-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
1/6
ELSEVIER
SERUM CREATININE MEASUREMENTS IN MEN WITH
LOWER URINARY TRACT SYMPTOMS SECONDARY TO
BENIGN PROSTATIC HYPERPLASIA
GLENN S. GERBER, EVAN R. GOLDFISCHER,
THEODORE G. KARRISON. AND GREGORY T. BALES
ABSTRACT
Objectives. To determine the usefulness of routine serum
creatinine measurements in men with lower urinary
tract symptoms secondary to benign prostatic hyperplasia (BPH)
and to correlate these findings with patient
age, symptom severity, and comorbid diseases.
Methods.
We analyzed serum creatinine measurements in 246 consecutive men
presenting for evaluation
of voiding symptoms and BPH. Multiple logistic regression
analysis was used to determine whether the
International Prostate Symptom Score (IPSS), quality-of-life
measure from the IPSS, patient age, or a history
of diabetes mellitus or hypertension predicted abnormal
creatinine levels.
Results. An elevated serum creatinine level was noted in 1 1 (26
of 245) of evaluable patients. Only a
history of diabetes or hypertension predicted the presence of
renal insufficiency. Among men with no history
of comorbid disease, increasing age was significantly associated
with the finding of an abnormal creatinine.
Neither the overall symptom score nor the quality-of-life
measure was significantly associated with the like-
lihood of detectable renal dysfunction.
Conclusions. Medical renal disease secondary to diabetes or
hypertension appears to be the most likely
cause of elevated serum creatinine measurements in men with BPH
and renal insufficiency. We were unable
to identify subgroups of patients in whom the risk of renal
dysfunction is sufficiently low to avoid routine
serum creatinine measurements.
UROLOGY
49: 697-702, 1997. 0 1997, Elsevier Science Inc. All rights
reserved.
I
t has been estimated that 25 of American men
will require treatment for the relief of lower urinary
tract symptoms secondary to benign prostatic hyper-
plasia (BPH) by the age of 8O.l In addition, many
other patients will present for evaluation of voiding
symptoms without subsequently receiving therapy.
Therefore, it is evident that the initial diagnostic eval-
uation of men with BPH should be performed in an
efficient and cost-effective manner to ensure proper
patient care. It is well known that bladder outlet ob-
struction secondary to BPH can lead to upper urinary
tract changes, hydronephrosis, and renal failure.2,3
For this reason, it has been recommended that all
From the Section of Urology, Department of Surgery, and De-
partments ofHealth Studies and Medicine, University of
Chicago
Pritzker Schoo l of Medicine, Chicago, Illinois
Reprint reque sts: Glenn S. Gerber, M.D., University of Chi-
cago, Section of UrologyNC 6038, 5841 South Maryland Ave-
nue, Chicago, IL 60637
Submitted: October 15, 1996, accepted (with revisions): No-
vember 30, 1996
0 1997, ELSEV IER SCIENCE INC.
ALL RIGHTS RESERVED
patients presenting with symptoms of prostatism un-
dergo an assessmentof renal function by the mea-
surement of serum creatinine.’ Although it has been
suggested hat approximately 14 of men with symp-
tomatic BPH have evidence of renal insufficiency, this
is likely to be an overestimation becausemost studies
evaluating the relationship between BPH and renal
function have been performed in patients undergoing
prostatectomy.
4+g In contrast, little information has
been presented regarding renal dysfunction in men
undergoing evaluation of lower urinary tract symp-
toms of varying severity.l’ In the present study, the
results of serum creatinine measurements n 246 con-
secutive men with symptomatic BPH were correlated
with symptom score, age, quality-of-life measures,
and comorbid disease to help define the usefulness
of creatinine determinations in the evaluation and
treatment of such patients.
MATERIAL AND METHODS
Between July 1995 and January 1996,246 consecutive men
(aged 45 years or older) who presented to the urology clini
c
0090-4295/97/$17.00
PI1 SOOUO-4295(97)00069-l 697
-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
2/6
TABLE I. Baseline data in 246 consecutive patients presenting
for
evaluation of lower urinary tract symptoms secondary to
benign
prostatic hyperplasia
History of
No History of
All Patients DM or HTN DM or HTN
(n = 246) (n = 109)
(n = 137)
Age [yr s, mean + SD) 66.0 + 9.8*
67.3 2 9.3 64.9 +- 1 O.O*
Symptom score-IPSS
[mean k SD) 13.4 2 7.9
13.5 f 7.9 13.3 + 8.0
Mild (O-7) 72 (29 ) 28 (26 ) 44 (32 )
Moderate (8- 19) 1 15 (47 ) 57 (52 ) 58 (42 )
Severe (20-35)
59 (24 ) 24 (22 ) 35 (26 )
Qual ity-of-life score (mean t SD) 2.9 + 1.6 3.0 f 1.5 2.8 -e
1.6
DM 35 (14 ) 35 (32 )
-
HTN 87 (35 ) 87 (80 )
-
Serum creatinine (mg/dL)
(mean ? SD)
1.12 + 0.29* 1.17 t 0.33 1.08 k 0.24*
Abnormal serum creatinine
(> 1.4 mg/dL) 26 (1 l )*
17 (16 ) 9 (70/o)*
K E Y .
DM = diabetes mellitus; HTN = hypertension; IPSS = International
Prostate Symptom Score.
*Missing
value in I patient.
at the University of Chicago with lower urinary tract symp-
toms secondary to BPH underwent initial e valuation as rec-
ommended by the guidelines panel of the Agency for Health
Care Policy and Research.’ This evaluation included comple-
tion of the International Prostate Symptom Score (IPSS),
med-
ical history, physical e xamination, urinalysis, and
measure-
ment of serum creatinine. Further testing of patients was at
the discretion of the treating physician. Patients with a
history
of chronic renal insufficiency, prostate cancer, or surgical
treatment for BPH, as well as those with co mplete urinary
retention at the time of evaluation, were excluded from this
analysis. The normal range of serum creatinine measurements
was considered to be 0.5 to 1.4 mg/dL. Those patients with
an elevated serum creatinine level underwent further evalu-
ation, including renal ultrasonography, measurement of post-
void residual (PVR) urine volume, or repeat serum creatinine
measurements, at the discretion of the treating physician.
The
decision to initiate medica l or surgical therapy for BPH
was
made based on patient preference after consultation with the
physician.
Statistic al analysis was performed using multiple logistic
regression to determine the risk (odds ratio) of having an
abnormal serum creatinine level as a function of age, symp-
tom score, quality-of-life score, and the presence of
comorbid
disease (diabetes mellitus or hypertension). Parameter esti-
mates were obtained using the method of maximum likeli-
hood, and significan ce levels were based on Wald ’s test.”
P values less than or equal to 0.05 were regarded as
statisti-
cally significant. The 95% confidence intervals for the true
odds ratios were also calculated.
RESULTS
Among the 246 consecutive patients presenting
for evaluation of lower urinary tract symptoms
secondary to BPH, 2 had incomplete data (Table
I). Descriptive statistics for all patients are shown
in the first column of Table I. The mean age was
66 years (range 43 to 90). Slightly fewer than one
third of the patients had symptom scores in the
698
mild range (0 to 7), nearly one half had scores in
the moderate range (8 to 19>, and about one quar-
ter had scores in the severe range (20 to 35). The
mean quality of life score from the IPSS was 2.9.
A history of diabetes or hypertension was noted in
14 and 35 of the patients, respectively. The
overall mean serum creatinine measurement was
1.12 mg/dL, and 11 of men (26 of 245) had an
abnormal level at the time of initial evaluation.
Results are also presented separately for men
with and without a history of diabetes or hyper-
tension, because the presence of these common,
chronic comorbid diseases is likely to affect serum
creatinine measurements independently of the ef-
fects of BPH. Men with a history of either of these
diseases were slightly older, but they had similar
symptom and quality-of-life scores. However, the
finding of an elevated serum creatinine was noted
more than twice as often in these men compared
with those without a history of these diseases (16
[17 of 1091 versus 7 [9 of 1361).
Descriptive data regarding serum creatinine lev-
els stratified by symptom score (mild, moderate,
or severe), as well as by the presence or absence
of the comorbid conditions, are presented in Table
II. Consistent differences in creatinine levels and
the percentage of patients with abnormal mea-
surements are again seen between those with a his-
tory of diabetes or hypertension compared with
those with no history of either of these diseases.
However, there is no apparent trend of increasing
creatinine levels with increasing symptom scores.
Based on multiple logistic regression analysis in-
corporating the effects of age, symptom score
(treated as a continuous variable), quality-of-life
UROLOGY 49 (51, 1997
-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
3/6
TABLE
II. Serum creatinine measurements and incidence of
abnormal creatinine levels in patients presenting with
symptomatic
BPH stratified by symptom score (IPSS)
Mild Moderate Severe
(IPSS O-7) (IPSS 8-l 9) (IPSS 20-35)
All patients
No. 72 115
58
Mean + SD 1.09 t 0.27 1.15 k 0.32 1.10 + 0.24
No. abnormal 9 (12.5 ) 13 (11.3 ) 4 (6.9 )
History of diabetes or
hypertension
No. 28 57
24
Mean 2 SD 1.14 t 0.32 1.20 2 0.35 1.1 1 2 0.28
No. abnormal
6 (2 1.4 ) 9 (15.8 ) 2 (8.3 )
No history of diabetes
or hypertension
No. 44 58
34
Mean t SD 1.06 t 0.22 1.09 k 0.27
1.09 5 0.20
No. abnormal
3 (6.8 ) 4 (6.9 ) 2 (5.9 )
KEY : IPSS = International Prostate Sympto m Score.
score, and comorbidity (Table III), only a history
of diabetes or hypertension was significantly as-
sociated with the presence o f renal insufficiency
(P = 0.045). After excluding patients with either
or both of these comorbid diseases, increasing age
was significantly associated with the finding of an
elevated creatinine (Table III). However, neither
the overall symptom score nor the quality-of-life
measure significantly predicted the finding of an
elevated creatinine measurement among the entire
group of patients studied or among those without
a history of diabetes or hypertension.
The mean age and symptom score in the 9 pa-
tients with an elevated creatinine measurement
(more than 1.4 mg/dL) and no history of diabetes
or hypertension were 71.4 years and 12.6, respec-
tively. In the 17 patients with an abnormal creat-
inine level and a history of either or both of these
diseases, the mean age and symptom score were
68.0 years and 10.9, respectively. Minimally ele-
vated creatinine measurements (1.5 to 1.6 mg/dL)
were noted in 6 of 9 men (67 ) without comorbid
disease, whereas 2 patients in this group had levels
of 1.7 mg/dL and 1 had a level of 2.4 mg/dL (Fig.
1). Evidence of upper urinary tract dilation or a
significantly increased PVR urine volume (100 cc
or greater) were noted in only 1 of these 9 men.
Among the 17 patients with an abnormal creati-
nine level as well as diabetes or hypertension, 7 of
17 men (41 ) had minimal elevations. The re-
maining 10 patients in this group had creatinine
measurements of 1.7 to 2.4 mg/dL, although only
3 of 17 (18 ) patients had evidence of hydrone-
phrosis or a PVR of greater than 100 cc. Finally,
among men younger than 60 years of age with or
without a history of comorbid disease, an abnor-
UROLOGY 49 (S), 1997
ma1 creatinine measurement was noted in only 1
of 23 (4.3 ) and 1 of 39 (2.6 ) cases, respectively
(Fig. 1).
COMMENT
Voiding dysfunction secondary to BPH signifi-
cantly affects the health and quality of life of many
TABLE III. Effects of patient age, symptom
score, quality-of-life score, and presence
of comorbid disease (diabetes mellitus or
hypertension) on incidence of abnormal serum
creatinine measurement using multiple logistic
regression analysis * in all patients and
in those men with no history of diabetes
mellitus or hypertension
(95
Odds Confidence
Ratio Interval1 P Value
All patients
Age (per decade) 1.56
Symptom score
(per 10 points) 0.46
Quality-of-life score 1.21
Presence of
diabetes or
hypertension 2.42
No history of
diabetes mellitus
or hypertension
Age (per decade) 2.17
Symptom score
(per 10 points) 0.57
Quality-of-life score 1.26
*Univariate analysis gave simila r results.
(0.97, 2.52) 0.067
(0.19, 1.14) 0.092
(0.80, 1.81)
0.363
(1.02, 5.76) 0.045
(1 .Ol, 4.67) 0.046
(0.13, 2.58) 0.469
(0.65, 2.44) 0.497
699
-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
4/6
2.5 A
i
2.0
1
E -
.-
.5
* l
3 . t * . .
s
" 1.5-
0 .
E
.
* f.
3k
i
*
2
. .
2
.
2..
v) . . . 2 . * l . . 12 . 2 *
l 2 . . . ** 222' * . .*
1.0 * l * 2 2 3 24*222 2 3'*2 2' *
2 .2 . 2 0. 3." .2... . f
0 2 * . . ..J.
.
.
OS . . . . . . . . . ..“ .“...“..““..“.........“.““~
40
50 70
0 60 90
Age
.
.
. f . .
*
*
.
. . .
. f . .
2 2 l *
* .
.
. . a . * . .
* . a . . . . . *
2
. . . 2. ‘2
.
3'2 2
**2* 4 322'3.
32. '2. f..
.
(I '4.2 .+.
. *
222' f
I .
. '2. . . 2
.
.
.
I
.
.
r
5 10 25
34 35
2.5
1
C
*
. I I
f
2
3
. .
" 1.5 . .
5 .*
.
f
0
$
2
3
4 2
cn -2 . 6 2 3 3
.2 6 4 5 2 .
1.0-2 6 a 9 2 5 3
.2 6 3 3 4 4 2
. 4 3 2 *
. . .
.
0.5 I
1 2 3 4 5 6
Quality of Life Score
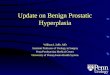
FIGURE 1. The re/UtionShip be-
tween (A) serum creatinine and
patient age, (B) symptom score,
and(C) qual ity-of-life score in men
with no history of diabetes or hy-
pertension. A single asterisk indi-
cates 1 patient, and the numbers
2 to 9 indicate the number of pa-
tients at each observation point.
Those patients with asterisks
above the horizontal line had ab-
normal serum creatinine levels.
700
UROLOGY 49 61, 1997
-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
5/6
older men. As a result, all aspects of the evaluation
and treatment of patients with lower urinary tract
symptoms warrant careful scrutiny. It has been
well documented that bladder outlet obstruction
by an enlarging prostate can lead to renal insuffi-
ciency. However, the likelihood of this occurrence,
the relationship between symptom severity and
the finding of an elevated serum creatinine mea-
surement, and the impact of age and comorbid dis-
ease on renal function in men with BPH have not
been well studied.3,5,10,12
In the present analysis of 246 consecutive men
presenting for the evaluation of voiding symp-
toms, the incidence of renal dysfunction (serum
creatinine greater than 1.4 mg/dL) was 11 (26 of
245). Among all patients studied, only a history of
diabetes or hypertension significantly predicted
the presence of an elevated creatinine measure-
ment. Minimal abnormalities (serum creatinine of
1.5 to 1.6 mg/dL) were noted in many patients,
and most men with renal insuff iciency had no ev-
idence of upper urinary tract changes or poor blad-
der emptying. Most importantly, symptom sever-
ity and quality-of-life measures correlated poorly
with the presence of elevated creatinine levels and
could not be used to accurately predict the likeli-
hood of renal insufficiency secondary to BPH. It is
possible, however,
that inclusion of men with
more severe symptoms, such as those with com-
plete urinary retention and those undergoing sur-
gery, would have demonstrated a correlation be-
tween increasing symptom severity and renal
dysfunction.
Previous attempts to define the incidence of renal
dysfunction in men with BPH have primarily fo-
cused on patients with complete urinary reten-
tionl2*l3
and those with sufficiently severe symp-
toms to warrant surgical intervention.2*4-g’14 In
these studies, as many as 30 of men had evidence
of renal insufficiency.4 More recently, Koch et al.”
reported that 9.5 of men with lower urinary tract
symptoms of varying severity had an elevated se-
rum creatinine, although this study also included
men with complete urinary retention. These au-
thors noted that only 3 of 32 (9 ) patients with
minimally abnormal creatinine measurements had
evidence of upper tract dilation, whereas 33 (7 of
21) of those men with a more significantly elevated
creatinine level had hydronephrosis of varying de-
grees. Although Koch et al. found no correlation
between symptom severity and the finding of renal
insufficiency, no attempt was made in their study
to investigate the relationship of comorbid disease
and abnormal creatinine measurements. Overall, it
appears that medical renal disease secondary to di-
abetes and hypertension is the most common cause
of renal dysfunction in older men with lower uri-
nary tract symptoms and BPH.
The limited likelihood of significant renal insuffi-
ciency in men presenting for the evaluation of symp-
tomatic BPH might suggest that determination of se-
rum creatinine could be omitted in selected groups
of patients in an effort to contain costs. In addition
to measuring creatinine, many patients with abnor-
malities will require an assessment of PVR urine vol-
ume or radiographic evaluation of the upper urinary
tract, which will further increase costs. Because the
number of men with BPH who annually undergo
evaluation in the United States is very large,l even
limited reduction of testing in such patients could
significantly lower the overall economic impact as-
sociated with the management of voiding symptoms
in older men. However, avoidance of screening for
renal dysfunction even in selected patients with BPH
appears to be unwise for several reasons. First, as
was noted by Koch et al.,lO we found it difficult to
identify subgroups of patients in whom the risk of
renal insufficiency was limited enough to avoid rou-
tine serum creatinine measurement. The lack of cor-
relation of symptom severity and renal dysfunction
is supported by the findings of Mukamel et al.,5 who
also reported on several patients with occult and
progressive renal damage secondary to BPH who had
minimal voiding symptoms. We did find, however,
that significant renal insufficiency was rare in men
younger than 60 years of age, which was also noted
by Mukamel and coworkers. In contrast, Koch et
allo could not identify a significant correlation be-
tween increasing patient age and a greater likelihood
of upper urinary tract dilation.
Other factors that argue against the omission of
screening for renal dysfunction in men with voiding
symptoms and BPH include the economic impact of
renal failure and its deleterious effects on overall
health.15 Irreversible upper urinary tract changes in
patients with prostatic enlargement may occur, and
progressive renal insufficiency leading to the need
for dialysis can be seen, despite relief of bladder out-
let obstruction.3z12 The long-term direct and indirect
costs associated with renal insufficiency and dialysis
are significant, and it is unlikely that the economic
benefit derived from the elimination of routine se-
rum creatinine measurements would outweigh the
costs associated with even the rare patient who de-
veloped chronic renal failure. Therefore, early detec-
tion of renal insufficiency in men with BPH is likely
to be cost-effect ive because it will presumably lead
to the introduction of appropriate therapy and
avoidance of long-term renal damage. Routine mea-
surement of serum creatinine in men with BPH also
serves as a baseline assessment of renal function,
which may be of value in those patients with pro-
gressive voiding dysfunction who return for repeat
evaluation. Finally, determination of serum creati-
nine in patients with symptomatic BPH is appropri-
ate because the potential effectiveness and morbidity
UROLOGY 49 (51, 1997
701
-
8/9/2019 SERUM CREATININE MEASUREMENTS IN MEN WITH LOWER URINARY
TRACT SYMPTOMS SECONDARY TO BENIGN PROSTATIC HYPERPLASIA
6/6
of therapy are adversely affected by the presence o f
renal insufficiency. Specifically, the use of alpha-l
receptor antagonists, such as terazosin and doxazo-
sin, may be problematic in men with renal dysfunc-
tion because of blood pressure abnormalities or
other factors. In addition, the results of prostatic sur-
gery in men with chronic bladder distension or az-
otemia are often less successful and are more fre-
quently associated with complications than in
patients with normal renal and bladder func-
tion.
12,16,17
CONCLUSIONS
In patients with lower urinary tract symptoms
secondary to BPH presenting for evaluation, a his-
tory of diabetes mellitus or hypertension is signif-
icantly associated with the likelihood of an abnor-
mally elevated serum creatinine measurement.
Among men with no history of these comorbid
diseases, increasing age also predicts a greater
chance of renal insufficiency. Neither symptom
score nor the quality-of-life measure from the IPSS
is associated with serum creatinine levels. In most
patients with BPH and renal dysfunction, medical
renal disease secondary to diabetes or hyperten-
sion is the most likely cause of elevated serum cre-
atinine measurements. Despite the infrequent oc-
currence of azotemia secondary to bladder outlet
obstruction in patients with voiding symptoms
and BPH, it still appears appropriate to measure
serum creatinine routinely to avoid long-term ad-
verse sequelae and improve the likelihood of suc-
cessful treatment outcomes.
REFERENCES
1. McConnell JD, Barry MJ, Bruskewitz RC, Bueschen AJ,
Denton SE, Holtgrewe HL, Lange JL, McClennan BL, Mebust
WK, Reilly NJ, et al: Benign Prostatic Hyperplasia:
Diagnosis
and Treatment. Quick Reference Guidefor Clinicians. (AHCPR
publication no. 94-0583). Rockville, Md, Agency for Health
Care Policy and Research, Public Health Service, US Depart-
ment o f Health and Human Services, February 1994.
2. Bohne AW, Urwiller RD, and Pantos TG: Routine in-
travenous urograms prior to prostatectomy. J Urol 86: 171-
172, 1961.
3. Sacks SH, Aparicio SAJR, Bevan A, Oliver DO, Will EJ,
and Davison AM: Late renal failure due to prostatic outflow
obstruction: a preventable disease. BMJ 298: 156-159, 1989.
4. Roehrborn CG: Initial diagnostic evaluation of men
with lower urinary tract symptoms, in Cockett ATK, Khoury
S, Aso Y, Chatelain C, Denis L, Griffiths K, Murphy G (Eds):
Proceedings of the 3rd International Consultation on Benign
Prostatic Hyperplasia (BPH). Geneva, Scient ific Communica-
tion International Ltd., 1996, pp 167-254.
5. Mukamel E, Nissenkom I, Boner G, and Servadio C: Oc-
cult progressive renal damage in the elderly male due to
benign
prostatic hypertrophy. J Am Geriatr Sot 27: 403-406, 1979.
6. Lilienfeld RM, Berman M, Khedkar M, and Sporer A:
Comparative evaluation of intravenous urogram and ultra-
sound in prostatism. Urology 26: 310-312, 1985.
7. Cascione CJ, Bartone FF, and Hussain MB: Transab-
dominal ultrasound versus excretory urography in preopera-
tive evaluation of patients with prostatism. J Urol 137:
883-
885, 1987.
8. Bauer DL, Garrison RW, and McRoberts JW: The health
and cost implications of routine excretory urography before
transurethral prostatectomy. J Urol 123: 386-389, 1980.
9. Donker PJ, and Kakiailatu F: Preoperative evaluation
of patients with bladder outlet obstruction with particular
re-
gard to excretory urography. J Urol 120: 685-686, 1978.
10. Koch WFRM, Ezz El Din K, de Wildt MJAM, Debruyne
FMJ, and de la Rosette JJMCH: The outcome of renal ultra-
sound in the assessment of 556 consecut ive patients with
be-
nign prostatic hyperplasia. J Urol 155: 186- 189, 1996.
11. Hosmer DW, and Lemeshow SL: Applied Logistic Re-
gression.
New York, John Wiley and Sons, 1989.
12. Nissenkorn 1, Savion M, and Servadio C: Renal and
bladder function recovery after prostatectomy in patients
with
a chronic residual urine of above 1,000 ml. Eur Urol14: 434-
436, 1988.
13. Marshall W, Singh M, and Blandy JP: Is urography nec-
essary for patients with acute retention of urine before
pros-
tatectomy? Br J Uro146: 73-76, 1974.
14. Fidas A, Mackinlay JY, Wild SR, and Chisholm GD:
Ultrasound as an alternative to intravenous urography in
prostatism. Clin Radio1 38: 479-482, 1987.
15. Strange PD, and Sumner AT: Predicting treatment costs
and li fe expectancy in end stage renal disease. N Engl J
Med
298: 372-376, 1978.
16. Mebust WK, Holtgrewe HL, Cockett ATK, and Peters PC:
Transurethral prostatectomy: immediate and postoperative
com-
plications. A cooperative study of 13 participating
institutions
evaluating 3885 patients. J Urol 141: 243-247, 1989.
17. Melchior J, Valk WL, Foret JD, and Mebust WK: Trans-
urethral prostatectomy in the azotemic patient. J Urol 112:
643-647, 1974.
702
UROLOGY 49 (5), 1997