Embed Size (px)
Citation preview
Serious Case Review ‘Joe’
CN14 June 2016
CN14
BABY JOE
Report author:
Karen Tudor April 2016
SERIOUS CASE
REVIEW
Serious Case Review, Baby Joe, Fourth Draft
CONTENTS
Page Number
INTRODUCTION Background to this Serious Case Review Management Review Independent Verification – review period and method
2 2 2 3
FINDINGS AND LEARNING 3 FAMILY BACKGROUND Summary of Family History Family Involvement in the Review
4 4 5
BABY JOE’S EXPERIENCE 6 KEY EVENTS 7 ANALYSIS PRE-BIRTH PERIOD Identification of Vulnerability What did happen and why? Recognition of the Risks of Domestic Abuse What has happened since 2014
8 8 10 10 11
ANALYSIS POST BIRTH PERIOD Referral to Children’s Social Care Children’s Social Care Assessment Police Involvement with the Family and the Relevance of the MARAC Conclusion of the Assessment Reasons for the poor quality Assessment Child in Need Plan April 2014 – May 2014 Action on Health Presentations Examples of Poor Information Sharing
12 12 12 13 15 16 17 18 18 20
SUMMARY 22
LEARNING POINTS 23
CONSIDERATIONS FOR THE DSCB 25
GLOSSARY AND APPENDIX 26
Serious Case Review, Baby Joe, Fourth Draft
INTRODUCTION
1. This Serious Case Review (SCR) concerns a five month old baby who, in May 2015, was taken to the local Minor Injuries Unit (MIU) by his parents with a painful leg. The baby was found to have a fractured tibia (lower leg) and further examination revealed healing fractures in his arm and another in the lower leg. The fractures were considered to be highly indicative of inflicted or non-accidental injury and child protection enquiries were initiated. The baby was discharged from hospital and placed with foster carers. He has since made a full physical recovery.
Background to this Serious Case Review
2. When abuse or neglect of a child is known or suspected and either the child has died or the child has been seriously harmed and there is cause for concern as to the way in which services have worked together to safeguard the child, the Local Safeguarding Children Board (LSCB) has to consider whether a Serious Case Review should be carried out.
3. Part of the role of the Serious Case Review Sub Group is to consider whether the case
meets the criteria for a Serious Case Review. In this case, although the baby had suffered harm he was expected to make a complete recovery and therefore the sub group concluded that the threshold for a SCR had not been reached. Acknowledging that there were some multi agency issues in this case and in other recent cases involving very young babies, the sub group considered that a Management Review1 would be the best way to identify any learning from the case which would help make the safeguarding systems safer.
Management Review 4. The Management Review was conducted using root cause analysis methodology, a time
frame for the case was agreed and terms of reference drawn up. A detailed chronology was prepared and a meeting held with the practitioners involved with the case to look at the actions and decisions made and also to discuss some of the organisational factors impacting on the work.
5. A comprehensive report was written by the lead reviewer, the report looked at the
history of the case, the key practice episodes and analysed the practice; it commented on what happened and why and identified learning. A number of recommendations were made.
1 A Management Review can take place if the case does not meet the threshold for a Serious Case Review, the
findings of a Management Review are shared with the agencies involved with the family but are not made public.
Serious Case Review, Baby Joe, Fourth Draft
Response of the National Panel of Independent Experts on Serious Case Reviews
6. The management review was submitted to the National Panel who indicated that they were satisfied that “the review contained all the information they would expect to see in a SCR” and asked that the review be “independently verified and published as a SCR”
From letter to the Chair of the Safeguarding Board, December 2015
Independent Verification – review period and method
7. The SCR sub group, which oversees the process, agreed the time scale for the review would be the same as the management review, 13 months from when the baby’s mother was known to be pregnant until the date the baby was found to have the injuries.
8. An Independent Reviewer was appointed and agreement was reached between the
Reviewer and the Serious Case Review Group about how the management review would be independently verified.
It was agreed the Independent Reviewer would:
Read the completed Management Review
Have access to all the documents used in the Management Review including the chronology and notes of the meeting with practitioners
Meet with the author of the Management Review in order to discuss and constructively challenge the findings
Meet with the managers who were involved with the case (the practitioners had already been seen as part of the management review)
Invite members of the family to meet with the Independent Reviewer
Write a Serious Case Review suitable for publication
FINDINGS AND LEARNING 9. The SCR Group collated the chronologies prepared by the agencies who had worked
with the family and identified seven themes for exploration and learning. The themes were devised to look at both general practice and the issues thought to arise from the case, they were:
(a) The effectiveness of multi-agency identification, analysis and
management of the risk of physical abuse and why the risk was managed
in that way.
(b) The effectiveness of multi-agency information sharing arrangements and
any identified ‘system’ barriers to achieving effective identification and
management of risk.
Serious Case Review, Baby Joe, Fourth Draft
(c) The quality of risk assessments and validity of any tools or processes used
to identify protective factors as well as risk factors.
(d) The quality and impact of multi-agency planning, decision and review
processes used to promote improved outcomes for children
(e) Knowledge and application of the pre-birth planning process in
contributing to management of risk of abuse
(f) The application of ‘thresholds’ and the degree of shared understanding
and agreement across the partnership of those thresholds
(g) The degree to which multi-agency practice in the field of risk and harm to
children under 1 years of age is informed by evidence and research
10. The management review included a meeting of the practitioners who knew and had worked with the family to discuss what had happened in this case and why. In addition to the actions of individual workers, organisational factors which might have impacted on the work and decisions taken were explored and these are reflected in the findings.
A glossary of terms is appended to explain the terminology
FAMILY BACKGROUND
11. In order to protect the privacy of the family the baby is known as Joe and his parents as Ms J and Mr J.
Significant family members are:
Baby Joe Subject of this Review, aged 5 months at the time the injuries were diagnosed
Ms J Baby’s mother, aged 19 when she became pregnant
Mr J Baby’s father, aged 18 at the time of the pregnancy
Summary of Family History
12. Baby Joe was born in December 2014, reports from family members suggest that Ms J and Mr J had been in a relationship for about a year. They grew up in the same area and had known one another for some years; by the time of the pregnancy they were living together.
13. Prior to becoming pregnant, Ms J was not known to the police or Children’s Services. Her family report that she left home when she was about 16 and had become estranged from her family. Although her family heard about her pregnancy from others, Ms J’s mother didn’t meet Baby Joe until after his injuries were diagnosed.
Serious Case Review, Baby Joe, Fourth Draft
14. Before becoming pregnant Ms J had been treated for depression and diagnosed with an eating disorder. (anorexia) She was known to the Community Mental Health Team (CMHT) although she never really engaged with any treatment. She was prescribed medication for the depression by her GP and this was the main reasons she was defined as vulnerable at the start of her pregnancy.
15. Mr J is almost two years younger than Ms J. Records indicate that he had a complicated history including mental health difficulties leading to hospital admissions and being taken into the care of the local authority. His grandmother was granted a Residence Order when he was a young teenager.
Family Involvement in the Review
16. Both Ms J and Mr J were told about the SCR and encouraged to meet the reviewer and share their views. Unfortunately both parents declined the invitation to participate. The independent Reviewer met Baby Joe and his maternal grandmother who was able to provide some helpful background information.
Serious Case Review, Baby Joe, Fourth Draft
BABY JOE’S EXPERIENCE
17. Police records show that there was friction in the young couple’s household from the day Baby Joe was born; the day he returned home from hospital his father reported that a drunk female was at the family home “kicking off.” Other examples of family life are Mr J reporting a family member banging on the window of their home late at night waking the baby, noise from the upstairs flat keeping the baby awake, an allegation that an associate of the family pushed their way into the flat and was threatening and abusive and on one occasion when Joe was about 2½ months, he was out with his mother when she had an altercation with a family member and alleged she was spat at.
18. The baby was seen at appropriate intervals by health professionals and by the social worker carrying out an assessment. The police and housing staff had seen the baby with his parents and, despite the family difficulties, there were many positive comments about Joe’s care, for example that Ms J was “fine with the baby” “safe with the baby” and that he was “appropriately cared for” “well presented” and that there was “good interaction.” One recording describes Ms J engaging with the baby, “smiling and cuddling him.” No one who saw Baby Joe with either parent was concerned enough about his care to take urgent action, for the professionals who worked with the family at the time this baby did not stand out as being at particular risk.
19. We now know that Baby Joe had three fractures, (broken bones) caused at different
times during the first 5 months of his life, which after investigation were considered to be the result of inflicted injuries. Although these would not necessarily have been visible when the baby was seen by the health professionals, it is possible he would have been in pain and distress at times. No one was charged with a criminal offence.
Serious Case Review, Baby Joe, Fourth Draft
KEY EVENTS
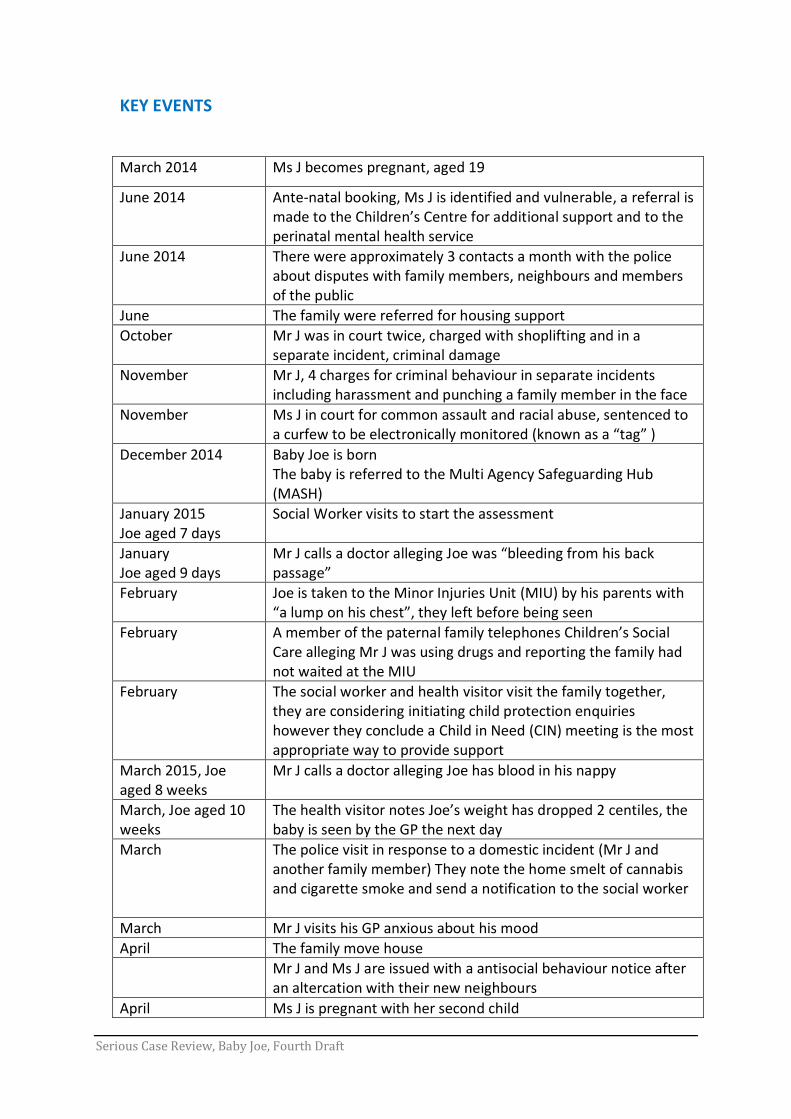
March 2014 Ms J becomes pregnant, aged 19
June 2014 Ante-natal booking, Ms J is identified and vulnerable, a referral is made to the Children’s Centre for additional support and to the perinatal mental health service
June 2014 There were approximately 3 contacts a month with the police about disputes with family members, neighbours and members of the public
June The family were referred for housing support
October Mr J was in court twice, charged with shoplifting and in a separate incident, criminal damage
November Mr J, 4 charges for criminal behaviour in separate incidents including harassment and punching a family member in the face
November Ms J in court for common assault and racial abuse, sentenced to a curfew to be electronically monitored (known as a “tag” )
December 2014 Baby Joe is born The baby is referred to the Multi Agency Safeguarding Hub (MASH)
January 2015 Joe aged 7 days
Social Worker visits to start the assessment
January Joe aged 9 days
Mr J calls a doctor alleging Joe was “bleeding from his back passage”
February Joe is taken to the Minor Injuries Unit (MIU) by his parents with “a lump on his chest”, they left before being seen
February A member of the paternal family telephones Children’s Social Care alleging Mr J was using drugs and reporting the family had not waited at the MIU
February The social worker and health visitor visit the family together, they are considering initiating child protection enquiries however they conclude a Child in Need (CIN) meeting is the most appropriate way to provide support
March 2015, Joe aged 8 weeks
Mr J calls a doctor alleging Joe has blood in his nappy
March, Joe aged 10 weeks
The health visitor notes Joe’s weight has dropped 2 centiles, the baby is seen by the GP the next day
March The police visit in response to a domestic incident (Mr J and another family member) They note the home smelt of cannabis and cigarette smoke and send a notification to the social worker
March Mr J visits his GP anxious about his mood
April The family move house
Mr J and Ms J are issued with a antisocial behaviour notice after an altercation with their new neighbours
April Ms J is pregnant with her second child
Serious Case Review, Baby Joe, Fourth Draft
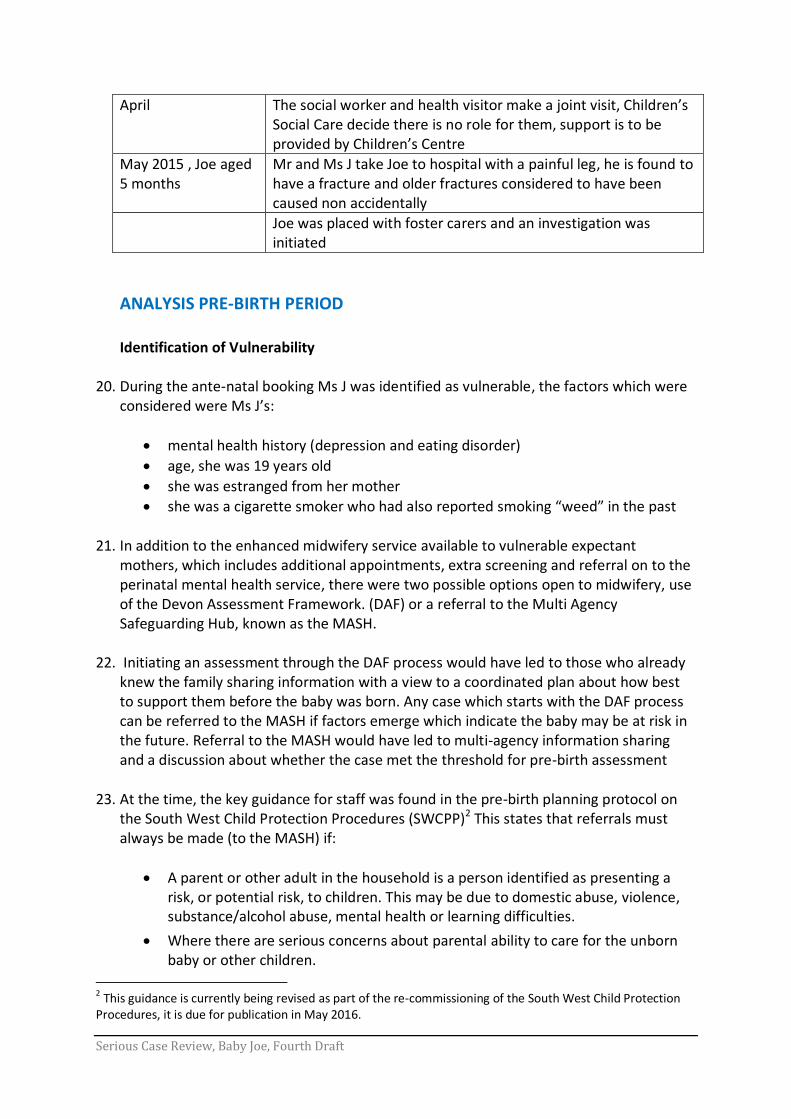
April The social worker and health visitor make a joint visit, Children’s Social Care decide there is no role for them, support is to be provided by Children’s Centre
May 2015 , Joe aged 5 months
Mr and Ms J take Joe to hospital with a painful leg, he is found to have a fracture and older fractures considered to have been caused non accidentally
Joe was placed with foster carers and an investigation was initiated
ANALYSIS PRE-BIRTH PERIOD Identification of Vulnerability
20. During the ante-natal booking Ms J was identified as vulnerable, the factors which were considered were Ms J’s:
mental health history (depression and eating disorder)
age, she was 19 years old
she was estranged from her mother
she was a cigarette smoker who had also reported smoking “weed” in the past 21. In addition to the enhanced midwifery service available to vulnerable expectant
mothers, which includes additional appointments, extra screening and referral on to the perinatal mental health service, there were two possible options open to midwifery, use of the Devon Assessment Framework. (DAF) or a referral to the Multi Agency Safeguarding Hub, known as the MASH.
22. Initiating an assessment through the DAF process would have led to those who already
knew the family sharing information with a view to a coordinated plan about how best to support them before the baby was born. Any case which starts with the DAF process can be referred to the MASH if factors emerge which indicate the baby may be at risk in the future. Referral to the MASH would have led to multi-agency information sharing and a discussion about whether the case met the threshold for pre-birth assessment
23. At the time, the key guidance for staff was found in the pre-birth planning protocol on the South West Child Protection Procedures (SWCPP)2 This states that referrals must always be made (to the MASH) if:
A parent or other adult in the household is a person identified as presenting a risk, or potential risk, to children. This may be due to domestic abuse, violence, substance/alcohol abuse, mental health or learning difficulties.
Where there are serious concerns about parental ability to care for the unborn baby or other children.
2 This guidance is currently being revised as part of the re-commissioning of the South West Child Protection
Procedures, it is due for publication in May 2016.
Serious Case Review, Baby Joe, Fourth Draft
Where there are maternal risk factors e.g. denial of pregnancy, concealed pregnancy, avoidance of antenatal care (failed appointments), non-co-operation with necessary services, non-compliance with treatment with potentially detrimental effects for the unborn baby.
Any other concern exists that the baby may be at risk of significant harm
24. In this case several criteria were met at booking and further factors emerged as the pregnancy progressed which suggested vulnerability of both parents. These were that Mr J was 18 years old, he had been in care as a child, he was a cannabis user and the couple were living in difficult circumstances, in a rented flat below a family member who was said to be “an alcoholic.”
25. Guidance on using the Devon Assessment Framework (DAF) sets out that ... (the DAF)
“will be undertaken by a Lead Professional who should provide support to the child and family, act as an advocate on their behalf and coordinate the delivery of support services. This could be a GP, Family Support Worker, Teacher, Health Visitor and/or Special Educational Needs Coordinator. It’s about who knows the child and family best and is best able to help things move forward.”
Early Help Practice Guidance, DSCB, July 2014
26. To assist staff with their decision making there is also a “Threshold Tool,” published in
the summer of 2014. This is a document for all agencies which sets out in table form the factors which identify levels of vulnerability and help practitioners decide the most appropriate service response for children, although it doesn’t specifically mention unborn babies.
27. Given the vulnerability factors identified by the midwifery team consideration should
have given to referral to the MASH or use of the Devon Assessment Framework (DAF). Even if the first appointments did not raise sufficient concerns, during the antenatal period as more information came to light, this should have prompted consideration of whether thresholds for intervention were reached. For example:
Repeated violent arguments between extended family members and criminal behaviour including common assault
Ms J’s non-engagement with the mental health services who subsequently closed the case
Weight loss and reduced foetal growth in context of Ms J’s known eating disorder
Unplanned admissions/reviews for reduced foetal movements and Ms J reporting abdominal pains
28. In isolation these episodes would not necessarily have reached the threshold for a MASH referral, however as this information emerged it should have prompted a greater curiosity about what was going on in this couples’ life and how that was likely to impact on the unborn child. The needs of the unborn baby appear to have been overlooked in light of the significant needs of the parents.
Serious Case Review, Baby Joe, Fourth Draft
What did happen and why? 29. The midwifery service was aware of this couple’s situation but did not find their
circumstances to be unusual and reported that they were similar to many other expectant parents. Another factor was that the midwives were encouraged that Ms J had engaged with the ante-natal services
30. Midwifery referred the family to the local Children’s Centre for support, in hindsight
they suggested the Children’s Centre might initiate a DAF, although this wasn’t made clear at the time of the referral.
31. Also the midwives in this case were not aware of the pre-birth planning protocol on the
South West Child Protection Procedures (SWCPP) website. Evidence from this review suggests that the midwifery team used their own in-house procedures and discretion to determine whether a family should be referred to the MASH and if this was considered at the start of a pregnancy, unless something dramatic happened, it was unlikely to be considered again.
32. Use of the Devon Assessment Framework to access Early Help has been an ongoing
challenge. In 2015 Ofsted reported the quality of DAFs was “variable, with most being seen by inspectors being of poor quality with limited information included.”
Ofsted Report 2015
33. In 2015 a Serious Case Review, known as CN13, was undertaken. That case concerned a four week old baby who was injured whilst in the care of her parents. The SCR commented on the DAF process saying that it was not well understood by practitioners some of who found the written guidance confusing. Among the conclusions the SCR said that, if the process was to work effectively, staff would need to be able to engage families effectively and be clear about thresholds for intervention.
34. The findings from this case indicate that some staff are concerned about their capacity
to be lead professional and, for others, the value of the DAF as an effective way to access and coordinate early help is still not uppermost in their minds.
Recognition of the Risks of Domestic Abuse
35. Although there was no known domestic abuse between Mr J & Ms J, both had a history of aggressive/violent behaviour and their relationships with some people in their extended family were beset by argument and violence.
36. Domestic abuse between those in an intimate relationship is well recognised by agencies
as detrimental to children’s safety and emotional development, however the significance of persistent aggression in the wider family in this case was not properly considered by any of the professionals who knew the family. Although the Domestic Abuse, Stalking and Harassment (DASH) risk assessment tool was used on 5 occasions during the ante-natal period (standard risk in four, medium risk in one) the police did
Serious Case Review, Baby Joe, Fourth Draft
not use the reporting system, forms known as a 121a3, to share this information with Children’s Social Care until after the baby was born.
37. The Police did develop a “Problem Solving Plan” in order to record and tackle the anti-
social behaviour but the purpose does not include consideration of the risk to the unborn baby from these behaviours; it was closed after the family moved house away from the family members with whom the couple were frequently arguing. The couple went on to have poor relationships with their new neighbours and have continued arguments with family members.
What has happened since 2014 38. For the pre-birth protocol to be effective practitioners need to know about it and
understand its purpose. This case indicates that during the second half of 2014 (and when discussing this case in October 2015) some midwives were not aware of the pre-birth protocol and were using their own agency guidance.
39. The DSCB is addressing this, for example by arranging Best Practice Seminars throughout the county in January 2016 focussing on unborn babies. Reports indicate that the events were well attended by a wide range of professionals, reaching in excess of one hundred and fifty front line practitioners across the county. GPs, health visitors, midwives, police,
3 The 121a form has since been replaced by an assessment tool known as a VIST which is more explicit about
risk factors.
Learning
Any information which emerges through the pregnancy must be considered, not just as isolated incidents, but as part of a whole picture. Retaining a focus on the unborn baby enables practitioners to consider the impact of the parent’s circumstances on their capacity to care for a baby.
Information sharing enables agencies to see the whole picture around this family and prevent what is known as silo working. The protocol for the protection of the unborn baby provided comprehensive guidance for sharing information, assessing need holistically and planning and coordinating intervention.
If an expectant parent demonstrates violence and aggression, even if this isn’t towards their current partner, the behaviour will have implications for the care of a baby. All agencies should be aware of needs of the unborn baby and the multi-agency protocol.
Serious Case Review, Baby Joe, Fourth Draft
probation officers and social workers, amongst others, contributed to discussion and debate arising from recent serious case reviews and multi-agency case audits.
For the DSCB
In order to address the findings from this case, The DSCB should satisfy itself that when the updated pre-birth protocol is published, the work undertaken to promote its use reaches midwifery services. Links with other documents (for example the DAF and Threshold document) should be clear and consistent. If agencies use their own versions, these should be aligned with the protocols agreed by DSCB.
This case indicates the DAF process is not working well. Further work needs to be done to look at whether this case is representative of a wider picture and if so, how access to Early Help can be improved, particularly within the midwifery service.
ANALYSIS POST BIRTH PERIOD
Referral to Children’s Social Care
40. Baby Joe was born in hospital in December 2014. Ms J, who allegedly had a “fear” of hospitals, discharged herself and the baby, against medical advice, soon after the birth.
41. During the birth, the midwives noticed that Ms J was wearing a “tag” indicating that she had been convicted of an offence and was subject to an electronically monitored curfew. They made enquires and discovered that Ms J had been convicted of an offence of assault and racial abuse. This led midwives to make a referral to the Multi Agency Safeguarding Hub. (MASH)
42. The MASH agreed that the case met the threshold for an assessment and it was
allocated to a social worker. Initial enquiries were made and the social worker noted some facts from Mr J’s history including his extensive police record, history of violence, “alcohol issues” and mental health history. The social worker was familiar with Mr J’s history as he had known him as a child.
Children’s Social Care Assessment
43. The assessment record indicates that it was based on three visits to the family and
liaison with midwifery and the health visitor. As part of this SCR the quality of the assessment was reviewed by a Safeguarding Manager and judged to be poor because of the insufficient consideration given to the risks around this family.
44. During the time the assessment was being undertaken additional information came to light which was not properly considered.
Serious Case Review, Baby Joe, Fourth Draft
45. The health visitor noted that the baby’s weight was faltering and that he had dropped two centiles (the baby’s weight is noted on a chart called a centile chart) this led to the health visitor asking the GP to see the baby.
46. Also a relative made a referral to Children’s Social Care reporting drug use by Mr J (cannabis and legal highs) and pointing out that Joe had been taken to hospital with a “lump on his chest” but had been taken home before being seen.
47. This referral was followed up by a joint visit two weeks later by the social worker and the
health visitor; by this time the lump could not be seen. It is impossible to tell whether this was an acute injury that had resolved over the intervening period, delaying the visit meant that it was not possible to make any further assessment.
48. The reason for the delay in this visit appears to be that neither the social worker or
health visitor were particularly concerned about this family and the new information did not change their view. It is notable though that the social worker was concerned enough to discuss with his manager whether child protection enquiries should be initiated ; they concluded that further information was deemed necessary in order to reach this threshold, it was not made clear what this information was.
Police Involvement with the Family and the Relevance of the MARAC 49. During the time the assessment was taking place there was continued involvement by
the police with the family. Between the baby’s birth and the diagnosis of his injuries, the police report that six notifications of domestic abuse, between Mr J and members of his extended family, were sent to Children’s Social Care. However Children’s Social Care report only three reached the case work record. No specific action was taken in response to the reported incidents, the information was considered as part of the overall assessment of the family although this was not evident in the assessment document.
50. When baby Joe was two weeks old, a new domestic abuse referral concerning Mr J and a family member led to a Multi-Agency Risk Assessment Conference, (known as a MARAC) this is a meeting held when a victim is considered to be at high risk to determine the nature of risk and agree a plan to help protect the victim.
51. During the MARAC it was noted that Mr J had allegedly threatened family members including:
Making threats to kill
Throwing hot water and threatening with a knife
Punching in the face
Threatening to “petrol” a family member’s house
Assaulting a family member whilst already on bail for another offence, ignoring the order of the court.
Serious Case Review, Baby Joe, Fourth Draft
52. The Devon Multi-Agency Practitioner Guide for Information Sharing and Referral Procedures for MARAC says that:
“In domestic violence or abuse incidents which are categorised as ‘very high’ where children are resident/present in the home, it will be the decision of the Children and Young People’s Service, as to whether or not a strategy meeting is convened in addition to the MARAC, based on the information provided to them and that held within their systems.”
53. The procedures around the use of the DASH risk assessment and MARAC currently focus on the victim and the child/ren of the victim. It is notable that the wording of the guidance reflects this and has in the past led those present at the meeting to consider only the children of the victim.
54. Part of the role of the MARAC is also to consider the risks the perpetrator poses to anyone else he has a relationship with, in this case Ms J and Baby Joe. The referral form for the MARAC was written up before Baby Joe was born although it does mention that Ms J is pregnant and the baby was due two weeks before the MARAC meeting.
55. The notes of the meeting refer to Mr J’s partner being pregnant. On reflection as part of
this review, the police representative believes that risk to the baby was discussed but it was agreed that there was no need for further action as Children’s Social Care were involved with the family. This is not reflected in the notes.
Was this a Missed Opportunity?
56. It is concerning that so little attention was paid to Mr J’s propensity for violence, his relative youth (he was still only 19) and the fact he had recently become a father. Whilst the high volume of referrals to the MARAC means that only about 10 minutes is given to discussing each case, the level of concern in this case indicates that further discussion should have taken place outside of the MARAC, focussed on the risk to Baby Joe.
57. The opportunity for a discussion was already there as Children’s Social Care were in the
process of carrying out an assessment. They also had other information about this family from which a fuller picture could be built.
58. Children’s Social Care assessment mentions that a MARAC was to be held but there is nothing in it about what was discussed at the meeting or the outcome. Had this been considered as part of the assessment, it is likely that the case would have met the threshold for child protection enquiries to be initiated.
Serious Case Review, Baby Joe, Fourth Draft
For the DSCB
A multi-agency case audit, to focus on families subject to the MARAC process, is already planned to take place during April and May 2016, with the best practice seminars to be held in September 2016. This case provides a useful example of the need for effective information sharing and risk assessment about children associated with the perpetrator of violence, who may not be children of the victim.
The DCSB should consider how learning from this case can be integrated into the audit and practice seminars and whether the current guidance is clear enough.
Conclusion of the Assessment
59. The conclusion of Children’s Social Care assessment was that baby Joe was “not at risk
of significant harm” but that the family would benefit from ongoing support which would be explored further in a Child in Need meeting.
60. It is difficult to understand this decision given the Social Worker was aware of the non-engagement of Ms J with services, the ongoing violence and aggression surrounding this family and the baby’s poor weight gain.
61. The assessment would have been improved by:
A more detailed and accurate description of the concerns which had emerged during Ms J’s pregnancy
Avoiding generalisations for example “no concerns.” What might not “concern” one professional might have a different meaning in the context of what another professional knows
Exploration of the impact of family factors, for example why both parents were estranged from their own families and the implication of this
An accurate picture of the police involvement with the family and the implications for risk to the baby
Learning Points
The MARAC is an important part of the safeguarding system, identifying adults engaging in violent and abusive behaviour within a domestic setting. Links between the MARAC and Children’s Social Care assessment processes should be robust.
Asking the question “what is life like for a child in this family?” will help practitioners retain a child focus.
Serious Case Review, Baby Joe, Fourth Draft
Exploration of the family’s history regarding engagement with services
Inclusion of information about the parents’ health and possible drug use
Information about the baby’s health and in particular his weight gain
A more timely response to the information received from the family member about the hospital visit
A robust analysis of the information and potential risks to the baby
Reasons for the poor quality Assessment
62. It is impossible to know whether, had things been done differently, for example, had the case been identified as meeting the threshold for child protection enquires, whether this would have made a difference to the outcome for Baby Joe.
63. Reflecting on this case with the benefit of hindsight, Children’s Social Care
acknowledged that the work done on this case was not robust enough. 64. Two factors impacted on the quality of practice; firstly the social worker (and the others
in the professional network) did not see this baby as at risk of harm. They perceived the parents as generally cooperative and engaged with services and as having reasonable explanations for their behaviour. The couple wanted to improve things for themselves and Baby Joe and were reassuring in their demeanour.
65. The social work team was especially busy during this period. In 2013, Ofsted had carried
out an inspection in the authority and had been critical of their response to referrals. Managers reported that this led to a substantial increase in cases being passed on to the front line teams for assessment. Management information supports this and shows that, for example, over a year there was a 25% increase in the number of children identified as “in need” (of a service) and that only 26% of assessments were being completed on time.
66. For the social worker this meant little time to reflect on cases and when a view was
formed about a family, often quite early in the case, if this was positive and it looked as if there might not be a role for Children’s Social Care, the view was unlikely to change. The concept of “fixed thinking” is a common theme in SCRs.
67. Once a positive view had been formed and the child was considered not to be at risk, other work was likely to take priority, leading to drift in completing assessments, arranging meetings and seeking out any additional information for less urgent cases.
68. Supervision within the team was compliant with the policy, with formal sessions taking
place once a month. For this team however, the rapid turnover of cases meant that decisions had to be taken outside of formal supervision. Part of the manager’s role is to ensure staff are coping with the work load, if a case was considered low priority, the manager was unlikely to ask a social worker to give more time to it when other more urgent work was waiting. In this case this meant that the manager did not challenge the quality of the assessment and ensure the tasks were completed.
Serious Case Review, Baby Joe, Fourth Draft
For the DCSB
The DSCB should be assured that all practitioners have access to a robust supervision/ advisory process which is monitored and evaluated as part of the quality assurance framework.
Child in Need Plan
69. When a family might benefit from support or services but there are no child protection concerns they can be offered help through a Child in Need plan. The social worker’s assessment, completed in February, had concluded this was the most appropriate way forward for this family. However a month later the social worker discussed the case again with his manager and it was decided that there was unlikely to be a role for Children’s Services and support and services would probably best be provided by Targeted Family Support, primarily through the local Children’s Centre; the health visitor would also continue to see the family.
70. In the light of other more urgent work, arranging the Child in Need meeting was not
seen as a priority and was still waiting to be arranged when baby Joe’s injuries were diagnosed.
Learning Points
If assessments are to be effective they must include a robust analysis of risk. Parental compliance and good intentions do not mean the risk reduced.
Rigorous supervision and management support is essential to ensure practitioners have adequate knowledge of risk factors, to help them reflect on their cases think systemically about risk and avoid over optimism.
Decisions made during both formal and informal supervision and the reasons for them should be recorded.
Children under 1 year old are especially vulnerable; managers should be especially alert to these cases and, where appropriate, challenge what might be fixed thinking.
Faltering weight in babies can be an indicator of parental neglect and should be thoroughly explored.
Serious Case Review, Baby Joe, Fourth Draft
April 2014 – May 2014 71. A the end of April 2014, two months after the assessment was completed and when
baby Joe was four months old, the social worker and health visitor saw the family at home. The visit was prompted by information from the police about conflict between Mr J and a family member (this was an ongoing issue) and a strong smell of cannabis and cigarette smoke in the house.
72. The couple had recently moved and the new home was described as clean and tidy and
the situation as “more positive.” Baby Joe was said to be growing “on a suitable centile line.”
73. Other information gleaned from this meeting was that the couple both admitted using
cannabis, Mr J was due to appear in court in two weeks time charged with assault and this was causing him considerable anxiety. Ms J was in the early stages of a new pregnancy and had stopped taking her anti-depressant medication, the notes don’t say if this was a good thing or a source of concern. She was advised to speak to her GP.
74. Although at the time the outcome for this baby was unknown, based on the factors which were evident, the decision for Children’s Social Care to withdraw seems overly optimistic.
75. Although parents had agreed to a package of support from the Targeted Family service,
their previous history indicated they did not engage with any of the services which had previously been offered and Children’s Social Care did not know whether this had changed.
76. Once the decision to step down the case had been made, it was not reviewed when the additional information became available. This is indicative of a lack of reflection and “fixed thinking” with a lack of rigorous challenge which should be a key part of effective supervision.
Action on Health Presentations
77. Ms J and Mr J were known to the doctors at the local practice. During the period of this review Mr J was seen six times and Ms J twice; Baby Joe was registered when he was a few weeks old and seen four times by three different doctors. The baby was also weighed at the clinic every two weeks. The key learning from this case is the importance of sharing information between health professionals and within the multi-agency team.
Learning Point
In order to avoid the pitfalls of initial bias, misjudgements or a fixed mind-set in the light of new evidence, practitioners must seek out any contrary evidence and critically appraise their own judgements.
Serious Case Review, Baby Joe, Fourth Draft
78. Joe had three unusual presentations to health agencies prior to the diagnosis of the
injuries which led to this review, these were:
Aged 9 days, Mr J rang 111 reporting that Baby Joe was bleeding from the “back-passage.” This presentation in an infant is highly significant. It can indicate serious disease or indicate recent trauma, both of which are potentially very serious and can be life threatening. It was therefore appropriate for the 111 service to pass the call onto the out of hours GP service with a two hour window for action.
A doctor visited and found nothing of significance.
Aged 5 weeks, attendance at the minor injuries unit with a “lump on chest, “the family did not wait to be seen. This information was relayed to the HV and GP.
Aged 2 months, Mr J called 111 and reported that he had seen blood in Joe’s nappy two days previously. He also reported that Joe “wouldn’t settle” and “appeared to be in pain”. The out of hours GP made a visit and could find nothing significant.
Why are these incidents significant? 79. These three presentations in such a young infant are unusual. Bleeding from any orifice
in an infant, in the absence of an underlying medical cause, can be an indicator of abuse. Non-attendance at health appointments, whether routine or unplanned, is recognised to be associated with medical neglect. Although the situation here was not waiting to be seen rather than non-attendance, it does suggest that the parents were unable to prioritise the needs of the child.
80. These presentations can also be considered sentinel events and are similar to sentinel injuries. These are defined as minor inflicted injuries/physical signs that are presented to physicians before the recognition that the child has been abused. Often this recognition comes later with the findings of a severe or catastrophic non-accidental injury. These injuries were present in 25% of children subsequently diagnosed with abuse in one study4.
81. It is the combination of the three events which raises suspicion, – 2 episodes of
unexplained bleeding (one of which was associated with unsettled behaviour) and one of a chest lump, the nature of which is still unclear.
82. The information regarding these individual contacts was shared between agencies but the significance of the combination of these presentations in the context of these
4 Sheets LK et al Paediatrics 2013: 131(4)
Serious Case Review, Baby Joe, Fourth Draft
vulnerable parents does not appear to have been recognised5. At the least it should have prompted a greater curiosity about what was happening in Joe’s life.
Examples of Poor Information Sharing
83. The day following the attendance at the minor injuries unit the GP saw the baby for his 8 week baby check; the following week the health visitor saw the baby for a routine review.
84. The information regarding the attendance at the Minor Injuries Unit was relayed to the GP and health visitor but does not appear to have reached their records quickly enough. Consequently, when the baby was seen by the GP the following day, the GP did not ask about or look for any signs of the “lump on the chest.” The GP did undress the baby, this suggests the lump was not visible.
85. Because the health visitor was not aware of the attendance at the MIU, the incident was
not reviewed at the appointment the following week when a history of “poor feeding” was noted along with the crossing of a weight centile.
86. Had the information been shared effectively this would have created an opportunity for the health visitor to consider the purpose of the visit to the MIU along with the problems with feeding, which might have provided some additional context. (the health visitor eventually received the information via a call from the social worker and they made a joint visit two weeks later, see paragraph on assessment)
87. The health visitor was not aware of the calls to the 111 service. 88. There was a delay in details of the visit from the out of hours GP service getting into the
baby’s GP’s records. Whether this was due to delay in sending the information from the out of hours service or including it in the GP records is unclear.
89. It is reasonable that the out of hours GP service will not have access to information
about families before they visit; it is also reasonable to assume practitioners will have awareness of the potential indicators of non-accidental injury /neglect. Whilst not
5 Christian C Paediatrics 2015: 135(5)
Learning Point
The presence of a number of apparently minor injuries to a baby can be considered sentinel injuries and may be an indication that the child is at risk of harm.
Serious Case Review, Baby Joe, Fourth Draft
necessarily significant in this case, delay in calling a doctor and seeking out alternative doctors from the usual GP, are indicators of concern.
90. The potential significance of the delay in presentation was not mentioned in the
chronology submitted by the out of hours doctors and there is no evidence that they had recognised the possible significance of this in the context of an unusual (and repeated) presentation.
For the DSCB
The DCSB needs to be satisfied that doctors employed by the out of hours GP service have an adequate level of safeguarding knowledge.
Learning Points
Delay in seeking medical attention for a child and seeking out different health professionals (for example out of hours) can be an indicator of child abuse.
Practitioners should cultivate their professional curiosity when dealing with unusual situations.
Serious Case Review, Baby Joe, Fourth Draft
SUMMARY
a) Baby Joe was five months old when he was found to have a fractured leg considered to have been inflicted by one of his parents. Investigations also found evidence of two older fractures although these were difficult to date accurately.
b) The baby’s parents were identified as vulnerable early on in Ms J’s pregnancy, the key issue in this case is the response of all the professionals to this vulnerability, keeping the baby’s welfare at the forefront and deciding when to initiate multi -agency planning and intervention.
c) The DAF process did not work in this case. Where early identification of vulnerability and the involvement of a number of agencies might have indicated the usefulness of an early assessment of need, the DAF was not seen as relevant. This is not a new issue and further thought needs to be given to how the process can be made more effective.
d) Throughout this case there were indications that the baby was at risk of harm yet the
child protection threshold was not considered to be met. There was evidence that the practice guidance which helps practitioners reflect on vulnerability factors was not used effectively and the assessment which took place was of poor quality. For all agencies this highlights the importance of rigorous supervision and management which will ensure compliance with procedures, challenge assumptions and encourage reflective practice.
e) It is particularly notable that all the agencies who knew this family knew that both parents had been convicted of violent offences and were aware of the ongoing violence and aggression within the extended family yet despite this knowledge, yet no-one considered early enough or during the pre-birth stage the impact of this on the care of the baby. Links between the MARAC and safeguarding systems should ensure agencies work together.
f) If a baby presents with a number of injuries, even if they appear to be minor,
research shows that they may be indicative of child abuse or neglect. Practitioners should be aware of the research about sentinel injuries and cultivate a sense of professional curiosity if a baby is seen to have several unusual medical presentations.
g) In common with most SCRs there were examples in this case of ineffective
communication and information sharing systems which need to be improved. It is important to remember that information sharing, whilst clearly essential, is not an end in itself. For communication to be effective information exchange must be timely and the meaning of the information and how it contributes to the overall picture of family functioning must be clear.
Serious Case Review, Baby Joe, Fourth Draft
LEARNING POINTS
Any information which emerges through the pregnancy must be considered, not just as isolated incidents, but as part of a whole picture. Retaining a focus on the unborn baby enables practitioners to consider the impact of the parent’s circumstances on their capacity to care for a baby.
Information sharing enables agencies to see the whole picture around this family and prevent what is known as silo working. The protocol for the protection of the unborn baby provided comprehensive guidance for sharing information, assessing need holistically and planning and coordinating intervention.
If an expectant parent demonstrates violence and aggression, even if this is not towards their current partner, the behaviour will have implications for the care of a baby. All agencies should be aware of needs of the unborn baby and the multi- agency protocol.
The MARAC is an important part of the safeguarding system, identifying adults engaging in violent and abusive behaviour within a domestic setting. Links between the MARAC and Children’s Social Care assessment processes should be robust.
Asking the question “what is life like for a child in this family?” will help practitioners retain a child focus.
If assessments are to be effective they must include a robust analysis of risk. Parental compliance and good intentions do not mean the risk is reduced.
Rigorous supervision and management support is essential to ensure practitioners have adequate knowledge of risk factors, to help them reflect on their cases think systemically about risk and avoid over optimism.
Decisions made during both formal and informal supervision and the reasons for them should be recorded.
Children under 1 year old are especially vulnerable; managers should be especially alert to these cases and where appropriate challenge what might be fixed thinking.
Faltering weight in babies can be an indicator of parental neglect and should be thoroughly explored.
In order to avoid the pitfalls of initial bias, misjudgements or a fixed mind-set in the light of new evidence, practitioners must seek out any contrary evidence and critically appraise their own judgements.
The presence of a number of apparently minor injuries to a baby can be considered sentinel injuries and may be an indication that the child is at risk of harm.

Serious Case Review, Baby Joe, Fourth Draft
Delay in seeking medical attention for a child and seeking out different health professionals (for example out of hours) can be an indicator of child abuse.
Practitioners should cultivate their professional curiosity when dealing with unusual situations.
Serious Case Review, Baby Joe, Fourth Draft
CONSIDERATIONS FOR THE DSCB
In order to address the findings from this case, The DSCB should satisfy itself that when the updated pre-birth protocol is published, the work undertaken to promote its use reaches midwifery services. Links with other documents (for example the DAF and Threshold document) should be clear and consistent. If agencies use their own versions, these should be aligned with the protocols agreed by DSCB.
This case indicates the DAF process is not working well. Further work needs to be done to look at whether this case is representative of a wider picture and if so, how access to Early Help can be improved, particularly within the midwifery service.
A multi-agency case audit, to focus on families subject to the MARAC process, is already planned to take place during April and May 2016, with the best practice seminars to be held in September 2016. This case provides a useful example of the need for effective information sharing and risk assessment about children associated with the perpetrator of violence, who may not be children of the victim.
The DCSB should consider how learning from this case can be integrated into the audit and practice seminars and whether the current guidance is clear enough.
The DSCB should be assured that all practitioners have access to a robust supervision/ advisory process which is monitored and evaluated as part of the quality assurance framework.
The DCSB needs to be satisfied that doctors employed by the out of hours GP service have an adequate level of safeguarding knowledge.
Serious Case Review, Baby Joe, Fourth Draft
GLOSSARY OF TERMS
Child in Need: Section 17 of the Children Act 1989 defines a child as being in need in law if:
He or she has a disability
He or she is unlikely to achieve or maintain or to have the opportunity to achieve or maintain a reasonable standard of health or development without provision of services from the LA;
His or her health or development is likely to be significantly impaired, or further impaired, without the provision of services from the LA;
Any child that comes under the legal definition as being “in need” will qualify for services from the local authority who will assess the extent of the child’s need and what services/support he or she may require. When the assessment is complete there will usually be a multi-agency meting to agree a plan for intervention.
Centiles : A centile chart is made up of lines called centiles. By recording the baby’s height and weight on the chart it is used to decide whether the size of a child falls within the normal (average) range or whether the child is larger or smaller than normal and to see if the baby is growing and gaining weight as expected.
Common Assessment Framework (CAF) known in Devon as the Devon Assessment Framework (DAF): this is a process for gathering and recording information about a child for whom a practitioner has concerns identifying the needs of the child and how the needs can be met. It is a shared assessment and planning framework for use across all children’s services and all local areas in the UK. Sometimes referred as Early Help, it helps to identify in the early stages the child’s additional needs and promote coordinated service provision to meet them Curfew: if someone commits an offence they can be sentenced to a curfew which means they have to be in a specified place, usually their home, between certain hours. Compliance with the order is monitored by the offender wearing an electronic tag, usually around their ankle. This links with a special phone system which can detect if the offender is present at the specified times.
DASH Risk Assessment: The introduction of the new Domestic Abuse, Stalking and Harassment and Honour Based Violence (DASH 2009) Risk Identification, Assessment and Management Model means that all police services and a large number of partner agencies across the UK use a common checklist for identifying and assessing risk. Multi Agency Risk Assessment Conference, MARAC: This is a meeting between representatives of local police, health, child protection, housing practitioners, Independent Domestic Violence Advisors (IDVAs) and other specialists from the statutory and voluntary sectors where information is shared about the highest risk domestic abuse cases. Multi Agency Safeguarding Hub: The MASH is the central resource for the whole of Devon receiving all safeguarding and child protection enquiries. It is staffed with professionals from
Serious Case Review, Baby Joe, Fourth Draft
a range of agencies including police, probation, fire, ambulance, health, education and social care. These professionals share information to ensure early identification of potential significant harm, and trigger interventions to prevent further harm.
Perinatal Mental Health : The perinatal period extends from when pregnancy begins to the first year after the baby is born. Mental health is determined by many factors including hormonal, social and psychological. Mental health problems are often associated with times of stress or change in our lives.
Residence Order: A residence order was a court order settling the arrangements about with whom a child should live. It has since been replaced with a Child Arrangements Order.
Root Cause Analysis: this is a method of analysing serious events which focuses on the underlying causes. It is widely used in health care settings.
Targeted Family Support Programme: This is Devon’s response to the three-year national Troubled Families Programme which works to improve the lives of families in complex situations, where children may be out of education, parents are not in work or if there is crime and antisocial behaviour in the family. The programme can provide long term help and support for families who meet the criteria for intervention. ViST: this is the new vulnerability risk assessment tool used by the police and implemented in Devon in December 2014.
Serious Case Review, Baby Joe, Fourth Draft
APPENDIX
The following Agencies took part in the Serious Case Review:
Practitioner Involvement SCR Review Panel Police Community Mental Health Team Housing Midwifery Health Visiting Children’s Social care GP
Senior Manager, Safeguarding, Devon County Council Social Care Named Nurse - Safeguarding Children, Devon Partnership NHS Trust Detective Inspector, Devon and Cornwall Police Designated Doctor Safeguarding Children, NEW Devon Clinical Commissioning Group Head of Midwifery, Named Midwife for Safeguarding, Royal Devon and Exeter NHS Foundation Trust Lead Designated Nurse Safeguarding Children, NEW Devon CCG Board Manager, Devon Safeguarding Children Board