Embed Size (px)
Citation preview
SCIENTIFIC LETTER TO THE EDITOR
Severe Limited Joint Mobility Syndrome in a Childwith Type 1 Diabetes Mellitus
Vandana Jain & Richa Jain
Received: 13 July 2011 /Accepted: 25 November 2011 /Published online: 13 December 2011# Dr. K C Chaudhuri Foundation 2011
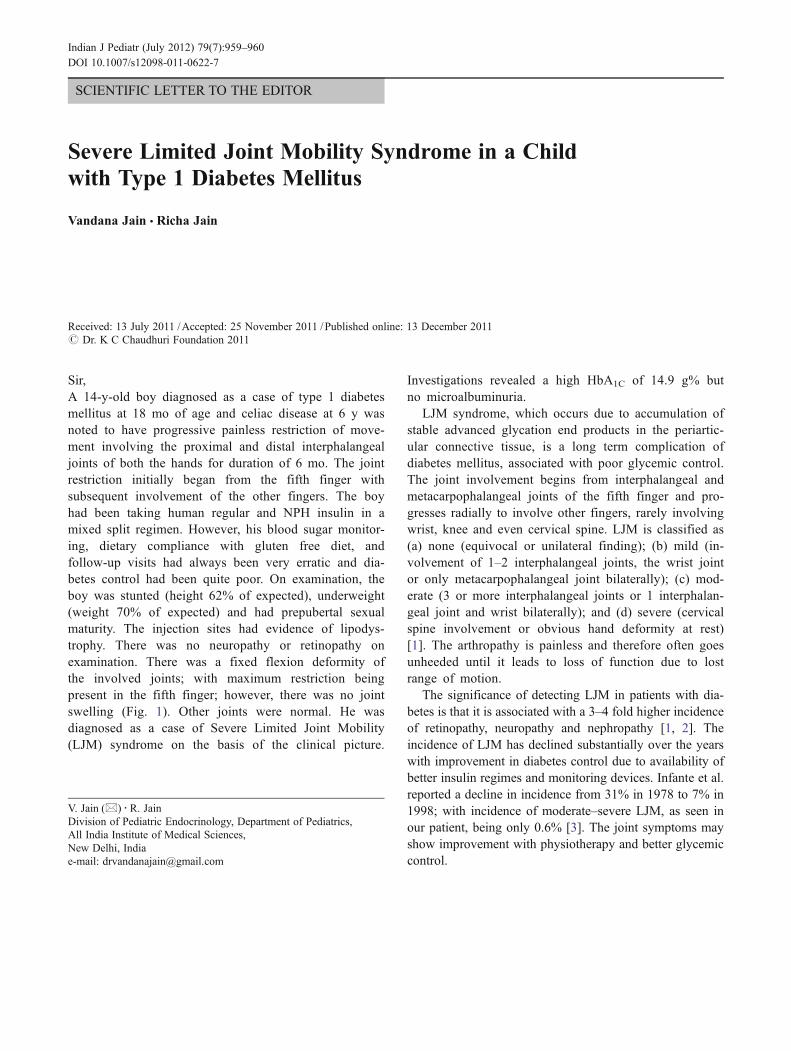
Sir,A 14-y-old boy diagnosed as a case of type 1 diabetesmellitus at 18 mo of age and celiac disease at 6 y wasnoted to have progressive painless restriction of move-ment involving the proximal and distal interphalangealjoints of both the hands for duration of 6 mo. The jointrestriction initially began from the fifth finger withsubsequent involvement of the other fingers. The boyhad been taking human regular and NPH insulin in amixed split regimen. However, his blood sugar monitor-ing, dietary compliance with gluten free diet, andfollow-up visits had always been very erratic and dia-betes control had been quite poor. On examination, theboy was stunted (height 62% of expected), underweight(weight 70% of expected) and had prepubertal sexualmaturity. The injection sites had evidence of lipodys-trophy. There was no neuropathy or retinopathy onexamination. There was a fixed flexion deformity ofthe involved joints; with maximum restriction beingpresent in the fifth finger; however, there was no jointswelling (Fig. 1). Other joints were normal. He wasdiagnosed as a case of Severe Limited Joint Mobility(LJM) syndrome on the basis of the clinical picture.
Investigations revealed a high HbA1C of 14.9 g% butno microalbuminuria.
LJM syndrome, which occurs due to accumulation ofstable advanced glycation end products in the periartic-ular connective tissue, is a long term complication ofdiabetes mellitus, associated with poor glycemic control.The joint involvement begins from interphalangeal andmetacarpophalangeal joints of the fifth finger and pro-gresses radially to involve other fingers, rarely involvingwrist, knee and even cervical spine. LJM is classified as(a) none (equivocal or unilateral finding); (b) mild (in-volvement of 1–2 interphalangeal joints, the wrist jointor only metacarpophalangeal joint bilaterally); (c) mod-erate (3 or more interphalangeal joints or 1 interphalan-geal joint and wrist bilaterally); and (d) severe (cervicalspine involvement or obvious hand deformity at rest)[1]. The arthropathy is painless and therefore often goesunheeded until it leads to loss of function due to lostrange of motion.
The significance of detecting LJM in patients with dia-betes is that it is associated with a 3–4 fold higher incidenceof retinopathy, neuropathy and nephropathy [1, 2]. Theincidence of LJM has declined substantially over the yearswith improvement in diabetes control due to availability ofbetter insulin regimes and monitoring devices. Infante et al.reported a decline in incidence from 31% in 1978 to 7% in1998; with incidence of moderate–severe LJM, as seen inour patient, being only 0.6% [3]. The joint symptoms mayshow improvement with physiotherapy and better glycemiccontrol.
V. Jain (*) :R. JainDivision of Pediatric Endocrinology, Department of Pediatrics,All India Institute of Medical Sciences,New Delhi, Indiae-mail: [email protected]
Indian J Pediatr (July 2012) 79(7):959–960DOI 10.1007/s12098-011-0622-7
References
1. Rosenbloom AL, Silverstein JH. Connective tissue and joint disordersin diabetes mellitus. Endocrinol Metab Clin North Am. 1996;25:473–83.
2. Rosenbloom AL. Limitation of finger joint mobility in diabetesmellitus. J Diabet Complications. 1989;3:77–87.
3. Infante JR, Rosenbloom AL, Silverstein JH, Garzarella L, PollockBH. Changes in frequency and severity of Limited joint mobility inchildren with type I diabetes mellitus between 1976–1978 and 1998.J Pediatr. 2001;138:33–7.
Fig. 1 Fixed flexiondeformity of proximal anddistal interphalangeal jointsof all fingers.
960 Indian J Pediatr (July 2012) 79(7):959–960





























