Embed Size (px)
Citation preview
Seronegative Spondyloarthropathies and Connective Tissue Disease
Victor Politi, M.D., FACP
Medical Director, SVCMC, School of Allied Health, Physician Assistant Program
Connective tissue disease
• A connective tissue disease is any disease that has the connective tissues of the body as a primary target of pathology.
• Many connective tissue diseases feature abnormal immune system activity with inflammation in tissues as a result of an immune system that is directed against one's own body tissues (autoimmunity).
Connective tissue disease
• Diseases in which inflammation or weakness of collagen tends to occur are also referred to as collagen diseases.
• Collagen vascular disease is a somewhat antiquated term used to describe diseases of the connective tissues that typically include diseases which can be (but are not necessarily) associated with blood vessel abnormalities.
Heritable Connective Tissue Disorders
• Marfan Syndrome - a genetic disease causing abnormal fibrillin.
• Epidermolysis bullosa (EB). With these disorders, the skin blisters when it is stressed. For example, a hug could cause a blister.
• Ehlers-Danlos syndrome - causes progressive deterioration of collagens, with different EDS types affecting different sites in the body, such as joints, heart valves, organ walls, arterial walls
• Osteogenesis imperfecta (brittle bone disease) - caused by insufficient production of good quality collagen to produce healthy, strong bones.
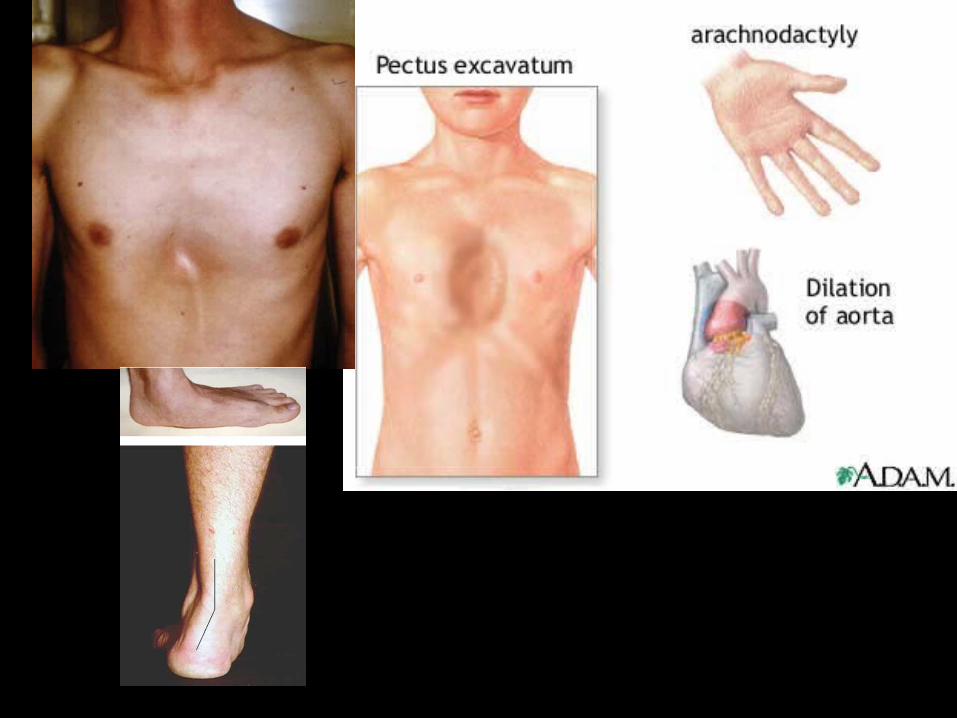
Marfan Syndrome
• A hereditary disorder of connective tissue characterized by tall stature, elongated extremities, subluxation of the lens, dilatation of the ascending aorta, and "pigeon breast." It is inherited as an autosomal dominant trait.
• Initial diagnosis is made on the basis of a careful examination of the three main affected areas; the heart, skeleton and eyes.
Marfan Syndrome
Ehlers-Danlos syndrome (EDS)
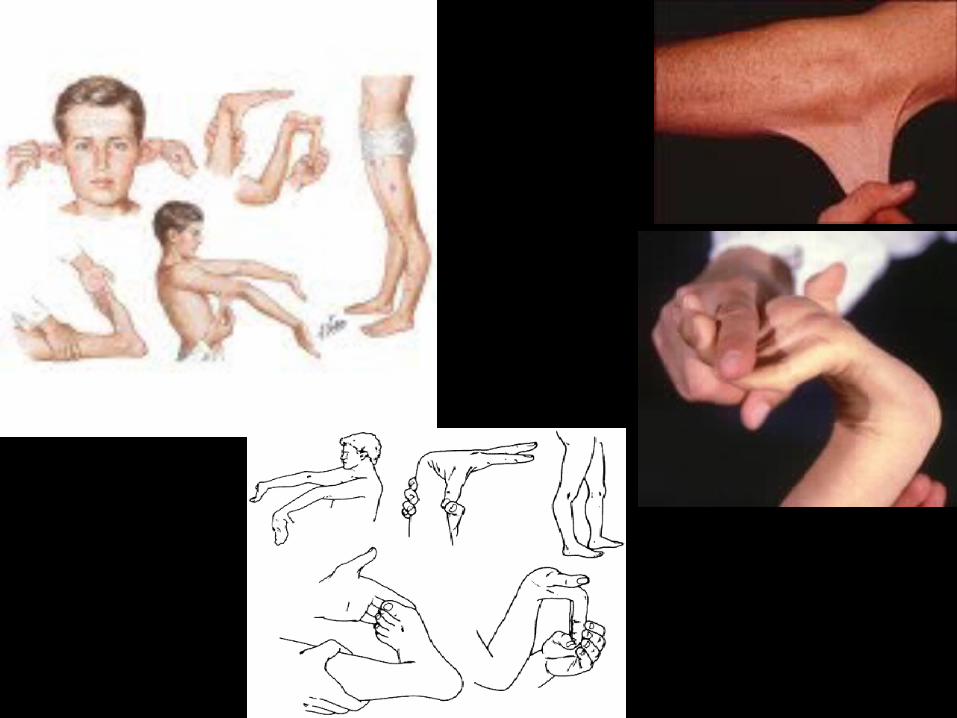
• Ehlers-Danlos syndrome (EDS) is a heterogeneous group of heritable connective tissue disorders characterized by articular hypermobility, skin extensibility and tissue fragility.
• At this time, research statistics of EDS show the prevalence as 1 in 5,000. It is known to affect both males and females of all racial and ethnic backgrounds.
Ehlers-Danlos syndrome (EDS)
• Clinical manifestations of EDS are most often joint and skin related and may include:– Joints: joint hypermobility; loose/unstable joints which
are prone to frequent dislocations and/or subluxations; joint pain; hyperextensible joints; early onset of osteoarthritis.
– Skin: soft velvet–like skin; variable skin hyper-extensibility; fragile skin that tears or bruises easily; severe scarring; slow and poor wound healing; development of molluscoid pseudo tumors .
SLE
• Inflammation of the connective tissues.• characterized by antinuclear antibodies and
multiorgan involvement.
• Peak incidence of systemic lupus erythematosus is in people aged 15-40 years, with a female-to-male ratio of at least 5:1.
• It is up to 9x more common in women than men.
SLE
• The criteria include malar rash, discoid rash, photosensitivity, oral ulcers, arthritis, serositis, renal disorder, neurologic disorder, hematologic disorder, immunologic disorder, and positive ANA.
Rheumatoid Arthritis
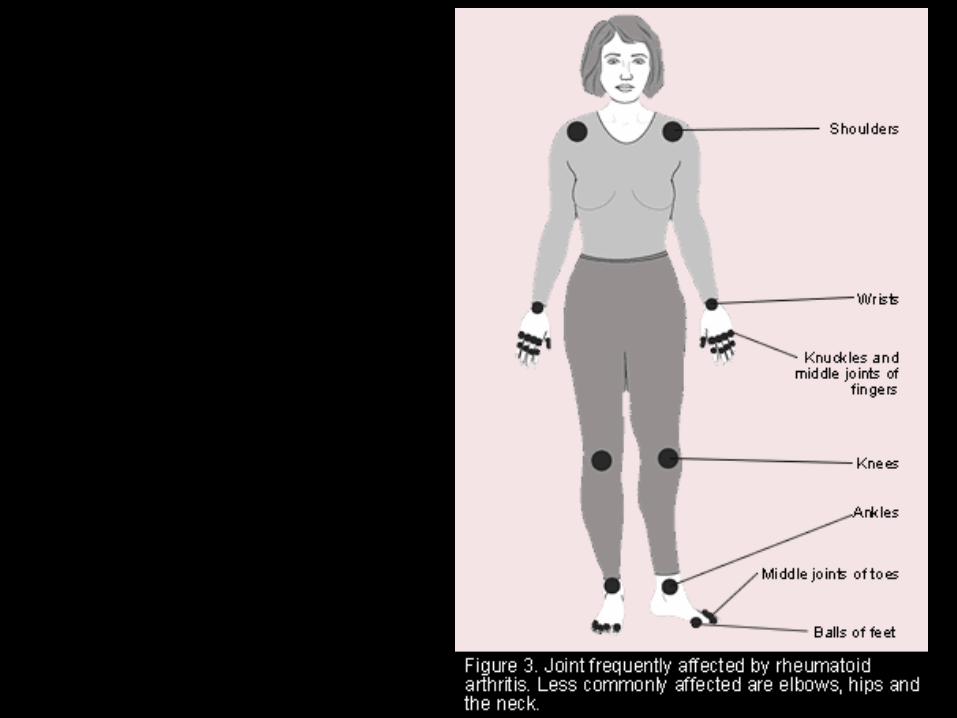
• Rheumatoid arthritis is a chronic inflammatory systemic disease primarily characterized by diarthrodial joint involvement.
• The prevalence of rheumatoid arthritis increases with age and has a peak incidence in persons aged 40-60 years, with a female-to-male ratio of 3:1.

RH
• The criteria include morning stiffness for at least 1 hour, arthritis of 3 or more joint areas, arthritis of the hands, symmetric arthritis, rheumatoid nodules, serum RF, and radiographic changes.
• RF is found in the serum of approximately 85% of patients with rheumatoid arthritis.
Rheumatoid Arthritis
Scleroderma
• Scleroderma is an activation of immune cells which produces scar tissue in the skin, internal organs, and small blood vessels.
• It affects women 3x more often than men overall, but increases to a rate 15 x > for women during childbearing years.
Sjögren's syndrome
• A chronic, slowly progressing inability to secrete saliva and tears.
• It can occur alone or with rheumatoid arthritis, scleroderma, or systemic lupus erythematosus.
• Nine out of 10 cases occur in women, most often at or around mid-life.
Sjögren’s syndrome
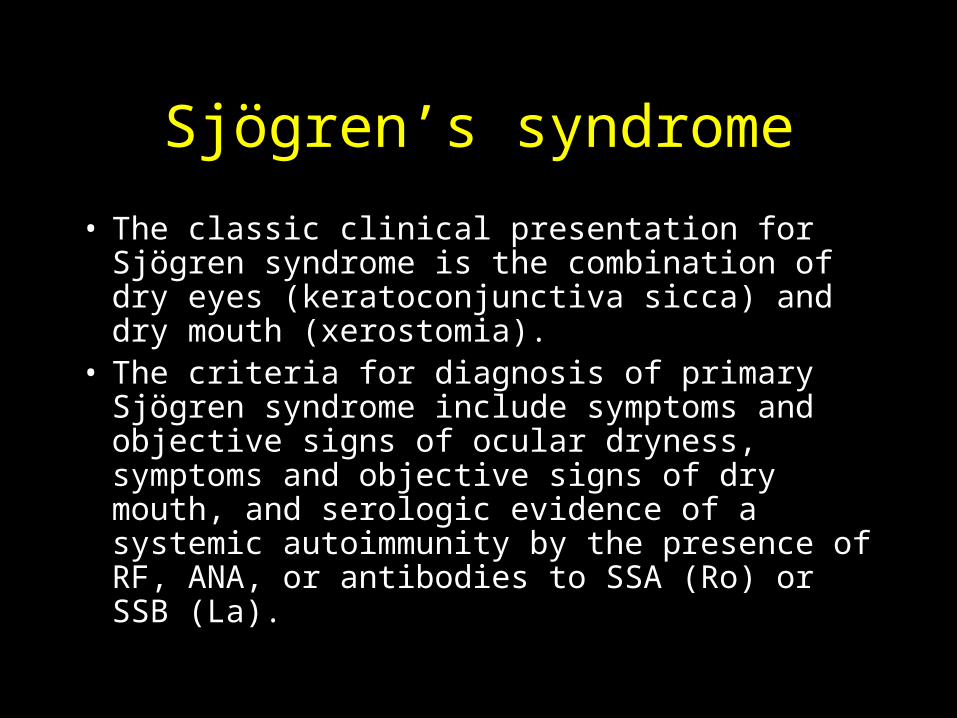
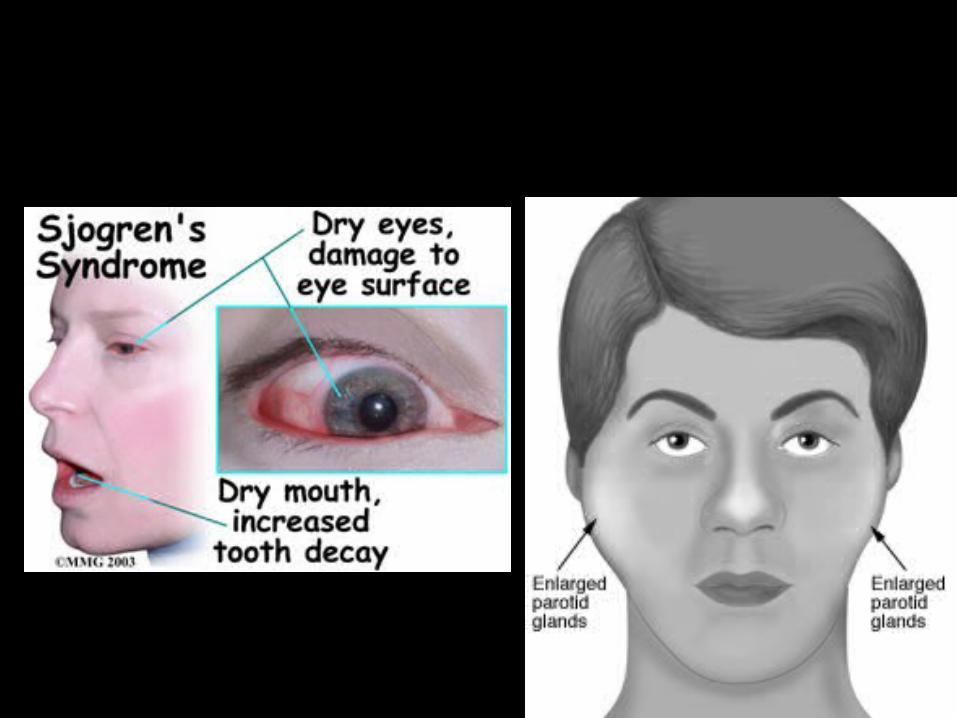
• The classic clinical presentation for Sjögren syndrome is the combination of dry eyes (keratoconjunctiva sicca) and dry mouth (xerostomia).
• The criteria for diagnosis of primary Sjögren syndrome include symptoms and objective signs of ocular dryness, symptoms and objective signs of dry mouth, and serologic evidence of a systemic autoimmunity by the presence of RF, ANA, or antibodies to SSA (Ro) or SSB (La).
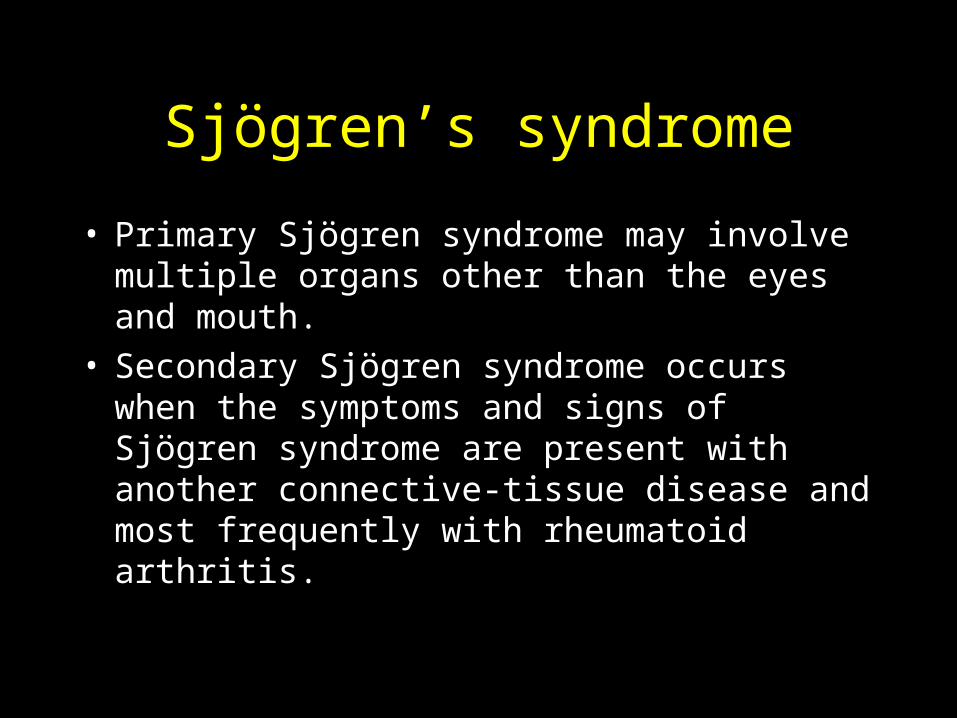
• Primary Sjögren syndrome may involve multiple organs other than the eyes and mouth.
• Secondary Sjögren syndrome occurs when the symptoms and signs of Sjögren syndrome are present with another connective-tissue disease and most frequently with rheumatoid arthritis.
Sjögren’s syndrome
Polymyositis/dermatomyositis
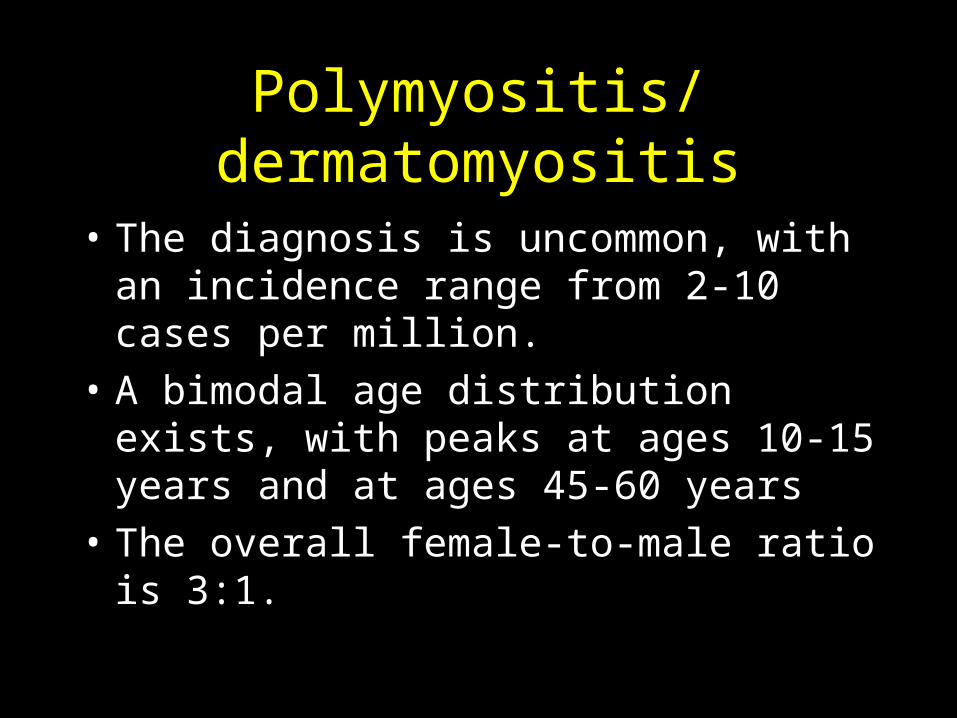
• The diagnosis is uncommon, with an incidence range from 2-10 cases per million.
• A bimodal age distribution exists, with peaks at ages 10-15 years and at ages 45-60 years
• The overall female-to-male ratio is 3:1.
• The 5 possible criteria for diagnosis are symmetrical weakness, elevation of muscle enzymes, electromyographic evidence, muscle biopsy evidence, and dermatologic features.
• A definite diagnosis of polymyositis must include 4 criteria without a rash.
• The diagnosis of dermatomyositis is made when 3 criteria are present plus the rash.
Polymyositis/dermatomyositis
Reactive Arthritis
• HLA-B27 positive (50-80% of cases)• Formerly called Reiter’s Syndrome• Tetrad of
urethritis,conjunctivitis/uveitis,mucocutaneous lesions (mouth ulcers) and aseptic arthritis (oligoarthritis)
• Most common in young men• Often follows infection
Reactive Arthritis
• Most cases develop days - weeks following dysenteric infection (shigella, salmonella, yersinia, Campylobacter) or sexually transmitted disease (chlamydia trachomatis or Ureaplasma urealyticum)
• To be distinguished from GC arthritis(migratory polyarthralgias) and non GC acute bacterial (septic) arthritis ie staph.
Reactive Arthritis
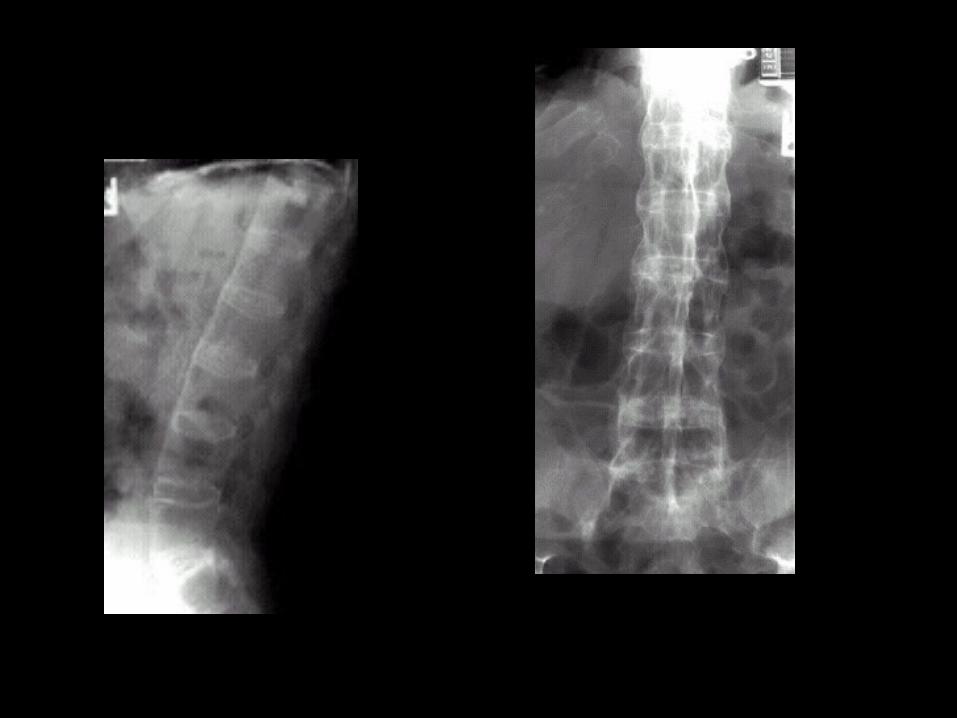
• Arthritis - usually asymmetric - involving large weight bearing joints (knees, ankle)– In 20% of cases - sacroiliitis or ankylosing
spondylitis present– systemic symptoms - fever & weight loss common
at initial stage of disease – Other symptoms -
• mucocutaneous lesions• carditis & aortic regurgitation may occur
Reactive Arthritis
• Most signs of the disease disappear within days to weeks – arthritis symptoms however may persist for
months or years– common for recurrences - can involve any
combination of clinical manifestations - can be followed by permanent sequelae (joints)
Reactive Arthritis- differential dx
• Gonococcal arthritis can mimic reactive arthritis– however, in gonococcal arthritis
• marked improvement 24-48 hrs after antibiotics
• culture results distinguish two disorders
• also must consider rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis
• no association between HIV and reactive arthritis
Reactive Arthritis - Tx
• NSAIDs
• tetracycline's
• sulfasalazine
• Anti-TNF agents (etanercept, infliximab)
Psoriatic Arthritis
• In 15-20% of psoriasis patients arthritis coexists
• There are several subsets of arthritis that may accompany psoriasis– joint disease resembles RA, polyarthritis -
symmetric, fewer joints involved than in RA– oligoarticular form - considerable destruction of
affected joints
Psoriatic Arthritis
– disease pattern where distal interphalangeal joints primarily affected ,pitting of nails, onycholysis frequent
– arthritis mutilans (severe deforming- with marked osteolysis) pencil in cup deformity
– spondylitic form (primary involvement - sacroiliitis, spinal involvement) 50% of cases HLA-B27 positive
Psoriatic Arthritis
• Psoriasis usually precedes arthritis in 80%– 20% of cases it occurs simultaneously– patient may have a single patch of psoriasis and
unaware of its connection to arthritis – psoriasis may not be present at time of exam
(important to obtain personal history)
Psoriatic Arthritis- Radiographic findings
– Help distinguish it from other forms of arthritis– marginal erosions of bone – irregular destruction of joint and bone– phalanx may appear - sharpened pencil– paravertebral ossification – fluffy periosteal new bone -
• @ insertion of muscles and ligaments into bone, shafts of metacarpals, metatarsals and phalanges
Psoriatic Arthritis- Treatment
• Symptomatic– NSAIDs– methotrexate– PUVA therapy for skin lesions
• Corticosteroids (less effective in psoriatic arthritis & may exacerbate psoriasis)
• antimalarials may also exacerbate psoriasis
Arthritis with GI symptoms
• 1/5 of patients with inflammatory bowel disease have arthritis
• 2/3 of patients with Whipple’s disease have arthralgia or arthritis (usually episodic/large joint polyarthritis) Arthritis usually precedes Whipple’s by years (fever,lymphadenopathy,arthralgias,malabsorption ,infection w/tropheryma whippelii.)
Arthritis with GI symptoms
• Two forms of arthritis are seen in Crohn’s disease and ulcerative colitis– peripheral arthritis (non deforming asymmetric
oligoarthritis of large joints)– spondylitis (indistinguishable by symptoms or
x-ray from ankylosing spondylitis)50% of cases are HLA-B27-positive
• In most cases arthritis improves with controlling intestinal inflammation.
Systemic Sclerosis
• Chronic disorder characterized by diffuse fibrosis/thickening of skin ,telangiectasia and pigmentation changes
• Cause unknown
• 3rd - 5th decade onset
• Women affected – 2 - 3 times more frequently than men
Systemic Sclerosis
• Two Forms– limited (80% of cases) CREST syndrome -
scleroderma limited to face and hands– diffuse (20% of cases) trunk and proximal
extremities also affected

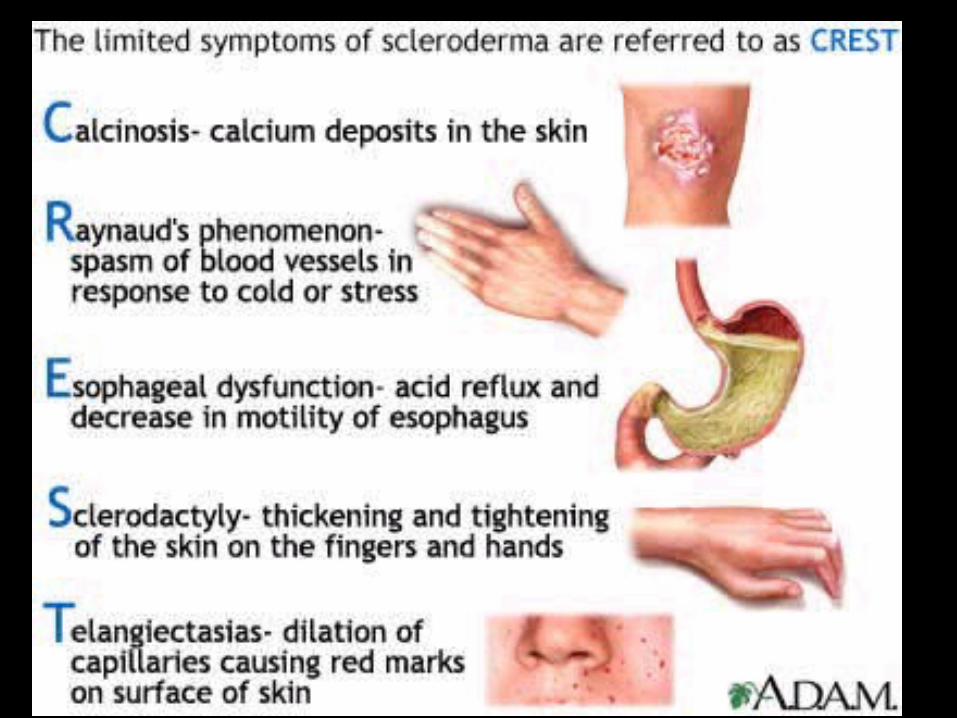
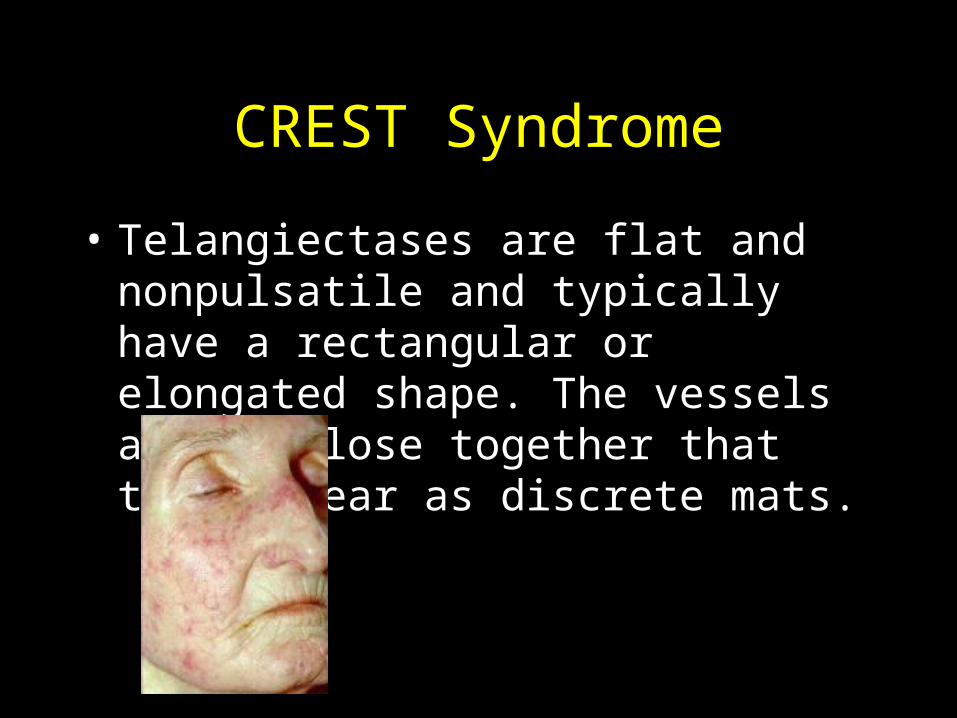
CREST Syndrome
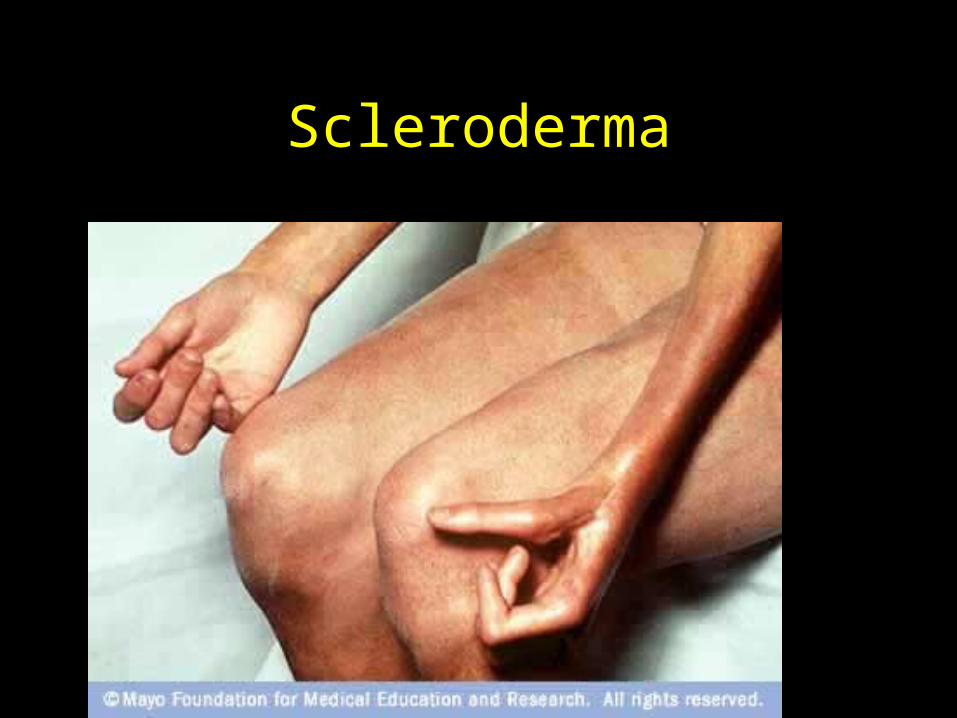
Scleroderma
CREST Syndrome
Calcinosis
In scleroderma, calcific deposits are found predominantly in the extremities, around joints, and around bony prominences.
Deposits typically are found in the flexor surfaces of the hands and the extensor surfaces of the forearms and knees.
The deposits rest in the dermis but can be found in deeper periarticular tissues.
CREST Syndrome
Raynaud phenomenon
Triphasic color changes of pallor, cyanosis, and erythema represent phases of vasoconstriction, slow blood flow, and reperfusion, respectively.
Color changes extend proximally from the tips of digits to various levels, with a well-demarcated border.
CREST Syndrome
Esophageal dysmotility
The earliest change in the distal esophagus (primarily smooth muscle) is an uncoordinated disorganized pattern of contractions resulting in low amplitude or absent peristalsis.
Lower esophageal sphincter (LES) pressure typically is lower than in healthy controls, and incomplete relaxation of the LES occurs, according to Sjögren.
CREST Syndrome
Sclerodactyly
The process typically begins in the distal fingers and advances proximally.
The process also may occur on the face, over the forehead, and around the mouth. Facial involvement can lead to a mauskopf (mouse head) appearance. Lips become thinner, and radial furrowing develops around the mouth. The oral aperture is reduced in size (microstomia). Wrinkles over the forehead diminish.
CREST Syndrome
• Telangiectases are flat and nonpulsatile and typically have a rectangular or elongated shape. The vessels are so close together that they appear as discrete mats.
Systemic Sclerosis- symptoms/signs
• Diffuse pulmonary fibrosis
• GI tract symptoms caused by fibrosis and atrophy– hypomotility– malabsorption from bacterial overgrowth– diverticular develop
Systemic Sclerosis- symptoms/signs
• Renal crisis (usually indicative of poor prognosis - though many cases treated successfully w/angiotensin-converting enzyme inhibitors)
• Cardiac symptoms– pericarditis– heart block– myocardial fibrosis– right heart failure secondary to pulmonary HTN
Systemic Sclerosis- Lab findings
• Mild anemia often present
• Antinuclear antibody tests - positive
• Scleroderma antibody (SCL-70) directed against topoisomerase III – 1/3 of patients w/diffuse systemic sclerosis– 20% of patients w/CREST syndrome
(anticentromere ab seen in 50% crest but 1% of syst. Scler.
Systemic Sclerosis - Treatment
• Symptomatic and supportive
• Intervention for management of specific organ manifestations (ie., Raynaud's syndrome - calcium channel blockers, esophageal disease - H2 blockers, etc.)
Questions ??











![Remitting seronegative symmetrical synovitis with … · Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) is a rare rheumatologic ... [7]. However, cases of](https://img.pdfslide.us/doc/110x75/5adb86477f8b9a4a268b69df/remitting-seronegative-symmetrical-synovitis-with-seronegative-symmetrical-synovitis.jpg)