Embed Size (px)
Citation preview

Shaping Sefton
Session 3: Primary Care
14 October 2015 with
Dr Jane Weatherstone,
GP Director, Northumbria Healthcare NHS Foundation Trust
Welcome

Shaping Sefton
Session 3: Primary Care
Welcome
Martin McDowell
Chief Finance Officer, NHS South Sefton CCG/NHS
Southport and Formby CCG
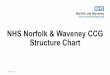
Agenda
Time Lead
13.15 Welcome Martin McDowell
13.25 Setting the Scene Martin McDowell
13.35 The Art of the Possible – Primary Care Services in
Northumbria
Dr Jane Weatherstone
14.00 What are we doing in Sefton?
Southport and Formby Dr Niall Leonard
14.15 South Sefton Dr Craig Gillespie
14.30 Local Workforce Issues and Opportunities and Opportunities Liz Thomas
15.00 Coffee break (inc freeflow until 5.30pm)
15.15 Sefton Community, Voluntary and Faith Sector Jan Campbell
15.25 Public Health Margaret Jones
15.35 Response and Reflections Dr Jane Weatherstone
15.45 Feedback, reminders and reflections from the earlier
sessions
Facilitators/ Dr Jane Weatherstone
16.00 What is the vision for Primary Care in Sefton?
Facilitated discussion
Dr Jane Weatherstone
17.30 Feedback Facilitators
17.45 Summary of the day – Actions and Next Steps Martin McDowell
18.00 Close and Thank You Martin McDowell
Setting the Scene
Martin McDowell
NHS Southport and Formby CCG
NHS South Sefton CCG
Chief Finance Officer

Vision
To create a sustainable healthy community based on health needs, with partners; focused on delivering high quality and integrated care services to all, to improve the health and wellbeing of our population
Strategic Priorities
• Caring for our older and vulnerable residents • Unplanned care • Primary care
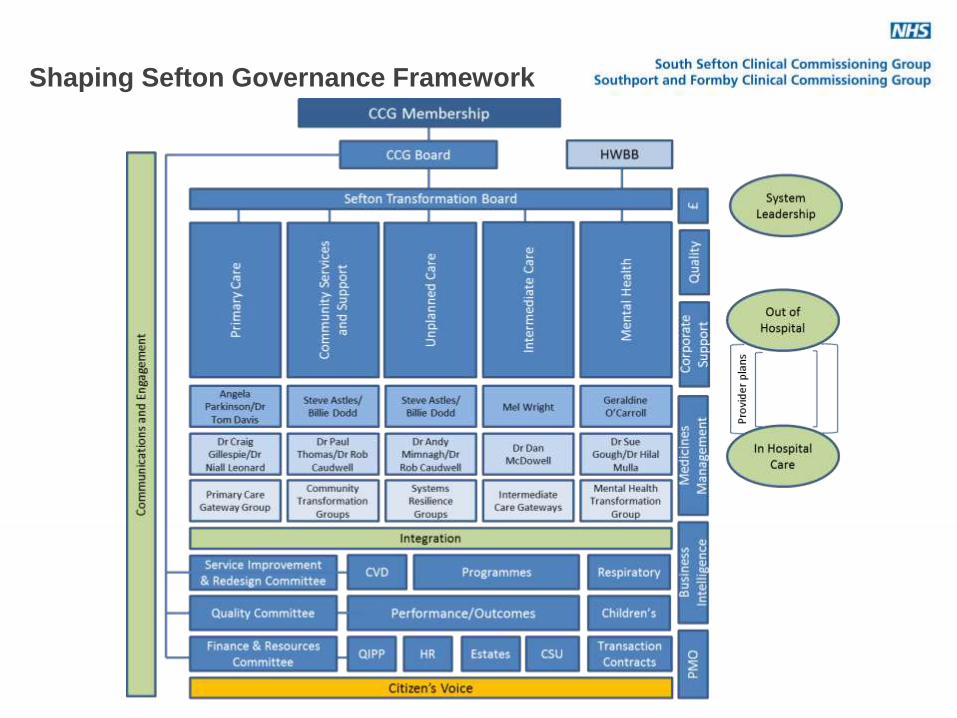
Shaping Sefton Governance Framework
Transformational Programmes – a refresher
Primary Care We will develop a population-based approach to primary care and support them to improve access to primary care and enhanced quality of service Community Care We will commission services that better link together right across health and social care – from hospital and community and social services, to GP practices and voluntary, community and faith sector organisations – and where as much care and support as possible is delivered outside of hospital, making it easier for people to access at the times that are more convenient to them Intermediate Care Our aim is to have ONE point of access, ONE assessment, ONE care planning process. We will do this by commissioning co-ordinated care for patients via integrated services and be responsive to patients needs
Transformational Programmes
Unplanned Care We will support urgent and unplanned care for our residents, focusing on admission prevention by developing quality primary and community services. We will ensure a quality and optimum experience for patients in acute care whilst also ensuring patients are supported to be in the right place for their care needs Mental Health Our aim is to have a cradle to grave mental health service across Sefton which is recovery focussed, visible, easily accessible, of high quality, safe and deliver beneficial outcomes. Emphasis will be placed on early intervention, recovery and integrated mental and physical health to enable patients to be managed better in the community with a reduced reliance on acute interventions. Dementia will be treated as a long term neurological condition within community based networks of care
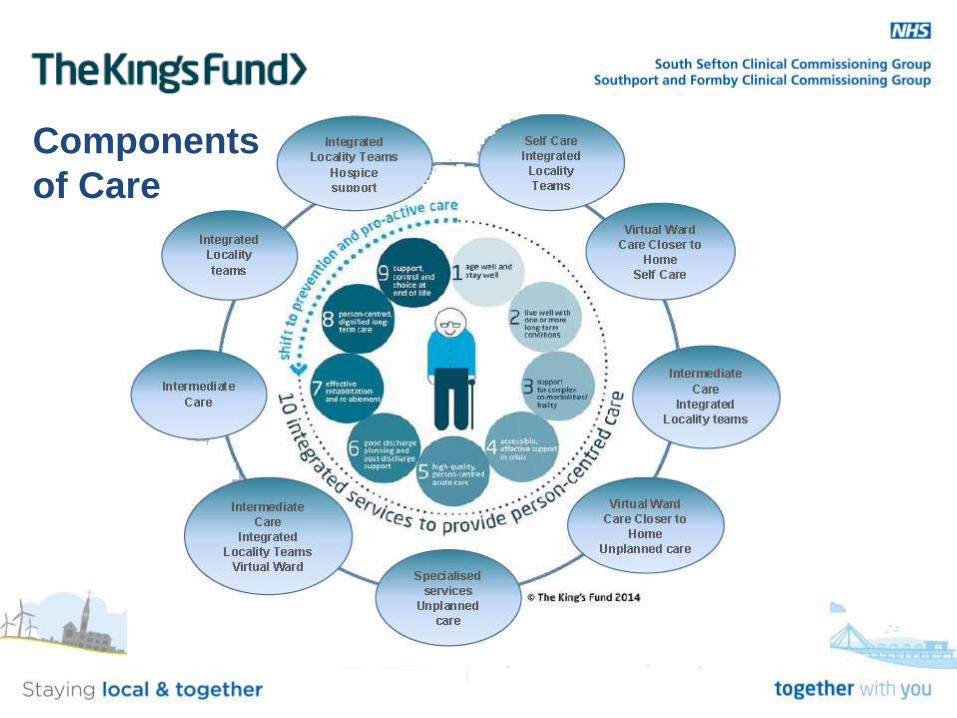
Components
of Care

• Northumbria Healthcare Foundation Trust, an Integrated Care Organisation
Dr Jane Weatherstone GP Clinical Director
A bit of background
• GP in local area for 22 years
• Set up GP consortium in North Tyneside
• Clinical co-chair of NT CCG
• First person nationally to do my role
10/15/2015
The art of the possible
• Is not…….
• Stepford primary care
• Reduced workload
• Reduced expectation
• Newcastle winning a match 10/15/2015
Northumberland
-Northumberland – 45 GP practices, 42 PMS, 3 GMS.
– Northumberland County Council/Care Trust
– Population 320+k, over most of the 2,500 sq miles. 4 natural localities.
– Mix of; rural, urban, affluent and very deprived
– Vanguard
- Long history of locality working and 3 federations
- Frail elderly population growing
10/15/2015
North Tyneside
– 29 Practices, 2/3 GMS.
– Population 220k, Urban and concentrated
– Mix of affluent and deprived
– North Tyneside Council
– 4 localities
– 1 GP federation
10/15/2015
The North East
• Mixed economy- reasonable disposable income
• Legacy of ship building and coal mining industry
• Great place to learn and live but decreased GPVTS applicants, difficulty retaining and recruiting
10/15/2015
Working with Primary Care -What we do !
Primary Care - Long History of GPs working with Northumbria
• GPs working in leadership roles within trust for many years
• GPs have attended Clinical Policy Group since 1998
• Clinical Leads Forum since 2005
• GP Medical Director since 2002
• Other roles; GP CIO, GP Clinical Directors of Community Business Unit, GP Public Health lead, Joint posts-A&E and GP, GP Vanguard lead
Working with Primary Care - Provision
• Engagement program, ‘you said we did’,
– ‘Excellence through Collaboration’
– GP Hotline, LMC co-opted members
• Working with Community Services - The Compact and ‘The Offer
• Direct working with Primary Care Providers and aligned incentives
– LINS, Frail elderly pathway, COPD, Care planning and YoC (DM)
– Federation development
• Hadrian Primary Care Alliance
• Lindisfarne Health Ltd
• Tyne Health Ltd
– Joint work with OOH GP provider
– GPs on the Base sites
– Business Joint ventures
• PointNorth CIC – Direct Primary Care provider (PMS contract)
• NORPRIME
– Northumbria Primary Care Ltd
Northumbria Primary Care Ltd Setting Up
• Solely owned company • Offer of support for Primary Care @ Different levels.
– One off requests for support – Back Office support, Pay roll, HR, Occ health, procurement, Education
and Training, CQC support, Lease Cars, Estates support, call handling? – Full Support – Full ownership
• Started with 2 practices for the higher levels of support – 1 GMS, 1 PMS, with several others interested
• 4 streams of work – HR – The NPC Offer – Organisational structures, regulation and legals – Finance and Performance
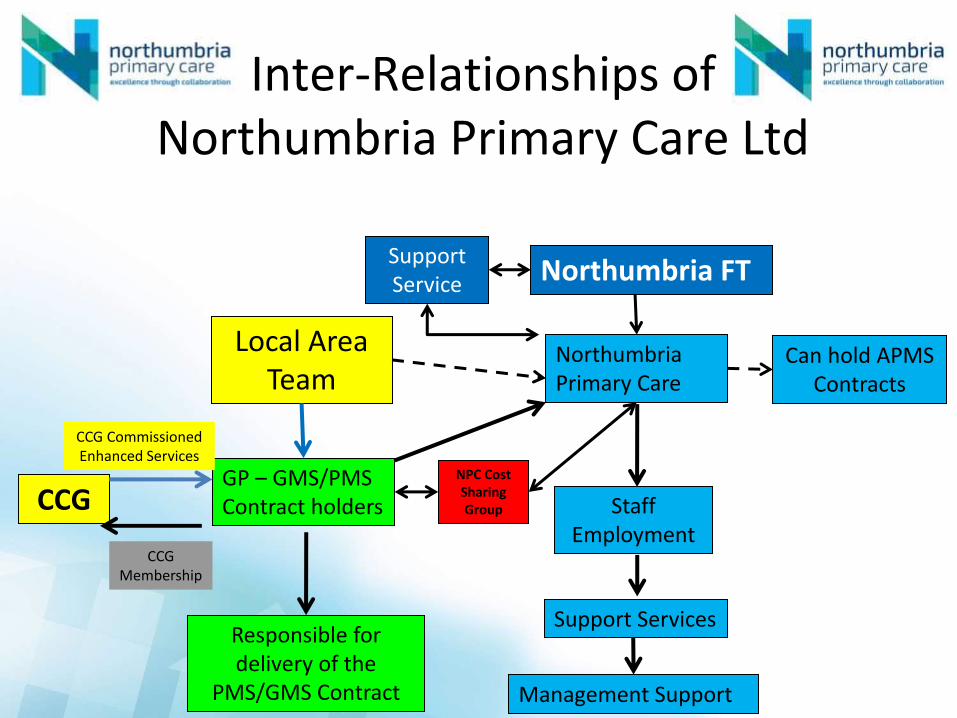
Inter-Relationships of Northumbria Primary Care Ltd
Local Area Team
GP – GMS/PMS Contract holders
Responsible for delivery of the
PMS/GMS Contract
Northumbria Primary Care
Staff Employment
Support Services
Management Support
Northumbria FT Support Service
Can hold APMS Contracts
CCG
CCG Membership
CCG Commissioned Enhanced Services
NPC Cost Sharing Group
Northumbria Primary Care Ltd, Where are we?
• Company and Board formed – Sept 14 , structure agreed.
• NHSE final approval of Sub-contract agreed and CQC approved
• Cost Share Group established, approved by HMRC
• Live, 1st April 2015, incl TUPE Transfer
• Achievements already
– Executive GPs for each practice - attend executive group
– Improved quality and financial stability
– ID potential waste to re-invest
– Joint Appointments of GP
– New models of acute delivery, eg pharmacists already running in 2 practices
The Local Future?
• Reshaping of local Primary Care or continue as we are – locally 4 models emerging
– Status Quo
– Mergers
– Practices working together more (incl Federations)
– Northumbria Primary Care
• NPC and rate of expansion
– Capacity and scaling up
– Expectations and the eye of scrutiny
• Threat and opportunity of the Vanguard
• Accountable Care Organisation
Northumberland Vanguard
4 Phases to project – delivery by 16/17 – full evaluation
Phase 1:
• Delivery of 7 day Specialist emergency care hospital – Separation of emergency and elective work streams
– 7 day specialist consultant presence and 7 day diagnostics
– 24/7 A&E consultant presence
– Primary care hubs across at NTGH, WGH and HGH
– Delivered on 16th June 2015
– Data collection for outcomes framework underway for phase 1
Phase 2 & 3 • Distinct phases but intrinsically linked – not sequential • Delivery of primary care at scale! Hub Creation
– H0: 7 day access to primary care as determined by the local population has no impact on A&E attendances / VFM
– Locality based model – not a one size fits all – Concept of primary care consultant – sickest / most
complex patients to be seen by most skilled – community NSEC (H)
– Efficiencies in primary care
• Requirement of an alternative workforce – national freedoms and local innovation
• Movement of primary and secondary care consultants – working into and out of hospitals / working into and outside of community / people’s homes
• VFM ??
Phase 2 & 3 • Workforce – key issue for PACS moving forward
– Local control and freedoms from centralised medical recruitment – Alternatives to medical workforce – NP, PA (theatres) already well
established in NSECH / base sites – Physicians assistant (gen med) – early days – Primary Care – Pharmacist and Nursing delivery models, integrated
PN, PA and DN – Community – blended skills/team between nursing and social care – Create Multi skilled support staff – Core sets of skills required - Recognition of NEAS, Pharm, nursing,
scientists ability to provide (working outside professional silos) – Development of condensed nurse training programme - 24 months
• IT – Interoperability and Information governance – Tele health and telemedicine
• Public Health, Population Health and Health promotion
Northumberland PACs & ACOs • Understanding the impact of whole system working across 7 days
• Move towards full integration (provision and commissioning)
• Development of an Accountable Care Organisation by April 2017
BUT
• Financial benefit and ability to move at speed to ACO earlier?
• Move to ‘Group model’ and ACO model across both CCGs - National support – Legal advice for governance arrangements of new model
– Membership of group ACO and role of NHCFT vs each local ACO
– Solution for adjacent patches in difficulties
• Managing public and partner expectations
• Moving into the unknown but some international evidence – potential learning
• System wide change required if we are to survive in the future
• PACS and ACOs – real opportunity to understand impact of 7 days, vfm of proposed services and removal of excess costs/waste
North Tyneside
• New model of care (again)
• Extensivist model
• Release capacity in primary care for those underneath the top of the triangle
• No new money
10/15/2015
Community based Initiatives • LINS/Frail elderly pathway (3 years)
– Creating practice-based MDTs, (GP, D/Ns, SW, Pharm)
– Tool-based creation of list of vulnerable patients
– Community Matron Assessments
– Care Plan developed
– Key Worker identified
• Short term support team (rapid and up to 6 wks intensive rehab)
• Admission avoidance team
• Nursing Homes; GPs, Matrons and SHINE project
• Single Point of Access
• Integrated Estate 10/15/2015
Nobody said it was easy….
• Things can be done differently
• Requires buy in from all parties- including the patient
• It wont happen overnight
10/15/2015
10/15/2015
Insanity: doing the same thing over and over again and expecting different results. Albert Einstein
Thank you
Any questions?
10/15/2015
What are we doing in Sefton
Southport and Formby
Dr Niall Leonard
Clinical Vice-Chair
NHS Southport and Formby CCG
The Facts
• 19 practices 2k-17k
• Population 122k and increasing
• 4 localities of 30k
• 1800 Care Home beds
• Popular retirement destination
• Demographics 25 years ahead rest of UK
• 45% adult unplanned care >75yrs
35
Strategic Priorities
• Caring for old and vulnerable
• Unplanned Care
• Primary Care
36

Local Quality Contract
• Frail and Elderly
• End of Life
• Practice Development
37
Federation
• Sign up/formation
• Find partners to bid with
• Sustainable at 12 months
38
Supporting Cast
• Community Emergency Response Team (CERT)
• Intermediate Care Beds
• Community Geriatric Service
• Respiratory Program
• Data Sharing
39

Opportunities
• Re-procurement Community Services
• Sustainability review – Southport & Ormskirk
• Voluntary Sector
• Prevention /Self Care Agenda
40

Threats
• Workforce
• Community Services
• Estate
41
Vision
• 4 Primary and Community Care Hubs where mental health service, Social Services, CVS, diagnostics are based
• Each serving 30k
• Urgent Care facility/Out of Hours facility with AED
• Smaller Hospital- Day case, diagnostics OPD, medical inpatients
• Enlarged Intermediate Care capacity
• Fit for purpose Out of Hours service
42

Where do we start?
• One Locality-Hub model ?Formby
• Urgent Care Centre model with AED
• Revisit Out of Hours
• Define what clinical quality is in Primary Care
• Develop Local Quality Contract to drive that quality
43
New Model of Primary Care
• Blank sheet
• Population needs
• Workforce capabilities
44
What are we doing in Sefton
South Sefton
Dr Craig Gillespie
Chair
NHS South Sefton CCG
Group of 31 practices serving 155,000 patients
22 independent practice mostly GMS
9 practices run by a regional multi-practice organization (SSP
health) - APMS contract due to expire around the beginning 2016
South Sefton CCG
Legal duty to “support quality improvement in primary care”
Co-commissioning----Greater involvement
so… GMS, PMS, APMS, QOF etc are all the responsibility of NHSE.
…however as system leaders we want to help NHSE shape general practice so
that it fits with other parts of health economy
What is South Sefton CCG’s role
in Primary Care?
What does high quality General Practice looks like?
…in a paper in 2013 The Kings Fund and The Nuffield Trust described 6
core attributes consistent with high quality General Practice:
comprehensive
patient centred
population oriented
coordinated
accessible
safe and high clinical quality
Supporting Quality Improvement
Accountable for meeting the majority of patients physical and mental health
care needs including:
wellness
prevention
acute conditions
long term conditions
organisations refer and coordinate other community and specialist services,
and signpost patients to local welfare and other social support services.
Comprehensive
Local Quality Contract: funding to offer a wider range of services. Understand
the needs of the population and ability to provide proactive and reactive
care through community services such as the virtual ward or Urgent care
team
Dragon’s den allowed practices to pitch innovative ideas to broaden and
enhance Pt care.
GRASP tools for AF and heart failure to support care
VCF—support wellness and reablement etc. VCF direct and Strand health and
well being shop
Comprehensive
Not just about being holistic, involving patient and carers in decision making
Also about continuity and trust
Bread & butter general practice but when it goes wrong it has marked
destabilising effects
Person centred
LQC funds practices to give a person centred approach to wellness and
prevention for patients >70yrs. Encourages a holistic approach involving
patients, family and carers.
EoL scheme person centred care of the dying.
VCF-support and funding for Sefton carers
Person centred
Practices have a responsibility for providing services to their registered patients
The CCG believe in the benefits of list based GP for continuity and better
understanding of population demographics
Most GPs in South Sefton have been GPs in SS for a long time and are Sefton
residents
Population orientated
LQC: funds practices to offer additional services to frail patients.
Respiratory projects- training for GPs, nurses and HCA’s, inhaler project rolled
out CCG wide, community respiratory teams to support Pts with COPD
The VCF and Strand health and wellbeing shop address health inequalities
WellSefton provided by the WellNorth team are looking broader aspects and
wider determinants of health. Aligning health system and economic growth
priorities to address health inequalities
Making every contact count is a training session GP staff to help them have
conversations with patients that support healthy lifestyle choices
Population orientated
Responsibility for ensuring care is co-ordinated across all elements of the
health care system
In particular, transitions between organisations
Co-ordinated
Considerable cross over between LQC frailty scheme and the avoiding
unplanned admission DES this promotes co-ordinated approach
Virtual ward, urgent care, CICT & discharge planning teams support practices
and patients to improve transitions between primary and secondary care
Pathfinder scheme is work with NWAS so that patients can be signposted to
most appropriate service
CHiP project which is a multifaceted project for care homes, providing
telehealth, community matrons to co-ordinate care
Co-ordinated
‘Appropriate’ waiting times
24/7 access to medical and nursing care
The organisation is responsive to patient preferences around access
Accessible
LQC: Incentivises improved access in and out of usual working hours
Opportunity to look at practice needs and consider which model
of care can best deliver those
Encourages practices to broaden skill mix
HCA: Apprentice scheme working with Hugh Baird College and practices.
CHiP: Provides community matron as first port of call for care homes
Provides telehealth for clinical advice
ERICOM: IT strategy that supports mobile working with tablets
Accessible/workforce
Housebound reviews: nursing review of vulnerable cohort
WIC: redesign to be GP led.
IPLATO: text messaging to reduce DNA’s etc
MMT: supporting every practice for high quality prescribing
AVS: for visits to care homes
(NW deanery have agreed to align SS to Liverpool (rather than S&O) trainees
tracks-more registrars training and hopefully staying in South Sefton)
Accessible/workforce
Care is evidence based
Peer support and review of performance for quality assurance
The organisation is financially sustainable, such that safety and quality
standards are not compromised by resource pressures!
Safe and high clinical quality
Peer review and support at locality group
LQC and PQS-support drive for high clinical quality
IT facilitators: audits for quality in management of AF and heart failure etc
Protected learning time: afternoon every month for professional and practice
development
Safe and high clinical quality
e-learning: package provided for practice nurses-clinical and mandatory
training
Quality Improvement: teaching on quality improvement techniques provided by
AQUA and Dr Chamberlain (QI fellow)
Financial sustainability: LQC represents a £3 million investment in general
practice
Safe and high clinical quality
Drivers:
GP, practice nurse and HCA workforce:
National shortage of GPs
Re-procurement of APMS contracts
Retirements
Estates: need modernisation, many not fit for purpose/DDA compliant
Long term strategy that requires CCG/NHSE/practices and public to
work together
So why transform General Practice?
I believe that we already have the building blocks for great general
practice in South Sefton
The question we need to answer is:
What model should we build?
…The Future?
Shaping Sefton Primary Care Workforce
Transformation
Liz Thomas
Senior Programme Manager Workforce Transformation
www.nw.hee.nhs.uk
twitter.com/HENorthWest
“HEE is here to improve the quality of
healthcare for the people and patients of
England through education, training and
lifelong development of staff.”
• One Health Education England • Thirteen Local Education Training Boards (LETBs), of which Health
Education North West is the largest • Three Local Education and Workforce Groups (LWEGs) covering
Cheshire and Merseyside, Cumbria and Lancashire, and Greater Manchester
Health Education England
www.nw.hee.nhs.uk
twitter.com/HENorthWest
What is Workforce Transformation
Developing a
workforce
responsive to
changes in
care, now and
in the future
• Future supply – more
of the same & more of
something different
• Up-skilling staff,
carers & volunteers
• Developing and
promoting new roles &
ways of working
www.nw.hee.nhs.uk
twitter.com/HENorthWest
How we work
Working across 3
key parts of the
system with
cultural
transformation
thread throughout
• In hospital
• Community based
care, including third
sector
• Primary care,
including dentistry,
optometry and
community pharmacy
www.nw.hee.nhs.uk
twitter.com/HENorthWest
Three Key Priorities
• Building the foundations –
developing the systems and
processes for systematic
transformation at pace
• Priority objectives – identifying
the key deliverables and ‘quick
wins’
• Transformational innovations –
generating the evidence base and
learning for wider adoption and
spread in the medium and long
term

www.nw.hee.nhs.uk
twitter.com/HENorthWest
Cultural Transformation Framework
Aim: To support organisations
with transforming workplace
culture
• Promote a shared understanding of
culture in the workplace
• Define changes in culture and
behaviours required by the healthcare
workforce
• Provide practical resources to support
cultural change
www.nw.hee.nhs.uk
twitter.com/HENorthWest
National Context
• Primary Care Commission http://hee.nhs.uk/wp-content/blogs.dir/321/files/2015/07/The-
future-of-primary-care.pdf
• 34 recommendations for HEE, NHS England, CCGs, General Practices
• Focusing on multi-disciplinary workforce, making better use of technology,
federations and networks of practices, integrating care, quality and safety, creating
learning organisations and particular recommendations for specific populations
• New Care Models Vanguard Sites http://www.england.nhs.uk/ourwork/futurenhs/5yfv-
ch3/new-care-models/ - in the North West:
• 3 Integrated Primary and Acute Care Systems
• 3 Multispecialty Community Providers
• 2 Acute Care Collaboration
www.nw.hee.nhs.uk
twitter.com/HENorthWest
National Context
• Shape of Caring Review http://hee.nhs.uk/wp-content/blogs.dir/321/files/2015/03/2348-
Shape-of-caring-review-FINAL.pdf
• 34 recommendations across 8 themes including enhancing the voice of the patient
& public, valuing the care assistant role, widening access for care assistants who
wish to enter nursing, developing a flexible (education) model and assuring high-
quality learning environments, on-going learning and funding and commissioning
• HEE Mandate https://www.gov.uk/government/publications/health-education-england-
mandate-april-2015-to-march-2016
• Over 100 deliverables either to be delivered in 2015/16 or for good evidenced
progress to be made
• Focuses on children and young people, integrated care, mental health, public
health, the right workforce with the right skills and behaviours (including e.g.
specified recruitmen number of GP trainees), value for money in education and
training funding
www.nw.hee.nhs.uk
twitter.com/HENorthWest
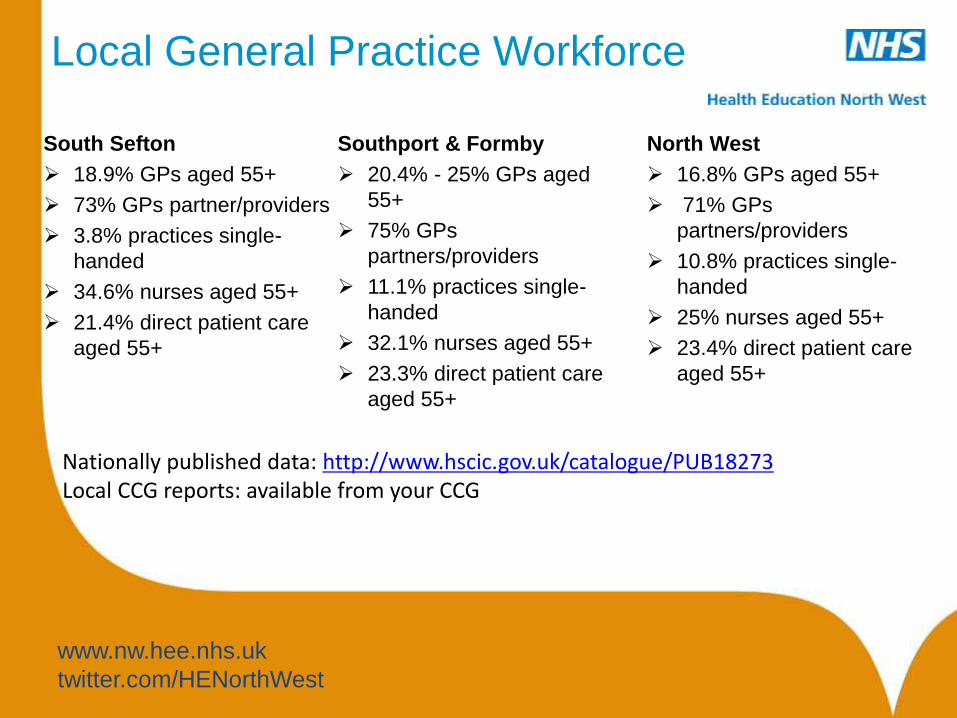
Local General Practice Workforce
South Sefton
18.9% GPs aged 55+
73% GPs partner/providers
3.8% practices single-
handed
34.6% nurses aged 55+
21.4% direct patient care
aged 55+
Southport & Formby
20.4% - 25% GPs aged
55+
75% GPs
partners/providers
11.1% practices single-
handed
32.1% nurses aged 55+
23.3% direct patient care
aged 55+
Nationally published data: http://www.hscic.gov.uk/catalogue/PUB18273 Local CCG reports: available from your CCG
North West
16.8% GPs aged 55+
71% GPs
partners/providers
10.8% practices single-
handed
25% nurses aged 55+
23.4% direct patient care
aged 55+
www.nw.hee.nhs.uk
twitter.com/HENorthWest
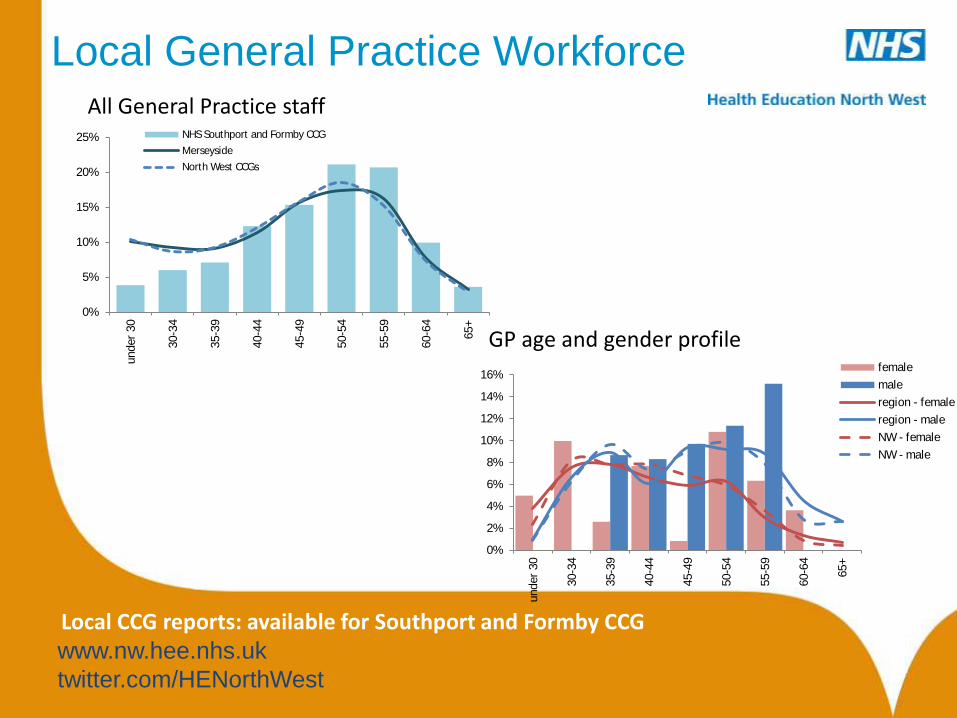
Local General Practice Workforce
Local CCG reports: available for Southport and Formby CCG
0%
5%
10%
15%
20%
25%under
30
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65+
NHS Southport and Formby CCG
Merseyside
North West CCGs
0%
2%
4%
6%
8%
10%
12%
14%
16%
under
30
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65+
female
male
region - female
region - male
NW - female
NW - male
All General Practice staff
GP age and gender profile
www.nw.hee.nhs.uk
twitter.com/HENorthWest
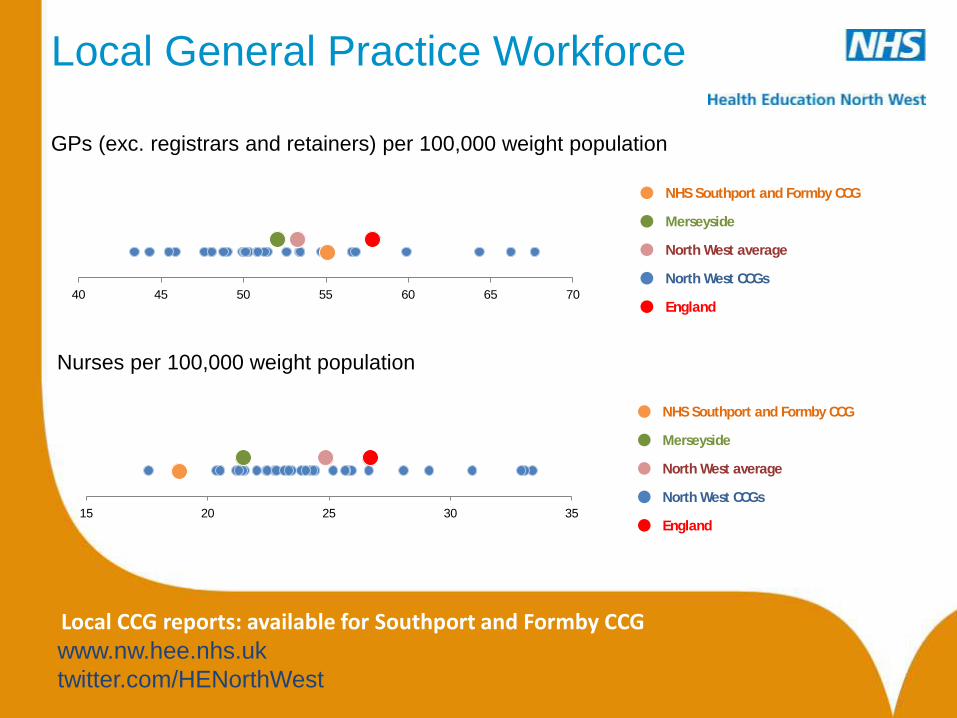
Local General Practice Workforce
GPs (exc. registrars and retainers) per 100,000 weight population
l NHS Southport and Formby CCG
l Merseyside
l North West average
l North West CCGs
l England 40 45 50 55 60 65 70
l NHS Southport and Formby CCG
l Merseyside
l North West average
l North West CCGs
l England 15 20 25 30 35
Nurses per 100,000 weight population
Local CCG reports: available for Southport and Formby CCG
www.nw.hee.nhs.uk
twitter.com/HENorthWest
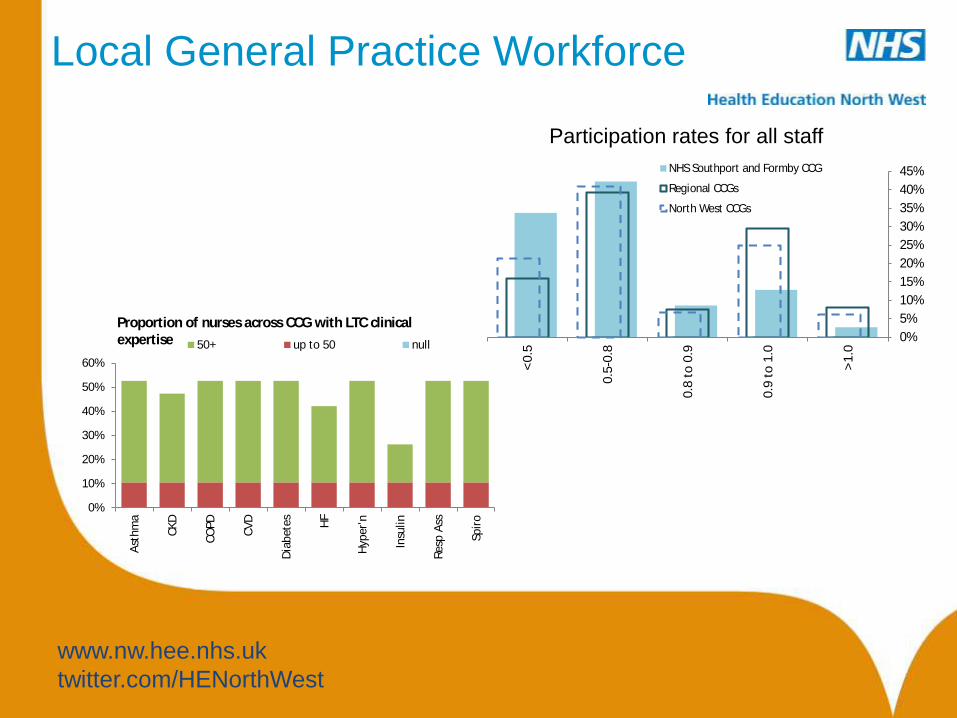
Local General Practice Workforce
Participation rates for all staff
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
>1.0
0.9
to 1
.0
0.8
to 0
.9
0.5
-0.8
<0.5
NHS Southport and Formby CCG
Regional CCGs
North West CCGs
0%
10%
20%
30%
40%
50%
60%
Ast
hm
a
CK
D
CO
PD
CV
D
Dia
bete
s
HF
Hyp
er'
n
Insu
lin
Resp
Ass
Spir
o
Proportion of nurses across CCG with LTC clinical
expertise 50+ up to 50 null
www.nw.hee.nhs.uk
twitter.com/HENorthWest
Case Studies
• Well being-coordinators within GP practices – Cheshire Age UK
• Pharmacy technicians in General Practice – East Cheshire
• Medicines management in practice
• Savings and improved quality service to patients
• Optometry Minor Eye Condition services – Greater Manchester
• Community Pharmacists non-medical prescribing and developing strong relationships
with GP and practice – Barrow-in-Furness
• Healthy Living Pharmacies
• Nurse educators working into care homes to educate nursing staff - North Devon
• Physician Associates in General Practice – North Yorkshire
• PAs (3) now see 21 appointments per day each, equivalent to 315 appointments per
week / 15120 per annum
• Previous GP appointments were equivalent to 165 per week, or 7260 per annum
• Telephone consultations
• Don’t just do “simple” patients
www.nw.hee.nhs.uk
twitter.com/HENorthWest
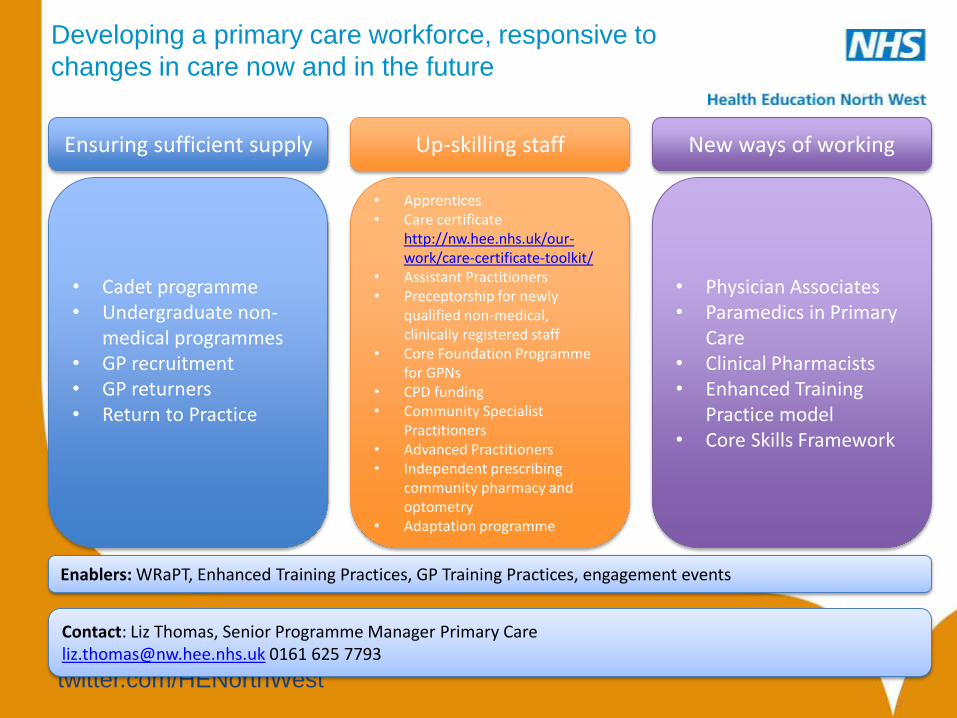
Developing a primary care workforce, responsive to
changes in care now and in the future
New ways of working Up-skilling staff
• Cadet programme • Undergraduate non-
medical programmes • GP recruitment • GP returners • Return to Practice
Ensuring sufficient supply
• Physician Associates • Paramedics in Primary
Care • Clinical Pharmacists • Enhanced Training
Practice model • Core Skills Framework
• Apprentices • Care certificate
http://nw.hee.nhs.uk/our-work/care-certificate-toolkit/
• Assistant Practitioners • Preceptorship for newly
qualified non-medical, clinically registered staff
• Core Foundation Programme for GPNs
• CPD funding • Community Specialist
Practitioners • Advanced Practitioners • Independent prescribing
community pharmacy and optometry
• Adaptation programme
Enablers: WRaPT, Enhanced Training Practices, GP Training Practices, engagement events
Contact: Liz Thomas, Senior Programme Manager Primary Care [email protected] 0161 625 7793
www.nw.hee.nhs.uk
twitter.com/HENorthWest
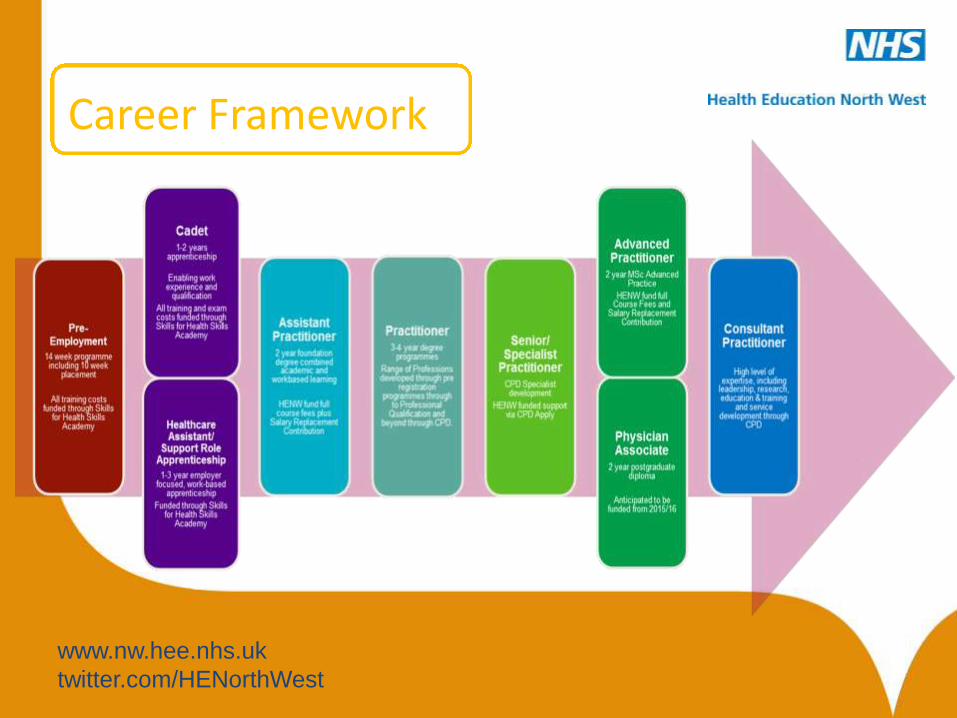
Career Framework
www.nw.hee.nhs.uk
twitter.com/HENorthWest
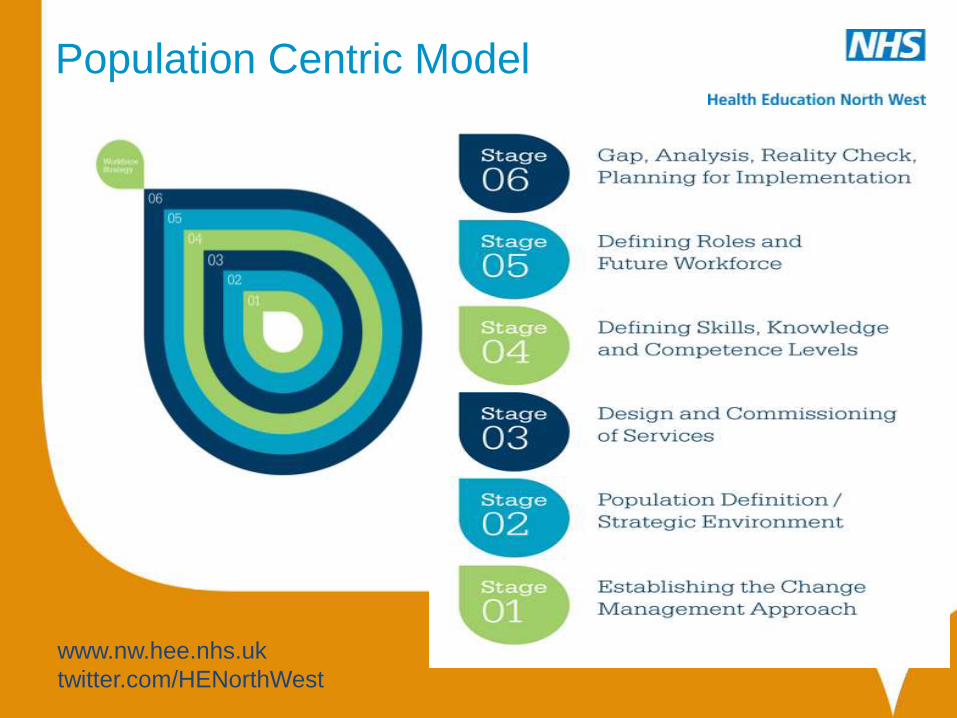
Population Centric Model

www.nw.hee.nhs.uk
twitter.com/HENorthWest
Head of Workforce Transformation [email protected] Senior Programme Manager, Cultural Transformation [email protected] Senior Programme Manager, Community-Based Care Lead Contact Project Officer Senior Programme Manager, Primary Care Lead [email protected] Project Officer [email protected]
The Workforce Transformation Team

Coffee
15.00 – 15.15
Sefton Community, Voluntary and
Faith Sector and Primary Care
Jan Campbell
Sefton CVS
Opportunities for Improving Health and
reducing Inequalities through Primary
Care Public Health
Margaret Jones
Interim Director of Public Health
Sefton Council
Five Year Forward View
• Warns – The health and wellbeing gap could widen, and
– Ability to fund beneficial new treatments will be lost due to spending on avoidable illness
Is this a local issue?
• 10-12 year gap in life expectancy between rich and poor areas
• Quarter of children living in poverty
• Half of people are overweight or obese
• 1 in 5 smoke – big inequalities
• In bottom 10 nationally for alcohol related deaths and hospital admissions for men
Yes
Sefton Council’s Strategic
Approach
Action across the four domains of public health:
•Population health care
•Health improvement
•Wider determinants
•Health protection
Through:
•Universal, and targeted proportionally services to reduce health
inequalities
•Influencing, enabling, commissioning
•In Sefton and across Merseyside (Cheshire)
88
Role for NHS set out in Forward
View
• Secondary prevention
• Empowering patients
• Engaging communities
• NHS as social movement
Health care
• Healthy Child Programme
• Prevent and treat avoidable illness – alcohol and sexual health services, NHS Health Checks, making every contact count
• Support those with Long Term Conditions and disabilities
90
Integrated Wellness in Sefton
• One point of contact
• Behaviour change programmes: alcohol, mental wellbeing, healthy weight, smoking cessation
• Health Trainers- Colleges, GPs, community venues, Health champions/Peer mentors
• Information & marketing
• IWS Network
91
Wider Determinants
Taking action on the causes of the causes through
influencing and enabling
Planning Local plan
And policies
Transport Active travel 20s plenty
Cost and availability of
alcohol Licensing
Obesogenic environment
Use of outdoor space
Food accessibility and availability
Housing Fuel
poverty
Port development
Air quality and health
92
Protecting Health – the
contribution of Primary Care,
CCGs & LA
• Incident and outbreak response
• Emergency preparedness and response
• Partnership approach to ensure quality of delivery of screening and immunisation
• Partner in planning and securing services needed to protect health, e.g. hepatitis treatment, community TB nursing service
• Assurance around health care associated infections & AMR
93
Opportunities for Primary Care to
improve the Public’s health
• Representational:
Represent the health and wellbeing interests of your practice/CCG and its communities, influencing the policies, priorities and services commissioned by the CCG and partner organisations
• Community Leadership: Ability to influence and encourage healthy behaviours of local residents. Ensure
the involvement of local communities when developing plans and strategies that address improving health and community wellbeing.
• Policy and Scrutiny: Commission to reduce health inequalities and inequity of access to services
• Partnership: Achieving healthy outcomes for communities through partnership work
• Advocacy: Influencing local and national policy leading to improvements in health and
wellbeing
What happens now?
What can my practice do?
What can the CCG do?
What can we do together with the council?
Health and Wellbeing Planning Grid
In Sefton
95
(1) Response and Reflections Dr Jane Weatherstone
(2) Your feedback, response and
reflections Facilitated session
What is the vision for Primary Care in
Sefton?
Dr Jane Weatherstone
Facilitated discussion
Feedback
Martin McDowell

Summary
Actions
Next Steps
Martin McDowell

Thank you
Date for your diary:
** Shaping Sefton 4: Unplanned Care **
2 November 2015
Contact:
martin.mcdowellsouthseftonccg.nhs.uk