Embed Size (px)
Citation preview

THE INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT
Int J Health Plann Mgmt 2011; 26: 449–470Published online in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/hpm.1112
Serve the people or close the sale? Profit-drivenoveruse of injections and infusions in China’smarket-based healthcare system
Lucy Reynolds and Martin McKee*European Centre on Health of Societies in Transition, London School of Hygiene and TropicalMedicine, Keppel Street, London, WC1E 7HT, United Kingdom
SUMMARY
Treatment by injection or infusion is widespread in China. Using the common cold as a tracercondition, we explored the reasons for over-prescription of injections and infusions inGuizhou, China. Interviews with prescribers, patients and key informants were supplementedby focus groups. These revealed how historical ideas encourage unnecessary use of percutane-ous treatment: faith in the healing power of needles is locally attributed to association withacupuncture. Many patients and some staff believe that injections per se are therapeutic. How-ever, the structure of health service financing and remuneration now reinforces this irrationalfaith. Market-based reforms have attempted to control costs and increase productivity with anincentive scheme which rewards prescribers financially for over-prescription in general andfor use of injections and infusions in particular. Aggressive marketing has displaced oral treat-ment from health facilities into independent pharmacies, leaving doctors functioning mainly asinjection providers. There is a need for a multi-faceted response encompassing education andreform of financial incentives to reduce the use of unnecessary treatment. Copyright © 2011John Wiley & Sons, Ltd.
KEY WORDS: China; utilisation; health financing
INTRODUCTION
Infection with blood-borne viruses is a major problem in China. In 2008, for the firsttime, deaths attributed to HIV exceeded those from any other infectious disease(Xinhua, February 2009). Although general HIV prevalence is low at 0.05%(UNGASS, 2008), rates are high in some most-at-risk groups: a recent systematicreview that brought together 40 studies reported overall HIV prevalence rates of12.6% in Chinese intravenous drug users, together with hepatitis C prevalence of67.0% (Bao and Liu, 2009). Hepatitis B is endemic, with a carrier rate of 7.2% inthe general population (Lu and Zhuang, 2009), although this prevalence has fallen
*Correspondence to: Martin McKee, European Centre on Health of Societies in Transition, London School ofHygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK. E-mail: [email protected]
Copyright © 2011 John Wiley & Sons, Ltd.

450 L. REYNOLDS AND M. MCKEE
from 10% following the introduction of universal childhood immunisation in 1992(Liang et al., 2009). Several factors play a role but among them is the high preva-lence of unsafe injections, with one recent survey of rural residents in central Chinareporting that almost a third had received at least one injection in the previous3months (Yan et al., 2007).As part of a larger study of risk factors for blood-borne virus transmission in
southern China, we sought to understand the health beliefs, preferences and practicesof patients and health professionals that might give rise to the high use of injectionsand intravenous (IV) infusions. In other papers, we have described the factors influ-encing overuse of antibiotics (Reynolds and McKee, 2009) and the risks associatedwith acupuncture (Reynolds and McKee, 2008) and blood transfusion (Reynolds andMcKee, 2010). In this paper, we use one common condition that does not requireinjections or infusions, the common cold, as a tracer condition to understand thebeliefs and the play of incentives that underlie the widespread and inappropriateuse of injections or infusions. The appropriate treatment for a common cold issymptomatic, involving rest, fluids to maintain hydration, gargling with warm saltwater, and cough drops, throat sprays or over-the-counter pain or cold medicines.Antibiotics and antiviral drugs are ineffective, and their use increases the risk thatother micro-organisms will develop resistance.
METHODS
The research was set in Guizhou, a landlocked, relatively poor province in southernChina, bordered by Sichuan and Chongqing to the north, Yunnan to the west,Guangxi to the south and Hunan to the east. Much of the province is mountainous,with forestry and coal mining dominating the economy.Semi-structured interviews were conducted with patients, health workers and
other key informants in rural and urban areas of the province. An interview guideprovided structure for data collection with questions on knowledge, attitudes andpractices related to infection control and on use of injections and infusions. Issuesarising in early interviews were tested in subsequent ones to assess their generalisa-bility. Sampling was purposive, to include health workers and patients at provincial,county and village facilities (Table 1).The professional informants targeted at each level were the following: village—
village leader, one-child family official and village doctor; county—hospital direc-tor, clinicians, officials in charge of safety and sterilisation and Centre for DiseaseControl staff; provincial—as at county level plus hospital administrators. Fiveother key informants working in local medical services were also interviewed. Threevillages were selected to include different levels of economic development and typesof village health provision. Village 1 was easily commutable from the provincialcapital and so was relatively wealthy. Villages 2 and 3 were both too far away tomake commuting feasible so they were much more dependent on local endeavoursand thus poorer. All villages were farming communities, but villages 2 and 3 wereprimarily economically dependent on farming whereas some people in village 1worked in the provincial capital. Village 3 had a bottle factory which employed some
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

Table 1. Categories of interviewees
Category Number of informants
Patients Rural patients 15Urban patients 9
Prescribers Village doctors 11Township hospital staff 4County hospital staff 7Provincial hospital medical staff 12Other local state system medical personnel 2Private sector healthcare workers 2NGO healthcare worker 1Expatriate health worker, Mandarin-speakinglong-term local resident
1
Key informants One-child family officials 3*Village leaders 2*Provincial hospital administrative staff 3CDC staff at provincial and county levels 3NGO healthcare worker 1Independent pharmacists 2Expatriate health workers, Mandarin-speakinglong-term local residents
2
Total 80*
CDC, Centre for Disease Control.*Officials were also interviewed in their capacity as health service users.
451SERVE THE PEOPLE OR CLOSE THE SALE?
local people; village 2 had a brick factory, but the work there was very unpleasantand involved only migrant workers from elsewhere and was the poorest of the three.As is usual in China, all three villages had a substantial portion of their young menand some young women resident elsewhere and remitting a portion of their earningsto the villages, but it was not possible to quantify this. The clinics in two of thevillages offered acupuncture as did county and provincial hospitals. All interviewswere carried out by L. R. in English with a local research assistant who was fluentin Mandarin and the local dialect. Immediately after each interview, they checkedtranscripts together to resolve any ambiguities. The transcriptions were read andanalysed by both authors to identify emerging themes. These themes were then exploredin more detail with key informants with knowledge of the Chinese health system. Anaudit trail was maintained using field notes and related materials. It included theuncoded transcripts, field observation notes, notes on working hypotheses, diagramsshowing how the different themes related and notes about trustworthiness andmotivations (Ulin et al., 2005).
Eighty interviews were undertaken altogether; the relatively small number in eachcategory had the advantage of allowing issues to be explored in considerable depth;the disadvantage was that the sample could not be considered as fully representative,so to avoid giving an impression of spurious precision, we have not quoted percen-tages expressing different views but instead have indicated whether such views werewidely held or exceptions.
The tracer method offers a means of exploring issues surrounding the deliveryof medical care (Sanderson, Bosch et al., 1987) and has previously been used to
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

452 L. REYNOLDS AND M. MCKEE
understand the customs and incentives relating to injections in Thailand (Reeler andHematorn, 1978) and in a study that assessed the extent and nature of over-treatmentin Chinese hospitals (Liu and Mills, 1999). In that study, the authors defined unnec-essary care as ‘care provided but medically not needed’ or that ‘on balance. . . doesnot benefit patients’, a definition that we also use. By focusing on the management ofa single, common, well-defined condition, it is possible to elicit information aboutthe motivation of those involved in the clinical encounter as they decide on a courseof action, while placing the information they provide within a broader understandingof the literature on health-seeking behaviour, clinical judgement and health systems.Patients were asked about what treatment they had taken for past episodes of thecommon cold, whereas doctors were asked about the treatments they usually pre-scribed. A series of focus groups was carried out to explore further certain issuesarising from the interviews (Table 2). Additional information was gathered fromnaturalistic observation of encounters between health workers and patients and ofthe routine work in health facilities.To place the findings in a broader context, and to assess whether they were atypical,
the findings were discussed with clinicians and researchers at the National Workshopon Rational Use of Antibiotics in China held in Beijing on 28–30 November 2005.
RESULTS
Explaining the disease
Colds were generally attributed to cold and windy weather, particularly to beingcaught with inadequate clothing in cold or wet weather, although two informantsattributed colds to excessive heat. A meteorological aetiology was identified bydoctors and patients, although two of the eight doctors also cited viruses, as didtwo of the 24 patients. Two doctors and one patient mentioned low immunity orbeing run-down, and two doctors blamed air pollution.
Treatments preferred by patients
Only two patients considered colds to be a minor irritation, needing no specific treat-ment. Most used traditional folk medicine, involving a therapeutic sweat invoked by
Table 2. Composition of focus groups
Participants Subject area
County CDC officials Overview of study area and planned work, HIV/AIDS responsein China
Village doctor patients Views on healthcare servicesVillage doctor group Local socioeconomic conditions, public health work in the
communityUniversity students,county town
Role of advertising of pharmaceuticals in health-seekingbehaviour
Provincial hospitalpharmacists
Procedural and legal constraints on prescription
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

453SERVE THE PEOPLE OR CLOSE THE SALE?
consuming ginger or chillies, exercising or piling blankets on the patient. Cutting theskin or the veins to release some blood and pinching and patting the skin on the chestand shoulders were also cited by many. These treatments are performed by familymembers and community elders rather than by professional traditional Chinesemedicine (TCM) practitioners. Many patients self-medicate, using branded over-the-counter cold remedies that typically contain combinations of pseudoephedrine,paracetamol, caffeine and the antiviral amantadine. Local pharmacies carry bothwestern mass-market products such as KanTaiKe (‘Contact’) and domestic brands.There was a high level of awareness of these preparations, which doctors attributedto widespread direct-to-patient advertising. One doctor commented: ‘Another bigproblem is medical advertising on TV, radio and in newspapers. If you pay to placean advert, you can cheat people.’ Q. Is there no regulation of these? A. There is, butthe regulations are not enforced.
A focus group of urban students reported that ‘people follow advertisements andbuy medicines for minor illness accordingly’. They cited television, newspapers andmagazines as the most influential media and listed the most memorable advertise-ments for cold treatments to be KuaiKe, GanKang (both paracetamol/amantadine),Baijiahei and KanTaiKe (both pseudoephedrine), all preparations identified byour interviewees. Some also purchased prescription-only drugs, such as antibiotics,with pharmacists circumventing the requirement for a prescription by employingdoctor-prescribers.
Only if the pills bought ‘do not work’, with symptoms continuing for more than aday or two, will the patient visit a clinic, where they will typically receive an injec-tion or the ‘strongest medicine’, an infusion. Except for penicillin, named by severalrespondents, patients were unaware of the treatment they received from physicians;it is unusual for the doctor to inform the patient or for the patient to ask what theyhave been prescribed. Instead, patients classify treatments in terms of the visibledifferences in their delivery, as if this were the key therapeutic process.
Injected treatment is considered necessary if the cold is ‘serious’. Several intervie-wees explained ‘serious’ in terms of the intensity or duration of symptoms; concernwas sometimes expressed that a ‘serious’ cold could ‘go to the lungs’ and kill.Hospitalisation is common if infection does spread to the chest or if symptoms lastover a week. Children are seen as especially vulnerable; an outpatient doctor inthe County Hospital reported how adults who will endure their own colds take theirchildren for infusions if they fall ill. In the present study, all three patients waiting inthe County Hospital Emergency clinic at 11 AM one day were children with coldsawaiting injections; one had already received several injections of penicillin.
The common cold: a major component of medical workload
Colds form a major component of workload in outpatient clinics at every level of thesystem and in both public and private sectors. Doctors were asked to estimate howmany patients they saw with colds each month. Village doctors reported between20 and 135 cases, varying with the weather, whereas staff at the County Hospitalsaw 10 to 60, with about 10 admissions to hospital. Staff at the Provincial Hospitaloutpatient department reported seeing 120 to 240 cases each month; on one
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

454 L. REYNOLDS AND M. MCKEE
randomly selected day, a review of diagnoses recorded in the prescriber’s register atthe Ear, Nose and Throat clinic revealed that 30% of patients attended because ofcommon cold. However, in urban areas it is reported that most patients visit smallprivate clinics on grounds of cost and convenience: a private doctor reported seeing300 to 400 cases of common cold per month at one clinic in a county town.
The views of doctors
Many but apparently not all doctors are aware that a cold is a self-limiting viralinfection. Some doctors share the lay belief that exercise will sweat out a cold. Manyadvise drinking more water, which seems wise advice given the widespread use ofsweating ‘cures’. However, most prescribe antivirals (usually ribavirin or acyclovir),antibiotics or both, sometimes combined with symptomatic relief, as well as tradi-tional Chinese medicines formulated as pills and injectables. Most doctors believethat antibiotics are effective against colds. Of the minority who know that they areineffective, most still prescribe them, typically citing patient demand.Nearly all doctors in the public sector commonly prescribed the antiviral ribavirin,
as did one of two private physicians (see Table 3). One reason for the widespread useof ribavirin seems to be the controls on prescribing antibiotics. As a County Hospitaldoctor noted: ‘When the patient comes to this hospital the doctors take a history todiagnose whether it is viral or bacterial, but because abusing antibiotics is socommon, doctors in this hospital are not allowed to prescribe antibiotics randomly.So they treat first with an antiviral, and if the patient is not cured after two or threedays, then they use antibiotics.’Doctors often combine western and Chinese systems of medicine. For instance, a
village doctor explained: ‘It depends on the season: colds are because of the wind inall seasons, but I prescribe more antivirals in winter. I also prescribe medicines toease the headache and pain: GanKang, ribavirin granules for children or IV infusionfor adults, and Kanbing gankeli [TCM remedy].’Traditional Chinese medicine practitioners are encouraged by the government to
combine acupuncture and herbal treatments with western medicine. One TCMspecialist working in a village used ribavirin to complement traditional treatment:Q. ‘Would you always use injected ribavirin, or would you use pills too?’ A. ‘I thinkif the cold is viral, it is best to use herbs for the inside of the body and ribavirininjection for the outside [this outside/inside distinction relates to the yin/yang
Table 3. Use of ribavirin in treating common cold
Usage
Usage for common cold by
Rural healthcareworkers
Countyhospital
Provincial referralhospital
First line treatment 2 1Serious cases only 1 1 2Not stated 1
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

455SERVE THE PEOPLE OR CLOSE THE SALE?
system]. Oral ribavirin is less useful, because some children are quite sensitive towestern pills, and it doesn’t work on some and can lengthen the duration of thedisease. If the pills haven’t worked in three hours, they won’t work.’
The TCM pharmacopoeia contains a number of symptomatic treatments, suchas mahuangsu (Ephedra), containing ephedrine, as prescribed at the ProvincialHospital. Some providers made reference to TCM ‘antivirals’ shuanghuanglian,banlangen and yinqiao. However, treatment of specific pathogens does not featurein TCM as the germ theory only arose in the 19th century: TCM aims to resolvesymptoms and correct underlying metabolic imbalances but does not specificallyaddress infections.
Oral versus percutaneous treatment
Given the frequent use of percutaneous treatment, the relative values placed on thesetreatment modes were investigated in detail with doctors and patients.
Doctors were asked ‘what are the benefits and disadvantages of each kind of treat-ment for the patient and for you?’ Table 4 contains illustrative examples of positiveand negative assessments; interviewees had much more to say in favour of percuta-neous administration, with a clear consensus that injections and infusions are the bestmedicine. Injected medication was preferred because of its speed of action, demandfrom patients and the large volume of fluid available to carry medication. Someexplicitly noted how administration of injections and infusions visibly demonstratedprofessional skills, important in building a successful practice. Doctors reportedpatient dislike of oral treatment because of its reputed slow action, gastric irritationand the bitterness of TCM decoctions.
Positive comments on oral medication included convenience, safety and lowerprice. Negative comments about injectables included the potential for pain, sideeffects and iatrogenic infection. Many practitioners commented that percutaneoustreatment was essential for ‘serious’ colds, with pills suitable only for mild cases,whereas IV infusions were reserved for the worst cases. Timing was also a factor.Two doctors commented that patients did not want oral medication because by thetime they sought professional help they had already exhausted that option. Further-more, by the time they are sufficiently ill to visit a hospital, they are in considerablediscomfort and seek the swiftest relief possible. This was consistent with findingsfrom the 2004 Third National Public Health Service Survey, which reported declin-ing usage of public medical services, with 36% of Chinese buying medicine at apharmacy without seeing a doctor (Lu, 2005), half of whom justified this as time-saving; 35% trusted their own diagnoses, and 15% felt that hospitals overpricedmedicines (Table 5). In general, the views of patients mirror those of doctors. Table 6contains illustrative responses to the question ‘What are the advantages and disad-vantages of oral treatment and injectable treatment?’ Patients are even more stronglyin favour of percutaneous medication than physicians, with two urban patients arguingthat injections cannot damage the body, whereas pills can. Disadvantages ofpercutaneous treatment were ignored, aside from one mention of pain, with pillsappreciated only for their convenience and lower cost. Most patients interviewed saworal medication as inferior to injections and infusions, acting more slowly and causingswallowing or gastric problems.
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

Table 4. Healthcare worker statements on relative benefits of oral and percutaneous medicine
Oral Percutaneous
Positive Townshipdoctor
Pills are convenientand involve no pain
Villagedoctor
Injections give quickrecovery because they hitthe bloodstream faster
Townshipdoctor
My experience frommany years’ practiceis that more peoplelike taking pills
Villagedoctor
In an injection or aninfusion, the medicine isabsorbed directly. Oralmedication is absorbedonly incompletely by thestomach. Infusions arebetter than injections;you can use a higherdosage because fluidcapacity is not a limitingfactor
Townshipdoctor
Pills are safer andcheaper
Villagedoctor
Infusion is very fast,especially forrehydration. Infusionspenetrate through thebody swiftly
Townshipdoctor
Injections and infusionsare faster and betterbecause they areabsorbed more efficiently
Townshipnurse
It is hard to changepatients’ idea thatinjections are better andfaster than pills
Townshipdoctor
For diarrhoea, you canuse IVs to supplementfluid levels if the patientcannot drink
Privatedoctor
Patients prefer infusionsdue to their fast action
Provincialprivateclinic
IV is even faster thaninjections because it goesstraight into the bloodrather than beingabsorbed via muscleWhen do you use IVinfusions in place ofinjections?It depends on thedisease or the problem.They are especiallygood for ganmao fever
UrbanTCMdoctor
Some patients think adoctor who doesn’t injectlacks full professionalskills. Some think thatwith an injection their
(Continues)
456 L. REYNOLDS AND M. MCKEE
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

Table 4. (Continued)
Oral Percutaneous
disease will disappearfasterIs this just the half-hourlag for the medication tohit the bloodstream?I think this is apsychological effect,perhaps an irrationalbelief
Negative Villagedoctor/OCF
Some patients hate thebitterness of infusionsmade from Chineseherbs. Oral medication isslower and may damagestomach or intestines,e.g. cold medicines
Townshipdoctor
Injections and infusionscause pain. I have seenvery few cases of sideeffects, and have had noproblems with infectionsfrom injections andinfusions
Townshipdoctor
Some patients may beafraid of taking pills asthey think they maydamage their stomachs ormake them want to vomit
Townshipdoctor
If pills can cure thepatient, I won’t giveinjections or infusions, asthey have disadvantagesincluding pain andinfection risks. We alwaysuse disposable equipment,but some patients are stillscared. We have strictrules on purchase and useof injecting equipment toblock reuse, againsttransmission of AIDS orother blood diseases.Patients are afraid of painmore than infection, butnow know about AIDS
Which pills do this?It could be a psychologicalthing for themDo any pills actuallydamage the stomach?Mainly aspirin and somepainkillersIs this fear linked toproblems with aspirinetc. or does it come fromsomewhere else?I think it is acombination
Townshipnurse
In many patients’ minds,pills are very slow
Villagedoctor
Some people areallergic
Townshipdoctor
Pills are slower, but noother disadvantages
Townshipdoctor
They often vomit afterthe salt and sugar watertreatment for diarrhoea
OCF, “One-child family policy” official.
Table 5. Percentage of people buying medicine at a pharmacy without seeing a doctor
% in 1998 % in 2004
ural 23 31rban 44 47otal 36
457SERVE THE PEOPLE OR CLOSE THE SALE?
RUT
Source: Third National Public Health Service Survey.
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

Table
6.Patient
statem
entson
relativ
ebenefitsof
oral
andpercutaneous
medicine
Oral
Percutaneous
Positive
OCF/
village
doctor
Personally,Iprefer
pills
Rural
patient
Percutaneousmedicationisquickerthan
oral
medication,
becauseittakestim
eformedicinegivenby
mouth
toreach
theblood
Urban
patient
Pillsarecheap
Rural
patient
Taking
pills
hasno
effecton
me.Imusttakepenicillin
injections
orthereisno
effect
Urban
patient
Itdependson
your
situation.
Ifyoutake
pills
andfeel
healthythen
that
isenough.T
headvantageisthat
they
can
restoreyour
health
quickly
Rural
patient
The
treatmentforacold
isusually
anIV
drip.Injections
aretooslow
,so
Iprefer
adrip
Urban
patient
Infusion
isbest.Itworks
quickly
Any
otherreason?
No
Urban
patient
Injections
workmorequicklythan
pills,andcannot
damageyour
body.Ifyouaretired
anddon’tknow
why,
thedoctor
will
give
youan
infusion,to
makethe
inflam
mationin
your
body
feelbetter.Maybe
infusion
can
help
youhave
agood
appearance,e.g.
good
moodand
refreshed.
Ifthereisalack
ofbloodin
your
head,maybe
infusionscanhelp
Negative
Rural
patient
Iprefer
IVdrips,especially
forcolds.Idon’tlikeoral
medicineso
much;
it’s
notas
good.Itisvery
slow
and
doesn’twork
Urban
patient
Isthereanydisadvantage
toan
infusion?
Itmay
bepainful
OCF/
village
doctor
Somepeoplefind
itvery
hard
tosw
allowthetablets;
thereforethey
prefer
injections,especially
oldpeoplelikemy
mother.Sherefusesto
take
pills
Whatistheproblem
with
pills?
Somearetoobigandsometoobitter
Urban
patient
Iprefer
IVinfusions,becausemytreatmentw
asfor
inflam
mationof
thestom
achlin
ing,andherb
decoctions
(Con
tinues)
458 L. REYNOLDS AND M. MCKEE
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

Table
6.(Contin
ued)
Oral
Percutaneous
mademefeelsick.W
estern
medicineisbetterthroughthe
mouth;Chinese
medicinetastes
reallybad
Urban
patient
The
disadvantage
ofpills
isthat
they
may
harm
thekidneys
orliver
ifyoutake
toomuch.Sometimes
they
donotw
ork.If
youtake
them
foralong
time,they
stop
working
(clarified
asanymedicinein
pillform
will
dothis,not
justantib
iotics)
Urban
patient
Are
thereanyproblemswith
pills?
The
side
effects
Dopills
have
side
effectsthat
infusionsdo
not?
Maybe
askin
allergy
Doyouthinkifthemedicinehadbeen
injected
itcouldnot
causethat?
Yes
459SERVE THE PEOPLE OR CLOSE THE SALE?
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

460 L. REYNOLDS AND M. MCKEE
Many of the reported problems with pills could be due to their excessive con-sumption in the quest for faster or surer recovery. Two respondents made commentsthat illuminate the observations of gastric ill-effects. A non-governmental organisa-tion (NGO) health worker admitted that, despite knowing that this was unwise, healways takes an extra dose of pills if they have not shown immediate effect. Aforeign paramedic married to a Chinese woman recounted: ‘My wife’s aunt is apharmacist and she treats my sinusitis. Last year she gave me some pills with instruc-tions to take three five times each day. I found out from the package that theywere amoxicillin, and I was taking three times the correct dose. They take handfulsof pills here.’The greater speed attributed to injectables is not solely due to their faster passage
into the bloodstream; the act of injection is commonly believed to hasten recoveryby several days. Many patients echoed comments by doctors that percutaneoustreatment was needed for ‘serious’ disease.
Interactions between patients and doctors
It was apparent that there was substantial information asymmetry between doctorsand patients. Doctors apply a rationale to their decisions but do not routinely sharethis with patients. As an expatriate healthcare worker noted: ‘Knowledge is power:medical practitioners will not tell patients what treatment they have received becausedoing so would diminish their expert power. Chinese society is very hierarchical anddoctors are much respected and trusted.’In their review of illness-related behaviour among Hong Kong Chinese, Lau and
Ng (1986) refer to ‘the traditional image of omnipotence and omniscience of everymedical doctor’. Such trust is vulnerable to exploitation when health workers faceorganisational or financial pressure to increase income, which distorts the doctor–patient relationship from one of care to one based on commerce (Ip, 2005). A retireddoctor key informant explained local beliefs about the common cold: ‘This thoughtis due to the doctors: few doctors will tell you the truth of your disease, as it is notprofitable to do so. Therefore they have told patients wrong things. Nowadaysdoctors are not so good—a good doctor will check the patient and if they only havea cold, they should recommend rest and drinking more water. It is rare to do this, butit is the responsibility of a doctor to tell the truth.’There is a widespread belief among Chinese that treatment is available for every
disorder, also noted by anthropologist Arthur Kleinman (1980). An NGO workerproviding health education to rural dwellers reported that: ‘I have just been teachingin the countryside that there is no medicine to cure cold, and villagers should savetheir money. They are so surprised by this idea.’ As a cold is normally self-limiting,the practitioner who treats it benefits reputationally from administering an apparentcure, a situation that encourages over-treatment in the future.Kleinman comments that Chinese healthcare workers know that the administra-
tion of an injection communicates to patients that they are receiving the best treat-ment; patients usually prefer medication to be injected where possible. Hesuggests that this has contributed to Taiwan’s epidemic of hepatitis B: writing inthe 1980s, he noted that almost all the patients with infectious hepatitis that he
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

461SERVE THE PEOPLE OR CLOSE THE SALE?
saw were on intravenous saline or glucose infusions of no medical benefit, generat-ing contaminated sharps. He noted that Taiwanese doctors knew the dangersinvolved but continued treatment to please customers. Research among Hong KongChinese has also noted how injections and infusions are viewed as the best treatmentavailable (Lau and Ng, 1986). Kleinman concluded that ‘in the popular culturalview, injections are the essence of all that is powerful in Western medicine. . . mod-ern, quick to administer and to take effect, powerful but with potential for dangerousside effects’. He dates this ‘magic bullet’ attitude to the advent of antibiotics; themystique then transferred to the injected mode of delivery.
Reeler refers to the ritual and symbolic significance of percutaneous medical proce-dures in many developing countries (Reeler, 1990). During the present study, an expa-triate community health worker suggested an association between acupuncture andlocal enthusiasm for injections, and her local colleague commented on the history ofthese preferences: ‘When the missionaries came, they treated with good medicine. Thisis why people believe in injections. There is also a connection with acupuncture, whichcomes from Taoism. There are myths surrounding Taoist medical practices. Any paincan be cured immediately, although it is likely to come back. Maybe injections are seenas a branch of acupuncture. People think injections are better than pills. Injections pushmedicine into the body’s vessels, but pills only put it in the stomach.’
Many prescribers, especially village doctors with only a few months of medicaltraining, firmly believed that ‘serious colds’ would benefit from the therapeutic ben-efits of injection per se. It seems likely that, in the Chinese context, percutaneoustreatment has a powerful placebo effect. There were, however, other doctors whoknew that injections would not affect the course of the cold but explained that theyprescribed as they did because the patients wanted them to and that the hospitalrequired doctors to please patients. Only one doctor reported taking a principledstand and resisting pressure from patients for an injection or an IV infusion to treattheir cold. Even he still provided antibiotic drips to patients who demanded them,to avoid complaints which would reduce the monthly bonus shared with his collea-gues and damage his promotion prospects.
Overuse of intravenous infusions
Intravenous perfusions are perceived in China as superior to injections. They arelimited to ‘serious’ disease principally because of their extra expense. The modeof delivery often seems more important than their content. For example, during thestudy a village doctor visited an 8-year-old boy with the aftermath of a cold at home.He received the second of 2 days’ treatment with IV infusions in his family’s livingroom. His family said he was expected to return to school the next day. Of the fourIV drip bottles for that day, two contained penicillin, and the other two, differentChinese traditional medicines.
Information from clinicians and patients on fees charged suggested that IV infu-sions are the most profitable basic treatment for providers, although much lower feesare charged for the same services by village clinics and the urban private sector thanby state hospitals. Several respondents linked the use of percutaneous medicationdirectly to the market-based healthcare system, with doctors administering infusions
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

462 L. REYNOLDS AND M. MCKEE
to maximise their income. The provider receives a fee for administering an injectionor infusion, significantly augmenting the permitted profit of 15% on western medi-cine and on the injecting equipment or 30% on TCM preparations (Liu and Li,1997). A city hospital nurse summarised the dynamics: Q. ‘Why are IVs so muchused?’ A. ‘Doctors make a living by charging for IVs, and if patients get no IV, thenthe doctors don’t get a bonus. From the perspective of patients, if the patient cannotget an IV, they will leave the hospital immediately.’Large hospitals manufacture IV fluids in bulk, enabling them to charge high profit
margins. An expatriate health worker reported from her experience in several cityhospitals in Guiyang: ‘IVs are mixed on the premises in hospitals, and sent out ontrolleys to all the wards. Each department is permitted to set its own pricing policy.For example, an IV with a particular antibiotic was 3RMB [21p] on the rehabilita-tion ward, but 36RMB [£2.50] on the surgical ward’.An NGO worker suggested that infusions appeal to patients precisely because they
are the most expensive option and that ‘the IV bottle is big and an injection is small,so IV must be better’. IV and intramuscular injections are also reportedly perceivedas ‘the best medicine’ partly on the basis of their higher cost. Thus, in this contextinfusion can be regarded as a luxury good as demand increases with price. In a paperexamining modern Chinese medical ethics, Ip notes that the commoditisation ofChinese healthcare leads the general public to believe that ‘the quality of the medicalcare depends on the amount of fees charged’ (Ip, 2005).The expatriate healthcare worker quoted above commented on the social construc-
tion of treatment by IV infusion: ‘My local colleagues sometimes say they were illbut have received ‘yanshui’ [salt water : IV saline] and are now feeling fine. Thereis social pressure to have them. Maybe being ill gives attention from familymembers, and having an IV is a socially legitimate reason for a break.’Irrational faith in infusions is strong even among healthcare workers. A nurse said
‘people who have very minor problems have IVs, even doctors and nurses. You cansee lines of scars along the hand veins of many people’. Despite her personal reser-vations about the value and safety of infusions, this interviewee had her son treatedwith them unnecessarily. This deep-seated faith in the use of injections and infusionsmakes overuse difficult to overcome. Thus, at the Provincial Hospital, seniormanagement had worked hard to minimise the use of infusions, but staff concededthat many patients still received them unnecessarily.
Disadvantages of percutaneous treatment
Only two healthcare workers and one patient commented about the pain of injectionsand infusions. When asked about possible risks of injections, the most commonresponse cited anaphylactic shock (doctors in Guizhou have treatment kits contain-ing adrenaline and are required to test skin reactions before using certain injectableantibiotics). Observation in health facilities from village to Provincial Hospitalrevealed strict adherence to rules to prevent cross-infection with all disposableequipment. This is not, however, the case in all parts of China: Yan et al., in a studycarried out in 10 district/township hospitals, 14 village clinics and 14 communityhealth stations in Hubei, found that 16% of 175 injections observed under fieldconditions were unsafe (Yan et al., 2006).
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

463SERVE THE PEOPLE OR CLOSE THE SALE?
In our study, in response to an open question about risks, no patient citedinfection, although some had received injections or infusions from informal provi-ders. Several studies indicate that many Chinese who receive frequent injectionsare unaware of the possible risks (Table 7). Rural people were more likely to reportseeking treatment in the unregulated informal sector, accessed through kinship andfriendship networks. A township hospital doctor cited examples of bacterial infec-tion caused by unlicensed local practitioners.
Medicine as a business
During the market reforms of the 1980s, state financing was cut to cover only basicpersonnel wages and capital investment, totalling around 25–30% of total costs (Liuet al., 2000). Health worker salaries fell behind the cost of living. Bonus schemes,funded from sales of drugs, tests or services (Liu et al., 2000), were established toimprove motivation, with fines for missed financial targets (Zheng and Hillier,1995). These bonuses now provide strong incentives to prescribe more items andmore expensive drugs (Meng et al., 2005).
According to a foreign informant who works in poorer areas of Guizhou, manyvillage doctors now receive no income apart from that generated by sales,although in the study area each practice reported receiving a small allocationfor salaries of 100 RMB [£6.90] per month. Rural hospitals must try to provideadequate services with limited local government funding and an impecuniousclientele. At one township hospital, local government covers building costs, 80% ofsalaries and 30% of the supplement for working in western China. The othertownship hospital reported 80% funding of salaries, with patient fees only ableto increase the salary to 90% of what is specified. Many facilities are, by westernstandards, overstaffed, with doctors underemployed and facing great economicpressure. Both they and their employers often need to sell medicine and servicesin order to survive financially.
Table 7. Awareness of injection risks among patients
Yan,Hubei 2007
Li Q,Chongqing 2003
Cao, Shanghaiarea 2001
Sample size n= 595 n= 199 n= 806% patients unaware of iatrogenictransmission risk for HBV
44 92 34
% patients unaware of iatrogenictransmission risk for HIV
26 87 31
% patients unaware of iatrogenictransmission risk for HCV
77 N/A 72
% patients preferring fever to betreated by injection
N/A 41 14
Number of injections per memberof general population/year
0.93 3.4 4.4
Sources: Cao et al. (2001); Li et al. (2003).
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

464 L. REYNOLDS AND M. MCKEE
Rational treatment under the profit motive
Injectable antibiotics are expensive, and prescribing them is profitable. For instance,‘statistics from the Paediatric Hospital affiliated to Shanghai’s Fudan Universityshow that its three most profitable medicines are all antibiotics’ (Lu, 2005). A doctorasked about this commented: ‘Abuse of antibiotics is common. In the past, antibio-tics were only used for treating high fever, but now they are used for very minordiseases such as common cold, and their effectiveness is decreasing. Most colds willgo away without treatment, but doctors can earn a lot through prescribing antibiotics,because these are expensive.’When we presented our findings to doctors at a national conference on antibiotic
use, those present highlighted the barriers to rational prescribing caused by the exist-ing financial arrangements in hospitals, asserting that a shift to rational prescribingwould take many hospitals below break-even point, leading to a deterioration inquality due to cost-cutting. There is some evidence for this view: introduction ofan approved drug list in Shanghai in 1992–1993 saw the contribution of drugs tohospital revenue drop from 60% in 1992 to 47% in 1993 in one study (Chenet al., 1995) and from 62% to 55% in another (Zhen et al., 1995).
Competition between providers
Because maximising one’s own revenue is a priority, referrals are rare. In any case,as a village doctor said, patients ‘generally do not act on referrals because the countyhospital is too expensive, with high charges for the many tests recommended’.Hospital staff reported a diminishing number of referrals among their caseload:10–15% at the Provincial Hospital outpatients department and ‘very occasionally,if they cannot treat them, if the case seems very serious or if they are unsure whatis wrong’ at the County Hospital. Some patients go straight to the large hospitals,whereas others seek a second opinion on their own initiative. Administration of med-icine by injection has a particular advantage for providers, noted also by Kleinman:once patients are prescribed medication, they may buy it at an independent phar-macy, which may be many times cheaper than the hospital, but if it needs to beinjected, the hospital can ensure that it supplies and profits from it.
DISCUSSION
Limitations
This study has a number of obvious limitations. It was undertaken in a single prov-ince of a vast and extremely diverse country, and the number of interviewees wasrelatively small. There is a clear need to replicate this work in other parts of China.However, the findings were discussed with participants at a national conference,eliciting a consensus that the findings were not atypical. The time required to conductsemi-structured interviews limited the numbers that could be included but also hadadvantages. These included the ability to probe responses fully to clarify any ambi-guities, to obtain information of greater depth and to resolve misunderstandings,
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

465SERVE THE PEOPLE OR CLOSE THE SALE?
while ensuring a high response rate (Bowling, 1997). The narratives elicited fromthose interviewed were consistent with each other and with our observations andreview of relevant literature. The treatments described by providers matched thosereported by patients, except that many patients did not know what was in the treat-ment they received because it is not normal for Chinese doctors to provide informa-tion to their patients (Kleinman, 1980).
Why is there a problem?
Before discussing the findings, it is relevant to revisit why what we have described isa problem. First, ineffective treatment with antibiotics and antivirals is costly,encourages drug resistance and in some cases can generate side effects or adversereactions. Second, percutaneous treatment carries small but non-trivial risks.Although we found good adherence to infection control measures, weaknesses havebeen reported elsewhere in China (Murakami et al., 2003; Yip, 2003), and a recentpaper notes deaths from anaphylactic shock occurring among people treated withTCM injections for common cold (Ji et al., 2009). Third, the existing financing sys-tem creates distortions in healthcare provision, with profiteering by well-patronisedhospitals and price-gouging by loss-making services. Finally, the vast scale ofunnecessary use of injections and infusions in China creates huge volumes of haz-ardous waste. The government-recommended means of medical waste disposal inrural areas is burning; usually no incinerator is available. Modern medical plasticsburnt at low temperature emit highly toxic fumes containing dioxins, furans andheavy metal residues (Valavanidis, 2008; Hoyos et al., 2008), leading to persistentenvironmental contamination. Inappropriate disposal risks needle-stick injuries tohealth workers and waste handlers. Discarded syringes complete with needles are evensold as toys, as witnessed by one of the authors in Kashgar, North-west China in 2002.Risks include not only transmission of blood-borne viruses, particularly HBV, but trau-matic injury, tetanus and septicaemia.
INTERPRETATION
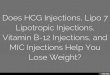
Our study solicited information from patients and healthcare workers about treat-ment of the common cold. Patients use a variety of providers, including informaland TCM practitioners within their own communities, private practitioners andstate-employed doctors. Many patients reported self-medicating instead of or inaddition to seeking treatment from a health worker. However, if symptoms persistafter over-the-counter remedies have been taken, the sufferer is likely to seek inject-able treatment from a health worker, often justifying this as ‘because pills havefailed’. In Figure 1, we represent diagrammatically how someone suffering from acommon cold comes to receive an injectable preparation. For simplicity, this prob-lem analysis focuses on the determinants of prescribing in the doctor–patient dyad,although other actors, such as hospital managers and medical suppliers, influencepatient and prescriber behaviour.
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

+
PATIENT The patient avoids prescriptions for pills because these are the same as at the pharmacy but
much more expensive, and they feel they have already tried this option. Patients focus on
the mode of treatment because this is observable; its content is not and it is rarely explained
to them. Thus people say that “pills have failed” and dismiss further oral treatment as
useless
+Some patients believe oral medication is not absorbed adequately
+Patients consider injected or infused treatment the best treatment. This belief may be
provider-created, but may also be associated with effective treatment through needles via
acupuncture, and the advent of antibiotic injections
+Social benefits, notably the opportunity for several hours’ rest, and the attentions of nursing
staff, may be attached to IV infusions
+Patients may believe the most expensive treatment options are the best
+Patients may value injection skills in place of the higher skills of diagnosis and treatment
management, perhaps because explanation for patients is rare
HEALTH CARE WORKER
If the prescriber prefers not to provide injections or infusions, patient perceptions of his
or her competence may suffer and his/her longer term income may drop through fall in
patient numbers or cut in bonus, disincentivising rational treatment
+The healthcare worker may recommend injected or infused treatment because of
his/her own belief that it is the best treatment
+
The healthcare worker may recommend injected or infused treatment because
personal or institutional financial gain follows; in particular the prescriber retains 100%
of injection fees and charges 15% of the cost of injection materials and contents
OUTCOME
Individual and community belief in need to medicate colds
Person decides to seek treatment
A person feels ill with common cold symptoms
Patient receives injected treatment for common cold
Person goes to a pharmacy for pills
The pills are not correctly chosen or taken and thus often do not clear symptoms
The person decides to visit a chosen medical provider, so entering the patient role
Figure 1. Determinants of over-prescription of injected medication for common cold
466 L. REYNOLDS AND M. MCKEE
The factors favouring percutaneous treatment appear to arise from the desire byproviders to maximise revenue, exacerbated by poor understanding of the aetiology,treatment and natural history of the common cold among both health workers andpatients. However, a further factor is the degree of patient choice in China. Under-employed doctors must strive to attract and retain patients and so face pressure toprescribe from, on the one hand, the financial benefit of over-treatment (and in par-ticular the need to extract as much money from the initial consultation as possible)and on the other, the risks that arise from failing to meet the patient’s expectations,which include complaints, or the loss of the patient to another provider.The existing funding system thus creates many barriers to rational treatment,
something that has been noted for almost two decades (Clayton et al., 1993). The re-ferral system is failing: in primary care, minimally trained workers retain patientsthey are unqualified to diagnose and treat, whereas in tertiary facilities, well-trained
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

467SERVE THE PEOPLE OR CLOSE THE SALE?
staff squander their time and expertise treating patients with the common cold so asto support the hospital financially. The Chinese Ministry of Health has identified thecore problem as being that ‘the relationship between different medical serviceschanged from coordination of division of labour to overall competition’ (Ministryof Health, 2005).
Developing a response
The challenge then is what to do about this situation. Changing clinical behaviourrequires an integrated package of approaches (Oxman et al., 1995): little impactcan be expected by tackling individual factors. Supply side interventions wouldseem to hold most promise, as the government regulates physician employment,training and licensing and is in a position to change the system of rewards. However,although the demand from patients may initially have been supplier-induced, itnow seems self-sustaining, as the expectations generated have become establishedwisdom.
Sciortino describes how mistaken beliefs by health workers that patients wantinjectables and by patients that this is the appropriate treatment creates positive feed-back which escalates use (Sciortino, 1993). Cao et al. report that, in Shanghai, 46%of physicians in focus group discussions reported patients frequently demandinginjections whereas their population survey found only 14% of people preferringinjections for a fever, with 39% preferring oral medication and 44% indifferent(Cao et al., 2001). In their focus groups, most patients reported that the choice ofinjections was typically initiated by the doctor. In contrast, Tables 5 and 6 show that,in our study, whereas health workers favour percutaneous treatments that benefitthem financially, enthusiasm is even greater among patients. An effective policy mustaddress these widely held popular beliefs, something that may be difficult in asituation where there is such a degree of patient choice. As Kleinman observed, ‘thecustomary view is that professionals organise health care for lay people. But typi-cally lay people activate their health care by deciding when and whom to consult,whether or not to comply, when to switch between treatment alternatives, whethercare is effective and whether they are satisfied with its quality’ (Kleinman, 1980).The ability of patients to choose their provider, including those in the private, infor-mal and traditional sectors, makes it difficult for a single provider or even sector tointroduce change. There is a clear need for measures that go beyond the traditionalremit of the Ministry of Health.
Some possibilities are suggested by the data, although much more investigation isneeded to understand how to shape messages that are culturally and contextuallyacceptable. There is a clear need to address fundamental misconceptions about theaetiology and treatment of the common cold (as well as other common disorders).Some people in rural and urban areas do consider a cold to be no more than a minor,self-limiting inconvenience; the challenge is to make this the norm. It is beyond thescope of this paper to examine all of the possible communication strategies, but thereis scope for the imaginative use of China’s mass media, for example insertingmessages into popular programmes.
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

468 L. REYNOLDS AND M. MCKEE
Action on the supply side will, however, also be needed. The relatively unfetteredclinical freedom of China facilitates profit-led use of medically unnecessary andpotentially dangerous treatments such as ribavirin. Manufacturers, distributors andretail pharmacists inflate demand by promoting profitable lines for off-label usesand without appropriate warnings. A recent study in four Chinese cities found that95% of acute respiratory infections were treated with antibiotics (Yang and Shen,2005), whereas a study in Gansu and Chongqing found that less than 2% of drug pre-scriptions overall and only 0.06% of those in village clinics could be consideredrational (Zhang et al., 2003). Insurers have been trying to rationalise prescribingbut clearly can do little when much care is paid for out of pocket (Liu et al.,2006). There are, however, some concrete actions that could be taken. These includea ban on advertising of injectable treatments and antibiotics to patients and on theemployment of prescribing doctors in pharmacies. The State Food and Drug Admin-istration could require pharmaceutical companies to formulate TCM remedies inways that avoid their bitter taste, as all are active orally. Licences for retail sale ofadult and paediatric injectable treatments not on the Essential Drugs List could berevoked, and more could be done within hospitals to review prescribing (Donget al., 1999).It will, however, ultimately be necessary to tackle the system of financing hospitals.
For three decades, drugs have been the most profitable item sold by hospitals (Menget al., 2005); the profits subsidise price-controlled services such as surgery, standarddiagnostics and some pharmaceuticals (Blumenthal and Hsiao, 2005). Hospitals areallowed to make a 15% profit on pills, injectables and disposable equipment butcan retain 100% of the fees for administering injections and infusions, creating apowerful incentive favouring this mode of administration. Village doctors receivethese sums directly, whereas hospital doctors share them through pooled bonuses.Commission-based bonuses thus transform prescribers into sales agents for suppliers.They set hospitals against retail pharmacies, delivering windfall profits to the hospitalsbecause of their much lower overheads while generating overuse of percutaneoustreatment.Any new policy must also address the low wages of doctors. One study of two
hospitals showed how attempts to reduce the cost of drugs to patients and insurersfailed because the doctors adjusted the volumes and products to maintain income(Meng et al., 2005). There is, however, evidence that change is possible. An exper-iment in five villages in two western provinces assessed the effect of communitiespaying doctors a fixed salary that would compensate for loss of their normal earningsfrom commission on drug sales (Yan et al., 2007). This change was followed by areduction in prescribing of multiple antibiotics and a drop in average prescriptioncost in four of the five sites.
CONCLUSION
A Chinese doctor faced with a patient seeking treatment for a common cold is likelyto provide percutaneous treatment, a situation that is now expected by patients.Indeed, people who do not obtain injected treatment may be admonished by others
Copyright © 2011 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

469SERVE THE PEOPLE OR CLOSE THE SALE?
for neglecting their health. A cycle of supplier and recipient-generated demandmeans that patients not only seek entirely ineffective medication but insist that itbe injected. The treatment of common colds using injected medications of no thera-peutic relevance has been fostered by the profit-led financing structure of theChinese healthcare system through a complex of mutually supporting beliefs amonghealthcare workers and patients. It is to be hoped that the recently announced 3-yearhealth reform plan (State Council, 2009) will address these matters through a coor-dinated programme of measures to further the goal of providing ‘a safe, effective,convenient and affordable’ basic healthcare system.
REFERENCES
Bao YP, Liu ZM. 2009. Systematic review of HIV and
HCV infection among drug users in China. Int J STD
AIDS 20(6): 399–405.
Blumenthal D, Hsiao W. 2005. Privatization and its dis-
contents—the evolving Chinese health care system. N
Engl J Med 353(11): 1165–1170.
Bowling A. 1997. Research Methods in Health: Investi-
gating Health and Health Services. Open University
Press: Buckingham.
Cao Y, Chen J, Cao JW. 2001. Injection Practices in
Health Care Facilities of Shanghai, China. World
Health Organization: Geneva.
Chen W, Cheng XZ, Li JM. 1995. The study of positive
impact of positive list of drugs coverage on hospital
use of drugs. Chinese Hospital Manage 15(7): 8–11.
Clayton S, Yang H, Guan J. 1993. Hepatitis B control in
China: knowledge and practices among village doc-
tors. Am J Public Health 83(12): 1685–1688.
Dong HL, Bogg L, Rehnberg C, Diwan V. 1999. Health
financing policies: providers’ opinions and prescrib-
ing behaviour in rural China. Int J Technol Assess
Health Care 15(4): 686–698.
Hoyos A, Cobo U, Aristizábal B, Córdoba F, Montes de
Correa C. 2008. Total suspended particulate, poly-
chlorinated dibenzodioxin and polychlorinated diben-
zofuran emissions from medical waste incinerators in
Antioquia, Colombia. Chemosphere 73(1 Suppl):
S137–S142.
Ip P-K. 2005. Developing medical ethics in China’s re-
form era. Developing World Bioethics 5(2): 176–187.
Ji K, Chen J, Li M, et al. 2009. Comments on serious
anaphylaxis caused by nine Chinese herbal injec-
tions used to treat common colds and upper respira-
tory tract infections. Regul Toxicol Pharmacol 55(2):
134–138.
Kleinman A. 1980. Patients and Healers in the Context of
Culture: an Exploration of the Borderland between
Anthropology, Medicine, and Psychiatry. University
of California Press: Berkeley.
Copyright © 2011 John Wiley & Sons, Ltd.
Lau WK, Ng MK. 1986. Illness behaviour in the Chinese
patients—observations from a rural general practice.
Hong Kong Practitioner 8(8): 1989–1996.
Li Q, Ou JM, Zeng G. 2003. A cross-sectional survey on
injection safety in health facilities in Wulong county,
Chongqing city. Zhonghua Liu Xing Bing Xue Za Zhi
24(3): 176–179.
Liang X, Bi S, Yang W, et al. 2009. Evaluation of the
impact of hepatitis B vaccination among children
born during 1992–2005 in China. J Infect Dis 200(1):
39–47.
Liu X, Li S. 1997. Drug policy in China. Transformations,
current status and future prospects. Pharmacoeco-
nomics 12(1): 1–9.
LiuX, Liu Y, ChenN. 2000. The Chinese experience of hos-
pital price regulation. Health Policy Plan 15(2): 157–63.
Liu X, Mills A. 1999. Evaluating payment mechanisms:
how can we measure unnecessary care? Health Policy
Plan 14(4): 409–413.
Liu Y, Berman P, Yip W, et al. 2006. Health care in China:
the role of non-government providers. Health Policy
77(2): 212–220.
Lu E. 2005. Strengthening control of antibiotics. Re-
trieved 12th April 2008, from http://www.chinatoday.
com.cn/English/e2005/e200503/p40.htm
Lu FM, Zhuang H. 2009. Management of hepatitis B in
China. Chin Med J (Engl) 122: 3–4.
Meng Q, Cheng G, Silver L, et al. 2005. The impact of
China’s retail drug price control policy on hospital
expenditures: a case study in two Shandong hospitals.
Health Policy Plan 20(3): 185–196.
Ministry of Health. 2005. Report on China’s Healthcare
System and Reform. Ministry of Health: Beijing.
Murakami H, Kobayashi M, Zhu X, et al. 2003. Risk of
transmission of hepatitis B virus through childhood
immunization in northwestern China. Soc Sci Med
57(10): 1821–1832.
Oxman AD, Thomson MA, Davis DA, et al. 1995. No
magic bullets: a systematic review of 102 trials of
Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm

470 L. REYNOLDS AND M. MCKEE
interventions to improve professional practice. Cmaj
153(10): 1423–1431.
Reeler AV. 1990. Injections: a fatal attraction? Soc Sci
Med 31(10): 1119–1125.
Reeler AV, Hematorn C. 1978. Injection Practices in the
Third World: a Case Study of Thailand. WHO Action
Programme on Essential Drugs. WHO: Geneva.
Reynolds L, McKee M. 2008. Possible risks of transmis-
sion of blood-borne infection via acupuncture needles
in Guizhou province, southwest China. J Altern Com-
plement Med 14: 1281–1285.
Reynolds L, McKee M. 2009. Factors influencing antibi-
otic prescribing in China: an exploratory analysis.
Health Policy 90: 32–36.
Reynolds L, McKee M. 2010. Matching supply and de-
mand for blood in Guizhou province, China: an unre-
solved challenge. J Public Health 32(i): 103–109.
Sanderson C, Bosch T, Goosen J, et al. 1987. Reviewing the
process and outcome of hospital care in Europe: the tracer
method. Int J Health Plann Manage 2(4): 293–299.
Sciortino R.1993. The myth of injections: providers and
patients in rural central Java. In The Impact of Injec-
tions on Daily Medical Practice, I Wolffers, M Bloem
(eds). VU University Press: Amsterdam.
State Council of China. 2009. Implementation plan for the
recent priorities of the healthcare system reform
(2009–2011).
Ulin PR, Robinson ET, Tolley EE, et al. 2005. Qualitative
Methods in Public Health: a Field Guide for Applied
Research. CA Jossey-Bass: San Francisco.
Copyright © 2011 John Wiley & Sons, Ltd.
UNGASS. 2008. People’s Republic of China Reporting
period January 2006–December 2007 State Council
AIDS Working Committee Office and UN Theme
Group on AIDS.
Valavanidis A. 2008. Metal leachability, heavy metals,
polycyclic aromatic hydrocarbons and polychlori-
nated biphenyls in fly and bottom ashes of a medical
waste incineration facility. Waste Manag Res 26(3):
247–255.
Yan Y, Zhang G, Chen Y, et al. 2006. Study on the injec-
tion practices of health facilities in Jingzhou district,
Hubei, China. Indian J Med Sci 60(10): 407–416.
Yan YW, Yan J, Zhang GP, et al. 2007. Prevalence of
injections and knowledge of safe injections among ru-
ral residents in central China. Singapore Med J 48(8):
769–774.
Yang YH, Shen XZ. 2005. An overview of antibiotic
resistance and usage found in past studies. Second
National Workshop on Rational Use of Antibiotics in
China, Beijing.
Yip R, UNICEF. 2003. Personal communication. Beijing.
Zhang X, Feng Z, Zhang L, et al. 2003. Analysis on qual-
ity of prescription of township hospitals in poor areas.
J Rural Health Serv Manage 23(12): 33–35.
Zhen SZ, Wang F, Wang LX, et al. 1995. The benefit
analysis of ‘revenue control and structure adjustment’
policy. China J Hospital Admin 11(9): 624–625.
Zheng X, Hillier S. 1995. The reforms of the Chinese
health care system: county level changes: the Jiangxi
Study. Soc Sci Med 41(8): 1057–1064.
Int J Health Plann Mgmt 2011; 26: 449–470.
DOI: 10.1002/hpm