Embed Size (px)
Citation preview

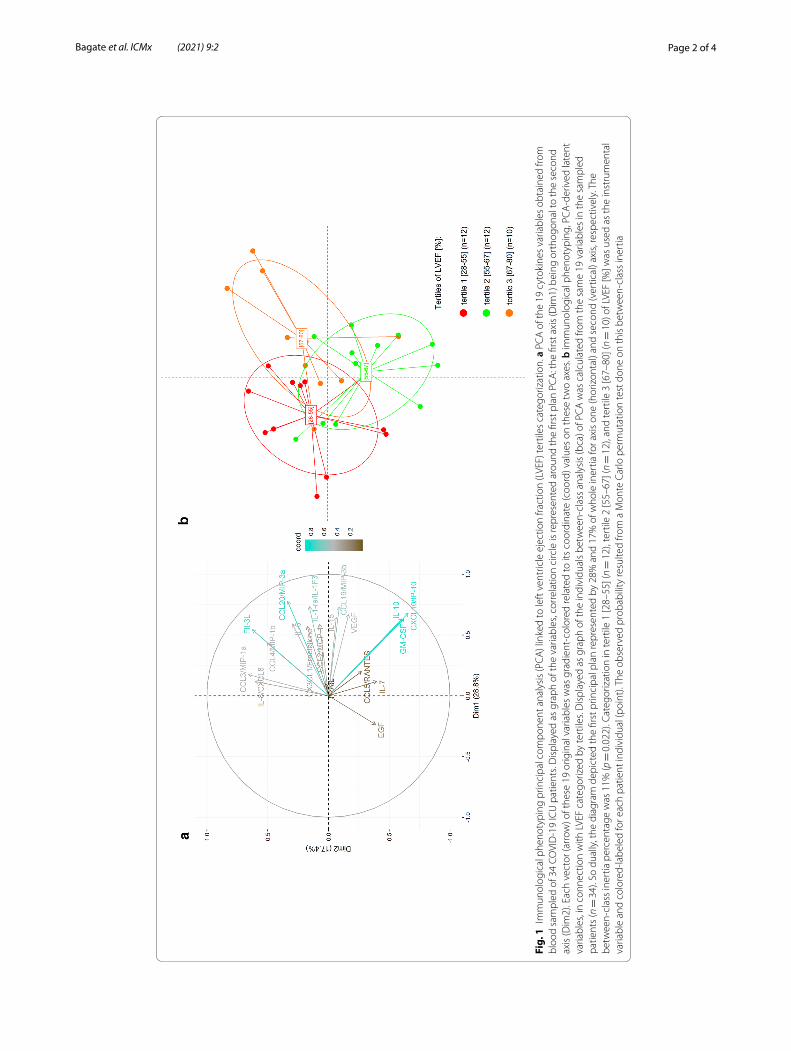
Serum cytokines profile of critically ill COVID‑19 patients with cardiac dysfunctionFrançois Bagate1,2* , Nicolas Maziers1, Sophie Hue3,4, Paul Masi1,2, Armand Mekontso Dessap1,2 and Nicolas de Prost1,2,4
To the Editor,
Most patients requiring intensive care unit (ICU) admission for Coronavirus disease 2019 (COVID-19) presented acute respiratory distress syndrome (ARDS) [1]. However, a significant proportion of critically ill COVID-19 patients developed an acute COVID-19 cardiovascular syndrome (ACovCS) characterized by acute myocardial injury, evi-denced by an increase in circulating biomarkers including serum troponin and B-type natriuretic peptide, associated with elevated interleukin-6 concentrations, myocar-dial dysfunction, ventricular arrhythmias, circulatory insufficiency and a high mortal-ity rate [2, 3]. The pathophysiology of ACovCS remains unclear. Infection by the novel severe acute respiratory syndrome coronavirus (SARS-CoV-2) seems to trigger peculiar innate and adaptive immune responses. High concentrations of circulating cytokines involved in the innate immune response [4], have been associated with poor outcomes in COVID-19 patients. We aimed at evaluating whether critically ill COVID-19 patients with cardiac dysfunction exhibited a peculiar immunological phenotype.
Here, we report on clinical and echocardiographic features together with serum lev-els of cytokines in a monocenter prospective study of critically ill COVID-19 patients admitted to the medical ICU of Henri Mondor Hospital, Créteil, France, between March 8th and March 30th, 2020. The study has received the approbation of an institutional review board (Comité de Protection des Personnes Ile de France II; reference number: 3675-NI). Informed consent was obtained from all patients or their relatives. Reverse-transcriptase polymerase chain reaction (RT-PCR) assays of nasopharyngeal swabs were positive for SARS-CoV-2 in all patients. Blood samples were drawn within 48 h of ICU admission to measure cytokines concentrations using Luminex® multiplex bead-based technology (R&D Systems, Minneapolis, MN, USA) on serum diluted ½. Echocardiog-raphies were performed within the same time frame to characterize cardiac dysfunction (see supplemental method section) and categorize patients according to LVEF tertiles. Patients were not receiving dobutamine at the time the first echocardiography was per-formed, except for one patient. Principal component analysis (PCA) was used to sum-marize cytokines profiles information and assess its relation with LVEF tertiles (see Additional file 1 for a detailed description of the statistical methods).
Open Access
© The Author(s) 2021. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the mate-rial. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creat iveco mmons .org/licen ses/by/4.0/.
LETTERS TO THE EDITOR
Bagate et al. ICMx (2021) 9:2 https://doi.org/10.1186/s40635‑021‑00368‑w Intensive Care Medicine
Experimental
*Correspondence: [email protected] 1 Service de Médecine Intensive Réanimation, AP-HP, CHU Henri Mondor, DHU A-TVB, 51, avenue du Mal de Lattre de Tassigny, 94010 Créteil Cedex, FranceFull list of author information is available at the end of the article
Page 2 of 4Bagate et al. ICMx (2021) 9:2
Fig.
1 I
mm
unol
ogic
al p
heno
typi
ng p
rinci
pal c
ompo
nent
ana
lysi
s (P
CA
) lin
ked
to le
ft v
entr
icle
eje
ctio
n fra
ctio
n (L
VEF)
tert
iles
cate
goriz
atio
n. a
PC
A o
f the
19
cyto
kine
s va
riabl
es o
btai
ned
from
bl
ood
sam
pled
of 3
4 CO
VID
-19
ICU
pat
ient
s. D
ispl
ayed
as
grap
h of
the
varia
bles
, cor
rela
tion
circ
le is
repr
esen
ted
arou
nd th
e fir
st p
lan
PCA
: the
firs
t axi
s (D
im1)
bei
ng o
rtho
gona
l to
the
seco
nd
axis
(Dim
2). E
ach
vect
or (a
rrow
) of t
hese
19
orig
inal
var
iabl
es w
as g
radi
ent-
colo
red
rela
ted
to it
s co
ordi
nate
(coo
rd) v
alue
s on
thes
e tw
o ax
es. b
imm
unol
ogic
al p
heno
typi
ng, P
CA
-der
ived
late
nt
varia
bles
, in
conn
ectio
n w
ith L
VEF
cate
goriz
ed b
y te
rtile
s. D
ispl
ayed
as
grap
h of
the
indi
vidu
als
betw
een-
clas
s an
alys
is (b
ca) o
f PC
A w
as c
alcu
late
d fro
m th
e sa
me
19 v
aria
bles
in th
e sa
mpl
ed
patie
nts
(n =
34)
. So
dual
ly, t
he d
iagr
am d
epic
ted
the
first
prin
cipa
l pla
n re
pres
ente
d by
28%
and
17%
of w
hole
iner
tia fo
r axi
s on
e (h
oriz
onta
l) an
d se
cond
(ver
tical
) axi
s, re
spec
tivel
y. T
he
betw
een-
clas
s in
ertia
per
cent
age
was
11%
(p =
0.0
22).
Cate
goriz
atio
n in
tert
ile 1
[28–
55] (n =
12)
, ter
tile
2 [5
5–67
] (n =
12)
, and
tert
ile 3
[67–
80] (n =
10)
of L
VEF
[%] w
as u
sed
as th
e in
stru
men
tal
varia
ble
and
colo
red-
labe
led
for e
ach
patie
nt in
divi
dual
(poi
nt).
The
obse
rved
pro
babi
lity
resu
lted
from
a M
onte
Car
lo p
erm
utat
ion
test
don
e on
this
bet
wee
n-cl
ass
iner
tia

Page 3 of 4Bagate et al. ICMx (2021) 9:2
Additional file 2: Table S1 shows the characteristics of the 34 consecutive patients included in this study cohort, four of whom had previously known moderate LVEF dysfunction (i.e., between 35 and 50%). The first plan of the PCA accounted for 46.2% of inertia, thus almost half the total variance or inertia, and was mainly driven, among the 19 serum cytokine assays, by three of them, involved in the innate immune response (i.e., IL-10, GM-CSF and CXCL10/IP-10), which were highly correlated between each other and thus formed a coherent cytokine group (Fig. 1a). Moreover, this data partitioning built on the immunological phenotyping at ICU admission was significantly, and independently, connected to LVEF tertiles categorization (Fig. 1b) (tertile 1: hypokinetic patients, LVEF between 28 and 55%; tertile 2: normokinetic patients, LVEF 55–67%; tertile 3: hyperkinetic patients, LVEF 67–80%), indicating that patients with different values of LVEF had contrasted serum cytokines profiles.
We herein showed that there were three distinct serum cytokines patterns according to cardiac function, as assessed by LVEF, in critically ill COVID-19 patients. Interest-ingly, LVEF tertiles were also significantly associated with blood troponin levels (Addi-tional file 3: Fig S1), highlighting a global association between serum cytokines profiles, cardiac dysfunction and troponin elevation. The finding of an IP-10, IL-10, and GM-CSF signature highlights the contribution of myeloid cells to pathogenic inflammation, as previously reported [5]. Such inflammation may amplify an auto-inflammatory loop leading not only to lung, but also myocardial, injury. Further studies, including myocar-dial tissue and cardiac magnetic resonance studies, are needed to assess the contribution of associated acute myocarditis lesions. Our study highlights the potentially pathogenic association between serum cytokines profiles and myocardial injury in critically ill COVID-19 patients. However, because up to 29% of patients with severe SARS-CoV-2 infection and cardiac dysfunction have a history of coronary heart disease [6], we cannot exclude that a substantial proportion of our patients had a previously unknown heart failure. Our study has a number of limitations related to the small number of patients included and the lack of a non-COVID-19 control group, making the results only explor-atory. In conclusion, our results establish a link between serum cytokines profiles and LVEF in patients with severe SARS-CoV-2 infection, but do not allow for causal infer-ences to be drawn regarding the mechanisms at play.
Supplementary InformationThe online version contains supplementary material available at https ://doi.org/10.1186/s4063 5-021-00368 -w.
Additional file 1: Supplemental methods.
Additional file 2: Table S1. Clinical characteristics of 34 critically ill COVID-19 patients, according to left ventricle ejection fraction (LVEF) tertiles.
Additional file 3: Figure S1. Serum troponin concentrations as a function of tertiles of left ventricle ejection fraction (LVEF) in critically ill COVID-19 patients.
AbbreviationsICU: Intensive care units; COVID-19: Coronavirus disease 2019; ARDS: Acute respiratory distress syndrome; ACovCS: Acute COVID-19 cardiovascular syndrome; SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2; LVEF: Left ventricle ejection fraction; RT-PCR: Reverse-transcriptase polymerase chain reaction; PCA: Principal component analysis.
AcknowledgementsWe are very indebted to all physicians and nurses of Henri Mondor medical Intensive Care Unit for their good hand in providing care to COVID-19 patients.
Page 4 of 4Bagate et al. ICMx (2021) 9:2
Authors’ contributionsFB and NdP designed the study and wrote the manuscript. NM realized the statistical analysis. FB and PM collected the data and performed echocardiography. SH measured cytokines concentrations. AMD reviewed the manuscript. All authors read and approved the final manuscript.
FundingThe present study has been conducted without any financial support.
Availability of data and materialsAll data generated and analyzed during the study are included in the published article and can be shared upon request. All authors helped to revise the draft of the manuscript. All authors read and approved the final manuscript.The study has received the approbation of an institutional review board (Comité de Protection des Personnes Ile de France II; reference number: 3675-NI). Informed consent was obtained from all patients or their relatives.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1 Service de Médecine Intensive Réanimation, AP-HP, CHU Henri Mondor, DHU A-TVB, 51, avenue du Mal de Lattre de Tassigny, 94010 Créteil Cedex, France. 2 Faculté de Médecine, Université Paris Est Créteil, Groupe de Recherche Clinique CARMAS, 94010 Créteil, France. 3 Département Immunologie-Hématologie, Hôpitaux Universitaires Henri Mondor, Assistance Publique – Hôpitaux de Paris (AP-HP), Créteil, France. 4 Université Paris-Est Créteil Val de Marne (UPEC), INSERM U95, Créteil, France.
Received: 30 September 2020 Accepted: 2 January 2021
References 1. Wu C, Chen X, Cai Y et al (2020) Risk factors associated with acute respiratory distress syndrome and death in
patients with coronavirus disease 2019 pneumonia in Wuhan China. JAMA Intern Med. https ://doi.org/10.1001/jamai ntern med.2020.0994
2. Hendren NS, Drazner MH, Bozkurt B, Cooper LT (2020) Description and proposed management of the acute COVID-19 cardiovascular syndrome. Circulation 141:1903–1914. https ://doi.org/10.1161/CIRCU LATIO NAHA.120.04734 9
3. Li X, Pan X, Li Y et al (2020) Cardiac injury associated with severe disease or ICU admission and death in hospitalized patients with COVID-19: a meta-analysis and systematic review. Crit Care Lond Engl 24:468. https ://doi.org/10.1186/s1305 4-020-03183 -z
4. Ruan Q, Yang K, Wang W et al (2020) Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 46:846–848. https ://doi.org/10.1007/s0013 4-020-05991 -x
5. Hue S, Beldi-Ferchiou A, Bendib I et al (2020) Uncontrolled innate and impaired adaptive immune responses in patients with COVID-19 ARDS. Am J Respir Crit Care Med. https ://doi.org/10.1164/rccm.20200 5-1885O C
6. Shi S, Qin M, Shen B et al (2020) Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol 5:802–810. https ://doi.org/10.1001/jamac ardio .2020.0950
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.