Embed Size (px)
DESCRIPTION
Services and Supports Array Provider Network Natural Helpers Financing – Track 2. Sheila A. Pires Human Service Collaborative [email protected] Vickie Miene Northeast Iowa [email protected] Matt Wojack Ingham County, Michigan [email protected]. State and Local Realities. - PowerPoint PPT Presentation
Citation preview

Services and Supports ArrayProvider NetworkNatural HelpersFinancing – Track 2 Sheila A. Pires
Human Service [email protected]
Vickie MieneNortheast [email protected]
Matt WojackIngham County, [email protected]

22
State and Local Realities
Growing evidence of effectiveness of home and community-based services & of system of care technologies – even for youth with
most challenging issues, e.g. youth with sex offenses, fire starting behaviors, dual diagnoses
+Potential cost savings to Medicaid, mental health, child
welfare, education, juvenile justice in HCB and SOC+
Lack of sufficient HCB service capacity +
Dollars are finite
Conclusion: Redirect spending from out of home placements with high costs and/or poor outcomes to home and community-based services and supports in a system of care
Pires, S. (2006). Primer Hands On . Washington, D.C.: Human Service Collaborative.

3
Redirection
Where are you spending resources onhigh costs and/or poor outcomes?
Residential Treatment?Group Homes?Detention?Hospital admissions/re-admissions?Too long stays in therapeutic foster care?Inappropriate psychotropic drug use?“Cookie-cutter” psychiatric and psychologicalevaluations?

4
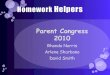
Wraparound Milwaukee – Example of Redirection and Pooled Funds
Child WelfareFunds thru Case Rate
(Budget for InstitutionalCare for CHIPS Children)
Mental Health•Crisis Billing•Block Grant
•HMO Commercial Insurance
Medicaid Capitation(1557 per Month
per Enrollee
Juvenile Justice(Funds Budgeted for
Residential Treatment for Delinquent Youth)
Management Entity:Wraparound Milwaukee
Management Service Organization (MSO)$30M
Child and Family Teams
ProviderNetwork
240 Providers85 Services
CareCoordination
Plans of Care
9.5M 2.0M10M8.5M
Per Participant Case Rate
Family Organization$300,000
Mgt. Entity: Co. BH Div.
Wraparound Milwaukee. (2002). What are the pooled funds? Milwaukee, WI: Milwaukee County Mental Health Division, Child and Adolescent Services Branch

5
Dawn Project Cost Allocation
How Dawn Project is Funded
Example of Braided FundsDAWN Project - Indianapolis, IN
2005 CHIOCES, Inc., Indianapolis, IN
RAINBOWS
(Family Organization)
CFT and Care Coordination Structure

6
Example of “Virtual” Pooled FundsCuyahoga County (Cleveland)
FCFC $$Fast/ABC $$Residential Treatment Center $$$$Therapeutic Foster Care $$$“Unruly”/shelter care $Tapestry $$SCY $$
County Administrative
Services Organization
Neighborhood Collaboratives &Lead Provider Agency
Care CoordinationPartnerships
Community Providers and Natural Helping Networks
Reinvestment of savings
Pires, S. (2006). Primer Hands On . Washington, D.C.: Human Service Collaborative.
}
}
StateEarly Intervention and Family Preservation
System of Care Grants
System of Care Oversight Committee
Child and Family Team Plan of
Care

7
KEY QUESTIONS
Expenditure and Utilization Questions:
1. Which State agencies spend dollars on BH services for children and youth?
2. How much do they spend?3. What types of dollars are spent (e.g., Fed’l., State)?4. What services are financed?5. How many children and youth use services?6. What are the characteristics of these children and youth
(e.g., by age, gender, race/ethnicity, diagnosis, region)?7. What services do they use? 8. How much service do they use?

8
Financing Strategies and Structures to Support Improved Outcomes for Children, Youth and Families
FIRST PRINCIPLE: System Design Drives Financing
Adapted from Friedman, M. (1995). Financing strategies to support improved outcomes for children. Washington, DC: Center for the Study of Social Policy.
REDEPLOYMENTUsing the money we already haveThe cost of doing nothingShifting funds from treatment to early intervention and preventionMoving across fiscal years
REFINANCINGGenerating new money by increasing federal claimsThe commitment to reinvest funds for families and childrenFoster Care and Adoption Assistance (Title IV-E)Medicaid (Title XIX)
RAISING OTHER REVENUE TO SUPPORT FAMILIES AND CHILDRENDonationsSpecial taxes and taxing districts for childrenFees & third party collections including child supportTrust funds
FINANCING STRUCTURES THAT SUPPORT GOALSSeamless services: Financial claiming invisible to families Funding pools: Breaking the lock of agency ownership of fundsFlexible Dollars: Removing the barriers to meeting the unique needs of familiesIncentives: Rewarding good practice

9
Medicaid Option Advantages Issues Example
Rehabilitation Services Option
•Flexibility to cover a broad array of services and supports provided in different settings (e.g., home, school)
•Service definitions often adult-oriented
•Federal scrutiny
•Many states
Managed Care Demos and Waivers - 1115 and 1915 (b)
•Accountability and management of cost through risk structuring/sharing
•Flexibility to cover wide range of services and populations
•Managed care not without risks/challenges
•Federal waiver process can be challenging
•Cost neutrality issues
•NM – covering MST
•AZ – covering family support, therapeutic foster care
Home and Community-Based Waivers - 1915 (c)
•Flexibility, broader coverage, waiver of income limits and comparability
•Alternative to hospital-level of care, but PRTF (i.e., residential treatment) may be issue
•Cost and management concerns limited to small number
•KS, NY, VT, IN, WI – have HCBS Waivers•AK, FL, GA, IN, KN, MD, MS, MT, SC, VA – have community alternatives to psychiatric residential treatment facilities demonstration grant
Examples of Medicaid Options States Use to Cover Evidence-Based and Promising Community-Based Practices (1)
Pires, S. 2005. Building systems of care. Human Service Collaborative. Washington, D.C.

10
Medicaid Option
Advantages Issues Example
Early and Periodic Screening, Diagnosis and Treatment - EPSDT
•Broadest entitlement
•Supports holistic (PH and BH) assessments and services
•No waiver or state plan amendment requirements
•Management mechanism critical because of cost concerns
•Oriented more to physical health in practice
•RI
•PA
Targeted Case Management
•Can be targeted to high need populations
•Supports small case load focus (e.g., 1-10)
•Not sufficient without other services
•Federal attention
•VT
•NY
Administrative Case Management
•Ability to cover basic case management services to support enrollment access
•Not sufficient without other services
•NJ – covering some activities of family-run organization
Examples of Medicaid Options States Use to Cover Evidence-Based and Promising Community-Based Practices (2)
Pires, S. 2005. Building systems of care. Human Service Collaborative. Washington, D.C.

11
Medicaid Option
Advantages Issues Example
Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA)
•Avenue to eligibility to community-based services for children who meet SSI disability criteria – allows disregard of family income
•SSI criteria not easy to meet for children with SED
•Does not expand types of covered services
•Cost issues, so generally small program
•MN
•WI
Medicaid as Part of a Blended or Braided Funding Approach (without a waiver)
•Holistic, integrated (across systems) financing, supports broad array of services, natural supports and individualized care
•Involves significant restructuring
•Milwaukee Wraparound
•DAWN Project
•Massachusetts Mental Health Services Program for Youth
•New Jersey Partnership
Examples of Medicaid Options States Use to Cover Evidence-Based and Promising Community-Based Practices (3)
Pires, S. 2005. Building systems of care. Human Service Collaborative. Washington, D.C.

12
Purchasing/Contracting OptionsPre-Approved Provider Lists:+ Flexibility for system of care + Choice for families - Could disadvantage small indigenous providers- Could create overload on some providers
Risk-Based Contracts+ Flexibility for providers+ Individualized care for families - Potential for under-service- Potential for overpaying for services
Fixed Price/Service Contracts+ Predictability and stability for providers - Inflexible-families have to “fit” what is available
Pires, S. (2002). Building systems of care: A primer. Washington, D.C.: Human Service Collaborative.

13
Capitation and Case Rate Distinctions
Capitation: Pays MCOs or providers a fixed rate per eligible user Incentive: #1: Prevent eligible users from becoming actual users (e.g., make it difficult to access services; engage in prevention)#2: Control the type and volume of services used
Case Rate: Pays MCOs or providers a fixed rate per actual userIncentive: #1: Control the type and volume of services used
Pires, S. Building systems of care: A primer. Washington, D.C.: Human Service Collaborative.

14
Risk-Based Contracting Arrangement
Pires, S. (1999). El paso county, colorado risk-based contracting arrangement. Washington, DC: Human Service Collaborative.
State-Capped Out of Home Placement Allocation
County Dept. of Human Services acts as Management Care Organization (contracting, monitoring, utilization review)
Child Welfare $$Case rate contract with CPA
BH Tx $$ matched by Medicaid. Capitation contract with BHO with risk-adjusted rates for child welfare-involved children
Joint treatment planning approved by Dept. of Human Services
Child Placement Agencies (CPA)
Responsible for full range of Child WelfareServices & ASFA (Adoption and Safe Families ACT) related outcomes
Mental Health Assessment and Service Agency (BHO)
Responsible (at risk) for full range of MH treatment services & clinical outcomes & ASO functions

Services/Supports Array, Provider Network, Natural Helpers and
Financing
Vickie MieneIowa

Iowa’s current system

Lessons Learned - Community Based Resources
• Building on existing Community Based Services is:– Empowering to the agency
providing the service– Better for youth and families
(fewer out of town trips saves gas, energy, and time)
– Creates better relationships with the service agencies and forces communication among providers and the SOC which results in less duplication of efforts.
– SOC values and principals are taught and applied on a local level, creating a common thread between service entities

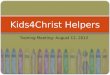
Community Circle of Care Buchanan, Delaware, Fayette
Mon
thly P
arent
Su
pport grou
p – D
ays In
n
Lam
ont K
ids nigh
t – com
mu
nity you
th
sup
port
B an
d D
skill buildin
g services
LS
I Crisis
Interven
tion S
ervices
Positive P
eer C
onn
ections
Back
bon
e Men
tal H
ealth C
enter
Exp
ress yourself art
events
Ou
tpatien
t therap
y – area agen
cies
Dep
artmen
t of Hu
man
S
ervices, FS
RP
services
LS
I Resp
ite Services
Fou
r Oak
s Skill
Bu
ilding S
ervices
Psych
iatric Services
(local provid
ers or UI)
Care C
oordin
ation
Services
Lu
theran
Services in
Iow
a Early
Interven
tion services
Ed
ucation
, advocacy
and
trainin
g op
portu
nities
Ph
ysical Assessm
ent
and
med
ical screenin
g
Local M
edical H
ome
for men
tal health
n
eeds
Hillcrest S
helter
Services
Brem
wood
Sh
elter S
ervices

Family Team Meeting• Natural Supports identified• Agenda set by family/youth• Community supports Family Team Meeting
Concept, (providers attend and provide input, they offer to host meetings at their location)
• Families report feeling empowered and like they really had choices
• Barriers discovered during family team meetings, are taken to advisory meetings for solution focused discussion.

Crisis Intervention Services• 1-800 number for over the phone crisis talk down• 1 hour face to face response with a crisis intervention
worker• Cool down respite placement that can be utilized for 48
hours.

STEP-IN Crisis Services
• 45 day program• Intensive Family
Preservation Model• 1 hour response time• Prevent hospitalization• Utilize respite if needed

Service/Supports Array, Provider Network, Natural
Helpers and Financing “2010 CHILD MENTAL HEALTH INITIATIVE NEW COMMUNITY
TRAINING”(Issue Briefs #3, #5, #6)
Matt Wojack
Ingham County, Michigan

Any Effective System of Care for Children with Serious Emotional Disturbance is Built Upon an Outcome Oriented Home-Based Mental Health Program
--Bob Friedman

Family Empowerment• How do We support Families in Using Voice• What Do Families Need• How are Supports Organized to
Accommodate Such

Commitment to SOC Changes the WorldShift in Values
Shift in Practice
Real Data Supports real Change

Bundle of Services• Home-Based Mental Health • Wraparound Facilitation• Family Advocacy Support

Cost Monitoring Supports the Long-Term Viability of the System
“How Do you Want to Spend Your Money?”
1 Residential = 8 System of Care
Broad Examination of Cost Savings>40% reduction in JJ; $1M saved by CPS

Case Rate Model• Up to One Year of Support• Three Components• Realigning Resources
Sustaining a System of Care“We were headed in the right direction…”
“There is no going back..”

Matt Wojack, Project DirectorImpact, Ingham County System of Care Initiative
517-346-8038
www.impactsystemofcare.org