Embed Size (px)
Citation preview

Cancer Detection and Prevention 27 (2003) 360–369
Service screening with mammography of women aged70–74 years in Sweden
Effects on breast cancer mortality
Håkan Jonsson, PhDa,∗, Sven Törnberg, MD, PhDb,Lennarth Nyström, PhDc, Per Lenner, MD, PhDa
a Department of Oncology, Umeå University, Umeå, Swedenb Oncologic Centre, Karolinska Hospital, Stockholm, Sweden
c Epidemiology, Public Health and Clinical Medicine, Umeå University, Umeå, Sweden
Accepted 24 July 2003
Abstract
Since the benefit of mammography screening for women 70 years and older is unclear, the aim of the present study was to evaluatethe effect on breast cancer mortality of the population-based service-screening program in Sweden inviting women 70–74 years. Amongthe counties with service-screening programs in Sweden which started 1986–1990 those with upper age limit 74 years were comparedto counties with 69 years as upper age limit with respect to refined breast cancer mortality. Allowance was made for potential biasesnamely inclusion of cases diagnosed before invitation and lead time. Two methods for estimation of breast cancer mortality were used;underlying cause of death (UCD) and excess mortality. With a mean follow-up of 10.1 years a reduction of the breast cancer excessmortality was estimated at 24%. Using the underlying cause of death the corresponding result was 6%. A non-significant reduction inbreast cancer mortality was found in the counties with service-screening program including the age group 70–74 years in Sweden. Theestimated reduction was larger when using excess mortality compared to the use of individual underlying cause of death.© 2003 International Society for Preventive Oncology. Published by Elsevier Ltd. All rights reserved.
Keywords:Breast cancer; Mortality; Mammography screening; Evaluation
1. Introduction
Randomized studies have shown that screening for breastcancer with mammography reduces the breast cancer mortal-ity [1,2], especially for women aged 50–69 years at invitationto screening. Theoretically, screening should be beneficialalso for women aged 70 years or more[3,4] however, thereis a lack of empirical evidence to support this statement.The only randomized screening trial that included women70 years and older was the Swedish Two-County trial[1].Today nationwide service-screening programs have been in-troduced in Sweden, Finland, The Netherlands, UK, Icelandand Luxembourg but only in Sweden and The Netherlandswomen aged 70 and older are invited to screening. Only theFinnish program, which invites women 50–59 years withoption to continue up to 64 years, was designed to facil-
∗ Corresponding author. Present address: Oncological Centre, UmeåUniversity Hospital, S-901 85 Umeå, Sweden. Tel.:+46-90-7851990;fax: +46-90-127464.E-mail address:[email protected] (H. Jonsson).
itate an evaluation[5]. Some attempts have been made toestimate the effects of service screening in Sweden. Breastcancer mortality in counties with screening programs wascompared with counties with no screening[6], or comparedover time[7] as well as related to surrogate measures[8].Evaluations of programs inviting women 40–49 and 50–69years to screening has previously been reported[9,10]. In aDutch study, women aged 68–83 years at first invitation toservice screening were studied[11].
The only randomized trial including the age group 70–74years was the Two-County study[1]. After 20 years offollow-up [12], the relative risk (RR) was 0.76 (95% CI0.44–1.33) and 0.73 (95% CI 0.45–1.19), respectively ineach of the two counties. The study group 70–74 years atrandomization were invited to screening for two rounds only.In a Dutch study the breast cancer mortality in women aged68–83 at first invitation to screening was reduced by 20%(P > 0.05) [11]. A study in northern Sweden[6] indicated anon-significant 17% reduction in excess mortality related tobreast cancer in a service-screened population in compari-son with an unscreened population for women 70–74 years.
0361-090X/$30.00 © 2003 International Society for Preventive Oncology. Published by Elsevier Ltd. All rights reserved.doi:10.1016/S0361-090X(03)00131-4

H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369 361
However, no reference period was used, hence some of thereduction may be explained by differences in baseline mor-tality in that study.
When the first results from the Two-County trial werepublished[1], the National Board of Health and Welfare inSweden issued guidelines for mammography screening[13]recommending a lower age limit not below 40 years and notover 50 years, and an upper age limit not below 69 years, andnot over 74 years. Consequently the age group 50–69 yearswas covered in all counties where screening was introduced.Service screening started in Sweden in 1986 and had in 1997been introduced in all 23 counties. Out of these, 13 countieshave 74 years as an upper limit for invitation to screening.The age limits were based on local political decisions andavailability of resources.
When studying the effect of screening in age-group 70–74years two main questions are of importance: (1) Does screen-ing per se in women aged 70–74 years reduce breast can-cer mortality? and (2) Does screening in this age group, asa continuation of screening of women 50–69 years, causea further reduction of the breast cancer mortality? It seemsadequate to answer the question one first and if the answeris positive, to continue with the second question. However,the first question is only a theoretical one as no screeningprogram has a lower age limit of 70 years. Therefore, the rel-evant issue should be to investigate how much screening inage 70–74 years adds to the reduction of breast cancer mor-tality. In this study, we have addressed this latter question.
The aim of the present study was to estimate the ef-fect on breast cancer mortality of the population-basedservice-screening program in Sweden inviting women with74 years as upper limit for invitation in comparison withcounties where the upper limit was 69 years.
2. Materials and methods
All organized mammography screening in Sweden ispopulation-based. Screening programs are usually orga-nized at county level. However, some of the counties weredivided into sub-regions that differed concerning startingtime and age limits. We therefore had to divide those coun-ties into smaller geographical areas to obtain homogeneousgeographical units. From the potential study populationconsisting of all 23 counties, we excluded counties or partsof counties where randomized studies had been performed(Kopparberg, Östergötland, Stockholm (south) and the citiesof Göteborg and Malmö). Also the county of Gävleborgwas excluded because population-based screening was in-troduced there already in 1974. Areas where the upper agelimit for invitation to screening was 74 years constituted thestudy population. For comparison, we used a control groupbased on the geographical areas where the upper limit forinvitation was 69 years (Table 1). In the county of Skaraborgan upper age limit of 74 years was used for the first 1.5years but thereafter it was changed to 69 years, thus also
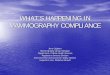
Fig. 1. Map of municipalities in Sweden illustrating areas included, inthe study group (dark gray), in the control group (light gray) and notincluded (white).
Skaraborg was excluded from this study. To ensure a rea-sonable follow-up time only the geographical areas wherescreening started early (1986–1990) were included. Ex-cluded were therefore also the counties or parts of counties;Landskrona (part of Skåne), Värmland, Älvsborg (north),Västerbotten, Jämtland and Gotland. The map inFig. 1shows areas included in the study and control groups. In1987, the mean number of women 70–74 years was 83,830

362H
.Jo
nsso
ne
ta
l./Ca
nce
rD
ete
ction
an
dP
reven
tion
27
(20
03
)3
60
–3
69
Table 1Female population 70–74 years (1987, mid-year), time for screening start, years of follow-up in the study, number of person-years, cumulative number of breast cancer deaths and mortality rates (70–74years at diagnosis and according to the refined mortality model) in the geographical areas for the reference and the study period, respectively
Geographical area County Number ofwomen
Starting(month/year)
Years offollow-up
Reference period Study period
Person-years× 1000
Cumulativenumber of breastcancer deaths
Cumulativenumber of breastcancer deaths per100,000
Person-years× 1000
Cumulativenumber of breastcancer deaths
Cumulativenumber of breastcancer deaths per100,000
Geographical areas study groupEksjö/Nässjö Jönköping 3121 8/86 12 52 17 390 55 14 303Kalmar Kalmar 6482 10/86 12 111 33 355 113 29 309Bohus Västra Götaland 6330 11/86 12 98 18 219 113 34 360Jönköping/Ryhov Jönköping 4838 4/87 11 67 23 379 78 28 396Trelleborg Skåne 2937 4/87 11 45 18 444 48 13 298Örebro Örebro 7405 10/87 11 113 37 362 120 30 275Uppsala Uppsala 5433 10/88 10 74 20 271 81 34 418Älvsborg (south) Västra Götaland 6645 11/88 10 93 20 216 97 15 154Halland Halland 5758 1/89 10 78 25 320 89 17 190Norrbotten Norrbotten 5835 3/89 9 69 14 184 75 19 227Helsingborg Skåne 4075 3/89 9 51 17 300 54 21 350Lund Skåne 3941 4/89 9 51 14 245 54 12 200Södermanland Södermanland 6299 11/89 9 80 21 237 87 18 187Västernorrland Västernorrland 7082 1/90 9 93 29 280 93 22 214Ängelholm Skåne 2403 1/90 9 29 10 309 33 10 274Kristianstad Skåne 5246 11/90 8 59 11 149 61 9 119
Total 83830 1163 327 1251 325
Geographical areas control groupVästmanland Västmanland 6165 10/86 12 91 26 342 109 29 319Blekinge Blekinge 4012 3/88 10 56 11 195 58 6 104Danderyd Stockholm 6783 8/89 9 86 20 210 95 30 283Karolinska Stockholm 4815 8/89 9 55 14 231 72 12 151Skärholmen/Huddinge Stockholm 7609 8/89 9 89 24 242 107 33 277Sabbatsberg/St Göran Stockholm 8081 3/90 8 108 25 186 89 26 233Kronoberg Kronoberg 4143 8/90 8 49 21 345 50 10 159
Total 41608 534 141 580 146

H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369 363
in the study population and 41,608 in the control population.Based on the information from the screening centers themean screening interval (weighted by the population) wasestimated at 22.8 months in the study population while itwas 23.1 months in the control population (screening up to69 years). The corresponding figures for the duration of thefirst screening round was 27.6 and 24.5 months for the studypopulation and the control population, respectively.
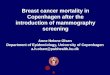
We have studied two time periods, a study period, in whichscreening was introduced 1986–1998, and a reference period1976–1988. The time for start of screening in the studypopulation varied between August 1986 and November 1990(Table 1) and was in average (weighted by the population)mid-July 1988. In the control population screening startedbetween October 1986 and August 1990. The average starttime was the end of March 1989. Each geographical area inthe study and the control populations constituted separatecohorts. During the study period the cohorts consisted of allwomen 65–74 years old at the first invitation to screening.Similar cohorts were also defined in the reference period 10years before the start of screening for respective area, withthe same age criterion. Women below 70 years at start wereincluded when they reached the age of 70. Breast cancercases in the study cohorts were accrued in age 70–74 years atdiagnosis from screening start and forward (Fig. 2). Accrualof breast cancer cases and follow-up was defined in thesame way for the cohorts in the reference period with start10 years ahead of the start of screening. The cohorts in thestudy period were followed through 1998 and the cohorts inthe reference period through 1988.
Individual information was used regarding date, age andresidence at breast cancer diagnosis, date of death and causeof death for the breast cancer cases. As we had no access toindividual screening data we had to make an approximation
Calendar time (1 Jan)
Age
1986 1988 1990 1992 1994 1996 1998 2000
6570
7580
8590
Follow-upAccrual
Fig. 2. Illustration of the inclusion and follow-up in the refined mortality model. Example is given with cases who died from breast cancer in a cohortwhere invitation to screening started January 1987. The plus sign denotes breast cancer diagnosis and squares symbolize death from breast cancer. Deathsvalid in the refined model are denoted by filled squares.
for time of invitation within each geographical area. Forthe calculation of person-years in the population, aggregateddata were used.
Information on month and year of start for each screen-ing program, progression of the building-up of screeningactivities within geographical areas, age groups invited andintervals between screening rounds were obtained from thescreening centers via a questionnaire. For each breast cancercase, date of diagnosis and date and cause of death for the de-ceased subjects were obtained from the nationwide SwedishCancer Registry. Breast cancer mortality data aggregated bycalendar year, municipality and 5-year age groups were ob-tained from the Swedish Cause of Death Registry and pop-ulation data aggregated by municipality, calendar year and5-year age groups from Statistics Sweden.
The mean follow-up time (weighted by the population)was 10.1 years (range 8–12) in the study cohorts and 9.3years in the control cohorts (range 8–12). By definition, themean follow-up times were the same in the reference period(10.1 years). Considering a mean time for the first roundof 27.6 months the mean individual follow-up time, withconsideration to both entry in the cohort and first invitationto screening, was estimated at 8.1 years.
A breast cancer case was defined as a case of invasive ade-nocarcinoma of the breast (site code= 174 in InternationalClassification of Diseases, ICD-9; and histo-pathologicalcode= 096 according to WHO/HS/CAN/24.1) diagnosedat age 70–74 years during the reference or the study period(Fig. 2). If a woman had two breast cancer diagnoses in oneof the periods 1976–1988 or 1986–1998, the second cancerwas excluded. A breast cancer death was defined as a breastcancer case with breast cancer as the underlying cause ofdeath (UCD) and reported to the Cause of Death Registrynot later than 31 December 1998.

364 H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369
In the Swedish cancer register cancer cases are not in-cluded based on death certificates only. It is therefore possi-ble that a deceased case was reported with breast cancer asunderlying cause to the Cause of Death Registry but not asa breast cancer case to the Cancer Registry. In a study[14],it was found that 1% of the deaths aged 40–74 years in theSwedish cause of death register reported with breast canceras underlying cause of death were not reported to the cancerregister.
Age specific breast cancer mortality for women 70–84years at death, was plotted for the study and the controlgroup. This was based on the total number of breast cancerdeaths each year, here referred to as total breast cancer mor-tality. To avoid including cases with a breast cancer diagno-sis before start of screening and below 70 years of age theso-called refined breast cancer mortality was used[6,15]. Inthe refined mortality model breast cancer deaths are includedonly if breast cancer was diagnosed at age 70–74 years afterscreening start in the study period or after the correspondingstart times in the reference period (Fig. 2). Refined breastcancer mortality cannot be interpreted for different years offollow-up in the same way as total breast cancer mortality.
During the follow-up women were between 70 and 86years of age. There might be uncertainty in the coded un-derlying cause of death among old women in these agesdue to competing diseases. We therefore used two differentoutcome measures; excess breast cancer mortality[6] andbreast cancer as the underlying cause of death. For each de-ceased case, UCD was used as it is recorded in the cause ofdeath register. Excess mortality is estimated by(O−E)/N
whereO is the total number of deaths among the breast can-cer cases, andE is the expected number of deaths amongthe breast cancer cases. It is derived as the population to-tal mortality times the number of person-years among thebreast cancer cases.N is the total number of person-years inthe studied group. The variance of the ln(RR) can be esti-mated byV̂ (ln(RR)) = O0/(O0 −E0)
2 +O1/(O1 −E1)2,
where the indexes correspond to the study group (1) and thecontrol group (0).
Cumulative refined breast cancer mortality per 100,000was computed with the mean number of person-years asdenominator (person-years divided by years of follow-up).Cumulative relative risks were estimated. In order to adjustfor possible geographical differences in breast cancer mor-tality between the study group and the control group therelative risk for the study period was divided by the rela-tive risk for the reference period. This ratio is the relativerisk due to invitation to screening assuming multiplicativeeffects between the groups and the time periods.
The refined breast cancer mortality was also analyzedin a multiplicative Poisson model with the number ofbreast cancer deaths (UCD) as the dependent variable andfollow-up year (3-year intervals), age during follow-up(5-year classes), geographical area and time period (studyor reference) as covariates, all categorical[16]. The ex-cess mortality was analyzed in the same way but with the
number of deaths among the breast cancer cases as the de-pendent variable[10]. The screening effect was measuredby a dummy variable set to 1 for the study group cohortsin the study period and to 0 elsewhere. The logarithm ofperson-years defined by the cohorts and the follow-up wastaken as offset.
Inclusion and lead time bias may be inherent in this ob-servational study.
2.1. Inclusion bias
One reason for dilution of the results stems from difficul-ties in defining the studied population at the beginning of thefollow-up since it takes the first screening round to progres-sively include all the women within a screening area. We in-cluded all incident breast cancer cases after start of invitationto screening within a geographical area in the study group,implicating the inclusion of an unknown number of cases di-agnosed before invitation to screening during the first round.This will of course lead to a dilution of the potential benefitsof screening, since a number of cases not yet invited weremixed with the already invited women. The magnitude ofthe problem was estimated by simulation[10] using the factthat the mean screening interval was 28 months in the firstscreening round. For a given 28-month calendar period weassumed a random time point for invitation to be uniformlydistributed over (0, 28) months for each woman with a breastcancer diagnosis. For this sample, the cumulative breastcancer mortality in the given period can be estimated for thewomen who had a breast cancer diagnosis before invitationto screening. Based on the breast cancer cases aged 70–74years and diagnosed in the two periods: December 1981to March 1984 and April 1984 to July 1986 for the studyand control groups combined, 200 replicates from each pe-riod were simulated. The cumulative refined breast cancermortality for the cases diagnosed before invitation was esti-mated. Based on the length of follow-up and the size of thepopulation the expected number of breast cancer deaths wasestimated for each geographical area. These were added toa total of 76.8 (24% (76.8/325) of the observed number ofbreast cancer deaths (UCD) in the study cohorts during thestudy period). If the relative risk adjusted for the referenceperiod is formulated asOC/EC, whereOC is the observednumber of breast cancer deaths andEC is the correspond-ing expected number without screening, we can perform anadjustment of the relative risk for inclusion bias by(OC −ψ)/((OC/RR) − ψ). Here,ψ denotes the expected numberof breast cancer deaths in women with a breast cancer diag-nosis before invitation to screening during the first screeninground.
2.2. Lead time bias
In the present study, age was defined as age at diagnosis,implicating that a lead time bias might have been introduced.The purpose of mammography screening is early detection

H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369 365
of breast cancer. Women who were diagnosed with and diedfrom breast cancer in the study areas during the study periodcould get their diagnosis in an earlier stage of the diseasethan in the control areas. For example a case in the groupinvited to screening may be classified as belonging to theage group below 75 years while a corresponding woman inthe control group may be 75 years or more at diagnosis,even though she had an otherwise comparable cancer anddied from it at the same time.
Since both the study group and the control group werefollowed from screening start and the ages 50–69 yearswere covered in all areas there should not be any lead timebias around the age limit 70 years. Five counties whichstarted screening late (between April 1993 and May 1997)for women up to 69 years were used as control group(Gotland, Värmland, Västerbotten, Jämtland and northernÄlvsborg). The geographical areas in the study group werefollowed from screening start and the control group wasfollowed from April 1988. All areas were followed for 8years. The estimated mean survival time for the womenwho died from breast cancer was 2.52 years in the studygroup and 2.42 years in the control group.
There was 0.1 years shorter survival among the cases whodied from breast cancer in the control population than inthe study population. Thus, five (1.7%) of the women in thestudy group who died from breast cancer were older than74.9 years at diagnosis during the study period. They shouldhave been 75 years or older if the diagnosis had not beenmade earlier by mammography assuming the same lead timefor every woman.
All calculations were done using the program S-Plus[17].
Year
Mor
talit
y/10
0,00
0
1975 1980 1985 1990 1995
050
100
150
Mortality 70-84 years, Study groupMortality 70-84 years, Control group
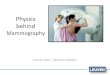
Fig. 3. Annual breast cancer mortality per 100,000 (UCD), 1974–1998 for women 70–84 years at death in the study group and the control group. In thecontrol group, a part of the target population for the Stockholm trial (14% of the control group) had to be included. The trial, which invited womenaged up to 65 years, started 1981 and invited its control group from 1985.
3. Results
For the study and the control group, the annualage-specific breast cancer mortality in age group 70–84years are shown inFig. 3. From 1974 to 1998 there has beena decrease in the breast cancer mortality for both the studyand the control group. However, it was more pronounced inthe study group during the study period.
3.1. Refined excess mortality
During the study period 1986–1998 there were 683 deathsamong breast cancer patients observed in the study cohortsand 256 in the control cohorts (Table 2). Based on the to-tal age and county specific mortality and the person-yearsamong the breast cancer cases, totally 12,056 in the studycohorts and 3651 in the control cohorts, the expected num-ber of deaths was 371.7 and 105.5, respectively. This givesthe excess number (O− E) of deaths, 311.3 and 150.5, re-spectively.
The cumulative breast cancer excess mortality per100,000 at 12 years in the study period was 299 and 311for the study group and the control group, respectively(Fig. 4B). The relative risk for the study group compared tothe control group was 0.96 and the 95% CI 0.73–1.25. Inthe reference period, the figures were 382 and 328, respec-tively (Fig. 4A). The relative risk in the reference periodwas 1.17. Hence, the RR adjusted for the reference periodwas 0.82 and the 95% CI 0.57–1.19 (Table 3).
The data were also fitted in a multiplicative Poisson model(Table 4). Three covariates were found to be statistically sig-nificant, namely 3-year follow-up intervals (P < 0.001), age

366 H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369
Table 2Number of deaths, person-years, expected and excess number of deaths in the breast cancer cases and person-years in all women in the cohorts (70–74years at diagnosis and according to the refined mortality model)
Group Period Breast cancer cases All women
Total numberof deaths
Person-years× 1000
Expected numberof deaths
Excess numberof deaths
Total number ofperson-years× 1000
Study cohorts Reference 611 6.9 241.0 370.0 1162.8Control cohorts Reference 258 3.3 112.4 145.6 533.4Study cohorts Study 683 12.1 371.7 311.3 1251.3Control cohorts Study 256 3.7 105.5 150.5 580.1
Fig. 4. Cumulative number of breast cancer deaths per 100,000 (refined mortality) for women 70–74 years at diagnosis for the study group (S) and thecontrol group (C) by year since start of follow-up. Excess mortality: (A) reference period, (B) study period Breast cancer mortality; (UCD): (C) referenceperiod, (D) study period.
Table 3Summary of results on refined breast cancer mortality using excess mor-tality and underlying cause of death (UCD) as outcome measures
Model RR 95% CI Adj RRa
Cumulative excess mortality 0.82 0.57–1.19 0.76Excess mortality, Poisson 0.84 0.59–1.19 0.78
Cumulative UCD 0.97 0.73–1.28 0.94UCD, Poisson 0.96 0.73–1.28 0.93
RR: relative risk, CI: confidence interval, UCD: underlying cause of deatha RR adjusted for inclusion bias and lead time bias.
at follow-up (P < 0.001) and geographical area (P = 0.02).The estimated relative risk due to invitation to screeningfrom this model was 0.84 (95% CI 0.59–1.19) (Table 3).
3.2. Refined breast cancer mortality based on underlyingcause of death (UCD)
During the study period 1986–1998, there were 325 breastcancer deaths (UCD) observed in the study cohorts and 146in the control cohorts. The cumulative number of breast can-

H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369 367
Table 4Summary of fitting multiplicative Poisson models to estimate refined breast cancer mortality using excess mortality and underlying cause of death (UCD)as outcome measures
Cause of death Model Terms included inthe model
Degree offreedom (d.f.)
Deviance Comparedmodels
Difference indeviance
Differencein d.f.
P-value
Excess mortality Null 365 508.6 –1 Years of follow-up 362 453.3 Null–1 55.3 3 <0.0012 1 + age at follow-up 360 410.9 1–2 42.4 2 <0.0013 2 + time period 359 407.6 2–3 3.2 1 0.074 3 + geographical area 337 371.0 3–4 36.6 22 0.025 4 + screening 336 370.0 4–5 1.0 1 0.32
UCD Null 365 523.6 –1 Years of follow-up 362 447.7 Null–1 75.9 3 <0.0012 1 + age at follow-up 360 394.5 1–2 53.3 2 <0.0013 2 + time period 359 393.7 2–3 0.8 1 0.374 3 + geographical area 337 358.6 3–4 35.1 22 0.045 4 + screening 336 358.5 4–5 0.1 1 0.79
cer deaths and cumulative breast cancer mortality by geo-graphical area and period are given inTable 1and the cu-mulative breast cancer mortality for the study group andthe control group in the two time periods are illustratedin Fig. 4C–D. The cumulative breast cancer mortality per100,000 at 12 years was 312 and 302 in the study periodfor the study group and the control group, respectively. Thecorresponding figures for the reference period were 337and 317, respectively. Hence, the adjusted relative risk inthe screening group was 0.97 and the 95% CI 0.73–1.28(Table 3).
The UCD data were also fitted in a multiplicative Pois-son model (Table 4). Three covariates were found to bestatistically significant, namely years of follow-up (P <
0.001), age at follow-up (P < 0.001) and geographical area(P = 0.004). The estimated relative risk due to invitationto screening from this model was 0.97 (95% CI 0.73–1.28)(Table 3).
3.3. Adjustment for inclusion and lead time biases
The expected number of breast cancer deaths in the studygroup due to cases diagnosed before invitation was estimatedat 76.8. This gives an adjustment of the RR based on excessmortality from 0.82 to 0.77. The corresponding adjustmentfor the UCD changed the RR from 0.97 to 0.96. Allowancefor lead time bias reduced the RR 1.7% to 0.76 and 0.94 forexcess mortality and UCD, respectively (Table 3).
4. Discussion
In the present study, the effect of service screening of agegroup 70–74 years on a routine basis has been studied. Weare not aware of any obvious differences in quality indicatorssuch as attendance rates, recall rates, screening intervals,cancer detection rates, etc. between service screening andthe randomized trials in this age group[18,19]. There are,
however some other possible sources of bias, relevant forstudies of service screening, not mentioned earlier, to takeinto consideration.
If women in the control group had a mammogram on theirown initiative, there is a possibility that the observed ef-fect on mortality reduction could have been diluted. Oppor-tunistic screening in Sweden is a phenomenon that mainlyappears in large cities[20]. Stockholm is the only largecity in the control group and constitutes 66% of the con-trol group. We believe that opportunistic screening is lessfrequent among older than among younger women.
The total breast cancer mortality time trends (Fig. 3) weresimilar in both groups except for a lower level in the studygroup from the late 1980s. However, the refined mortality in-dicates, for both outcome measures, a difference during thereference period towards a higher breast cancer mortality inthe study group. The impact of adjustment for refined mortal-ity in the reference period was substantial for the estimates ofrelative risk. Therefore, we believe that the adjustment wasjustified although the confidence intervals became wider.The difference in the reference period could indicate differ-ent background mortality in the study and control groups.
The discrepancy between the number of breast cancerdeaths in the defined cohorts (refined mortality) and the morecommonly used total mortality for 70–84 or 75–84 years atdeath is considerable. In a study of the effects of screeningin age 50–69 years on breast cancer mortality[10] only 27%of the deaths in the total mortality of women 50–79 years atdeath consisted of cases valid in the refined mortality modelafter 11 years of follow-up. Thus, especially when evaluatingscreening effects in certain age intervals, total mortality canbe insufficiently discriminative for effects of screening.
We have used two methods in measuring breast cancermortality; individual underlying cause of death coded by theNational Cause of Death Registry and excess mortality. Us-ing individual data, it can be difficult in many cases to de-cide whether breast cancer is an underlying cause of death.The degree of complication increases by increasing age due

368 H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369
Fig. 5. Ratio of the number of breast cancer deaths (UCD) (numerator) and excess mortality (EM) (denominator) by age groups in the invited group(IG) and the control group (CG) from the paper by Larsson et al.[21].
to intercurrent diseases[14]. Excess mortality compares ob-served and expected mortality among breast cancer patients.It is therefore a measure of all mortality caused from breastcancer. In the latest overview of all Swedish randomizedstudies these two measures were compared[21]. In the agegroup 70–74 years at randomization a 16% non-significantexcess breast cancer mortality reduction was seen after amean individual follow-up of 11–12 years. The correspond-ing relative risk was 1.05 when using UCD, thus a differ-ence of 21%. The corresponding difference for the age group50–69 years was 3–4%. In the present study, the differencebetween the two measures was 10–13%.
A possible explanation for these differences could be thehigher incidence of breast cancer in the study group dueto screening. For some of the deceased breast cancer casesin a population it may be difficult to decide whether theunderlying cause of death was breast cancer or not. However,for some of these cases the decision by the clinician wouldbe breast cancer. On the other hand, if the same populationhad been screened the number of breast cancer cases wouldhave been increased. If among this increment some deceasedsubjects also had caused decision problems there will be apossibility for a differential bias of overestimation of thenumber of breast cancer deaths in the study population.
Using data from the paper mentioned above[21] the ratiobetween the breast cancer mortality (UCD) and the excessmortality from breast cancer for different ages at random-ization is shown inFig. 5 for the invited and the controlgroup, respectively. The breast cancer mortality (UCD) washigher in the study group for all ages and the difference wasmost pronounced in the age group 70–74 years. This sug-gests that breast cancer mortality using UCD may be lessvalid when comparing a screened group with a group whohad not been screened especially in women over 70 years.Thus, the relative risks using UCD might be biased.
To summarize, with a mean screening interval of 22.8months and with a mean follow-up time of 10.1 years of thecounty based Swedish service-screening program for womenof age 70–74 years, the reduction of the breast cancer excessmortality was estimated to be 18% when compared to thecontrol group. Using the breast cancer mortality based onindividual cause of death the corresponding result was 3%.Adjusting for the inclusion of cases in the study cohorts di-agnosed before invitation and for lead time bias, the reduc-tion was 24 and 6% for excess mortality and breast cancermortality (UCD), respectively (Table 3).
Acknowledgements
The present study was supported by the Swedish Can-cer Society and the European Commission. The authorsare indebted to the responsible radiologists in the respec-tive screening centers who gave us valuable and necessaryinformation by kindly answering the questionnaire; A.-M.Berggren, P. Bordas, S. Cederblom, J.-O. Englund, B. Ep-stein, E. Frodis, B. Heddson, H. Håkansson, J. Johanson,M. Kubista, M. Löfgren, T. Mathiesen, Z. von Pàlffej, L.F.Samuelsson, H. Svensson, P.-Å. Svensson, M. Tholin, E.Thurfjell, K. Yde.
References
[1] Tabár L, Fagerberg CJG, Gad A, et al. Reduction in mortality frombreast cancer after mass screening with mammography: randomisedtrial from the Breast Cancer Screening Working Group of the SwedishNational Board of Health and Welfare. Lancet 1985;1:829–32.
[2] Nyström L, Rutqvist L, Wall S, et al. Breast cancer screeningwith mammography: overview of Swedish randomised trials. Lancet1993;341:973–8.

H. Jonsson et al. / Cancer Detection and Prevention 27 (2003) 360–369 369
[3] Hwang ES, Cody III HS. Does the proven benefit of mammographyextend to breast cancer patients over age 70? South Med J1998;91:522–6.
[4] Kopans DB. Screening mammography in women over age 65. J.Gerontol. 1992;47(Spec. No.):59–62.
[5] Hakama M, Pukkala E, Söderman B, et al. Implementation ofscreening as a public health policy: issues in design and evaluation.J Med Screen 1999;6:209–16.
[6] Lenner P, Jonsson H. Excess mortality from breast cancer in relationto mammography screening in northern Sweden. J Med Screen1997;4:6–9.
[7] Tabár L, Vitak B, Chen HH, et al. Beyond randomized controlledtrials. Cancer 2001;91:1724–31.
[8] Thurfjell EL, Lindgren JAÅ. Breast cancer survival rates withmammographic screening: similar favourable survival rates forwomen younger and those older than 50 years. Radiology1996;201:421–6.
[9] Jonsson H, Törnberg S, Nyström L, et al. Service screening withmammography in Sweden: evaluation of effects from screening in age40–49 years on the breast cancer mortality. Acta Oncol 2000;39:617–23.
[10] Jonsson H, Nyström L, Törnberg S, et al. Service screening withmammography of women aged 50–69 years in Sweden: effects onmortality from breast cancer. J Med Screen 2001;8:152–60.
[11] van Dijck JA, Verbeek AL, Beex LV, et al. Breast-cancer mortalityin a non-randomized trial on mammographic screening in womenover age 65. Int J Cancer 1997;70:164–8.
[12] Tabár L, Vitak B, Chen HH, et al. The Swedish Two-Countytrial twenty years later: updated mortality results and new insights
from long-term follow-up. Radiol Clin North Am 2000;38:625–51.
[13] NBHW. Mammographic screening for early detection of breast cancer(in Swedish). Stockholm: The National Board of Health and Welfare;1986.
[14] Nyström L, Larsson L-G, Rutqvist LE, et al. Determination ofcause of death among cancer cases in the Swedish randomizedmammography screening trials: a comparison between officialstatistics and validation by an endpoint committee. Acta Oncol1995;34:145–52.
[15] Hakama M, Pukkala E, Heikkila M, et al. Effectiveness of the publichealth policy for breast cancer screening in Finland: population basedcohort study. Br Med J 1997;314:864–7.
[16] Breslow NE, Day NE. The design and analysis of cohort studies.Lyon: IARC; 1987.
[17] Venables WN, Ripley BD. Modern applied statistics with S-PLUS,2nd ed. New York: Springer; 1997.
[18] Lidbrink EK, Törnberg SA, Azavedo EM, et al. The generalmammography screening program in Stockholm. Acta Oncol1994;33:353–8.
[19] Thurfjell E. Mammography screening: methods and diagnosticresults. Thesis. Uppsala: Uppsala, Sweden; 1995.
[20] Törnberg S. A survey on mammography examinations performed inprivate clinics during the period 1992–1993 (in Swedish). Stockholm:Socialstyrelsen; 1994.
[21] Larsson LG, Nyström L, Wall S, et al. The Swedish randomisedmammography screening trials: analysis of their effect on thebreast cancer related excess mortality. J Med Screen 1996;3:129–32.