The use of short implants rangingfrom 6.5 to 8.5 mm has historicallybeen related with low implant
survival success rates.1,2 However, cur-rent data suggest that the same level ofclinical success may be reached forshort implants compared to longerimplants.3,4 In fact, survival rates from88% to 100% have been reported for theatrophic mandible,5 whereas rehabilita-tion of partial edentulism and severelyresorbed maxillae with short implantsleads to survival rates around 95%.6
Recently, we reported that survivalrates of 532 short dental implants‡ in-stalled in the posterior regions of the jawsand under different surgical approacheswere 99.2% and 98.7% for the implantand subject-based analysis, respec-tively.7 In all the cases, short implantswere installed following a low-speed dril-ling procedure8 and they were humidi-fied, before installation, with a liquidformulation of plasma rich in growth fac-tors (PRGF). The latter consists of a lim-ited volume of plasma enriched inplatelets and growth factors rapidlyobtained from the patient and easily pre-pared, and may enhance and accelerateimplant osseointegration.9,10 The initialevidence suggesting high predictabilityof short implants has been reinforcedby the different biomechanical studiesaddressing that maximum bone stressis practically independent of implant
* Private practice, Vitoria, Spain.† Biotechnology Institute, Vitoria, Spain.
doi: 10.1902/jop.2010.090637
‡ BTI Implant system, Biotechnology Institute, Vitoria,Spain.
J Periodontol • June 2010
819

length2 and even that implant width is more importantthan the additional length.11 Based on these data, it isbelieved that with an optimized implant design andsurgical protocol, short implants may play an out-standing role in oral implantology, reducing the indi-cations for such procedures as sinus lift and additionalgrafting techniques.
The objective of this retrospective study is to pro-vide new data on the survival rate of short implants§
(6.5 to 8.5 mm) installed both in the maxillae andmandible following a consistent and predictableprotocol. A total of 1,287 implants installed in 661consecutive patients have been evaluated and an im-plant-based and a patient-based analysis of failureshas been carried out. The potential influence of demo-graphic factors, clinical factors, surgery-dependingfactors, and prosthetic variables on implant survivalhas been analyzed.
MATERIALS AND METHODS
The protocol of this retrospective longitudinal studywas approved following the national and interna-tional (International Conference of Harmonizationrules) policies on clinical studies. All implant instal-lations were performed by two experienced sur-geons and rehabilitations were done by threeprosthodontists. The inclusion criteria included sub-jects demanding rehabilitation of posterior areas bymeans of dental implants with a residual ridge that im-pedes the insertion of implants longer than 8.5 mm.Subject selection was based on an absence of any localor systemic diseases that might contraindicate thetreatment. Exclusion criteria included subjects withsystemic diseases and subjects taking drugs that alterthe bone metabolism. All subjects gave their writtenconsent to carry out the treatment according to the de-scribed protocol.
Subjects were treated with short implantsi witha length ranging from 6.5 to 8.5 mm and a diameterranging from 2.5 to 6 mm. In this study, selected pa-tients were treated with at least one short implant(£8.5 mm) from January 2001 to July 2008, whoseimplants were loaded, and with a minimum follow-up time of 12 months since the date of insertion.A total of 661 subjects and 1,287 implants were eva-luated. If needed, dentate subjects were treated peri-odontally to obtain periodontal health before implantplacement.
Thirty minutes before the surgery, 1 g amoxicillinwas administered, and the same antibiotic (500 mgevery 8 hours) was prescribed to all patients for thenext 6 days. Anti-inflammatory and analgesic drugswere also administered 30 minutes preoperatively.Briefly, subjects received 1 g paracetamol, 1 hour be-fore the surgery and for the next 3 days (1 g per 8hours). Depending of the clinical situation, subjects
were prescribed magnesium metamizol during the 2days following the surgery (1 g per 8 hours).
Saline solution rinses (during 48 hours) and addi-tional twice-daily chlorhexidine (0.12% wt/vol) rinseswere recommended until sutures were removed. Thelatter was mainly used in patients with poor oral hy-giene. Subjects were instructed on how to maintainproper oral hygiene around implants.
The clinical histories of all the patients were evalu-ated carefully, and the surgical procedures were cho-sen in function of the subjects’ characteristics, theanatomic peculiarities of the insertion places, and in-trinsic properties of the different short implants. Allimplant installations were performed following an ad-equate treatment plan and rehabilitations were madeby three prosthodontists.
A complete radiologic evaluation (conventional or-thopantomogram plus analysis of three-dimensionalreconstruction from a computed tomography scanusing a dedicated software¶) was carried out as re-ported elsewhere.7 In addition, surgery guides wereelaborated and provisional and final prostheses adap-ted to each patient were prepared. All implant recep-tion sites were prepared using a novel low-speeddrilling procedure (50 rpm) without irrigation.8 Beforeinstallation, implants were carefully embedded in liq-uid PRGF with the aim of bioactivating the implant sur-face.9,10 Liquid PRGF was prepared from the patient’sblood. Peripheral blood from each patient was takenby venipuncture before surgery and placed directlyinto 9-ml blood collecting tubes that contained 3.8%(wt/vol) sodium citrate as anticoagulant. Liquid PRGFwas prepared by centrifugation# at 580 · g for 8 min-utes at room temperature. The 1-ml plasma fractionlocated just above the red cell fraction was collectedand activated with calcium chloride** (50 mL PRGFactivator per milliliter of preparation) to initiate clot-ting and the continuous release of platelet growth fac-tors and proteins.
These short implants are characterized by theirself-tapping apex with ‘‘drive’’ capacity. The samefeatures allow a gentle approach in the posterior max-illa, because it allows the collection of bone by theimplant during its advance, whereas it avoids thedanger of compressing the most apical bone againstthe mental nerve. In addition, the special design ofthese short implants allows drilling 1 or 2 mm awayfrom the mental nerve and then introducing the im-plant practically to the limit, placing it with excellentdepth control. Implants were inserted in one-stagesurgery only when bone densitometry was >400
§ BTI Implant system, Biotechnology Institute.i BTI Implant system, Biotechnology Institute.¶ BTI Scan, Biotechnology Institute.# BTI blood collecting tubes, Biotechnology Institute.** PRGF system, Vitoria, Spain.
A 1- to 8-Year Follow-Up of Short Implants Volume 81 • Number 6
820

Hounsfield units and when the primary stabilityranged between 45 and 60 Ncm. From January2001 to July 2009, the patients were called in for oralhygiene and clinical and radiographic examinationsat least once a year.
STATISTICAL ANALYSES
Data collection and analyses were performed by twoindependent examiners (other than restorative den-tists). Descriptive statistics were performed, absoluteand relative frequency distributions were calculatedfor qualitative variables, and means – SD were cal-culated for quantitative variables. A database wasused for the analysis. Implant loss was the principalvariable of this study and included any implant lostbecause of biologic (failure to achieveosseointegration or loss of acquiredosseointegration) or biomechanicalcauses. The other variables includeddemographic factors, clinical factors,surgery-depending factors, and pros-thetic variables. The full list of vari-ables under analysis included age atinitial examination (categorized intothree categories: <45 years, 45 to 64years, and ‡65 years); gender; smok-ing habits (subjects smoking at leastone cigarette per day were classifiedas smokers); implant position (maxil-lary or mandibular); implant diameter(ranging from 3.3 to 5.5 mm); implantlength; implant staging (one- versustwo-stage approach); special tech-niques including vertical bone growth,ridge expansion, and bone grafting(this variable was divided into two cat-egories depending on the use or non-use of the special techniques); andprosthetic factors, divided into fixedpartial prostheses, hybrid overden-tures, and unitary prostheses, and intocemented or screwed prosthesis.
The overall survival rate of implantswas estimated both by an implant-based and subject-based analysis. In the implant-based analysis, each inserted implant was consideredas the analysis unit, whereas in the subject-basedanalysis each subject was followed-up until the fail-ure of his or her first implant. In both types of anal-ysis, the implant survival as a function of the timewas analyzed using a life table analysis (actuarialmethod), comparing the survival rates among thedifferent variables with the Wilcoxon test (Gehan).Data analysis was performed with a statistical soft-ware package.†† The level of statistical significancewas P <0.05.
RESULTS
The mean – SD age of the 661 subjects was 59 – 10years (range 28 to 94) at the beginning of the study.A total of 478 were female (72.3%). One hundredthirty-eight subjects were smokers (20.9%).
The frequency of the lengths and diameters of the1,287 short implants is shown in Table 1. Regardingimplant position, 570 were inserted in the maxilla(44.3%), whereas 717 were inserted in the mandible.The detailed anatomic distribution of the short
Table 1.
Characteristics of the Inserted ShortImplants
Diameter (mm)
Length (mm) 2.5 3.0 3.3 3.5 3.75 4.0 4.5 5.0 5.5 6.0 Total
6.5 0 0 0 0 1 0 16 19 1 0 37
7 0 0 0 0 55 55 1 0 0 0 111
7.5 0 0 0 0 5 0 110 102 16 1 234
8.5 1 12 41 8 139 158 281 243 21 1 905
Total 1 12 41 8 200 213 408 364 38 2 1,287
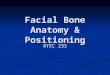
Figure 1.Anatomic distribution of the 1,287 short dental implants. The y axis shows the anatomic locationof implants, whereas the x axis illustrates both the frequency of the inserted implants (lower side)and the jaw location (upper side).
†† SPSS, Chicago, IL.
J Periodontol • June 2010 Anitua, Orive
821

implants is given in Figure 1. The surgicalapproach used for implant insertion wascarefully evaluated. A total of 750 implants(58.3%) were placed using one-stage sur-gery and 537 followed a two-stage sur-gery. A total of 272 implants (21.1%)were placed following special techniques.Regarding the prostheses used, most ofthe implants supported fixed partial den-tures (85.6%); 142 implants supportedhybrid overdentures (11%); and only 43implants had unitary prostheses (3.3%).In addition, most of the prostheses werecemented (82.9%).
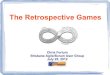
At the end of the study period, the sur-vival rates using the actuarial method were99.3% and 98.8% for the implant and sub-ject-based analysis, respectively (Fig. 2).The mean follow-up period for all the im-plants was 47.9 – 24.46 months (range 1to 102 months) after the definitive restora-tion was placed. Table 2 shows the lengthof observation by subject and by implant.
Only 9 out of 1,287 implants were lost during theobservation period. Table 3 discusses the main rea-sons for each implant loss.
The evaluation of the potential influence of differentvariables on implant survival revealed that none ofthem resulted in being statistically associated withimplant failure. This result is caused by the reducednumber of individuals with implant loss (only nine im-plant failures), which reduces the power of statisticalanalysis and the possibility of detecting potential riskfactors. Figures 3 and 4 illustrate the clinical situationof two patients involved in the study before and afterimplant placement.
DISCUSSION
One critical decision in oral implantology is related tothe importance of dental implant selection. In thepast, surgeons preferred the use of the longest possi-ble implant in any given site as long as its placementdid not hinder the final prosthetic result in terms of es-thetics. At that time, the placement of longer andwider implants was clearly associated with highersuccess rates.12 However, in patients with advancedlevels of alveolar bone resorption, the provision ofdental implants is often problematic and may requireadditional surgical intervention to augment bonelevels. This is in particular the case of the posteriormandibular and maxillary regions, where there isa risk of involving the inferior alveolar nerve or pene-trating the maxillary sinus during implant placementwhen alveolar bone is deficient. Furthermore, the pos-terior maxillae presents additional challenges for im-plant placement including difficult and challenging
access, limited visibility, reduced space, and poorbone quality.
One alternative to compensate for the limited boneheight is the use of different surgical techniques thatfacilitate bone augmentation. Sinus lift procedurehas been well documented by a growing number ofclinical and experimental studies.13-19 A lateral surgi-cal approach to the maxillary sinus is generally per-formed when the residual bony crest is extremelyatrophic (<5 mm height). The Caldwell-Luc proce-dure, consisting of a lateral approach by way of
Figure 2.Implant survival rates for the implant (green) and subject-based analysis (red).
Table 2.
Months of Follow-Up by Patients andImplants From Implant Insertion
Patients Implants
Follow-Up (months) n % Cum % n % Cum %
12 to <24 131 20.1 20.1 261 20.4 20.4
24 to <36 96 14.7 34.8 207 16.2 36.6
36 to <48 86 13.2 47.9 188 14.7 51.3
48 to <60 92 14.1 62.0 171 13.4 64.7
60 to <72 85 13.0 75.0 172 13.5 78.2
72 to <84 78 11.9 87.0 148 11.6 89.7
84 to <96 68 10.4 97.4 110 8.6 98.4
96 to 102 17 2.6 100 21 1.6 100
Total 653 100 1,278 100
Cum = cumulative.
A 1- to 8-Year Follow-Up of Short Implants Volume 81 • Number 6
822

a trapdoor access to the maxillary sinus, was firstreported as a sinus lift approach.20-23 However, thistechnique for sinus grafting has a considerable mor-bidity, especially when autologous bone is harvestedfrom extraoral sites, such as the calvarian and the iliaccrest, because a second surgical site is needed. An-other approach originally introduced by Summers24
in 1994 consists of using osteotomes. This approacheliminated the need for a trapdoor access, becauseelevation of sinus floor was performed by inwardcollapse of the residual crestal floor using speciallydesigned osteotomes.25 One limiting drawback ofthe crestal approach is that schneiderian membraneperforations (whose incidence is variable up to25%) are hardly detectable during the intervention,potentially leading to later complications. In general,these additional surgical approaches add consider-ably to treatment duration and cost and may detersome patients from undergoing prosthetic rehabilita-tion.
When the residual bone height is ‡5 mm, it is pos-sible to use other treatment alternatives to sinus graft-ing procedure. The use of short implants is longdebated because of their presumed high failure ratecompared to longer implants that guarantee a betteranchorage to bone and a better distribution of occlusal
load. However, it has not been demonstrated that theprognosis of an implant is affected by its length. Manyclinical4,6 and biomechanical studies11,25 and recentreviews26-28 demonstrated that short implant predict-ability is comparable to that of implants of normallength. In addition, eliminating or minimizing the lateralforce on the prosthesis and force distribution fromsplinting multiple implants plays a significant role in re-ducing stress on implants and especially on short im-plants.2 In fact, the splinted implant crowns used forthe present study might have transmitted less stressto bone–implant interfaces, leading to high survivalrates.
In the present article a long-term retrospectivestudy evaluating 1,287 short implants‡‡ placed in661 subjects is reported. The overall survival ratesof short implants were 99.3% and 98.8% for the im-plant and subject-based analysis, respectively, witha mean follow-up period for the implants of 47.9 –24.46 months. Only nine implants were lost duringthe observation period and after studying specificallyeach case, it is probable that the excessive torque insome cases and the combination of a bone type IV(bone type IV according to the classification of
Table 3.
Description of Implant Failures and Main Reasons for Each Implant Loss
Patient Implant Prostheses Implant Loss
Age
(years) Gender Smoker
Length
(mm)
Diameter
(mm) Tooth*
Implant
Staging
Special
Technique
No.
Implants
Received
Type of
Prosthesis Cause
Follow-Up
(months)
64 Female No 8.5 4.5 14 2-stage Yes 4 Complete 3SI + 3LI Bone Class IV + sinuselevation
4
64 Female No 8.5 3.75 12 1-stage No 4 Complete 3SI + 3LI Poor primary stability 7
62 Female Yes 8.5 4 3 2-stage No 4 Bridge 1SI + 1LI Bone Class IV + lowtorque (10 Nw)
5
54 Female No 7 4 30 1-stage Yes 1 Bridge 1SI + 2LI Pushed out by thetongue; high torque(60 Nw)
1
68 Female No 8.5 3.75 12 2-stage Yes 8 Complete 5SI + 5LI Bone Class IV + lowtorque (15 Nw)
5
57 Male No 8.5 5 19 1-stage No 2 Unitary 1SI Bone Class III + hightorque (65 Nw)
3
36 Female No 8.5 4.5 18 1-stage Yes 4 Bridge 1SI + 1LI Excessive torque(75 Nw)
4
75 Female No 8.5 5 3 2-stage No 6 Bridge 1SI + 1LI Bone Class IV + lowtorque (15 Nw)
8
66 Female No 8.5 4.5 19 1-stage No 3 Bridge 1SI + 1LI Low bone densityClass II + hightorque (70 Nw)
9
No. = number; SI = short implant; LI = long implant.* Tooth numbering follows American Dental Association classification.
‡‡ BTI Implant system, Biotechnology Institute.
J Periodontol • June 2010 Anitua, Orive
823

Lekholm and Zarb29) with poor primary stability inothers are the main reasons for these implant failures.The better understanding of each implant loss will pro-vide data for the planning of new studies and improv-ing clinical decision-making, which consequently willenhance future implant success.
The univariate relationships between the study var-iables and implant failure did not reveal risks factorsbecause it could be logically deduced assuming thatonly 9 out from 1,287 implants failed during the study.Although powerful and efficient statistical analyses ofthe data have been performed, the reduced number of
implant failures has impeded the identification of riskfactors.
One important issue that should be kept in mindwhen interpreting these results is that they come froma retrospective study. This type of study has less val-idity than randomized prospective clinical trials be-cause of issues of selection bias and confoundingfactors. Additionally, retrospective studies rely onthe completeness of data entered in the patient’schart, which may implicate the risk of missing databecause of misplaced, misfiled, or missing informa-tion in the chart. However, we do not have reasons
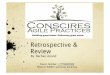
Figure 3.Example of one case involved in the study. A) A 55-year-old womanwith advanced periodontal disease.B) The scanner enables surgical planning of the case.C) Orthopantomography shows occlusal and periodontal condition. D) Radiograph 2 years after treatment. E) Situation before treatment; one can observethe malocclusion. F) Situation after 2 years of treatment.
A 1- to 8-Year Follow-Up of Short Implants Volume 81 • Number 6
824

to believe that any of these records were selectivelymissing because of the presence or absence of anykey variable. The present article describes one ofthe largest amounts of consecutively placed short im-plants in the literature. Additionally, the long-termsafety and functionality of the implants is well docu-mented because approximately 50% of the total num-ber of implants have been followed from 48 to 102months.
CONCLUSIONS
This paper reports the 1- to 8-year clinical experiencewith short dental implants. Survival rates of 99.3% and98.8% were obtained for the implant and patient-based analysis, respectively. These results mayclearly demonstrate the predictability and biosafetyof the short implants§§ when used under the carefultreatment planning and clinical protocol. In our dailypractice, the possibility to use short implants in a pre-dictable way enables reducing the indications for spe-cial procedures, such as sinus lift and bone-graftingprocedures. The data reported in this study might helpclinicians to improve their decision-making with theaim of enhancing implant success.
ACKNOWLEDGMENTS
This study was funded by the Biotechnology Institute(BTI), Vitoria, Spain, the manufacturer of the implants
used in this study. Dr. Anitua is the Scientific Directorof BTI. Dr. Orive is a researcher at BTI.
REFERENCES1. Bahat O. Treatment planning and placement of dental
implants in the posterior maxillae: Report on 732consecutive Nobelpharma implants. Int J Oral Max-illofac Implants 1993;8:151-161.
2. Pierrisnard L, Renouard F, Renault P, Barquins M.Influence of implant length and bicortical anchorageon implant stress distribution. Clin Implant Dent RelatRes 2003;5:254-262.
3. Fugazzotto PA, Beagle JR, Ganeles J, Jaffin R, VlassisJ, Kumar A. Success and failure rates of 9 mm orshorter implants in the replacement of missing max-illary molars when restored with individual crowns:Preliminary results 0 to 84 months in function. Aretrospective study. J Periodontol 2004;75:327-332.
4. Goene R, Bianchesi C, Huerzeler M, et al. Performanceof short implants in partial restorations: 3-year follow-upof Osseotite implants. Implant Dent 2005;14:274-280.
5. Stellingsma C, Vissink A, Meijer HJ, Kuiper C,Raghoebar GM. Implantology in the severely resorbededentulous mandible. Crit Rev Oral Biol Med 2004;15:240-248.
6. Renouard F, Nisand D. Short implants in the severelyresorbed maxilla: A 2-year retrospective clinical study.Clin Implant Dent Relat Res 2005;7(Suppl. 1):S104-S110.
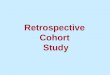
Figure 4.Example of another case involved in the study. A) Panoramic radiograph of a 53-year-old subject receiving implants in the lower jaw. B) Final panoramicradiograph 8 years after implant placement. C) Situation 5 years post-treatment. D) Final situation of the patient 8 years after implant placement.
§§ BTI Implant system, Biotechnology Institute.
J Periodontol • June 2010 Anitua, Orive
825

7. Anitua E, Orive G, Aguirre JJ, Andıa I. Five-yearclinical evaluation of short dental implants placed inposterior areas: A retrospective study. J Periodontol2008;79:42-48.
8. Anitua E, Carda C, Andia I. A novel drilling procedureand subsequent bone autograft preparation: A technicalnote. Int J Oral Maxillofac Implants 2007;22:138-145(erratum 2007;22:309).
9. Anitua E, Orive G, Pla R, Roman P, Serrano V, Andıa I.The effects of PRGF on bone regeneration and ontitanium implant osseointegration in goats: A histologicand histomorphometric study. J Biomed Mater Res A2009;91:158-165.
10. Anitua E, Sanchez M, Orive G, Andıa I. The potentialimpact of the preparation rich in growth factors(PRGF) in different medical fields. Biomaterials 2007;28:4551-4560.
11. Anitua E, Tapia R, Luzuriaga F, Orive G. Influence ofimplant length, diameter and geometry on stressdistribution: a finite element analysis. Int J Peri-odontics Restorative Dent 2010;30:89-95.
12. Buser D, Mericske-Stern R, Bernard JP, et al. Long-term evaluation of non-submerged ITI implants. Part 1:8-year life table analysis of a prospective multi-centerstudy with 2359 implants. Clin Oral Implants Res 1997;8:161-172.
13. Tong DC, Rioux K, Drangsholt M, Beirne OR. A reviewof survival rates for implants placed in grafted maxil-lary sinuses using meta-analysis. Int J Oral MaxillofacImplants 1998;13:175-182.
14. Wallace SS, Froum SJ. Effect of maxillary sinusaugmentation on the survival of endosseous dentalimplants. A systematic review. Ann Periodontol 2003;8:328-343.
15. Del Fabbro M, Testori T, Francetti L, Weinstein RL.Systematic review of survival rates for implants placedin grafted maxillary sinus. Int J Periodontics Restor-ative Dent 2004;24:565-577.
16. Graziani F, Donos N, Needleman I, Gabriele M, TonettiM. Comparison of implant survival following sinusfloor augmentation procedures with implants placedin pristine posterior maxillary bone: A systematicreview. Clin Oral Implants Res 2004;15:677-682.
17. Del Fabbro M, Rosano G, Taschieri S. Implant survivalrates after maxillary sinus augmentation. A systematicreview. Eur J Oral Sci 2008;116:497-506.
18. Pjetursson BE, Tan WC, Zwahlen M, Lang NP. Asystematic review of the success of sinus floor eleva-tion and survival of implants inserted in combinationwith sinus floor elevation. Part I: Lateral approach. JClin Periodontol 2008;35(Suppl. 8):216-240.
19. Anitua E, Prado R, Orive G. A lateral approach forsinus elevation using PRGF technology. Clin ImplantDent Relat Res 2009;11(Suppl. 1):e23-e31.
20. Boyne PJ, James RA. Grafting of the maxillary sinusfloor with autogenous marrow and bone. J Oral Surg1980;38:613-616.
21. Tatum H Jr. Maxillary and sinus implant reconstruc-tions. Dent Clin North Am 1986;30:207-229.
22. Smiler DG, Johnson PW, Lozada JL, et al. Sinus liftgrafts and endosseous implants. Treatment of theatrophic posterior maxilla. Dent Clin North Am 1992;36:151-186; discussion 187-188.
23. Lazzara RJ. The sinus elevation procedure in endo-sseous implant therapy. Curr Opin Periodontol 1996;3:178-183.
24. Summers RB. A new concept in maxillary implantsurgery: The osteotome technique. Compendium 1994;15:152,154-156, 158 passim; quiz 162.
25. Summers RB. Staged osteotomies in sinus areas:Preparing for implant placement. Dent Implantol Up-date 1996;7:93-95.
26. Griffin TJ, Cheung WS. The use of short implants inposterior areas with reduced bone height: A retrospec-tive investigation. J Prosthet Dent 2004;92:139-144.
27. das Neves FD, Fones D, Bernardes SR, do Prado CJ,Neto AJ. Short implants – An analysis of longitudinalstudies. Int J Oral Maxillofac Implants 2006;21:86-93.
28. Fugazzotto PA. Shorter implants in clinical practique:Rationale and treatment results. Int J Oral MaxillofacImplants 2008;23:487-496.
29. Lekholm U, Zarb GA. Patient selection. In: BranemarkPI, Zarb GA, Alberktsson T, eds. Tissue-IntegratedProstheses. Chicago: Quintessence Publishing; 1965:199-201.
Correspondence: Dr. Eduardo Anitua, Instituto EduardoAnitua, c/ Jose Maria Cajigal 19, 10005 Vitoria, Spain. Fax:34-945155095; e-mail: [email protected].
Submitted November 14, 2009; accepted for publicationFebruary 8, 2010.
A 1- to 8-Year Follow-Up of Short Implants Volume 81 • Number 6
826