Embed Size (px)
Citation preview
Prepared for the Foundation of the American College of Healthcare Executives
Session 101AB Not If, but When: Drug Diversion in
Hospitals
Presented by: Christopher Fortier, PharmD

1
Not if, but When: Drug Diversion in Hospitals
Christopher Fortier, PharmD, FASHPChief Pharmacy OfficerMassachusetts General HospitalBoston, MA
Disclosure of RelevantFinancial Relationships
The following faculty of this continuing education activity has no relevant financial relationships with commercial interests to disclose:
– Christopher Fortier
2
2
Faculty
• Christopher Fortier, PharmD, FASHP
3
Learning Objectives
• Outline the DEA’s new focus on drug diversion in hospitals
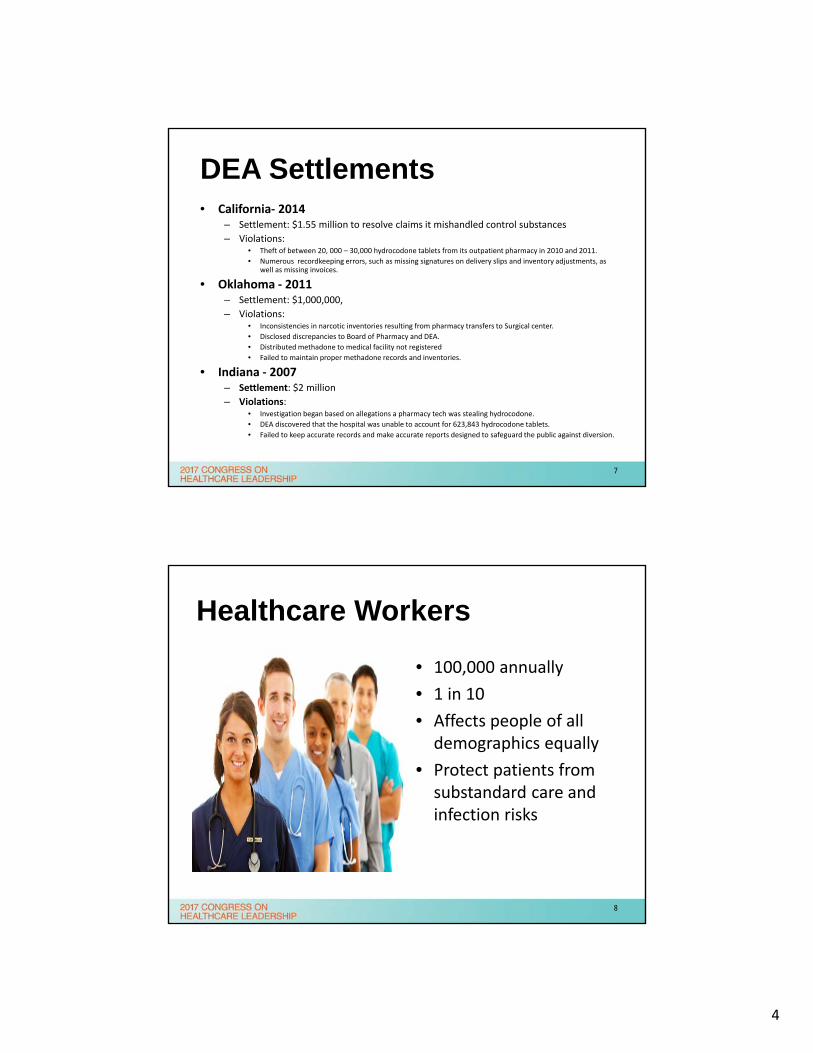
• Describe the various national hospital diversion headlines and data specific to healthcare provider drug abuse and the opioid crisis
• Discuss MGH’s 2-year DEA investigation experience and the results of a corrective action plan
• Share essential components and key strategies of a comprehensive and proactive drug diversion program
4
3
5
6
4
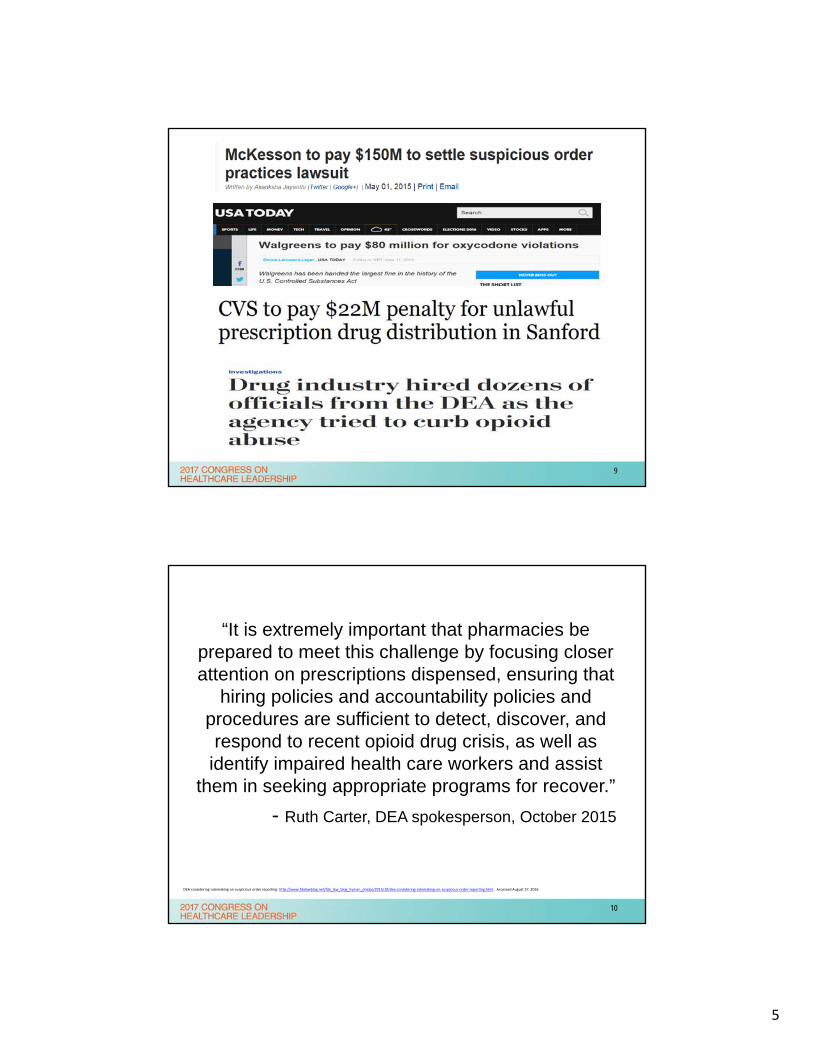
DEA Settlements• California‐ 2014
– Settlement: $1.55 million to resolve claims it mishandled control substances
– Violations: • Theft of between 20, 000 – 30,000 hydrocodone tablets from its outpatient pharmacy in 2010 and 2011.
• Numerous recordkeeping errors, such as missing signatures on delivery slips and inventory adjustments, as well as missing invoices.
• Oklahoma ‐ 2011– Settlement: $1,000,000,
– Violations:• Inconsistencies in narcotic inventories resulting from pharmacy transfers to Surgical center.
• Disclosed discrepancies to Board of Pharmacy and DEA.
• Distributed methadone to medical facility not registered
• Failed to maintain proper methadone records and inventories.
• Indiana ‐ 2007 – Settlement: $2 million
– Violations:• Investigation began based on allegations a pharmacy tech was stealing hydrocodone.
• DEA discovered that the hospital was unable to account for 623,843 hydrocodone tablets.
• Failed to keep accurate records and make accurate reports designed to safeguard the public against diversion.
7
Healthcare Workers
• 100,000 annually
• 1 in 10
• Affects people of all demographics equally
• Protect patients from substandard care and infection risks
8
5
9
“It is extremely important that pharmacies be prepared to meet this challenge by focusing closer attention on prescriptions dispensed, ensuring that
hiring policies and accountability policies and procedures are sufficient to detect, discover, and respond to recent opioid drug crisis, as well as
identify impaired health care workers and assist them in seeking appropriate programs for recover.”
- Ruth Carter, DEA spokesperson, October 2015
DEA considering rulemaking on suspicious order reporting. http://www.fdalawblog.net/fda_law_blog_hyman_phelps/2015/10/dea‐considering‐rulemaking‐on‐suspicious‐order‐reporting.html. Accessed August 27, 2016
10
6
11
Agenda
• The MGH Experience
• Top 10 critical components
• Managing a DEA investigation
• Organizational resources
• Questions
12
7
Strategic Priorities
Write down 5 strategic control substance diversion priorities that you plan to begin to
implement when you return to your organization
Share with the audience 2-3 of those strategic priorities
13
EXPERIENCETHE MGH
14
8
Mass General Hospital
• 1,000 bed academic medical center and clinics across Boston-metro area
• 2 million control substances dispensed annually– 2.3 ADM control substance transactions annually
• 30,000 employees– 2,400 physicians– 380 pharmacy employees– 3,800 nurses– 450 anesthesia providers
• Automation– 190 automated dispensing machines– 85 anesthesia workstations
15
DEA Violations at MGH
• Major nurse diversion
• Failure to report within timeframe
• No biennial inventory
• Not utilizing DEA 222 for off-site license transfer
• Unable to provide 2 years worth of readily-retrievable ADM records
16
9
MGH Corrective Action
• Employ a full time Drug Diversion Compliance Officer
• Establish a drug diversion team
• Conduct mandatory annual training for all staff
• Purchasing controlled substance surveillance software
• ADM’s having timed password-reset (90 days) and biometrics
• Requiring the MGH Department of Pharmacy to conduct daily operating room post case reconciliation of controlled substances dispensed, used or wasted.
• Requiring at least one nursing leader per clinical area to:
– Conduct weekly reviews of all controlled substance surveillance software anomalous usage reports for ADM’s in that clinical area
– Conduct daily M-F reviews of controlled substances dispensed from the ADM’s in that clinical area
17
MGH Corrective Action• Requiring clinical nursing supervisors to review certain ADM reports on
Saturdays, Sundays and holidays• Requiring Associate Chief Nurses to conduct monthly compliance
checks on their nursing leader direct reports• Requiring trend and pattern reports to be reviewed quarterly by the
DDTF• During each year of this CAP, MGH will conduct a self evaluation of all
its DEA registered facilities to review compliance with all requirements of the ACT
• MGH will maintain reports of disciplinary actions taken against employees found to have lost a significant quantity of controlled substances or found to have stolen or diverted controlled substances.
• MGH will complete biennial inventories of all of its DEA-registered facilities using physical counts (including all ADMs) witnessed by 2 individuals
18
10
MGH Corrective Action• MGH will take the following corrective actions in addition to the
enhanced controls:– MGH will hire external auditors to conduct unannounced audits
at all MGH facilities with active DEA registrations of 5 Schedule CII-V randomly chosen by the auditors.
– Each audit report will be reviewed and signed by the pharmacist in charge or the registrant’s DEA-designated person
– MGH will have 30 days to cure/resolve any deficiencies identified in the audit report and efforts to cure will be documented in the report
– If the auditors find any discrepancies/losses, MGH will send the audit report within 5 days of the end of the 30 day period
– MGH will maintain audit records and make them available for the DEA upon request for up to a 2 years after the CAP expires
19
MGH SUD Strategic Initiative
• Multidisciplinary inpatient consult team (ACT)• Post-discharge bridge clinic• Opioid task force• Recovery coaches• Enhanced community health center treatment• Education throughout MGH and broader
community• Research and evaluation• Culture change
20
11
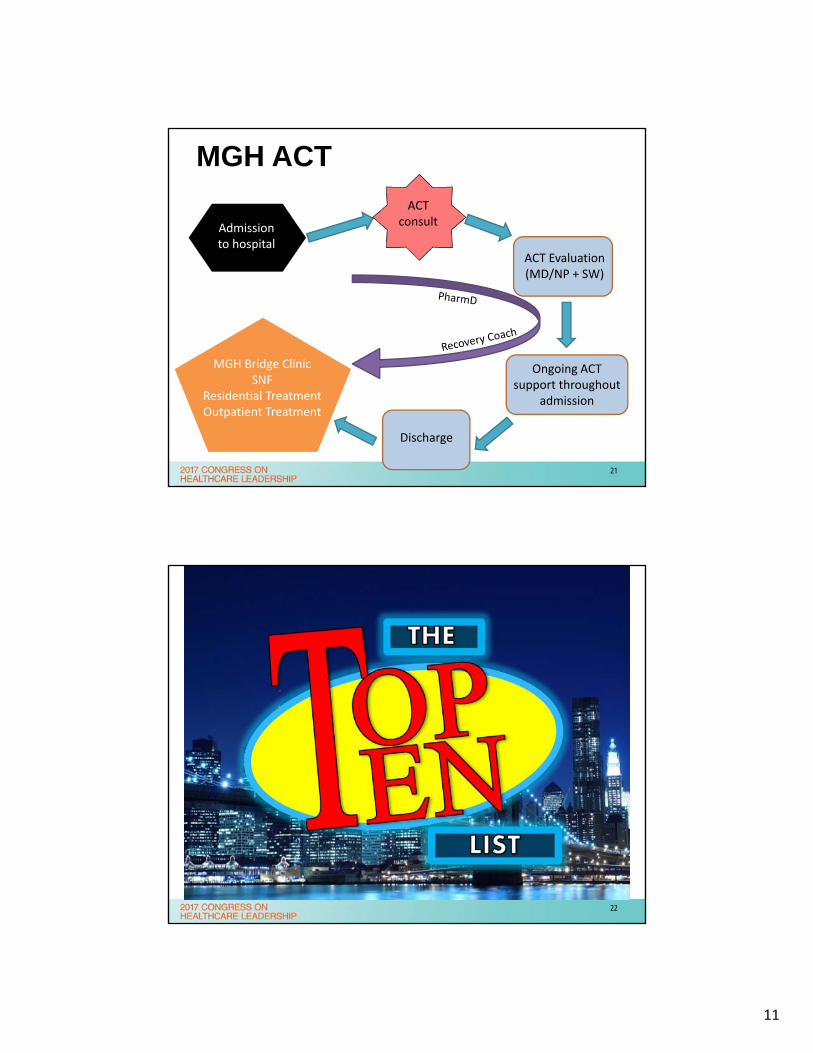
MGH ACT
Admission to hospital
ACT Evaluation (MD/NP + SW)
Ongoing ACT support throughout
admission
Discharge
MGH Bridge ClinicSNF
Residential TreatmentOutpatient Treatment
ACT consult
21
22
12
Top 10
1. Task force
2. Training
3. Surveillance
4. Investigation
5. Reporting
6. Auditing
7. Technology
8. Pharmacy controls
9. Human resources
10. Multidisciplinary
23
#1TASK FORCE
24
13
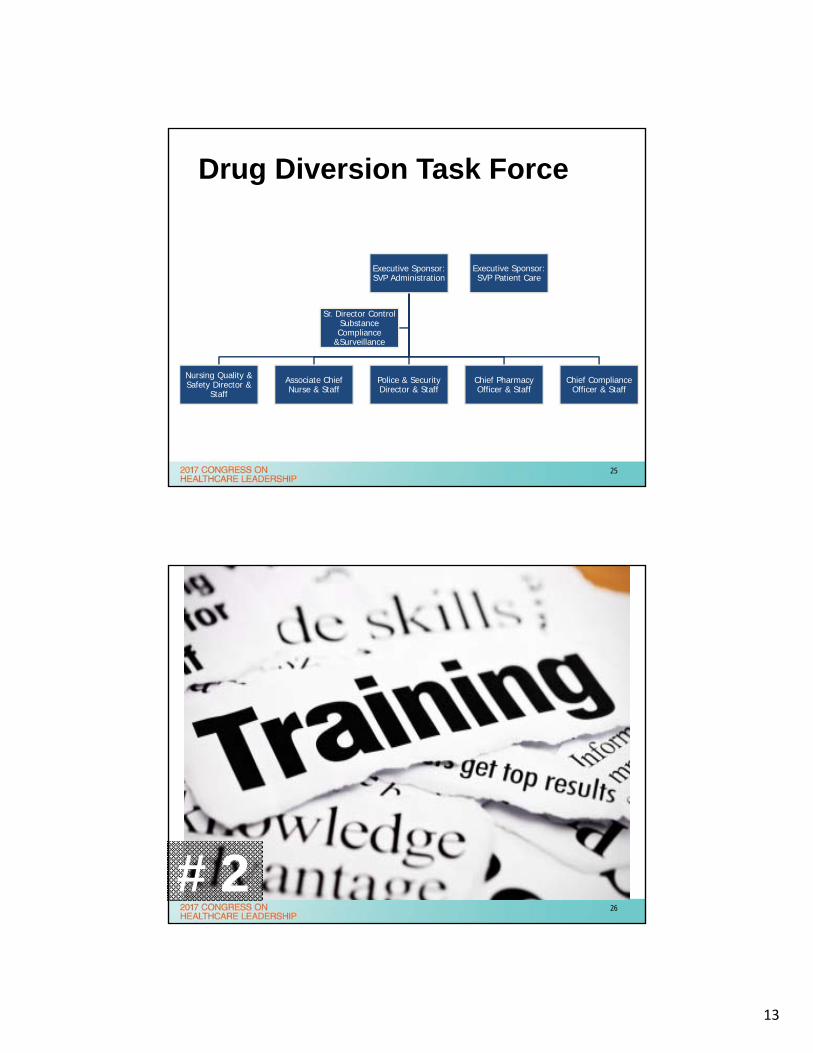
Drug Diversion Task Force
Executive Sponsor: SVP Administration
Nursing Quality & Safety Director &
Staff
Associate Chief Nurse & Staff
Police & Security Director & Staff
Chief Pharmacy Officer & Staff
Chief Compliance Officer & Staff
Sr. Director Control Substance Compliance
&Surveillance
Executive Sponsor: SVP Patient Care
25
• education
#226
14
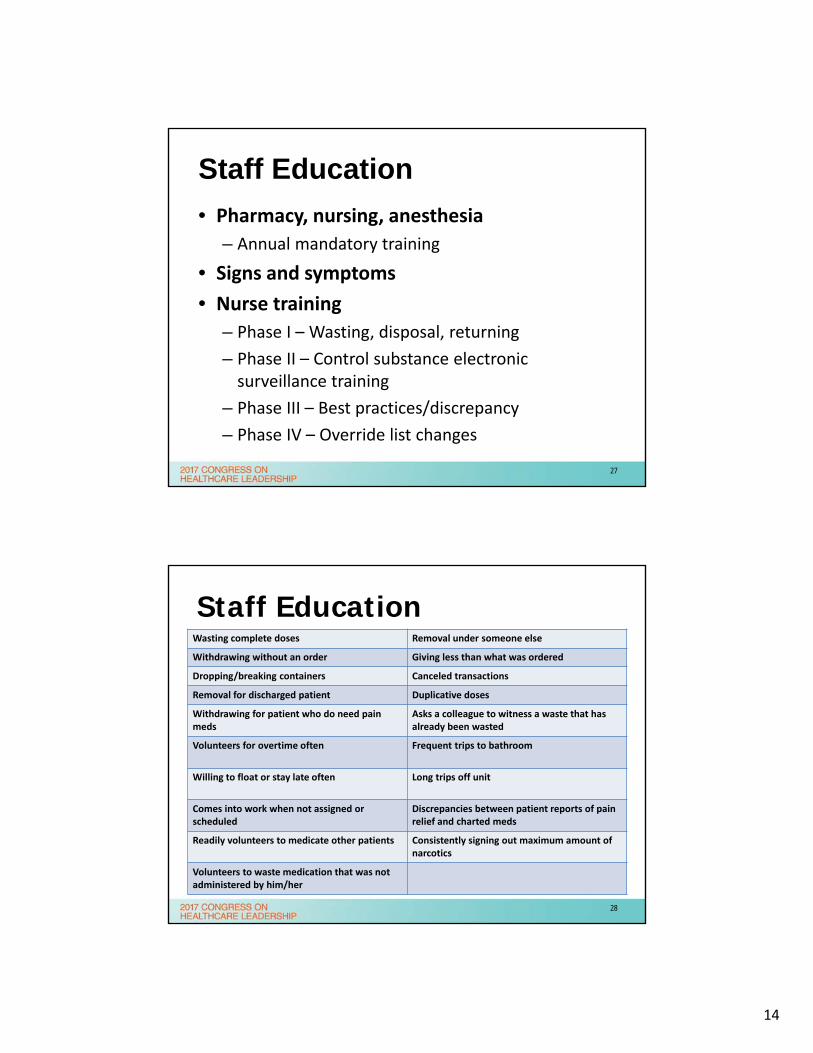
Staff Education
• Pharmacy, nursing, anesthesia
– Annual mandatory training
• Signs and symptoms
• Nurse training
– Phase I – Wasting, disposal, returning
– Phase II – Control substance electronic surveillance training
– Phase III – Best practices/discrepancy
– Phase IV – Override list changes
27
Staff EducationWasting complete doses Removal under someone else
Withdrawing without an order Giving less than what was ordered
Dropping/breaking containers Canceled transactions
Removal for discharged patient Duplicative doses
Withdrawing for patient who do need pain meds
Asks a colleague to witness a waste that has already been wasted
Volunteers for overtime often Frequent trips to bathroom
Willing to float or stay late often Long trips off unit
Comes into work when not assigned or scheduled
Discrepancies between patient reports of pain relief and charted meds
Readily volunteers to medicate other patients Consistently signing out maximum amount of narcotics
Volunteers to waste medication that was not administered by him/her
28
15
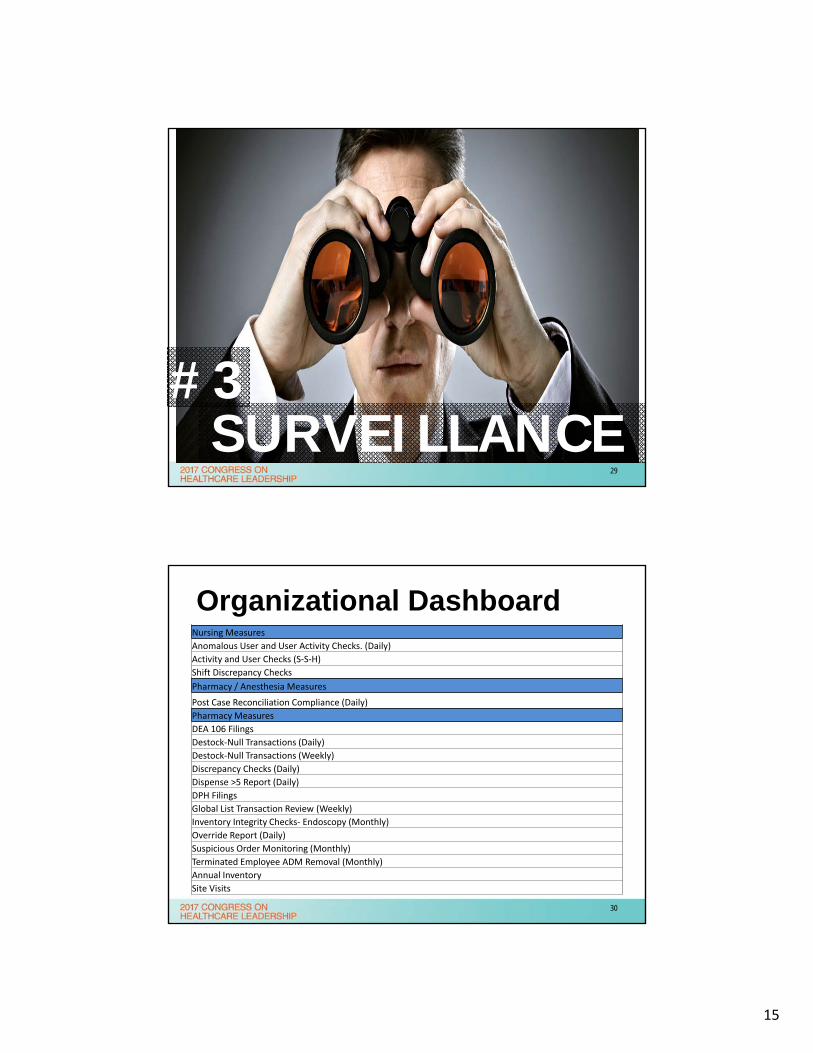
SURVEILLANCE#3
29
Organizational DashboardNursing Measures
Anomalous User and User Activity Checks. (Daily)
Activity and User Checks (S‐S‐H)
Shift Discrepancy Checks
Pharmacy / Anesthesia Measures
Post Case Reconciliation Compliance (Daily)
Pharmacy Measures
DEA 106 Filings
Destock‐Null Transactions (Daily)
Destock‐Null Transactions (Weekly)
Discrepancy Checks (Daily)
Dispense >5 Report (Daily)
DPH Filings
Global List Transaction Review (Weekly)
Inventory Integrity Checks‐ Endoscopy (Monthly)
Override Report (Daily)
Suspicious Order Monitoring (Monthly)
Terminated Employee ADM Removal (Monthly)
Annual Inventory
Site Visits
30
16
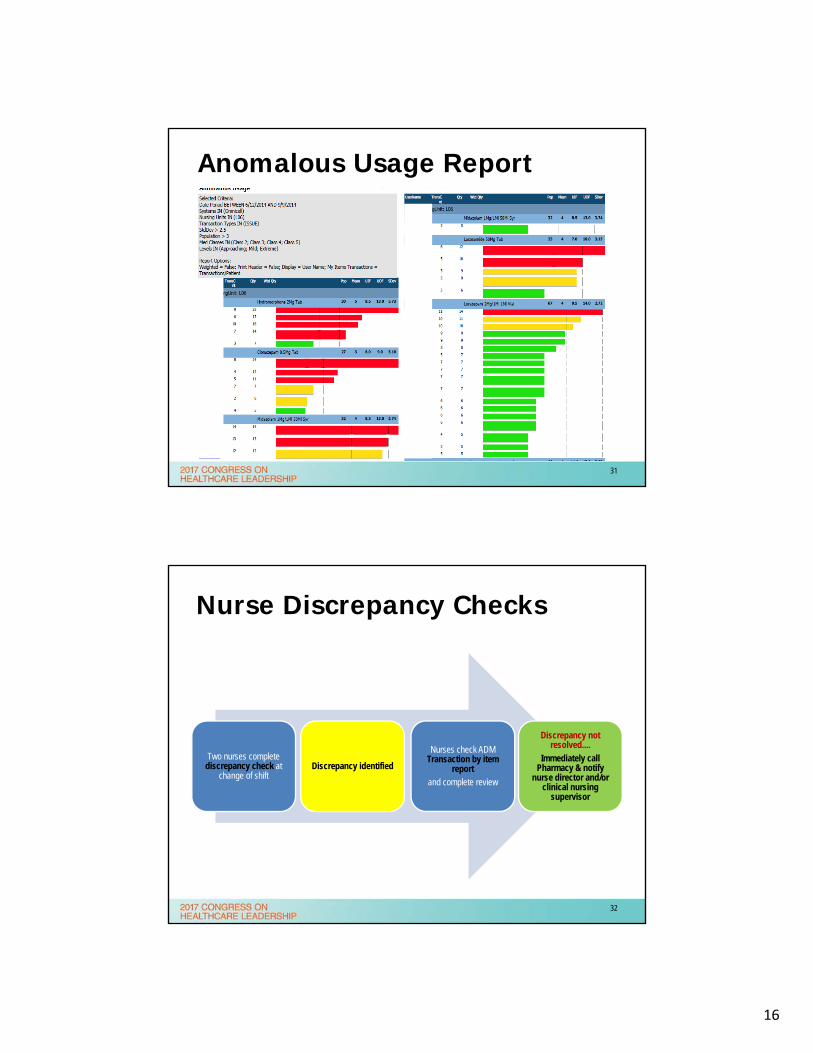
Anomalous Usage Report
31
Nurse Discrepancy Checks
Two nurses complete discrepancy check at
change of shiftDiscrepancy identified
Nurses check ADM Transaction by item
report and complete review
Discrepancy not resolved....
Immediately call Pharmacy & notify
nurse director and/or clinical nursing
supervisor
32
17
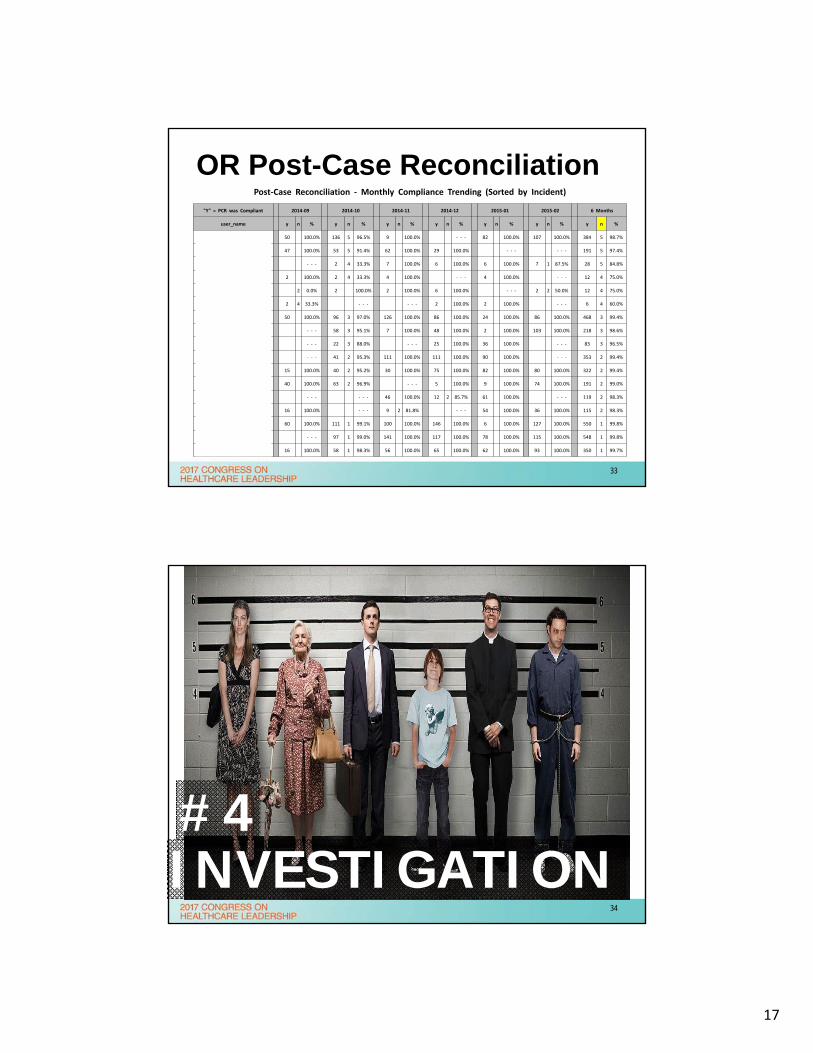
OR Post-Case ReconciliationPost‐Case Reconciliation ‐ Monthly Compliance Trending (Sorted by Incident)
"Y" = PCR was Compliant 2014‐09 2014‐10 2014‐11 2014‐12 2015‐01 2015‐02 6 Months
user_name y n % y n % y n % y n % y n % y n % y n %
Gelineau, Amanda Maria 50 100.0% 136 5 96.5% 9 100.0% ‐ ‐ ‐ 82 100.0% 107 100.0% 384 5 98.7%
Spencer, Rebecca 47 100.0% 53 5 91.4% 62 100.0% 29 100.0% ‐ ‐ ‐ ‐ ‐ ‐ 191 5 97.4%
Greenberg, Deborah ‐ ‐ ‐ 2 4 33.3% 7 100.0% 6 100.0% 6 100.0% 7 1 87.5% 28 5 84.8%
Levine, Amy 2 100.0% 2 4 33.3% 4 100.0% ‐ ‐ ‐ 4 100.0% ‐ ‐ ‐ 12 4 75.0%
Lighthall, Samantha 2 0.0% 2 100.0% 2 100.0% 6 100.0% ‐ ‐ ‐ 2 2 50.0% 12 4 75.0%
Holley, Catherine 2 4 33.3% ‐ ‐ ‐ ‐ ‐ ‐ 2 100.0% 2 100.0% ‐ ‐ ‐ 6 4 60.0%
Gao, Lei 50 100.0% 96 3 97.0% 126 100.0% 86 100.0% 24 100.0% 86 100.0% 468 3 99.4%
Walsh, Tomas ‐ ‐ ‐ 58 3 95.1% 7 100.0% 48 100.0% 2 100.0% 103 100.0% 218 3 98.6%
Sayal, Puneet ‐ ‐ ‐ 22 3 88.0% ‐ ‐ ‐ 25 100.0% 36 100.0% ‐ ‐ ‐ 83 3 96.5%
Bartels, David DB#2046 ‐ ‐ ‐ 41 2 95.3% 111 100.0% 111 100.0% 90 100.0% ‐ ‐ ‐ 353 2 99.4%
Norato, Christine 15 100.0% 40 2 95.2% 30 100.0% 75 100.0% 82 100.0% 80 100.0% 322 2 99.4%
Yelle,Marc 40 100.0% 63 2 96.9% ‐ ‐ ‐ 5 100.0% 9 100.0% 74 100.0% 191 2 99.0%
Kim, Peggy 1890 ‐ ‐ ‐ ‐ ‐ ‐ 46 100.0% 12 2 85.7% 61 100.0% ‐ ‐ ‐ 119 2 98.3%
Cox, Jessica #1975 16 100.0% ‐ ‐ ‐ 9 2 81.8% ‐ ‐ ‐ 54 100.0% 36 100.0% 115 2 98.3%
Vanneman, Matthew 60 100.0% 111 1 99.1% 100 100.0% 146 100.0% 6 100.0% 127 100.0% 550 1 99.8%
Safavi, Kyan DB#2044 ‐ ‐ ‐ 97 1 99.0% 141 100.0% 117 100.0% 78 100.0% 115 100.0% 548 1 99.8%
Dougherty, Kelly 16 100.0% 58 1 98.3% 56 100.0% 65 100.0% 62 100.0% 93 100.0% 350 1 99.7%
33
http://premium.wpmudev.org/blog/wp-content/uploads/2012/07/user-logging-lineup.jpg• investigation
INVESTIGATION#4
34
18
Investigation
• Diversion Response Team
– Pharmacy, nursing, police & security, occupational health, HR, employee assistance
• Data collection time period
– 3‐6 months, 1‐2 year, depends on scenario
• Police & Security interview
• Drug screen
• Reporting to local police?
35
• reporting
REPORTING#5
36
19
Reporting
• Utilize organizational safety report system to file loss– Rule of Thumb: < or >5
• Regulatory filings– DPH within 7 days (<5) – Massachusetts regulation– DEA 106 with 24 hours (>5)– Addendums within 45 days
• Will document what disciplinary action took place
• Other agencies– BOP, DPH, CMS, FDA, Board of Nursing, Board of Medical Practice
37
http://cx.aos.ask.com/question/aq/700px-700px/far-back-can-irs-audit_30c97076e46eeec2.jpg
AUDITING#6
38
20
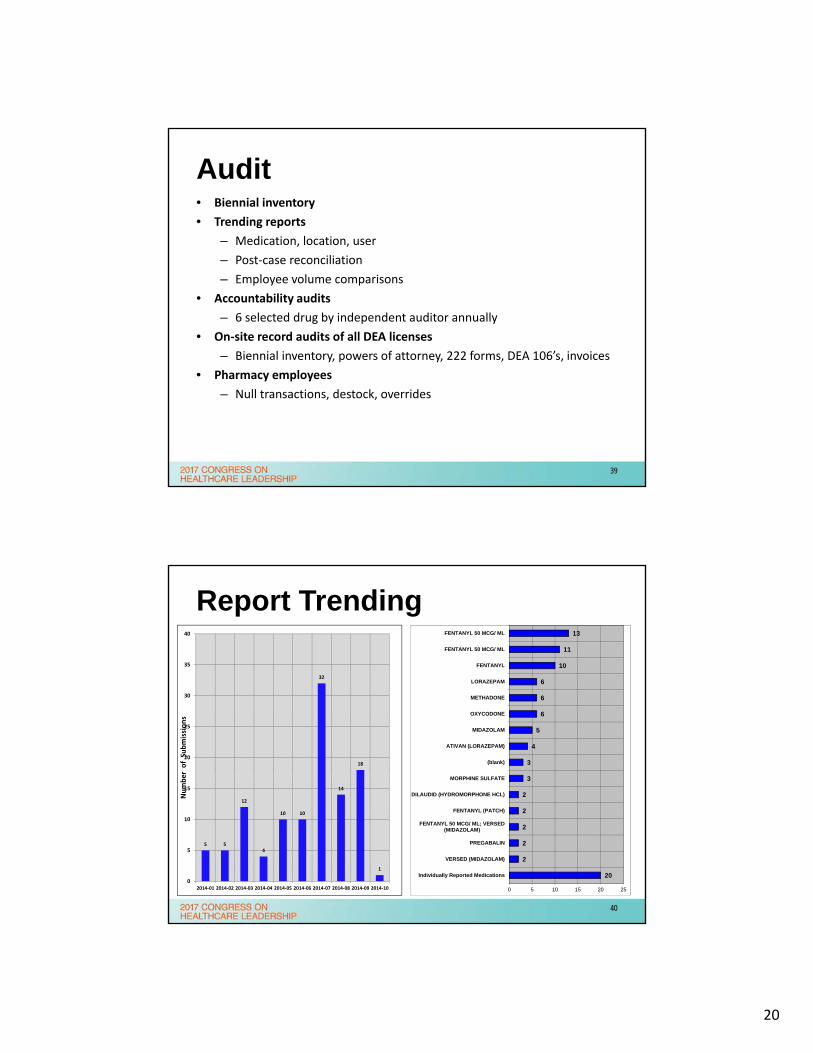
Audit• Biennial inventory
• Trending reports
– Medication, location, user
– Post‐case reconciliation
– Employee volume comparisons
• Accountability audits
– 6 selected drug by independent auditor annually
• On‐site record audits of all DEA licenses
– Biennial inventory, powers of attorney, 222 forms, DEA 106’s, invoices
• Pharmacy employees
– Null transactions, destock, overrides
39
Report Trending
20
2
2
2
2
2
3
3
4
5
6
6
6
10
11
13
0 5 10 15 20 25
Individually Reported Medications
VERSED (MIDAZOLAM)
PREGABALIN
FENTANYL 50 MCG/ ML; VERSED(MIDAZOLAM)
FENTANYL (PATCH)
DILAUDID (HYDROMORPHONE HCL)
MORPHINE SULFATE
(blank)
ATIVAN (LORAZEPAM)
MIDAZOLAM
OXYCODONE
METHADONE
LORAZEPAM
FENTANYL
FENTANYL 50 MCG/ ML
FENTANYL 50 MCG/ ML
5 5
12
4
10 10
32
14
18
1
0
5
10
15
20
25
30
35
40
2014‐01 2014‐02 2014‐03 2014‐04 2014‐05 2014‐06 2014‐07 2014‐08 2014‐09 2014‐10
Number of Submissions
40
21
• technology
TECHNOLOGY#7
41
Automation/Technology• Control substance
surveillance system• Automated dispensing
cabinets, anesthesia workstations• Biometrics
• Access to quick and usable data– 2 years worth of readily
retrievable “usable” data
• Security cameras• Understanding how
technology works/limitations• When patients are discharged
from system• System configurations, upgrades
42
22
http://fullhdwp.com/images/wallpapers/Bank_Vault_3D_Wallpaper-HD.jpghttp://fullhdwp.com/images/wallpapers/Bank_Vault_3D_Wallpaper-HD.jpg
• Pharmacy totes
PHARMACYCONTROLS
#8
43
Ordering, Receiving, Storage, Returning
• Ordering– Different than person
receiving– Limited to certain
employees/POA
• Receiving– Totes immediately to vault
and processed– CSOS matching– Limiting vault and staff
access
• Distribution– Limited daily pulls– Locked delivery cabinets
• Storage– Patients own meds– Cameras– Biometrics– Override list– Profile vs. non‐profiled– Downtime procedures
• Returning– Return bins– Drug waste– Reverse distributors
44
23
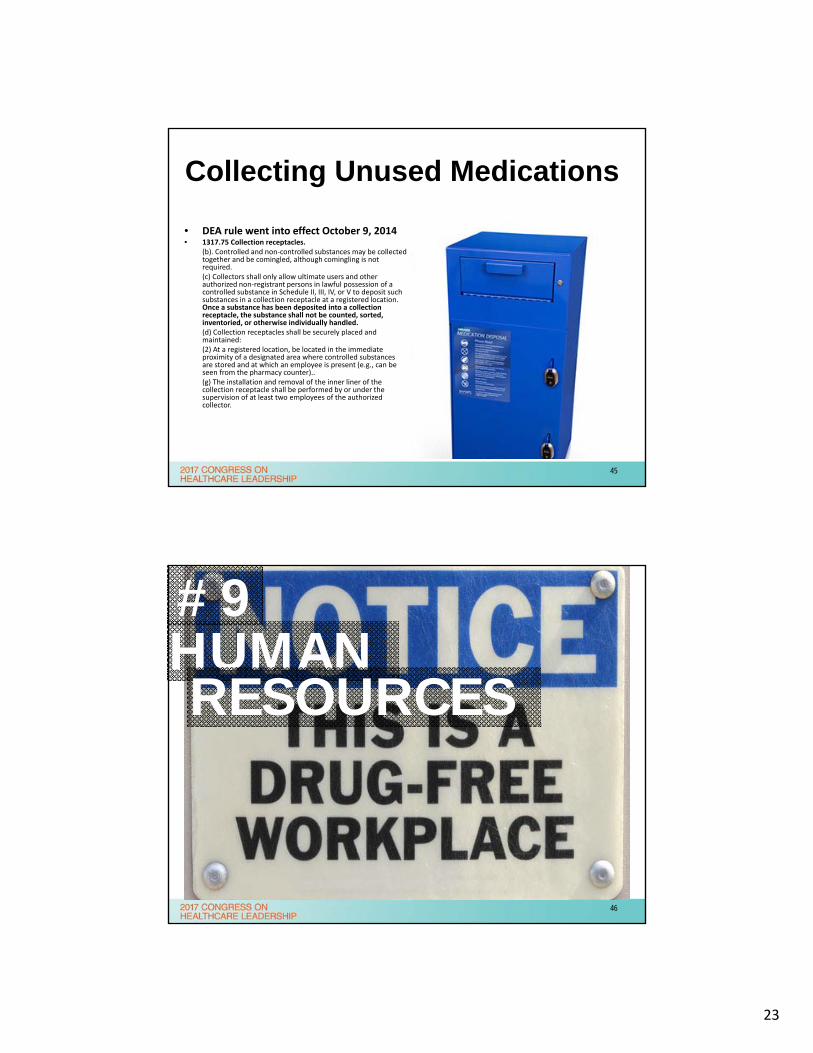
Collecting Unused Medications
• DEA rule went into effect October 9, 2014• 1317.75 Collection receptacles.
(b). Controlled and non‐controlled substances may be collected together and be comingled, although comingling is not required.(c) Collectors shall only allow ultimate users and other authorized non‐registrant persons in lawful possession of a controlled substance in Schedule II, III, IV, or V to deposit such substances in a collection receptacle at a registered location. Once a substance has been deposited into a collection receptacle, the substance shall not be counted, sorted, inventoried, or otherwise individually handled.(d) Collection receptacles shall be securely placed and maintained:(2) At a registered location, be located in the immediate proximity of a designated area where controlled substances are stored and at which an employee is present (e.g., can be seen from the pharmacy counter)..(g) The installation and removal of the inner liner of the collection receptacle shall be performed by or under the supervision of at least two employees of the authorized collector.
45
#9HUMANRESOURCES
46
24
Human Resources
• Drug testing upon hire, random?
• Corrective action
• Investigational leave, FMLA
• Bringing employees back after treatment
47
#10MULTI-DISCIPLINARY
48
25
Multi-Disciplinary Collaboration
• Executive leadership
• Pharmacy
• Anesthesia– Policy compliance
– Leadership accountability
– Employee corrective action
• Nursing– Daily surveillance
– Discrepancies
– Weekly cycle counts
– Policy and process accountability
– Employee corrective action
49
OTHER AREAS OF CONSIDERATION
• Non‐pharmacy DEA licenses
• Non‐clinical hospital employees
• Removing employee access
• Policy updates
• Research
• Waste containers
• Patients own meds
50
26
WORKINGWITHTHE DEA
51
Working with the DEA
• Legal counsel
• Cause or no cause
• Be organized
• Readily retrievable data
• Lack understanding of hospital operations and processes
• Accountability audits
• Outside auditor or consultants
• Implement improvements while investigation ongoing
• Understand hot buttons
52
27
Working with the DEA
• Which violations are you agreeing to or contesting
• Double counting violations
• How audits were conducted
• Precedent based on previous cases
• Corrective action plan
53
RESOURCES54
28
Resources
• Dedicated resources
• Technology/automation– Control substance
surveillance software
– Automated dispensing cabinets
– Anesthesia workstations
– Biometrics
– Cameras
• Waste receptacles
• Indirect costs– Nursing time
– Meetings
– Investigations
55
MGH INITIAL COSTS
56
29
Strategic Priorities
Write down 5 strategic control substance diversion priorities that you plan to begin to
implement when you return to your organization
Share with the audience 2-3 of those strategic priorities
57
Resources
• ASHP Guidelines on Preventing Diversion of Control Substances
• ASHP Controlled Substances Diversion Prevention Program Elements of Implementation
• Use for gap analysis
58
30
Lessons Learned• Are you looking hard enough?
• Proactive vs. reactive
• Comprehensive
• Multidisciplinary collaboration is critical
• Variety of surveillance and audit tools
• Resources dedicated to sustaining program
• Program visibility is major deterrent
59
60
31
Questions?
Chris Fortier
Faculty Biography & Contact Info
• Christopher Fortier, PharmD, FASHP ([email protected])– Chief Pharmacy Officer, Massachusetts General Hospital,
Boston, MA
– Graduated from the University of Connecticut with a Doctor of Pharmacy degree in 2003
– Completed a PGY-1 Practice and PGY-2 Health-System Pharmacy Administration Residency at the Medical Univ. of South Carolina in Charleston, SC
– Adjunct Associate Professor: Univ. of Connecticut, Northeastern University, and Massachusetts College of Pharmacy
62