Embed Size (px)
Citation preview

Severe Hypertension: Does This Patient Need to Go to the ER?
Joseph P. Martinez, MD, FACEP, FAAEM
Associate Professor of Emergency Medicine and Medicine
Assistant Dean for Student Affairs
University of Maryland School of Medicine
Baltimore, Maryland

Scary numbers

Scary numbers

Scary numbers


Cases
• Case 1
• 68 yo presents to office with BP 220/140
• Complains of “ripping” pain between shoulder blades
• Options
• No medications, have patient start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER

Aortic Dissection

Cases
• Case 2
• 68 yo presents to office with BP 220/140
• Complains of acute onset severe headache
• Altered mental status, not moving one side
• Options
• No medications, have patient start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER

Hypertensive ICH

Cases
• Case 3
• 68 yo presents to office with BP 220/140
• Complains of dyspnea, PND, orthopnea
• Saturations 78% in office, tachypneic, pink sputum
• Options
• No medications, have start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER

Acute Pulmonary Edema

Some Decisions in Medicine are Easy!

• Case 4
• 68 yo presents to office with BP 220/140
• No complaints
• Options
• No medications, have patient start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER
Cases

• Case 5
• 68 yo presents to office with BP 220/140
• No complaints
• Recently started TID ibuprofen for arthritis pain
• Options
• No medications, have patient start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER
Cases

• Case 6
• 68 yo presents to office with BP 220/140
• Complains of mild frontal headache; “I get it
when my pressure is up”
• Options
• No medications, have patient start BP log
• Start medication and see in one week
• Have family take patient to ER
• Have EMS take patient to ER
Cases

Objectives
• Discuss terminology of hypertension
• Discuss whether nonspecific symptoms still count
as “asymptomatic”
• Describe an effective office approach to
asymptomatic HTN
• Deliberate about the pros and cons of rapidly
lowering BP

Demographics
• 35 million office visits yearly
• Affects 25% of population
• 50 million in the US
• 1 billion worldwide
• 30% don’t know they have it
• Control rates fall short in 50%

From JNC VII
“The risk of CVD, beginning at 115/75 mm Hg,
doubles with each increment of 20/10 mm Hg”
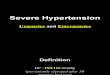
JNC 8

Hypertension
• Accurate (appropriate cuff, repeated measurements)
• Regression to the mean
• Reactive (pain, anxiety, withdrawal, drugs)

How Quickly to Treat?

From JNC VII
• “Elevated blood pressure alone, in the absence of
symptoms or new or progressive target organ
damage, rarely requires emergency therapy”

From JNC VII
• “Elevated blood pressure without target organ
damage does not require hospitalization but should
receive immediate combination oral therapy”
• (No references)

Terminology

Classic Terminology

Hypertensive Urgency?
• Is it really urgent?
• Framing phenomenon
• Education• Patients
• Nurses

New Terminology

Hypertensive Urgency
• Severely increased BP
• High-risk for rapidly progressive end-organ
damage
• CHF
• CAD
• Renal disease
• TIA/CVA

Hypertensive Urgency
• Increased level of scrutiny
What is Asymptomatic?
• 26% of patients with elevated BP will have a
complaint of a “hypertension” symptom
• Nearly 68% will have them if prompted
• No correlation between symptoms and level
of blood pressure elevation
• History
• Physical
• Labs
• Follow-up
How to approach these patients

• History
How to approach these patients

How to approach these patients
• History
• Previous diagnosis
• Previous medications
• Compliance
• Perturbers
• Symptoms
Perturbers
• Illness
• Pain
• Anxiety
• Ingestions• Illicits
• Sympathomimetics
• MAO-I
• NSAIDs


• History
• Physical
• Labs
• Follow-up
How to approach these patients

• Physical
How to approach these patients

• Physical
• Mental status
• Cardiopulmonary examination
• Neurological examination
• FUNDUS
How to approach these patients

Fundus

Fundus

Fundus

Fundus

How to approach these patients
• History
• Physical
• Labs
• Follow-up

How to approach these patients
• Labs

Labs
• JNC VII
• EKG, UA, Glucose, Hematocrit, Potassium,
Creatinine, Calcium, Fasting Lipid Profile

• CXR and EKG not helpful
• 116 patients
• 2/116 had interventions based on tests
• None influenced BP management
Labs

• Renal function is important to know
• 167 asymptomatic patients
• 7.2% had abnormal BMP requiring admission
• Urinalysis instead of blood work
• All patients with significantly elevated creatinine had
hematuria or proteinuria
• Specificity improved with 1+ proteinuria
Labs

Treatment
• VA Cooperative Trial
•NO adverse events in the first three months
among patients with DBP 115-129 irrespective of
whether they received treatment or placebo

• Zeller 1989: DBPs 116-139; randomized to:
• Clonidine load to decrease BP
• Hourly placebo x 4
• Immediate discharge
• All received prescription on discharge
• No difference in outcomes or BP control at 3
months
Treatment

• VALUE trial
• Valsartan vs. amlodipine
• Increased cardiovascular events in 6 months when BP
not controlled
• Difference in events diminished as control became
similar
• BP control is important in relatively short time
• Months NOT days
Treatment

• What’s the downside to treating aggressively?
Treatment

• No studies have definitively shown benefit to
acutely lowering blood pressure in asymptomatic
patients
• Multiple studies demonstrate HARM
JAMA. 1996;276:1328-1331
Treatment

• Follow-up is the key!
• This is where PCPs have the advantage
• If known HTN, restart/adjust meds
• If newly diagnosed, recheck in 24-48 hours
• Can initiate treatment if very high
• Look for perturbers!
Treatment

Send to ED?
• Hypertensive emergencies
• YES!
• Severe asymptomatic hypertension
• Almost never
• Hypertensive urgency (new definition)
• Probably not, but on occasion

What usually happens in ED
• Waiting and waiting and waiting
• History and physical
• Labs
• Observation
• Likely discharge home with large bill

What might happen in ED
• Waiting and waiting and waiting
• History and physical
• Labs
• Admit to hospital
• Started on meds and discharged with larger
bill

• Waiting and waiting and
waiting
• History and physical
• Labs
• Someone panics over the
numbers and gives IV
Hydralazine
What could happen in ED

Summary
• Severe hypertension is common
• Try to get away from the term “hypertensive urgency”
• Blood pressure needs treatment!• Weeks to months NOT hours to days
• Numbers are scary• Educate patients, nurses, other providers
• Stop practicing “eminence-based medicine”