Embed Size (px)
Citation preview

233Saudi Journal of Medicine & Medical Sciences | Vol. 3 | Issue 3 | September 2015 | 233-237
Sertoli-Leydig Cell Tumor of the Ovary in a Young Female: A Case Report and Literature Review
Madan M. Gupta, Nandini U. Bahri, Rathod KetanDepartment of Radiodiagnosis and Imaging, Gurugovind Singh Hospital, M. P. Shah Medical College, Jamnagar, Gujarat, India
Correspondence: Dr. Madan Mohan Gupta, Department of Radiodiagnosis and Imaging, Gurugovind Singh Hospital, M.P. Shah Medical College, Jamnagar, Gujarat, India. E-mail: [email protected]
CASE REPORT
A 21-year-old nulliparous female presented with complaints of pelvic pain, acne, hirsutism, hoarseness of voice and oligomenorrhea for the last 6 months. No history of anorexia, weight loss, increased libido, or breast recession was noted. Her medical and family history was unremarkable. Vaginal examination revealed clitoromegaly and a firm and mobile solid mass in the left adnexa. Laboratory tests showed elevated serum testosterone 27.6 ng/mL (normal range: 0.2-1.2 ng/mL) and dehydroepiandrosterone of 16.3 ng/mL (normal range: 0.8-3.2 ng/mL), and normal CA-125 of 22 U/mL (normal range <35 U/mL). All other laboratory tests including complete blood count, renal, bone, hepatic and coagulation profiles, alkaline phosphatase, carcinoembryonic antigen, luteinizing hormone, follicle stimulating hormone levels were within normal ranges.
The patient was referred to imaging workup to our department. Ultrasound showed a large well-circumscribed, well-marginated heterogeneous mixed
Access this article onlineQuick Response Code:
Website:www.sjmms.net
DOI:10.4103/1658-631X.162038
A B S T R A C T
Sertoli-Leydig cell tumor (SLCT) of the ovary is an exceedingly unusual neoplasm that belongs to a group of sex-cord-stromal tumors of ovary and accounts for <0.5% of all primary ovarian neoplasms. We present a case of primary ovarian SLCT in a 21-year-old female, who presented with a 6-month history of a pelvic pain, acne, hirsutism, and oligomenorrhea with elevated testosterone and dehydroepiandrosterone levels. Ultrasound and contrast computed tomography revealed well-defined hyper vascular heterogeneous solid lesion in left adnexa. Magnetic resonance imaging demonstrated ovarian origin of tumor, which turned out SLCT on histopathology. In this case, we discuss multimodality imaging findings of SLCT and its management aspects with review of literature.
Key words: Acne, hirsutism and oligomenorrhea, primary ovarian neoplasms, Sertoli-Leydig cell tumor
ملخص البحث :تعتبر خاليا سيرتولى اليدج السرطانية بالمبيض من األورام النادرة وتشكل اقل من %0.5 من كل سرطانات المبيض. يستعرض الباحثون حالة لمريضة في الواحد والعشرين من عمرها تشكو من الم في الحوض، حب الشباب، اضطراب ونقص في الدورة الشهرية، ظهور الشعر في غير
مواضعه مع ارتفاع هرمون التستيرون في الدم. بينت األشعة الصوتية والمقطعية وجود ورم بالقرب من المهبل كما وضح الفحص بالرنين المغنطيسي أن منشأ الورم هو المبيض وأظهر الفحص المجهري خاليا سيرتولي السرطانية بالمبيض. يناقش الباحثون الجوانب واألدبيات.
INTRODUCTION
Sertoli-Leydig cell tumor (SLCT) is a rare ovarian tumor that belongs to the group of sex-cord-stromal tumors. These constitute <0.5% of ovarian tumors.[1] Most tumors are unilateral, confined to the ovaries, and are seen during the second and third decades of life. These tumors are characterized by the presence of testicular structures that produce androgens. Hence, many patients have symptoms of virilization depending on the quantity of androgen production. We present a case of SLCT with multimodality imaging findings and its management issues.
case repOrt
[Downloaded free from http://www.sjmms.net on Wednesday, February 24, 2016, IP: 41.45.223.130]
Gupta, et al.: Sertoli-Leydig Cell Tumor of the Ovary
Saudi Journal of Medicine & Medical Sciences | Vol. 3 | Issue 3 | September 2015234
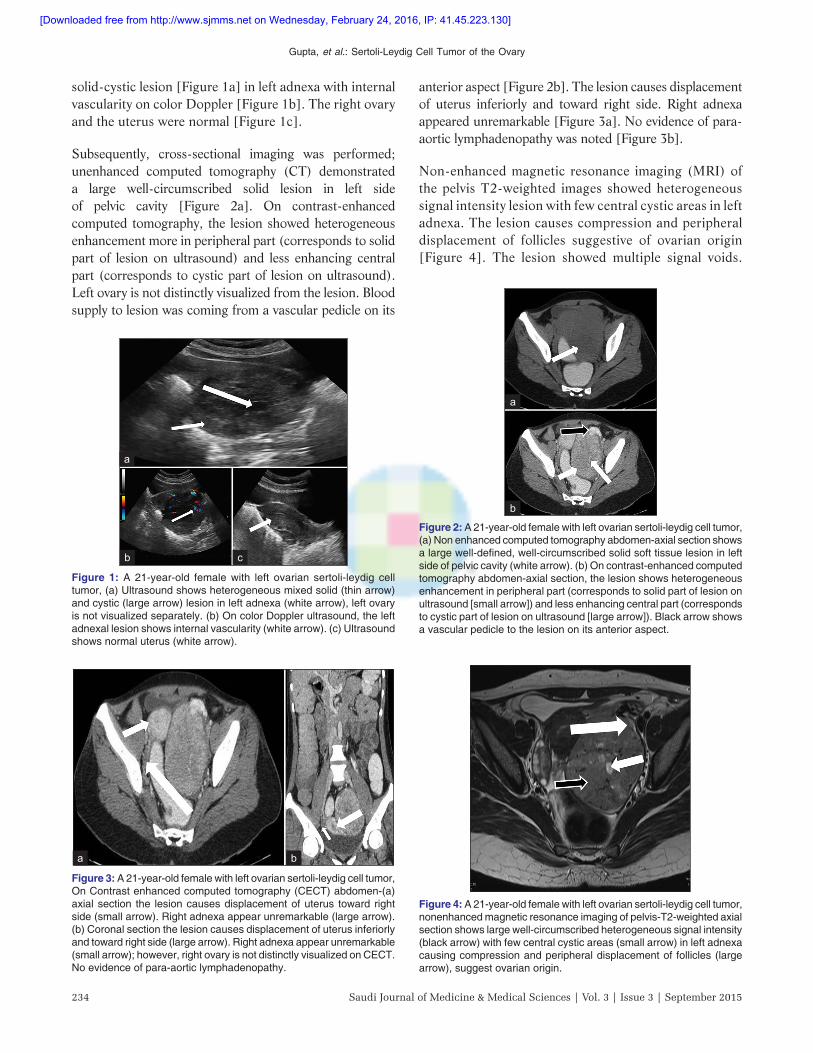
anterior aspect [Figure 2b]. The lesion causes displacement of uterus inferiorly and toward right side. Right adnexa appeared unremarkable [Figure 3a]. No evidence of para-aortic lymphadenopathy was noted [Figure 3b].
Non-enhanced magnetic resonance imaging (MRI) of the pelvis T2-weighted images showed heterogeneous signal intensity lesion with few central cystic areas in left adnexa. The lesion causes compression and peripheral displacement of follicles suggestive of ovarian origin [Figure 4]. The lesion showed multiple signal voids.
solid-cystic lesion [Figure 1a] in left adnexa with internal vascularity on color Doppler [Figure 1b]. The right ovary and the uterus were normal [Figure 1c].
Subsequently, cross-sectional imaging was performed; unenhanced computed tomography (CT) demonstrated a large well-circumscribed solid lesion in left side of pelvic cavity [Figure 2a]. On contrast-enhanced computed tomography, the lesion showed heterogeneous enhancement more in peripheral part (corresponds to solid part of lesion on ultrasound) and less enhancing central part (corresponds to cystic part of lesion on ultrasound). Left ovary is not distinctly visualized from the lesion. Blood supply to lesion was coming from a vascular pedicle on its
Figure 4: A 21-year-old female with left ovarian sertoli-leydig cell tumor, nonenhanced magnetic resonance imaging of pelvis-T2-weighted axial section shows large well-circumscribed heterogeneous signal intensity (black arrow) with few central cystic areas (small arrow) in left adnexa causing compression and peripheral displacement of follicles (large arrow), suggest ovarian origin.
Figure 1: A 21-year-old female with left ovarian sertoli-leydig cell tumor, (a) Ultrasound shows heterogeneous mixed solid (thin arrow) and cystic (large arrow) lesion in left adnexa (white arrow), left ovary is not visualized separately. (b) On color Doppler ultrasound, the left adnexal lesion shows internal vascularity (white arrow). (c) Ultrasound shows normal uterus (white arrow).
a
b c
Figure 2: A 21-year-old female with left ovarian sertoli-leydig cell tumor, (a) Non enhanced computed tomography abdomen-axial section shows a large well-defined, well-circumscribed solid soft tissue lesion in left side of pelvic cavity (white arrow). (b) On contrast-enhanced computed tomography abdomen-axial section, the lesion shows heterogeneous enhancement in peripheral part (corresponds to solid part of lesion on ultrasound [small arrow]) and less enhancing central part (corresponds to cystic part of lesion on ultrasound [large arrow]). Black arrow shows a vascular pedicle to the lesion on its anterior aspect.
a
b
Figure 3: A 21-year-old female with left ovarian sertoli-leydig cell tumor, On Contrast enhanced computed tomography (CECT) abdomen-(a) axial section the lesion causes displacement of uterus toward right side (small arrow). Right adnexa appear unremarkable (large arrow). (b) Coronal section the lesion causes displacement of uterus inferiorly and toward right side (large arrow). Right adnexa appear unremarkable (small arrow); however, right ovary is not distinctly visualized on CECT. No evidence of para-aortic lymphadenopathy.
a b
[Downloaded free from http://www.sjmms.net on Wednesday, February 24, 2016, IP: 41.45.223.130]

Gupta, et al.: Sertoli-Leydig Cell Tumor of the Ovary
235Saudi Journal of Medicine & Medical Sciences | Vol. 3 | Issue 3 | September 2015
Uterus and right ovary appeared unremarkable [Figure 5a]. T1-weighted image demonstrated isointense signal and multiple signal voids [Figure 5b]. On the basis of above clinical, biochemical and imaging findings diagnosis of androgenic neoplastic primary ovarian tumor was made. The patient underwent for exploratory laparotomy. Intraoperatively left ovary is replaced by a large capsulated solid grey-white mass [Figure 6a]. The right ovary and uterus were found unremarkable. Left salpingo-oophorectomy was performed. Gross examination of the pathologic specimen [Figure 6b] showed an ovarian mass with smooth external grayish surface. A cut-section of the specimen [Figure 6c] revealed solid as well as cystic areas filled with clear fluid. The histopathological examination showed a tumor composed of poorly formed cords, nests, and tubules of tumor cells. Tumor cells had hyperchromatic nuclei, a moderate amount of cytoplasm (Sertoli cells), and occasional mitosis [Figure 6d]. Interspersed between these were nests of polygonal cells with round nuclei and abundant granular cytoplasm (Leydig cells). Final diagnosis was intermediately differentiated SLCT on histopathology. After her consent, one cycle for four cycles of chemotherapy with a bleomycin, etoposide, and cisplatin regimen were administered every 3 weeks. The patient tolerated the chemotherapy well, with no major complications. During 10-month of follow-up, the patient has resumed her periods, with resolution of her virilization symptoms. There is also no increase of
her hirsutism. Repeat testosterone levels on follow-up were within normal range. After 2 years of operation, at present the patient leads a symptom free life.
DISCUSSION
Sertoli-Leydig cell tumor is a very rare ovarian tumor that included in the group of sex-cord-stromal tumors and they account for <0.5% of all primary ovarian tumors.[1] It is usually seen during reproductive age group (second and third decades of life).[1-5] Clinical presentation is related to either hormonal production (mostly androgen and rarely estrogen)[6] or presence of mass-occupying lesion.[1-5] Androgen-excess manifestations include virilism, hirsutism, and hoarseness of voice, clitoromegaly, oligomenorrhea, and amenorrhea.[7,8]
Imaging studies can be utilized in the diagnosis of ovarian SLCTs. Sonography remains the best imaging modality of preference for initial assessment of adnexal masses, due to its high sensitivity, suitability, and cost-effectiveness.[7,9] In general, SLCTs exhibit solid sonographic appearance[7,9] and mostly unilateral tumors.[1-3,5] Mixed (solid and cystic) components are most commonly encountered in roughly 60% of all ovarian SLCTs.[1] Color Doppler sonography offers further categorization and evaluation of neoplastic masses. Moderate-to-rich ovarian vascular masses with low-resistance indices highly suggest malignant rather than benign lesions. Other imaging modalities such as
Figure 5: A 21-year-old female with left ovarian sertoli-leydig cell tumor, nonenhanced magnetic resonance imaging of pelvis-(a) T2-weighted axial section, the left ovarian lesion shows multiple signal voids (large arrow) and causes displacement of uterus toward right side (curved arrow). Uterus and right ovary appears unremarkable (small arrow). (b) T1-weighted axial section, the left ovarian lesion isointense signal intensity (small arrow) and multiple signal voids (large arrow).
ab Figure 6: (a) Intraoperative highly vascular ovarian lesion (small arrow)
and fallopian tube (large arrow) and uterus (black arrow). (b) Gross specimen shows well-encapsulated grayish solid mass. (c) Cut-section of specimen shows tan-yellow nodular appearance (white arrow). (d) Microscopically, Photomicrograph showing hyperchromatic nuclei, moderate cytoplasm (Sertoli cells [black arrow]) and nests of polygonal cells with round nuclei and abundant granular cytoplasm (Leydig cells with heterologous elements showing mucinous epithelium of the gastrointestinal type [white arrow]) (H and E ×40).
a b
dc
[Downloaded free from http://www.sjmms.net on Wednesday, February 24, 2016, IP: 41.45.223.130]

Gupta, et al.: Sertoli-Leydig Cell Tumor of the Ovary
Saudi Journal of Medicine & Medical Sciences | Vol. 3 | Issue 3 | September 2015236
CT, MRI, and positron imaging tomography scans can be used for better characterization of ovarian SLCTs, detection of extra ovarian disease/metastasis. SLCTs appear hyper vascular mixed solid-cystic lesion within adnexa on CT or MRI. Cross-sectional imaging can be used for staging of tumor preoperatively.
Macroscopically,[10] SLCTs are well-encapsulated, solid, firm, and yellow-gray mass. Cut-section surface exhibits varying degrees of greasy/fleshy consistency, straw-colored fluid, necrosis, hemorrhage, and cystic spaces separated by fibrous septae. Microscopically,[10] SLCTs are made up of uncontrolled proliferation of differentiation of tubules lined by Sertoli cells and intervening nests of Leydig cells. Leydig cells are typically found in clusters in interstitial stroma and exhibit polygonal cells with well-defined margins, centric nuclei, prominent nucleoli, and eosinophilic cytoplasm. Sertoli cells typically form tubular structures lined by single or multiple layers of cuboidal-columnar cells with well-bounded margins, oval dark nuclei, inconspicuous nucleoli, and eosinophilic or vacuolated cytoplasm.
Pathologically, SLCT are divided into four subtypes: Well-(11%), intermediately-(54%), and poorly differentiated (13%) and contained heterologous elements (22%). Heterologous elements are various, such as carcinoid, mesenchymal, and mucinous epithelial tissues with the commonest being gastrointestinal-types.[10] Retiform pattern presents in 15% of SLCT, and is found only in intermediately and poorly differentiated SLCT, and often occurs in younger women.[10] SLCT contains Sertoli cells, Leydig cells, gonadal stromal cells and heterologous cells in tumors with heterologous elements. Leydig cells scatter among numerous Sertoli cells, which may arrange into open or closed tubules.
The most important prognostic factors in these tumors are their stage and degree of differentiation. In a review of 207 cases by Young and Scully in 1985,[10] all well-differentiated tumors were benign, whereas 11% of tumors with intermediate differentiation, 59% of tumors with poor differentiation, and 19% of those with heterologous elements were malignant. In another study of 64 patients who had intermediate or poorly differentiated SLCT, a survival rate of 92% was noted at both 5 and 10 years.[11]
Most of these tumors are unilateral and diagnosed in Stage I, so conservative surgery in a young patient
is an appropriate treatment. There have also been case reports of successful laparoscopic management of these tumors.[11] Adjuvant chemotherapy is considered for patients who have poor prognostic factors.
The malignancy rate in tumors with heterologous elements is 15-20%. Adjuvant chemotherapy in Stage I is given to those patients who have poorly differentiated SLCT or SLCT with heterologous elements or a metastatic tumor of any histologic type.[12]
Surgical resection represents the mainstay of management of ovarian SLCTs.[4] Therefore, fertility-sparing surgery (unilateral salpingo-oophorectomy) can be considered in all patients with well-differentiated ovarian SLCTs. In general, postoperative chemotherapy is considered for patients with poor prognostic factors such as advanced disease staging, moderate-to-poor tumor grading, high mitotic profile, existence of heterologous elements, and tumor rupture.[1-3] Prognosis of ovarian SLCTs is significantly correlated with degree of tumor differentiation (grading) and tumor extent (staging).[1] Long-term follow-up is highly advised in all patients.
CONCLUSION
Sertoli-Leydig cell tumor is a rare ovarian sex-cord tumor of the ovary with good prognosis postoperatively. Hence, imaging findings may help in early detection and preoperative differentiation and staging of SLCT in young female. Its management depends on degree of differentiation and staging of tumor, which mostly depend on histopathology.
REFERENCES1. Young RH, Scully RE. Ovarian Sertoli-Leydig cell tumors. A
clinicopathological analysis of 207 cases. Am J Surg Pathol 1985;9:543-69.
2. Zaloudek C, Norris HJ. Sertoli-Leydig tumors of the ovary. A clinicopathologic study of 64 intermediate and poorly differentiated neoplasms. Am J Surg Pathol 1984;8:405-18.
3. Roth LM, Anderson MC, Govan AD, Langley FA, Gowing NF, Woodcock AS. Sertoli-Leydig cell tumors: A clinicopathologic study of 34 cases. Cancer 1981;48:187-97.
4. Weng CS, Chen MY, Wang TY, Tsai HW, Hung YC, Yu KJ, et al. Sertoli-Leydig cell tumors of the ovary: A Taiwanese Gynecologic Oncology Group study. Taiwan J Obstet Gynecol 2013;52:66-70.
5. Young RH, Scully RE. Sex cord-stromal, steroid cell, another ovarian tumors. In: Kurman RJ, editor. Blaustein’s Pathology of Female Genital Tract. 5th ed. New York, NY, USA: Springer; 2002. p. 929.
[Downloaded free from http://www.sjmms.net on Wednesday, February 24, 2016, IP: 41.45.223.130]
Gupta, et al.: Sertoli-Leydig Cell Tumor of the Ovary
237Saudi Journal of Medicine & Medical Sciences | Vol. 3 | Issue 3 | September 2015
How to cite this article: Gupta MM, Bahri NU, Ketan R. Sertoli-leydig cell tumor of the ovary in a young female: A case report and literature review. Saudi J Med Med Sci 2015;3:233-7.
Source of Support: Nil, Conflict of Interest: None declared.
6. Zanotti KM. The clinical manifestations and diagnosis of Sertoli-Leydig cell tumors of the ovary. CME J Gynecol Oncol 2002;7:129-33.
7. Osborn RH, Yannone ME. Plasma androgens in the normal and androgenic female: A review. Obstet Gynecol Surv 1971;26:195-228.
8. Prunty FT. Hirsutism, virilism and apparent virilism and their gonadal relationship. II. J Endocrinol 1967;38:203-27.
9. de Oliveira Franzin CM, Kraft ML, Faundes D, Zeferino LC, Alvarenga M, Marussi EF. Detection of ovarian Sertoli-Leydig cell tumors exclusively by color Doppler sonography. J Ultrasound Med 2006;25:1327-30.
10. Nouriani M, Felix JC, Dubeau L. Histogenesis and histopathological characteristics of Sertoli-Leydig cell tumors. CME J Gynecol Oncol 2002;7:114-20.
11. Kriplani A, Agarwal N, Roy KK, Manchanda R, Singh MK. Laparoscopic management of Sertoli-Leydig cell tumors of the ovary. A report of two cases. J Reprod Med 2001;46:493-6.
12. Sood AK, Gershenson DM. Management of early-stage ovarian cancer. In: Bristow RE, Karlan BY, editors. Surgery for Ovarian Cancer Principles and Practice. London, UK: Taylor and Francis; 2005. p. 57-86.
[Downloaded free from http://www.sjmms.net on Wednesday, February 24, 2016, IP: 41.45.223.130]