Embed Size (px)
Citation preview

Shape of Change in Cognitive Behavioral Therapy for Youth Anxiety:Symptom Trajectory and Predictors of Change
Brian C. Chu, Laura C. Skriner, and Laurie J. ZandbergRutgers University
Objective: Multilevel growth analysis was used to establish the mean growth trajectory (shape ofchange) for cognitive behavioral therapy (CBT) for youth with anxiety disorders. Two-level growthanalysis was conducted to identify important between-youth predictors of session-by-session symp-tom change. Method: Fifty-five youth (ages 7–17; 50.9% male) and their parents participated in a 16- to20-week CBT that emphasized affective, cognitive, and exposure-based exercises. Multilevel growth models(MLMs) were estimated to model session symptom data taking into account an “anxiety spike” hypothesizedto occur at initiation of exposure sessions. Three models were compared: a cubic curve, a log-linear curveplus an exposure covariate, and a linear curve plus exposure covariate. Two-level MLM examined theeffect of demographic traits (sex, age, race/ethnicity), pretreatment symptom severity, comorbid schoolrefusal, early treatment factors (use of selective serotonin reuptake inhibitor medication, therapeuticalliance, treatment attrition), and pretreatment coping (engagement, disengagement, and involuntarycoping). Results: Fit indices provided support for the cubic growth model using either parent or youth anxietydata. Level 2 analysis identified youth age, symptom severity (anxiety, externalizing), early attrition, andengagement and disengagement coping as significant predictors of symptom trajectories. Predictors accountedfor 34%–37% of between-youth variance in midtreatment anxiety scores. Conclusions: Findings suggest thatthe symptom course of CBT, and the effect of between-youth factors on treatment outcomes, is more complexthan previously thought. Educating therapists and clients about findings can aid treatment expectations anddissemination efforts of empirically supported treatments.
Keywords: symptom trajectory, predictors of treatment outcome, multilevel modeling, child and adoles-cent anxiety, cognitive behavioral therapy
Treatment research has focused predominantly on questions ofefficacy and less on when and how change takes place. Cognitivebehavioral therapy (CBT) for youth anxiety has been designated“probably efficacious” based on randomized pre–post experimen-tal trials (Silverman, Pina, & Viswesvaran, 2008). However, indi-vidual growth modeling is increasingly recognized for its ability toclarify the timing and mechanisms of change (Hayes, Laurenceau,Feldman, Strauss, & Cardaciotto, 2007; Singer & Willett, 2003). Inthe current study, we examined mean symptom trajectories forCBT and between-youth factors that predicted individual variation.
Symptom Time Course: Nonlinear Trajectories
Many assume therapy improvement occurs incrementally and ata constant rate (a linear trend). That is, clients make relativelyconsistent, additive progress across sessions from pre- to posttreat-ment. However, evidence exists that symptoms improve at differ-ent rates across therapy. For example, adult research has identifiedevidence for early rapid response in CBT, whereby 50%–65% oftotal client improvement can be achieved by the fifth week oftreatment (Tang & DeRubeis, 1999). Research has also demon-strated the nonlinear phenomenon of sudden gains (i.e., large,stable improvement that occurs during a single, between-sessioninterval). Whereas early response has yet to be established inanxiety treatments, sudden gains have been found in the treatmentof panic disorder, social phobia, and generalized anxiety disorder(e.g., Clerkin, Teachman, & Smith-Janik, 2008; Hofmann, Schulz,Meuret, Moscovitch, & Suvak, 2006).
Curvilinear (e.g., cubic) and other nonlinear symptom coursesmay be particularly relevant to exposure therapies for anxiety. Byencouraging clients to confront distressing stimuli without escapeor avoidance, exposure therapy explicitly elicits short-term anxietyin the service of long-term habituation or emotional processing(Foa & Kozak, 1986). Such a theory might suggest a symptom“spike” during phases of treatment that emphasize exposures(Hayes, Laurenceau, et al., 2007). Anxiety spikes may not only beexpected but also desired, as this pattern would provide evidenceof sufficiently activated fear networks.
This article was published Online First June 24, 2013.Brian C. Chu, Department of Clinical Psychology, Rutgers University;
Laura C. Skriner, Department of Psychology, Rutgers University; Laurie J.Zandberg, Department of Clinical Psychology, Rutgers University.
We acknowledge Eun-Young Mun for her early manuscript review andconsultation on multilevel analysis and Tara Harrison for early databasedevelopment and management. We also thank the families who partici-pated and the many Youth Anxiety and Depression Clinic interviewers,therapists, and research assistants who made this work possible.
Correspondence concerning this article should be addressed to Brian C.Chu, Department of Clinical Psychology, Graduate School of Applied andProfessional Psychology, Rutgers University, 152 Frelinghuysen Road,Piscataway, NJ 08854. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Journal of Consulting and Clinical Psychology © 2013 American Psychological Association2013, Vol. 81, No. 4, 573–587 0022-006X/13/$12.00 DOI: 10.1037/a0033390
573

Preliminary research supports the possibility of a symptomspike. Nishith, Resick, and Griffin (2002) identified a curvilinearchange pattern across sessions reflecting an increase and subse-quent decrease in anxiety during prolonged exposure for posttrau-matic stress disorder. In exposure-based cognitive therapy fordepression, evidence was found for a “depression spike” among65% of the sample (Hayes, Feldman, Beevers, Cardaciotto, &Lewis-Smith, 2007). Depression spikes were predictive of positiveoutcome provided they occurred during the exposure phase and notskills phase of treatment. In both studies, symptom escalation wasreported during exposure sessions.
Symptom Trajectory in CBT for Youth Anxiety
Anxiety disorders are among the most prevalent psychiatricconditions affecting children and adolescents, and CBT has dem-onstrated positive, enduring effects (Kendall, Hudson, Gosch,Flannery-Schroeder, & Suveg, 2008; Silverman et al., 2008). Stud-ies of symptom patterns in CBT for youth anxiety are lacking.However, such research, particularly of change processes duringexposure sessions, can elucidate important change mechanisms(Hudson, 2005).
Randomized trials of youth anxiety CBT imply two models ofsymptom course. The first suggests linear, steady, and gradualchange. The Child-Adolescent Multimodal Study (Walkup et al.,2008) compared CBT, medication, and their combination. Usingdata from four time points (Weeks 0, 4, 8, 12), hierarchical linearmodeling indicated a linear trajectory for CBT compared withplacebo. A second model proposes greater symptom change duringexposure sessions. Kendall et al. (1997) compared 16-week CBTwith 8-week waitlist (WL) and reported nonsignificant differencesbetween CBT and WL at midtreatment but significant differencesat posttreatment. The authors concluded the majority of symptomchange occurred during the second half of therapy when exposureexercises began.
Conclusions about change trajectories are limited by a relianceon group means and relatively few repeated measures. Meta-analyses document that the large majority of child clinical trialsrely on assessments conducted at pre-, post-, and follow-up (Chu& Harrison, 2007). Estimating curvilinear trajectories requiresmore frequent assessments (a minimum of three assessments toestimate quadratic and four to estimate a cubic shape), with greaterprecision and power coming from increased assessments (Singer &Willet, 2003). Furthermore, there is often an incongruity betweenassessment tool and assessment period. For example, Walkup et al.(2008) used a clinician anxiety scale assessing symptoms in thepreceding week, but assessments were conducted every 4 weeks.This mismatch may obscure curvilinear trajectories even wherethey exist. Complex symptom patterns (including cubic trajecto-ries) have been found in small case studies and open trials usingweekly assessments (Kane & Kendall, 1989; Thienemann, Moore,& Tompkins, 2006). However, sample sizes are too small toformally test curvilinear trajectories.
The current study fit weekly symptom data, collected from 16-to 20-week CBT, to multiple growth trajectory models to deter-mine the typical change trajectory and to examine the anxietyspike theory (Hayes, Laurenceau, et al., 2007). Models testedincluded a cubic model, a log-linear model with an exposurecovariate representing an anxiety “spike,” and a linear model with
the exposure covariate. We hypothesized each model would fitsession data better than linear or quadratic models. We hypothe-sized that a cubic model would visually be represented by adecrease in anxiety in early sessions, followed by a midtreatmentincrease in anxiety, and then a final decrease by treatment end. Thelog-linear function models change as curvilinear, occurringquickly at first, then tapering off over time. A time-varying cova-riate was used to model the effect of exposure initiation. A sig-nificant, positive covariate coefficient would indicate an anxietyspike at the start of exposure sessions. The linear model replacedthe log-linear function with a linear parameter.
Our second aim was to identify between-youth client and treat-ment factors that predict individual trajectories. Identifying pre-dictors of outcomes can answer questions about which youth arelikely to benefit from treatment and provide information aboutprognosis (Southam-Gerow, Kendall, & Weersing, 2001). Predic-tor studies are common, but few have predicted symptom trajec-tories. Predictors fell into five domains: (a) youth demographics(sex, age, race/ethnicity), (b) pretreatment severity (anxiety, de-pression, externalizing symptoms), (c) important diagnostic co-morbidity and clinical problems (school refusal), (d) early treat-ment variables (adjunctive antianxiety medication, treatmentattrition, therapeutic alliance), and (e) pretreatment coping styles.Predictor–outcome relations are inconsistent and typically onlyevaluate effects on posttreatment outcomes. Poorer response inCBT has been associated with older age, pretreatment anxiety,depression (Berman, Weems, Silverman, & Kurtines, 2000;Southam-Gerow et al., 2001), and school refusal (Layne, Bern-stein, Egan, & Kushner, 2003). Studies have identified predictorsof early attrition from therapy (Kendall & Sugarman, 1997; Pina,Silverman, Fuentes, Kurtines, & Weems, 2003), but none haveexamined symptom trajectories associated with attrition. We esti-mate symptom trajectories for youth who drop out prior to Session10 and those who stay in treatment longer (i.e., begin exposuresessions). Selective serotonin reuptake inhibitors (SSRIs) treat-ment has been associated with positive outcomes when taken aloneor in combination with CBT (Walkup et al., 2008), but less isknown about SSRIs’ impact on symptom course when the youthinitiates CBT on a stable dose. Finally, research has shown con-sistent, small relations between therapeutic alliance and anxietyoutcomes (McLeod, 2011). We hypothesized that these predictorswould have similar effects on symptom trajectories, but theseanalyses were exploratory as equivalent research is largely absent.
Youth coping styles have been identified as important mediatorsin anxiety CBT (Chu & Harrison, 2007; Prins & Ollendick, 2003)and are associated with anxiety and depression in communitysamples (Connor-Smith, Compas, Wadsworth, Thomsen, Saltz-man, 2000). We included three stress response styles as predictors:engagement coping, disengagement coping, and involuntary re-sponding (Compas, Connor-Smith, Saltzman, Thomsen, & Wads-worth, 2001). Engagement coping is conscious effort directedtoward a stressor (e.g., problem solving, emotional regulation,cognitive restructuring). Disengagement coping is conscious effortto avoid stressors (e.g., denial, wishful thinking, behavioral avoid-ance). Involuntary responding reflects conditioned reactions thatare not under volitional control (e.g., rumination, intrusive think-ing, emotional arousal, cognitive interference, inaction). Disen-gagement coping and involuntary coping have been positivelycorrelated, and engagement coping negatively correlated, with
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
574 CHU, SKRINER, AND ZANDBERG

internalizing symptoms (Connor-Smith et al., 2000). Given thatCBT requires active participation by youth and willingness toprocess emotional challenges, we hypothesized that greater pre-treatment disengagement and involuntary coping would predictpoorer treatment response throughout therapy. Inversely, we ex-pected those with higher engagement coping to experience greatersymptom recovery than those with lesser engagement coping.
Method
Participants
Participants were 55 youth (ages 7–17; M � 12.63, SD � 2.67)and parents who received CBT at a university-based outpatientclinic. Eligible youth met Diagnostic and Statistical Manual ofMental Disorders, fourth edition, text revision (DSM–IV–TR;American Psychiatric Association, 2000) criteria for a principalanxiety disorder, including generalized anxiety disorder (n � 24),social phobia (n � 17), panic disorder (n � 7), separation anxietydisorder (n � 4), and specific phobia (n � 3). The majority(87.3%) were diagnosed with at least one additional disorder orclinical problem. Of these, 96.4% met criteria for another anxietydisorder, 32.7% a mood disorder (depression or dysthymia), 32.7%an externalizing disorder (attention-deficit/hyperactivity disorder,oppositional defiant disorder, conduct disorder), and 38.2% schoolrefusal. Exclusions were minimized to maximize external validityand were mental retardation, autism, psychotic disorder, and bi-polar disorder. Twenty-two (40%) were taking SSRI medication atintake and were eligible if parents reported 4 weeks of stabledosage with no plans to change. The sample was 50.9% male (n �28); 72.8% White, 9.1% Asian, 3.6% Latino, 1.8% African Amer-ican, and 12.7% multiracial. Family income was below $30,000for 7.3%, from $30,001 to $60,000 for 20.8%, from $60,001 to$80,000 for 23.7%, and above $80,001 for 43.7% (data unknownfor two families). For parent-reported measures, mothers wereprimary reporters for 45 cases, fathers for nine, and an older sisterfor one case.
Measures
Anxiety Disorders Interview Schedule for Children (ADIS-IV) Child/Parent Interviews. The ADIS-IV (Silverman & Al-bano, 2000) is a semistructured interview that assesses presenceand severity of DSM–IV–TR diagnoses. Diagnostic profiles includeparent, child, and consensus diagnosis. Impairment (Clinician’sSeverity Rating; CSR) is rated per disorder on a 0 (not at all) to 8(debilitating) scale, where 4 represents clinical threshold. Inter-viewers were considered reliable when they matched expert ratingsof diagnosis and CSRs (Cohen’s � � 0.80). Actual mean interraterreliability was � � 0.94 (range � 0.85–0.99). Thirty-one percentof study interviews were randomly selected and coded for studyadherence. Reliability remained strong (mean � � .91, range �.78–1.00).
State-Trait Anxiety Inventory for Children–Trait–Child/Parent Versions (STAIC, STAIC-P). The STAIC-T (Spiel-berger, 1973) is a 20-item child self-report scale that measuresenduring trait anxiety. The STAIC-T-P (Strauss, 1987) is a 26-itemparent report version. Both are rated on a 1 (hardly ever) to 3(often) scale (youth range � 20–60; parent range � 26–78).
Strong psychometric properties have been reported (Southam-Gerow & Chorpita, 2007). In the current sample, internal consis-tencies at pretreatment were strong for both scales (� � .89).
Revised Child Anxiety and Depression Scales–Child/ParentVersions (RCADS-C/P). The RCADS-C/P (Chorpita, Yim,Moffitt, Umemoto, & Francis, 2000) are 47-item youth and parentreport questionnaires of youth symptoms consistent with DSM–IVanxiety and mood disorders. Items are rated on a 0 (never) to 3(always) scale. RCADS has demonstrated good internal consis-tency and strong convergent and discriminant validity. The MajorDepression Disorder (MDD) subscale (range � 0–30) and totalanxiety score (range � 0–111) were used. In the current sample,internal consistencies for youth and parent scales were strong(mean � � .89; range � 0.82–0.96).
Child Behavior Checklist (CBCL). The CBCL (Achenbach& Rescorla, 2001) is a 118-item parent-reported checklist of youthbehaviors using a 0 (not true) to 2 (often true) scale. The Exter-nalizing broadband scale was used to measure conduct and impul-sivity problems. T scores were normalized for age and gender(M � 50, SD � 10), and scores over 63 indicate clinicallysignificant problems. Validity, internal consistency, and retestreliability of the CBCL have been well documented across clinicalpopulations (Achenbach & Rescorla, 2001).
Responses to Stress Questionnaire–Child/Parent Versions(RSQ-C/P). The RSQ (Connor-Smith et al., 2000) has 57 items,rated on a 1 (not at all true) to 4 (often true) scale, measuring youthcoping strategies. Factor analysis identified three higher orderscales: engagement coping (21 items; range � 21–84), disengage-ment coping (nine items; range � 9–36), and involuntary respond-ing (27 items; range � 27–108), with adequate to strong internalconsistency and retest reliability. Confirmatory factor analysisdemonstrated the superiority of this factor structure over othermodels (Connor-Smith et al., 2000). Some conceptual overlapexists between anxiety symptoms and involuntary respondingitems, but coping and distress show moderate, but not redundant,correlations (r � .36–.53; Compas et al., 2001). In the currentsample, ranges of parent, child (age 12 and under), and adolescentinternal consistencies for the three coping scales were � � .72–.90,� � .62–.96, and � � .85–.97, respectively.
Therapeutic Alliance Scale for Children/Adolescents(TASC/A). The TASC/A (Shirk & Saiz, 1992) are 12-itemscales measuring youth and therapist perceptions of the therapeuticrelationship. TASC uses a 1 (not at all) to 4 (very much) scale, andTASA uses a 1 (not true at all) to 6 (very true) scale. TASC/A hasdemonstrated excellent psychometrics and acceptable associationswith other relationship measures (McLeod, 2011). Internal con-sistencies here ranged from adequate to strong (mean � � .85;range � 0.71– 0.92). Total scores were transformed to standard-ized z scores to make child and adolescent scales comparable.
Procedure
All parent and youth participants provided informed consent/assent consistent with the university’s Internal Review Board. Atintake, the ADIS-IV and parent and youth report measures werecompleted. Eligible youth entered a 2-week baseline phase whereanxiety severity (STAIC-C/P) was assessed each week. Symptomseverity was then assessed prior to each treatment session. Youthand therapists completed the TASC/A at the fourth session.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
575SYMPTOM TRAJECTORY FOR YOUTH ANXIETY

All enrolled youth received 16- to 20-week manual-based CBT(Kendall & Hedtke, 2006). The first half focuses on affective andcognitive skills (emotions education, relaxation, cognitive restruc-turing, problem solving, rewards) and the second half on exposureexercises. The Coping Cat protocol has produced reliable changeat posttreatment and long-term follow-up (Kendall et al., 1997,2008) and is considered “probably efficacious” (Silverman et al.,2008). Therapists were 20 doctoral-level psychology graduatestudents (16 female). All therapists completed a semester-longdidactic seminar before treating any cases and then receivedweekly supervision that used videotape feedback. Videotapes of arandom sample (20%) of cases (n � 120 sessions) were coded byindependent raters (trained to reliability; � � .80) to assess treat-ment adherence. Ratings indicated all major Coping Cat skills(somatic education, relaxation, cognitive restructuring, problemsolving, reward, exposures) were represented in the expectedphase of treatment for 98.5% of cases.
Analytic Overview
Data screening was conducted to examine normality of out-comes within and across time. Estimates of skewness and kurtosiswere within expected limits. Pairwise correlations among all in-dependent variables did not identify concerning multicollinearity(all rs � .70). During model building, QQ and scatterplots ofpredicted model residuals were used to evaluate multivaritatenormality and homoscedascity; no case outliers were identified.There was no evidence of heteroscedascity.
Before fitting predicted models, observed group data wereplotted to identify mean trends and examine individual growthheterogeneity. To bolster confidence in hypothesized models,individual STAIC scores were plotted over time and catego-rized by independent raters. Multilevel growth curve models(Raudenbush & Bryk, 2002; Singer & Willet, 2003) were thenused to compare unconditional growth models. All models wereestimated with hierarchical linear modeling 6.08 (HLM;Raudenbush, Bryk, & Congdon, 2009) using full maximumlikelihood estimation procedures. Three multilevel growthmodels were estimated separately for parent and child STAICscores based on hypothesized and observed patterns of change:a cubic model, a log-linear model using a natural log transfor-mation (base e) of sessions (LnSessions) that included an ex-posure covariate, and a linear model plus exposure covariate.The “exposure” variable was a time-varying covariate, dummycoded (0 � no exposure, 1 � exposure) to represent the start ofeach youth’s exposure phase. Repeated observations of sessionSTAIC scores (Level 1) were nested within youth (Level 2).1
Data were limited to the first 18 sessions to minimize balanceissues in the data set, such that all participants had a possibletotal of 20 assessments (i.e., intake, baseline, Sessions 1–18).2
For the cubic model, session number (the time variable) wascentered at midtreatment (Session 9) to help address multicol-linearity at the within-person level (Raudenbush & Bryk, 2002)and to aid interpretation, such that growth parameters repre-sented overall average symptom change over treatment. Thelog-linear time variable was not centered. As examples, theparent cubic unconditional growth model was:
STAIC � Pti � �00 � �10�session � 10�ti � �20�session � 10�ti2
� �30�session � 10�ti3 � �r0i � r1i�session � 10�ti
� r2i�session � 10�ti2 � r3i�session � 10�ti
3 � eti�.
The log-linear model formula was:
STAIC � Pti � �00 � �10�LnSession�ti � �20�exposure�ti
� �r0i � r1i�LnSession�ti � r2i�exposure�ti � eti�.
Evaluation of model fit was accomplished using multiple sta-tistical criteria, including deviance difference (�Dev), the Akaikeinformation criterion (AIC), and the Bayesian information crite-rion (BIC), with added consideration for interpretability and modelparsimony.3 Deviance statistics provide a measure of comparablefit across nested models where smaller numbers indicate better fit.The AIC adjusts for the number of parameters in a model, and theBIC adjusts for both number of parameters and sample size (Singer& Willett, 2003).
After the cubic model was chosen to best fit the data (seeResults), two-level growth models were estimated to determinewhat factors accounted for significant between-youth variance ingrowth parameters (intercept, linear, quadratic, and cubic param-eters). Five categories of Level 2 predictors were examined: de-mographic traits (sex, age, race/ethnicity), pretreatment severity(RCADS MDD, RCADS Anxiety, CBCL-Externalizing), comor-bid school refusal, early treatment variables (adjunctive SSRI,therapist and youth-rated Session 4 alliance, treatment attritionprior to Session 10), and pretreatment coping (engagement, disen-gagement, and involuntary subscales of the RSQ). All Level 2variables that did not have a meaningful zero value were grandmean centered (i.e., age, RCADS, RSQ). A full model was firstestimated with all 14 Level 2 predictors. Level 2 variables wereretained in a final model if they were predictors of a Level 1 effectin the full model at p � .10 and then interpreted as significant ifthey reached p � .05 in the final model.4 Full and final models
1 Three-level models (time nested within youth and therapist) wereexamined, but therapists (Level 3) contributed nonsignificant variance,likely because mode number of cases per therapist was 2, limiting distinc-tion between case and therapist. Thus, two-level models were used.
2 Multilevel change models can accommodate varying numbers of datacollection waves, but potential problems can result from severely unbal-anced data sets (Singer & Willet, 2003). Models using balanced data setscan be parameterized more easily and random effects estimated moreprecisely. We limited data to the first 18 sessions to remove outliers andminimize balance issues. Very little data were cut to create this balance:82% of youth received 18 sessions or fewer, and the first 18 sessionsaccounted for 97% of total Level 1 symptom data.
3 �Dev was compared with critical values of a �2 distribution with df setto the difference in number of parameters between the two models. �AICand �BIC greater than 10 suggests “strong evidence” for significantdifferences between models (smaller values represent better fit), eventhough definitive guidelines for AIC and BIC in MLM are still developing(Raftery, 1995).
4 Although stepwise selection of covariates is common in regressionanalysis, recent criticism has suggested these approaches bias parameterestimates high and bias p values low (Harrell, 2001). Lasso, regularizedregression, and cross-validation methods are encouraged in all multipleregression analyses (not just multilevel). We use stepwise selection to stayconsistent with contemporary clinical science, but p values should beviewed cautiously.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
576 CHU, SKRINER, AND ZANDBERG
were compared by fit indices. Cubic models are inherently difficultto interpret, particularly when examining interactions betweengrowth parameters and Level 2 predictors. In a cubic model, thelinear parameter refers to the initial direction and rate of change.The quadratic parameter references acceleration/deceleration inthe linear rate of change, and the cubic parameter references rateof change in the acceleration (Shek & Ma, 2011). For concreteinterpretation, we relied on graphical examination of trajectories.
Missing data. The multilevel growth model allows for vary-ing numbers of waves of data collection and individualized col-lection schedules (Singer & Willet, 2003). HLM uses all availableLevel 1 data to estimate individual growth trajectories. However,HLM requires complete Level 2 (youth-level) data (Raudenbush &Bryk, 2002). All participants had complete Level 2 predictor dataexcept for six cases, who dropped out before TASC/A was col-lected at Session 4 (an additional six youth dropped out prior toSession 10 but had TASC/A data). For therapist-rated TASC/A,we carried forward the closest preceding alliance score. For youthTASC/A, missing data were replaced with the sample mean.5
Missing Level 1 data were considered in two ways. Due toplanned flexibility in the CBT protocol, there was variability inattended sessions. Youth attended a total of 741 sessions (M �13.5 sessions per youth, SD � 5.4, range � 1–18). Over 78%(n � 43) reached Session 9, 60% (n � 33) reached Session 16, and25% (n � 14) reached Session 18. Including intake and baseline,807 and 821 Level 1 data points were available for parent andyouth models, respectively. HLM handles this type of imbalancedLevel 1 data as long as data are missing at random (MAR; Singer& Willet, 2003). Data fit MAR criteria if probability of missing-ness is dependent on other observed data, including predictors oroutcomes, but not on unobserved variables. In the current study,the probability of missingness could be attributed to the permittedflexibility in treatment duration or to our observed “attrition”variable, which is included as a predictor in our two-level model.However, we cannot guarantee that unobserved variables did notaffect missingness. As an added level of evaluation, pattern mix-ture modeling procedures (Hedeker & Gibbons, 1997) were usedto examine the influence of missing data. Participants were dividedinto groups depending on their missing-data patterns (attritionbefore Session 10 or before Session 16). Dummy-coded variablesbased on those groups were used as Level 2 model covariates; inboth parent and youth models, these missing data covariates werefound nonsignificant, indicating missing data patterns did notinfluence fit of model.
Results
Descriptive Data
Pretreatment diagnostic and symptom data are presented inTable 1. Typical of outpatient settings, youth met criteria formultiple diagnoses (M � 3.60, SD � 1.72) of moderate severity(CSR M � 5.12, SD � 0.69). Parent measures showed moderate tosevere anxiety, mild depression, and subclinical externalizingsymptoms. Youth measures showed moderate anxiety and milddepression. Paired sample t tests demonstrated significant pre- toposttreatment change in parent STAIC, t(39) � 7.39, p � .001, andyouth STAIC, t(41) � 8.77, p � .001.
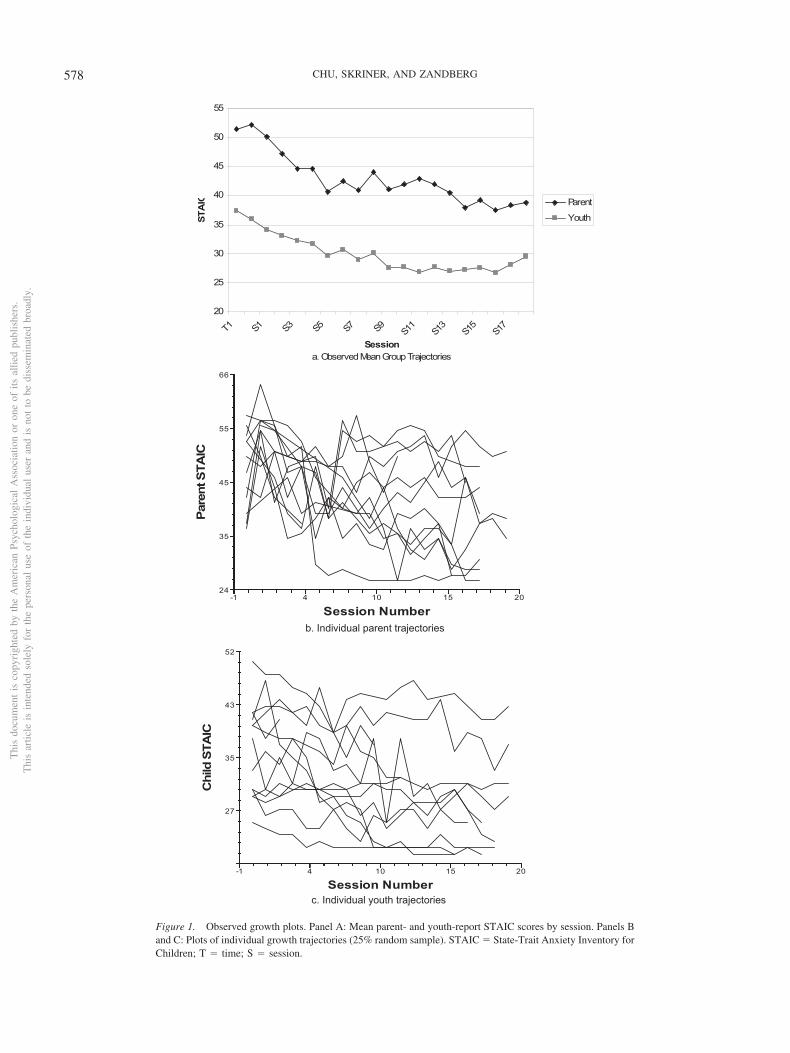
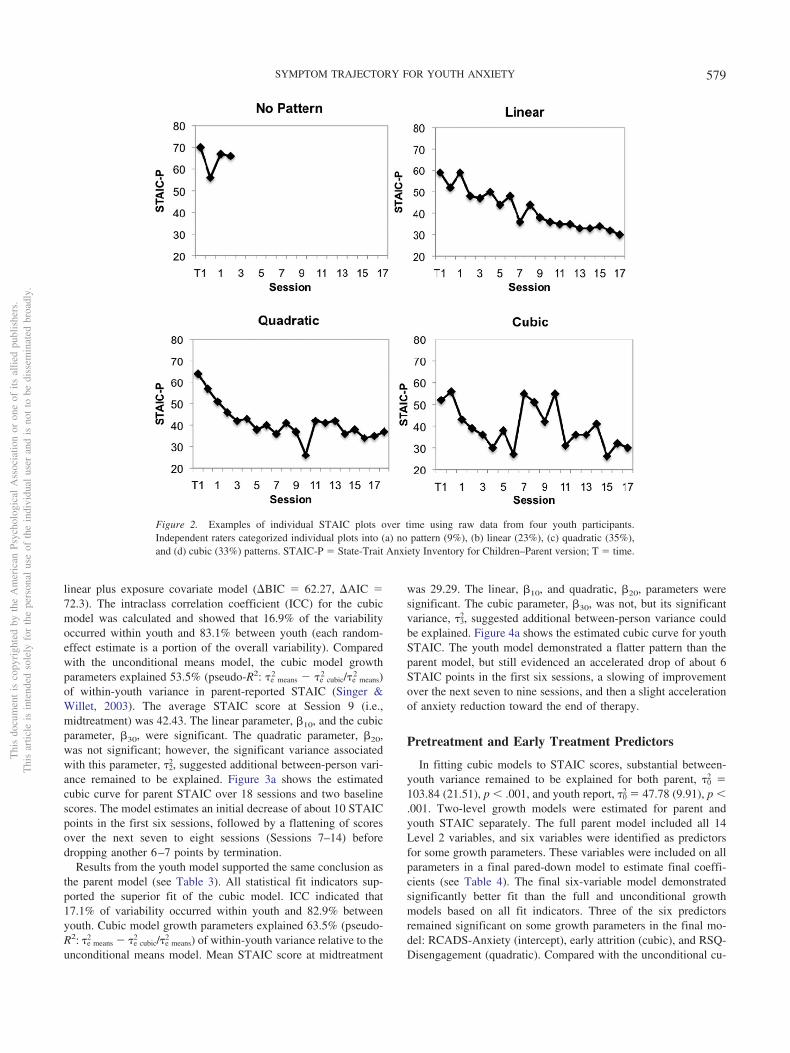
Plots of observed group data demonstrated overall decliningtrends, with parent STAIC showing a logarithmic or cubic shapeand youth STAIC showing a logarithmic or quadratic shape (seeFigure 1a). Individual line plots showed substantial variability inparent and youth report of growth (see Figure 1b and 1c). Inde-pendent ratings of individual growth plots identified 9% with nopattern, and 23% linear, 35% quadratic/logarithmic, and 33%cubic patterns (see Figure 2).
Mean Growth Trajectory
To identify mean shape of change for parent-reported anxiety, aseries of growth models were fit to the data, including an uncon-ditional means model with no time element; unconditional linear,quadratic, and cubic models; and linear and log-linear models withexposure entered as a time-varying covariate (see Table 2). Thecubic model fit the data significantly better than all other modelsbased on all statistical fit indicators and was selected as the bestfitting model. The log-linear model was considered because itoffered greater parsimony (fewer parameters) and eased interpre-tation (i.e., the exposure covariate provided a direct test of anxietyspike); however, both BIC and AIC for the cubic model weresubstantially lower than for the log-linear model (�BIC � 29.02,�AIC � 39.06), and the exposure parameter was nonsignificant.The cubic model was also superior to the linear (�BIC � 73.8,�AIC � 91.87), quadratic (�BIC � 17.18, �AIC � 27.22), and
5 Therapists rated alliance each session, permitting a carry-forward pro-cedure. Youth-rated TASC/A was collected only at Session 4. If youthattrited before Session 4, there would be no prior data to carry forward.Group mean substitution is acceptable for missing data up to 40% of totaldata (Gibson & Olejnik, 2003). Here, missing youth data was 11% (n � 6).
Table 1Pretreatment Symptom Severity and Early Treatment Predictors(N � 55)
Variable M SD Min Max
ADIS CSR for primary Dx 5.89 0.88 4.00 8.00Average CSR across all Dx 5.12 0.69 4.00 8.00Total number of Dx 3.60 1.72 1.00 8.00STAIC-Parent 51.38 9.85 29.00 73.00RCADS Total Anxiety-Parent 34.31 17.49 6.00 88.00RCADS MDD-Parent 8.15 5.26 0.00 21.00CBCL Externalizing T-score 53.60 10.30 34.00 74.00RSQ Engagement-Parent 37.16 9.34 20.00 61.00RSQ Disengagement-Parent 18.38 5.03 11.00 32.00RSQ Involuntary-Parent 57.44 15.04 33.00 95.00STAIC-Youth 37.31 8.41 22.00 60.00RCADS Total Anxiety-Youth 32.87 20.95 2.00 107.00RCADS MDD-Youth 9.18 5.68 0.00 27.00RSQ Engagement Coping-Youth 49.71 11.90 24.00 74.00RSQ Disengagement Coping-Youth 20.27 5.67 8.00 36.00RSQ Involuntary Coping-Youth 58.82 20.74 26.00 108.00Session 4 Therapist TASC/A (z score) 0.00 0.99 �2.25 1.49Session 4 Child TASC/A (z score) 0.00 0.99 �3.19 1.64
Note. ADIS CSR � Anxiety Disorders Interview Schedule-ClinicianSeverity Rating; Dx � diagnosis; STAIC � State-Trait Anxiety Inventoryfor Children; RCADS � Revised Child Anxiety and Depression Scale;MDD � Depression subscale; CBCL � Child Behavior Checklist; RSQ �Responses to Stress Questionnaire; TASC/A � Therapeutic Alliance Scalefor Children/Adolescents.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
577SYMPTOM TRAJECTORY FOR YOUTH ANXIETY
20
25
30
35
40
45
50
55
T1 S1 S3 S5 S7 S9 S11
S13
S15
S17
Sessiona. Observed Mean Group Trajectories
STA
IC Parent
Youth
24
35
45
55
66
Pare
nt S
TAIC
-1 4 10 15 20
Session Number
-1 4 10 15 20
27
35
43
52
Session Number
Chi
ld S
TAIC
b. Individual parent trajectories
c. Individual youth trajectories
Figure 1. Observed growth plots. Panel A: Mean parent- and youth-report STAIC scores by session. Panels Band C: Plots of individual growth trajectories (25% random sample). STAIC � State-Trait Anxiety Inventory forChildren; T � time; S � session.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
578 CHU, SKRINER, AND ZANDBERG
linear plus exposure covariate model (�BIC � 62.27, �AIC �72.3). The intraclass correlation coefficient (ICC) for the cubicmodel was calculated and showed that 16.9% of the variabilityoccurred within youth and 83.1% between youth (each random-effect estimate is a portion of the overall variability). Comparedwith the unconditional means model, the cubic model growthparameters explained 53.5% (pseudo-R2: e means
2 � e cubic2 /e means
2 )of within-youth variance in parent-reported STAIC (Singer &Willet, 2003). The average STAIC score at Session 9 (i.e.,midtreatment) was 42.43. The linear parameter, 10, and the cubicparameter, 30, were significant. The quadratic parameter, 20,was not significant; however, the significant variance associatedwith this parameter, 2
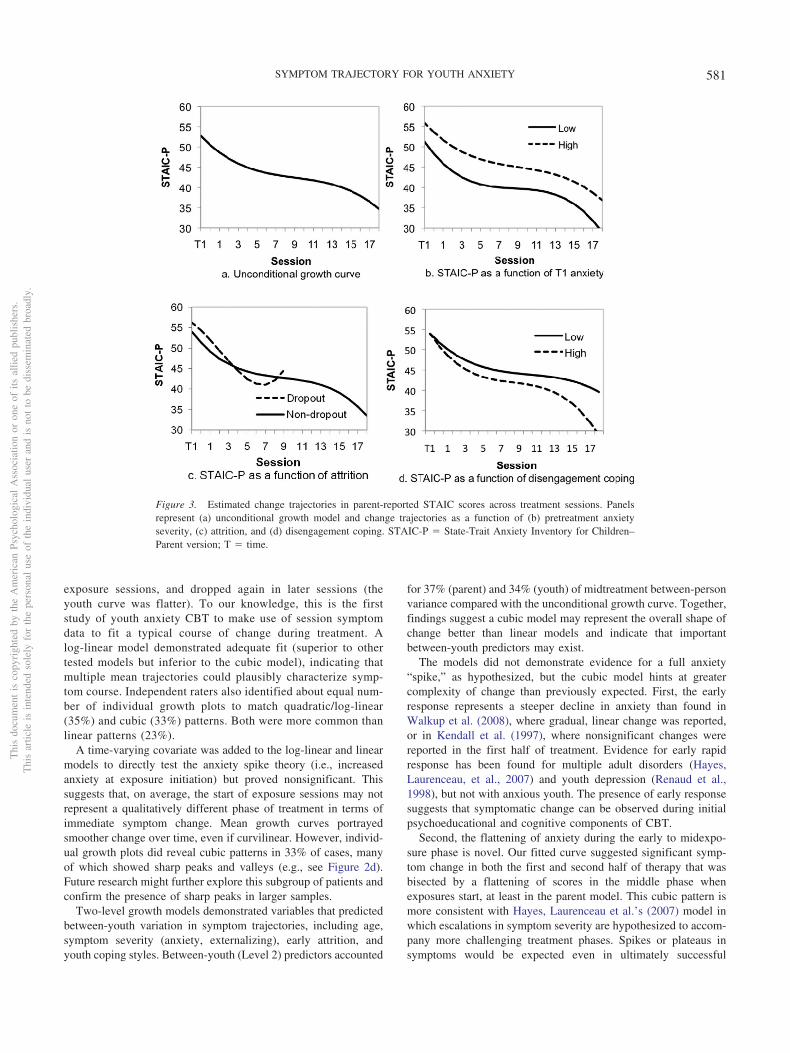
2, suggested additional between-person vari-ance remained to be explained. Figure 3a shows the estimatedcubic curve for parent STAIC over 18 sessions and two baselinescores. The model estimates an initial decrease of about 10 STAICpoints in the first six sessions, followed by a flattening of scoresover the next seven to eight sessions (Sessions 7–14) beforedropping another 6–7 points by termination.
Results from the youth model supported the same conclusion asthe parent model (see Table 3). All statistical fit indicators sup-ported the superior fit of the cubic model. ICC indicated that17.1% of variability occurred within youth and 82.9% betweenyouth. Cubic model growth parameters explained 63.5% (pseudo-R2: e means
2 � e cubic2 /e means
2 ) of within-youth variance relative to theunconditional means model. Mean STAIC score at midtreatment
was 29.29. The linear, 10, and quadratic, 20, parameters weresignificant. The cubic parameter, 30, was not, but its significantvariance, 3
2, suggested additional between-person variance couldbe explained. Figure 4a shows the estimated cubic curve for youthSTAIC. The youth model demonstrated a flatter pattern than theparent model, but still evidenced an accelerated drop of about 6STAIC points in the first six sessions, a slowing of improvementover the next seven to nine sessions, and then a slight accelerationof anxiety reduction toward the end of therapy.
Pretreatment and Early Treatment Predictors
In fitting cubic models to STAIC scores, substantial between-youth variance remained to be explained for both parent, 0
2 �103.84 (21.51), p � .001, and youth report, 0
2 � 47.78 (9.91), p �.001. Two-level growth models were estimated for parent andyouth STAIC separately. The full parent model included all 14Level 2 variables, and six variables were identified as predictorsfor some growth parameters. These variables were included on allparameters in a final pared-down model to estimate final coeffi-cients (see Table 4). The final six-variable model demonstratedsignificantly better fit than the full and unconditional growthmodels based on all fit indicators. Three of the six predictorsremained significant on some growth parameters in the final mo-del: RCADS-Anxiety (intercept), early attrition (cubic), and RSQ-Disengagement (quadratic). Compared with the unconditional cu-
Figure 2. Examples of individual STAIC plots over time using raw data from four youth participants.Independent raters categorized individual plots into (a) no pattern (9%), (b) linear (23%), (c) quadratic (35%),and (d) cubic (33%) patterns. STAIC-P � State-Trait Anxiety Inventory for Children–Parent version; T � time.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
579SYMPTOM TRAJECTORY FOR YOUTH ANXIETY

bic model, pseudo-R2 statistics (0 cubic2 � 0 final
2 /0 cubic2 ) suggested
36.7% of midtreatment between-person variance was accountedfor by the six Level 2 predictors (Singer & Willett, 2003). In total,the final model ICC indicated that 24.3% of the variability oc-curred within youth and 75.7% between youth.
Figure 3 illustrates the effect of each Level 2 predictor on parentreport growth after adjusting for other variables in the model.Figure 3b depicts the difference in estimated growth for youth withRCADS-Anxiety scores in either the 25th or 75th percentile.Pretreatment anxiety predicted absolute differences in STAICthroughout therapy but had little impact on trajectory shape. Youthwith higher disengagement coping demonstrated similar earlysymptom course to youth with lower disengagement coping, butthen showed sharp improvement in STAIC in the last five to sevensessions (see Figure 3d). Youth who dropped out of therapy priorto Session 10 (see Figure 3c) followed a course similar to treat-ment completers during the first few sessions, experienced a steepdecline in symptoms compared with completers from about Ses-sions 4–7, and were then predicted to show a sharp increase insymptoms just before dropout.
The full youth model included all 14 Level 2 variables, andseven were identified as predictors for some growth parameters.These variables were included on all parameters in a final model(see Table 5), which demonstrated significantly better fit than thefull and unconditional growth models based on all fit indicators.Four of the seven predictors remained significant for some growthparameters in the final model: age (intercept, linear, cubic), CBCL-Externalizing (linear, cubic), RSQ-Engagement (linear, cubic), andRCADS-Anxiety (quadratic). Compared with the unconditionalcubic model, pseudo-R2 statistics suggested 34.3% of midtreat-
ment between-person variance was accounted for by the seven L2predictors. The final model ICC indicated that 24.1% of thevariability occurred within youth and 75.9% between youth.
Figure 4 illustrates Level 2 predictor effects on youth growthafter controlling for other variables. Younger youth (25th percen-tile) showed lower anxiety and a steeper initial decline comparedwith older youth (75th percentile; see Figure 4b). Anxiety scoreswere nearly identical in the last five sessions. Lower pretreatmentRCADS-Anxiety contributed to slightly lower STAIC scoresthroughout therapy compared with higher RCADS-Anxiety scores(see Figure 4c). Lower pretreatment CBCL-Externalizing wasassociated with lower anxiety throughout treatment, and withsteeper initial and final declines in anxiety compared with higherCBCL-Externalizing scores (see Figure 4d). Finally, youth withgreater engagement coping showed a trajectory similar to youthwith lower engagement coping; however, greater engagement cop-ing was associated with less STAIC improvement over the first 10sessions (see Figure 4e).
Discussion
CBT demonstrates successful outcomes in treating youth anxi-ety, but little is known about the course of change or what predictsvariation in trajectories. In this small sample, a cubic model fitparent and youth weekly symptom reports better than othertested models. In total, 54% of within-person variation in parentSTAIC (64% of youth scores) was accounted for by growthparameters in the cubic model. Both parent and youth modelsfollowed a similar pattern where anxiety declined relativelyrapidly over the first half of treatment, flattened during early
Table 2Fixed Effects and Variance Components for Parent Unconditional Growth Models: STAIC by Session
Model A: Meansmodel
Model B: Linear �Exposure model
Model C: Log-linear �Exposure model
Model D: Cubicmodel
Variable Parameter r Estimate (SE) Estimate (SE) Estimate (SE) Estimate (SE)
Fixed effects
Intercept 00 44.70 (1.2)��� 50.41 (1.1)��� 53.20 (1.2)��� 42.43 (1.4)���
Session# (or LnS#) 10 �0.89 (.1)��� �4.56 (.58)��� �0.31 (.13)�
(Session)2 (or exp. covar) 20 2.52 (.9)�� �0.07 (.79) 0.002 (.02)(Session)3 30 �.007 (.002)���
Variance components
Level 1Within-person e
2 45.42 (2.3)��� 25.29 (1.4)��� 24.09 (1.3)��� 21.14 (1.2)���
Level 2Intercept 0
2 72.76 (14.6)��� 59.43 (12.8)��� 58.81 (13.9)��� 103.84 (21.5)���
Linear (or log-linear) 12 .45 (.1)��� 12.58 (3.5)��� 0.48 (.2)���
Quadratic (or exposure) 22 22.9 (9.5)��� 15.08 (5.9)��� 0.01 (.003)���
Cubic 32 0.0005 (.00003)��
Goodness-of-fit statistics
# Parameters 3 10 10 15Deviance 5538.6 5196.5 5163.3 5114.2AIC 5544.6 5216.5 5183.3 5144.2BIC 5550.6 5236.6 5203.4 5174.3
Note. Intercept is set at Time 1 for Models A, B, and C, and at midtreatment for Model D. STAIC � State-Trait Anxiety Inventory for Children; LnS# � naturallog of sessions; (Session)2 � estimate for quadratic parameter; (Session)3 � estimate for cubic parameter; exp. covar � exposure as a time-varyingcovariate; AIC � Akaike’s information criterion; BIC � Bayesian information criterion.� p � .05. �� p � .01. ��� p � .001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
580 CHU, SKRINER, AND ZANDBERG
exposure sessions, and dropped again in later sessions (theyouth curve was flatter). To our knowledge, this is the firststudy of youth anxiety CBT to make use of session symptomdata to fit a typical course of change during treatment. Alog-linear model demonstrated adequate fit (superior to othertested models but inferior to the cubic model), indicating thatmultiple mean trajectories could plausibly characterize symp-tom course. Independent raters also identified about equal num-ber of individual growth plots to match quadratic/log-linear(35%) and cubic (33%) patterns. Both were more common thanlinear patterns (23%).
A time-varying covariate was added to the log-linear and linearmodels to directly test the anxiety spike theory (i.e., increasedanxiety at exposure initiation) but proved nonsignificant. Thissuggests that, on average, the start of exposure sessions may notrepresent a qualitatively different phase of treatment in terms ofimmediate symptom change. Mean growth curves portrayedsmoother change over time, even if curvilinear. However, individ-ual growth plots did reveal cubic patterns in 33% of cases, manyof which showed sharp peaks and valleys (e.g., see Figure 2d).Future research might further explore this subgroup of patients andconfirm the presence of sharp peaks in larger samples.
Two-level growth models demonstrated variables that predictedbetween-youth variation in symptom trajectories, including age,symptom severity (anxiety, externalizing), early attrition, andyouth coping styles. Between-youth (Level 2) predictors accounted
for 37% (parent) and 34% (youth) of midtreatment between-personvariance compared with the unconditional growth curve. Together,findings suggest a cubic model may represent the overall shape ofchange better than linear models and indicate that importantbetween-youth predictors may exist.
The models did not demonstrate evidence for a full anxiety“spike,” as hypothesized, but the cubic model hints at greatercomplexity of change than previously expected. First, the earlyresponse represents a steeper decline in anxiety than found inWalkup et al. (2008), where gradual, linear change was reported,or in Kendall et al. (1997), where nonsignificant changes werereported in the first half of treatment. Evidence for early rapidresponse has been found for multiple adult disorders (Hayes,Laurenceau, et al., 2007) and youth depression (Renaud et al.,1998), but not with anxious youth. The presence of early responsesuggests that symptomatic change can be observed during initialpsychoeducational and cognitive components of CBT.
Second, the flattening of anxiety during the early to midexpo-sure phase is novel. Our fitted curve suggested significant symp-tom change in both the first and second half of therapy that wasbisected by a flattening of scores in the middle phase whenexposures start, at least in the parent model. This cubic pattern ismore consistent with Hayes, Laurenceau et al.’s (2007) model inwhich escalations in symptom severity are hypothesized to accom-pany more challenging treatment phases. Spikes or plateaus insymptoms would be expected even in ultimately successful
Figure 3. Estimated change trajectories in parent-reported STAIC scores across treatment sessions. Panelsrepresent (a) unconditional growth model and change trajectories as a function of (b) pretreatment anxietyseverity, (c) attrition, and (d) disengagement coping. STAIC-P � State-Trait Anxiety Inventory for Children–Parent version; T � time.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
581SYMPTOM TRAJECTORY FOR YOUTH ANXIETY
courses of treatment. Should this pattern persist, future researchcould explore change processes that distinguish first and secondhalves of treatment. For example, some have suggested this type ofpattern is consistent with models of first-order and second-orderchange (Greenberg, 2002), where the former is associated withsymptom reduction, improved coping, support, and stress reduc-tion, and the latter involves more enduring cognitive-affective-behavioral-somatic mechanisms.
Methodologically, our results argue for more frequent assess-ments, as earlier studies did not have sufficient assessment pointsto identify the complex curves found here (e.g., Kendall et al.,1997; Walkup et al., 2008). We recognize that the cubic modelmoves away from a direct test of an anxiety spike. It models ageneral down-up-down curve, but does not directly tie the anxietypeak to the onset of exposures. Future research might work toidentify the exact “turning points” (peak and trough) of anxietytrajectory, or identify distinct phases of therapy, to spotlight crit-ical sessions, treatment strategies, and processes of change.
Establishing expected trajectories of change is important. Somehave used such evidence to develop track-and-alert systems thatidentify cases at risk for treatment failure or premature dropout(e.g., Lambert, Hansen, & Finch, 2001). Individual therapists canuse this knowledge to set realistic expectations and to assessprogress more accurately. For example, expecting an anxiety “pla-teau” can help prepare therapists for challenges during early ex-posure sessions and may be used to promote continued adherenceto exposures in CBT despite some return of client anxiety. Like-wise, it is important to encourage families and clients to stay intreatment even after initial improvement and to stick with CBT asexercises get more challenging.
This knowledge, in turn, can enhance therapist training andtreatment dissemination. Surveys of clinicians indicate the minor-ity of psychologists use exposure techniques, and their reasonsinclude fear of patient decompensation, dropout, and allianceruptures (Becker, Zayfert, & Anderson, 2004). Such fears wereidentified even for respondents trained in exposure techniques.Thus, clinicians may misinterpret temporary flattening (or spikes)in anxiety as a disruption in clinical progress. The current studysuggests that a flattening of scores during early exposures repre-sents a temporary transition between two phases of symptomdecline. This is consistent with evidence that onset of exposureexercises are not linked with negative therapeutic alliance (Kendallet al., 2009). Together with previous research (Hayes, Feldman, etal., 2007; Nishith et al., 2002), it appears that curvilinear changepatterns are not only benign but also typical of successful treat-ment courses.
It should be noted that the observed mean curve for youth-reported anxiety appeared flatter than parent report even as thecubic model fit for both. Differing reports can offer methodolog-ical and substantive insights. Methodologically, youth STAICscores started and remained lower than parents’ throughout, cre-ating a “floor effect” where scores did not have much room to“move” (or vary) in the second half of therapy. Reduced variabilitymay have contributed to challenges in visually detecting complexcurves. Substantively, this effect may reflect a tendency for anx-ious youth to disclose fewer symptoms than parents, particularly inclinical settings where parents primarily seek treatment. The flattertrajectory may reflect reporter differences and its subsequent im-pact on variance/model fitting.
Table 3Fixed Effects and Variance Components for Youth Unconditional Growth Models: STAIC by Session
Model A:Means model
Model B: Linear �Exposure model
Model C: Log-linear �Exposure model
Model D: Cubicmodel
Variable Parameter Estimate (SE) Estimate (SE) Estimate (SE) Estimate (SE)
Fixed effects
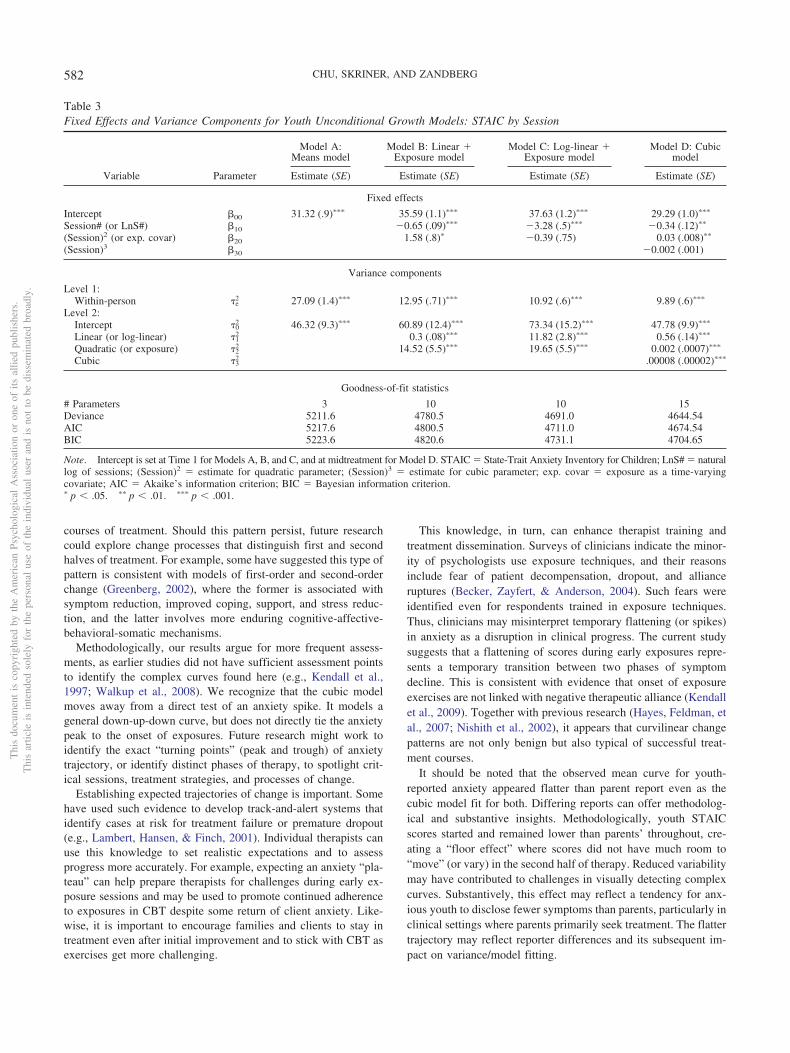
Intercept 00 31.32 (.9)��� 35.59 (1.1)��� 37.63 (1.2)��� 29.29 (1.0)���
Session# (or LnS#) 10 �0.65 (.09)��� �3.28 (.5)��� �0.34 (.12)��
(Session)2 (or exp. covar) 20 1.58 (.8)� �0.39 (.75) 0.03 (.008)��
(Session)3 30 �0.002 (.001)
Variance components
Level 1:Within-person e
2 27.09 (1.4)��� 12.95 (.71)��� 10.92 (.6)��� 9.89 (.6)���
Level 2:Intercept 0
2 46.32 (9.3)��� 60.89 (12.4)��� 73.34 (15.2)��� 47.78 (9.9)���
Linear (or log-linear) 12 0.3 (.08)��� 11.82 (2.8)��� 0.56 (.14)���
Quadratic (or exposure) 22 14.52 (5.5)��� 19.65 (5.5)��� 0.002 (.0007)���
Cubic 32 .00008 (.00002)���
Goodness-of-fit statistics
# Parameters 3 10 10 15Deviance 5211.6 4780.5 4691.0 4644.54AIC 5217.6 4800.5 4711.0 4674.54BIC 5223.6 4820.6 4731.1 4704.65
Note. Intercept is set at Time 1 for Models A, B, and C, and at midtreatment for Model D. STAIC � State-Trait Anxiety Inventory for Children; LnS# � naturallog of sessions; (Session)2 � estimate for quadratic parameter; (Session)3 � estimate for cubic parameter; exp. covar � exposure as a time-varyingcovariate; AIC � Akaike’s information criterion; BIC � Bayesian information criterion.� p � .05. �� p � .01. ��� p � .001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
582 CHU, SKRINER, AND ZANDBERG
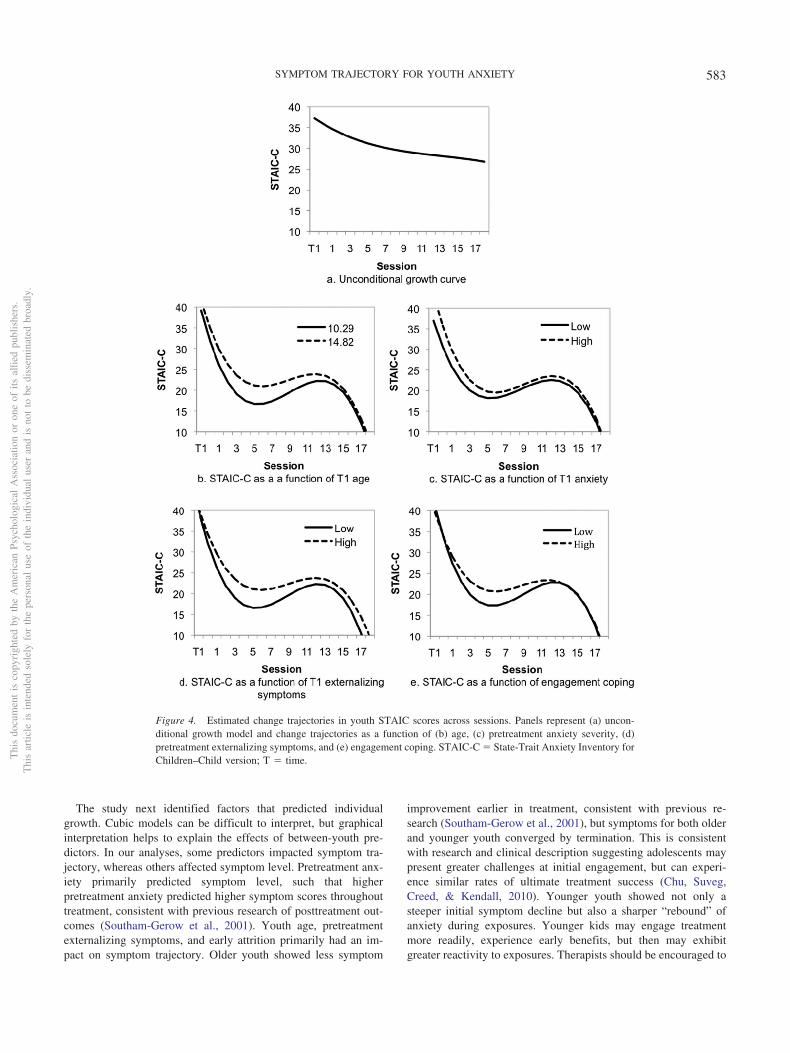
The study next identified factors that predicted individualgrowth. Cubic models can be difficult to interpret, but graphicalinterpretation helps to explain the effects of between-youth pre-dictors. In our analyses, some predictors impacted symptom tra-jectory, whereas others affected symptom level. Pretreatment anx-iety primarily predicted symptom level, such that higherpretreatment anxiety predicted higher symptom scores throughouttreatment, consistent with previous research of posttreatment out-comes (Southam-Gerow et al., 2001). Youth age, pretreatmentexternalizing symptoms, and early attrition primarily had an im-pact on symptom trajectory. Older youth showed less symptom
improvement earlier in treatment, consistent with previous re-search (Southam-Gerow et al., 2001), but symptoms for both olderand younger youth converged by termination. This is consistentwith research and clinical description suggesting adolescents maypresent greater challenges at initial engagement, but can experi-ence similar rates of ultimate treatment success (Chu, Suveg,Creed, & Kendall, 2010). Younger youth showed not only asteeper initial symptom decline but also a sharper “rebound” ofanxiety during exposures. Younger kids may engage treatmentmore readily, experience early benefits, but then may exhibitgreater reactivity to exposures. Therapists should be encouraged to
Figure 4. Estimated change trajectories in youth STAIC scores across sessions. Panels represent (a) uncon-ditional growth model and change trajectories as a function of (b) age, (c) pretreatment anxiety severity, (d)pretreatment externalizing symptoms, and (e) engagement coping. STAIC-C � State-Trait Anxiety Inventory forChildren–Child version; T � time.T
his
docu
men
tis
copy
righ
ted
byth
eA
mer
ican
Psyc
holo
gica
lA
ssoc
iatio
nor
one
ofits
allie
dpu
blis
hers
.T
his
artic
leis
inte
nded
sole
lyfo
rth
epe
rson
alus
eof
the
indi
vidu
alus
eran
dis
not
tobe
diss
emin
ated
broa
dly.
583SYMPTOM TRAJECTORY FOR YOUTH ANXIETY
stick through anxiety rebounds during exposures knowing thatanxiety will ultimately decline.
Youth with greater externalizing symptoms exhibited higheranxiety symptom scores throughout treatment, but ultimately re-ported improvement similar to youth with low externalizing symp-toms by termination. Clinical commentary notes several challengesincumbent to treating comorbid externalizing problems (e.g., Hud-son, Krain, & Kendall, 2001). It is possible that youth withexternalizing symptoms require greater behavioral management insession, reducing time that can be spent on practicing treatmentskills. Attrition prior to Session 10 was predictive of symptomcourse in the parent model, in which dropouts were estimated tohave an increase in anxiety after midtreatment. This implies anexacerbation of symptoms just prior to attrition. Results should beinterpreted cautiously as relatively few youth dropped out (21.8%),and mean number of attended sessions for dropouts was 3.53.Dropouts were also not followed after attrition. Both issues resultin limited data to reliably estimate trajectories.
We hypothesized that youth coping styles would portend benefitfrom therapy. Effects occurred in the opposite direction thananticipated. In the youth model, greater engagement coping (com-pared with lower engagement) predicted less improvement over
the first 10 sessions, even as both trajectories looked similar bytreatment end. Regardless of the effect engagement coping hadearly in treatment, exposures appeared to have an equalizingeffect, such that youth with high or low engagement styles expe-rienced comparable gains by termination. Results from the parentmodel suggest that greater disengagement coping (compared withlower disengagement) predicted greater symptom improvementthroughout therapy, with gains accelerating for the high-disengagement group. This pattern is opposite of the one weexpected; however, it should be noted that youth with both highand low disengagement scores improved overall. Future researchmay benefit from more frequent assessments and qualitative dataof youth coping to determine how youth with varying coping stylesare processing and making use of weekly therapy lessons.
Other variables did not predict level or trajectory of symptomcourse. School refusal has been associated with poorer outcomes inprevious studies (Layne et al., 2003), but it was not here. SSRIs didnot predict level or trajectory of symptoms as expected given theprevious success of combined SSRI and CBT treatment (Walkupet al., 2008). Here, youth were included only after a stable SSRIdose of at least 4 weeks. Given acute effects of SSRIs occur in thefirst 4–8 weeks, it is possible our trajectories reflected the symp-
Table 4Parent Model: Final Growth Models With Between-Youth (Level 2) Predictors
Midtreatment status (�0) Linear growth (�1) Quadratic growth (�2) Cubic growth (�3)
Fixed and random effects Estimate (SE) Estimate (SE) Estimate (SE) Estimate (SE)
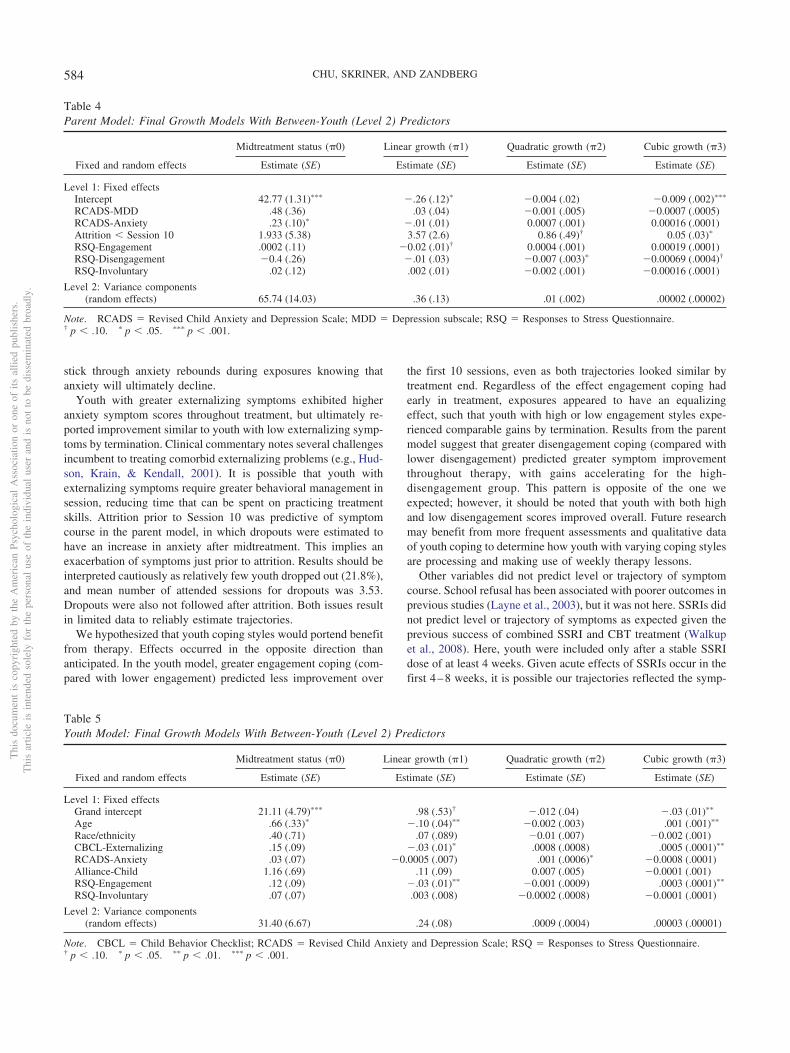
Level 1: Fixed effectsIntercept 42.77 (1.31)��� �.26 (.12)� �0.004 (.02) �0.009 (.002)���
RCADS-MDD .48 (.36) .03 (.04) �0.001 (.005) �0.0007 (.0005)RCADS-Anxiety .23 (.10)� �.01 (.01) 0.0007 (.001) 0.00016 (.0001)Attrition � Session 10 1.933 (5.38) 3.57 (2.6) 0.86 (.49)† 0.05 (.03)�
RSQ-Engagement .0002 (.11) �0.02 (.01)† 0.0004 (.001) 0.00019 (.0001)RSQ-Disengagement �0.4 (.26) �.01 (.03) �0.007 (.003)� �0.00069 (.0004)†
RSQ-Involuntary .02 (.12) .002 (.01) �0.002 (.001) �0.00016 (.0001)
Level 2: Variance components(random effects) 65.74 (14.03) .36 (.13) .01 (.002) .00002 (.00002)
Note. RCADS � Revised Child Anxiety and Depression Scale; MDD � Depression subscale; RSQ � Responses to Stress Questionnaire.† p � .10. � p � .05. ��� p � .001.
Table 5Youth Model: Final Growth Models With Between-Youth (Level 2) Predictors
Midtreatment status (�0) Linear growth (�1) Quadratic growth (�2) Cubic growth (�3)
Fixed and random effects Estimate (SE) Estimate (SE) Estimate (SE) Estimate (SE)
Level 1: Fixed effectsGrand intercept 21.11 (4.79)��� .98 (.53)† �.012 (.04) �.03 (.01)��
Age .66 (.33)� �.10 (.04)�� �0.002 (.003) .001 (.001)��
Race/ethnicity .40 (.71) .07 (.089) �0.01 (.007) �0.002 (.001)CBCL-Externalizing .15 (.09) �.03 (.01)� .0008 (.0008) .0005 (.0001)��
RCADS-Anxiety .03 (.07) �0.0005 (.007) .001 (.0006)� �0.0008 (.0001)Alliance-Child 1.16 (.69) .11 (.09) 0.007 (.005) �0.0001 (.001)RSQ-Engagement .12 (.09) �.03 (.01)�� �0.001 (.0009) .0003 (.0001)��
RSQ-Involuntary .07 (.07) .003 (.008) �0.0002 (.0008) �0.0001 (.0001)
Level 2: Variance components(random effects) 31.40 (6.67) .24 (.08) .0009 (.0004) .00003 (.00001)
Note. CBCL � Child Behavior Checklist; RCADS � Revised Child Anxiety and Depression Scale; RSQ � Responses to Stress Questionnaire.† p � .10. � p � .05. �� p � .01. ��� p � .001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
584 CHU, SKRINER, AND ZANDBERG

tom course of CBT alone, rather than any combined effects. Earlytherapy alliance marginally predicted midtreatment status in thefull youth model but not in the final model. Consistent alliance–outcome relationships have been found in youth treatment, butstronger relationships are typically found when alliance is mea-sured later in therapy (Shirk & Karver, 2003). Here, alliance wasmeasured at Session 4.
A cautionary note: The fitted youth mean curve appears rela-tively flat, whereas the fitted covariate models (see Figure 4b–e)appear much more cubic. We examined descriptive plots to con-firm support for such trajectories. Plots revealed relatively uniformsymptom decline in the first six to seven sessions, but substantialvariation in individual curves afterward (suggesting each signifi-cant covariate impacted trajectory). From visual inspection, webelieve the data reflect the presence of many different classes ofindividual trajectories. We did not have sufficient sample size toconduct such analysis (e.g., growth mixture modeling), but weencourage this in future efforts. We believe the fitted cubic modelattempts to accommodate this occurrence.
Limitations and Future Directions
The current investigation has several methodological limita-tions. The uncontrolled design of the study means that the fittedcubic model represents symptom change over 20 sessions that isthe aggregated result of specific (e.g., CBT intervention, therapisttechnique), nonspecific (e.g., therapeutic alliance), and external(e.g., time, historical events) factors. Control conditions help iso-late observed effects to specific experimentation factors. Futureresearch will want to fit models to data from randomized trials toclarify whether curvilinear trajectories are specific to CBT oruncontrolled factors. Nonetheless, the current growth models rep-resent CBT as it is likely delivered in the real world—as acombination of specific and nonspecific components. This is ar-guably a more generalizable and useful model, with greater trans-lation to real-world practice.
The relatively small sample size (N � 55) limits some ability tofit complex models, but our model-building approach accommo-dated this by fitting a full model with all predictors of interest, andthen retaining only significant predictors to estimate final coeffi-cients and variances in a parsimonious model. A priori power testswere not completed, and the results require replication to deter-mine whether any findings generalize to other samples (Zucker-man, Hodgins, Zuckerman, & Rosenthal, 1993). Finally, the CBTprotocol allowed therapists flexibility to conduct between 16 and20 sessions (guided by manual recommendations and clinicalsupervision). This flexibility produced increasingly “missing”Level 1 anxiety scores in later sessions (imbalanced data set).Nearly 80% of youth reached midtreatment and 60% completed 16sessions, but less than 2% reached Session 18 (as might be ex-pected). HLM can estimate models with substantial missing data,but greater proportions of “missing” data toward the end of therapymake estimates of the tail end of trajectories less reliable andprecise.
The cubic trajectory observed in this study provides avenues forfuture research. Both the initial early response and the flattening ofscores at midtreatment provide targets for examining treatmentmediators. Although the average trajectory would suggest mostyouth improve after a midtreatment lull in growth, some youth
may continue to show flat symptom trajectories, and yet othersmay experience worsening symptoms. It would be useful to ex-amine this early phase of exposures to detect what treatmentstrategies and mechanisms are responsible for variation in youthtrajectory. Furthermore, it remains to be determined whether othernonlinear growth patterns (e.g., sudden gains) can be identifiedwithin the mean cubic trajectory and whether they are associatedwith treatment outcomes. This study found preliminary evidencefor multiple plausible mean growth curves (cubic, log-linear),suggesting that multiple trajectory classes could be identified inlarger sample sizes. Finally, greater diversity in participants (race,ethnicity, socioeconomic status) and outcomes is warranted.Symptoms were the sole indicator of treatment outcome. Futureresearch will want to include greater breadth of clinical (symptom,impairment, functional) and process (cognitive, behavioral, phys-iological) outcomes to develop a more comprehensive understand-ing of the shape and process of change. This includes an evaluationof predictors and mediators that covary with outcome to determineboth predictive and reciprocal relations between outcomes andhypothesized predictors.
References
Achenbach, T., & Rescorla, L. (2001). Manual for the ASEBA School-AgeForms. Burlington: University of Vermont, Research Center for Chil-dren, Youth, and Families.
American Psychiatric Association. (2000). Diagnostic and statistical man-ual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Becker, C., Zayfert, C., & Anderson, E. (2004). A survey of psychologists’attitudes towards and utilization of exposure therapy for PTSD. Behav-iour Research and Therapy, 42, 277–292. doi:10.1016/S0005-7967(03)00138-4
Berman, S. L., Weems, C. F., Silverman, W. K., & Kurtines, W. M. (2000).Predictors of outcome in exposure-based cognitive and behavioral treat-ments for phobic and anxiety disorders in children. Behavior Therapy,31, 713–731. doi:10.1016/S0005-7894(00)80040-4
Chorpita, B. F., Yim, L., Moffitt, C., Umemoto, L. A., & Francis, S. E.(2000). Assessment of symptoms of DSM-IV anxiety and depression inchildren: A revised child anxiety and depression scale. Behaviour Re-search and Therapy, 38, 835–855. doi:10.1016/S0005-7967(99)00130-8
Chu, B. C., & Harrison, T. L. (2007). Disorder-specific effects of CBT foranxious and depressed youth: A meta-analysis of candidate mediators ofchange. Clinical Child and Family Psychology Review, 10, 352–372.doi:10.1007/s10567-007-0028-2
Chu, B. C., Suveg, C., Creed, T. A., & Kendall, P. C. (2010). Involvementshifts, alliance ruptures, and managing engagement over therapy . In D.Castro-Blanc & M. Karver (Eds.), Elusive alliance: Treatment engage-ment strategies with high-risk adolescents (pp. 95–121). Washington,DC: American Psychological Association. doi:10.1037/12139-003
Clerkin, E. M., Teachman, B. A., & Smith-Janik, S. B. (2008). Suddengains in group cognitive-behavioral therapy for panic disorder. Behav-iour Research and Therapy, 46, 1244–1250. doi:10.1016/j.brat.2008.08.002
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H., &Wadsworth, M. E. (2001). Coping with stress during childhood andadolescence: Problems, progress, and potential in theory and research.Psychological Bulletin, 127, 87–127. doi:10.1037/0033-2909.127.1.87
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A. H.,& Saltzman, H. (2000). Responses to stress in adolescence: Measure-ment of coping and involuntary stress responses. Journal of Consultingand Clinical Psychology, 68, 976–992. doi:10.1037/0022-006X.68.6.976
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
585SYMPTOM TRAJECTORY FOR YOUTH ANXIETY
Foa, E. B., & Kozak, M. J. (1986). Emotional processing of fear: Exposureto corrective information. Psychological Bulletin, 99, 20 –35. doi:10.1037/0033-2909.99.1.20
Gibson, N. M., & Olejnik, S. (2003). Treatment of missing data at thesecond level of hierarchical linear models. Educational and Psycholog-ical Measurement, 63, 204–238. doi:10.1177/0013164402250987
Greenberg, L. S. (2002). Integrating an emotion-focused approach totreatment in psychotherapy integration. Journal of Psychotherapy Inte-gration, 12, 154–189. doi:10.1037/1053-0479.12.2.154
Harrell, F. E. (2001). Regression modeling strategies. New York, NY:Springer-Verlag. doi:10.1007/978-1-4757-3462-1
Hayes, A. M., Feldman, G. C., Beevers, C. G., Cardaciotto, L., & Lewis-Smith, J. (2007). Discontinuities and cognitive changes in an exposure-based cognitive therapy for depression. Journal of Consulting and Clin-ical Psychology, 75, 409–421. doi:10.1037/0022-006X.75.3.409
Hayes, A. M., Laurenceau, J. P., Feldman, G., Strauss, J. L., & Cardaciotto,L. (2007). Change is not always linear: The study of nonlinear anddiscontinuous patterns of change in psychotherapy. Clinical PsychologyReview, 27, 715–723. doi:10.1016/j.cpr.2007.01.008
Hedeker, D., & Gibbons, R. D. (1997). Application of random-effectspattern-mixture models for missing data in longitudinal studies. Psycho-logical Methods, 2, 64–78.
Hofmann, S. G., Schulz, S. M., Meuret, A., Moscovitch, D., & Suvak, M.(2006). Sudden gains during therapy of social phobia. Journal of Con-sulting and Clinical Psychology, 74, 687–697. doi:10.1037/0022-006X.74.4.687
Hudson, J. L. (2005). Mechanisms of change in cognitive behavioraltherapy for anxious youth. Clinical Psychology: Science and Practice,12, 161–165. doi:10.1093/clipsy.bpi019
Hudson, J. L., Krain, A. L., & Kendall, P. C. (2001). Expanding horizons:Adapting manual-based treatments for anxious children with comorbiddiagnoses. Cognitive and Behavioral Practice, 8, 338–346.
Kane, M. T., & Kendall, P. C. (1989). Anxiety disorders in children: Amultiple-baseline evaluation of a cognitive-behavioral treatment. Behav-ior Therapy, 20, 499–508. doi:10.1016/S0005-7894(89)80129-7
Kendall, P. C., Comer, J. S., Marker, C. D., Creed, T. A., Puliafico, A. C.,Hughes, A. A., . . . Hudson, J. (2009). In-session exposure tasks andtherapeutic alliance across the treatment of childhood anxiety disorders.Journal of Consulting and Clinical Psychology, 77, 517–525. doi:10.1037/a0013686
Kendall, P. C., Flannery-Schroeder, E., Panichelli-Mindel, S. M., Southam-Gerow, M., Henin, A., & Warman, M. (1997). Therapy for youths withanxiety disorders: A second randomized clinical trial. Journal of Con-sulting and Clinical Psychology, 65, 366–380. doi:10.1037/0022-006X.65.3.366
Kendall, P. C., & Hedtke, K. (2006). Cognitive-behavioral therapy foranxious children: Therapist manual (3rd ed.). Ardmore, PA: WorkbookPublishing.
Kendall, P. C., Hudson, J. L., Gosch, E., Flannery-Schroeder, E., & Suveg,C. (2008). Cognitive-behavioral therapy for anxiety disordered youth: Arandomized clinical trial evaluating child and family modalities. Journalof Consulting and Clinical Psychology, 76, 282–297. doi:10.1037/0022-006X.76.2.282
Kendall, P. C., & Sugarman, A. (1997). Attrition in the treatment ofchildhood anxiety disorders. Journal of Consulting and Clinical Psy-chology, 65, 883–888. doi:10.1037/0022-006X.65.5.883
Lambert, M. J., Hansen, N. B., & Finch, A. E. (2001). Patient-focusedresearch: Using patient outcome data to enhance treatment effects.Journal of Consulting and Clinical Psychology, 69, 159–172. doi:10.1037/0022-006X.69.2.159
Layne, A. E., Bernstein, G. A., Egan, E. A., & Kushner, M. G. (2003).Predictors of treatment response in anxious-depressed adolescents withschool refusal. Journal of the American Academy of Child & AdolescentPsychiatry, 42, 319–326. doi:10.1097/00004583-200303000-00012
McLeod, B. D. (2011). The relation of the alliance with outcomes in youthpsychotherapy: A meta-analysis. Clinical Psychology Review, 31, 603–616. doi:10.1016/j.cpr.2011.02.001
Nishith, P., Resick, P. A., & Griffin, M. G. (2002). Pattern of change inprolonged exposure and cognitive-processing therapy for female rapevictims with posttraumatic stress disorder. Journal of Consulting andClinical Psychology, 70, 880–886. doi:10.1037/0022-006X.70.4.880
Pina, A. A., Silverman, W. K., Fuentes, R. M., Kurtines, W. M., & Weems,C. F. (2003). Exposure-based cognitive-behavioral treatment for phobicand anxiety disorders: Treatment effects and maintenance for Hispanic/Latino relative to European-American youths. Journal of the AmericanAcademy for Child & Adolescent Psychiatry, 42, 1179–1187. doi:10.1097/00004583-200310000-00008
Prins, P. J. M., & Ollendick, T. H. (2003). Cognitive change and enhancedcoping: Missing mediational links in cognitive behavior therapy withanxiety-disordered children. Clinical Child and Family Psychology Re-view, 6, 87–105. doi:10.1023/A:1023730526716
Raftery, A. E. (1995). Bayesian model selection in social research. Soci-ological Methodology, 25, 111–163. doi:10.2307/271063
Raudenbush, S. W., & Bryk, A. S. (2002). Hierarchical linear models:Applications and data analysis methods (2nd ed.). Thousand Oaks, CA:Sage.
Raudenbush, S. W., Bryk, A. S., & Congdon, R. T. (2009). Hierarchicallinear modeling 6.08 [Computer software]. Lincolnwood, IL: ScientificSoftware International.
Renaud, J., Brent, D. A., Baugher, M., Birmaher, B., Kolko, D. J., &Bridge, J. (1998). Rapid response to psychosocial treatment for adoles-cent depression: A two-year follow-up. Journal of the American Acad-emy of Child & Adolescent Psychiatry, 37, 1184–1190. doi:10.1097/00004583-199811000-00019
Shek, D. T. L., & Ma, C. M. S. (2011). Longitudinal data analyses usinglinear mixed models in SPSS: Concepts, procedures and illustrations.The Scientific World Journal, 11, 42–76. doi:10.1100/tsw.2011.2
Shirk, S. R., & Karver, M. (2003). Prediction of treatment outcome fromrelationship variables in child and adolescent therapy: A meta-analyticreview. Journal of Consulting and Clinical Psychology, 71, 452–464.doi:10.1037/0022-006X.71.3.452
Shirk, S. R., & Saiz, C. C. (1992). Clinical, empirical, and developmentalperspectives on the therapeutic relationship in child psychotherapy.Development and Psychopathology, 4, 713–728. doi:10.1017/S0954579400004946
Silverman, W. K., & Albano, A. M. (2000). Anxiety Disorders InterviewSchedule for Children (ADIS-IV) Child and Parent Interviews. NewYork, NY: Oxford University Press. doi:10.1017/CBO9780511663239
Silverman, W. K., Pina, A. A., & Viswesvaran, C. (2008). Evidence-basedpsychosocial treatments for phobic and anxiety disorders in children andadolescents. Journal of Clinical Child & Adolescent Psychology, 37,105–130. doi:10.1080/15374410701817907
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis:Modeling change and event occurrence. New York, NY: Oxford Uni-versity Press. doi:10.1093/acprof:oso/9780195152968.001.0001
Southam-Gerow, M., & Chorpita, B. F. (2007). Fears and anxieties. In E. J.Mash & R. A. Barkley (Eds.), Assessment of child disorders (4th ed., pp.347–397). New York, NY: Guilford Press.
Southam-Gerow, M. A., Kendall, P. C., & Weersing, V. R. (2001). Ex-amining outcome variability: Correlates of treatment response in a childand adolescent anxiety clinic. Journal of Clinical Child Psychology, 30,422–436. doi:10.1207/S15374424JCCP3003_13
Spielberger, C. (1973). Manual for State-Trait Anxiety Inventory for Chil-dren. Palo Alto, CA: Consulting Psychologists Press.
Strauss, C. (1987). Modification of trait portion of State–Trait AnxietyInventory for Children–Parent Form. Unpublished manuscript, Univer-sity of Florida, Gainesville.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
586 CHU, SKRINER, AND ZANDBERG

Tang, T. Z., & DeRubeis, R. J. (1999). Reconsidering rapid early responsein cognitive behavioral therapy for depression. Clinical Psychology:Science and Practice, 6, 283–288.
Thienemann, M., Moore, P., & Tompkins, K. (2006). A parent-only groupintervention for children with anxiety disorders: Pilot study. Journal ofthe American Academy of Child & Adolescent Psychiatry, 45, 37–46.doi:10.1097/01.chi.0000186404.90217.02
Walkup, J. T., Albano, A. M., Piacentini, J., Birmaher, B., Compton, S. N.,Sherrill, J. T., . . . Kendall, P. C. (2008). Cognitive behavioral therapy,sertraline, or a combination in childhood anxiety. The New EnglandJournal of Medicine, 359, 2753–2766. doi:10.1056/NEJMoa0804633
Zuckerman, M., Hodgins, H. S., Zuckerman, A., & Rosenthal, R. (1993).Contemporary issues in the analysis of data: A survey of 551 psychol-ogists. Psychological Science, 4, 49–53. doi:10.1111/j.1467-9280.1993.tb00556.x
Received January 22, 2011Revision received April 11, 2013
Accepted May 9, 2013 �
Additional Journal Information
Copyright and Permission: Those who wish to reuseAPA-copyrighted material in a non-APA publication mustsecure from APA written permission to reproduce a journalarticle in full or journal text of more than 800 cumulativewords or more than 3 tables and/or figures. APA normallygrants permission contingent on permission of the author,inclusion of the APA copyright notice on the first page ofreproduced material, and payment of a fee of $25 per page.Libraries are permitted to photocopy beyond the limits ofU.S. copyright law: (1) post-1977 articles, provided theper-copy fee in the code for this journal (0022-006X/11/$12.00) is paid through the Copyright Clearance Center,222 Rosewood Drive, Danvers, MA 01923; (2) pre-1978articles, provided that the per-copy fee stated in the Pub-lishers’ Fee List is paid through the CopyrightClearanceCenter. Formore information along with a permission re-quest form go to: www.apa.org/about/contact/copyright/index.aspx
Electronic access: Individuals subscribers to this journalhave automatic access to all issues of the journal in thePsycARTICLES® full-text database. See http://www.apa.org/pubs/journals.ccp and click on View Table of Con-tents.
Reprints: Authors may order reprints of their articles fromthe printer when they receive proofs.
Single Issues, Back Issues, and Back Volumes: For in-formation regarding single issues, back issues, or backvolumes, visit www.apa.org/pubs/journals/subscriptions.aspx or write to Order Department, American Psycholog-ical Association, 750 First Street, NE, Washington, DC20002-4242; call 202-336-5600 or 800-374-2721.
Subscription Claims Information: A claim form to assistmembers, institutions, and nonmember individuals who have aproblem with their subscription is available at http://forms.apa.org/journals/subclaim/; or call 1-800-374-2721.
Microform Editions: For information regarding micro-form editions, write to University Microfilms, Ann Arbor,MI 48106.
Change of Address: Send change of address notice and arecent mailing label to the attention of Subscriptions De-partment, APA, 30 days prior to the actual change ofaddress. APA will not replace undelivered copies resultingfrom address changes; journals will be forwarded only ifsubscribers notify the local post office in writing that theywill guarantee periodicals forwarding postage.
APA Journal Staff: Susan J. A. Harris, Senior Director,Journals Program; Paige W. Jackson, Director, EditorialServices; Tyler Krupa, Lead Editor; Skip Maier, Director,Journal Services; Richard Pepple, Account Manager; JodiAshcraft, Director, Advertising Sales and Exhibits.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
587SYMPTOM TRAJECTORY FOR YOUTH ANXIETY





























