Embed Size (px)
Citation preview
Points to consider when contemplating an
adaptive design study
Friedhelm Hornig Executive Director Biostatistics and Data Management Operations
Cytel Inc.
Clinical Operations in Oncology Trials Amsterdam, 2. Dec. 2015
1
Shaping the Future of Drug Development
Agenda
• Introduction and Motivation • An Example – The Valor Trial • Practical Considerations • Conclusions • An Encore – 10 Questions to Ask Yourself
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study 2
Introduction and Motivation
Definitions Terminology Variations Potential Benefits and Concerns
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 3
Three definitions of adaptive designs
FDA Draft Guidance for Industry (2010)
By adaptive design we refer to a clinical study design that uses accumulating data to decide how to modify aspects of the study as it continues, without undermining the validity and integrity of the trial.
PhRMA White Paper (2006) A study design is called “adaptive”, if statistical methodology allows the modification of a design element (e.g. sample-size, randomization ratio, number of treatment arms) at an interim analysis with full control of the type I error.
EMEA Reflection Paper (2007) An adaptive design clinical study is defined as a study that includes a prospectively planned opportunity for modification of one or more specified aspects of the study design and hypotheses based on analysis of data (usually interim data) from subjects in the study.
02/12/2015
F. Hornig: Points to consider when contemplating an adaptive design study 4
Some Types of Adaptations • Group sequential designs
o Early stopping for efficacy/harm/futility • Sample size re-estimation (blinded/unblinded) • CRM and modified CRM designs (Ph I, II) • Ph I/II designs (Dose-toxicity/Proof-of-Concept) • Adaptive Dose Finding
o Frequentist/Bayesian dose-response modeling • Treatment/dose selection (Ph IIb/ III) • Adaptive designs for combination therapies • Subgroup selection
o “Enrichment” (e.g., Biomarkers) o Incl./Excl. criteria change
• Changing objectives, o e.g. switching between non-inferiority and superiority
• Adaptive randomization • Change of primary endpoint or analysis
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 5
Possible Benefits
• Combine learning and confirming o Eliminate "White Space"
• Adress uncertainties with study-internal data • Option to check and correct assumptions • More ethical treatment of patients
o Fewer patients treated, with more optimal doses
• More efficient drug development o Better focused resources o Combine data from phases
• Overall, more flexibility and higher probability of success
02/12/2015
F. Hornig: Points to consider when contemplating an adaptive design study. 6
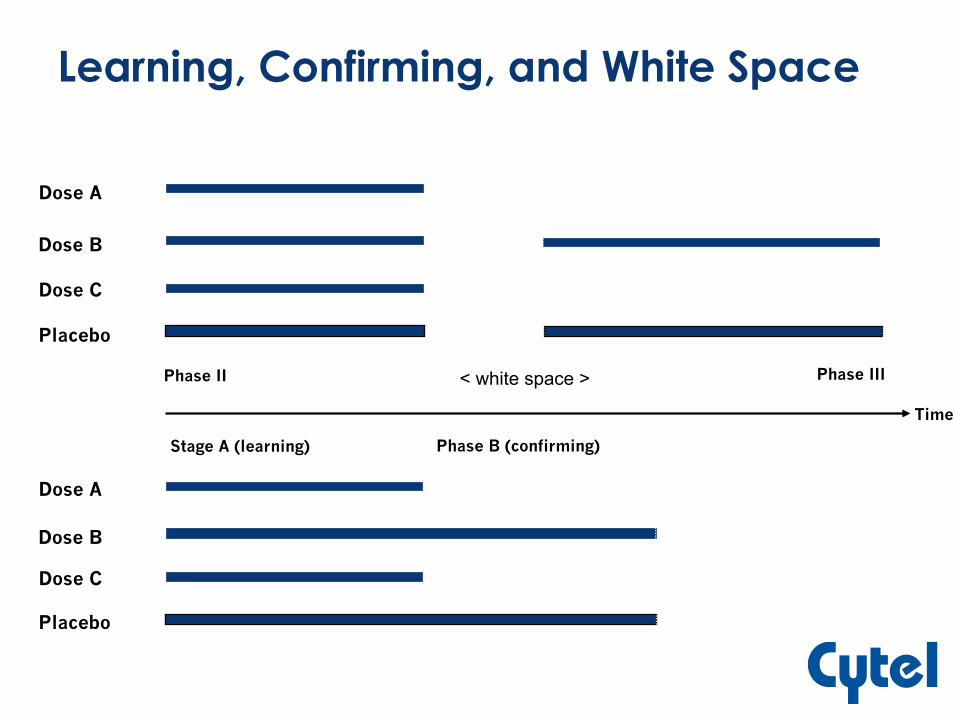
Learning, Confirming, and White Space
Dose A
Dose B
Dose C
Placebo
Dose A
Dose B
Dose C
Placebo
n < white space > Phase II Phase III
Stage A (learning) Phase B (confirming)
Time
In Contrast: Classical Full Development
Fixed Trial Designs Paradigm • Design features (assessments, patient population,
sample size, treatment arms ….) are fixed • No learning within study/phase • Exception: group-sequential trials allow early
stopping for superiority/futility
Strictly separated development phases • Planning and initiation of next phase time
consuming • No formal combination of evidence between
phases
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 8
Concerns by Health Authorities
Some illustrative concerns • Adaptation not a substitute for bad planning!
o Must have convincing reason for choosing AD
• Control of Type I error in confirmatory studies! • Avoidance of bias
o E.g., Adequate firewalls
• Adaptations defined in advance, and protocol for interim monitoring known in advance
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 9
An Example
The VALOR Trial
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 10
An Example – Valor Trial
Vosaroxin and Cytarabine combination evaluating Overall Survival in relapsed/refractory Acute Myeloid Leukemia (AML)
• Phase 3, double-blind, placebo- controlled, multinational trial
• Design for 90 % power at 5% significance level
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 11
Sponsor’s Dilemma
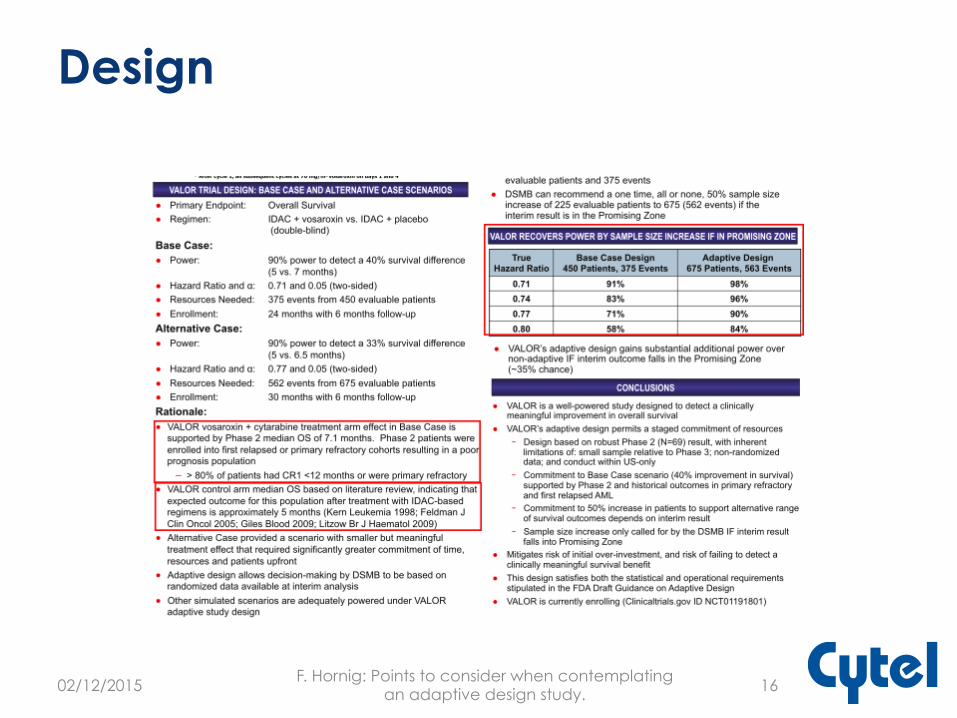
• Based on phase II data (N=69) o Assume HR = 0.71 o Requires 375 events, and 450 subjects
• But phase 2 estimates are subject to uncertainty: o What if HR = 0.77? (still clinically meaningful) o Require 616 events and 732 subjects o Not feasible for sponsor
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 12
Strategy of Staged Investment
• Power study to detect HR = 0.71 up-front • One interim analysis after 50% information
o Stop early if overwhelming evidence of efficacy o Stop early for futility if low conditional power o Increase number of events and sample size if
results are promising
This way risk is reduced and exit possible Higher investment only when more data / certainty
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 13
The Promising Zone Design
• Partition the interim outcome into three zones based on the interim estimate of conditional power o Favorable: CP ≥ 80% à no change to design o Promising: 30% ≤ CP < 80% à increase resources o Unfavorable: CP ≤ 30% à no change to design
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 14
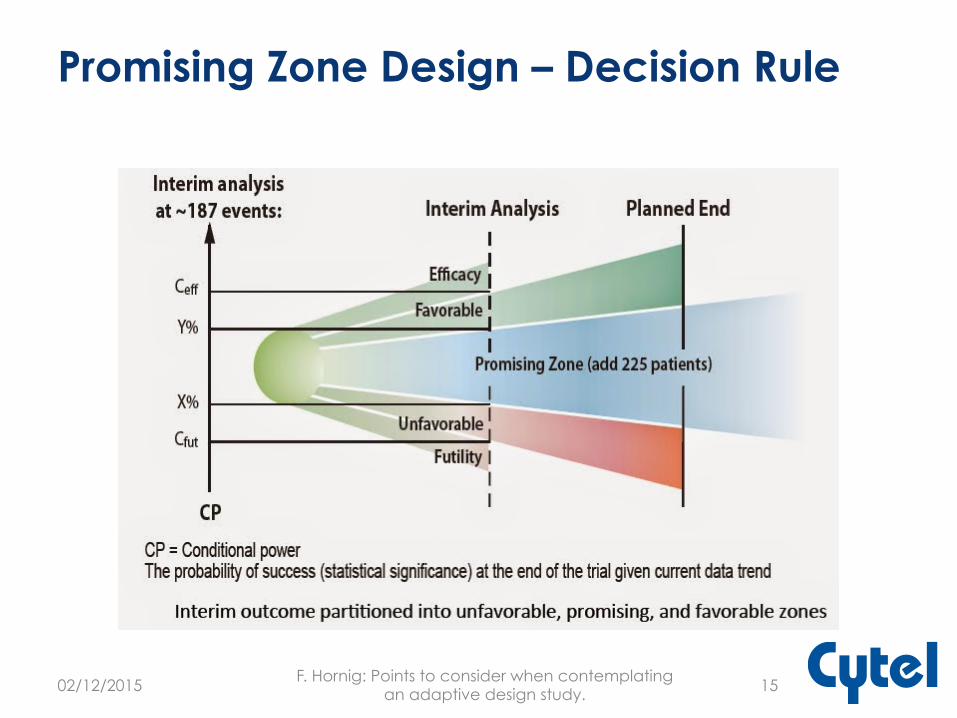
Promising Zone Design – Decision Rule
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 15
Design
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 16
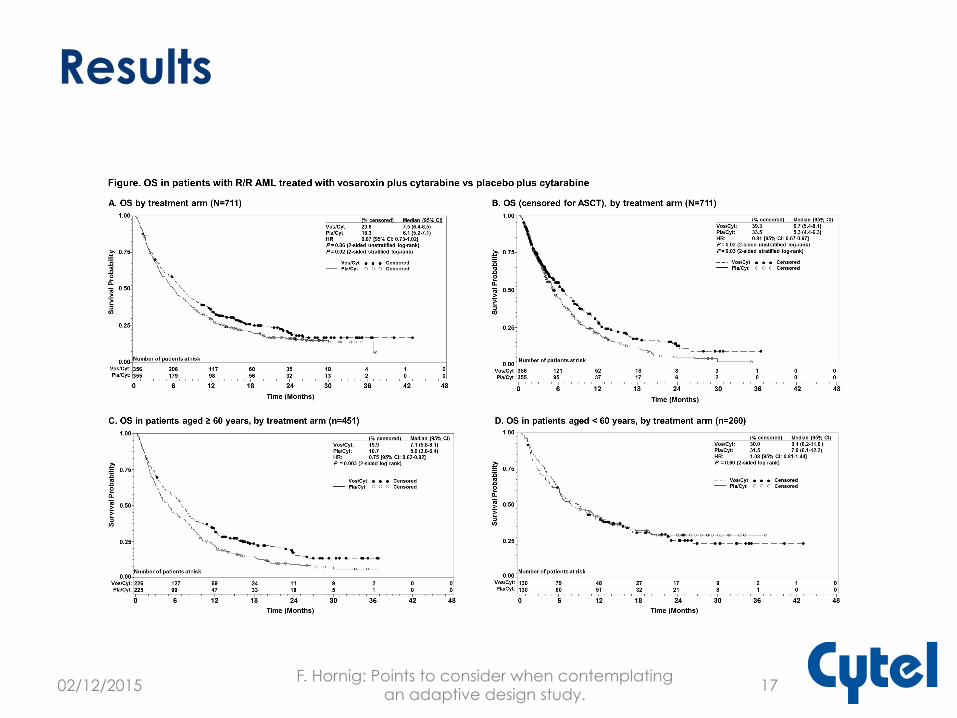
Results
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 17
Conclusions from results
• Study didn’t meet primary endpoint • Adaptation has increased chances of
success • Adaptation lowers the risk of failure, but
doesn’t eliminate it completely!
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 18
Practical Considerations
Planning Budgeting Health Authority Interactions Simulation Drug Supply CRF Design Preserving Trial Integrity Software
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 19
Planning
More up front time and effort for design and planning
• 12 months as rule of thumb • Thus, need early identification of candidates in
development plan
• Internal lobbying/training of all company stakeholders
• Health Authority / IRB dicussions • Simulations of study scenarios / decision rules à SAP • Randomization and drug supply • DMC and Independent Data Center preparation
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 20
Main Parameter - Enrollment vs. Endpoint
The length of time needed to make a decision relative to the time of enrollment must be small
• Shorter read-out time better (incl. data processing/analysis) • Otherwise enrollment must be paused
Using a surrogate marker could be a way out Rule of thumb: Overall recruitment duration is at least four times the observational period required before the primary endpoint reads out in any one patient.
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study 21
Budgeting
• Adaptive designs come with flexible budgets, but staged investments
• This can be a challenge to your finance department and process
• One option: Initially requesting the maximal budget, but with a probability assessment of likely expenditure
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 22
Health Authority Interactions
• For later phase studies up-front discussion with the HA is a MUST!
• Recommendation to contact HAs a year before starting your study! o Expect long and sometimes difficult discussions o Get support from extenal experts and experts in
the agencies (good experience with help from internal statisticians)
• The same for IRBs o Offer training and support
• Obviously, more important for later phase
trials, less concern for early phases
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 23
SIMULATIONS
• Essential to investigate the various potential outcomes of the trial under a range of plausible scenarios
• Investigate operating characteristics • Through probing the design options and
assessing “what-ifs” we understand sensitivity to or robustness of assumptions
• Main simulation results should be included in the protocol or analysis plan
• EAST Software as a tool
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 24
Drug Supply
• Number of subjects per treatment arm not known at the start of the trial o Flexible dosing options are important
• Thus, overage can be very substantial • Planning of supply can become very
complex • Simulation is a way to limit the risk
o Simulate probability for different outcome scenarios and drop low probability ones at risk
o Example: Simulations show that the total #kits can be reduced from 552 to 286 if one accepts a probability of stock-out of about 1/500 = 0.002
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 25
CRF Design
• Some scenarios may require changes to the CRF design as part of adaptation
• Important to prepare for CRF redesign, revalidation, and redeployment
• Not a necessity, but may be smart to plan for more probable scenarios
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 26
Preserving Trial Integrity
• Must have SOPs in place regulating process and adaptive decisions
• Need firewall between blinded and unblinded team
• Clear decision process and authority for DMC/sponsor/steering bodies
• More documentation needed o Simulation results and operating
characteristics to be documented in detail in protocol/SAP/publication
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 27
DMC and Independent Statistical Center
Need • Data Monitoring Committee (DMC)
o Safety AND efficacy (risk/benefit) o Ability to handle adaptive algorithms/process
• Independent Statistical Center (ISC)
Both unblinded • Importance to have watertight firewalls
between these unblinded bodies and anybody in the project team involved in the day-to-day running of the study
02/12/2015
F. Hornig: Points to consider when contemplating an adaptive design study. 28
Decision Making at Interim Analysis
Decision by DMC / steering body?! Sponsor participation – not encouraged
• If yes, need to document rationale • Sponsor reps distanced from trial conduct • Number limited!
Need to have competence in DMC and ISC to take decisons on adaptations
• ISC needs to have expertise in place, and be available for questions at very short notice
Give authority for decision to DMC! • Careful pre-specification extremely important!
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 29
Software
• Commercial software available for the planning and implementation of adaptve designs
• Simulation for decision scenarios and for drug supply are helpful tools
• See, for instance, at Cytel.com
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 30
Conclusions • Adaptive designs offer potential, on
ethics, efficiency and flexibility, and probability of success over classical development paradigm, but is no solution to all problems
• Need good rationale to justify additional efforts in upfront planning and logistics, to preserve validity and integrity of study
• Check whether conditions are met, get expert advise where needed, and use modern simulation tools, and it can be done!
02/12/2015
F. Hornig: Points to consider when contemplating an adaptive design study. 31
An Encore
10 Questions To Ask Yourself
See also cytel.com “To adapt or not to adapt“
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 32
10 questions to ask yourself (1-2)
Question1: • Assess whether the time between the interim
observation for adaptation and the enrollment of the last patient is enough to warrant an adaptive design.
Question 2: • If there is NOT enough time between interim
observation and final patient enrollment, determine whether there is a reliable surrogate or biomarker.
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 33
10 questions to ask yourself (3)
Question 3: • Determine whether there are any
regulatory concerns or reservations which would prohibit the use of an adaptive design
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 34
10 questions to ask yourself (4-5)
Question 4: • Consider how an adaptive design will
affect patient enrollment
Question 5: • Ascertain whether there is sufficient drug
supply to support all possible adaptations.
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 35
10 questions to ask yourself (6-7)
Question 6: • Can the required drug supply reach the
site under all possible scenarios. Requires simulations.
Question 7: • Is data acquisition and interim analysis
rapid enough?
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 36
10 questions to ask yourself (8-9)
Question 8: • Ensure there is sufficient statistical
expertise
Question 9: • How can software help to inform the
decision to adapt?
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 37
10 questions to ask yourself (10)
Question 10: • Given all the information above, decide
whether there are sufficient improvements to cost, savings in time and resources, and the quality of the data to warrant an adaptive design.
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 38
Thank You Very Much
Any Questions?
02/12/2015 F. Hornig: Points to consider when contemplating
an adaptive design study. 39