Embed Size (px)
Citation preview
Verapamil Increases the Bactericidal Activity of 1 Bedaquiline Against Mycobacterium tuberculosis in the 2
Mouse Model 3 4 5 6 Shashank Guptaa, b, Sandeep Tyagia, William R. Bishaia, b,# 7 8 9 10 11 aCenter for Tuberculosis Research, Department of Medicine, JHU, Baltimore, 12 Maryland, USA 13 bHoward Hughes Medical Institute, Chevy Chase, Maryland, USA 14 15 16 Running Title: Verapamil Adds to Bedaquiline Killing 17 Activity in Mice 18 19 20 21 # Address correspondence to William R Bishai, [email protected] 22 23 24
AAC Accepts, published online ahead of print on 20 October 2014Antimicrob. Agents Chemother. doi:10.1128/AAC.04019-14Copyright © 2014, American Society for Microbiology. All Rights Reserved.
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Abstract 25 Bedaquiline is a newly approved drug for multidrug resistant tuberculosis with concerns 26 about its safety in humans. We found that co-administration of verapamil with sub-27 inhibitory doses of bedaquiline gave the same bactericidal effect in mice as full human-28 bioequivalent bedaquiline dosing. Adding verapamil to bedaquiline monotherapy also 29 protected from development of resistant mutants in vivo. Adjunctive use of verapamil 30 may permit use of lower doses of bedaquiline and thereby reduce its dose-related 31 toxicities in tuberculosis patients. 32 33 34
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
Body: 35 36 Bedaquiline (also known as Sirturo, TMC-207, R207910, or the “J” compound) 37 represents the first novel drug class to be approved by the US Food and Drug 38 Administration in last forty years for the treatment of multidrug-resistant tuberculosis 39 (MDR-TB) (1, 2). The recommended human dosage of bedaquiline is 400 mg once daily 40 for the first 2 weeks followed by 200 mg three times per week from weeks 3-24 (3). 41 Bedaquiline usage in patients presents several safety concerns including increased 42 mortality and hepatic-related adverse drug reactions. Bedaquiline also prolongs the QT 43 interval in patients, which is a measure of the time between the start of the Q wave and 44 the end of the T wave in the heart's electrical cycle. In a phase 2 trial involving patients 45 with advanced MDR-TB, a significantly higher number of participants receiving 46 bedaquiline died than those receiving placebo although the causes of mortality were not 47 directly attributable to the drug (4, 5). Thus strategies to reduce the human dose of 48 bedaquiline while retaining antibacterial activity may be valuable. 49 50 Active efflux of drugs is known to play a major role in antimicrobial resistance in 51 Mycobacterium tuberculosis (6). Small molecule inhibition of efflux pumps improves the 52 activity of several anti-mycobacterial agents that are subject to efflux. Verapamil is an 53 efflux pump inhibitor that has been shown to have an antimicrobial potentiating effect in 54 the treatment of M. tuberculosis both in vitro and in vivo (7). Recently, it has been shown 55 that inhibiting efflux pumps of M. tuberculosis by verapamil reduces the bacterial drug 56 tolerance induced in the intracellular compartment within macrophages and in zebrafish 57 granuloma-like lesions (8). Addition of verapamil to standard TB treatment accelerates 58 both the bactericidal and the sterilizing activities of the regimen in mouse model (9). 59 60
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

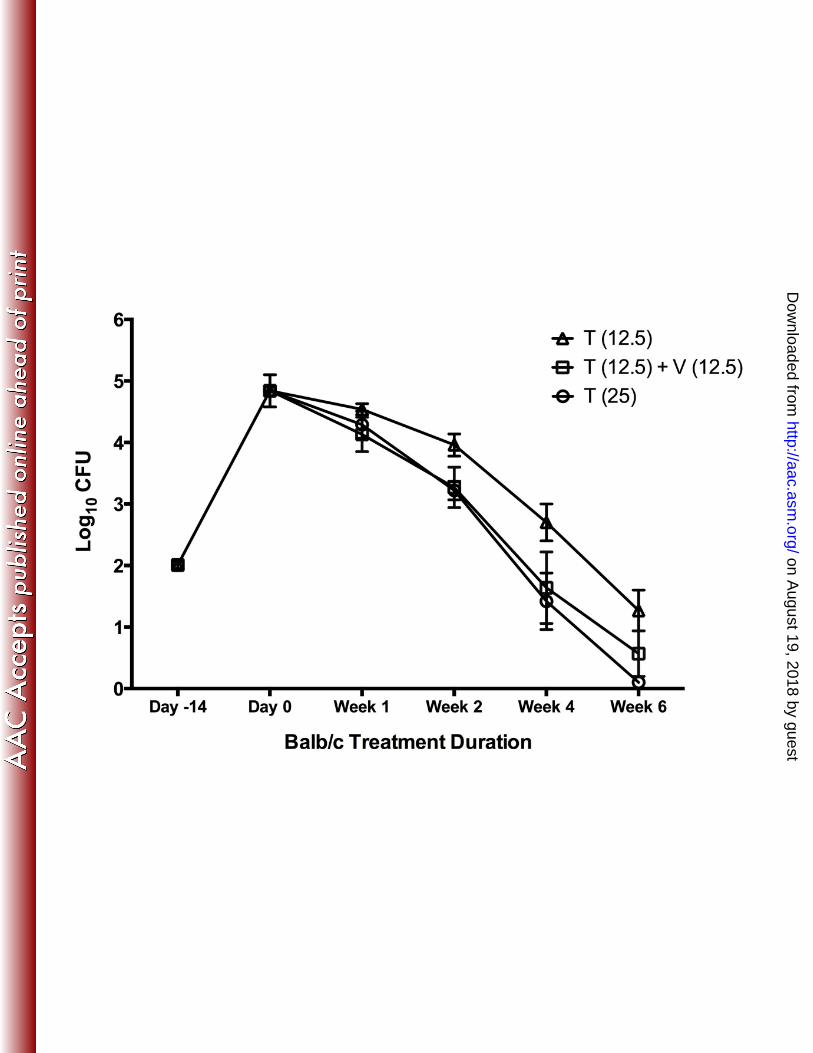
We have recently shown that supplementing bedaquiline with verapamil profoundly 61 decreases the MIC of bedaquiline in the wild type strain M. tuberculosis H37Rv, and also 62 in drug-susceptible and drug-resistant clinical isolates. The MIC of clofazimine against 63 M. tuberculosis H37Rv also decreased significantly in the presence of 50 μg/ml of 64 verapamil (10). We hypothesized that these results may extend to an in vivo infection 65 model, and that verapamil may potentiate the killing of M. tuberculosis by bedaquiline 66 and accelerate clearance of mycobacteria. Shortening treatment regimens and reducing 67 the required doses may be a promising strategy to reduce the incidence of bedaquiline-68 related adverse effects and thereby improve MDR-TB treatment outcomes. In the 69 present study, we investigated the effect of verapamil on the activity of bedaquiline 70 against M. tuberculosis in a mouse model of infection. In addition to investigating the 71 effects of verapamil on the full human bioequivalent dose of bedaquiline (25 mg/kg), we 72 also used a sub-optimal dose of bedaquiline (12.5 mg/kg) daily, with or without 73 verapamil to test if verapamil may potentiate the activity of bedaquiline. 74 75 We evaluated the activity of bedaquiline with or without verapamil in an acute mouse 76 model of TB infection. Female BALB/c (6 weeks old) were infected with M. tuberculosis 77 H37Rv in an aerosol chamber so as to implant 2.01 log10 CFU counts in the lungs on the 78 day after infection. Two weeks after infection, treatment for 6 weeks was started (day 0) 79 when the lung CFU counts were 4.84 log10 units. Positive control mice were treated with 80 rifampin (R), isoniazid (H), and pyrazinamide (Z) for 6 weeks. The test mice were treated 81 with bedaquiline at 25 mg/kg daily or with half of that dose (12.5 mg/kg) daily, with or 82 without oral doses of verapamil (12.5 mg/kg). Lungs were plated on selective 7H11 and 83 0.4% charcoal-containing 7H11 plates for CFU counts at days -14, 0, 7, 14, 28 and 42 to 84 assess the effect of verapamil on anti-mycobacterial activity of bedaquiline. After 85 stopping treatment, a subset of mice in the groups treated with bedaquiline (25 mg/kg) 86
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

were held with no treatment and sampled at day 70 for the presence of bedaquiline-87 resistant mutants to determine whether verapamil can protect bedaquiline monotherapy 88 from the development of resistance. 89 90 The infected mice receiving control RHZ treatment showed similar lung CFU responses 91 to those seen in our earlier studies (9). Bedaquiline monotherapy in mice was superior to 92 RHZ over the full six weeks of therapy (Fig. 1A). The human bioequivalent bedaquiline 93 dosing treatment group, T(25), yielded a CFU decrease of 0.55 log units at week 1, 94 whereas the bedaquiline plus verapamil group, T(25) + V, showed a reduction in 95 quantitative CFU counts by 1.15 log units at week 1 (P value = 0.051, Student’s t test 96 used for statistical significance). This difference of 0.5 to 0.6 log units between the two 97 groups of mice was sustained over the course of treatment. 98 99 The total lung CFU burden in mice receiving T(12.5) was similar to that of the RHZ 100 treated control animals over the course of treatment (P value > 0.05) (Fig. 1B). As 101 expected, the human bioequivalent dose of 25 mg/kg bedaquiline had a greater effect on 102 the reduction of lung CFU counts when compared with the sub-optimal dose of 12.5 103 mg/kg bedaquiline (P value < 0.0001). The 12.5 mg/kg bedaquiline and verapamil group, 104 T(12.5) + V, performed better than the control RHZ regimen (P value < 0.0001). 105 106 The lung CFU counts in mice receiving the sub-optimal dose of bedaquiline, T(12.5) 107 dropped by 0.30 log units while the reduction was 0.71 log units in mice treated with 108 bedaquiline and verapamil, T(12.5) + V during the first week of treatment (P value = 109 0.01). These differences in the lung CFU counts between the T(12.5) and the T(12.5) 110 plus verapamil group were 0.69 log units at 2 weeks, 1.06 log units at 4 weeks, and 0.7 111 log units at 6 weeks of treatment (P value for the two treated groups is <0.01 for weeks 2 112
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

and 4). In fact, the T(12.5) plus verapamil group showed the same bactericidal effect as 113 T(25) alone (non-significant P value of 0.2 for T(12.5) + V versus T(25)). 114 115 To assess the number of mice in which bedaquiline resistant mutants were generated 116 during drug monotherapy, we held groups of mice after 6 weeks of treatment for an 117 additional 4 weeks without drug therapy, and then sacrificed them to determine the 118 fraction of mice having bedaquiline resistant bacteria in their lungs (Table 1). 119 Surprisingly, 2 out of 10 demonstrated bedaquiline resistant mutants in the 25 mg/kg 120 bedaquiline group while none (0 out of 10) of the mice from the bedaquiline plus 121 verapamil group had resistant bacteria. Using MABA and broth dilution assay, we 122 determined that the MIC for the bedaquiline mutants was at least 8-fold higher than the 123 susceptible strain M. tuberculosis H37Rv. While bedaquiline has a long half-life and 124 achieves high tissue concentrations which may confound plate counts due to carry-over 125 of residual antibiotic, both of the above groups of mice received the same doses of 126 bedaquiline and were exposed to the same 4 week washout period. Moreover, plating at 127 day 70 was performed on (i) drug-containing agar, (ii) drug-free agar, and (iii) drug-free 128 0.4% charcoal agar (used to sequester carry-over drug in the homogenates), and this 129 comparative plating revealed that >85% of the colonies on all three sets of plates from 130 bedaquiline-treated mice were bedaquiline resistant. Hence, the verapamil protection 131 from resistance development appears to have occurred in vivo prior to sacrifice. 132 133 This is the first in vivo report that the efflux pump inhibitor verapamil can potentiate sub-134 optimal doses of bedaquiline to its full anti-microbial effectiveness in the mouse model. 135 In the present study, we found that co-administration of verapamil with 12.5 mg/kg of 136 bedaquiline gave the same bactericidal activity over six weeks as 25 mg/kg of 137 bedaquiline alone. The observation that verapamil potentiates a sub-optimal dose of 138
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

bedaquiline in BALB/c mice extends previous work showing that verapamil added to the 139 standard TB treatment and related regimens accelerates the bactericidal activity of the 140 regimen in mice (7, 9). It has been recently shown that adding verapamil to bedaquiline 141 slightly increased the bactericidal effect at a single time point (4 weeks) in mice (11). It 142 has been shown in the previous studies that the administration of 12.5 mg/kg dose of 143 verapamil to mice results in Cmax of approximately 500 ng/ml and an AUC of 792 ng-144 h/ml, which is close to the reported human AUC of 841 ng-h/ml when 240 mg Calan SR 145 was administered with food (9). Using in vitro studies, we found that verapamil has very 146 weak anti-bacterial effect against M. tuberculosis H37Rv with MIC ranging from 200 – 147 400 μg/ml and so verapamil at 12.5 mg/kg will not have in vivo anti-bacterial effect by 148 itself. 149 150 Our finding that verapamil potentiates bedaquiline raises the possibility of extending 151 these findings to TB patients where the daily doses of bedaquiline may be reduced when 152 co-administered with verapamil. A lower human dose of bedaquiline is likely to reduce 153 the frequency of bedaquiline-related adverse effects such as QTc prolongation and 154 hepatic toxicity. 155 156 Another interesting observation from our study is that verapamil decreased the mouse 157 lung CFU counts by approximately 4-fold at week 1 when administered with the standard 158 dose of 25 mg/kg of bedaquiline. Diacon et al. reported that the loading doses of 159 bedaquiline were required to overcome the delayed antimicrobial activity observed in 160 patients (12). We observed early bactericidal activity for bedaquiline in presence of 161 verapamil starting at week 1 (Fig. 1A) with a similar treatment response as bedaquiline 162 alone in the following weeks. In addition to potentiation of reduced doses of bedaquiline 163 by verapamil, this observation raises the possibility that verapamil use may also 164
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

abrogate or reduce the need for bedaquiline loading doses in the first two weeks of 165 therapy. Another strain of mouse namely C3HeB/FeJ when infected with M. tuberculosis 166 display lung granulomas with prominent necrotic areas of degenerating cells and dense 167 infiltrates of neutrophils, which more closely resemble human granulomas. In our 168 previous studies, we have shown that the differences with verapamil co-administration 169 occurred not only in the C3HeB/FeJ mice, but also in wild-type C3H/HeJ mice where the 170 observed differences were modest (9). We anticipate that the differences between the 171 treated groups with or without verapamil would be similar and more pronounced in the 172 C3HeB/FeJ strain. 173 174 Verapamil has been previously shown to block the acquisition of drug resistance in 175 Trypanosoma cruzi and Leishmania donovani (13), and chloroquine-resistance in 176 Plasmodium falciparum (14). It is well know that antibiotic pressure, usually from 177 monotherapy, may select spontaneous mutants and facilitate the emergence of de novo 178 drug resistance. We found that verapamil protects bedaquiline monotherapy against 179 resistance development after 6 weeks of treatment. Thus verapamil use may also assist 180 in preserving the activity of bedaquiline. 181 182 For multidrug therapy, the drug-drug interactions and overlapping toxicities are crucial 183 variables particularly in the management of TB and MDR-TB where patients receive 184 drug cocktails for many months. Bedaquiline is known to prolong the QTc interval (15), 185 whereas verapamil extends the PR interval (16) of the cardiac conduction system. While 186 some have expressed concerns for using a combination of two drugs that each have 187 effects on the cardiac conduction system, there is evidence that calcium channel 188 blockers like verapamil may exert cardio-protective effects against dangerous 189 arrhythmias associated with QTc prolongation including Torsades de Pointes (TdP). 190
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Verapamil has been shown to completely suppress TdP induced by dofetilide (17) or by 191 an anticholinergic overdose (18). Verapamil can also improve repolarization 192 abnormalities induced by epinephrine in congenital long QT syndrome (19). Together 193 with increasing the bactericidal activity of bedaquiline as suggested by our data, these 194 protective effects of verapamil on QTc prolongation, may limit, or even abrogate, the 195 negative cardiac effects of bedaquiline. 196 197 Our results indicate that verapamil potentiates the activity of bedaquiline against M. 198 tuberculosis in an in vivo mouse model. This potentiating effect may be due to efflux 199 pump inhibition by verapamil resulting in higher intracellular anti-mycobacterial drug 200 levels and enhanced drug activity. Our data suggest that adjunctive use of verapamil 201 may permit lower doses of bedaquiline and thereby reduce its dose-related toxicities. 202 Further studies are needed to investigate the synergistic effects of verapamil and 203 bedaquiline in humans during TB infection. 204 205 Acknowledgements: 206 207 The financial support from NIH grants AI37856, AI36973, AI097138 and the Howard 208 Hughes Medical Institute is gratefully acknowledged. 209 210
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Figure Legends: 211 212 Figure 1. Adding verapamil to bedaquiline increases bactericidal activity during 213 active disease. 214 BALB/c mice were infected with 2.01 log10 units of Mycobacterium tuberculosis H37Rv, 215 and treatment was started 14 days after infection. The mice were treated for 42 days 216 with rifampin (R; 10 mg/kg), isoniazid (H; 10 mg/kg), pyrazinamide (Z; 150 mg/kg) daily 217 for 5 d/wk. Groups of mice were also treated daily for 5 d/wk with bedaquiline (T) at two 218 different doses of 25 mg/kg (A) or 12.5 mg/kg (B) with or without verapamil (V; 12.5 219 mg/kg) for 42 days. The T(25) group in 1B is same as 1A and is included to compare the 220 bactericidal activity of T(12.5) + verapamil to the T(25) alone. The lungs were 221 homogenized, diluted, and plated for CFU counts and expressed as log10 CFU (±SD). 222 223
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

References: 224 225 226
1. U.S. Food and Drug Administration 2013. FDA news release. 227 www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333695.htm. 228 Accessed 31 July 2014. 229
2. Andries, K., P. Verhasselt, J. Guillemont, H. W. Gohlmann, J. M. Neefs, H. Winkler, 230 J. Van Gestel, P. Timmerman, M. Zhu, E. Lee, P. Williams, D. de Chaffoy, E. 231 Huitric, S. Hoffner, E. Cambau, C. Truffot-Pernot, N. Lounis, and V. Jarlier. 2005. A 232 diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. 233 Science 307:223-7. 234
3. Sirturo product information for health care providers. 235 http://www.sirturo.com/sites/default/files/pdf/SIRTURO-product-guide.pdf. Accessed 31 236 July 2014. 237
4. Mingote, L. R., D. Namutamba, F. Apina, N. Barnabas, C. Contreras, T. Elnour, M. 238 W. Frick, C. Lee, B. Seaworth, D. Shelly, N. Skipper, and E. T. Dos Santos Filho. 239 11 July 2014. The use of bedaquiline in regimens to treat drug-resistant and drug-240 susceptible tuberculosis: a perspective from tuberculosis-affected communities. Lancet. 241 http://dx.doi.org/10.1016/S0140-6736%2814%2960523-7. 242
5. Diacon, A. H., A. Pym, M. Grobusch, R. Patientia, R. Rustomjee, L. Page-Shipp, C. 243 Pistorius, R. Krause, M. Bogoshi, G. Churchyard, A. Venter, J. Allen, J. C. 244 Palomino, T. De Marez, R. P. van Heeswijk, N. Lounis, P. Meyvisch, J. Verbeeck, 245 W. Parys, K. de Beule, K. Andries, and D. F. Mc Neeley. 2009. The diarylquinoline 246 TMC207 for multidrug-resistant tuberculosis. N. Engl. J. Med. 360:2397-405. 247
6. da Silva, P. E., A. Von Groll, A. Martin, and J. C. Palomino. 2011. Efflux as a 248 mechanism for drug resistance in Mycobacterium tuberculosis. FEMS Immunol. Med. 249 Microbiol. 63:1-9. 250
7. Louw, G. E., R. M. Warren, N. C. Gey van Pittius, R. Leon, A. Jimenez, R. 251 Hernandez-Pando, C. R. McEvoy, M. Grobbelaar, M. Murray, P. D. van Helden, and 252 T. C. Victor. 2011. Rifampicin reduces susceptibility to ofloxacin in rifampicin-resistant 253 Mycobacterium tuberculosis through efflux. Am. J. Respir. Crit. Care Med. 184:269-76. 254
8. Adams, K. N., K. Takaki, L. E. Connolly, H. Wiedenhoft, K. Winglee, O. Humbert, P. 255 H. Edelstein, C. L. Cosma, and L. Ramakrishnan. 2011. Drug tolerance in replicating 256 mycobacteria mediated by a macrophage-induced efflux mechanism. Cell 145:39-53. 257
9. Gupta, S., S. Tyagi, D. V. Almeida, M. C. Maiga, N. C. Ammerman, and W. R. 258 Bishai. 2013. Acceleration of tuberculosis treatment by adjunctive therapy with 259 verapamil as an efflux inhibitor. Am. J. Respir. Crit. Care Med. 188:600-7. 260
10. Gupta, S., K. A. Cohen, K. Winglee, M. Maiga, B. Diarra, and W. R. Bishai. 2014. 261 Efflux Inhibition with Verapamil Potentiates Bedaquiline in Mycobacterium tuberculosis. 262 Antimicrob. Agents Chemother. 58:574-6. 263
11. Andries, K., C. Villellas, N. Coeck, K. Thys, T. Gevers, L. Vranckx, N. Lounis, B. C. 264 de Jong, and A. Koul. 2014. Acquired Resistance of Mycobacterium tuberculosis to 265 Bedaquiline. PLoS One 9:e102135. 266
12. Diacon, A. H., R. Dawson, F. Von Groote-Bidlingmaier, G. Symons, A. Venter, P. 267 R. Donald, A. Conradie, N. Erondu, A. M. Ginsberg, E. Egizi, H. Winter, P. Becker, 268 and C. M. Mendel. 2013. Randomized dose-ranging study of the 14-day early 269 bactericidal activity of bedaquiline (TMC207) in patients with sputum microscopy smear-270 positive pulmonary tuberculosis. Antimicrob. Agents Chemother. 57:2199-203. 271
13. Neal, R. A., J. van Bueren, N. G. McCoy, and M. Iwobi. 1989. Reversal of drug 272 resistance in Trypanosoma cruzi and Leishmania donovani by verapamil. Trans. R. 273 Soc. Trop. Med. Hyg. 83:197-8. 274
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

14. Martin, S. K., A. M. Oduola, and W. K. Milhous. 1987. Reversal of chloroquine 275 resistance in Plasmodium falciparum by verapamil. Science 235:899-901. 276
15. Diacon, A. H., P. R. Donald, A. Pym, M. Grobusch, R. F. Patientia, R. Mahanyele, 277 N. Bantubani, R. Narasimooloo, T. De Marez, R. van Heeswijk, N. Lounis, P. 278 Meyvisch, K. Andries, and D. F. McNeeley. 2012. Randomized pilot trial of eight 279 weeks of bedaquiline (TMC207) treatment for multidrug-resistant tuberculosis: long-280 term outcome, tolerability, and effect on emergence of drug resistance. Antimicrob. 281 Agents Chemother. 56:3271-6. 282
16. Johnston, A., C. D. Burgess, and J. Hamer. 1981. Systemic availability of oral 283 verapamil and effect on PR interval in man. Br. J. Clin. Pharmacol. 12:397-400. 284
17. Oros, A., M. J. Houtman, P. Neco, A. M. Gomez, S. Rajamani, P. Oosterhoff, N. J. 285 Attevelt, J. D. Beekman, M. A. van der Heyden, L. Ver Donck, L. Belardinelli, S. 286 Richard, G. Antoons, M. A. Vos, and C. investigators. 2010. Robust anti-arrhythmic 287 efficacy of verapamil and flunarizine against dofetilide-induced TdP arrhythmias is 288 based upon a shared and a different mode of action. Br. J. Pharmacol. 161:162-75. 289
18. Liao, W. B., M. J. Bullard, C. T. Kuo, C. T. Hsiao, P. H. Chu, and C. W. Chiang. 290 1996. Anticholinergic overdose induced torsade de pointes successfully treated with 291 verapamil. Jpn. Heart J. 37:925-31. 292
19. Shimizu, W., T. Ohe, T. Kurita, M. Kawade, Y. Arakaki, N. Aihara, S. Kamakura, T. 293 Kamiya, and K. Shimomura. 1995. Effects of verapamil and propranolol on early 294 afterdepolarizations and ventricular arrhythmias induced by epinephrine in congenital 295 long QT syndrome. J. Am. Coll. Cardiol. 26:1299-309 296 297
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
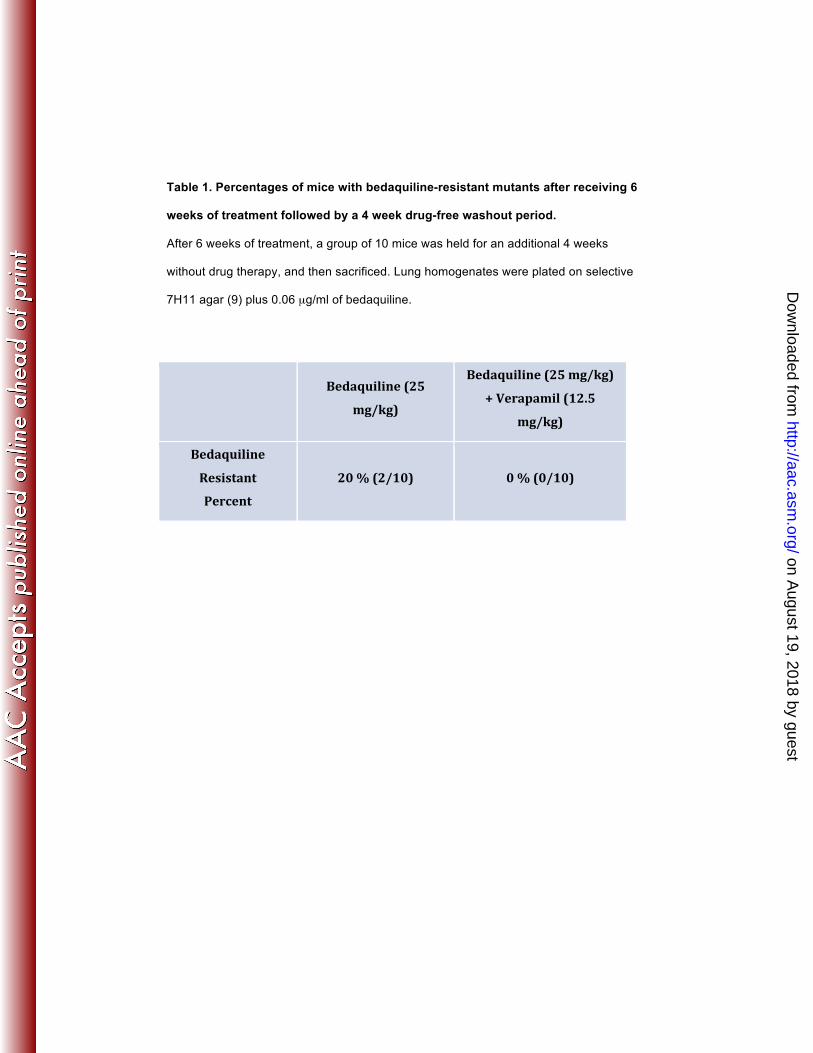
Table 1. Percentages of mice with bedaquiline-resistant mutants after receiving 6
weeks of treatment followed by a 4 week drug-free washout period.
After 6 weeks of treatment, a group of 10 mice was held for an additional 4 weeks
without drug therapy, and then sacrificed. Lung homogenates were plated on selective
7H11 agar (9) plus 0.06 µg/ml of bedaquiline.
Bedaquiline (25
mg/kg)
Bedaquiline (25 mg/kg)
+ Verapamil (12.5
mg/kg)
Bedaquiline
Resistant
Percent
20 % (2/10) 0 % (0/10)
on August 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from