Embed Size (px)
DESCRIPTION
Shaped for the Future Health article
Citation preview

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
savings
efficienciesdisposals
wasted
spacelatent capacity
potential
betteroutcomes
SHAPED FOR THE FUTURE - REFORMING THE NHS ESTATEEC Harris’ third annual service and estate efficiency review considers how to unlock the potential within the NHS estate and avoid inherent paradoxes in an era of localism to improve health outcomes.

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE | PRECIS
In 2008/09 there was more than 3 million m² of underused or wasted space in the NHS. In 2009/2010 this figure dropped to 2.1 million m².
The latest figures released for 2010/11 show that since our last annual review the ‘wasted’ space in the NHS has been reduced by circa 210,000 m², leaving 1.898 million m² (of which 1.23 million is in the acute) underused or unused.
This is a step forward and should be celebrated, however, major financial and efficiency opportunities remain - getting the NHS estate in shape for the future. To put the opportunity into context, the footprint of the ‘wasted’ space in the NHS is still approximately equivalent to Sainsbury’s entire UK store base or 264 premier league football pitches placed end-to-end.
We estimate conservatively, that through efficient asset management, the NHS could unlock a capital sum of £1 billion,by only disposing of 50% of this area. We also predict that through: better procurement (as exemplified by NAO reports); improved third and fourth quartile FM performance; and efficiences associated with land disposal, a further £1 billioncould be saved. Indeed, by simply decommissioning all FM services from 50% of the unused space, the NHS could save £228 million alone. There is also currently a 190 - 276% gap between first and third quartiles in aspects of FM performance; is there any other industry where an organisation which isthree times less competitive than the top 25% can still trade successfully?
The NHS’ rainy day has come. We recognise that clinical change remains the biggest challenge and cost opportunity to the reform agenda but radical and concerted action is also needed to unlock latent capacity from its estate and assets in order to keep improving healthcare outcomes with the limited funds available. Overall tariff reductions are here to stay, possibly for much of the next decade, so there remains little choice. The challenge now is that most of the ‘wasted’ space is owned by Foundation Trusts and is therefore not accessible to the Treasury to dispose of or leverage its value for investment via procurement options. Local collaboration will therefore be more important than ever. ‘Competing’ trusts in localities should also consider working together to maximise the opportunities available to them, generating economies of scale. This also applies to the sunk costs of developing such proposals and covering legal and financial costs.

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
The move to form regional “prop co’s” for the non trust related estate is a welcome step, and one we have recommended in previous reports to ensure efficient procurement as it provides economies of scale to both potential land and asset bidders, whilst maximising likely returns to Government departments. Nevertheless, achieving scale both in terms of commercial offering and financial value particularly in JV or LABV type transactions are the new prerequisites. Too often trusts come to the market to look at one or two services or a small part of the estate to dispose of, and wonder why the value offered is at the lower end of the scale. Maximising such opportunities in either market testing or selling large plots of land will nearly always give better value for money.
Those trusts that do dispose of land can maximise the value by looking carefully at future clinical usage and being more radical on performance outcomes than in previous years. Such action will benefit all stakeholders and provide tariff compliance and minimise overheads, providing much needed efficiency savings and/or re-aligning to clinical priorities for the NHS.
A better plan for better healthcare outcomes
To unlock the potential within the NHS estate and avoid the inherent paradoxes associated with localism and the efficiency drive, we suggest four areas are key to generate better health outcomes.
Our plan focuses on:
1 Efficient asset management to unlock capital receipts
2 Securing FM savings by reducing the performance variation of trusts
3 Encouraging greater collaboration between trusts and GP consortia
4 Improving clinical care and governance
We will now consider each of the points in detail.
1 EFFICIENT ASSET MANAGEMENT TO UNLOCK CAPITAL RECEIPTS
We believe that based simply on NHS asset values and without maximising the sites that are free, the NHS could conservativelyunlock a £1 billion capital receipt.
Understandably, there are concerns raised in response to this - most commonly that land is often ‘locked in.’ This is a valid challenge and is the reason why we would recommend a more achievable reduction target of 50%. In 2008/09 this meant a target of 1.5 million m²; if we deduct the 1 million m² that has already been saved since then, that leaves at least 500,000 m² still to go for. At this rate we are about two to three years away from reaching a prudent level.
We also hear from the NHS that land values are currently low, and this is mostly correct until one considers two assertions: ■ The NHS takes considerable process time to deliver such projects■ Schemes considered now will probably not be signed off legally with commercial partners until the third quarter 2013 or beyond.
By that time, the market should have improved considerably, although admittedly not up to 2007 values, which we are not likely to see again for some time. Likewise we have many of the top PLC organisations desperately short of large sites and whom have still been looking to expand their bases over the past two years, whilst the market has been at its worst. This makes commercial sense for the cash rich supermarkets, retailers and large scale land banks and technology organisations.
Alternative use
There are opportunities for joint ventures and as collateral alongside private sector partners for developing such space (where it is meaningful) for alternative use. Of course some estate is worthless, but we still find estates where whole tracts of land support isolated support buildings, with all the FM, energy, security and utilities costs associated. In most cases (not all) demolition is the answer.

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
2 SECURE FM SAVINGS BY REDUCING THE PERFORMANCE VARIATION
The NHS is the fifth largest organisation in the world but one that doesn’t maximise its scale. Too many organisations have narrow or piecemeal approaches.
In addition a 190 - 276% gap exists between first and third quartile performance - is there any other industry where an organisation can still trade which is nearly three times less competitive than the top 25%?
Savings of over £1 billion per annum in Estates/Procurement/FM only are evidently possible across the NHS. Based on simplyreducing only 50% surplus/underused space, the savings per organisation type are represented in table one below.
50% disposal of underused/surplus space
Acute PCT Mental Health
Total
Revenue £157.4 M £34.7 M £36.4 M £228.6 M
Capital (Based on 09/10 Asset Values)
£633.3 M £182.9 M £158.5 M £974.7 M
Total £1.2 Billion
One needs to standardise areas and create a culture where investment occurs on basis of evidence and usage so that every m² pays for itself, ideally over a ten year period.
At EC Harris we have been working up a model (the prototype of which is called ECost), which looks at the totality of each organisations estate assets, costs and specifically compares them to each individual workforce by type and ‘what if scenariomodelling’ including service specification and performance/pay changes.
This means where a trust wants to exceed or change the national standards for an FM service, for local reasons, it can see the direct costs and therefore quantify the cost-benefit. Likewise a trust can see its entire FM service and each staff member input against “should cost” based on recent actual tenders from our database. The client selects its individual inputs, beds, local ethnicity mix which impacts on food/meal requirements. The model also includes all pay weightings and geographic locality and the model then generates the quantum of “should” costs using regular market data.
The FM table below shows the differences currently between first and third quartile performance by organisation type. As indicated earlier it’s too volatile and the outcomes show a pressing case for reform. The cost differentials cannot be explained by simply mapping to older or more decayed accommodation. This is one factor, but management, leadership, vision and creativity remain major drivers for achieving lower costs and better service delivery.
Foundation Trusts can do more to use these land resources, by packing the core of hospitals using software tools to assess ‘gross to net’ clinical/non clinical areas and devising plans using such ratios to bring them in line with best practice. Inevitably this will offer some spare land to either develop for health, alternative uses or disposal.
Indeed local trusts working together may be able to leverage better value from a developer than on their own, likewise the NHS can learn much from the growth of Local Asset Backed Vehicle (LABV) options in other sectors such as housing and local government. Again one of the issues is to be more commercial with regards to what the trust wants to achieve for its land and working up proposals being sufficiently hard-edged to achieve its planning need.
This doesn’t necessarily sit comfortably with NHS organisationsworking closely with their town planners but commercial companies are interested in achieving a deal (even if it requires multiple planning applications) to achieve their singular aims. Their vision, singular objective and “know-how” on development is the reason why they tend to do commercially better than most NHS organisations on such deals.
Renewed pace
Finding opportunities is not brain-surgery. Indeed, on a recent project we identified in just a stroll around a site a host of opportunities, which could effectively help fund better infrastructure and contribute to improving or expanding front line services for patients as well as reducing fixed costs.
Practitioners using the Premises Assurance model should know exactly where the issues are they need to deal with; and these problems are also often known by Boards.
As is frequently the way, it is the implementation that is the really challenging part and renewed pace is therefore needed to overcome any obstacles.

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
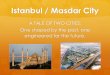
First and Third Quartile Performance 2010/11 per m²
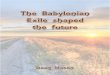
Likewise when one looks at the changes in average mean costs across the last three years there is little consistency. Energy costs did go down, due to passive measures and a campaign but with energy costs being more than £500 million per annum and global economic increases year on year predicted this is another of those areas where the NHS will have to work hard to stand still in cost terms. Some FM deals with the private
Acute Trusts Primary Care Trusts Mental Health
1st Quartile
3rd Quartile
1st Quartile
3rd Quartile
1st Quartile
3rd Quartile
Hard £80.15 £196.00 £58.84 £205.22 £73.47 £192.03
Soft £89.45 £137.51 £38.21 £79.14 £58.41 £100.23
Energy £17.70 £23.04 £12.26 £17.82 £11.64 £16.60
Capital £57.14 £134.46 £34.25 £137.65 £48.55 £124.95
Backlog £5.57 £20.58 £6.01 £27.79 £4.49 £15.00
Acute Trusts
Primary Care Trusts
Mental Health and Community Health Trusts
2008/09 2009/10 2010/11 2008/09 2009/10 2010/11 2008/09 2009/10 2010/11
Hard (£/m2) £117.20 £93.24 £136.14 £142.22 £133.16 £135.49 £111.58 £127.19 £140.70
Soft (£/m2) £107.71 £113.34 £114.07 £61.28 £63.45 £60.23 £69.00 £75.06 £76.40
Energy (£/m2) £26.18 £21.27 £20.27 £16.68 £16.68 £14.92 £16.14 £15.32 £14.25
Capital (£/m2) £86.80 £100.61 £90.56 £78.94 £88.83 £69.81 £72.01 £83.26 £84.22
Backlog(£/m2) £12.37 £14.04 £12.36 £15.60 £12.48 £14.79 £8.96 £9.42 £7.87
Whilst clinical savings dominate, the estate can greatly contribute. We believe the following areas offer the biggest opportunities to reduce operational expenditure:■ Reducing the number of high cost, low outcome acute facilities■ Amalgamate hospital groups to achieve economies of scale and drive efficiencies■ Change clinical sessions to more evenly match weekly us age of facilities - removing the peaks (where possible) ■ Multi use of space - similar procedures/use through same room and a debate about what ‘dedicated facilities’ actually consist of, including beds■ Extended hours of occupation of all high cost assets aiming for 40-50 hours usage routinely of OPD, theatres, GP rooms, treatment rooms, diagnostics etc ■ Rationalisation of community facilities across health and local authority provision
■ Standardisation of room types, this could reduce floor areas by 5% with IT booking - good design offers real opportunities to implement integrated ancillary accommodation efficiently and at a lower cost. ■ Government property companies look like being one of the vehicles taken forward for parts of the NHS estate and will help achieve scale benefits ■ Better procurement in IT/equipment and FM represents savings of hundreds of millions - this is a nationally accepted position ■ End the 190 - 276% difference between the first and third quartile with regards to aspects of estate performance■ The backlog position of more than £4.2 billion is likely to be over-estimated but demonstrates capital is still needed to pump prime service improvements and system integration.
The Biggest operational opportunities/issues
sector have proved very good value for money, to the point where in many retendering costs are increasing as the private sector push back, or the local NHS has increased its performance specifications. Where possible this should be avoided where good quality national standards have been agreed.
2008-11 Estate Costs per M²

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
3 ENCOURAGING GREATER COLLABORATION BETWEEN TRUSTS AND GP CONSORTIA
With policy changes on the horizon and the need for efficiency the overall amount of unused space is likely to grow again. The main driver for this is another reduction in the primary care estate, with bigger practices merging. The amalgamation of small district hospital functions and the urban fringe acute federated networks will also lead to driving utilisation advances which will compound the excess space dimension.
The aim must therefore be for localities, even so called ‘competing’ trusts to collaborate around the asset usage. The clusters for primary care represent one method, as do the vertical integration care programmes, enabling visibility of all assets. This means local groups of trusts can asses the needs of the locality, plan the combined services/asset uses, and rationally look at how they could be best provided from the assets available. The remaining assets can then be disposed of or committed for wider use. This approach supports the ethos from central government, but more importantly improves value for the taxpayer and ensures local communities are served in the most appropriate way.
Clearly the above is grossly simplified but it is achievable. The key will be activity analysis to drive top quartile performance, moving through areas such space utilisation, estate strategy, governance, performance and sustainability.
For trusts/PCTs which form part of the £4 billion plus backlog maintenance issue in an era of low NHS capital you have a handful of solutions to move forward:■ Use Prudential Borrowing Limits - amass year by year to box a scheme together. This is probably fine if you are a 900 bed tertiary hospital generating good surpluses but not great if you are a small district general hospital with around £2 million per annum■ Form JV or procurement vehicles to maximise opportunities - such as those that Clapham, Bexley and several other councils have undertaken via LABV, using the land/built assets as collateral■ Increase surpluses by radical profiling- delivering a higher net performance through increased hours or quicker turnover, reducing cost per episode and freeing asset usage ■ Use P21+ or LIFT (where available) to be the engine by linking complimentary skills and reduce revenue costs after the introduction of the project. This though has echoes of the early PFI programme which did not deliver the operating reduction returns predicted in business cases ■ Pray for change on capital policy and a return to the financial world of 2007. Whilst this may be well-intentioned it’s not likely to lead to a clear strategic direction that is implementable anytime this decade.
“The aim must therefore be for localities, even so called ‘competing’ trusts to collaborate around the asset usage.”

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
Our view is that efficiency moves in line with current first quartile clinical performance and will have to be sought by all trusts over the next 24 months and that should drive less cost in the estate footfall, combined with the good housekeeping measures outlined in our 10 point plan.
Go to: www.echarris.com/health
The opportunity for GP Consortia
Primary Care Trusts (PCTs) and GP Consortia are also going to have to play by the rules. The days of GPs getting practice grants and estates monies that were never fully spent on the asset have gone.
Managers are paid to protect the tax payer, so buildings that have no disability access, no mobility conveniences, poor fire safety and are poorly maintained, often little more than converted houses, need to consider the public interest and the law should be ruthlessly imposed. This will speed the process to get good quality stock in primary care better used. Good GPs should also recognise the significant benefit to their working environment and importantly to their patients of being in community multi-speciality facilities. We have the present corollary of an investment programme in primary care with LIFT providing some good quality but underused facilities, but some GPs still operate within a mile of each other out of facilities that breach health and safety. Moving this cohort inside the tent, either by persuasion or via a legislation clamp down (it’s existing but needs enforcing) would quickly mean utilisation was up and property costs down.
The benefits of collaboration are obvious for all involved. GPs who sign up for a multi fund agreement can maintain the separateness of their practices should they wish (at the cost of obvious economic and flexibility benefits), whilst patients sit in a decent waiting rooms and have access to a range of supporting community facilities and complimentary services such as a pharmacy, imaging etc. The medics gain a better place to work and have less to worry about regarding repairs and maintenance. The PCTs and GP consortia also gain the benefits of modern IT, standardisation and scale.
Ten years on from the investment drive in primary care, aside from rural practices, what is the benefit of very small GP practices in a modern 24/7 world? The patients have little complimentary health services, less access to GPs across an average year and are often referred more frequently into hospital for services they could gain elsewhere in the community. This is a structural system issue. Major Primary care hubs may feel utilitarian in some cases but the service that the patient receives is more comprehensive to their needs and modern living, in many cases with access to local authority and welfare services in the same location.
4 IMPROVING CLINICAL CARE AND GOVERNANCE
The issue of clinical care standards in the NHS continues to be debated both in the media and within the NHS. The already known public submissions from the Mid Staffs Enquiry (pre the Report) and the recent Patients Association study, does underline that both the DOH and CQC need to be ready to embark on significant and much more powerful accreditation tools or change the monitoring mechanisms completely.
The best trusts are being pulled down by organisations that aren’t fit for purpose. It’s fine for such bodies to be talking tough now, but they and their previous organisations have failed to create a system that properly regulates and safeguards the NHS’ reputation. The public failures are of course not their direct fault, since that rests with system failure including clinicians and management not focusing on achieving the desiredinternational good practice clinical and operating standards.
We have hundreds of good providers and a handful of really failing ones. The media attention is on the lowest outcome not the best. A suggestion maybe to either move to an external accreditation system, as much of the world does via JCI, QHA or the Canadian or Australian systems; or the commissioning board act much more ruthlessly with failing standards of care from provider units.
Hospitals should be inspected very regularly to ensure they meet the required standards of care and public value. This should maybe form part of the same story emerging from what recently has come under the title “disruptive innovation.” Circle‘s recent deal for Hinchingbrooke provides the opportunity for this scenario to be studied in the UK.

EC HARRIS | HEALTH | SHAPED FOR THE FUTURE
8196EC
Conclusion
Progress for the second year on the run is to be welcomed; let’s hope this is maintained and enhanced in next year’s figures. This is likely to be more challenging with more PCT estate likely to be freed up and the majority of remaining ‘wasted’ space under Foundation Trust control.
Trusts which up to now have buried their heads in the sand really do need to embrace the opportunities that are available;ideally collaborating with local healthcare organisations and their local government to maximise the opportunities. Piecemeal investment and building incremental wards and facilities is no longer appropriate. Taxpayers and service users alike deserve trusts at least progressing to reach current mean performance.
The regulatory aspects are going to make the headlines and rightly so, we need to see wholesale change not just tinkering around the edges. With a groundswell of public sentiment, demanding NHS improvement, likely to follow the headlines, coupled with the localism agenda, there has never been a better time for trusts to collaborate and push through radical plans that will improve healthcare outcomes.
Those trusts who want to achieve will do, those that want to wait for central guidance and someone to bail them out may find this time there is no magic saviour. The best the NHS achieves is great, the third and fourth quartile performers need to change what they are doing rapidly or rightly run the risk of their organisations disappearing over the next five years.
EC Harris has developed a ten step approach to helping trusts unlock the latent value from within their estates, which contains practical methods for dealing with many of the issues laid out in this paper, this include the robust FM benchmarking model (E Cost).
To discuss any of the elements in this paper in more detail, please get in contact.
Conor Ellis Partner, Global Account Leader m +44 (0) 7920 070 740 e [email protected]
Dr Rachel Dick Consultant m +44 (0) 7770 496 295 e [email protected]
www.echarris.com/health