Embed Size (px)
Citation preview
Int Arch Occup Environ Health ( 1990) 62:189-193 International Archives of
O Ce CpalionalndEnvironmentalHealthO Springer-Verlag 1990
Serum vitamin D metabolites in cadmium-exposed personswith renal damage
Koji Nogawa l , Ikiko Tsuritani 2 , Teruhiko Kido 2 , Ryumon Honda 2 , Masao Ishizaki 2 , and Yuichi Yamada 2
'Department of Hygiene, School of Medicine, Chiba University, Inohana, Chiba, 280, Japan2 Department of Hygiene, Kanazawa Medical University, Uchinada, Ishikawa, 920-02, Japan
Received December 1, 1989 / Accepted January 24, 1990
Summary Serum concentrations of 25-hydroxyvitamin Dl 25 (OH)Dl, 24,25-dihydroxyvitamin D l 24,25 (OH) 2Dl,and la,25-dihydroxyvitamin D llac,25 (OH) 2Dl weremeasured in ten cadmium (Cd)-exposed subjects andfive non exposed subjects The Cd-exposed subjectswere divided into two groups according to serumla,25 (OH) 2D levels No significant differences for25 (OH)D were found between the Cd-exposed groupwith low or normal serum la,25 (OH) 2D and the non ex-posed group The concentrations of 24,25 (OH) 2D werethe lowest in the Cd-exposed group with low serumla,25 (OH) 2 D, highest in the non exposed group, andsignificantly lower in the Cd-exposed group with normalserum la,25 (OH) 2 D than in the non exposed group.Renal function was much worse in the Cd-exposed groupwith low serum l,25 (OH) 2D than in the group withnormal serum la,25 (OH) 2D These findings indicatethat Cd initially disturbs hydroxylation from 25 (OH)Dto 24,25 (OH) 2D and then disturbs hydroxylation from25 (OH)D to la,25 (OH) 2D The decrease of serum24,25 (OH) 2D and la,25 (OH) 2D in Cd-exposed subjectsis not due to a decrease of the serum 25 (OH)D level.
Key words: Cadmium Bone change Vitamin D meta-bolites Renal damage
tients with renal damage caused by Cd exposure late inthe clinical course l 12, 14, 17 l.
The mechanism of bone damage is still not known.One hypothesis is that the vitamin D metabolism in thekidney is disturbed by Cd exposure, which leads to inter-nal vitamin D deficiency causing bone damage We pre-viously reported that serum la,25-dihydroxyvitamin Dlla,25 (OH) 2Dl levels were lower and serum parathyroidhormone (PTH) levels higher in Cd-exposed subjectswith renal damage than in non exposed subjects l 20, 21 l.Decreases in serum la,25 (OH) 2D levels are closely re-lated to serum concentrations of PTH, 2 -microglobulin(P 2-m) and percentage tubular reabsorption of phosphate(%TRP) l 21 l On the basis of these results, we assumedthat a disturbance in vitamin D and PTH metabolismmay be one of the causative factors for Cd-induced bonedamage It has been reported that the concentration of25-hydroxyvitamin D l 25 (OH)Dl in the serum of patientswith chronic renal failure is within the normal range,while the concentrations of the renal metabolites of vita-min D, e g 24,25-dihydroxyvitamin D l 24,25 (OH) 2Dland la,25 (OH) 2D, are consistently low l 3, 6, 10, 26,30, 31 l.
The purpose of this study was to analyze the major vi-tamin D metabolites in the serum of Cd-exposed sub-jects and to clarify the disturbance of vitamin D metabo-lism in the kidney.
Introduction Subjects and methods
Exposure to cadmium (Cd) causes kidney and bonedamage which is seen in Cd-workers in industry and inpeople living in Cd-polluted areas in Japan l 5 l It isthought that the kidney is a critical organ in chronic cad-mium poisoning and low molecular weight proteinuria,such as P 2 -microgloburinuria, is a sensitive indicator ofrenal involvement l 1, 5, 16, 25 l On the other hand,bone damage is similar to the combined findings of os-teomalacia and osteoporosis and is usually found in pa-
Offprint requests to: K Nogawa
Population The target subjects in this study were selected from 36subjects who had renal damage caused by exposure to Cd and wereofficially recognized as "subjects requiring observation" by the Re-search Committee organized by the Ishikawa Prefectural HealthAuthority Their serum l,25 (OH) 2D levels had already been mea-sured in the previous study l 21 l On the basis of these previouslymeasured serum la,25 (OH) 2D levels, five women were selected atrandom from the low serum la,25 (OH) 2D group (< 40 pg/ml) andanother five subjects (two men and three women) were selectedfrom normal serum la,25 (OH) 2D group (> 50 pg/ml) They werenot taking any vitamin-containing drugs at the time of this exami-nation For the non exposed control group, five men in our labora-

190
tory were selected None of them had any history of exposure toCd and all were healthy at the time of the examination.
Collection of samples Venous blood samples were obtained fromeach subject from September to October and centrifuged for col-lection of the serum within 2 h Each sample was kept frozen at-20 °C until analysis could be performed.
Vitamin D-metabolite assay A tracer amount of la,25 (OH) 2l 23,24 (n)-3 Hl D (Radiochemical Center, Amersham, UK) wasadded to the serum samples After equilibration and addition oftetrahydrofuran, the samples were successively extracted withethylacetate at room temperature The extracts were evaporatedto dryness under nitrogen in a 37 °C water bath Each serum ex-tract was taken up in a mixture of hexane: isopropanol ( 96:4, v/v)and chromatographed on a minicolumn (Sep Pak Silica, WatersAssociates, USA) using a mixture of hexane: isopropanol ( 80:20,v/v) as an eluent The appropriate fractions were collected andevaporated as above The residues containing lu,25 (OH) 2D weredissolved in small volumes of a mixture of hexane and isopropanol( 92:8, v/v) and subjected to high pressure liquid chromatography(HPLC) This was performed on a p-Porasil column (length 30 cm,Waters Associates, USA) connected to a Model SPD-2 A fixedspectrophotometric detector eluting with hexane: isopropanolmixture at a flow rate of 2 0 ml/min using a LC-6 A type pump andSIL-1 A type injector (all equipment from Shimazu Seisakusho,Japan) After collection of the appropriate fractions and evapora-tion of the solvent, the residues were dissolved in ethanol, countedfor radioactivity and assayed for 1 a,25 (OH) 2D amount by radiore-ceptor assay (Receptor protein of la,25 (OH) 2D: Yamasa SyoyuCo., Japan) A detailed description of the radioimmunologicalprocedures is reported by Nishii et al l 18 l.
Regarding the assays for 25 (OH)D and 24,25 (OH) 2D, traceramounts of 25 (OH)l 26,27-methyl- 3HlD and 24,25 (OH) 2l 23,24 (n)-3HlD were added to the serum samples After equilibration, thesamples were extracted with a dichloromethane: methanol mixture( 1: 2, v/v) at room temperature Each supernatant was poured intoa mixture of 0 2 M KOH and methylene chloride ( 1:1, v/v) Aftercentrifugation, the lower phase was washed by adding methanol:distilled H 20 ( 1:1, v/v) and then centrifuged This step was re-peated The extract was evaporated to dryness under nitrogen in a37 °C water bath The residues were taken up in a mixture ofhexane: chloroform: methanol ( 9:1:1, v/v) and chromatographedon 16 x 1 cm Sephadex LH-20 columns using the same mixture asthe eluent The appropriate fractions were collected and evapo-rated as above The residues containing 24,25 (OH) 2D were puri-fied using the same HPLC method as mentioned in the la,25 (OH) 2D
assay The residues of the 25 (OH)D and 24,25 (OH) 2D containingfractions were dissolved in a small volume of ethanol Parts ofthese solutions were used for recovery estimations by measuringthe radioactivity in a 13-scintillation counter In the remainingsolution, concentrations of 25 (OH)D and 24,25 (OH) 2D were mea-sured by competitive protein-binding assay using the kit( 25-Hydroxy)vitamin D l 3Hl assay system (Amersham InternationalPlc, UK) Column calibrations were performed using the 3H-label-led derivatives and the positions of the peaks were determined be-fore each HPLC session using synthetic 25 (OH)D, 24,25 (OH) 2Dand la,25 (OH) 2D (donated by Chugai Seiyaku Co , Japan) Re-coveries of added radioactivity after extraction and chromatog-raphy were 87 6 ± 4 6 % (mean + SD) 76 9 + 4 4 %, and 73 O + 3 2 %for 25 (OH)D, 24,25 (OH) 2D and la,25 (OH) 2D, respectively Re-covery of non radioactive l,25 (OH) 2D added to five serum sam-ples was 95 5 ± 8 8 % (mean + SD) The percentage recoveryranges were from 84 7 to 111 2 % Coefficients of variation be-tween assays of serum levels of the metabolites were 4 0, 8 8 and14.5 % for 25 (OH)D, 24,25 (OH) 2D and la,25 (OH) 2D, respec-tively.
Other analyses for serum and urine The determinations of creati-nine, 32-microglobulin, calcium and phosphorus in serum, and 32-microglobulin, total protein and Cd in urine were carried out asdescribed previously l 20 l Blood Cd was directly measured using aZeeman Effect Flameless Atomic Absorption Spectrometer(Hitachi Co , Japan) without ashing and extraction Measure-ments of creatinine clearance, percentage tubular reabsorption ofphosphate (%TRP) and base excess were also performed as previ-ously described l 19 l.
Statistical analysis Differences between two means were testedwith Student's t-test Differences between three means were testedwith ANOVA and Duncan's test.
Results
The arithmetic means and standard deviations for the con-centrations of three serum metabolites of vitamin D andthe ratio of 24,25 (OH) 2D and 25 (OH)D ( 24,25 (OH) 2D/25 (OH)D x 100 % = 24,25 (OH) 2 D index) are shown inTable 1 Data are shown separately for the Cd-exposedsubjects with low or normal serum la,25 (OH) 2D leveland non exposed subjects In Table 2, arithmetic means
Table 1 Serum vitamin D metabolites in Cd-exposed subjects with low or normal serum la,25-dihydroxyvitamin D and in non exposedsubjects
Cd-exposed subjects Cd-exposed subjects Non exposed subjectswith low la,25 (OH) 2D with normal la,25 (OH) 2Dlevel in serum level in serum
N Mean SD N Mean SD N Mean SD
Age 5 84 0 7 1 5 73 0 3 4 5 33 8 4 2
Serum25 (OH)D (ng/ml) 5 20 6 7 9 5 26 6 10 0 5 22 0 4 3la,25 (OH) 2D (pg/ml) 5 34 7 4 6 a b 5 59 9 6 9
a c 5 49 6 8 O b c24,25 (OH) 2D (ng/ml) 5 0 34 0 0 7 a, b 5 0 86 0 34 a c 5 1 44 0 28
b, C
24,25 (OH)2D/25 (OH)D (%) 5 1 9 0 9 a 5 3 3 2 6 a 5 6 5 O 8 b ' c
Notes: Values are expressed as arithmetic means ± SDa Significantly different from nonexposed subjectsb Significantly different from Cd-exposed subjects with normal serum l,25 (OH) 2Dc Significantly different from Cd-exposed subjects with low serum la,25 (OH) 2D
191
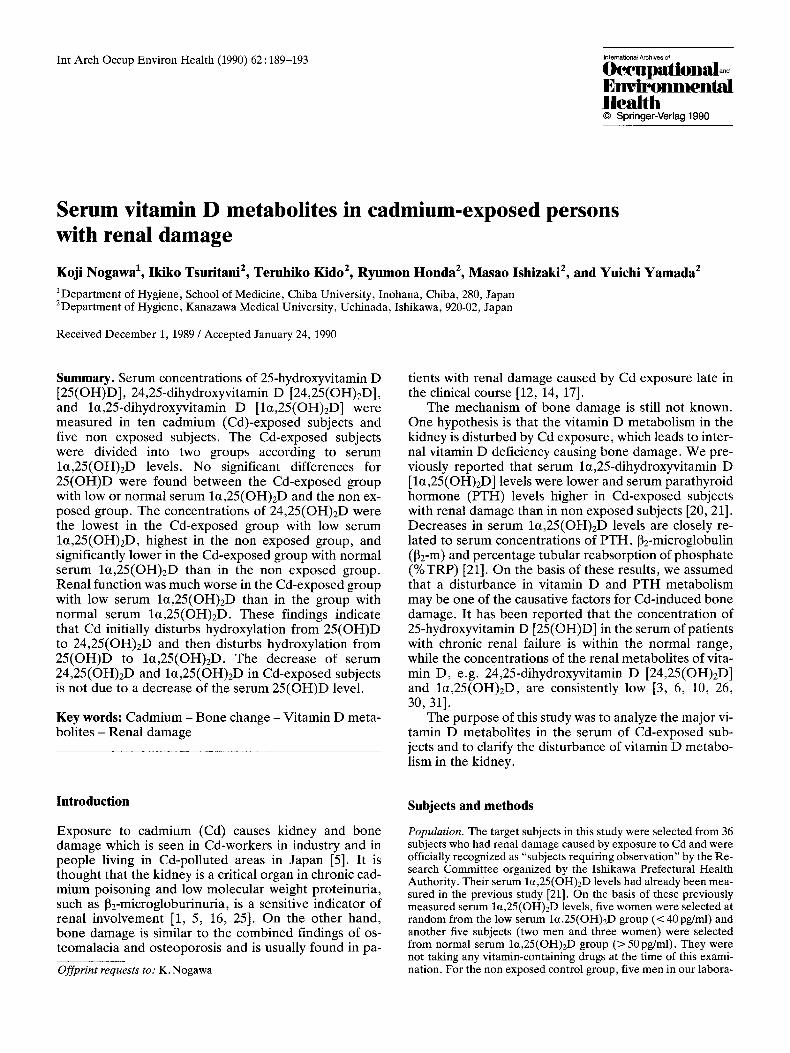
Table 2 Results of serum and urine analysis in Cd-exposed subjects with low or normalserum la,25-dihydroxyvitamin D
Cd-exposed subjects Cd-exposed subjectswith low la,25 (OH) 2D with normal la,25 (OH) 2Dlevel in serum level in serum
N Mean SD N Mean SD
Age 5 84 0 7 1 5 73 0 3 4
SerumCreatinine (mg/dl) 5 1 7 0 4 * 5 1 0 0 132-microglobulin (gg/l) 4 4498 366 ** 4 2266 245Calcium (mg/dl) 5 9 0 0 5 5 9 4 0 6Inorganic phosphorus (mg/dl) 5 2 6 0 2 5 2 7 0 2
Urinel 32-microglobulin (gg/g cr) 5 83749 19184 ** 5 10225 12924Total protein (mg/g cr) 5 780 238 ** 5 102 152
Renal functionCreatinine clearance (ml/min) 5 34 5 13 5 * 5 63 5 20 1%TRP (%) 5 58 0 11 5 ** 5 79 4 6 7Base excess (m Eq/1 blood) 4 5 7 3 3 * 5 0 28 0 73
Cd in blood (gg/l) 5 9 2 2 8 5 8 1 4 7Cd in urine (g/g cr) 5 9 3 3 3 5 8 6 5 2
Notes: Values are expressed as arithmetic means ± SDSignificantly different from Cd-exposed subjects with normal serum0.01 ; * P < O 05)
and standard deviations for the other results of serumand urine analyses in the two Cd-exposed groups arepresented.
There were no significant differences in the concen-tration of 25 (OH)D among the Cd-exposed subjects inthe low la,25 (OH) 2 D group (low level group), subjectsin the normal la,25 (OH) 2D group (normal level group)and subjects in the non exposed group Significant differ-ences among the three groups were found in the concen-trations of la,25 (OH) 2D and 24,25 (OH) 2D.
The la,25 (OH) 2D level was significantly higher inthe normal level group than in the low level or non ex-posed groups The low level group showed significantlylower concentrations of la,25 (OH) 2D than the non ex-posed group.
The concentration of 24,25 (OH) 2D was the lowest inthe low level group and the highest in the non exposedgroup, with significant differences found between eachgroup.
The 24,25 (OH) 2D index was the lowest in the lowlevel group and the highest in the non exposed group.The difference between the low or normal level groupand the non exposed group is significant, but the differ-ence between the low level and normal level groups wasnot significant.
Serum concentrations of creatinine and 2 -micro-globulin and urinary concentrations of 32-microglobulinand total protein were significantly higher in the lowlevel than in the normal level group Creatinine clear-ance, % TRP and base excess were significantly lower inthe low level than in the normal level group No signifi-cant differences were observed in the blood and urinaryconcentrations of Cd.
la( 25)OH 2 D (**P<
Discussion
The Cd-exposed subjects used in this study were dividedinto two groups, namely low or normal serum la,25 (OH) 2D groups, according to previous determinationsof la,25 (OH) 2D in serum Different methods were usedfor the determination of la,25 (OH) 2D in the previousand present studies In the previous study, a radiorecep-tor assay using the la,25 (OH) 2D assay system developedby Amersham International Plc (UK) was employed.
This method does not include an HPLC-samplepurification procedure Many factors which potentiallyinterfere with la,25 (OH) 2D assays have traditionallybeen removed by sample purification methodology suchas HPLC as the final step We found a good agreementbetween the previous and present values of the same Cd-exposed subjects (N = 10, r = 0 96) and confirm that theCd-exposed subjects were correctly divided into low ornormal la,25 (OH) 2D groups in this study Our meanvalues for the three vitamin D metabolites in the non ex-posed subjects are similar to previously reported valuesl 10, 18, 24, 26, 32 l.
Vitamin D is catalyzed by a liver vitamin-D-25-hy-droxylase and transformed into 25 (OH)D The reactionproduct is the major circulation vitamin D metabolite inplasma 25 (OH)D is further hydroxylated to la,25 (OH) 2Dby 25-hydroxyvitamin-D-lca-hydroxylase (la-hydroxy-lase) and 24,25 (OH) 2D by 25-hydroxyvitamin-D-24-hydroxylase ( 24-hydroxylase) in the kidney Amongthem, la,25 (OH) 2D seems to be the major biologicallyactive form of vitamin D l 29 l.
Seasonal variations in the serum concentrations of25 (OH)D, la,25 (OH) 2D and 24,25 (OH) 2D have been

192
reported l 11 l We obtained the blood samples in the au-tumn The serum levels of the three metabolites do notvary according to sex and age in adults l 13, 24, 32 l We,therefore, think that age differences between the groupsdid not significantly influence the results of this study.
We have already reported that serum la,25 (OH) 2Dlevels are lower in itai-itai disease patients and Cd-ex-posed subjects with renal damage than in non exposedsubjects and that decreases in the la,25 (OH)2 D level areclosely related to serum concentrations of PTH, 2-microglobulin and %TRP l 19 l Based on these results, itwas concluded that Cd-induced bone effects are mainlydue to disturbances in vitamin D and parathyroid hor-mone metabolism, which are caused by the Cd-inducedkidney damage.
In the present study, no significant differences inserum 25 (OH)D levels among the Cd-exposed groupswith low or normal la,25 (OH) 2D and the non exposedgroups were found These results indicate that the syn-thesis of vitamin D does not differ among these groups.
Serum 24,25 (OH) 2D and 24,25 (OH) 2D indices weresignificantly lower in the Cd-exposed groups than in thenon exposed group These values were lowest in the Cd-exposed group with low serum la,25 (OH) 2D Significantdecreases of these values were also found in the Cd-ex-posed group with normal serum la,25 (OH) 2D, com-pared to the non exposed group Therefore, it appearsthat a disturbance of hydroxylation from 25 (OH)D to24,25 (OH) 2D is already present when hydroxylation of25 (OH)D to la,25 (OH) 2D is smoothly performed.
Renal function is much worse in the Cd-exposedgroup with low-serum la,25 (OH) 2D than in the groupwith normal serum la,25 (OH) 2D These results are inaccordance with the results of the previous study l 21 l.
Based on the results of the present and previousstudies, it may be concluded that Cd induces kidneydamage, which, in turn, leads to a disturbance in vitaminD metabolism Cd initially suppresses hydroxylationfrom 25 (OH)D to 24,25 (OH) 2D and then causes suppres-sion of hydroxylation from 25 (OH)D to la,25 (OH) 2D.The low concentrations of 24,25 (OH) 2D and la,25 (OH) 2Din Cd-exposed subjects are not due to a decrease of theserum 25 (OH)D level.
Although a role for 24,25 (OH) 2D has not yet clearlybeen established, some studies suggest that it may havedistinctive biological actions of physiological and thera-peutic importance l 2, 4, 7, 8, 9, 15, 22, 23, 27, 28 l Itshould be noted that a slight-to-moderate degree of Cd-induced kidney damage could result in a decrease of theserum 24,25 (OH) 2D level.
References
1 Bernard A, Buchet JP, Roels H, Masson P, Lauwerys R( 1978) Renal excretion of proteins and enzymes in workers ex-posed to cadmium Eur J Clin Invest 9:11-22
2 Binderman I, Somjen D ( 1984) 24,25-dihydroxycholecalciferolinduces the growth of chick cartilage in vitro Endocrinol115:430-432
3 Clemens TL, Hendy GN, Papapoulos SE, Fraher LJ, CareAD, O'riordan JLH ( 1979) Measurement of 1,25-dihydroxy
cholecalciferol in man by radioimmunoassay Clin Endocrinol11:225-234
4 Corvol MT, Dumontier MF, Garabedian M, Rappaport R( 1978) Vitamin D and cartilage II Biological activity of 25-hydroxycholecalciferol and 24,25 and 1,25-dihydroxycholecal-ciferols on cultured growth plate chondrocytes Endocrinol102:1269-1274
5 Friberg L, Elinder CG, Kjellstr Om T, Nordberg GF ( 1986)Cadmium and health: A toxicological and epidemiological ap-praisal Vol II Effects and response CRC Press, Boca Raton,Florida
6 Haussler MR, Baylink DJ, Hughes MR, Brumbach PF,Wergedal JB, Slen FH, Nielsen RL, Counts SJ, Bursac ND,McCain TA ( 1976) The assay of 1,25-dihydroxyvitamin D 3:physiologic modulation of circulating hormone levels Clin En-docrinol 5:151-165
7 Henry HL, Norman AW ( 1978) Vitamin D: Two dihydroxy-lated metabolites are required for normal chicken egg hatch-ability Science 201: 835-837
8 Hinek A, Reiner A, Poole AR ( 1987) The calcification of car-tilage matrix in chondrocyte culture: studies of the C-propep-tide of type II collagen (chondrocalcin) J Cell Biol 104:1435-1441
9 Holic MF, Baxter LA, Schraufrogel PK, Tavela TE, DelucaHF ( 1976) Metabolism and biological activity of 24,25-dihy-droxyvitamin D 3 in the chick J Biol Chem 251: 397-402
10 Juttmann JR, Buurman CJ, Kam ED, Visser TJ, BirkenhagerJC ( 1981) Serum concentrations of metabolites of vitamin D inpatients with chronic renal failure (CRF) Consequences forthe treatment with 1-a-hydroxyderivatives Clin Endocrinol14: 225-236
11 Juttmann JR, Visser TJ, Buurman C, Kam E, Birkenhager JC( 1981) Seasonal fluctuations in serum concentrations of vita-min D metabolites in normal subjects Br Med J 282:1349-1352
12 Kajikawa K, Kitagawa M, Nakanishi I, Ueshima H, KatsudaS, Kuroda K ( 1974) A pathological study of itai-itai disease JJuzen Med Soc 83:309-347 (in Japanese)
13 Kano K, Hosaki J, Yata J, Yoshida H, Abe E, Suda T ( 1979)Competitive protein binding assay for 25-hydroxyvitamin Dand 24 R,25-dihydroxyvitamin D in human serum Vitamins(Japan) 53:11-19 (in Japanese)
14 Kitagawa M ( 1982) Autopsy cases of patients with itai-itai dis-ease in Toyama Prefecture Kankyo Hoken Report No 48:204-206 (in Japanese)
15 Lidor C, Atkin I, Ornoy A, Dekel S, Edelstein S ( 1987) Heal-ing of rachitic lesions in chicks by 24 R,25-dihydroxycholecal-ciferol administered locally into bone J Bone Mineral Res2:91-98
16 Lauwerys RR, Roels HA, Buchet JP, Bernard A, Stanescu D( 1979) Investigations on the lung and kidney function in work-ers exposed to cadmium Environ Health Perspect 28: 137-145
17 Nakagawa S ( 1960) A study of osteomalacia in Toyama Pre-fecture (so-called itai-itai disease) J Radiol Phys Ther UnivKanazawa 56:1-51 (in Japanese)
18 Nishii Y, Nanjo M ( 1981) Methods for assay of vitamin D 3.Multiple assay of vitamin D and it's metabolites Vitamins(Japan) 55:595-605 (in Japanese)
19 Nogawa K, Kobayashi E, Honda R, Ishizaki A, Kawano S,Ohmura T, Nakagawa H, Toga H, Matsuda H ( 1981) Clinico-chemical studies on chronic cadmium poisoning (Part 5) Renalfunctions Jpn J Hyg 36:512-517 (in Japanese)
20 Nogawa K, Kobayashi E, Yamada Y, Honda R, Kido T,Tsuritani I, Ishizaki M ( 1984) Parathyroid hormone concentra-tion in the serum of people with cadmium induced renal dam-age Int Arch Occup Environ Health 54:187-193
21 Nogawa K, Tsuritani I, Kido T, Honda R, Yamada Y, IshizakiM ( 1987) Mechanism for bone disease found in inhabitants en-vironmentally exposed to cadmium: decreased serum l,25-dihydroxyvitamin D level Int Arch Occup Environ Health 59:21-30

22 Norman AW, Leathers V, Bishop JE ( 1983) Normal egghatchability requires the simultaneous administration to thehen la,25-dihydroxycholecalciferol and 24 R,25-dihydroxy-cholecalciferol J Nutr 113:2505-2515
23 Ornoy A, Goodwin D, Noff D, Edelstein S ( 1978) 24,25-di-hydroxyvitamin D is a metabolite of vitamin D essential forbone formation Nature 276:517-519
24 Parviainen MT, Savolainen KE, Korhonen PH, Alhava EM,Visakorpi JK ( 1981) An improved method for routine determi-nation of vitamin D and its hydroxylated metabolites in serumfrom children and adults Clin Chim Acta 114:233-247
25 Piscator M ( 1978) P 2-Microglobulin in the diagnosis of chroniccadmium poisoning In: Peterson PA, Lauwerys R (eds) Beta 2-microglobulin in proliferative disorders and heavy metal intox-ication Eur Press Gent, pp 69-77
26 Shepard RM, Horn RL, Hamstra J, Deluca HF ( 1979) Deter-mination of vitamin D and its metabolites in plasma from nor-mal and anephric man Biochem J 182:55-69
27 Schwartz Z, Boyan B ( 1988) The effects of vitamin D metabo-lites on phospholipase A 2 activity of growth zone and restingzone cartilage cells in vitro Endocrinol 122:2191-2198
193
28 Somjen D, Binderman I, Weisman Y ( 1983) The effect of24 R,25-dihydroxycholecalciferol on ornithine decarboxylaseactivity and on DNA synthesis in the epiphysis and diaphysis ofrat bone and in the duodenum Biochem J 214:293-298
29 Suda T, Ogata E, Ogura Y, Nishi Y ( 1982) Vitamin D Tokyo,Kodansha (in Japanese)
30 Taylor CM, Mawer EB, Wallace JE, John JT, Cochran M,Russell RGG, Kanis JA ( 1978) The absence of 24,25-dihy-droxycholecalciferol in anephric patients Clin Sci Mol Med55:541-547
31 Taylor CM, John J, John JH, Wallace JE, Mawer EB ( 1979)1,25-dihydroxycholecalciferol in human serum and its relation-ship with other metabolites of vitamin D 3 Clin Chim Acta96:1-8
32 Yamamoto I, Asonuma K, Yamamura S, Dokoh S, KitamuraN, Aoki J, Hino M, Shigeno C, Morita R, Torizuka K ( 1986)Evaluation of serum 1,25-dihydroxyvitamin D measurement inhealthy normals Vitamins (Japan) 60:371-377 (in Japanese)





























