Embed Size (px)
Citation preview

Nichole Sheridan
November 2, 2015
Dr. Rose
Hist 3300-002/Fall 2015
“Shell shock” in WWII
Ralph T Collier was medically discharged from the Navy in 1945 with a diagnosis of
“psychological neurosis.” Several years later in 1952, Collier was one of sixty-three people
arrested for the terrorizing of 18 months as part of the Ku Klux Klan. While Collier was on trial
for this charge, however, the judge learned that Ralph had been diagnosed as “shell shocked” and
commuted Ralph’s 18 to 20 month jail sentence, instead charging him a $1,000 fine. 1
The military newspaper The Stars and Stripes criticized lenient treatment such as this, the
“psycho neurosis fad,” claiming in 1945 that “every screwball with thick lenses…. was an expert
on the returning veteran.” Just one of many such articles published in the media after World War
II (WWII), this piece suggested that physicians and psychologists were handing out the diagnosis
of war neurosis like it was candy. All of a sudden, everyone considered themselves experts on
“shell shock.”2
The previous example is a far cry from how some people in society viewed the diagnosis.
In the 1946 article “Psychiatry and the Veteran,” the New York Times called on society to
remove the “stigma of shame” associated with mental illnesses.3 As this article suggests, some 1 “Klan Aide Avoids Jail: Carolina Commutes Sentence of Shell-Shocked Veteran,” New York Times, September 3, 1952, sec. Amusements.2 “Paper Defends Veterans: Stars and Stripes Hits ‘Psycho- Neurosis Fad’ in U.S.,” New York Times, May 1, 1945.3 “Psychiatry and the Veteran,” New York Times, January 21, 1946.
1

called on the development of programs to help the readjustment of veterans from war mentality
back to civilian life.4 Studying this subject in depth is extremely important because one third of
all veterans discharged by 1944 were because of psychiatric disabilities.5 Since it was such a
large number, why does it seem like it took an extended amount of time to figure out how to help
these veterans?
Because of the long-standing stigma against those labeled with mental illnesses, Veterans
Administration (VA) officials, civilians, physicians, and fellow veterans all debated the
diagnosis, treatment, and potential “cure” of “shell shock” during and after World War II. The
issue of this diagnosis went through a cycle of being “denied, talked about widely, understood,
and finally, forgotten.”6 As a result, shell-shocked veterans faced discrimination from the civilian
world, unfavorable media accounts, and when seeking medical treatment after being discharged
with mental disability. This raises the questions of who set the standards of “shell shock” at the
time, could these veterans be cured, and how did they go about reintegrating into society? By
exploring the different articles and resources available at the time and since, I will examine the
path shell shock (and its descendants) took during and after WWII.
Psychiatry, Background, Symptoms and Language
During and after World War I (1914-1918) many veterans were discharged on account of
“anxiety” and “nervousness.” This became a regular diagnosis and in 1918, “shell shock”
became a popular term associated with veterans who were discharged from the military.7 At the
4 “Veteran Clinics to aid Neurotics: Administration Will Establish 50 Mental Hygiene and Neurosis Stations for Treatment To Use Intensive Therapy The Locations Chosen,” New York Times, July 29, 1945.5 “Main Types of Mental Disorders Explained for Red Cross Class,” New York Times, March 20, 1944.6 Ben Shephard, A War of Nerves: Soldiers and Psychiatrists in the Twentieth Century (Harvard University Press, 2003).7 Sheena M. Eagan Chamberlin, “Emasculated by Trauma: A Social History of Post-Traumatic Stress Disorder, Stigma, and Masculinity,” Journal of American Culture 35, no. 4 (December 2012): 358–65, doi:10.1111/jacc.12005.
2

time it was mostly associated with a physical injury that caused nervous system breakdowns
rather than a mental injury itself. Shell shock, described as the condition after a soldier’s head
came into impact with a shell, caused a concussion, which then affected the nervous system,
much like what we now know as a traumatic brain injury (TBI).8
Prior to 1940, American psychology had three different approaches to the American
military. The first being psychiatric hospitals experimenting with somatic treatment methods that
were developed in the 1930’s.8 With this, physicians hoped to find a biological cause for mental
illnesses. Secondly, involving outpatient agencies, physicians advocated for psychotherapy by
“arguing that those mental disorders that did not constitute mental illness, among them neurosis,
were worthy of their attention.”8 Finally, the third, represented by psychiatrists sought to help
people recognize the importance of prevention.
Still, as a relatively new field in 1944, psychiatry was divided into two categories:
civilian and military. The main distinction between the two lay in the fact while civilian
psychiatrists focused on the patient and keeping society safe from each other, the military
psychiatrists had a primary allegiance to the Army. This often meant that the psychiatrists would
do what was best for the military at the time, including sending soldiers back to the battlefront
before they were ready. The question that is posed then, weren’t military personnel also
considered people? This question haunted many psychiatrists in the war, as they were there to
“conserve the fighting strength, and to help win the war.”5 The psychiatrists had difficulty
pinpointing exactly where the needs of the individual and the needs of the military were able to
intersect.
8 Marjorie Van de Water, “Soldiers Wounded in Mind,” The Science News-Letter 45, no. 17 (April 22, 1944): 262–69, doi:10.2307/3921102.
3

December 1940, psychoanalytic psychiatrist Harry Stack Sullivan was appointed by the
Selective Service System to oversee the process of examining draftees. While he was appointed,
he broadened the criteria for “unfit soldiers” to include rejecting potential soldiers who could not
adjust to everyday life changes. With his extensive criteria, the rejection rate was often high, up
to at least twenty-five percent at times. 9 Prior to joining the military, draftees were examined by
psychiatrists at induction centers. During this time, each man would spend anywhere between
three (for "normal" draftees) to five or fifteen minutes (for more complex cases) being asked
questions which would determine whether or not he had any type of prior illness which would
cause him to “break down” during combat.10 Little time, however, was spent on patient history,
which was the most crucial part in these diagnoses.6 During these examinations, the men went in
nervous, and would only believe one of two things, he was “either a nut” or “not a nut.”11 The
belief that only men who were considered weak, or were ill before enlistment were the only ones
to suffer from a psychoneurotic break down was a popular one, and was accepted by physicians
as well as VA officials. This reason is why four out of five draftees were rejected for mental and
emotional reasons.12
Throughout the wars, no matter what this illness was called, the symptoms were mostly
the same. These included tiredness, headaches, confusion, nausea, nightmares, insomnia,
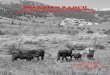
paranoia, and being easily irritated. While still on the battlefront, most soldiers had what they
called the “thousand yard stare” which was the number one sign for the “shell shock” diagnosis.
9 Hans Pols, “War Neurosis, Adjustment Problems in Veterans, and an Ill Nation: The Disciplinary Project of American Psychiatry during and after World War II,” Osiris 22, no. 1 (2007): 72–92, doi:10.1086/521743.10 Paul Wanke, “American Military Psychiatry and Its Role among Ground Forces in World War II,” Journal of Military History 63, no. 1 (January 1999): 127–46.11 “Main Types of Mental Disorders Explained for Red Cross Class.”12 Merl E. Bonney, “Personality Problems of Soldiers,” Marriage and Family Living 6, no. 2 (May 1, 1944): 29–31, doi:10.2307/346665.
4

Soldiers exhibiting the “thousand yard stare.”
During World War II however, medical military officers stopped using the term “shell
shock” and started using “war neurosis.”13 The latter term was used to describe those individuals
who were inherently susceptible to breakdowns because of parenting or upbringing. Shortly
after, other words to describe mental illnesses caused by war started to become known; including
terms like destroyer stomach, war nerves, combat fatigue, combat stress reaction, and flying
fatigue, irritable heart, battle shock, combat exhaustion, and condition red. These professionals
did not use these terms, however because they did not want to give the assumption that this type
of disease was unknown.14 The medical personnel wanted to remain in control and fix the
“unknown” problem by initiating the use of the abbreviation “N.P” which stood for neuro-
psychotic disabilities. Simply meaning, it was a nervous or mental disability for the veteran
being discharged. Military physicians also attempted to halt the casual usage of words like
“breakdown,” instead emphasizing words such as “exhaustion.” By doing so, physicians
attempted to try to distance these veterans from those who were considered “mad” and were
13 Katherine N. Boone, “The Paradox of PTSD,” Wilson Quarterly 35, no. 4 (October 2011): 18–22.14 E. Wittkower and J. P. Spillane, “Medical Problems In War Neuroses In War,” The British Medical Journal 1, no. 4127 (February 10, 1940): 223–25.
5

institutionalized without having been to war. While this may have been a step in the right
direction, it would take the rest of the United States and civilians a little bit longer to see that
these veterans needed programs and assistance after they were discharged from the military.
Cures and treatment
Toward the end of the ‘40s, the military began to argue the idea that we needed to remove
the increasingly popular “stigma of shame” associated with psycho neurosis veterans. Military
officials struggled to explain to the American public that psycho neurosis was not insanity, and
did not originate in the brain. The military believed that if veterans with these disabilities were
treated early and properly, their recovery chances were excellent and the veterans could go on
with a relatively normal life.15 Within the Army there were two or three different beliefs about
preventing and curing veterans who suffered from mental disabilities. The treatment one
received depended on what class one was, as well as on whether the veteran was diagnosed as a
psychoneurosis with hysteria (symptoms such as blindness, tremors, unusual gait and
overemotional) or neurasthenia (inverted and depressed).16 First and foremost though, prevention
was key. During recruitment, examining doctors spent most of their time on whether or not the
man was prone to breakdowns before enlistment. After that, it was the military's call whether or
not they would accept the potential soldier.
Within the psychoneurosis spectrum, there are two subcategories: hysteria and
neurasthenia. The latter, Tom Brown (a Canadian historian) argued, almost all observers agreed
was reserved for the officers and higher military personnel.13 They were often treated better than
the lower class soldiers, and these treatments included tranquility country spas. Whereas on the 15 “Psychiatry and the Veteran.”16 Mark Osborne Humphries and Kellen Kurchinski, “Rest, Relax and Get Well: A Re-Conceptualisation of Great War Shell Shock Treatment,” War & Society 27, no. 2 (October 2008): 89–110.
6

other hand, the veterans diagnosed with the hysteria were often lower class, and could not afford
the luxuries of relaxation and time to get better.13 The most popular belief among military
physicians was that “shell shock” should be cured as close to the front lines as possible, and by
keeping the man in a “military environment” his chances of getting back to “normal” improved.17
Psychoneurotic-hysteria diagnosed soldier showing off his unusual gate.
One thing that all physicians agreed (during the later stages of the war) on was that the
soldier was in a state of shock; and did not need any type of shock treatment, sodium amytrol,
metrazol, insulin, or any type of electric treatment. These types of treatment would cause the
soldier’s nervous system to go haywire and cause more harm than good. The treatment that the
soldier did receive while he was on the front lines consisted of sedatives, rest, and a large amount
of reassurance from the military physician. The veteran needed to be told that he was not crazy,
and he was going to be alight.
17 Wanke, “American Military Psychiatry and Its Role among Ground Forces in World War II.”
7

Soldier being given shock treatment for “shell shock.”
If the soldier could not able to be “cured” at the front lines, then he was often moved to a
nearby hospital (which could have been 100 miles away) and was treated there. In that
circumstance, even though the soldier was taken away from his position, he was still expected to
fetch his own food, make up his bed, and keep his area tidy.18
Another approach used by military personnel was that unless a soldier could re-remember
and relive his harrowing experience, his chances of developing permanent symptoms increased.19
In order for the soldiers to relive their experience, physicians often used hypnosis or the drug
sodium amytal to induce their memory. While this may seem like an extreme and inhumane
treatment, it was believed that the soldiers must be able to get through the visions that put him in
that particular state, in order for him to move on with his life or return to active duty.
18 Marjorie Van de Water, “Mental Combat Casualties,” The Science News-Letter 45, no. 25 (June 17, 1944): 391–96, doi:10.2307/3920732.19 “War Neurosis Effects,” The Science News-Letter 42, no. 9 (August 29, 1942): 134, doi:10.2307/3919037.
8

Soldier being injected with sodium amytal in order to relive his experience.
If the soldier was discharged with a N.P. or other related injury, the veteran had to abide
by several rules. The primary recommendation the military gave the veteran was that he should
not take time, or take it easy, but rather he was encouraged to go straight to work right away. The
military emphasized that physical labor was the best of therapy. If that did not work, however,
the military handed out pamphlets that said “a man’s problem is his own” and that if he cannot
“nip it in the bud himself;” he should not hesitate to get help right away.20 That is what Robert
Lombard, who was diagnosed with neurosis did in 1946, when he felt he was “unable to control
himself” and asked to be put in jail. Instead of a jail sentence the judge arranged for Lombard to
enroll in a psychiatric treatment center.21
Reintegrating and Society’s Views
20 Michael Carolan, “Breaking Point: The Search for a Postwar Grandfather,” Massachusetts Review 49, no. 3 (Fall 2008): 321–39.21 “Jailed at Own Request: War Veteran Paroled in Fight ‘Unable’ to Control Himself,” New York Times, August 30, 1946.
9

Right after wars we, as a surrounding community treat our veterans as heroes; the
government gives pensions, and creates bills to help the veterans, yet after a while society seems
to forget them, or start caring less.22 In 1944, the G.I. Bill of Rights hoped to provide access to
employment and loans, as well as expand educational opportunities for veterans. 23 With twelve
million veterans coming home, educational sociologist and WWI veteran, Willard Waller warned
society that, “the veteran is, and has always been, a problematic element in society … A threat to
every institution.” 22This is also apparent with The Ugly Laws that were established by some
states in 1867 after the Civil War, creating an “us versus them” mentality. These laws created
strict limitations on when and where “mangled, maimed, and unsightly” veterans were allowed
to be, and prohibited veterans from “begging.” 24 As a society we tend to go from one extreme to
the other when dealing with veterans, especially those discharged with neuro- psychotic related
diagnoses.
Russ Dean, a WWII veteran discharged in 1945 was excited to be home, and eager to
continue on his life, no longer a staff sergeant of the United States Air Force, but a civilian in the
United States.25 Three weeks after coming home, Dean went to see Howard Rusk (who founded
the Army air forces convalescent training program) no longer as the excited, eager man to be
home, but someone coming down from “combat hangover.” 25 Russ Dean appeared to be irritable,
rebellious, and confused. He had spent the last three weeks looking for employment, a place to
live, and to get his affairs in order. After visiting seventeen different places, he had no luck. 25
22 Carolan, “Breaking Point.”23 Pols, “War Neurosis, Adjustment Problems in Veterans, and an Ill Nation.”24 Susan M. Schweik, The Ugly Laws: Disability in Public (NYU Press, 2009).25 M. D. COL. Howard A. Rusk, “REHABILITATION: Human Side of Reconversion Stressed in Approach to Veterans’ Problems With Action to Reduce Red Tape, Delay Typical ‘Combat’ Hangover Variance in Breaking Point Time and Psychiatric Care Lack of Right Understanding Emerging From ‘Condition Red’ Cooke to Command 7th Fleet,” New York Times, December 9, 1945.
10

How were the veterans supposed to provide for themselves and their families if they were
discriminated and stigmatized, and could not find work after they were discharged with a
psychoneurosis disability? In regards to psycho neurosis discharges in the military, the difference
between WWI and WWII was a drastic one, almost doubling itself, causing the reintegration in
civil society among veterans in the 1940’s and 50’s to be a very difficult one, even more so after
World War I.26
The veterans who were discharged with N.P. diagnoses not only had trouble “coming
out” to other people, but they had difficulty admitting to themselves that they needed help.27
When veterans were discharged, they often had no support system, and if they did, it
overwhelmed them entirely. Such was the case with a young veteran in 1945 who returned for his
homecoming party after a 14 month tour, and ended up running out on the whole event because
while he may have been there physically, emotionally he was thousands of miles away, still with
his brigade. 28
In many cases, the veteran also struggled with feelings of guilt, and thoughts of “it should
have been me” when they came back from tragedies and their comrades did not.29 Within the
same type of situations, they may have also developed a super ego status. The development of
this status meant that the veteran thought he was strong enough to handle anything, and did not
need anyone to help him, nor did he need or seek medical treatment. This concept appeared in an
26 Frederick R. Barkley, “Most ‘Shell Shocked’ Cases Now Cured at the Front: Army’s Studies of the Soldier’s Nervous Upsets Have Brought Good Results,” New York Times, November 28, 1943, sec. Review of the Week Editorial.27 “Neuroses In War Time: Memorandum For The Medical Profession,” The British Medical Journal 2, no. 4119 (December 16, 1939): 1199–1201.28 M. C. Chief Convalescent Training Division COL. Howard A. Rusk, “The Journey Down From ‘Condition Red’: Colonel Rusk Explains the Returning Soldier’s Emotional Problems and Offers a Solution. Journey From ‘Condition Red,’” New York Times, July 29, 1945, sec. The New York Times Magazine.29 William Laurence, “‘Guilt Feelings’ Pictured in Fliers: Army Air Force Psychiatrists Tell Associates of ‘Mental X-Rays’ After Missions,” New York Times, May 17, 1944, sec. Business Fina.
11

article in The New York Times that also debunked the myth that it was only the phenomenon of
weaklings that came back with psycho neurosis diagnoses or disabilities. On the other hand,
however, the Army still thought that their problem of “crazies” came from lack of leadership,
and if they were able to train effective leaders then it would cut down on the percentage of
psycho neurotic discharge cases.30 Even though these veterans were not dead, the military still
thought of them as casualties.
It was unanimously agreed upon that veterans had a hard time adjusting back to
civilization after coming back from war, and often became delinquent. In a 1944 article, The New
York Times expressed that we must assume everyone coming back from war has “shell shock” to
some degree, and that the pension “is neither a crux nor a solution.”31 That’s why in the late ‘40s
and early ‘50s the military’s and civilian world’s views regarding discharged veterans started to
change. Around this time, the VA started to notice that there was a delay in mental hygiene
regarding discharged veterans and help in their reintegration, so they began to push for new and
improved mental health facilities.32 In 1945, the VA called for a psychology rehabilitation
program that “was neutral, had no political, religion, racial, social or class ties.”33 Soon after,
veterans were able to visit one of the fifty mental hygiene and neurosis stations for treatment
whenever was convenient for them, day or night and would help them adjust back to civilian life.
It became important that society did not look at the veteran as a discharged psychoneurotic, but
instead remember that they once held responsible jobs in society.
30 “The Army Ponders Why G.I.’S Crack Up: ‘Human Engineering’ Course Given at Benning--Aim Is to Cut Down ‘Psycho’ Cases One of Most Important,” New York Times, July 4, 1951.31 “Bitterness of Veterans Viewed As Dominant Political Factor: Attitude Likely to Shape Conditions in Nation for 20 Years, Educator Asserts -- Plan of Rehabilitation Now Urged,” New York Times, April 23, 1944.32 M. D. Howard A. Rusk, “Survey by VA Stresses Lag in Mental Hygiene: Agency Pushes Program to Restore Service Men to Civilian Life N.P.’s Need Treatment Unemployment Benefits VA Psychiatrists More Facilities Needed,” New York Times, September 15, 1946, sec. The Week In Review.33 “Veteran Clinics to aid Neurotics.”
12

Veterans in a therapy group. A neuropsychiatrist discussing a patient.
Conclusion
In the early years
of the war, military
physicians were still
in the process of
understanding “shell shock,” what caused it, and how to
help the veteran suffering from it. Finding these answers became increasingly important because
psychiatric disabilities accounted for one third of all the veterans coming home, and if given the
wrong idea, these veterans would have faced more harm than good coming home.34 Toward the
end of the war, family and friends started understanding that veterans who were discharged
needed understanding, sympathy, reassurance, and a lot of encouragement. It was important that
people in the civilian world understood exactly how important their role in helping veterans
readjust was.
34 “Many More Neurotic Ills Caused By This War Than by the Last One: How to Recognize Such Afflictions and Deal With Fighting Men Who Come Home With Them Is Told in Lecture,” New York Times, March 27, 1944, sec. SPORTS.
13

Maxwell Gitelson the author of “The Role of the Community in Relation to the
Emotional Needs of the Returning Soldiers” said it perfectly in 1945 when he wrote that “as
citizens we owe much to the returning soldier, much more than compensation and clinics. We
owe him a human society in which respect for the individual, politically, economically, and
socially, grants him a genuine sense of personal significance, a genuine personal stake, and, out
of this, a real participation with ourselves in the possibilities of a decent life.”35
A soldier returning home. A soldier being drawn by a volunteer.
35 Maxwell Gitelson, “The Role of the Community in Relation to the Emotional Needs of the Returning Soldier,” Social Service Review 19, no. 1 (March 1, 1945): 93–95.
14

Bibliography
Primary
“Artist Who Sketched Portraits of Soldiers an ‘unsung Hero’ of WWII." Artist Sketched
Portraits of Soldiers in WWII. Web. 2 Dec. 2015.
http :// america.aljazeera.com/articles/2013/11/10/artist-who-
sketchedportraitsofsoldiersnowunsungheroofwwii.html.
Barkley, Frederick R. “Most ‘Shell Shocked’ Cases Now Cured at the Front: Army’s Studies of
the Soldier’s Nervous Upsets Have Brought Good Results.” New York Times. November
28, 1943, sec. REVIEW OF THE WEEK EDITORIAL.
“Bitterness of Veterans Viewed As Dominant Political Factor: Attitude Likely to Shape
Conditions in Nation for 20 Years, Educator Asserts -- Plan of Rehabilitation Now
Urged.” New York Times. April 23, 1944.
Bonney, Merl E. “Personality Problems of Soldiers.” Marriage and Family Living 6, no. 2 (May
1, 1944): 29–31. doi:10.2307/346665.
COL. Howard A. Rusk, M. C. Chief Convalescent Training Division. “The Journey Down From
‘Condition Red’: Colonel Rusk Explains the Returning Soldier’s Emotional Problems and
Offers a Solution. Journey From ‘Condition Red.’” New York Times. July 29, 1945, sec.
The New York Times Magazine.
COL. Howard A. Rusk, M. D. “Survey by VA Stresses Lag in Mental Hygiene: Agency Pushes
Program to Restore Service Men to Civilian Life N.P.’s Need Treatment Unemployment
15

Benefits VA Psychiatrists More Facilities Needed.” New York Times. September 15,
1946, sec. The Week In Review.
COL. Howard A. Rusk, M. D. “REHABILITATION: Human Side of Reconversion Stressed in
Approach to Veterans’ Problems With Action to Reduce Red Tape, Delay Typical
‘Combat’ Hangover Variance in Breaking Point Time and Psychiatric Care Lack of Right
Understanding Emerging From ‘Condition Red’ Cooke to Command 7th Fleet.” New
York Times. December 9, 1945.
Gitelson, Maxwell. “The Role of the Community in Relation to the Emotional Needs of the
Returning Soldier.” Social Service Review 19, no. 1 (March 1, 1945): 93–95.
“Jailed at Own Request: War Veteran Paroled in Fight ‘Unable’ to Control Himself.” New York
Times. August 30, 1946.
“Klan Aide Avoids Jail: Carolina Commutes Sentence of Shell-Shocked Veteran.” New York
Times. September 3, 1952, sec. Amusements.
Laurence, William. “‘Guilt Feelings’ Pictured in Fliers: Army Air Force Psychiatrists Tell
Associates of ‘Mental X-Rays’ After Missions.” New York Times. May 17, 1944, sec.
Business Fina.
“Main Types of Mental Disorders Explained for Red Cross Class.” New York Times. March 20,
1944.
“Many More Neurotic Ills Caused By This War Than by the Last One: How to Recognize Such
Afflictions and Deal With Fighting Men Who Come Home With Them Is Told in
Lecture.” New York Times. March 27, 1944, sec. Sports.
“Neuroses In War Time: Memorandum For The Medical Profession.” The British Medical
Journal 2, no. 4119 (December 16, 1939): 1199–1201.
16

"Office of Medical History - Neuropsychiatry in WWII." Office of Medical History -
Neuropsychiatry in WWII. Web. 2 Dec. 2015.
http :// history.amedd.army.mil/booksdocs/wwii/NeuropsychiatryinWWIIVolI/DEFAULT.htm .
“Paper Defends Veterans: Stars and Stripes Hits ‘Psycho- Neurosis Fad’ in U.S.” New York
Times. May 1, 1945.
“Psychiatry and the Veteran.” New York Times. January 21, 1946.
"PTSD and the Effect on DNA Part 1." Veterans Today. 24 Aug. 2013. Web. 2 Dec. 2015.
http ://www.veteranstoday.com/2013/08/24/ptsd-and-the-effect-on-dna-part-1 / .
"Shell Shock." I Hope to Be Remembered for My Atrocities. 28 Dec. 2013. Web. 2 Dec. 2015.
https ://miepvonsydow.wordpress.com/2013/12/28/shell-shock / .
“The Army Ponders Why G.I.’S Crack Up: ‘Human Engineering’ Course Given at Benning--
Aim Is to Cut Down ‘Psycho’ Cases One of Most Important.” New York Times. July 4,
1951.
“Veteran Clinics to Aid Neurotics: Administration Will Establish 50 Mental Hygiene and
Neurosis Stations for Treatment To Use Intensive Therapy The Locations Chosen.” New
York Times. July 29, 1945.
“War Neurosis Effects.” The Science News-Letter 42, no. 9 (August 29, 1942): 134.
doi:10.2307/3919037.
Water, Marjorie Van de. “Mental Combat Casualties.” The Science News-Letter 45, no. 25 (June
17, 1944): 391–96. doi:10.2307/3920732.
“Soldiers Wounded in Mind.” The Science News-Letter 45, no. 17 (April 22, 1944): 262–69.
doi:10.2307/3921102.
17

Wittkower, E., and J. P. Spillane. “Medical Problems In War Neuroses In War.” The British
Medical Journal 1, no. 4127 (February 10, 1940): 223–25.
Secondary
Boone, Katherine N. “The Paradox of PTSD.” Wilson Quarterly 35, no. 4 (October 2011): 18–
22.
Carolan, Michael. “Breaking Point: The Search for a Postwar Grandfather.” Massachusetts
Review 49, no. 3 (Fall 2008): 321–39.
Eagan Chamberlin, Sheena M. “Emasculated by Trauma: A Social History of Post-Traumatic
Stress Disorder, Stigma, and Masculinity.” Journal of American Culture 35, no. 4
(December 2012): 358–65. doi:10.1111/jacc.12005.
Humphries, Mark Osborne, and Kellen Kurchinski. “Rest, Relax and Get Well: A Re-
Conceptualisation of Great War Shell Shock Treatment.” War & Society 27, no. 2
(October 2008): 89–110.
Pols, Hans. “War Neurosis, Adjustment Problems in Veterans, and an Ill Nation: The
Disciplinary Project of American Psychiatry during and after World War II.” Osiris 22,
no. 1 (2007): 72–92. doi:10.1086/521743.
Schweik, Susan M. The Ugly Laws: Disability in Public. NYU Press, 2009.
Shephard, Ben. A War of Nerves: Soldiers and Psychiatrists in the Twentieth Century. Harvard
University Press, 2003.
Wanke, Paul. “American Military Psychiatry and Its Role among Ground Forces in World War
II.” Journal of Military History 63, no. 1 (January 1999): 127–46.
18