Embed Size (px)
Citation preview

3/7/2016
1
Serologic Weak D Phenotype
to RHD Genotyping:
How will I know?
Sue Johnson, MSTM, MT(ASCP)SBB
Director, Clinical Education
BloodCenter of Wisconsin
Immucor User’s Group Meeting
San Ramon, CA
March 8, 2016
How will I know?
Objectives
• Identify at least 3 different causes for
variability of expression of the RhD antigen
• List the challenges of typing for RhD by
serologic methods
• Define the management of pregnant
women and transfusion options for patients
who present with weak or variable RhD
typing
How will I know?
Objectives
• Discuss the recent recommendations of the
Inter-organizational Work Group on RHD
genotyping for managing pregnant women
and transfusion recipients who have a
serologic weak D phenotype.

3/7/2016
2
CONTRIBUTORS
OF VARIABILITY
VARIABLES
RHD Gene Weak D C in Trans
to RHD
Partial D DEL
D epitopes on
RhCE Protein
ceCF ceHAR
Anti-D Reagents Polyspecific
Slide and
Modified Tube
Human IgG
Monoclonal
IgG
Monoclonal
IgM
Monoclonal
IgM
Human IgG
Monoclonal
Blends
Testing Platform Test Tubes
IS & IAT
Column
Agglutination
Solid Phase Liquid
Microtiter
Individual being
Rh Typed
Transfusion
Recipient
Obstetrical
Patient
Cord Blood Donor Blood
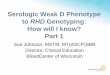
Variables Impacting Rh Typing
Transfusion Technology Report Vol. #013 Immucor, Inc.
2 3 4 9 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 10
Locus 1 Locus 2
RH Genes – Rh Positive
RHD
RHCE
Chromosome 1
Locus 1 - presence of RHD
codes for the presence of D or
no D.
Locus 2 - presence of RHCE
codes for Ce, CE, cE, ce.
RhD Protein
COOH
417 NH2
53 107 167 230
321
358
391
Vestibule
282
•Crosses RBC membrane 12 times
•No sugars attached
http://www.jic.ac.uk/corporate/about/publications/advances/images_10/protein.jpg
231 347

3/7/2016
3
11 72
32 53 94 107 158 167 230 231 282 290 347 358
75 131 135 186 201 263 266 321 324 391
417
RhD differs from RhCE by 34 to 37 amino acids =
E= C=
RhD vs. RhCE Protein
Adapted from Flegel, Curr Opin in Hemat 2006, 13:476–483
RhD Negative
• Deletion of RHD
• Inactivating mutations of RHD
• RHD in African Americans
• Hybrid RHD-CE-D in African backgrounds
9 1 2 3 4 5 6 7 8 10
9 1 2 3 4 5 6 7 8 10
9 1 2 3 4 5 6 7 8 10
Gene Conversion
• Portions of RHCE into RHD
1
2
3
4
6
5
7
9
8
10
5’
3’ 1
0
9
8
7
5
6
4
2
3
1 5
’ 3
’
6
5
4
7

3/7/2016
4
Gene Conversion
• Portions of RHD into RHCE
1
2
3
4
6
5
7
9
8
10
5’
3’ 1
0
9
8
7
5
6
4
2
3
1 5
’ 3
’
6
5
4
7
4
Missense, Nonsense, Frameshift
& Splice Site Mutations
1 2 3 4 6 5 7 9 8 10
5’ 3’
10 9 8 7 5 6 4 2 3 1
5’ 3’
G>C
C>G
RHD
RHCE
Missense – amino acid change
Nonsense or Frameshift – prevent expression
Splice site – no or reduced expression
RH Gene Diversity
• RHD: > 200 alleles
• Weak D “Types”
• Partial D
• DEL

3/7/2016
5
Serologic Weak D Phenotype
Definition
• Anti-D reagent giving no or weak
(≤2+) reactivity in initial testing, but
agglutinating moderately or strongly
with antihuman globulin
Identified by weak reactivity or
by discordant typing results
Sandler SG, et al Transfusion 2015 Mar;55(3):680-9
Weakened Expression of D
2 Categories
• Not at risk of making anti-D
• At risk of making anti-D
WEAK D
Not at Risk of Making Anti-D

3/7/2016
6
Weak Expression of D Not at Risk of Making Anti-D
• C in trans with RHD
(Ceppellini effect)
• r’ haplotype (R1r’ – DCe/Ce)
• Weak D “Types”: amino acid change(s),
usually a single change
• Types 1, 2, 3
Weak D Types
Most Not At Risk of Making Anti-D
• Changes in regions of RHD predicted to be
in the RBC membrane or inside RBC
• Less Rh protein in RBC membrane
• Can type as Rh-positive or Rh-negative by
direct agglutination with monoclonal (IgM)
anti-D reagents
IS D IAT Ct. IAT
Anti-D 0 3 0
IS
Anti-D w+ - 2+ or
11 72
32 53 94 107 158 167 230 231 282 290 347 358
75 131 135 186 201 263 266 321 324 391
417
Type 2
Gly(385)Ala
Type 1 Val(270)Gly
Account for 80-90% of Weak D
Not at risk of making Anti-D
Type 3 Ser(3)Cys
Adapted from Flegel, Curr Opin in Hemat 2006, 13:476–483

3/7/2016
7
Normal RhD Positive
Normal Rh Protein
Normal RhD antigen
~ Antigens/RBC*
DCe/ce 9900-14,600
DcE/ce 12,000-19,700
DCe/DCe 14,500–22,800
*Daniels G. Human Blood Groups
Weak D Type 1- 81
Fewer Copies of Rh Protein
Normal RhD antigen
~ Antigens/RBC*
Type 1 759
Type 2 491
Type 3 1948
*Wagner, et al. Blood 2000;95:2699-2708
WEAK EXPRESSION OF D
At Risk of Making Anti-D

3/7/2016
8
Weak Expression of D
At Risk of Making Anti-D
• Partial Ds: hybrid RHD alleles
• DVI
• DIIIa
• Others
• DEL: detected by adsorption/elution
• D epitopes on RHCE gene
Partial D
• Lack exofacial epitopes or have
altered exofacial epitopes
• Hybrid proteins
• Missense mutations affecting
exofacial protein
Partial D
Missing RhD Epitopes
Normal RhD antigen

3/7/2016
9
Partial D
Altered RhD Epitopes
Normal RhD antigen
D Epitope on RHCE Genes
• ceHAR - formally known as R0Har or DHAR
• ceCF (ceRT, ceSL) - Crawford phenotype
1 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 10
Locus 1 Locus 2
Exons
No D antigens ce antigens
RHCE
ceHAR results from one RHD exon inserted into the RHCE gene.
D Epitope on RHCE Gene - ceHAR
IS
Anti-D 3+

3/7/2016
10
ceHAR Phenotype: Reactivity with Reagent Anti-D
Anti-D RBCs
Reagent IgM IgG ceHAR
Gamma-Clone GAMA401 F8D8 Pos*
Immucor-4 MS201 MS26 Pos*
Immucor-5 TH28 MS26 Pos*
Ortho Bioclone MAD2 Human
polyclonal
Neg
Ortho (ID-MTS) MS201 Pos
Biotest (Bio-Rad) BS232 BS221
H41 11B7
Pos
Quotient - Alpha LDM1 Pos
Quotient - Delta LDM1 ESD1M Pos
*Positive reactions often weaker at IAT
AABB Tech Manual, 18th ed. 2014
1 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 10
Locus 1 Locus 2
Exons
No D antigens ce antigens
RHCE
ceCF results from 3 nucleotide changes,
48G>C, 697C>G, 733C>G in RHce
gene.
D Epitope on RHce Gene - ceCF
GammaClone
IS
Anti-D 3+
Anti-D Reagents: Reactions with Crawford Phenotype RBCs
Anti-D RBCs
Reagent IgM IgG Crawford
IS/IAT
GammaClone GAMA401 F8D8 Pos/Neg
Immucor-4 MS201 MS26 Neg/Neg
Immucor-5 TH28 MS26 Neg/Neg
Ortho Bioclone MAD2 Human
polyclonal
Neg/Neg
Ortho (ID-MTS) MS201 Neg/Neg
Biotest (Bio-Rad) BS232 BS221
H41 11B7
Neg/Neg
Quotient - Alpha LDM1 Neg/Neg
Quotient - Delta LDM1 ESD1M Neg/Neg
AABB Tech Manual, 18th ed. 2014

3/7/2016
11
Anti-D
Reagents & Methods
Monoclonal Reagent Types
• Blend of monoclonal & polyclonal antibodies
• Blend of two or more monoclonal antibodies,
each secreted by a different cell line
• IgG or IgM, or combination of IgG + IgM
• Why?
• D antigen has >30 different epitopes
• Variant D antigens
FDA Approved Reagent Anti-D - Tubes
Anti-D
Reagent IgM IgG
Gamma-Clone GAMA401 F8D8
Immucor-4 MS201 MS26
Immucor-5 TH28 MS26
Ortho Bioclone Tube MAD2 Human polyclonal
Bio-Rad Seraclone - Blend BS232 BS221
H41 11B7
Bio-Rad Seraclone - 226 BS226
Quotient (Alba) – Alpha LDM1
Quotient (Alba) – Beta LDM3
Quotient (Alba) – Delta* LDM1
ESD1-M
Quotient (Alba) – Blend LDM3 EDS1
*Not for patient testing, detects DVI at IS

3/7/2016
12
FDA Approved Reagent Anti-D - Other Methods
Anti-D
Anti-D Method IgM IgG
Immucor – Series 4 Galileo Echo®/Neo® MS201 MS26
Immucor– Series 5 Galileo Echo®/Neo® TH28 MS26
Ortho Gel/Provue® MS201
PK1 PK7200®/PK7300® P3X61
PK2 PK7200®/PK7300® HM10
Blend PK7200®/PK7300® P3X61
P3X21223B10
P3X290
P3X35
Bio-Rad 226 Tango® BS226
Bio-Rad 232 Tango® BS232
Solidscreen II Blend
(weak D testing)
Tango® H411B7
BS221
Grifols DG Gel/Erytra® P3x61
Specificity of Anti-D CFR 660.26
• Panel of antigen positive RBCs must be
tested and include at least 3 donors of
each phenotype:
• DCe/ce, Dce/ce
• dCe/ce, dce/cE
• Group A, B and O dce/dce
• Most include testing with DVI
Sensitivity of Anti-D
• Reagent Anti-D compared to Reference
Blood Grouping Sera (FDA) for potency
• Monoclonal Anti-D WILL NOT detect all
weak D and partial D
• Weak D Test (IAT/AHG) enhances
reactivity with most examples of weak
D and partial D

3/7/2016
13
Monoclonal IgM/IgG ANTI-D
Monoclonal IgM/IgG ANTI-D #1
Direct Agglutination - IS
Method Variability
• Test Tube Methods
• Reagents used
• Technologist-dependent
• Weak D IAT/AHG or not…
• Other Methods
• Liquid microtiter
• Column Agglutination

3/7/2016
14
Direct Agglutination in Test Tubes
Reading Direct Agglutination
ABO vs. RhD Reagents
Anti-A / Anti-B Anti-D
Antibody Class IgM IgM or
IgM & IgG
Antigen Structure
Carbohydrate
Integral Membrane
Protein
Antigen Sites/RBC ~2 – 10 x 105
~ 9,900 – 33,000
Reading Direct Agglutination
Shake, Rock, Roll, Swirl, Tilt, or some combination… Grade as soon as
RBC button is
resuspended

3/7/2016
15
Microplate ABO/Rh Typing
Fluid Phase – Hemagglutination by Settling
www.beckmancoulter.eu/diagnostics/3108_PK7300.htm
PK7300
Settling Method
Neg Pos
Microplate ABO/Rh Typing Fluid Phase – Hemagglutination
Galileo Echo® & NEO ®
Microtiter Plate ABO/Rh Typing
Hemagglutination Method
Monoclonal Control
Anti-A
Anti-B
Anti-D Series 4
Anti-D Series 5
A1 Cells
B Cells

3/7/2016
16
Microplate ABO/Rh Typing Hemagglutination by Aggitation
Column Agglutination Hemagglutination Methods
http://www.grifols.com
www.ortho-wire.com/en/blood-group-serology/learning-library/AgAb/page5.cfm
Questionable RhD Typing Results
Using Automation
Microplate
Anti-D ? Or NTD
Discordant with historical typing
Gel
Anti-D ? or <2+
or

3/7/2016
17
RhD Typing Results
Test Tube Method
Tube IS IAT
Anti-D 0-2+ 2-4+
Consider RHD genotyping
Tube IS
Anti-D 3-4+
or
Serologic Weak D Phenotype
Commentary
It’s time to phase-in RHD genotyping
for patients with a serologic
weak D phenotype
Sandler SG, Flegel WA, Westhoff CM, Denomme GA,
Delaney M, Keller MA, Johnson ST, Louis Katz,
Queenan JT, Vassallo RR, Simon CD
Transfusion 2015 Mar;55(3):680-9
http://www.aabb.org/advocacy/statements/Pages/statement150722.aspx

3/7/2016
18
Recommendation of the Work Group
• “RHD genotyping is recommended
whenever a weak D phenotype is
detected by routine Rh blood typing of
pregnant women and other females of
childbearing potential.”
• Strong Recommendation: based on
high-quality evidence from
observational studies (1A)
Additional Notes
• New CPT code 81403
for RHD genotyping (Tier 2 Molecular
pathology procedure, Level 4)
• Reimbursement rates for the Tier 2 code
are being established
• updating its Practice Bulletin!!
p. 360
“Testing for “weak D”, formerly
“Du” antigen is being
recommended in a new
approach due to new
genotyping capabilities and
information. …They can be
genotyped and if their genotype
is type 1, 2 or 3, they may be
managed as RhD-positive…”

3/7/2016
19
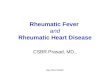
Sandler SG, et al. Commentary – Transfusion March 2015)
Low Resolution
High Resolution
Serologic Weak D Phenotype Detected
Molecular Testing
Appropriate for
Phenotype
Molecular Testing
includes weak D type
and partial D assays
Molecular Testing
explains phenotype Yes No
Sequencing
Result Reported
Adapted from Wagner, F. Perspectives in
Transfusion Medicine, Issue 5, Grifols, 2015.
57 All Content © 2015 Immucor, Inc.
RHD BeadChip
Exon
Amino Acid
change/Mar
ker
Nucleotide
Change
Exon
Amino Acid
change/Mark
er
Nucleotide
Change
1
S3C 8 C>G
5
E233K 697 G>A
W16C 48 G>C V238M 712 G>A
W16X 48 G>A V245L 733 G>C
2
L62F 186 G>T G263R 787 G>A
R70Q 209 G>A
6
V270G 809 T>G
3
R114W 340 C>T V279M 835 G >A
A137V 410 C>T G282D 845 G > A
A149D 446 C>A T283I 848 C>T
N152T 455 A>C M295I 885 G>T
IVS3+1G/A In3+1G>A
7
I342T 1025 T>C
4 psi D
In3 -19 37 bp
duplication D350H 1048 G > C
M170T 509 T>C G353W 1057 G>T
I172F 514 A>T G355S 1063 G>A
T201R 602 C>G
9
G385A 1154 G>C
5
F223V 667 T>G E398V 1193 A>T
A226P 676 G>C 1227G/A 1227 G>A
S230I 689 G>T
E233Q 697 G>C

3/7/2016
20
58 All Content © 2015 Immucor, Inc.
RHD BeadChip High-throughput Genotyping Platform
DNA Sequencing
• Gold standard for mutation detection
• Determines precise order of nucleotides
• Any method or technology used to
determine order of the four bases—
adenine, guanine, cytosine, and thymine—in
DNA strand
• Next Generation sequencers simplify
sequencing of genomes (introns & exons)
• Analyze many genes at one time
ex1
(148
bp)
ex2 (187 bp) ex3
(151 bp)
ex4
(148 bp)
ex5
(167 bp)
48 1
5
0
1
7
8
1
8
6
2
0
1
2
0
3
2
5
1
3
0
7
3
2
5
3
2
9
3
3
0
3
6
1
3
8
0
3
8
3
4
1
0
4
5
5
5
0
5
5
0
9
5
1
4
5
3
9
5
4
4
5
6
0
5
7
7
5
9
4
6
0
2
6
3
6
6
6
7
6
7
4
6
7
6
6
9
7
7
1
2
7
3
3
7
4
4
7
8
7
8
0
0
8
0
7
8
1
9
G T A G G G T T A T G T T A C A A T A G T T G A C C
(A)
T C G G G G C G A T G
ex6
(138
bp)
ex7 (134 bp) ex8
(80 bp)
ex9
(70 bp)
ex10
(24
bp)
3'UT
R
9
1
6
9
3
2
9
4
1
9
5
7
9
6
7
9
7
4
9
7
9
9
8
5
9
8
6
9
8
9
9
9
2
9
9
8
1
0
0
6
1
0
2
5
1
0
4
8
1
0
5
3
1
0
5
7
1
0
5
9
1
0
6
0
1
0
6
1
1
0
6
3
1
1
3
2
1
1
3
6
1
1
7
0
1
1
7
7
1
1
9
3
1
2
5
0
1
2
7
3
G A G G C G A G G A A G G T G C G A G C G C C T T A T G
RHD Reference Sequence
http://www.ncbi.nlm.nih.gov/projects/gv/mhc/xslcgi.cgi?cmd=bgmut/systems_info&system=rh

3/7/2016
21
Reasons to Resolve Weak Expression
Pregnancy
• Avoid giving RhIG to women who do not
need it (Rh status is confirmed for
historical discrepancies)
• Resolve early in pregnancy to eliminate
false-positive rosette tests
Negative Control Positive Control Weak D+ Mom
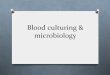
Unnecessary RhIG Injections in USA
3,953,000 Live Births
3,812,000 Pregnancies
556,500 RhD-negative
16,700 Serologic Weak D
13,360 weak D types 1,
2, or 3
RHD Genotype
24,700
Unnecessary
ante- & postpartum
RhIG
Sandler SG, et al Transfusion 2015 Mar;55(3):680-9
Unnecessary RhD-Negative
Transfusions in USA
5,000,000 Individuals Transfused Annually
730,000 RhD-negative
21,900 Serologic Weak D
17,520 weak D types 1, 2,
or 3
RHD Genotype
Could receive
RhD-positive units
(47,700)
Sandler SG, et al Transfusion 2015 Mar;55(3):680-9

3/7/2016
22
Case 1
• 57 y/o female
• Diagnosis – dehydration,
hypotension, anemia
• Patient is RhD positive with anti-D
Referred for Partial D Analysis
Case 1 - IRL Results
Test Tube Method
IS IAT
Anti-D – S-clone 0 4+
Anti-D – Series 5 0 3+
Anti-D – Gamma-Clone 0 4+
Anti-D – B-clone 0 4+
Rh Control 0 0
RHD Genotype - Weak D Type 4.2 (DAR)
Case 1
Summary
• Weak D Type 4.2 (DAR)
• Partial D
• At risk of making Anti-D (did!)
• A candidate for RhIg (not anymore)
• Treat as Rh negative for transfusion

3/7/2016
23
Case 2
• 25 y/o female
• Prenatal Visit
• RhD Discrepancy observed
Referred for RhD Discrepancy Analysis
Case 2 - IRL Results
Test Tube Method
IS IAT
Anti-D – S-clone 0 3+
Anti-D – Series 5 0 2+
Anti-D – Gamma-Clone 0 2+
Anti-D – B-clone 0 3+
Rh Control 0 0
RHD Genotype - Weak D Type 1
Case 2
Summary
• Weak D Type 1
• RhD Positive
• Not at risk of forming Anti-D
• Not a candidate for RhIg
• Treat as Rh positive for transfusion

3/7/2016
24
Impossible to Know with Serology!
All negative at IS
Case 1
Weak D
Type 4.2
Case 2
Weak D
Type 1
IAT IAT
Anti-D – S-clone 4+ 3+
Anti-D – Series 5 3+ 2+
Anti-D – Gamma-Clone 4+ 2+
Anti-D – B-clone 4+ 3+
Rh Control 0 0
How will I know?
Objectives
• Identify at least 3 different causes for
variability of expression of the RhD antigen
• List the challenges of typing for RhD by
serologic methods
• Define the management of pregnant
women and transfusion options for patients
who present with weak or variable RhD
typing
How will I know?
Objectives
• Discuss the recent recommendations of the
Inter-organizational Work Group on RHD
genotyping for managing pregnant women
and transfusion recipients who have a
serologic weak D phenotype.

3/7/2016
25
References • Wagner FF, Gassner C, Mu¨ller TH, et al. Molecular basis of weak D
phenotypes. Blood 1999; 93:385–393.
• Wagner FF, Frohmajer A, Ladewig B, Eicher NI, Lonicer CB, Mu¨ller TH,
Siegel MH, Flegel WA. Blood 2000;95:2699-2708.
• Denomme GA, Wagner FF, Fernandes BJ, et al. Partial D, weak D types,
and novel RHD alleles among 33 864 multiethnic patients: implications for
anti-D alloimmunization and prevention. Transfusion 2005; 45:1554–1560.
• Flegel WA, Denomme GA, Yazer MH. On the complexity of D antigen
typing: a handy decision tree in the age of molecular blood group
diagnostics. J Obstet Gynaecol Can. 2007;29:746-52.
• Flegel WA. How I manage donors and patients with a weak D phenotype.
Curr Opin Hematol 2006;13:476–483.
• Denomme GA, Dake LR, Vilensky D, Ramyar L, Judd WJ. Rh
discrepancies caused by variable reactivity of partial and weak D types with
different serologic techniques.Transfusion 2008;48:473-476.
• Roback JD, Grossman BJ, Harris T, Hillyer CD. Technical Manual, 18 th ed.
2014.
• Sandler SG, Flegel WA, Westhoff CM, Denomme GA, Delaney M, Keller
MA, Johnson ST, Louis Katz, Queenan JT, Vassallo RR, Simon CD,
Transfusion. 2015 Mar;55(3):680-9.
References • Flegel WA. Molecular genetics and clinical applications for RH.
Transfusion and Apheresis Science 2011;44:81-91.
• Sandler SG, Li W, Langeberg AL, Landy HJ. New Laboratory
Procedures and Rh Blood Type Changes in a Pregnant Woman. Obstet
Gynecol 2012;119:426–8.
• Wang D, Lane C, Quillen K. Prevalence of RhD variants, confirmed by
molecular genotyping, in a multiethnic prenatal population. Am J Clin
Pathol 2010;134:438-442
• Credidio DC, Pellegrino J, Castilho L, Serologic and molecular
characterization of D variants in Brazilians: impact for typing and
transfusion strategy. Immunohematology 2011;27:6-11.
• Abelrazik AM, Elshafie SM, Ahmed GME, Abdelaziz HM. Combining
serology and molecular typing of weak D role in improving D typing
strategy in Egypt. Transfusion. 2013 Nov;53(11 Suppl 2):2940-4
• Chou ST, Jackson T, Vege S, Smith-Whitley K, Friedman DF, Westhoff
CM. High prevalence of red blood cell alloimmunization in sickle cell
disease despite transfusion from Rh-matched minority donors. Blood.
2013 Aug 8;122(6):1062-71.
References
• Reid ME, Hipsky CH, Hue-Roye, K, Hoppe C. Genomic analysis of RH
alleles to improve transfusion therapy in patients with sickle cell
disease. Blood Cells Mol Dis. 2014 Apr;52(4):195-202
• Garratty G, Glynn SA, McEntire for the Retrovirology Epidemiology
Donor Study. ABO and Rh(D) phenotype frequencies of different
racial/ethnic groups in the United States. Transfusion 2004;44:703-6.
• Haspel RH, Westhoff CM. How do I manage Rh typing in obstetrical
patients. Transfusion 2015;55;470–474.
• Cannon M, Pierce R, Taber EB, Schucker J. Fatal hydrops fetalis
caused by anti-D in a mother with partial D. Obstet Gynecol. 2003
Nov;102(5 Pt 2):1143-5.
• Lacey PA, Caskey CR, Werner DJ, Moulds JJ. Fatal hemolytic disease
of a newborn due to anti-D in an Rh-positive Du variant mother.
Transfusion. 1983 Mar-Apr;23(2):91-4.