Embed Size (px)
Citation preview

BIOS222
Pathology and Clinical Science 2 & 3
www.endeavour.edu.au
Session 26
Multi System Disorders 3
Bioscience Department

© Endeavour College of Natural Health www.endeavour.edu.au 2
Session Learning Outcomes
At the end of the session, you should be able to:
o Outline the risk factors and aetiology of hypertension
o Detail the impact of hypertension on the target organs
o Describe the diagnostic measures, complications and management of hypertension.
o Understand the triggers, clinical presentation, diagnosis and management of chronic fatigue syndrome
o Understand the aetiology, clinical features, diagnosis and management of SLE
o Discuss the aetiology, clinical features, diagnosis and management of Marfan’s syndome

© Endeavour College of Natural Health www.endeavour.edu.au 3
Session Plan
o Hypertension
o Chronic fatigue syndrome
o Systemic lupus erythematosus
o Marfan’s Disease

© Endeavour College of Natural Health www.endeavour.edu.au 4
Hypertension
Chronic fatigue syndrome
© Endeavour College of Natural Health www.endeavour.edu.au 5
Hypertension
o Definition: Hypertension is a condition in which arterial
BP is chronically elevated. BP occurs within a
continuous range, so cut-off levels are defined according
to their effect on patients' risk.
o Classification:
• Primary (essential) hypertension: It is the term applied
to 95% of cases in which no cause for hypertension
can be identified.
• Secondary hypertension: The elevation of blood
pressure results from an identifiable underlying
secondary cause, such as kidney or endocrine
disease.

© Endeavour College of Natural Health www.endeavour.edu.au 6
Hypertension
o Risk factors for primary hypertension
• Family history
• Age
• Race
• Insulin resistance and hyperinsulinemia
• A high salt intake,
• Heavy consumption of alcohol
• Obesity,
• Lack of exercise
• Impaired intrauterine growth

© Endeavour College of Natural Health www.endeavour.edu.au 7
Hypertensiono Aetiology for secondary hypertension:
• Pregnancy (pre-eclampsia)
• Renal disease
• Endocrine disease
• Drugs
• Coarctation of the aorta
o Clinical features:
• Asymptomatic initially
• Long term hypertension leads to target organ
damage: Blood vessels, central nervous system,
heart, kidney and retina

© Endeavour College of Natural Health www.endeavour.edu.au 8
Hypertension
o Target organ damage:
• Blood vessels:
– Dilation of vessels due to smooth muscle atrophy
– Hyaline arteriosclerosis in the smaller arteries
• Heart:
– Left ventricular hypertrophy
– Angina or prior myocardial infarction
– Prior coronary revascularization
– Heart failure

© Endeavour College of Natural Health www.endeavour.edu.au 9
Hypertension
o Target organ damage:
• CNS:
– Stroke, Carotid atheroma and TIA
– Subarachnoid haemorrhage, papilloedema
• Retina:
– ‘Cotton wool’ exudates with retinal ischaemia or
infarction
– Central retinal vein thrombosis
• Kidneys:
– Proteinuria and progressive renal failure

© Endeavour College of Natural Health www.endeavour.edu.au 10
Hypertension
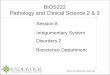
Hypertensive retinopathy showing
swollen optic disc, retinal
haemorrhages and multiple cotton
wool spots (infarcts)
Central retinal vein thrombosis
showing swollen optic disc and
widespread fundal
haemorrhage, commonly
associated with systemic
hypertension.

© Endeavour College of Natural Health www.endeavour.edu.au 11
Hypertension
o Diagnosis:
• Urinalysis: for blood, protein and glucose
• Blood urea, electrolytes and creatinine
• Blood glucose
• Serum total and HDL cholesterol
• Thyroid function tests
• 12-lead ECG for left ventricular hypertrophy,
coronary artery disease

© Endeavour College of Natural Health www.endeavour.edu.au 12
Hypertensiono Complications:
o Malignant’ or ‘accelerated’ phase hypertension:
• Accelerated microvascular damage
• Necrosis in the walls of small arteries and
arterioles
• Intravascular thrombosis
• Rapidly progressive end organ damage
• retinopathy (grade 3 or 4), renal dysfunction (especially
proteinuria) and/or hypertensive encephalopathy
• Left ventricular failure
• Death

© Endeavour College of Natural Health www.endeavour.edu.au 13
Hypertensiono Management:
• Non-drug therapy
– Weight loss
– Reduction of alcohol and smoking
– Increase exercise
• Antihypertensive drugs
– Diuretics and Beta-blockers
– ACE inhibitors
– Angiotensin receptor blockers
– Calcium channel antagonists

© Endeavour College of Natural Health www.endeavour.edu.au 14
Chronic Fatigue Syndrome
o Definition: It is characterised by excessive fatigue after
minimal physical or mental exertion, poor concentration,
dizziness, muscular aches and sleep disturbance.
o Triggering factors:
• Viral infection
• Immune disorders
• Stress
• Trauma
• Toxins

© Endeavour College of Natural Health www.endeavour.edu.au 15
Chronic Fatigue Syndrome
o Clinical features: The fatigue of CFS is accompanied by
below characteristic illness symptoms lasting at least 6
months.
• Increased malaise following physical activity or
mental exertion
• Problems with sleep
• Difficulties with memory and concentration
• Persistent muscle pain
• Joint pain (without redness or swelling)
• Headache
• Tender lymph nodes in the neck or armpit
• Sore throat
© Endeavour College of Natural Health www.endeavour.edu.au 16
Chronic Fatigue Syndromeo Diagnosis:
• Clinical symptoms
• A detailed medical history
• Physical and mental status examination
• Laboratory screening tests
o Management:
• Rest
• Education
• Emotional support
• Treatment of symptoms
• Overall management of general health

© Endeavour College of Natural Health www.endeavour.edu.au 17
Systemic Lupus Erythematosus
Marfan’s Disease

© Endeavour College of Natural Health www.endeavour.edu.au 18
Systemic Lupus Erythematosus
(SLE)o Definition: SLE is a chronic inflammatory disease that
can affect virtually any organ system, including the
musculoskeletal system.
o Aetiology:
• Autoimmune attack
• Genetic factors
• Environmental factors
© Endeavour College of Natural Health www.endeavour.edu.au 19
Systemic Lupus Erythematosus
(SLE)o Clinical features:
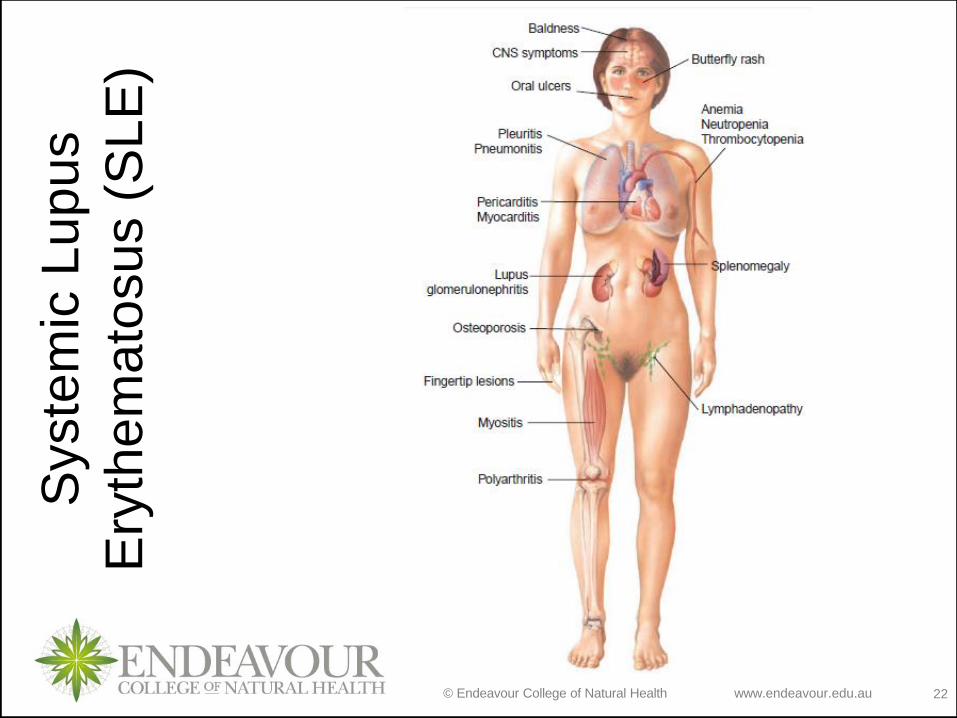
• Musculoskeletal system: Arthralgias and polyarthritis,
tenosynovitis, rupture of the intrapatellar and Achilles
tendons, and avascular necrosis
• Skin: Malar or “butterfly” rash on the nose and
cheeks, hives, discoid rash, periungual erythema, nail
fold infarcts, and splinter hemorrhages, Hair loss,
Sun sensitivity
• Gastrointestinal: Mouth ulcers, Mesenteric vasculitis
with abdominal pain, bowel infarction or perforation
© Endeavour College of Natural Health www.endeavour.edu.au 20
Systemic Lupus Erythematosus
(SLE)o Clinical features: (cont.)
• Cardiovascular system: Pericarditis, myocarditis,
hypertension, Ischemic heart disease
• Lungs: pleural effusions or pleuritis
• Kidneys: Glomerulonephritis, Interstitial nephritis,
Nephrotic syndrome, proteinuria with resultant edema
in the legs and abdomen, and around the eyes
© Endeavour College of Natural Health www.endeavour.edu.au 21
Systemic Lupus Erythematosus
(SLE)o Clinical features: (cont.)
• Central nervous system: Strokes or hemorrhage,
seizures, depression and unnatural euphoria,
decreased cognitive functioning, confusion, and
altered consciousness
• Haematological system: hemolytic anaemia,
leukopenia, lymphopenia, or thrombocytopenia,
Lymphadenopathy, Raynaud’s phenomenon
© Endeavour College of Natural Health www.endeavour.edu.au 22
Syste
mic
Lupus
Ery
them
ato
sus (
SLE
)

© Endeavour College of Natural Health www.endeavour.edu.au 23
Systemic Lupus Erythematosus
(SLE)
Severe secondary Raynaud’s phenomenon leading to
digital ulceration

© Endeavour College of Natural Health www.endeavour.edu.au 24
Systemic Lupus Erythematosus
(SLE)
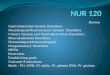
Butterfly (malar) rash of systemic
lupus erythematosus, sparing the
nasolabial folds

© Endeavour College of Natural Health www.endeavour.edu.au 25
SLE
o Diagnosis:
• Complete history, Physical examination
• Analysis of blood:
• RBC, WBC, Platelet count,
• ESR, CRP
• Autoantibodies: ANA
• Clinical criteria

© Endeavour College of Natural Health www.endeavour.edu.au 26
SL
E

© Endeavour College of Natural Health www.endeavour.edu.au 27
SLE
o Management:
• Avoid sun and UV light exposure and to employ sun
blocks
• Analgesics
• NSAIDs
• Hydroxychloroquine
• Corticosteroids
• Immunosuppressants

© Endeavour College of Natural Health www.endeavour.edu.au 28
Marfan’s Syndrome
o Definition: This is a disorder of connective tissue
inherited as an autosomal dominant trait
o Aetiology:
• Genetic mutation: fibrillin gene on chromosome 15.

© Endeavour College of Natural Health www.endeavour.edu.au 29
Marfan’s Syndrome
o Clinical features:
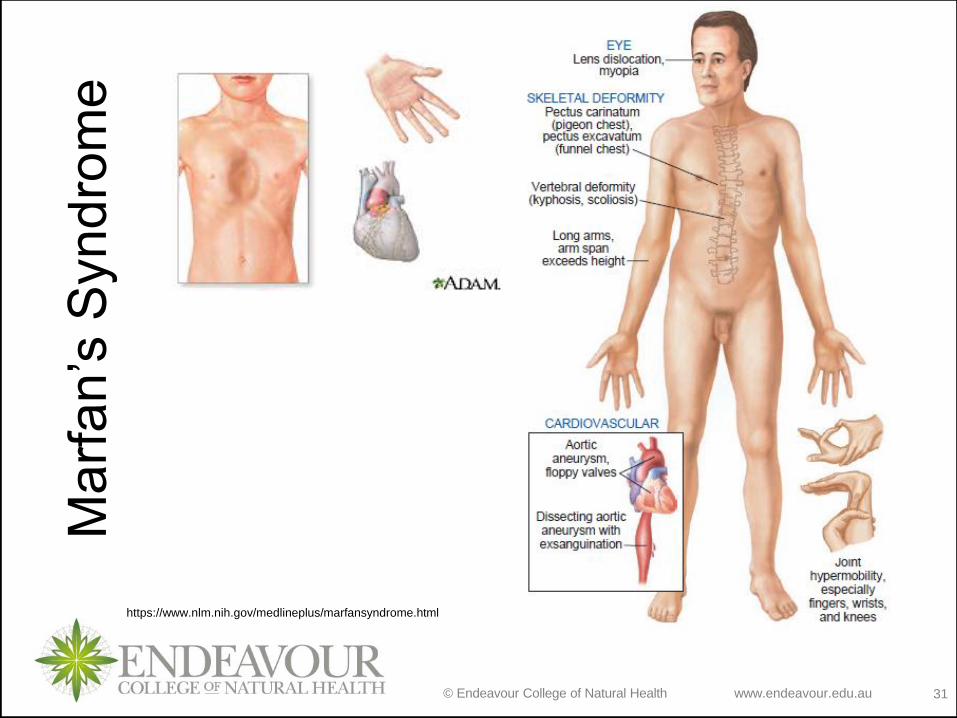
• Skeletal deformities: a long, thin body with
exceptionally long extremities spider fingers,
hyperextensible joints, kyphosis, and scoliosis
• Chest deformities: pectus excavatum, pigeon chest
deformity
© Endeavour College of Natural Health www.endeavour.edu.au 30
Marfan’s Syndrome
o Clinical features:
• Eye disorders: Bilateral dislocation of the lens,
Myopia and predisposition to retinal detachment
• Cardiovascular defects: mitral valve prolapse,
progressive dilation of the aortic valve ring, and
weakness of the aorta and other arteries. Dissection
and rupture of the aorta, premature death.
© Endeavour College of Natural Health www.endeavour.edu.au 31
Ma
rfa
n’s
Syn
dro
me
https://www.nlm.nih.gov/medlineplus/marfansyndrome.html

© Endeavour College of Natural Health www.endeavour.edu.au
32
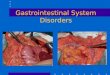
Marfan’s Syndrome
o Arachnodactyly (“spider fingers”)
Image courtesy of Prof. Vardaxis.
Endeavour College

© Endeavour College of Natural Health www.endeavour.edu.au
33
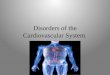
Marfan’s
Syndrome
Dissecting
aneurysm of the
aorta
Image courtesy of Prof. Vardaxis.
Endeavour College

© Endeavour College of Natural Health www.endeavour.edu.au
34
Marfan’s Syndrome
o CT scan of dissecting aneurysm of the aorta
Image courtesy of Prof. Vardaxis.
Endeavour College

© Endeavour College of Natural Health www.endeavour.edu.au
35
Marfan’s Syndrome
Subluxation of the lensImage courtesy of Prof. Vardaxis.
Endeavour College
© Endeavour College of Natural Health www.endeavour.edu.au 36
Marfan’s Syndrome
o Diagnosis:
• Major and minor diagnostic criteria that include
skeletal, cardiovascular, and ocular deformities
• Chest X-ray,
• Echocardiography
• MRI or CT scan

© Endeavour College of Natural Health www.endeavour.edu.au 37
Marfan’s Syndrome
o Management:
• No curative treatment
• β-blockers
• Elective replacement of the ascending aorta
• Pain medication and physiotherapy
• Genetic counseling

© Endeavour College of Natural Health www.endeavour.edu.au 38
Reading and Resourceso Crowley LV, 2012, An Introduction to Human Diseases – Pathology and
Pathophysiology Correlations, 9th edn, Jones and Bartlett Learning
o Grossman SC & Porth CM 2014, Porth’s Pathophysiology- Concepts of
Altered Health States, 9th edn. Wolters Kluwer Health - Lippincott, Williams
& Wilkins
o Hinson, J, Raven, P & Chew, S 2010, The endocrine system: basic science
and clinical conditions, 2nd edn, Churchill Livingstone Elsevier, Edinburgh
o Jamison, JR 2006, Differential diagnosis for primary care: a handbook for
health care practitioners, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh.
o Jarvis, C, 2012 Physical Examination & Health Assessment, 6th ed.,
Elsevier Saunders, Philadelphia.
o Kumar, P & Clark, M 2012, Kumar and Clark’s clinical medicine, 8th edn,
Saunders Elsevier, Edinburgh.
o Kumar, V, Abbas, AK & Aster, JC 2015, Robbins & Cotran pathologic basis
of disease, 9th edn, Elsevier Saunders, Philadelphia.

© Endeavour College of Natural Health www.endeavour.edu.au 39
Reading and Resourceso Lee, G & Bishop, P 2009, Microbiology and infection control for health
professionals, 4th edn, Pearson Education, Frenchs Forest, NSW.
o McCance, KL, Heuther, SE, & Brashers, VL 2014, Pathophysiology: the
biologic basis for disease in adults and children, 7th edn, Elsevier.
o Michael-Titus, A, Revest, P & Shortland, P 2010, The nervous system: basic
science and clinical conditions, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh
o Mosby’s dictionary of medicine, nursing and health professions 2013, 9th
edn, Elsevier, St. Louis, MO.
o Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology,
14th edn, John Wiley & Sons, Hoboken, NJ.
o VanMeter, KC & Hubert, RJ 2014, Gould's pathophysiology for the health
professions, 5th edn, Elsevier, St Louis, MO.
o Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014,
Davidson’s principles and practice of medicine, 22nd edn, Churchill
Livingstone Elsevier, Edinburgh.

© Endeavour College of Natural Health www.endeavour.edu.au 40
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.