Embed Size (px)
Citation preview

4/9/2015
1
AOHC 2015 is ACOEM’s 100th
Session 310: Prescription Drugs & Safety for Transportation Workers
Topic: Drugs, Adverse Effects, Recommendations
James H. Diaz, MD, MHA, MPH, DrPH, DABA, FCCM, FCCP, FACPM, FACOEM, FACMT*
*Professor of Public Health/Preventive Medicine & Anesthesiology/Critical Care MedicineLSU Schools of Public Health & Medicine
New Orleans, LA 70112
Rx Drug Epidemic: Outline1. An epidemic of Rx drug abuse
2. Amphetamines
3. Barbiturates
4. Benzodiazepines
5. Benzodiazepine receptor‐agonist sleep drugs (“Z”
drugs)
5. Opioid agonists & agonists/ antagonists
6. An “array” of antipsychotics
7. Lethal combinations
8. Conclusions
• We are in an epidemic of Rx drug abuse. Refs:
• Yu HY. The prescription drug abuse epidemic. Clin Lab Med. 2012;32(3):361‐377.
• Maxwell JC. The prescription drug epidemic in the united states: A perfect storm. Drug Alcohol Rev. 2011;30(3):264‐270.
• 3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: Prescription drug overdoses ‐ a U.S. epidemic. MMWR Morb Mortal Wkly Rep. 2012;61(1):10‐13.
Rx Drug Epidemic: Amphetamines 1.• The most commonly prescribed
amphetamines for ADHD have included methylphenidate(Concerta®, Ritalin®) & Adderall®.
• Adderall® is a combination drug composed of 2 amphetamine salts (aspartate & sulfate) & 2 dextroamphetamine salts (saccharide & sulfate) & is more potent than methylphenidate with a longer period of efficacy even at low doses.
• In ADHD, amphetamines increase attention span and concentration by inhibiting the reuptake of dopamine and norepinephrine in the brain.
• Ref: Cox DJ, Merkel RL, Moore M, et al. Relative benefits of stimulant therapy with OROS methylphenidate versus mixed amphetamine salts extended release in improving the driving performance of adolescent drivers with attention‐deficit/hyperactivity disorder. Pediatrics 2006; 118: e704‐10.

4/9/2015
2
Rx Drug Epidemic: Amphetamines 2.• Patients taking amphetamines
for ADHD are at risk of potentially fatal drug‐drug interactions from the co‐administration of any other centrally‐acting dopamine, norepinephrine, or serotonin reuptake inhibitor (MAOIs, SSRIs, SNRIs, tricyclics, meperidine, tramadol, & buproprion).
• Acute myocardial infarction & sudden cardiac death have been reported in young adults taking prescribed Adderall®, especially when combined with alcohol, cocaine, or methamphetamines.
• Ref: Jiao X, Velez S, Ringstad J, et al. Myocardial infarction associated with Adderall XR and alcohol use in a young man. J Am Board Family Med 2009; 22: 197‐201.
Rx Drug Epidemic: Amphetamines 3.• Untreated ADHD has been
associated with a 3‐ to 4‐fold increase in driving‐related accidents and associated injuries, especially in young male drivers.
• In placebo‐controlled investigations, study subjects with ADHD demonstrated significantly less driving variability & better driving performance, especially in the evenings, when taking therapeutic doses of amphetamine stimulants compared to placebo.
• Ref: Cox DJ, Merkel RL, Penberthy JK, et al. Impact of methylphenidate delivery profiles on driving performance of adolescents with attention‐deficit /hyperactivity disorder: a pilot study. J Am Acad Child Adolesc Psych 2004; 43: 269‐75.
Recommendations:
• Employees who are diagnosed with ADHD by physicians & who are medically prescribed amphetamine stimulants in order to increase concentration & attention span at work should be monitored by their personal physicians, may qualify for CDLs, & may also perform other safety sensitive duties at work as indicated in their job descriptions.
• They may work without restrictions and be subject to the same DOT‐required urine drug tests as all other employees.
Rx Drug Epidemic: Barbiturates 1.• Barbiturates are cardiorespiratory &
CNS depressants that produce a spectrum of clinical effects ranging from anxiolysis to coma & death.
• Although barbiturates remain in very limited use today as anesthesia induction agents & in combined preparations for migraine headaches (Fiorinal®) & heartburn (Donnatal®), their use has declined even further as newer drugs have proven to be more effective.
• Chronic barbiturate use is associated with greatly increased risks of physical dependence, psychological addiction, withdrawal effects, & death.
• Ref: Wenzel RG, Sarvis CA. Do butalbital‐containing products have a role in the management of migraine? Pharmacotherapy 2002; 22: 1029‐35.
4/9/2015
3
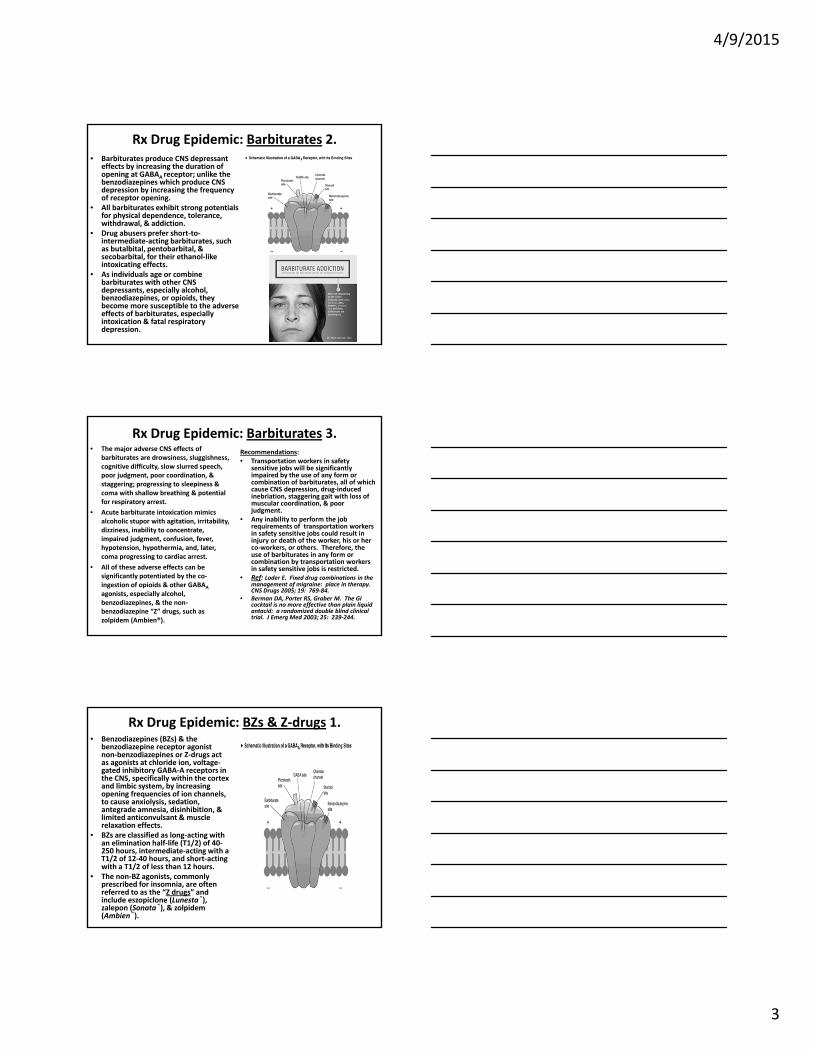
Rx Drug Epidemic: Barbiturates 2.• Barbiturates produce CNS depressant
effects by increasing the duration of opening at GABAA receptor; unlike the benzodiazepines which produce CNS depression by increasing the frequency of receptor opening.
• All barbiturates exhibit strong potentials for physical dependence, tolerance, withdrawal, & addiction.
• Drug abusers prefer short‐to‐intermediate‐acting barbiturates, such as butalbital, pentobarbital, & secobarbital, for their ethanol‐like intoxicating effects.
• As individuals age or combine barbiturates with other CNS depressants, especially alcohol, benzodiazepines, or opioids, they become more susceptible to the adverse effects of barbiturates, especially intoxication & fatal respiratory depression.
Rx Drug Epidemic: Barbiturates 3.• The major adverse CNS effects of
barbiturates are drowsiness, sluggishness, cognitive difficulty, slow slurred speech, poor judgment, poor coordination, & staggering; progressing to sleepiness & coma with shallow breathing & potential for respiratory arrest.
• Acute barbiturate intoxication mimics alcoholic stupor with agitation, irritability, dizziness, inability to concentrate, impaired judgment, confusion, fever, hypotension, hypothermia, and, later, coma progressing to cardiac arrest.
• All of these adverse effects can be significantly potentiated by the co‐ingestion of opioids & other GABAA
agonists, especially alcohol, benzodiazepines, & the non‐benzodiazepine “Z” drugs, such as zolpidem (Ambien®).
Recommendations:• Transportation workers in safety
sensitive jobs will be significantly impaired by the use of any form or combination of barbiturates, all of which cause CNS depression, drug‐induced inebriation, staggering gait with loss of muscular coordination, & poor judgment.
• Any inability to perform the job requirements of transportation workers in safety sensitive jobs could result in injury or death of the worker, his or her co‐workers, or others. Therefore, the use of barbiturates in any form or combination by transportation workers in safety sensitive jobs is restricted.
• Ref: Loder E. Fixed drug combinations in the management of migraine: place in therapy. CNS Drugs 2005; 19: 769‐84.
• Berman DA, Porter RS, Graber M. The GI cocktail is no more effective than plain liquid antacid: a randomized double blind clinical trial. J Emerg Med 2003; 25: 239‐244.
Rx Drug Epidemic: BZs & Z‐drugs 1.• Benzodiazepines (BZs) & the
benzodiazepine receptor agonist non‐benzodiazepines or Z‐drugs act as agonists at chloride ion, voltage‐gated inhibitory GABA‐A receptors in the CNS, specifically within the cortex and limbic system, by increasing opening frequencies of ion channels, to cause anxiolysis, sedation, antegrade amnesia, disinhibition, & limited anticonvulsant & muscle relaxation effects.
• BZs are classified as long‐acting with an elimination half‐life (T1/2) of 40‐250 hours, intermediate‐acting with a T1/2 of 12‐40 hours, and short‐acting with a T1/2 of less than 12 hours.
• The non‐BZ agonists, commonly prescribed for insomnia, are often referred to as the “Z drugs” and include eszopiclone (Lunesta®), zalepon (Sonata®), & zolpidem (Ambien®).

4/9/2015
4
Rx Drug Epidemic: BZs & Z‐drugs 2.• The relationships between the
use of BZs & Z‐drugs & traffic accidents with & without injuries and fatalities have now been evaluated in several peer‐reviewed, meta‐analytic investigations & have concluded that the greatest associated accident risks are statistically associated with (1) the use of long and some intermediate and even short half‐life BZs; (2) the use of one Z‐drug (Lunesta® [eszopiclone]); (3) increasing dosages of any BZ; & (4) the first few weeks of use of BZs.
• Ref: Thomas RE. Benzodiazepine use and motor vehicle accidents: Systematic review of reported association. Can Fam Phys 1998; 44: 799‐808.
The abuse of BZs by types taken
Rx Drug Epidemic: BZs & Driving• In a 2010 meta‐analysis of 66
epidemiological studies, Smink and co‐investigators demonstrated that benzodiazepines were associated with impaired driving skills and increased accident risks, & the greatest accident risks were associated with the use of long‐acting benzodiazepines, such as diazepam and clonazepam.
• In another investigation designed to assess the presence of psychoactive substances detected in the blood samples of hospitalized and seriously injured drivers in Denmark, the most frequently detected medicinal drugs detected in blood included diazepam(4.4%), tramadol (3.2%), and clonazepam (3.0%).
• Ref: Smink BE, Egberts ACG, Lusthof KJ, et al. The relationship between benzodiazepine use and traffic accidents: A systematic literature review. CNS Drugs 2010; 24: 639‐53.
Rx Drug Epidemic: The Classes of BZs
The BZs By classes & generic names
Trade names®
T1/2 (hours) Extra T1/2 Imposed by metabolites
Recommended use by vehiculardrivers
Long half‐life BZs:Chlor‐diazepoxide ClorazepateDiazepamFlurazepam
Librium®
Tranxene®Valium® Dalmane®
5‐3030‐10020‐802‐3
36‐20036‐10040‐12047‐100
RESTRICTEDRESTRICTEDRESTRICTEDRESTRICTED
Intermediate half‐life BZs:
AlprazolamClonazepamLorazepam
Xanax®Klonopin®Ativan®
9‐2018‐5010‐20
NANANA
RESTRICTEDRESTRICTEDRESTRICTED
Short half‐life BZs:Oxazepam Temazepam
Serax® Restoril®
5‐158‐22
NANA
RESTRICTEDRESTRICTED

4/9/2015
5
Rx Drug Epidemic: The Z‐drugs
The Z‐drugs Generic names
Trade names®
T1/2 (hours)
Extra T1/2 Imposed by metabolites
Recommended use by
vehiculardrivers
Eszopiclone Lunesta® 2‐6 NA RESTRICTEDZalepon Sonata® 2‐6 NA ACCEPTABLE
(under review)Zopiclone (Canada only)
Imovane® 2‐6 NA RESTRICTED
Zolpidem Ambien® 2‐6 NA ACCEPTABLE(under review)
Rx Drug Epidemic: Acceptable Drugs to Treat Anxiety &/or Insomnia in Transportation Workers
Drug classes Generic names(Trade ®)
Half‐life (hrs.)
Dose (mg po hs)
SleepEfficacy
AnxietyEfficacy
Herbal supplement
Valerian(Alluna®)
3.5 hrs. 2 tabs po hs = 400‐900 mg valerian
extract po hs
X
Neuro‐transmittingprodrug
Melatonin(Generic only)
30 min.‐2 hrs.
0.5‐5 mg po hs X
Tricyclic anti‐depressant
Doxepin(Sinequan®)
8‐24 hrs. (Mean = 17 hrs.)
6 mg po hs X X
Tetracyclicanti‐depressant
Trazodone(Desyrel®)
4‐9 hrs. 50‐150 mg po hs X X
SSRI Escitalopram
(Lexapro®)
27‐32
hrs.
10‐20 mg po hs X X
Rx Drug Epidemic: Opioid Agonists 1.• Transdermal fentanyl systems should
only be prescribed in opioid‐tolerant patients with severe chronic pain, e.g. cancer pain.
• Opioid‐tolerant patients are defined as those who require daily doses of opioids for longer than 1 week with the following minimal daily dosages of the most commonly prescribed opioids alone or in combination with NSAIDs: (1) 30‐67 mg of morphine daily; (2) 30 mg of hydrocodone daily; or (3) 8 mg of hydromorphone daily.
• Chronic pain is defined as pain that requires management with continuous, high‐dose opioid administration for prolonged periods & cannot be adequately controlled by non‐steroid anti‐inflammatory drugs (NSAIDs) & immediate release opioids, opioid combinations (oxycodone & hydrocodone + acetaminophen combinations)

4/9/2015
6
Rx Drug Epidemic: Opioid Agonists 2.• Since 2005, several manufacturer
recalls of transdermal fentanyl patches have been issued because of excessive leakage of fentanyl citrate across the delivery membrane resulting in life‐threatening respiratory depression and death despite proper prescription practices.
• FDA has issued the following advisories on the safe use of fentanyl patches as a result of increasing reports of deaths and life‐threatening adverse events: (1) sudden severe respiratory depression may occur during treatment even under medical supervision; (2) respiratory depression can be potentiated by other hypnotic‐sedatives, including alcohol; (3) patches should only be prescribed for opioid‐tolerant patients; (4) opioid‐tolerant patients may not manifest the most important early warning signs of impending respiratory depression.
Rx Drug Epidemic: Opioid Agonists 3.• Transportation workers who are wearers
of fentanyl patches at any dose delivery concentration will be considered opioid‐dependent & may not return to work for 3 months after medically supervised weaning off fentanyl patches.
• Should chronic pain refractory to NSAIDs and/or opioid dependence require treatment after cessation of fentanyl patch use, employees performing safety sensitive jobs may return to work and may be treated with sublingual buprenorphine‐naloxone (Suboxone®) 3 months after medically supervised weaning off fentanyl patches.
• Transportation workers who are either current wearers of fentanyl patches or have worn fentanyl patches within 3 months will be considered ineligible for commercial drivers’ licenses (CDLs).
Fentanyl transdermal patches
Rx Drug Epidemic: Opioid Agonists/Tramadol 1.• In low back & osteoarthritic joint
pain, recent studies have compared the effectiveness of NSAIDs (celicoxib, 200 mg po bid) v. tramadol (50 mg po qid) in the management of flare‐ups & have found celicoxib to be a more effective analgesic with fewer adverse effects than tramadol.
• Physical dependence on tramadol occurs as quickly as 3 months after use of the maximum dose of ≤ 400 mg/day.
• The independent risk factors for tramadol‐associated seizures have now been studied and include the following: (1) male gender; (2) age range 25‐54 years; (3) 4 or more prescriptions for tramadol; (4) pre‐existing seizure disorder; (5) prior stroke or head injury, and (6) any history of alcohol abuse.

4/9/2015
7
Rx Drug Epidemic: Opioid Agonists/Tramadol 2.
• Seizure activity may occur during tramadol therapy or during tramadol withdrawal at any time and is independent of the dose of tramadol taken.
• Grand mal, tonic‐clonic seizure activity may occur at low to therapeutic doses (100‐400 mg orally) and with excessive single oral (> 400 mg) or intravenous (300‐400 mg) doses.
• Tremors, muscle contractions, systemic shock‐like activity, and seizure activity are not uncommon within 12‐24 hours of tramadol withdrawal in dependent patients.
References:• Barsotti CE, Mycyk MB, Reyes J.
Withdrawal syndrome from tramadol hydrochloride. Am J Emerg Med 2003; 21: 87‐8.
• Talaie H, Panahandeh R, Fayaznouri M, et al. Dose‐independent occurrence of seizure with tramadol. J Med Toxicol 2009; 5: 63‐7.
• Gardner JS, Blough D, Drinkard CR, et al. Tramadol and seizures: a surveillance study in a managed care population. Pharmacotherapy 2000; 24: 1423‐31.
Rx Drug Epidemic: Opioid Agonists/Tramadol 3.• Tramadol can both release serotonin &
block the reuptake of serotonin & norepinephrine (venlafaxine‐like activity) & cause a potentially lethal serotonin syndrome if co‐administered with either selective serotonin reuptake inhibitors (SSRIs) or serotonin & norepinephrine reuptake inhibitors (SNRIs).
• The serotonin syndrome is characterized by agitation, confusion, shivering, sweating myoclonus, hyperreflexia, tachycardia, hyperpyrexia, “lead‐pipe” muscle rigidity, seizure activity, rhabdomyolysis, & metabolic acidosis.
• The serotonin syndrome has been repeatedly described in patients on tramadol and SSRI or SNRI therapy for chronic pain & depression, which frequently coexist, and can be fatal.
• Ref: Talaie H, Panahandeh R, Fayaznouri M, et al. Dose‐independent occurrence of seizure with tramadol. J Med Toxicol 2009; 5: 63‐7.
• Gardner JS, Blough D, Drinkard CR, et al. Tramadol and seizures: a surveillance study in a managed care population. Pharmacotherapy 2000; 24: 1423‐31.
Recommendations:
• Employees in safety‐sensitive positions should not be prescribed tramadol due to the low, but real risk of seizures.
• Employees may be weaned from tramadol during monitored weaning as delayed onset of seizures is possible & current recommendations have advised slow, tapered weaning to prevent the tramadol withdrawal syndrome.
• Following successful withdrawal from tramadol therapy, employees in safety sensitive positions should not pose significant risks to themselves, or to others, or require any work restrictions in order to perform their jobs.
Rx Drug Epidemic: Opioid Agonists + Antagonists 1.Buprenorphine is an opioid agonist‐antagonist, which has long been used as an effective analgesic with little to no respiratory depression but with dependency potential in several preparations including: (1) a parenteral preparation (Buprenex®) to treat acute postsurgical pain; (2) an old oralprep (Subutex®) to treat subacute & chronic pain; (3) a transdermalprep (Butrans®); (4) a trans‐mucosal prep that dissolves in the mouth; & (5) a sublingual prep combined with the opioid‐antagonist naloxone (Suboxone®) to treat opioid addiction in opioid agonist‐antagonist therapy replacing opioid substitution.
Butrans® transdermal patch: 5, 10, 20 mcg/hr.; induction 5 mg/hr., maintenance range 5‐20 mcg/hr.
4/9/2015
8
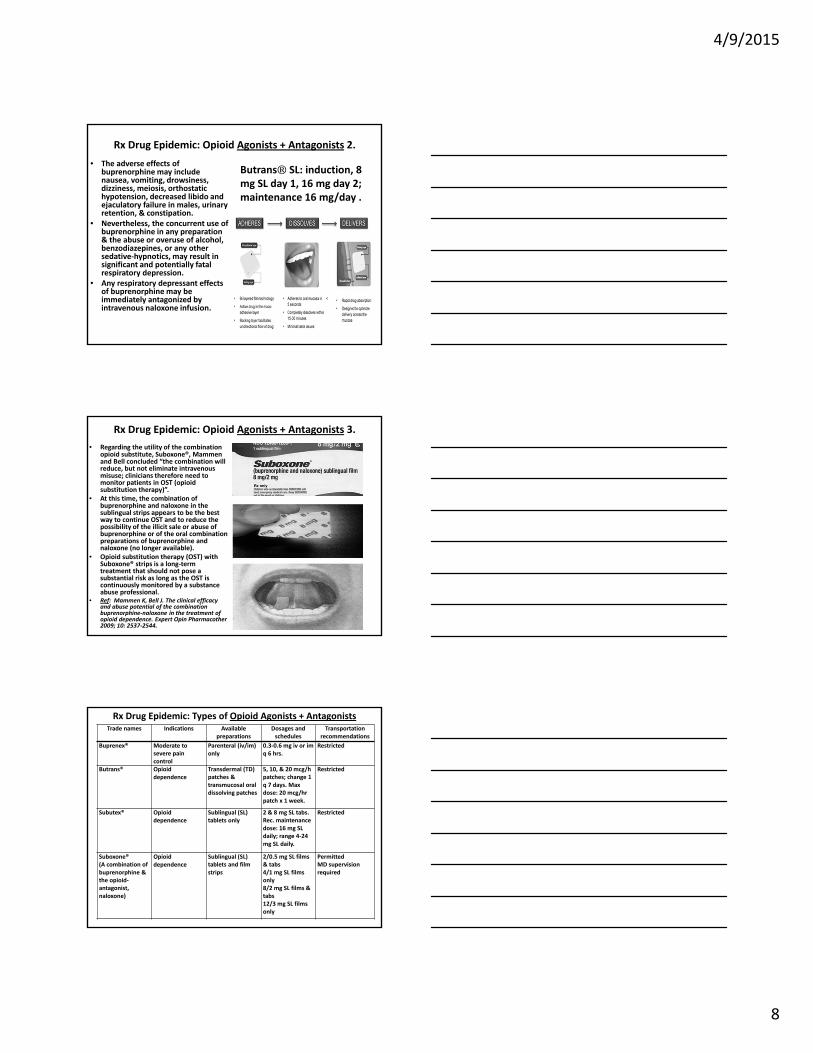
Rx Drug Epidemic: Opioid Agonists + Antagonists 2.
• The adverse effects of buprenorphine may include nausea, vomiting, drowsiness, dizziness, meiosis, orthostatic hypotension, decreased libido and ejaculatory failure in males, urinary retention, & constipation.
• Nevertheless, the concurrent use of buprenorphine in any preparation & the abuse or overuse of alcohol, benzodiazepines, or any other sedative‐hypnotics, may result in significant and potentially fatal respiratory depression.
• Any respiratory depressant effects of buprenorphine may be immediately antagonized by intravenous naloxone infusion.
Butrans® SL: induction, 8 mg SL day 1, 16 mg day 2; maintenance 16 mg/day .
Rx Drug Epidemic: Opioid Agonists + Antagonists 3.
• Regarding the utility of the combination opioid substitute, Suboxone®, Mammen and Bell concluded “the combination will reduce, but not eliminate intravenous misuse; clinicians therefore need to monitor patients in OST (opioid substitution therapy)”.
• At this time, the combination of buprenorphine and naloxone in the sublingual strips appears to be the best way to continue OST and to reduce the possibility of the illicit sale or abuse of buprenorphine or of the oral combination preparations of buprenorphine and naloxone (no longer available).
• Opioid substitution therapy (OST) with Suboxone® strips is a long‐term treatment that should not pose a substantial risk as long as the OST is continuously monitored by a substance abuse professional.
• Ref: Mammen K, Bell J. The clinical efficacy and abuse potential of the combination buprenorphine‐naloxone in the treatment of opioid dependence. Expert Opin Pharmacother 2009; 10: 2537‐2544.
Rx Drug Epidemic: Types of Opioid Agonists + Antagonists Trade names Indications Available
preparations Dosages and schedules
Transportationrecommendations
Buprenex® Moderate to severe pain control
Parenteral (iv/im) only
0.3‐0.6 mg iv or im q 6 hrs.
Restricted
Butrans® Opioid dependence
Transdermal (TD) patches & transmucosal oral dissolving patches
5, 10, & 20 mcg/h patches; change 1 q 7 days. Max dose: 20 mcg/hr patch x 1 week.
Restricted
Subutex® Opioid dependence
Sublingual (SL) tablets only
2 & 8 mg SL tabs. Rec. maintenance dose: 16 mg SL daily; range 4‐24 mg SL daily.
Restricted
Suboxone® (A combination of buprenorphine & the opioid‐antagonist, naloxone)
Opioid dependence
Sublingual (SL) tablets and film strips
2/0.5 mg SL films & tabs4/1 mg SL films only8/2 mg SL films & tabs12/3 mg SL films only
Permitted MD supervision required
4/9/2015
9
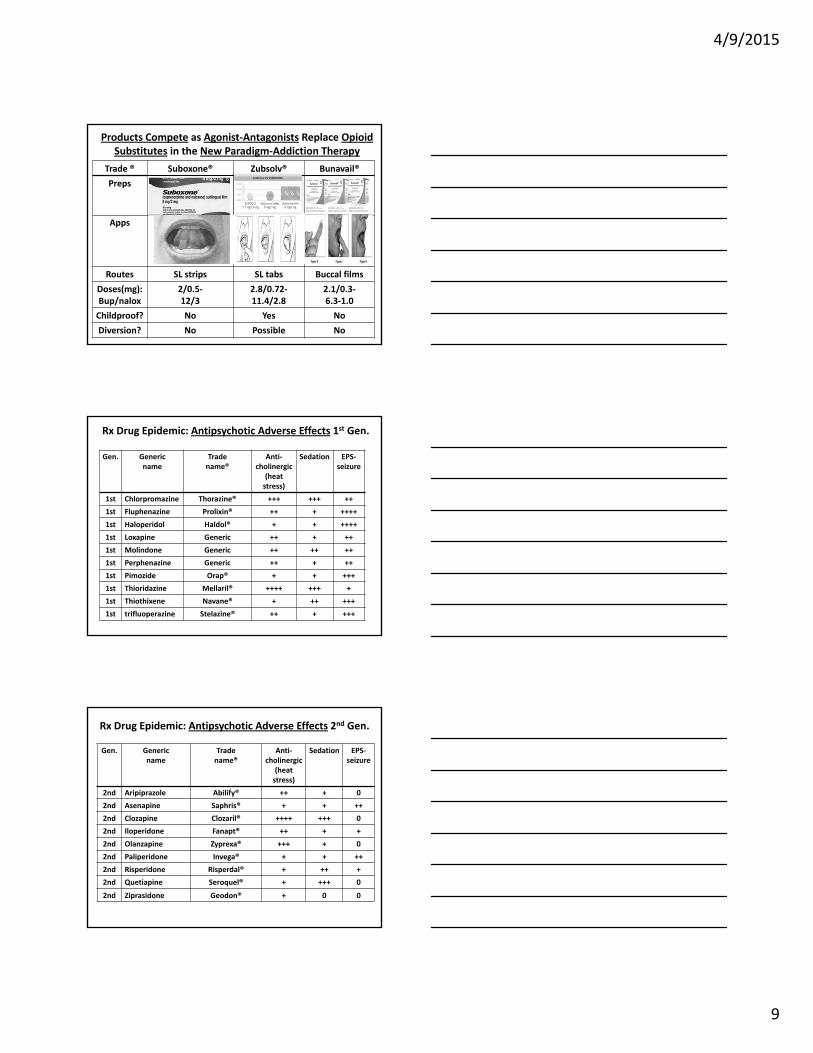
Products Compete as Agonist‐Antagonists Replace OpioidSubstitutes in the New Paradigm‐Addiction Therapy
Trade ® Suboxone® Zubsolv® Bunavail®
Preps
Apps
Routes SL strips SL tabs Buccal films
Doses(mg):Bup/nalox
2/0.5‐12/3
2.8/0.72‐11.4/2.8
2.1/0.3‐6.3‐1.0
Childproof? No Yes No
Diversion? No Possible No
Rx Drug Epidemic: Antipsychotic Adverse Effects 1st Gen.
Gen. Generic name
Trade name®
Anti‐cholinergic
(heatstress)
Sedation EPS‐seizure
1st Chlorpromazine Thorazine® +++ +++ ++
1st Fluphenazine Prolixin® ++ + ++++
1st Haloperidol Haldol® + + ++++
1st Loxapine Generic ++ + ++
1st Molindone Generic ++ ++ ++
1st Perphenazine Generic ++ + ++
1st Pimozide Orap® + + +++
1st Thioridazine Mellaril® ++++ +++ +
1st Thiothixene Navane® + ++ +++
1st trifluoperazine Stelazine® ++ + +++
Rx Drug Epidemic: Antipsychotic Adverse Effects 2nd Gen.
Gen. Generic name
Trade name®
Anti‐cholinergic
(heatstress)
Sedation EPS‐seizure
2nd Aripiprazole Abilify® ++ + 0
2nd Asenapine Saphris® + + ++
2nd Clozapine Clozaril® ++++ +++ 0
2nd Iloperidone Fanapt® ++ + +
2nd Olanzapine Zyprexa® +++ + 0
2nd Paliperidone Invega® + + ++
2nd Risperidone Risperdal® + ++ +
2nd Quetiapine Seroquel® + +++ 0
2nd Ziprasidone Geodon® + 0 0

4/9/2015
10
Rx Drug Epidemic: Lethal Combinations 1.• The combination of hydrocodone
(Vicodin®) and carisprodal (Soma®)is known to be highly addictive causing reported effects similar to heroin addiction.
• The withdrawal symptoms from the addiction are also significant and feature intense abdominal cramps and spasms which the patient frequently reported when either self‐withdrawing from her prescribed drugs or in drug rehab.
• Although Soma® is a non‐controlled muscle relaxant, its active metabolite, meprobamate, is a Class IV Controlled Substance.
• Ref: Reeves RR, Carter OS, Pinkofsky HB, Struve FA, Bennett DM. Carisprodal (Soma): abuse potential and physician unawareness. J Addictive Dis 1999; 18: 51‐56.
Rx Drug Epidemic: Lethal Combinations 2.• The US Drug Enforcement
Administration (DEA) is now monitoring reports of Soma® abuse and has recommended listing the drug under the US Controlled Substances Act.
• In 1984, Brooker and co‐authors reported the case of a 53‐year‐old man who developed significantly impaired brain function due to the combined abuse of meprobamate and diazepam. The interaction of these 2 drugs caused severe cognitive, memory, and motor function deficits.
• Ref: Brooker AE, Wiens AN, Wiens DA. Impaired brain function due to diazepam and meprobamate abuse in a 53‐year‐old male. J Nervous & Mental Dis 1984; 172: 498‐501.
Rx Drug Epidemic: Lethal Combinations 3.• Between 2003 and 2009, drug overdose
deaths in Florida from hydrocodone alone increased 34.9% and for other prescription drugs (including carisprodal/meprobamate) increased 141.6%. The US death rates from prescription drug overdoses has now exceeded the death rates from illicit drug overdoses, including cocaine and heroin overdoses.
• In 1999, Reeves and co‐authors reported the usage patterns of 40 patients who had taken Soma® for 3 or more months and compared 20 patients with a prior history of substance abuse with 20 patients with no history of substance abuse. Results demonstrated that some patients who used Soma® for 3 or more months were likely to abuse the medication, especially those with a history of prior substance abuse.
• Ref: Drug Overdose Deaths—Florida, 2003‐2009. MMWR Morb Mort Weekly Rep 2011; 60 (26): 869‐872.
• Reeves RR, Carter OS, Pinkofsky HB, Struve FA, Bennett DM. Carisprodal (Soma): abuse potential and physician unawareness. J Addictive Dis 1999; 18: 51‐56.

4/9/2015
11
Rx Drug Epidemic: Conclusions
Conclusions:1. Know the prescribed drugs.2. Know all of their adverse
effects alone & in interactions.
3. Know all predisposing factors for adverse effects alone & in interactions.
4. Implement early interventions based on urine drug tests.
5. Suggest acceptable alternatives to PCPs.
6. Recidivism is common; continue close restricted drug compliance monitoring.





























