Embed Size (px)
Citation preview

Postgraduate Medical Journal (1988) 64, 791-795
Severe disseminated intravascular coagulation associatedwith massive ventricular mural thrombus following acutemyocardial infarction
S.A. Solomon, D.W.K. Cotton, F.E. Preston and L.E. Ramsay
University Departments of Haematology, Pathology and Therapeutics, Royal Hallamshire Hospital, SheffieldS1O 2JF, UK
Summary: We describe three patients who developed severe disseminated intravascular coagula-tion associated with large ventricular mural thrombi shortly after presenting with acute myocardialinfarction. To our knowledge this association has not been reported before.
Introduction
Disseminated intravascular coagulation (DIC) hasbeen reported in a wide variety of disorders, withinfection, malignancy, trauma and surgery account-ing for most cases.1 Modest increases in fibrindegradation products have been reported inpatients with severe myocardial infarction but overtDIC is rare.2 We describe three patients whodeveloped severe DIC associated with large ventri-cular thrombi shortly after presenting with acutemyocardial infarction. Large intravascular thrombiarising from intra- or extracardiac sites have beenreported to cause DIC."",2 We propose that thelarge ventricular mural thrombi may have initiatedDIC in our patients.
Case reports
Case I
A 63 year old woman was admitted with a trans-mural anterior myocardial infarction. She had beenfit previously apart from a partial gastrectomy forpeptic ulceration. Investigation showed peak serumcreatine kinase (CPK) >2000 Pmol/l (normal< 195 umol/1); peak lactate dehydrogenase (LDH)2320 pmol/l (normal <265 umol/l), haemoglobin10.9g/dl with features of iron deficiency, platelets423 x 109/l and blood glucose 14.0 mmol/l. Subse-quent blood glucose values were around 9.0mmol/l.During the first hospital day she had a single
episode of ventricular fibrillation, which was cor-rected promptly by defibrillation, followed by epi-sodes of supraventricular and broad-complextachycardia. She was well on day 2, but developedmild left ventricular failure and right lower lobeconsolidation on the third day. Streptococcus pneu-moniae was cultured from sputum, but blood cul-tures were sterile. The heart failure and pneumoniaresponded to diuretic and antibiotic treatment.Progress was then uncomplicated until the 12thhospital day, when she developed spontaneousbleeding from venepuncture sites and purpura.Investigations were suggestive of DIC (Table I).The blood film showed the features of microangio-pathic haemolysis with numerous schistocytes,microspherocytes and polychromasia. OccasionalHowel-Jolly bodies were noted.
Despite treatment with low-dose subcutaneousheparin and transfusions of whole blood and plate-lets she developed, over the next 5 days, slowlyprogressing arterial occlusion in both legs, deepvein thrombosis in both legs, severe abdominalpain, and renal failure progressing to anuria. Shedied 17 days after admission. The drugs admin-istered before the onset of DIC were lignocaine,mexiletine, amiodarone, spironolactone andfrusemide.
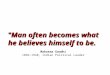
Post-mortem examination revealed a recent trans-mural infarct involving both ventricles, with a largelamellated mural thrombus overlying the infarct(Figure 1). All three coronary arteries were involvedby moderate to severe atheroma and the bifurcationof the left coronary artery contained recent throm-bus blocking both branches. The right pulmonaryartery was blocked by a large embolus and therewere in addition multiple peripheral thrombi and
C The Fellowship of Postgraduate Medicine, 1988
Correspondence: S.A. Solomon, M.R.C.P., UniversityDepartment of Therapeutics, Royal Hallamshire Hospital,Sheffield SlO 2JF, UK.Accepted: 19 May 1988
copyright. on June 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.756.791 on 1 October 1988. D
ownloaded from

792 CLINICAL REPORTS
Table I Results of coagulation studies in three cases
Investigation Patients
Case I Case 2 Case 3
1. Platelet count (normal range 150-400 x 109/1) 5.0 27.0 88.02. Prothrombin time (control) (seconds) 15.0 (12.0) 23.0 (13.0) 45.0 (12.0)3. KCCT (control) (seconds) 38.0 (40.0) 58.0 (42.0) 63.0 (41.0)4. Thrombin time (control) (seconds) 10.0 (11.0) 25.0 (10.0) 13.0 (11.0)5. Fibrin degradation products (normal range 0-8 ng/ml) 64.0 256.0 128.06. Fibrin monomer Positive Positive Positive7. Fibrinogen (g/l) (normal range 1.6-3.9g/1) 1.7 0.3 1.28. Haemoglobin (g/dl) 8.5 14.8 12.69. White cell count x 109/1 16.4 24.0 19.7
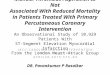
infarcts. In the legs both femoral and posteriortibial veins contained extensive thrombi. The livershowed several infarcts associated with multiplehepatic vein thromboses, and several fibrin plugswere seen in the spleen (Figure 2).
.. :. .~ ~~~~ :: ... ...:.: ... .....~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. .. .. I.. ...I .........~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ............. ...... .!
d'"g l l ,.....~~~~~~~~~~~~~ ~~~~~~~~~~~~~~~~~~~~~~~~~..... ...... ..~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...;.... ..... .... . : .. . ....Figure 1 Low power photomicrograph of left ventri-cular free wall with recent infarction and laminatedthrombus overlying it (Case 1). (H & BEx2.8).
Case 2
A 52 year old man was admitted with a transmuralanterior myocardial infarction. He was previouslyfit. Serum CPK peaked at >20001imol/1 and LDH
Figure 2 High power photomicrograph of the spleenwith thrombin plugs in small vessels (Case 1). (H &E x 42.5).
copyright. on June 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.756.791 on 1 October 1988. D
ownloaded from

CLINICAL REPORTS 793
at > 2280 yimol/l. On admission haemoglobin was14.6 g/dl; platelet count 269 x 109/1, and blood glu-cose 12.2 mmol/l.He had a single episode of ventricular fibrillation,
which responded to defibrillation, on the firsthospital day. On day 2, he had pericarditis andmild left ventricular failure which responded todiuretic treatment. Blood cultures were sterile. Hewas then well until day 7 when he became drowsy,generally unwell and dehydrated. Investigationsrevealed a hyperosmolar non-ketotic diabetic statewith blood glucose 30.5 mmol/l and calculatedserum osmolality 345mosm/l. He was treated withintravenous saline and insulin, and the blood glu-cose had fallen to 8.3mmol/1 6 hours later. At thistime he developed spontaneous bleeding from vene-puncture sites and his nose, and tests of coagula-tion indicated DIC (Table I). His blood film wasgrossly abnormal and showed the characteristicfeatures of microangiopathic haemolysis. Howell-Jolly bodies were also prominent.He was treated with cryoprecipitate and subcuta-
neous heparin, 5000 units 8-hourly, but developedslowly progressing arterial occlusion in both legs,renal failure progressing to anuria and worseningleft ventricular failure. He died on the 12th hospitalday. The drugs administered before the onset ofDIC were frusemide, glibenclamide and aspirin.Post-mortem examination showed a circumferen-
tial left ventricular infarct of 1-2 weeks durationcovered by organizing thrombus. The left anteriordescending coronary artery was blocked by throm-bus. The liver showed evidence of chronic conges-tive cardiac failure and the lungs were oedematousand congested with early consolidation at the bases.Histology confirmed the myocardial infarction andrevealed centrilobular necrosis in the liver. Thelungs showed diffuse alveolar damage consistentwith adult respiratory distress syndrome (Figure 3).
Case 3
A 61 year old man with asymptomatic mitral valveprolapse was admitted with a transmural anteriormyocardial infarction. Peak serum CPK was>2000 ,umol/l and LDH >3000 ymol/l. On admis-sion haemoglobin was 12.5 g/dl; platelet count209 x 109/1 and blood glucose 11.0 mmol/l. Hedeveloped worsening left ventricular failure andcardiogenic shock, which did not respond to treat-ment, and by day 5 had renal failure (serumcreatinine 469mmol/1) and metabolic acidosis. Onthe fifth day he developed purpura and sponta-neous bleeding from venepuncture sites and therewas unequivocal laboratory evidence of DIC (TableI). He continued to deteriorate, developed arterialocclusion in both legs and died 6 days after admis-
'fw '.,y 1.t *.***
Figure 3 High power photomicrograph of lung show-ing debris within the alveoli and hyaline materiallining their walls (Case 2). (H & E x 42.5).
sion. The drugs administered before the onset ofDIC were frusemide, dopamine and ResoniumA.Post-mortem examination showed an established
circumferential, transmural myocardial infarction ofthe left ventricle. There was mural thrombus over-lying the infarct within each ventricle. Recentthrombus occluded the right coronary and all threecoronary arteries showed moderate to severe ather-oma. The mitral valve showed 'floppy mitral valve'changes with a prolapsing posterior leaflet. Thelungs and liver showed evidence of acute andchronic cardiac failure respectively. Histology con-firmed the macroscopic findings in the heart andrevealed centrilobular necrosis in the liver. Nodirect evidence of small vessel occlusion wasrecognized.
Discussion
Modest increases of fibrinogen degradation pro-ducts have been noted in some patients with severe
copyright. on June 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.756.791 on 1 October 1988. D
ownloaded from

794 CLINICAL REPORTS
myocardial infarction, but clinically overt DICseems to be very rare.2 We have found only onereport of overt DIC possibly complicating acutemyocardial infarction.3 However, the patient de-scribed also had severe heart failure and multipleangiolipomata, and these were considered the prin-cipal causes of the DIC. The three patients de-scribed here, who presented in one hospital within aperiod of 5 months, all developed severe DIC 5-12days after an acute myocardial infarction. Onepatient (Case 3) would probably have died ofcardiogenic shock in any event, but the other twopatients were recovering from their myocardialinfarctions satisfactorily and died of overwhelmingDIC. Possible causes of DIC could be identified intwo of these patients. Case 2 had developed ahyperosmolar ketotic state 7 days after myocardialinfarction. Severe DIC is a recognized but rarecomplication of severe diabetic ketoacidosis and hasbeen reported occasionally in the hyperosmolarnon-ketotic diabetic state.4'5 Case 3 had severeshock and acidosis, factors which may triggerDIC.6 However DIC has not been reported com-monly in cardiogenic shock.
Case 1 is of particular interest because no recog-nized cause of DIC could be identified. She had asingle episode of ventricular fibrillation shortly aftermyocardial infarction. Patients who survive a car-diac arrest may show laboratory evidence of DIC,but this is mild and transient.7 In any event thecardiac arrest occurred 11 days before the onset ofDIC. She also had pneumococcal pneumonia 9days before the onset of DIC but this had res-ponded rapidly to antibiotic treatment and was notcomplicated by septicaemia.The striking observation was that all three
patients had massive ventricular mural thrombi.Mural thrombus develops in about one third ofpatients with anterior myocardial infarction, but thethrombi observed in these cases were exceptionallylarge.8 We believe that the association with severeDIC was not fortuitous. The association of DICwith massive left ventricular mural thrombus hasbeen reported previously in one patient with heartfailure.9 The authors suggested that DIC led toincorporation of fibrin into a pre-existing muralthrombus resulting in growth of the thrombus to
massive proportions. This interpretation is sup-ported by evidence that DIC can cause formationof mural thrombus even when coronary thrombosisand myocardial infarction have not occurred.10 It istherefore conceivable that DIC caused growth ofpre-existing mural thrombus and resulted in mas-sive thrombus formation in our patients. However,if this was the complete explanation for the associa-tion, the development of DIC in Case 1 wouldremain entirely unexplained. We suggest that themassive mural thrombi actually caused, or at leastcontributed to, the development of DIC in ourpatients. In support of this is the observation thatgiant left atrial thrombus in mitral stenosis 112 hasbeen associated with DIC. One explanation is thatthese thrombi 'consume' coagulation factors locally,as evidenced by incorporation of fibrin and fibrino-genl" but a more likely mechanism is that injury tored cells, platelets, or both act as a trigger to thecoagulation mechanism.' The abnormal pattern ofblood flow over large intravascular thrombi mayresult in red cell and platelet injury, leading toactivation of coagulation and platelets and wide-spread dispersion of activated clotting factors.1 Thenet result being enhanced coagulation at the surfaceof the thrombus and DIC. In support of this, Case1, who had no recognized cause of DIC, showedfibrin plugs, thrombi, and infarcts in several organs.These findings could not be explained by 'consump-tion' of coagulation factors. In addition the bloodfilms of Cases 1 and 2 showed the presence of largenumbers of schistocytes which provide good sup-portive evidence of DIC. It is well established thatthese are red cells that have sustained mechanicaldamage on thin fibrin strands.13We propose that formation of large ventricular
mural thrombi may have initiated the DIC in ourpatients. DIC may then have caused further en-largement of the mural thrombi with consequentworsening of DIC.
Acknowledgements
We thank Dr C.D. Holdsworth and Dr J.J. Daly forallowing us to report cases under their care, Dr N.Rooney and Dr S. Dundas for the histopathology reportsand Mrs E. Grassam for typing the manuscript.
References
1. Colman, R.W., Robbey, J.S. & Minnor, J.S.Disseminated intravascular coagulation (DIC): anapproach. Am J Med 1972, 52: 679-689.
2. Okuno, T. & Nelson, C. Value of determination ofserum fibrin-fibrinogen degradation products in acutemyocardial infarction. Am J Clin Pathol 1974, 61:155-159.
3. Rustin, G.J.S. Diffuse intravascular coagulation inassociation with myocardial infarction and multipleangiolipomata. Postgrad Med J 1977, 53: 228-229.
4. Kwaan, H.C., Colwell, J.A. & Suwanwela, N. Dis-seminated intravascular coagulation in diabetesmellitus, with reference to the role of increasedplatelet aggregation. Diabetes 1972, 21: 108-113.
copyright. on June 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.756.791 on 1 October 1988. D
ownloaded from

CLINICAL REPORTS 795
5. Timperley, W.R., Preston, F.E. & Ward, J.D.Cerebral intravascular coagulation in diabeticketoacidosis. Lancet 1974; i: 952-956.
6. Hardaway, R.M., James, P.M., Anderson, R.W. et al.Intensive study and treatment of shock in man.JAMA 1967, 99: 779-790.
7. Mehta, B., Briggs, D.K., Sommers, S.C. & Karpatkin,M. Disseminated intravascular coagulation followingcardiac arrest: a study of 15 patients. Am J Med Sci1972, 264: 353-363.
8. Asinger, R.W., Mikell, F.L., Elsperger, J. & Hodges,M. Incidence of left ventricular thrombosis after acutetransmural myocardial infarction. N Engl J Med 1981,305: 297-302.
9. Heckman, T.A. & Tosove, M.H. Massive leftventricular mural thrombosis with consumptioncoagulopathy in congestive heart failure. West J Med1980, 133: 442-444.
10. Sigiura, M., Hiroaka, K., Ohkawa, S., Ueda, K.,Malsuda, J. & Murakami M. A clinicopathologicalstudy on cardiac lesions in 64 cases of disseminatedintravascular coagulation. Jpn Heart J 1977, 18:57-69.
11. Ikematsu, S., Itoh, O., Samori, T. et al. A case ofconsumption coagulopathy due to atrial giantthrombus. Rinsho Ketsueki 1975, 16: 530-536.
12. McIlraith, D.M., Mount, M.J. & Brien, F.W. Chronicconsumptive coagulopathy due to intracardiacthrombus. Am J Med 1987, 82: 135-136.
13. Bull, B.S., Rubenberg, M.L., Dacie, J.V. & Brain,M.C. Microangiopathic haemolytic anaemia;mechanisms of red-cell fragmentation: in vitro studies.Br J Haematol 1968, 14: 643-652.
copyright. on June 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.756.791 on 1 October 1988. D
ownloaded from