Embed Size (px)
Citation preview

ABCDEFG
UNIVERS ITY OF OULU P .O . Box 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
EDITORIAL SECRETARY
Professor Mikko Siponen
Professor Harri Mantila
Professor Juha Kostamovaara
Professor Olli Vuolteenaho
Senior Assistant Timo Latomaa
Communications Officer Elna Stjerna
Senior Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publication Editor Kirsti Nurkkala
ISBN 951-42-8192-6 (Paperback)ISBN 951-42-8193-4 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
OULU 2006
D 888
Olli Tenhunen
MITOGEN-ACTIVATED PROTEIN KINASES AND TRANSCRIPTION FACTORS DURING INCREASED CARDIAC WORKLOAD AND REMODELLING
FACULTY OF MEDICINE, DEPARTMENT OF PHARMACOLOGY AND TOXICOLOGY, BIOCENTER OULU,UNIVERSITY OF OULU
D 888
AC
TA O
lli Tenhunen
D888etukansi.fm Page 1 Tuesday, September 12, 2006 12:45 PM


A C T A U N I V E R S I T A T I S O U L U E N S I SD M e d i c a 8 8 8
OLLI TENHUNEN
MITOGEN-ACTIVATED PROTEIN KINASES AND TRANSCRIPTION FACTORS DURING INCREASED CARDIAC WORKLOAD AND REMODELLING
Academic dissertation to be presented, with the assent ofthe Faculty of Medicine of the University of Oulu, forpublic defence in the Auditorium of the Department ofPharmacology and Toxicology, on September 22nd, 2006,at 12 noon
OULUN YLIOPISTO, OULU 2006

Copyright © 2006Acta Univ. Oul. D 888, 2006
Supervised byProfessor Heikki RuskoahoDoctor Hanna Leskinen
Reviewed byDocent Anna-Liisa LevonenProfessor Eero Mervaala
ISBN 951-42-8192-6 (Paperback)ISBN 951-42-8193-4 (PDF) http://herkules.oulu.fi/isbn9514281934/ISSN 0355-3221 (Printed )ISSN 1796-2234 (Online) http://herkules.oulu.fi/issn03553221/
Cover designRaimo Ahonen
OULU UNIVERSITY PRESSOULU 2006

Tenhunen, Olli, Mitogen-activated protein kinases and transcription factors duringincreased cardiac workload and remodellingFaculty of Medicine, Department of Pharmacology and Toxicology, Biocenter Oulu, University ofOulu, P.O. Box 5000, FI-90014 University of Oulu, Finland Acta Univ. Oul. D 888, 2006Oulu, Finland
AbstractCardiac hypertrophy and remodelling are mechanisms of adaptation to increased workload and acuteinjuries of the heart. In the long-term, these initially beneficial mechanisms become detrimental andultimately lead to the development of heart failure. The molecular determinant of myocardialremodelling and heart failure is altered intracellular signal transduction and a modified geneexpression pattern in the individual cardiomyocyte. This study was aimed at characterising thechanges in mitogen-activated protein kinases (MAPKs) and their nuclear effector, GATA-4, and theirfunctional significance and interaction in experimental models of increased cardiac workload andremodelling.
To study the effects of increased cardiac workload on MAPKs and GATA-4, isolated perfused rathearts were subjected to increased left ventricular wall stress and their activities were determinedusing western blot and gel mobility shift assays. Left ventricular wall stress rapidly activated theDNA binding of GATA-4, and this activation was abolished in the presence of endothelin-1 (ET-1)and angiotensin II receptor antagonists. Furthermore, the activation of GATA-4 DNA binding wassignificantly attenuated by p38 MAPK and extracellular signal regulated kinase (ERK) inhibition. Togain further insights into the role of p38 MAPK as a regulator of cardiac transcription factors, geneexpression and remodelling, a gene transfer protocol of increased p38 MAPK activity wasestablished. Direct adenovirus-mediated gene transfer of wild-type p38α and constitutively activeupstream kinase mitogen-activated kinase kinase 3b (MKK3b) selectively increased p38 MAPKactivity in the left ventricle, which was followed by up-regulation of cardiac gene expression,myocardial inflammation and fibrosis. Using a DNA microarray approach, the cardiac target genesof p38 MAPK were identified, including several cell division, inflammation and signal transduction-associated genes. Furthermore, p38 MAPK over-expression was found to increase the DNA bindingactivities of several transcription factors, including GATA-4. Finally, the functional role of p38MAPK was determined using adenovirus-mediated gene transfer in an experimental model ofmyocardial infarction. Post-infarction remodelling was characterised by a sustained down-regulationof p38 MAPK, while rescue of p38 MAPK activity attenuated post-infarction remodelling throughanti-apoptotic and angiogenic mechanisms.
These results indicate that p38 MAPK is a key regulator of GATA-4 transcription factor andcardiac gene expression during left ventricular wall stress and remodelling. They demonstrate thatp38 MAPK, being cardioprotective in the infarcted heart but promoting inflammation and fibrosis inthe normal heart, has a unique dual role in the myocardium.
Keywords: mitogen-activated protein kinases, signal transduction, transcription factors,ventricular remodelling


Acknowledgements
This work was carried out at the Department of Pharmacology and Toxicology, University of Oulu, during the years 2000-2006. I wish to thank the head of the department, Professor Olavi Pelkonen, for the opportunity to do research there. His leadership, encouraging attitude and wide knowledge of science and culture created a perfect atmosphere for scientific work.
I owe my deepest gratitude to my supervisor Professor Heikki Ruskoaho, whose excellent guidance has formed the basis of this thesis. In addition to his broad knowledge and experience, patience and ability to generate inspiration, I highly appreciate the unique innovative and enthusiastic attitude towards science that he possesses. I also express my sincere thanks to my other supervisor, Hanna Leskinen, MD, PhD. Her expert knowledge, methodological guidance and above all the constructive attitude and support that she shows towards younger scientists have been of the utmost importance. Methodological guidance received from Docent Ylermi Soini and Professor Juha Tuukkanen is also warmly acknowledged.
I am grateful to Docent Anna-Liisa Levonen and Professor Eero Mervaala for their thorough review of this manuscript and for their constructive criticism. I express my thanks to Malcolm Hicks for his careful revision of my English.
I have been privileged to work with István Szokodi, MD, PhD, who taught me much about critical scientific work in addition to the basics of the Langendorff method. I also wish to thank my other co-authors, Nina Hautala, Balázs Sármán, Risto Kerkelä, Lajos Papp, Miklós Tóth, Jaana Rysä, Mika Ilves, Raisa Serpi and Harri Pennanen, for their collaboration. All the past and present members of our group deserve my sincere thanks: Jarkko Piuhola, Pietari Kinnunen, Sampsa Pikkarainen, Heikki Tokola, Maria Suo-Palosaari, Tanja Rauma-Pinola, Marja Luodonpää, Tuomas Peltonen, Jani Aro, Erja Mustonen, Anna-Maria Kubin, Marja Paso, Sini Rautio, and Mika Välimäki. Other colleagues at the Department of Pharmacology and Toxicology are warmly acknowledged as well.
I am indebted to the staff of the Department of Pharmacology and Toxicology for their skilful technical assistance, which has been essential for this work. I owe a particular debt of gratitude to Sirpa Rutanen, Kaisa Penttilä, Tuulikki Kärnä, Pirjo Korpi, Marja Arbelius and Kati Viitala, and also to Raija Hanni, Esa Kerttula, Marja Räinä and Terttu Keränen.

All my friends deserve thanks for keeping me socially alive. My special thanks go to Jarkko Karvonen, MD, PhD, for numerous discussions on scientific and non-scientific topics, and I thank Miia Turpeinen, MD, for listening. Without her support this thesis would probably never have been completed.
Finally, and most of all, I wish to thank my parents Päivi and Antero Tenhunen and my brother Lauri and his family for their care, support and encouragement.
This work was supported financially by the Academy of Finland, the Sigrid Juselius Foundation, the Finnish Foundation for Cardiovascular Research, the Finnish Medical Foundation, the Research and Science Foundation of Farmos, the Foundation of Oulu University, the Aarne Koskelo Foundation and the Ida Montin Foundation.
Oulu, July 2006 Olli Tenhunen

Abbreviations
ACE angiotensin-converting enzyme aFGF acidic fibroblast growth factor AMI acute myocardial infarction Ang II angiotensin II ANP atrial natriuretic peptide AP-1 activator protein-1 ARF adenosine diphosphate ribosylation factor ATF activating transcription factor ATx receptor angiotensin receptor subtype AVP arginine-vasopressin bFGF basic fibroblast growth factor BMD-MC bone marrow-derived mononuclear cell BMP bone morphogenetic protein BNP B-type natriuretic peptide CAMK calcium/calmodulin-dependent kinase cAMP cyclic adenosine monophosphate cDNA complementary deoxyribonucleic acid cGMP cyclic guanosine monophosphate CNP C-type natriuretic peptide COX-2 cyclo-oxygenase 2 CSC cardiac stem cell CTGF connective tissue growth factor DAG diacylglycerol EF ejection fraction EMSA electrophoretic mobility shift assay EPC endothelial progenitor cell ERK extracellular signal–regulated kinase EST expressed sequence tag ET-1 endothelin-1 FOG friend of GATA FS fractional shortening

G-protein guanine nucleotide binding protein GPCR G-protein-coupled receptor GSK-3β glycogen synthase kinase 3β HDAC histone deacetylase HGF hepatocyte growth factor HIF hypoxia-inducible factor IGF insulin-like growth factor IL interleukin IP3 inositol triphosphate JNK c-Jun N-terminal kinase LAD left anterior descending coronary artery LVESD left ventricular end-systolic diameter LVEDD left ventricular end-diastolic diameter LW/BW left ventricular weight vs. body weight MAPK mitogen-activated protein kinase MAPKAPK MAPK activated protein kinase MAPKK/MEK/MKK MAPK kinase MAPKKK/MEKK/MKKK MAPK kinase kinase MEF-2 myocyte enhancer factor-2 MHC myosin heavy chain MLK mixed lineage kinase MKP MAPK phosphatase mTOR mammalian target of rapamycin NCX Na+-Ca2+ exchanger NFAT nuclear factor of activated T cells NF-κB nuclear factor κB NPR natriuretic peptide receptor PAI-1 plasminogen activator inhibitor-1 PDGF platelet-derived growth factor PE phenylephrine PI3K phosphoinositide 3-kinase PKA protein kinase A PKC protein kinase C PLC phospholipase C PRAK p38-regulated/activated kinase ROKα/ROCK Rho-dependent kinase RSK ribosomal p90 S6 kinase RT-PCR reverse transcriptase polymerase chain reaction SAC stretch-activated channel SEM standard error of means SERCA-2 sarcoplasmic reticulum Ca2+-ATPase-2 α-SkA skeletal α-actin SHR spontaneously hypertensive rat SRE serum response element SRF serum response factor TCF ternary complex factor

TGF-β transforming growth factor-β TIMP-1 tissue inhibitor of metalloproteinase-1 TNF tumour necrosis factor TUNEL terminal deoxyribonucleotidyl transferase-mediated dUTP nick end labelling VEGF vascular endothelial growth factor WT wild type


List of original papers
This thesis is based on the following articles, which are referred to in the text by their Roman numerals:
I Hautala N, Tenhunen O, Szokodi I & Ruskoaho H (2002) Direct left ventricular wall stretch activates GATA4 binding in perfused rat heart: involvement of autocrine/paracrine pathways. Pflugers Arch 443: 362-369.
II Tenhunen O, Sarman B, Kerkelä R, Szokodi I, Papp L, Toth M & Ruskoaho H (2004) Mitogen-activated protein kinases p38 and ERK 1/2 mediate the wall stress-induced activation of GATA-4 binding in adult heart. J Biol Chem 279: 24852-24860.
III Tenhunen O, Rysä J, Ilves M, Ruskoaho H & Leskinen H (2006) Identification of cell cycle regulatory and inflammatory genes as predominant targets of p38 MAPK in the heart. Circ Res, in press.
IV Tenhunen O, Soini Y, Ilves M, Rysä J, Tuukkanen J, Serpi R, Pennanen H, Ruskoaho H & Leskinen H (2006) p38 kinase rescues failing myocardium after myocardial infarction: evidence for angiogenic and anti-apoptotic mechanisms. FASEB J, in press.
In addition some unpublished data are presented.


Contents
Abstract Acknowledgements Abbreviations List of original papers Contents 1 Introduction ................................................................................................................... 17 2 Review of the literature ................................................................................................. 19
2.1 Pathophysiology of heart failure.............................................................................19 2.1.1 Definition and aetiology of heart failure..........................................................19 2.1.2 Cardiac hypertrophy and hypertensive heart failure........................................20 2.1.3 Post-infarction remodelling and heart failure ..................................................21 2.1.4 Paracrine and neurohumoral mechanisms in heart failure ...............................22
2.1.4.1 The renin-angiotensin-aldosterone system ...............................................22 2.1.4.2 Endothelin-1 .............................................................................................23 2.1.4.3 Natriuretic peptides...................................................................................24
2.2 Cellular mechanisms of myocardial remodelling ...................................................26 2.2.1 Hypertrophic growth and gene expression of cardiac myocytes .....................26 2.2.2 Apoptotic cell death .........................................................................................28 2.2.3 Neovascularisation ..........................................................................................29 2.2.4 Cardiac stem cells............................................................................................31 2.2.5 Myocardial fibrosis..........................................................................................31 2.2.6 Inflammation ...................................................................................................32
2.3 Intracellular signal transduction pathways in myocardial remodelling ..................33 2.3.1 Mechanotransduction.......................................................................................34 2.3.2 G proteins ........................................................................................................35 2.3.3 Small G proteins ..............................................................................................36 2.3.4 Protein kinase C...............................................................................................38 2.3.5 Mitogen-activated protein kinases...................................................................39
2.3.5.1 p38 MAPK................................................................................................40 2.3.5.2 Extracellular signal-regulated kinase........................................................44 2.3.5.3 JNK...........................................................................................................45

2.3.5.4 MAPK inactivation and MAPK phosphatases..........................................47 2.3.6 Ca2+/calmodulin-dependent protein kinase and calcineurin ............................47 2.3.7 The PI3K - Akt pathway..................................................................................48
2.4 Cardiac transcription factors...................................................................................49 2.4.1 The GATA family of transcription factors .......................................................49
2.4.1.1 GATA-4 ....................................................................................................50 2.4.1.2 Other members of the GATA family.........................................................55
2.4.2 AP-1.................................................................................................................55 2.4.3 NF-κB..............................................................................................................56 2.4.4 MEF-2 .............................................................................................................58 2.4.5 SRF..................................................................................................................59
3 Aims of the research ...................................................................................................... 60 4 Materials and methods................................................................................................... 61
4.1 Materials .................................................................................................................61 4.2 Experimental protocols...........................................................................................62
4.2.1 Experimental animals ......................................................................................62 4.2.2 Preparation of isolated perfused rat hearts.......................................................63 4.2.3 Preparation of isolated rat atria........................................................................64 4.2.4 Adenoviral gene transfer in vivo......................................................................64 4.2.5 Experimental myocardial infarction ................................................................65
4.3 Echocardiographic measurements (III, IV) ............................................................65 4.4 Extraction of cytoplasmic and nuclear protein (I-IV).............................................65 4.5 Western blot analysis and kinase activity assays (II-IV) ........................................66 4.6 Gel mobility shift assays (I-III) ..............................................................................67 4.7 Isolation and analysis of RNA (I-IV)......................................................................68 4.8 DNA microarrays (III) ............................................................................................69 4.9 Histological analysis (III, IV) .................................................................................69 4.10 Statistical analysis.................................................................................................70
5 Results ........................................................................................................................... 71 5.1 Activation of cardiac transcription factors by increased wall stress (I, II)..............71
5.1.1 Wall stress rapidly activates GATA-4 and AP-1 binding .................................71 5.1.2 Activation of cardiac gene expression by left ventricular wall stress ..............72 5.1.3 Paracrine/autocrine mechanisms of wall stress-induced GATA-4 and
AP-1 activation................................................................................................72 5.2 Regulation of wall stress-induced GATA-4 activity by p38 MAPK and
ERK 1/2 (II)...........................................................................................................73 5.2.1 Activation of p38 MAPK and ERK 1/2 by left ventricular wall stress ............73 5.2.2 Effect of pharmacological p38 MAPK and ERK 1/2 inhibition on
GATA-4 binding ..............................................................................................73 5.2.3 Effect of PKC and Rho kinase inhibition on GATA-4 binding........................74
5.3 Functional role of p38 MAPK in the intact heart (III)............................................75 5.3.1 Activation of p38 MAPK by adenovirus-mediated gene transfer....................75 5.3.2 Up-regulation of cardiac gene expression by p38 MAPK: a DNA
microarray analysis..........................................................................................76 5.3.3 Northern blot and RT-PCR analysis of microarray results...............................78 5.3.4 Activation of GATA-4 by p38 MAPK over-expression...................................78

5.3.5 Activation of other cardiac transcription factors by p38 MAPK .....................78 5.3.6 Function of hearts over-expressing p38 MAPK ..............................................79 5.3.7 Inflammation ...................................................................................................79 5.3.8 Fibrosis ............................................................................................................80 5.3.9 Proliferation.....................................................................................................80
5.4 Role of p38 MAPK in the infarcted heart (IV) .......................................................81 5.4.1 Haemodynamic changes after myocardial infarction ......................................81 5.4.2 Inactivation of p38 MAPK after myocardial infarction...................................82 5.4.3 Restoration of p38 MAPK activity by adenovirus-mediated gene
transfer.............................................................................................................82 5.4.4 Rescue of cardiac function in hearts over-expressing p38 MAPK
during post-infarction remodelling ..................................................................83 5.4.5 Normalisation of p38 MAPK activity reduces infarct size, apoptosis
and fibrosis ......................................................................................................84 5.4.6 Enhanced coronary angiogenesis in hearts over-expressing p38
MAPK .............................................................................................................85 5.5 Altered GATA-4 binding during post-infarction remodelling.................................86
5.5.1 Transient inactivation of GATA-4 binding after myocardial infarction...........86 5.5.2 AP-1, NF-κB and SRF binding activities after myocardial infarction .............86 5.5.3 p38 MAPK-independent regulation of GATA-4 in the infarcted heart ............87
6 Discussion ..................................................................................................................... 89 6.1 Transcription factor activities during wall stress and remodelling .........................89 6.2 The role of p38 MAPK in the regulation of GATA-4 .............................................90 6.3 Other mechanisms of GATA-4 regulation ..............................................................92 6.4 The role of p38 MAPK in cardiac gene expression ................................................92 6.5 The dual role of p38 MAPK in normal and infarcted hearts...................................94
7 Summary and conclusions ............................................................................................. 98 References Original papers


1 Introduction
Chronic heart failure is a major cause of morbidity and mortality in industrialised societies (Jessup & Brozena 2003). The prevalence of symptomatic heart failure in Europe is estimated to be 0.4-2.0% and is rising as the proportion of the elderly population increases (Remme et al. 2001). Despite appropriate pharmacological and operative interventions, symptomatic heart failure continues to confer a poor prognosis, with a one-year mortality of approximately 45%. The aetiology of heart failure is multi-factorial, and it can be considered the final pathway for a number of diseases affecting the heart. Two primary causes account for the majority of heart failure cases, however: hypertension and hypertensive cardiomyopathy, and myocardial infarction with subsequent left ventricular remodelling. (Francis 2001, Jessup & Brozena 2003.)
Hypertension and other forms of cardiac overload initiate cardiac hypertrophy and hypertensive remodelling as an adaptive process to counterbalance the increased wall stress (Lorell & Carabello 2000). At the physiological level, they are characterised by an increase in the myocardial mass and alterations in ventricular structure, while at the cellular level, both the size of individual myocytes and sarcomeric assembly of myofibrils are increased (Sugden & Clerk 1998a). Myocardial infarction in turn induces a unique pattern of myocardial remodelling characterised by an early phase with infarct expansion and a late phase with progressive scar formation and hypertrophy of the non-infarcted area. Eventually both types of myocardial remodelling lead to a progressive loss of systolic and diastolic function and symptomatic heart failure. (Sutton & Sharpe 2000.)
The cellular and structural changes in the myocyte in hypertrophy and remodelling result from alterations in gene expression and protein synthesis. For these to occur, the primary stimulus has to be transduced from the cell membrane to the nucleus of the myocyte. Indeed, both cardiac hypertrophy and post-infarction remodelling involve changes in intracellular signalling pathways (Sugden & Clerk 1998a, Swynghedauw 1999). However, due to the complex nature of intracellular signal transduction pathways, the specific changes in signalling molecules remain poorly understood and it is not known which of them contribute to the pathogenesis of heart failure. Mitogen-activated protein kinases (MAPKs) represent one of the best-conserved cytoplasmic signal transduction systems in the myocyte, and previous studies have suggested that they may be involved in the development of different forms of cardiac hypertrophy and ischaemia-

18
reperfusion injury (Sugden & Clerk 1998b, Behr et al. 2001). There is a limited amount of evidence regarding their functional importance in ventricular remodelling in vivo, however, and the downstream targets connecting MAPKs to gene expression remain poorly understood, even though it is evident that the alterations in cardiac gene expression are not directly controlled by them but require specific changes in nuclear transcription factors. GATA-4, a conserved cardiac-restricted zinc finger transcription factor, has been identified as a regulator of cardiac development, hypertrophy and myocyte apoptosis (Kuo et al. 1997, Molkentin et al. 1997, Liang et al. 2001a, Kim et al. 2003, Pikkarainen et al. 2003, Suzuki & Evans 2004), but it is not known whether MAPKs and GATA-4 are linked to each other in vivo in order to coordinate cardiac gene expression, hypertrophy and remodelling.
In the present study experimental approaches representing the two major primary stimuli for heart failure, increased wall stress and myocardial infarction, were used to examine the changes in cytoplasmic signal transduction pathways and nuclear transcription factors. More specifically, the aim was to characterise the changes in GATA-4 activity and the role of MAPKs in the regulation of GATA-4 and cardiac gene expression during increased wall stress and remodelling. In addition, the functional role of p38 MAPK in the myocardium was determined.

2 Review of the literature
2.1 Pathophysiology of heart failure
2.1.1 Definition and aetiology of heart failure
Heart failure is defined as the inability of the heart to pump a sufficient amount of blood to the peripheral organs to meet the metabolic requirements of the body (Jessup & Brozena 2003, Liew & Dzau 2004). It is a complex clinical syndrome manifested by impairment of cardiac function and circulatory congestion and by many extra-cardiac features, including neuroendocrine activation (Francis 2001, Jessup & Brozena 2003). In this context it can be regarded as a continuous process of ventricular remodelling initiated by an index event, followed by progressive changes in shape, size and function of the heart and culminating in the clinical symptoms (Francis 2001). Heart failure is divided into two broad categories, systolic heart failure and diastolic heart failure. Systolic heart failure is characterised by impaired systolic function and contractility, while the most typical features of diastolic heart failure are abnormal filling characteristics due to impaired ventricular relaxation (Jessup & Brozena 2003).
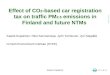
Heart failure has diverse etiologies, including both inherited and environmental factors (Jessup & Brozena 2003), but as defined above, it is almost universally a consequence of antecedent cardiovascular disease (Fig. 1). Two major causes can be distinguished among these: coronary artery disease with myocardial infarction, and prolonged systemic hypertension. Indeed, clinical studies have demonstrated that previous myocardial infarction can be found in over 60% of patients with heart failure and a history of hypertension in up to 90% (Bourassa et al. 1993, Levy et al. 1996). Uncorrected valvular disease, such as aortic stenosis or mitral regurgitation, may also lead to heart failure via pressure-volume overload (Francis 2001, Jessup & Brozena 2003). Also among the known causes are idiopathic cardiomyopathies, the use of chemotherapeutic drugs and toxic agents such as alcohol (Jessup & Brozena 2003). Mutations of single genes encoding structural proteins of the sarcomere, for instance, have been identified as rare genetic causes of heart failure (Morita et al. 2005).

20
Fig. 1. A summary of the mechanisms involved in myocardial remodelling. For reviews, see Jessup & Brozena (2003) and Swynghedauw (1999).
2.1.2 Cardiac hypertrophy and hypertensive heart failure
Normal adult cardiomyocytes are terminally differentiated cells, and instead of cellular hyperplasia, the heart shows primarily a hypertrophic response to increased workload. Cardiac hypertrophy in its broadest sense is defined as an increase in myocardial muscle mass due to the enlargement of individual myocytes. (Lorell & Carabello 2000.) Functionally, it is considered an adaptive response aimed at alleviating the elevation in wall stress according to LaPlace’s principle (Lips et al. 2003). Two morphological phenotypes of cardiac hypertrophy are classically distinguished: concentric hypertrophy, characterised by parallel addition of sarcomeres and lateral growth of cardiomyocytes, and eccentric hypertrophy, characterised by the addition of sarcomeres in series and longitudinal cell growth (Lorell & Carabello 2000, Dorn et al. 2003). Although increased wall stress represents the major stimulus for both phenotypes, concentric hypertrophy is generally observed in response to pressure overload, whereas eccentric hypertrophy more often occurs due to volume overload or prior infarction (Lorell & Carabello 2000).
The course of hypertrophic transformation has been traditionally divided into three stages: (1) developing hypertrophy, in which the load exceeds the output, (2) compensatory hypertrophy, characterised by a normalised workload/mass ratio and maintained cardiac output, and (3) overt heart failure, with progressive ventricular dilatation and functional decline (Meerson 1961). The initial functional benefits of
Heart failure
LV LVLV
Remodelling
Index event:Myocardial infarctionIncreased workload
Normal heart
Adaptive responses:Neurohumoral activation
Myocyte hypertrophyApoptotic cell death
Stem cell recruitmentNeovascularisation
Inflammation Fibrosis
Heart failure
LV LVLV
Remodelling
Index event:Myocardial infarctionIncreased workload
Normal heart
Adaptive responses:Neurohumoral activation
Myocyte hypertrophyApoptotic cell death
Stem cell recruitmentNeovascularisation
Inflammation Fibrosis

21
developing and compensatory hypertrophy include an increase in the number of contractile elements and in stroke volume and a lowering of wall stress and oxygen consumption (Grossman et al. 1975). Even though the phases of hypertrophic transformation have been known for decades, the exact pathophysiological mechanisms whereby the initially beneficial and compensatory response progresses to overt heart failure remain poorly understood. The increased left ventricular stiffness that is characteristic of the hypertrophied heart may directly lead to diastolic dysfunction via abnormal left ventricular filling, but the mechanisms leading to systolic dysfunction are presumably far more complex (Jessup & Brozena 2003, Kass et al. 2004). The structural abnormalities that are observed in the transition from hypertrophy to heart failure include ventricular dilatation, excessive interstitial fibrosis and loss of myocytes due to an increased rate of apoptosis (Meerson 1961, Bing 1994, Lips et al. 2003). At the functional level, afterload excess due to the inability of the heart to compensate for the wall stress itself reduces systolic performance, and subendocardial ischaemia due to a reduced coronary flow reserve may also limit the exercise reserve (Gunther & Grossman 1979, Nakano et al. 1989). Functional perturbations include changes in intracellular calcium handling, which may contribute to the depression of the force-frequency relationship predispose the subject to increased arrhythmogenicity (Hill 2003). Complex alterations in structure, intracellular signalling and energy metabolism are observed within the myocytes (Lorell & Carabello 2000, Lips et al. 2003).
2.1.3 Post-infarction remodelling and heart failure
Acute myocardial infarction induces a unique pattern of left ventricular remodelling affecting the structural and functional architecture of the infarcted area, the ischaemic border zone and the remote, non-infarcted regions of the heart (Pfeffer & Braunwald 1990, Sutton & Sharpe 2000). Post-infarction remodelling has been arbitrarily divided into an early phase (within 72 hours of the onset of myocardial infarction) and a late phase (beyond 72 hours) (Sutton & Sharpe 2000).
The very first hours of myocardial infarction are characterised by an acute loss of cardiomyocytes, oedema and inflammation localised in the infarcted regions (Pfeffer & Braunwald 1990). Also associated with this early phase of remodelling are abrupt changes in the left ventricular loading conditions (Sutton & Sharpe 2000). The acute loss of myocytes is immediately followed by expansion of the infarct area, originally defined by Hutchins and Balkley as an acute dilatation and thinning of the area of infarction that cannot be explained by additional myocardial necrosis (Hutchins & Bulkley 1978). At the cellular level, early remodelling and infarct expansion are at least partially explained by degradation of the intermyocyte collagen struts by serine proteases and the activation of matrix metalloproteinases released from neutrophiles (Sutton & Sharpe 2000). Infarct expansion, in turn, results in further elevation of both systolic and diastolic wall stresses, an altered Frank-Starling response and deformation of the remote myocardium (Pfeffer & Braunwald 1990, Sutton & Sharpe 2000). Early remodelling also evokes multiple adaptive responses at the systemic level, e.g. sympathetic activation, activation of the renin-angiotensin-aldosterone system and increased production of A-type (ANP) and B-

22
type (BNP) natriuretic peptides (Sutton & Sharpe 2000). Early remodelling with infarct expansion is most frequently observed in the case of large transmural infarctions, and patients with pronounced infarct expansion are more likely to develop myocardial rupture or aneurysm (Pfeffer & Braunwald 1990).
The elevated wall stress and neurohumoral activation associated with early remodelling are powerful stimuli for the hypertrophic growth of myocytes, and thus partially initiate the mechanisms of late remodelling (Lorell & Carabello 2000, Lips et al. 2003). To stabilise the distending forces and distribute the increased wall stress more evenly, the non-infarcted region of the heart undergoes hypertrophic growth and the infarcted area develops a collagen scar, which are hallmarks of late post-infarction remodelling (Sutton & Sharpe 2000). At the functional level, however, the loss of functional myocytes due to the increased rate of apoptosis gradually detracts from systolic function, which results in an increased end-systolic volume and ventricular dilatation (Olivetti et al. 1997). Hypertrophy and excessive interstitial fibrosis in turn result in increased diastolic pressure and volume, leading to diastolic dysfunction (Volders et al. 1993). Peripheral mechanisms further increase both the pre-load and after-load in late post-infarction remodelling. Collectively, these changes lead to a progressive decline in both systolic and diastolic function, and eventually to clinical symptoms of congestive heart failure.
2.1.4 Paracrine and neurohumoral mechanisms in heart failure
Although the traditional haemodynamic model emphasised inadequate left ventricular systolic function as the key mechanism in heart failure, it has become evident from later studies that the circulus viciosus of neuroendocrine activation is a critical determinant of its pathogenesis (Francis 2001).
In most cases of heart failure cardiac output is decreased, and this together with the subsequent arterial underfilling lead to baroreceptor-mediated activation of the sympathetic tone. The major haemodynamic consequences of this sympathetic activation include α-receptor-mediated peripheral vasoconstriction, increased myocardial contractility and tachycardia, which lead to an increase in both cardiac pre-load and afterload. Increased sympathetic tone and the subsequent haemodynamic changes are also powerful activators of other paracrine and endocrine mechanisms, such as the renin-angiotensin-aldosterone system. (Schrier & Abraham 1999, Francis 2001.)
2.1.4.1 The renin-angiotensin-aldosterone system
Both the low renal perfusion pressure and the increased beta-adrenergic stimulation activate the renin-angiotensin-aldosterone system in the presence of heart failure (Schrier & Abraham 1999). The circulating renin-angiotensin-aldosterone system includes renin, which cleaves angiotensinogen to inactive angiotensin I, which in turn is further converted to the active octapeptide angiotensin II by the angiotensin-converting enzyme (ACE) (Kim & Iwao 2000, Bader et al. 2001).

23
Although the renin-angiotensin-aldosterone system is considered to be endocrine in nature, evidence is accumulating that the heart and several other tissues contain and/or synthesise its components in an autocrine or paracrine manner, and the functional effects of renin and angiotensin in remodelling and heart failure have been at least partially attributed to local modulation of tissue function (Bader et al. 2001). The presence of renin, angiotensin I, angiotensin II and angiotensin II receptors has been reported in the heart, and the local angiotensin production is activated in the hypertrophied heart and in response to pressure and volume overload (Pieruzzi et al. 1995, Bader et al. 2001). Furthermore, mechanical stretch has been shown to induce the local release of angiotensin II in the myocardium, which increases the expression of other components of the renin-angiotensin system via a positive feedback loop (Sadoshima et al. 1993, Tamura et al. 1998).
The functional effects of angiotensin II are mediated via guanine nucleotide binding protein (G-protein) coupled receptors (GPCRs). Angiotensin II is bound by two distinct receptor isoforms, both of which are expressed in the heart (Kim & Iwao 2000). Although the type 1 angiotensin II receptor (AT1), which can be further divided into the subtypes AT1A and AT1B in rodents, shares structural homology with the type 2 receptor (AT2), they are functionally distinct and differentially distributed (Unger et al. 1996, Kim & Iwao 2000). The classical systemic effects of angiotensin II include vasoconstriction via increased contraction of the vascular smooth muscle, aldosterone biosynthesis, increased sodium and water reabsorption and increased catecholamine synthesis. Angiotensin II increases collagen synthesis and fibrosis locally and is able to directly induce hypertrophic growth of the heart. Angiotensin II also has a direct positive inotropic effect. (Kim & Iwao 2000.)
In addition to its effects on fluid homeostasis, aldosterone may have direct adverse effects in the pathophysiology of heart failure. Both cardiac myocytes and vascular smooth muscle cells express aldosterone receptors (Scott et al. 1987, Lombes et al. 1992), and cardiac aldosterone levels are increased in failing human hearts, hypertensive rats and rats with myocardial infarction (Silvestre et al. 1999, Takeda et al. 2000, Mizuno et al. 2001). Treatment with the aldosterone antagonist eplerenone is able to attenuate post-infarction remodelling and fibrosis without affecting systemic blood pressure (Suzuki et al. 2002), and infusion of aldosterone will similarly induce cardiac hypertrophy without any effects on blood pressure (Young et al. 1995).
2.1.4.2 Endothelin-1
Endothelin-1 (ET-1), a 21-amino acid vasoactive peptide, was originally identified in the cultured media of porcine endothelial cells (Yanagisawa et al. 1988). ET-1 shares structural homology with three closely related isopeptides ET-2, ET-3, ET-4 and with the snake venom sarafotoxin (Lüscher & Barton 2000, Teerlink 2002). ET-1 is produced by a variety of tissues, including endothelial cells, vascular smooth muscle cells, cardiomyocytes, brain and kidney (MacCumber et al. 1989, Lerman et al. 1991, Suzuki et al. 1993). The synthesis of ET-1 from its precursor peptides prepro-ET-1 and big ET-1 is a complex process activated by shear stress, mechanical strain, hypoxia, other

24
vasoconstrictors, growth factors and cytokines and inhibited by nitric oxide, prostacyclin and ANP. ET-1 is transported and released via a constitutive pathway from secretory vesicles and in an inducible manner from the Weibel-Palade bodies of the endothelial cells in response to shear stress, angiotensin II and growth factors (Remuzzi et al. 2002).
While ET-1 is the most powerful vasoconstrictory peptide identified, ET-2 and ET-3 do not appear to have significant roles in cardiovascular pathophysiology (Yanagisawa et al. 1988, Teerlink 2002). Functionally, ET-1 is a versatile vasoactive peptide. Besides the well-characterised vasoconstrictory effect, it has been reported to be mitogenic, to stimulate the production of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) and to potentiate the effects of transforming growth factor β (TGF-β) and platelet-derived growth factor (PDGF) (Lüscher & Barton 2000). ET-1 also modulates water and salt balance and has a powerful inotropic and chronotropic effect in the heart (Ishikawa et al. 1988a, Ishikawa et al. 1988b, Yamada & Yoshida 1991). The production of ET-1 is up-regulated in vivo under pathophysiological conditions such as pressure overload, experimental myocardial infarction, or chronic heart failure (Yorikane et al. 1993, Sakai et al. 1996b, Kobayashi et al. 1999).
The functional effects of ET-1 are mediated by two GPCR subtypes, ETA and ETB receptors (Arai et al. 1990, Sakurai et al. 1990). These have different tissue distributions, different affinities for ET isopeptides and partially distinct functional effects. ETA receptors are found more abundantly in cardiomyocytes and smooth muscle cells, whereas ETB receptors are predominantly expressed in endothelial cells (Lüscher & Barton 2000). The vasoconstrictory and proliferative effects of ET-1 are primarily mediated by ETA receptors, while the stimulation of ETB receptors promotes vasodilation via nitric oxide and prostacyclin. In the context of cardiovascular pathophysiology, ETA receptors are thought to be responsible for the majority of the effects of ET-1. (Lüscher & Barton 2000, Remuzzi et al. 2002.) Indeed, a specific blockade of ETA receptors with pharmacological inhibitors was reported to attenuate pressure overload-induced cardiac hypertrophy and left ventricular remodelling after experimental myocardial infarction (Ito et al. 1994, Sakai et al. 1996a).
2.1.4.3 Natriuretic peptides
The first evidence of the existence of a natriuretic substance in the atrial tissue of the heart was obtained in the pioneering experiments of de Bold and co-workers, which demonstrated a natriuretic and diuretic effect in rats after the injection of atrial tissue extract (de Bold et al. 1981). This was followed by the identification and cloning of atrial natriuretic peptide, the molecule responsible for these effects (Atlas et al. 1984). Soon after the characterisation of ANP, two additional peptides that shared considerable structural and functional homology with ANP were identified and designated as B-type and C-type (CNP) natriuretic peptides (Sudoh et al. 1988, Sudoh et al. 1990). As implied by the initial studies, the main biological function of ANP and BNP is the regulation of sodium and fluid homeostasis and blood pressure, while CNP is mainly involved in endothelial cell responses (Ruskoaho 1992).

25
ANP is mainly synthesised, stored and secreted by the atria of the adult heart (see Table 1), its protein being found in 100 times higher concentrations in the atrial tissue than in the ventricle, so that ANP mRNA can constitute up to 3% of all atrial mRNA (Gardner et al. 1986, Ruskoaho 1992). ANP is also expressed in the ventricular tissue, although to a lesser extent relative to tissue weight. Outside the heart, ANP mRNA or immunoreactivity has been detected in the lung, brain, adrenal glands, kidney, adipose tissue, aorta, gastrointestinal tract, thymus and eye (Ruskoaho 1992). The biological effects of ANP are mainly mediated by type A natriuretic peptide receptors (NPRA), which are most abundantly expressed in the adrenal gland, lung, kidney and aorta (Nakao et al. 1992). ANP is removed from the circulation by both clearance receptors and neutral endopeptidase-mediated hydrolysis. The circulating plasma levels of ANP and its pro-hormone NT-proANP are increased in heart failure, and measurement of NT-proANP is widely recognised as being of diagnostic value for the clinical management of heart failure patients. The mechanism underlying the increased ANP plasma levels is the synthesis and release of ANP from the atrial and ventricular tissue due to increased wall stretch. In addition, elevated levels of circulating hormones and cytokines may contribute to the increased ANP release. (Ruskoaho 2003.) ANP lowers the cardiac workload through its effects on natriuresis and diuresis, thereby affecting blood pressure and vascular tone. The central role of ANP in controlling blood pressure is also reflected in the gain-of-function and loss-of-function studies that have demonstrated that ANP deletion causes salt-sensitive hypertension (John et al. 1996), and conversely, that ANP over-expression leads to arterial hypotension (Steinhelper et al. 1990). However, the effects of ANP are not restricted to the systemic maintenance of blood pressure and fluid homeostasis, but also include paracrine functions. Importantly, both protein synthesis and hypertrophic gene expression are increased when cultured cardiomyocytes are treated with an ANP receptor antagonist (Horio et al. 2000), and conversely, the treatment of cardiomyocytes with synthetic ANP attenuates GPCR-agonist-induced hypertrophic responses (Calderone et al. 1998).
Although it had originally been isolated from porcine brain, it soon became evident that BNP is mainly expressed in cardiac ventricular myocytes (Ruskoaho 1992). Its ventricular expression is dramatically increased during cardiac overload and hypertrophy, leading to plasma levels that can exceed those of ANP in advanced cases of heart failure (Gardner 2003). Indeed, BNP and NT-proBNP also represent diagnostic markers of heart failure, as normal levels have a consistent and very high negative predictive value. Furthermore, these levels may also have a prognostic value, as they appear to correlate with the progression of heart failure (Ruskoaho 2003). ANP and BNP share several common functional and structural features: they contain a common structural motif consisting of a 17-amino-acid loop, initiate their actions mainly via NPRA receptors, and both have mechanical stretch as the major determinant for their release (Ruskoaho 1992, Ruskoaho 2003). The gene expression and secretion of both peptides are activated by a number of other stimuli, including GPCR agonists and cytokines. The physiological effects of BNP also partially resemble those of ANP, since high concentrations of BNP induce hypotensive, natriuretic and diuretic effects (Ogawa et al. 1994, Kuhn 2005). The phenotype of transgenic mice with targeted deletion of BNP differs from that of ANP knock-out mice, however, as they do not show signs of hypertension or hypertrophy but develop focal fibrotic lesions within their hearts (Tamura et al. 2000). BNP also

26
suppresses collagen production and induces metalloproteinase activity in cardiac fibroblasts (Tsuruda et al. 2002), which further supports the role of BNP as an important paracrine regulator of myocardial fibrosis. Nevertheless, these findings suggesting paracrine functions for BNP do not exclude a role for it as a systemic regulator of cardiovascular homeostasis in heart failure patients. Importantly, BNP and its synthetic analogues appear to have ameliorative effects on the central haemodynamics of heart failure patients, suggesting a therapeutic potential (Gardner 2003).
The third member of the natriuretic peptide family, CNP, shares their common 17-amino-acid ring structure, and is the most highly conserved of all of them between species. Circulating levels of CNP are typically low in the absence of disease, suggesting that CNP acts in a paracrine or autocrine rather than an endocrine fashion. (Scotland et al. 2005.) It does indeed appear to differ functionally from the other two members of the natriuretic peptide family. It is mainly produced in the neural system and vascular endothelial cells rather than the heart (Komatsu et al. 1991, Chen & Burnett 1998), and it preferentially binds to NPRB receptors, which are found in the brain, kidney, adrenal glands and vascular smooth muscle (Levin et al. 1998, Scotland et al. 2005). It has recently been suggested that CNP may be a local regulator of vascular tone, since it has been found to cause vasodilation and increase blood flow when injected locally into the human forearm (Honing et al. 2001). In addition, it has been suggested that, acting via NPRC receptors, CNP could represent an endothelium-derived hyperpolarising factor (Scotland et al. 2005). Finally, CNP knock-out mice show impaired endochondral ossification, suggesting that CNP may be involved in bone development during embryogenesis (Chusho et al. 2001).
Table 1. Comparison of receptors, tissue distribution and effects of natriuretic peptides. For reviews, see Ruskoaho 1992, Ruskoaho 2003 and Scotland 2005.
ANP BNP CNP Receptor NPRA NPRA NPRB Tissue distribution atria > ventricles ventricles > atria neural system, vascular
endothelial cells Main functions natriuresis
diuresis natriuresis diuresis paracrine regulation of fibrosis
local regulation of vascular tone bone development
2.2 Cellular mechanisms of myocardial remodelling
2.2.1 Hypertrophic growth and gene expression of cardiac myocytes
Although recent studies have suggested the existence of a small subpopulation of replicating myocytes, adult ventricular myocytes are considered to be terminally differentiated cells that have withdrawn from the cell cycle during the perinatal period.

27
Instead of mitosis, the primary response of the myocyte to increased workload is cellular hypertrophy, which can be defined as an increase in the content of cellular components in the absence of cell division. (Sugden & Clerk 1998a.) Indeed, the hallmark of cardiac hypertrophy is an increase in the size of the myocytes compared with normal cells (Dorn et al. 2003). The two macroscopic types of cardiac hypertrophy, concentric and eccentric, differ in terms of the cellular features of cardiomyocyte hypertrophy, the former being characterised by an increase in myocyte cross-sectional area relative to cell length and the latter by an increase in myocyte length relative to cross-sectional area (Gerdes et al. 1988, Campbell et al. 1989, Campbell et al. 1991, Sugden & Clerk 1998a).
The hypertrophic growth of the cardiomyocyte is a result of an accumulation of total cellular protein, increased sarcomerogenesis and myofibrillar assembly (Dorn et al. 2003, Sugden & Clerk 1998a). An increase in the rate of cardiomyocyte protein synthesis was originally reported in the isolated guinea-pig heart, as shown by radioactive amino acid labelling and confirmed in various experimental setups thereafter (Schreiber et al. 1970, Swynghedauw 1999). Later studies have also indicated that not only is cardiomyocyte hypertrophy the result of an increase in non-specific protein synthesis, but the profile of contractile protein expression is selectively modulated. The sarcomere consists of thick and thin filaments that are organised into contractile units. The thick filament is composed of myosin and C-protein molecules, and the myosin molecules of a pair of myosin heavy chains (MHC) and two different pairs of myosin light chains (MLC). The rat heart contains three isomyosins which differ in their MHC composition. Myosin with αα-type heavy chains is predominant in the adult rat heart, while β-MHC is primarily expressed during fetal development. The expression of β-MHC is increased in response to haemodynamic overload, and a molecular shift from αα-MHC to ββ-MHC is observed. (Swynghedauw 1999.) Modifications in sarcomeric proteins other than myosin may also occur in the hypertrophied myocyte, so that haemodynamic overload is associated with up-regulation of the skeletal isoform of α-actin (α-SkA), for instance (Sugden & Clerk 1998a).
The mechanism behind the selectively altered cardiomyocyte protein expression pattern is selective up-regulation of gene expression, i.e. activation of the hypertrophic gene programme, which is a common feature of various types of hypertrophy and therefore represents an excellent marker of cardiac hypertrophy in general. In addition to up-regulation of the β-MHC and α-SkA genes, this programme includes changes in immediate early genes and in the genes for the natriuretic peptides. (Sugden & Clerk 1998a.) The first detectable change on the exposure of myocytes to hypertrophic stimuli is up-regulation of the expression of the immediate early genes c-jun, c-fos, c-myc and Egr-1. These are proto-oncogenes which primarily encode transcription factors, and their expression in cardiomyocyte hypertrophy is generally considered transient, as their levels may return to baseline within hours after the onset of hypertrophic stimulation. (Komuro et al. 1990, Sadoshima et al. 1992.) The longer-term genetic response in cardiomyocyte hypertrophy is the recapitulation of fetal genes, including the above mentioned β-MHC and α-SkA genes, and genes encoding cardiac muscle α-actin and ventricular MLC-2 (Sugden & Clerk 1998a).
It became evident soon after characterisation of ANP and BNP that the altered expression profile of their genes is a part of the hypertrophic gene expression pattern. The expression of BNP upon hypertrophic stimulation generally shows many of the

28
characteristics of immediate early genes, while the expression of ANP is increased simultaneously with the activation of the fetal gene programme (Tokola et al. 2001). The ANP gene responds to virtually all types of hypertrophic stimulation, such as mechanical stress, pressure and volume overload, GPCR agonists and growth factors (Calderone et al. 1995, de Bold et al. 1996). BNP gene expression is increased in vitro in response to GPCR agonists and mechanical stretch in cultured cardiomyocytes, and also by atrial stretch and increased left ventricular wall stress in the isolated heart (Magga et al. 1997a, Tokola et al. 2001, Tenhunen et al. 2005), while increased BNP mRNA levels are observed in vivo in various experimental models of haemodynamic overload (Dagnino et al. 1992, Magga et al. 1994). Mechanistically, both transcriptional and post-transcriptional factors appear to mediate the up-regulation of BNP gene expression in response to hypertrophic stimulation (Nakagawa et al. 1995, Liang et al. 1997, Magga et al. 1997b, Suo et al. 2002, Tenhunen et al. 2005).
2.2.2 Apoptotic cell death
As a cause of the loss of functional contractile tissue, compensatory hypertrophy and reparative fibrosis, cell death is a critical determinant of myocardial remodelling (Swynghedauw 1999). Cell death can be classified on the basis of the pathophysiological cause, the molecular mechanism or the morphology of the cells involved. Viewed morphologically, it can occur via either necrosis or apoptosis, where cardiomyocyte apoptosis is a form of genetically controlled programmed cell death due to the activation of endogenous endonuclease. The typical morphological features of an apoptotic cell include condensation of chromatin, cell shrinkage and nuclear fragmentation, which are followed by cell fragmentation and rapid phagocytosis of apoptotic bodies by adjacent cells. (Takemura & Fujiwara 2004.)
Even though both necrosis and apoptosis occur in response to myocardial ischaemia, the major cause of cell loss during ischaemia is not necrosis but apoptosis (Kajstura et al. 1996, Swynghedauw 1999). Apoptotic cell death in response to ischaemia-reperfusion injury was originally reported by Gottlieb et al. (1994) in isolated rabbit hearts. A substantial number of apoptotic cardiomyocytes were later observed in acute ischaemia induced in vivo by coronary artery ligation within the ischaemic region (Fliss & Gattinger 1996). In humans, DNA fragmentation and apoptosis are observed in cardiomyocytes at autopsies following fatal acute myocardial infarction (Itoh et al. 1995, Saraste et al. 1997). At the mechanistic level, the causal relationship between heart failure and cardiomyocyte apoptosis was demonstrated by Wencker et al. (2003), for instance, who showed the development of heart failure in transgenic mice over-expressing pro-apoptotic caspase-8. Conversely, over-expression of anti-apoptotic Bcl-2 has recently been shown to attenuate heart failure in a rabbit model of ischaemia-reperfusion (Chatterjee et al. 2002).
An increased rate of apoptosis is observed not only during acute myocardial infarction but also during the chronic period of remodelling. In experimental models of myocardial infarction apoptotic cardiomyocytes with fragmented DNA are observed even in the remote non-infarcted regions at late time points, suggesting continuous and persistent

29
cardiomyocyte apoptosis during post-infarction remodelling (Oskarsson et al. 2000, Sam et al. 2000). In humans, apoptotic cardiomyocytes were found in samples from hearts explanted from patients with ischaemic heart failure or with idiopathic dilated cardiomyopathy (Narula et al. 1996, Olivetti et al. 1997). Furthermore, persistent and progressive loss of myocytes via apoptosis occurs in the ischaemic border zone of the infarction during the subacute stage (Baldi et al. 2002), and the rate of apoptosis is significantly reduced after recanalisation of the responsible coronary artery (Abbate et al. 2002).
Although the detailed mechanistic relationship between cardiomyocyte apoptosis and hypertrophy is not well established in vivo, several lines of evidence support a connection between these two mechanisms. A wave of apoptosis is associated with thoracic aortic banding-induced hypertrophy without heart failure (Teiger et al. 1996), and increased cardiomyocyte apoptosis is also observed in spontaneously hypertensive rats (SHR) and may be involved in the transition of left ventricular hypertrophy to ventricular dysfunction (Hamet et al. 1995, Condorelli et al. 1999). It has been proposed that hypertrophic stimuli such as mechanical forces, growth factors, cytokines or neurohormones may produce a contradictory genetic demand during the chronic phases of hypertrophy which would trigger the apoptotic process in the cardiomyocytes (Fortuno et al. 2001).
2.2.3 Neovascularisation
The vasculature comprises 35% of the volume of the myocardium. Endothelial cells are at least as susceptible to ischaemic injury as cardiomyocytes, and irreversible ischaemia is followed by a profound loss of myocardial reperfusion capacity. (Gavin et al. 1998.) Microvessel function is also impaired in the ischaemic peri-infarct region, as demonstrated, for instance, by the lack of corresponding improvements in microvascular perfusion when the coronary artery obstruction is relieved clinically (Ito et al. 1992). Both irreversible loss of myocardial vasculature and reversible microvascular dysfunction, also known as microvascular stunning, therefore contribute to the pathogenesis of post-infarction heart failure (Gavin et al. 1998).
To avoid further functional and structural impairment, the heart attempts to respond to the loss of sufficient coronary perfusion by compensatory neovascularisation (Tabibiazar & Rockson 2001, Fukuda et al. 2004). The formation of new blood vessels in the ischaemic heart consists of angiogenesis, i.e. capillary formation and the development of new vessels lacking in developed media, and arteriogenesis, the appearance of new arteries possessing a fully developed tunica media (Simons et al. 2000). In addition to these two forms of myocardial neovascularisation, vasculogenesis, de novo formation of blood vessels from progenitor cells, has been reported to occur in the ischaemic myocardium (Fukuda et al. 2004). The stimuli for myocardial angiogenesis can be classified conceptually into three broad categories: mechanical, chemical and molecular factors (Tabibiazar & Rockson 2001). The mechanical factors include both increased haemodynamic overload and shear stress. It has been shown that small vessels with a chronically increased load tend to enlarge, while large vessels with low flow show a

30
tendency to decrease in endovascular diameter (Schaper & Ito 1996). Shear stress may induce coronary angiogenesis either directly or via the up-regulation of endothelial adhesion molecules or growth factors, and also by the attraction of inflammatory cells (Tabibiazar & Rockson 2001). Tissue ischaemia per se may not be the main trigger for an angiogenic response in the ischaemic heart, but it may in turn activate the expression of several angiogenic factors and their receptors (Simons et al. 2000, Tabibiazar & Rockson 2001). The molecular triggers of myocardial angiogenesis also include multiple endothelial cell responses and alterations in various extracellular matrix proteins (Tabibiazar & Rockson 2001).
The alterations in the coronary vasculature are not restricted to post-infarction remodelling but are also observed in the hypertrophied heart without myocardial infarction. The coronary haemodynamics is impaired in chronic hypertension due to arteriolosclerosis, and the coronary reserve may be reduced to 40% in hypertrophy induced by a pressure overload (Strauer 1990, Strauer et al. 1991). While young individuals with pressure overload hypertrophy show a preserved capillary/myocyte ratio, the hypertrophied adult heart is characterised by decreased capillary density and therefore seems to fail to maintain a sufficient blood flow (Flanagan et al. 1991, Rakusan et al. 1992). Interestingly, a recent study employing transgenic mice over-expressing the Akt 1 gene demonstrated that coronary angiogenesis was enhanced during the compensatory hypertrophy but was reduced as the hearts underwent pathological remodelling, suggesting that the disruption of coordinated angiogenesis may contribute to the transition from adaptive hypertrophy to overt heart failure (Shiojima et al. 2005).
Nevertheless, the compensatory angiogenic response is insufficient under normal conditions to restore an appropriate coronary blood flow in the peri-infarct region after myocardial infarction (Angoulvant et al. 2004). Myocardial angiogenesis is therefore an emerging therapeutic target in patients who have residual symptoms or myocardial ischaemia despite maximal pharmacological and operative interventions. Intracoronary administration of FGF induced angiogenesis and attenuated post-infarction remodelling in an experimental myocardial infarction model (Rajanayagam et al. 2000). Similarly, local administration of VEGF either in an intra-coronary manner or via peri-adventitial mini-pumps was able to enhance coronary blood flow and collateralisation (Banai et al. 1994, Hariawala et al. 1996). In addition to treatment with angiogenic growth factors, myocardial angiogenesis can be achieved using cell-based therapies. Endothelial progenitor cells (EPCs), bone marrow-derived progenitor cells that express endothelial cell markers, increase angiogenesis and attenuate adverse remodelling in rat and swine models of myocardial infarction (Kawamoto et al. 2001, Kawamoto et al. 2003, Kocher et al. 2001). In addition to EPCs, the implantation of skeletal myoblasts expressing VEGF may also be angiogenic, and likewise treatment with bone marrow-derived mononuclear cells (BMD-MCs) (Fuchs et al. 2001, Kamihata et al. 2001, Suzuki et al. 2001). The relative accessibility of the heart and coronary vasculature also makes them attractive targets for angiogenic gene therapy approaches. Indeed, the gene transfer of angiogenic growth factors has been studied in several preclinical models (Ylä-Herttuala & Alitalo 2003). Direct adenoviral gene transfer of VEGF encoding complementary DNA (cDNA) enhanced collateralisation and myocardial perfusion in a porcine model (Mack et al. 1998), while post-infarction treatment of mice with an adenoviral vector over-expressing hepatocyte growth factor (HGF) also attenuated adverse left ventricular

31
remodelling (Li et al. 2003), and beneficial effects have also been reported with gene transfer delivery of VEGF and HGF via the implantation of transfected cardiomyocytes (Miyagawa et al. 2002, Yau et al. 2001). The effects of VEGF and FGF have also been studied in phase I and early phase II clinical trials, but the results have been controversial and the final clinical applicability of the experimental observations remains to be elucidated (Laham et al. 1999, Hedman et al. 2003, Henry et al. 2003, Ylä-Herttuala & Alitalo 2003).
2.2.4 Cardiac stem cells
Autologous transfer of bone marrow-derived progenitor cells to infarcted hearts has been reported to have potentially beneficial effects in several experimental models, and early-phase clinical trials have also been conducted (Dimmeler et al. 2005). Recent studies have suggested, however, that progenitor cells may also be resident in the heart. The existence of adult cardiomyocytes undergoing mitosis in the failing human heart was first reported by Kajstura et al. (1998). This recognition of a small replicating subpopulation of cardiomyocytes led to the discovery of their founders, cardiac stem cells (CSCs) (Beltrami et al. 2003).
CSCs were originally identified as small cardiac cells distributed throughout the ventricular and atrial myocardium and expressing the common stem cell markers c-kit, Sca-1 and MDR as well as the myocyte-specific transcription factors GATA-4, Nkx-2.5 and myocyte enhancer factor 2 (MEF-2). CSCs were shown in vitro to be self-renewing, clonogenic and multipotent, giving rise to three cell types: myocytes, smooth muscle cells and endothelial cells. (Beltrami et al. 2003.) Given these findings, the functional significance of CSCs in myocyte renewal and myocardial remodelling is currently a major area of research interest. So far, intravenously administered Sca-1-positive CSCs have been shown to home to the injured myocardium after reversible ischaemia injury in mice, constituting 5% of the myocytes in the left ventricle 2 weeks after grafting (Oh et al. 2003). Furthermore, c-kit-positive CSCs injected into the border zone of a new infarction in a rat model were able to regenerate functional myocardium (Beltrami et al. 2003). In humans, increased CSC growth and senescence have been reported in ischaemic heart failure and cardiac hypertrophy (Urbanek et al. 2003, Urbanek et al. 2005).
2.2.5 Myocardial fibrosis
In the context of myocardial remodelling, fibrosis is considered either reparative or reactive. Extensive reparative fibrosis and collagen deposition are observed as a compensatory phenomenon in post-infarction remodelling. Transient collagen degradation in the infarcted area is triggered by matrix metalloproteinases after myocardial infarction, but this is rapidly followed by reparative fibrosis and organised scar formation, a complex process initiated by the formation of a fibrin-fibronectin matrix preceding collagen synthesis and fibroblast transformation and regulated by various

32
cytokines, including TGF-β1, and vasoactive peptides. (Swynghedauw 1999, Sutton & Sharpe 2000.) Fibrosis occurs during both early and late post-infarction remodelling, and a definitively constituted scar composed of 40% type I collagen, 35% type III and 25% type V is observed as late as some weeks after myocardial infarction (Swynghedauw 1999). The non-infarcted area is equally affected by reactive fibrosis after myocardial infarction, since increased collagen deposition has been reported in both the non-infarcted left ventricle and the right ventricle (Cleutjens et al. 1995).
Reactive fibrosis is observed in hypertensive heart failure and in the late phases of hypertrophic transformation as well. At the level of hypertrophic stimulation, pressure and volume overload are known to increase myocardial fibrosis. Collagen mRNA levels increase rapidly in response to a pressure overload, and increased fibrosis has been documented in several models of chronic pressure overload. Fibrosis may be a direct consequence of cardiac overload, related to neurohumoral responses or the local production of vasoactive peptides. (Swynghedauw 1999.) Angiotensin II induces massive fibrosis in both the left and right ventricles in vivo, and it is able to increase collagen synthesis directly in isolated fibroblasts (Brilla et al. 1990, Brilla et al. 1994). ET-1 increases collagen synthesis and fibroblast proliferation, and fibrosis occurs in response to aldosterone treatment when high sodium levels are present (Guarda et al. 1993, Young et al. 1995, Swynghedauw 1999).
Functionally, myocardial fibrosis has three major adverse consequences. First, the increased extracellular matrix promotes mechanical stiffness and thereby contributes to diastolic dysfunction. Second, a fibrotic heart may be more prone to arrhythmias, as the increased collagen content disrupts the electrotonic connectivity between the myocytes. Finally, perivascular fibrosis surrounding coronary arterioles may impair myocyte oxygen availability. (Brown et al. 2005.)
2.2.6 Inflammation
Inflammation and cytokine elaboration are integral components of the host response to tissue injury. An inflammatory response is present at both the acute and chronic stages of myocardial remodelling. Among the well-characterised inflammatory mediators of remodelling are the pro-inflammatory cytokines interleukin-6 (IL-6), tumour necrosis factor α (TNF-α) and IL-1β. (Nian et al. 2004.)
Although pro-inflammatory cytokines are not constitutively expressed in the myocardium, virtually all the nucleated cell types in the myocardium are able to up-regulate their synthesis upon stress stimuli such as myocardial infarction (Mann 2003). Indeed, up to 50-fold increases in IL-6, TNF-α and IL-1β expression levels can be observed in the infarcted area within one day of the onset of myocardial infarction (Deten et al. 2002, Irwin et al. 1999). The up-regulation of cytokine expression is not specific to myocardial infarction, however, since increased cytokine levels are observed in response to mechanical stress or pressure overload and in acute myocarditis, for instance. Altogether, it appears that the heart possesses an innate cytokine response system which is activated by various stress stimuli. (Wilson et al. 2004.)

33
The acute inflammatory response has a dual role in early post-infarction remodelling. Depending on the conditions, the pro-inflammatory cytokines may promote myocyte hypertrophy or apoptosis, or affect cardiac contractility (Nian et al. 2004). TNF-α, in particular, has been reported to have paradoxal effects on cardiomyocyte survival and apoptosis (Engel et al. 2004, Higuchi et al. 2004). At the physiological level, these effects may lead to healing and restoration of cardiac function, or when unfavourable, to increased left ventricular dilatation or cardiac rupture (Nian et al. 2004).
IL-6, TNF-α and IL-1β levels begin to decrease towards baseline levels within one week of myocardial infarction, but may remain up-regulated even beyond this time when the size of the infarcted area is large, and can thus contribute to late post-infarction remodelling (Ono et al. 1998). Most notably, the effects of pro-inflammatory cytokines are also pleiotropic in late remodelling, as they may exercise a protective influence by affecting the extracellular matrix and integrins and contributing to vascular and cardiac regeneration and myocardial angiogenesis (Nian et al. 2004). Conversely, a cytokine-mediated pathogenesis for chronic heart failure has been hypothesised. Persistent inflammation and increased circulating levels of cytokines are present in heart failure patients, and by influencing heart contractility, inducing hypertrophy and promoting apoptosis, they may lead to a deterioration in cardiac function during the chronic phases of heart failure (Wilson et al. 2004, Torre-Amione 2005).
2.3 Intracellular signal transduction pathways in myocardial remodelling
The gene and protein expression patterns of the individual myocyte are altered in myocardial remodelling. These changes require signal transduction of the primary stimulus from the cell membrane to the nucleus. The cytoplasmic signal transduction network of the myocyte consists of a number of sequentally acting protein kinases and phosphatases, which transmit the signal from the cell membrane receptors to modulate transcription and translation. (Sugden & Clerk 1998a, Swynghedauw 1999.) An overview of cardiomyocyte signal transduction is provided in Figure 2.

34
Fig. 2. A schematic overview of myocyte signal transduction with special emphasis on MAPKs. Modified from Liang & Molkentin (2003). Activation of cell membrane GPCRs, receptor tyrosine kinases and stretch-activated channels activates a complex array of intracellular signalling molecules. The signals are re-converged in MAPKs.
2.3.1 Mechanotransduction
Mechanical stress triggers molecular events in the cardiomyocyte both via direct activation of signalling molecules and through the release of humoral or paracrine factors (Force et al. 2002). Even though mechanotransduction is considered a highly conserved process, the molecular identity of the cardiomyocyte mechanosensors is unknown and the detailed mechanisms by which the primary mechanical stimulus is converted to biochemical cellular signals remain poorly understood (Knöll et al. 2003). Three major groups of molecules have been suggested to be involved in the cardiomyocyte mechanotransduction: integrins, stretch-activated channels (SACs) of the cell membrane and GPCRs (Force et al. 2002).
Integrins are heterodimeric membrane proteins that link the extracellular matrix to the cytoskeleton at focal adhesion sites. Mechanical stretch may therefore cause the integrins to transmit the signal to cytoskeletal components such as actin filaments. This process may require several intermediary molecules. (Ruwhof & van der Laarse 2000.) In addition, an alternative mechanism whereby integrins are involved in

35
mechanotransduction may exist. Focal adhesion sites are functionally associated with a collection of signalling molecules, such as focal adhesion kinase, non-receptor tyrosine kinases and Src, suggesting that mechanical stretch-activated integrins may serve as the true receptors that transmit the signal to these downstream kinases (Ruwhof & van der Laarse 2000, Force et al. 2002). Furthermore, stretch and adrenergic-mediated hypertrophic responses appear to require normal integrin signalling (Ross et al. 1998, Aikawa et al. 2002), and pressure overload induced by aortic constriction has been linked with the up-regulation of integrin expression (Babbitt et al. 2002).
The cardiomyocyte SACs are mainly K+-selective channels, Ca2+-channels and non-selective cation channels. Opening of the cardiomyocyte SACs leads to an increase in intracellular calcium content, since the Ca2+ influx from Ca2+ sensitive SACs causes Ca2+ -induced Ca2+ release. (Hu & Sachs 1997, Sadoshima & Izumo 1997.) The change in intracellular calcium homeostasis may lead to alterations in cardiac contractility, and as Ca2+ is involved in intracellular signalling in the myocyte, to the activation of several remodelling and hypertrophy-associated downstream pathways. Whether SACs are critical initiators of stress-induced myocardial remodelling remains to be determined. (Sadoshima & Izumo 1997.)
Autocrine release of endogenous angiotensin II and other paracrine substances is obviously partially responsible for cardiomyocyte mechanotransduction. A blockade of AT1 receptors with pharmacological receptor antagonists attenuated stretch-induced myocyte signal transduction and gene expression, indicating that a paracrine release of angiotensin II is required (Sadoshima et al. 1993). Even so, the involvement of angiotensin II does not exclude other parallel mechanisms, since AT1A-deficient cardiomyocytes are able to develop features of cellular hypertrophy (Kudoh et al. 1998), and pressure overload hypertrophy is observed in AT1A knock-out mice (Harada et al. 1998a, Harada et al. 1998b). In addition to angiotensin II, the paracrine effects of growth factors such as insulin-like growth factor 1 (IGF-1) and IL-6 have been suggested as being involved in stretch-induced responses (Force et al. 2002), and a blockade of endothelin receptors with bosentan was shown to attenuate stretch-induced BNP gene expression, suggesting a role for paracrine ET-1 (Magga et al. 1997a). Finally, it has been suggested that mechanical stretch per se may modulate both GPCRs and receptor tyrosine kinases without the presence of receptor agonists (Sadoshima & Izumo 1997, Force et al. 2002).
2.3.2 G proteins
The cell membrane receptors that bind extracellular ligands can be classified into three categories: GPCRs, ionic channels and tyrosine kinases (Svoboda et al. 2004). GPCRs in themselves lack catalytic activity, but initiate their actions via heterotrimeric GTP-proteins (G proteins), which are composed of two functional subunits, Gα and Gβγ. Interaction of the GPCR with an agonist induces a conformational change in the receptor molecule, which promotes the dissociation of G proteins into active Gα and Gβγ subunits, both of which are able to propagate and amplify the primary signal by interaction with the respective downstream effectors. (Rockman et al. 2002.) The downstream effectors of

36
Gα and Gβγ include adenylyl cyclases, phospholipases and ion channels, which in turn regulate the intracellular concentrations of secondary messengers such as cyclic adenosine monophosphate (cAMP), cyclic guanosine monophosphate (cGMP), diacylglycerol (DAG), phosphatidylinositol 1,4,5-trisphosphate (IP3), arachidonic acid and sodium, potassium or calcium ions (Svoboda et al. 2004).
G proteins can be classified on the basis of their subunit composition. So far, 15 α-subunit, 6 β-subunit and 12 γ-subunit variants have been cloned (Rockman et al. 2002). The α-subunits are then further divided into four groups according to their sequence homology: αs, αi, αq, and α12 (Schnabel & Bohm 1996). The G protein complexes differ from each other in terms of their affinity to downstream effectors (Fig. 2), so that the stimulation of Gαs, for example, primarily activates adenylyl cyclase to produce cAMP, while the stimulation of Gαq leads to the generation of IP3 and DAG by phospholipase C (PLC) (Rockman et al. 2002). The primary intracellular downstream target of cAMP is protein kinase A (PKA), while DAG preferentially activates protein kinase C (PKC) isoforms. IP3, in turn, regulates intracellular calcium homeostasis (Schnabel & Bohm 1996).
Angiotensin II, ET-1 and the sympathetic nervous system initiate their intracellular actions via GPCRs (Arai et al. 1990, Kim & Iwao 2000, Schrier & Abraham 1999). G proteins are also involved in the cardiac stretch response, Gαi and Gαq being activated within seconds of mechanical stretch in cardiac fibroblasts (Gudi et al. 1998), while Gαs and Gαi are involved in the regulation of myocardial contractility via cAMP, PKA and phospholamban (Molkentin & Dorn 2001). Transgenic mice over-expressing Gαs showed enhanced cardiomyocyte hypertrophy and apoptosis as well as increased myocardial fibrosis (Iwase et al. 1996, Geng et al. 1999). Gαi expression, for its part, is increased in experimental models of cardiac hypertrophy and heart failure (Marzo et al. 1991, Bohm et al. 1992), and up-regulation of Gαi is also observed in heart failure patients (Neumann et al. 1988).
The role of Gαq has been most intensively studied in experimental models of cardiac hypertrophy. GPCR agonists activating Gαq are widely used to stimulate the hypertrophic growth of cardiac myocytes in vitro (Sugden & Clerk 1998a). Over-expression of heart-specific Gαq in transgenic mice in vivo resulted in a phenotype with features of both compensated and decompensated hypertrophy (D'Angelo et al. 1997), and superimposition of a pressure overload on Gαq over-expression caused a rapid development of eccentric hypertrophy and functional decompensation (Sakata et al. 1998). Over-expression of dominant negative Gαq, on the other hand, is able to attenuate pressure overload hypertrophy (Akhter et al. 1998). Finally, expression of Gαq has been reported to be increased in the peri-infarct region after experimental myocardial infarction in rats (Ju et al. 1998).
2.3.3 Small G proteins
The small G protein family consists of 5 subfamilies of approximately 21 kDA proteins, Ras, Rho, ADP ribosylation factors (ARFs), Rab and Ran. The role and expression of ARFs, Rab and Ran within the heart are unknown, whereas those of the Ras and Rho

37
subfamilies have been studied in several experimental models. The small G protein subfamilies can be further classified into subclasses, the Rho group consisting of RhoA, Rac1 and Cdc42, and the Ras group consisting of Ras, Rap and Ral. (Clerk & Sugden 2000.)
The hypertrophic agonists ET-1, angiotensin II and phenylephrine (PE) activate Ras via their GPCRs (Fig. 2) (Clerk & Sugden 2000). The upstream mechanisms that connect the GPCRs with Ras remain partially unknown, although a PKC-dependent mechanism has been suggested (Chiloeches et al. 1999). Unlike the heterotrimeric G proteins, the Ras group of small G proteins is activated not only by GPCRs but also by the receptor protein tyrosine kinases and integrins (Sugden & Clerk 2000, Sugden 2003). The downstream effectors of Ras include phosphoinositide 3-kinase (PI3K), c-Raf, Ral-GDS and PLCε (Sugden 2003). In addition, Ras activates all the MAPKs (Fig. 2) (Molkentin & Dorn 2001). The activation and mechanisms of Rho signalling are less well characterised than those of Ras, but it is known that treatment with ET-1 and PE activates both Rac1 and RhoA (Clerk & Sugden 2000, Clerk et al. 2001). Interestingly, the downstream Rho-dependent kinase p160ROCK is rapidly activated by pressure overload in the intact heart (Torsoni et al. 2003). The main downstream effectors of RhoA are Rho kinase (ROKα or ROCK2) and the related kinase p160ROCK, which further activate the downstream kinases, including MAPKs (Clerk & Sugden 2000, Galaria et al. 2004). Rac may activate MAPK cascades either directly by phosphorylating MEKs or via c-Raf (Clerk et al. 2001).
Considerable indirect evidence concerning the role of small G-proteins in cardiovascular pathophysiology has been obtained using selective Rho kinase inhibitors such as Y-27632 and fasudil. ET-1-induced hypertrophy is attenuated by Y-27632 in cultured cardiomyocytes (Kuwahara et al. 1999), and the long-term inhibition of Rho kinase by fasudil suppresses angiotensin II-induced hypertrophic changes in cardiomyocytes and vascular smooth muscle cells in vivo (Higashi et al. 2003). Furthermore, the inhibition of Rho kinase by fasudil is able to attenuate post-infarction remodelling and monocrotaline-induced pulmonary hypertension in rats (Abe et al. 2004, Hattori et al. 2004). Interestingly, HMG CoA reductase inhibitors also affect the small G-proteins, and it has been suggested that they may attenuate cardiac hypertrophy via Rac1 and Rho A inhibition (Laufs et al. 2002). Experiments performed using dominant negative and activated forms of small G-proteins have provided further insights into the ir functional role. Microinjection of activated Ras increased ANP gene expression (Thorburn et al. 1993), and constitutively active Ras induced the hypertrophy associated with enhanced ANP, BNP, α-SkA and β-MHC transcription (Thuerauf & Glembotski 1997, Fuller et al. 1998). Conversely, dominant negative Ras inhibited hypertrophic gene expression and protein synthesis (Abdellatif et al. 1998). The over-expression of Ras in transgenic mice induced a hypertrophic phenotype via the activation of c-jun N-terminal kinase (JNK) (Hunter et al. 1995, Ramirez et al. 1997). The over-expression of activated Rac-1 has induced myocyte hypertrophy both in vitro and in vivo (Pracyk et al. 1998, Sussman et al. 2000), while activated RhoA stimulated hypertrophic gene expression in cardiomyocytes (Sah et al. 1996), but resulted in an in vivo phenotype with atrial enlargement and conduction defects rather than in hypertrophy (Sah et al. 1999).

38
2.3.4 Protein kinase C
The protein kinase C family comprises twelve serine/threonine kinases which form three subgroups on the basis of their activation characteristics. The subgroup of conventional, i.e. classical, PKCs includes isozymes α, β1, β2, and γ, which are activated by phosphatidylserine, DAG and Ca2+. (Malhotra et al. 2001, Vlahos et al. 2003.) The novel PKCs (δ, ε, θ, η, and μ) are activated by DAG but not Ca2+, and the atypical PKCs (ι, ζ and λ) by distinct lipids (Vlahos et al. 2003, Braz et al. 2004). Cardiomyocytes express α, β, δ, ε, μ, ζ, ι, and λ, PKCα being the predominant isoform (Mackay & Mochly-Rosen 2001).
The multiplicity of PKC family members produces variable cellular and physiological responses in the heart depending upon the isoform activity and physiological context. The activity of any given PKC isoform is dependent on three factors: expression, localisation within the cell and phosphorylation state (Dorn & Force 2005). The downstream molecular targets of the PKC isoforms that have been identified so far include troponin I, MAPKs, Akt, caveolae proteins, L-type calcium channels, sarcoplasmic reticulum Ca2+-ATPase 2 (SERCA-2) and many other transcription and translation-related proteins (Ping 2003).
The functional roles of PKCα, PKCβ, PKCδ, and PKCε have been studied in the context of cardiovascular pathophysiology, while those of PKCμ, PKCζ, PKCι, and PKCλ remain obscure (Mackay & Mochly-Rosen 2001, Vlahos et al. 2003). The initial studies of neonatal rat cardiomyocytes showed that PKCα is activated by hypertrophic stimuli such as norepinephrine, and that over-expression of PKCα induces hypertrophic growth associated with increased ANP gene expression and activation of the extracellular signal-regulated kinase (ERK) cascade (Disatnik et al. 1994, Braz et al. 2002). In the context of PKCα activation, the in vivo findings are consistent with those obtained in vitro, since PKCα is up-regulated in response to pressure overload and myocardial infarction (Simonis et al. 2002, Bayer et al. 2003). Functionally, the results regarding the role of PKCα seem to differ between the adult heart and cultured cardiomyocytes, since transgenic mice over-expressing PKCα do not show features of cardiac hypertrophy but instead diminished contractility, suggesting that PKCα may affect the propensity for heart failure (Braz et al. 2004). PKCβ is up-regulated in human heart failure and in diabetes mellitus (Dorn & Force 2005). Transfection of myocytes with constitutively active PKCβ1 in vitro induces hypertrophic gene expression (Kariya et al. 1991), while the effects of PKCβ over-expression in vivo appear to be dependent on the quantitative level of over-expression and the experimental model used (Vlahos et al. 2003). Over-expression of PKCβ2 under the α-MHC promoter results in cardiac hypertrophy and subsequent heart failure accompanied by increased expression of c-fos, ANP and β-MHC (Wakasaki et al. 1997), whereas lower levels of PKCβ over-expression are associated with mild hypertrophy with impaired diastolic relaxation (Bowman et al. 1997). On the other hand, the hypertrophic response is not attenuated in PKCβ knock-out mice (Roman et al. 2001), indicating that PKCβ involvement is not a prerequisite for the development of cardiac hypertrophy.
It has been suggested that PKCδ may have a more significant role in myocardial ischaemia and infarction than in cardiac hypertrophy. Its expression is increased in rat

39
hearts coincidently with the development of heart failure (Simonis et al. 2002), and it has been shown to mediate cardiomyocyte apoptosis in response to ischaemia-reperfusion injury (Murriel et al. 2004). On the other hand, a pro-hypertrophic role has been suggested for PKCδ in transgenic models that modify its translocation (Dorn & Force 2005). In contrast, the role of PKCε has been more extensively studied in cardiac hypertrophy, although its relative involvement in adaptive and maladaptive hypertrophy is somewhat controversial. Mechanical stress, over-expression of Gαq and pressure overload are known to activate PKCε and the over-expression of PKCε in cultured cardiomyocytes is sufficient to induce hypertrophic gene expression, although not a hypertrophic phenotype (D'Angelo et al. 1997, Strait et al. 2001, Dorn & Force 2005). Transgenic PKCε mice develop adaptive hypertrophy (Takeishi et al. 2000, Dorn & Force 2005), but knock-out PKCε mice do not exhibit any basal cardiac phenotype (Khasar et al. 1999). PKCε may be cardioprotective in ischaemic preconditioning (Qiu et al. 1998).
2.3.5 Mitogen-activated protein kinases
MAPKs represent one of the most conserved and widespread mechanisms of cellular signal transduction, as all eukaryotic cells possess multiple MAPK pathways (Kyriakis & Avruch 2001). All MAPKs share several common biochemical features. First, each MAPK cascade consists of a similar three-kinase module: a MAPK kinase kinase (MAPKKK, MEKK or MKKK), a MAPK kinase (MAPKK, MEK or MKK), and a MAPK. Activation of such a cascade is initiated by the activation of MAPKKK, which is followed by phosphorylation of MAPKK, leading to phosphorylation of the terminal MAPK. Second, in addition to the common three-kinase module, all MAPK pathways share common organisation features with respect to their regulation mechanisms. The integrities of all MAPK pathways are regulated by scaffold proteins, which are partially responsible for the ability of MAPKs to distinguish the specificity of the extracellular stimuli. Furthermore, the mechanism of activation of all MAPKKKs includes three key phenomena: membrane recruitment, oligomerisation and phosphorylation. Finally, the MAPKs have similar mechanisms of action: all MAPKs are proline-directed serine/threonine kinases, i.e. they preferentially initiate their actions by phosphorylating serine or threonine residues having proline at their immediate COOH terminal site. (Kyriakis & Avruch 2001, Ravingerova et al. 2003.)
MAPKs are classified into subfamilies based on their sequence homology and the mechanism of their activation (Kyriakis & Avruch 2001). The first mammalian MAPK pathway to be identified was the ERK cascade (Cooper et al. 1982, Ray & Sturgill 1988). This was followed by the identification of two parallel MAPK pathways, the p38 and c-jun N-terminal kinase pathways (Kyriakis & Avruch 1990, Han et al. 1994). In view of their modes of activation, the ERK cascade is also referred to as insulin/mitogen-regulated kinase and p38 and JNK as stress-responsive MAPKs. ERK, p38, JNK are encoded by different genes and have different amino acid activation motifs (Kyriakis & Avruch 2001). At least two additional MAPK subfamilies, ERK5/big MAPK 1 (BMK1) and ERK 3/4, are known (Boulton et al. 1991, Zhou et al. 1995). The properties of the main MAPK families are summarised in Table 2.

40
Table 2. Properties of MAPKs.
p38 MAPK ERK 1/2 JNK Molecular mass in SDS-PAGE
p38 kDA 44/42 kDA 46/54 kDA
Phosphorylation motif Thr-Gly-Tyr Thr-Glu-Tyr Thr-Pro-Tyr Upstream MKK MKK3/6 MKK 1/2 MKK4/7 Upstream MKKK unknown MKKK1-3
Raf MKKK1-2
Downstream targets ATF-2, ATF-6, AP-1, SRF, MEF-2, Elk-1 NF-κB, MAPKAPK-2, MAPKAPK-3, PRAK, Mnk1, Mnk2
Elk-1, phospholipase A2, MAPKAPK-l, p90 S6 RSK
c-Jun, ATF-2
The three main MAPK pathways, p38, ERK and JNK, respond to a variety of extracellular stimuli, including cellular stress stimuli, such as ischaemia, osmotic shock and radiation, hormones and growth factors acting through receptor protein tyrosine kinases or GPCRs. The central role of the main MAPK subfamilies in cellular signal transduction is further emphasised by their ability to regulate an extraordinarily wide array of fundamental cellular processes. Depending on the cell type and stimulus, MAPKs may affect transcription, protein synthesis, the cell cycle machinery, cell death and differentiation. (Kyriakis & Avruch 2001.) As the myocyte loses its capacity for division and differentiation after birth, the function of MAPKs in the heart is especially targeted at transcriptional events, stress response and cell death (Ravingerova et al. 2003).
2.3.5.1 p38 MAPK
p38 MAPK was originally identified as a 38-kDa polypeptide that underwent tyrosine phosphorylation in response to osmotic shock and endotoxin treatment (Han et al. 1994, Kyriakis & Avruch 2001). Four mammalian p38 MAPK isoforms have been described so far, p38α, p38β, p38γ and p38δ. The major cardiac isoform appears to be p38α, since p38β has been reported to be non-detectable in both the human and rodent heart and p38γ and p38δ show low transcript levels as well (Sugden & Clerk 1998b, Lemke et al. 2001, Liao et al. 2001).
p38 MAPKs are generally considered to respond poorly to mitogenic stimuli but strongly to pro-inflammatory cytokines, TNF-α, IL-1, heat stress, osmotic shock and metabolic inhibitors. The activation of p38 MAPK requires phosphorylation of the Thr-Gly-Tyr motif of the p38 protein, and its threonine phosphorylation is specifically regulated by two upstream MKKs, MKK3 and MKK6 (Fig. 3). These show some degree of preference with respect to the p38 MAPK isoforms, MKK3 primarily phosphorylating p38α and p38γ while MKK6 is able to activate p38α, p38β and p38γ. (Ravingerova et al. 2003.) In contrast to the MKKs, the MKKKs regulating the primary activation of the p38 cascade remain poorly understood, although it has been suggested that certain members

41
of the Ras superfamily, Src and ASK1, may be located upstream of p38 MAPK (Fig. 2) (Sugden & Clerk 1998b, Kyriakis & Avruch 2001, Aikawa et al. 2002). The complexity of the upstream mechanisms affecting p38 MAPK activity is further highlighted by the ability of mixed-lineage kinases (MLKs) to activate both p38 and JNK cascades (Gallo & Johnson 2002).
Within the cardiomyocytes, p38 MAPK is activated in response to GPCR agonists, PE, ET-1 and angiotensin II (Sugden & Clerk 1998b). Mechanical stretch and electrical pacing in cultured cardiomyocytes and stretching in the isolated perfused heart will increase p38 MAPK phosphorylation (Hines et al. 1999, Liang & Gardner 1999, Takeishi et al. 2001). Ischaemia and ischaemia-reperfusion injury in vitro, originally reported by Bogoyevitch et al. (1996), are powerful activators of p38 MAPK (see also Ravingerova et al. 2003). The stimuli that activate p38 MAPK in vivo have been less extensively studied, but consistent with the in vitro studies, isoproterenol and angiotensin II increase its activity (Zhang et al. 2004, Zhang et al. 2005). Pressure overload resulting from aortic banding also activates p38 MAPK and its downstream kinases, as does reversible ischaemia-reperfusion injury (Fischer et al. 2001, Kaiser et al. 2004). Hypertensive rats also show increased p38 MAPK activity during the development of left ventricular hypertrophy (Behr et al. 2001). While it seems that the findings regarding p38 MAPK activation in response to acute ischaemia and pressure overload are consistent, the activity of p38 MAPK in heart failure is highly controversial. Three studies have so far demonstrated decreased p38 MAPK activity in human heart failure (Lemke et al. 2001, Communal et al. 2002, Takeishi et al. 2002), two have suggested activation (Cook et al. 1999, Haq et al. 2001) and one has demonstrated an increase in p38 MAPK activity after mechanical unloading of the hypertrophied heart by a left ventricular assist device (Flesch et al. 2001). The down-regulation of p38 MAPK in heart failure is nevertheless supported by experimental observations on SHRs in the phase of decompensated hypertrophy (Behr et al. 2001, Kacimi & Gerdes 2003). Taken together with the fact that the activation of p38 MAPK in most experimental models is rapid and transient in nature, it appears that its activity is dynamically regulated and can be either increased or decreased in cardiovascular diseases.
Fig. 3. Regulation of p38 MAPK activity in the heart. p38 MAPK is activated by stress stimuli, ischemia and GPCR agonists. MKKKs regulating p38 MAPK pathway remain largely unknown.
p38 MAPK
MKKK
Stress, GPCR agonists, electricalpacing, ischemia-reperfusion injury
MKK3/6
p38 MAPK
MKKK
Stress, GPCR agonists, electricalpacing, ischemia-reperfusion injury
MKK3/6

42
p38 MAPK activates multiple downstream targets, including transcription factors and other kinases, by phosphorylating their serine/threonine residues (Table 2). The transcription factors regulated by p38 MAPK in vitro include activating transcription factor (ATF) 2, ATF-6, activator protein 1 (AP-1), serum response factor (SRF), MEF-2, Elk-1 and nuclear factor κB (NF-κB). Other kinases that have been reported to be sensitive to p38 MAPK are MAPK activated protein kinases 2 and 3 (MAPKAPK-2 and MAPKAPK-3), p38-regulated/activated kinase (PRAK), Mnk1 and Mnk2 (Kyriakis & Avruch 2001). At the level of cardiac gene expression in vitro, p38 MAPK activation has been reported to be involved in the regulation of ANP, BNP, α-SkA, Na+-Ca2+ exchanger (NCX), glucose transporter GLUT4 and cyclo-oxygenase 2 (COX-2) gene expression (Zechner et al. 1997, Thuerauf et al. 1998, Liang & Gardner 1999, Degousee et al. 2003, Montessuit et al. 2004, Xu et al. 2005).
Based on findings in cultured cardiomyocytes, p38 MAPK was originally considered a pro-hypertrophic kinase (Table 3). Over-expression of constituvively active MKK3 or MKK6 induces cardiomyocyte hypertrophy associated with increased ANP gene expression (Nemoto et al. 1998, Wang et al. 1998). Conversely, the specific small molecule p38 inhibitors SB203580 and SB202190 attenuate agonist-induced cardiomyocyte hypertrophy and gene expression, as does inhibition of p38 MAPK activity by dominant negative p38 isoforms (Zechner et al. 1997, Nemoto et al. 1998, Wang et al. 1998). A few opposite findings have been reported in cultured cardiomyocytes, however, suggesting, for example, that early p38 inhibition is insufficient to completely inhibit the morphological changes in the myocyte in ET-1 or PE-induced hypertrophy (Clerk et al. 1998). The evidence obtained with transgenic models has nevertheless revealed that the in vivo role of p38 MAPK in cardiac hypertrophy is more complex. A pro-hypertrophic in vivo role for p38 MAPK was originally suggested by Behr et al., who demonstrated a significant attenuation of hypertensive end-organ damage following treatment with the p38 MAPK inhibitor SB239063 (Behr et al. 2001). Confusingly, none of the studies using transgenic models has so far confirmed this hypothesis (Table 3). Transgenic mice with targeted over-expression of constitutively active MKK3 or MKK6 exhibit increased interstitial fibrosis and expression of ANP, β-MHC and α-SkA, but virtually no signs of cardiomyocyte hypertrophy. At the functional level, MKK3 transgenic animals developed a phenotype of dilated cardiomyopathy characterised by increased end-systolic chamber volumes and thinned ventricular walls, whereas hearts over-expressing MKK6 had reduced end-diastolic chamber size without myocyte atrophy. (Liao et al. 2001.) Furthermore, cardiac-specific dominant-negative p38α, MKK3 and MKK6 transgenic mice showed enhanced myocardial hypertrophy in response to aortic banding or treatment with hypertrophic agonists (Braz et al. 2003), and cardiac-specific p38α knock-out mice developed massive fibrosis in response to pressure overload (Nishida et al. 2004).
Considerable attention has been focused on p38 MAPK in the context of ischaemia-reperfusion injury. Most in vitro studies have favoured the hypothesis that p38 MAPK activation is detrimental in the presence of ischaemia-reperfusion injury (Ravingerova et al. 2003). Pharmacological inhibition of p38 MAPK activity during ischaemia-reperfusion has been shown to enhance post-ischaemic recovery of cardiac function and cell survival, delay the development of infarcts and reduce apoptosis (Ma et al. 1999, Barancik et al. 2000, Schneider et al. 2001). Numerous opposite findings have also been

43
reported in this context, however, suggesting that p38 MAPK inhibition either fails to affect the extent of ischaemia-reperfusion injury or even increases it (Ravingerova et al. 2003). The protective role of p38 MAPK is further supported by in vitro studies suggesting that it may act as a mediator of ischaemic preconditioning (Sato et al. 2000). A similar amount of controversy appears to underlie the in vivo results obtained with transgenic models of ischaemia-reperfusion injury. Transgenic mice expressing dominant negative mutants of p38α or MKK6 were reported to be protected from ischaemia-reperfusion injury via anti-apoptotic mechanisms (Kaiser et al. 2004), but equal signs of functional recovery and protection were later observed in response to MKK6 over-expression (Martindale et al. 2005).
Table 3. Functional effects of p38 MAPK in different experimental models.
Model Main finding Reference Over-expression of constitutively active MKK3 and MKK6 in cultured cardiomyocytes
Cardiomyocyte hypertrophy, increased hypertrophic gene expression
Wang et al. 1998
Pharmacological inhibition of p38 MAPK in cultured cardiomyocytes
Inhibition of cardiomyocyte hypertrophy
Zechner et al. 1997 Nemoto et al. 1998
Pharmacological inhibition of p38 MAPK in hypertensive rats
Attenuation of hypertensive end-organ damage
Behr et al. 2001
Over-expression of constitutively active MKK3 in transgenic mice
Dilated cardiomyopathy and thinned ventricular walls
Liao et al. 2001
Over-expression of constitutively active MKK6 in transgenic mice
Reduced end-diastolic chamber size without myocyte atrophy
Liao et al. 2001
Aortic banding in dominant-negative p38α, MKK3 and MKK6 transgenic mice
Enhanced hypertrophic response Braz et al. 2003
Pressure overload in cardiac-specific p38α knock-out mice
Enhanced fibrosis and cardiac dysfunction
Nishida et al. 2004
Ischemia-reperfusion in dominant negative p38α and MKK6 mice
Protection from ischemia-reperfusion injury
Kaiser et al. 2004
Ischemia-reperfusion in MKK6 over-expressing mice
Protection from ischemia-reperfusion injury
Martindale et al. 2005
The detailed cellular mechanisms whereby the effects of p38 MAPK are mediated in cardiovascular pathology remain obscure, and it may therefore be these that are responsible for the controversial results obtained with different experimental models. Besides its effects on the hypertrophic growth of myocytes, p38 MAPK has been shown be involved in cardiomyocyte apoptosis, p38α having originally been reported to be the pro-apoptotic isoform (Wang et al. 1998). Processes in the extracellular matrix may also be involved, as demonstrated by the findings regarding fibrosis in p38 MAPK transgenic models (Liao et al. 2001). Finally, p38 MAPK may directly affect cardiac function, since it has been shown to confer a negative inotropic effect on cultured cardiomyocytes (Liao et al. 2002). Notably, the p38 isoforms may have differential effects on other cellular events as well as apoptosis, and the ability of upstream kinases to preferentially activate different isoforms may partially account for the persistent controversy.

44
2.3.5.2 Extracellular signal-regulated kinase
The mammalian cell expresses five isoforms of extracellular signal-regulated kinase, ERK 1-5. Among these, ERK 1/2, also known as p44/42 MAPK, is the most abundantly expressed isoform within the cardiomyocytes. ERK 1/2 is specifically activated through phosphorylation of the Thr-Glu-Tyr motif by the upstream kinase MEK 1/2, which is activated by several MAPKKKs, including MAPKKK1-3, and Raf, which is activated by Ras, PKC and Src. (Sugden & Clerk 1998c.)
Originally reported to be activated by mitogenic stimuli and growth factors via tyrosine kinases and GPCRs, the ERK 1/2 cascade is activated by a variety of stimuli in cardiomyocytes. These stimuli partially resemble those activating p38 MAPK, as hypertrophic GPCR agonists, ET-1 and PE as well as mechanical stretch of the myocytes will stimulate the ERK cascade. The paracrine and hormonal activators of ERK 1/2 include a wide array of factors that affect cytokine receptors or receptor protein tyrosine kinases, such as cardiotrophin-1, interferon-γ, TNF-α, FGF, IGF-1 and insulin. (Michel et al. 2001, Ravingerova et al. 2003.) Receptor-independent activation has been shown by phorbol ester, for example, which directly activates PKC (Zou et al. 1996). In addition, osmotic shock and hypotonic cell swelling activate ERK 1/2 in vitro (Michel et al. 2001), while ERK in the intact heart is activated by ischaemia-reperfusion but not by ischaemia alone (Mizukami & Yoshida 1997, Omura et al. 1999). Activation by mechanical stretch has also been observed in the isolated heart (Takeishi et al. 2001, Domingos et al. 2002), and in vivo studies have confirmed activation by CPCR agonists and pressure overload (Pellieux et al. 2000, Rapacciuolo et al. 2001).
Like p38 MAPK, ERK 1/2 is the converging point of a system of signal transduction that regulates a large number of downstream targets. Among the well-characterised targets are transcription factor Elk-1 and cytoplasmic phospholipase A2, but ERK 1/2 has also been reported to phosphorylate the downstream kinases MAPKAPK-1 and ribosomal p90 S6 kinase (RSK) (Ravingerova et al. 2003). RSK, in turn, regulates a variety of downstream effectors, including NF-κB, glycogen-synthase kinase 3β (GSK-3β), c-fos and cAMP response element-binding protein (Eldar-Finkelman et al. 1995, Frödin & Gammeltoft 1999).
ERK 1/2 is involved in hypertrophic gene expression and growth in cultured cardiomyocytes, although there is no general consensus regarding its necessity in this process (Molkentin & Dorn 2001). Anti-sense oligonucleotide inhibition of ERK 1/2 and transfection of dominant negative MEK1 attenuate PE-induced ANP gene expression (Glennon et al. 1996), and conversely, transfection of constitutively active MEK 1 increases ANP promoter activity (Gillespie-Brown et al. 1995). Treatment with the selective MEK 1/2 inhibitor PD98059 is able to partially inhibit stretch-induced BNP gene expression, but not PE-induced expression of ANP (Post et al. 1996, Liang et al. 2000). Anti-sense inhibition of ERK 1/2 is also able to attenuate the morphological features of cardiomyocyte hypertrophy (Glennon et al. 1996), and PD98059 was originally reported to reverse agonist-induced sarcomeric assembly (Clerk et al. 1998). Furthermore, treatment of cardiomyocytes with another MEK 1/2 inhibitor, U0126, and the Raf inhibitor SB-386023 has been shown to attenuate PE and ET-1-induced protein synthesis and the increase in cell size, suggesting that ERK activation is needed for a

45
hypertrophic response (Yue et al. 2000a). Nevertheless, a number of in vitro studies have concluded the opposite by showing that pharmacological inhibition of ERK 1/2 fails to inhibit the hypertrophic morphology or cytoskeletal organisation of the cardiomyocyte (Molkentin & Dorn 2001). The in vivo data concerning ERK 1/2 are limited, although gain-of-function studies in transgenic mice have provided some support for the role of ERK 1/2 in the development of concentric hypertrophy. Bueno et al. (2000) demonstrated that transgenic mice over-expressing MEK1 develop concentric hypertrophy within 12 months of age. Furthermore, these mice showed no signs of decompensation over time, but instead, were partially protected from apoptotic stimuli, suggesting that ERK 1/2 also possesses cardioprotective characteristics (Bueno et al. 2000). In contrast, even though Ras is an upstream regulator of ERK 1/2, the phenotype of Ras transgenic mice involves diastolic dysfunction rather than concentric hypertrophy (Hunter et al. 1995).
Ischaemia-reperfusion studies have mostly suggested a cardioprotective role for ERK 1/2. Its inhibition in a swine model of ischaemia-reperfusion increased the infarction size (Strohm et al. 2000), and a similar detrimental effect associated with enhanced apoptosis was observed upon ERK inhibition both in cultured neonatal cardiomyocytes and in isolated perfused rat hearts (Yue et al. 2000b). Similarly, MEK1 transgenic mice were partially protected from ischaemia/reperfusion-induced DNA laddering (Bueno et al. 2000). Finally, the anti-apoptotic effects of IGF-1 and cardiotrophin-1 may be partially mediated by ERK 1/2 (Bueno & Molkentin 2002).
2.3.5.3 JNK
The cardiac JNK family of MAPKs consists of two major isoforms, JNK1 and JNK2. Differential splicing and exon usage result in the expression of at least ten JNK isoforms in other tissues, but their presence in the heart has not been documented. JNK1 antibody recognises two proteins in the heart, 46 kDa and 54 kDA isoforms, and most reports regarding JNK in the heart refer to these two isoforms (Michel et al. 2001).
Like p38 MAPK, JNK is a stress-activated kinase, being responsive to heat shock, γ-irradiation, hyperosmolarity and reactive oxygen species (Kyriakis & Avruch 2001), and in the cardiomyocytes, too, it is mainly activated by stress stimuli such as hypoxia, reactive oxygen species, mechanical stretch, anisomycin and daunomycin. The paracrine and endocrine JNK activators include the cytokines TNF-α and leukaemia inhibitory factor, as well as angiotensin II receptors and α and β-adrenoceptors (Michel et al. 2001). The immediate upstream kinases of JNK are MKK4 and MKK7, which activate JNK by phosphorylating the Thr-Pro-Tyr motif in the activation loop domain. MKK4 and MKK7 are regulated by two upstream kinases, MEKK1 and MEKK2. The regulators of the JNK cascade upstream of MEKK1 and MEKK2 are poorly understood within the myocyte, although some evidence exists for Ras, Rac, cdc42 and Grb2 etc. in other cell types. (Garrington & Johnson 1999, Molkentin & Dorn 2001, Baines & Molkentin 2005.) G-protein dependent mechanisms are also supported by the inhibition of JNK activation in a transgenic model over-expressing a Gq inhibitor (Esposito et al. 2001). PKC inhibition together with Ca2+ chelation affects angiotensin II-induced JNK activation, but phorbol ester alone only weakly affects JNK, suggesting that it may be synergistically regulated

46
by Ca2+ and PKC (Bogoyevitch et al. 1995, Kudoh et al. 1997). On the other hand, stretch-induced JNK activation was reported to be independent of PKC or Ca2+ (Komuro et al. 1996). JNK affects cellular processes primarily by phosphorylating nuclear downstream targets. The two main targets of JNK in the cardiomyocyte are c-Jun, which is preferentially phosphorylated by JNK, and ATF-2, which is also regulated by p38 MAPK (Sugden & Clerk 1998b).
JNK is sensitive to hypertrophic stimulation in vivo, as its activity is increased in load-induced hypertrophy and in remote non-infarcted regions after experimental myocardial infarction (Li et al. 1998, Choukroun et al. 1999, Esposito et al. 2001). Ischaemia does not activate JNK in perfused rat heart or in vivo rabbit models, but ischaemia-reperfusion is associated with JNK activation (Yin et al. 1997, He et al. 1999). A similar level of confusion as with p38 activity nevertheless underlies JNK activity in cases of heart failure, since increased, decreased and unchanged activities have been reported depending on the conditions and the phase of heart failure (Cook et al. 1999, Haq et al. 2001, Takeishi et al. 2001, Communal et al. 2002).
Although the lack of specific pharmacological inhibitors has limited investigations into the functional role of JNK in cardiovascular pathophysiology in vivo, considerable evidence has been obtained from transgenic gain-of-function and loss-of-function studies. The first loss-of-function study, by Choukroun et al. (1999), suggested that the inhibition of JNK activity by dominant negative MKK4 prevents the development of aortic banding-induced pressure-overload hypertrophy, and supporting findings were obtained by crossing MEKK1 knock-out transgenic mice with Gq over-expressing mice, resulting in a significant attenuation of hypertrophy, contractile dysfunction and ANP gene expression (Minamino et al. 2002). In contrast, MEKK1 null mice failed to show a reduced hypertrophic response to aortic constriction, even though JNK activation was abolished (Sadoshima et al. 2002). Furthermore, targeted over-expression of MKK7 resulted in cardiomyopathy and early lethality without any signs of cardiomyocyte hypertrophy (Petrich et al. 2004). Even an anti-hypertrophic role for JNK has been suggested in transgenic studies, because JNK dominant negative mice were reported to have enhanced hypertrophic responses via interaction with calcineurin-nuclear factor of activated T-cells (NFAT) signalling (Liang et al. 2003).
The controversial role of JNK in cardiovascular pathophysiology does not seem to be restricted to the hypertrophic response, since evidence has accumulated regarding its role in cardiomyocyte apoptosis, where both pro-apoptotic and anti-apoptotic effects have been implicated (Baines & Molkentin 2005). Inhibition of JNK1, but not of JNK2, protected cardiomyocytes from ischaemia-induced apoptosis (Hreniuk et al. 2001), and the expression of dominant negative JNK inhibited β-adrenergic-stimulated apoptosis (Remondino et al. 2003). MEKK1 knockout mice, however, were shown to be more susceptible to cardiomyocyte apoptosis and inflammation (Sadoshima et al. 2002). The confusion regarding the role of JNK in cardiomyocyte apoptosis has been further extended by the very recent observations of Kaiser et al. (2005) suggesting that mice expressing dominant negative JNK 1/2 as well as activated MKK7 were protected from ischaemia-reperfusion induced apoptosis.

47
2.3.5.4 MAPK inactivation and MAPK phosphatases
The mechanisms of MAPK inactivation in the cardiomyocyte are less well-known than those of MAPK activation, although it is evident that inactivation is an important mechanism for regulating MAPK function. MAPKs are activated by the phosphorylation of threonine and tyrosine residues, and conversely, their inactivation occurs via dephosphorylation of the same residues. The dephosphorylation of MAPKs is mediated via specific dual-specificity (Thr/Tyr) MAPK phosphatases (MKPs), serine/threonine phosphatases and tyrosine phosphatases. (Theodosiou & Ashworth 2002.)
MKPs consist of a kinase-binding domain and a phosphatase domain, and exhibit little enzymatic activity in the absence of their physiological substrates. Thus their function is tightly coupled to MAPK activation. The MKPs are divided into three categories based on their preference for dephosphorylating tyrosine, serine/threonine or both tyrosine and threonine, and they also show specificity with respect to their substrates, p38, ERK and JNK. (Theodosiou & Ashworth 2002.) At least 9 families of MKPs with different specificities, tissue distributions, subcellular localisations and expression profiles exist. A significant role has been suggested for MKP-1 within the heart. (Bueno et al. 2001.)
The role of MKPs in cardiovascular pathophysiology remains largely unknown, but it has been suggested that they may antagonise hypertrophic gene expression and cardiomyocyte growth in vitro, in coordination with ERK inhibition (Fuller et al. 1997). Furthermore, transgenic mice expressing physiological levels of cardiac MKP-1 showed no MAPK activation, diminished developmental myocardial growth and attenuated hypertrophic responses to pressure overload or catecholamines, implying that the dephosphorylation of MAPKs by MKP-1 may be of functional importance (Bueno et al. 2001).
2.3.6 Ca2+/calmodulin-dependent protein kinase and calcineurin
Cardiac hypertrophy and heart failure are associated with altered Ca2+ signalling. Besides its well-documented role in cardiomyocyte excitation-contraction coupling, intracellular Ca2+ is involved in cardiomyocyte signal transduction via several kinases and phosphatases (Frey et al. 2000).
Intracellular Ca2+ is functionally associated with calmodulin, and most of the calcium-activated signal transduction events are regulated by Ca2+/calmodulin complexes. Among the direct targets are the Ca2+/calmodulin-dependent protein kinases (CaMKs). Several CaMK isoforms are known, the CaMKII isoforms being the most extensively studied in the heart. (Zhang & Brown 2004.) SHRs and animals with aortic constriction show increased CaMKII activity in vivo (Boknik et al. 2001, Hagemann et al. 2001, Colomer et al. 2003), whereas CAMKII is down-regulated in rats with experimental myocardial infarction (Netticadan et al. 2000). Transgenic mice over-expressing calmodulin and the CAMKIIδB isoform develop cardiac hypertrophy, suggesting a role for CAMKII in cardiac hypertrophy in vivo (Gruver et al. 1993, Zhang et al. 2002).
Calcineurin, also known as protein phosphatase 2B, is a conserved serine-threonine phosphatase that is uniquely activated by calcium-calmodulin complexes (Molkentin

48
2000a). The downstream effector of calcineurin is NFAT, which was first identified as a transcriptional regulator of T-cell IL-2 gene expression (Clipstone & Crabtree 1992, Liu et al. 1991). NFAT is controlled by calcineurin via dephosphorylation of its N-terminal serine residues, leading to translocation of NFAT to the nucleus and the activation of NFAT-dependent gene expression (Vega et al. 2003). The transcriptional effects of NFAT are mediated by direct NFAT-DNA interaction, which is strengthened by interaction with other transcription factors such as GATA-4 or MEF-2 (Bueno et al. 2002, Wilkins & Molkentin 2004).
A calcineurin-dependent transcriptional pathway in cardiac hypertrophy was identified by Molkentin et al. (1998), who established several transgenic lines expressing either activated NFATc4 or calcineurin A subunits, each of them showing variable forms of hypertrophic response depending on the type and level of transgene expression. They also demonstrated that calcineurin inhibition by cyclosporine was able to attenuate hypertrophic responses and described a pattern of NFATc4-GATA-4 interaction-dependent hypertrophic gene expression (Molkentin et al. 1998). A large number of studies have been published since then regarding the role of calcineurin in cardiovascular pathophysiology. Although the results have been relatively consistent regarding the sufficiency of calcineurin for producing hypertrophic responses, as most models with transgenic calcineurin-NFAT over-expression show signs of hypertrophic growth, no general consensus has been reached regarding the necessity for calcineurin-NFAT signalling in cardiac hypertrophy. Over 30 studies employing cyclosporine or FK-506 in in vitro or in vivo models have been published, the majority of them reporting anti-hypertrophic effects, but a considerable number of them reporting no effect of calcineurin inhibition. (Wilkins & Molkentin 2004.) Notably, cyclosporine and FK506 also have a number of systemic side effects, including nephrogenic and neurogenic toxicity as well as immunosuppression, which makes their clinical usefulness doubtful (Molkentin 2000a).
2.3.7 The PI3K - Akt pathway
The phosphoinositide 3-kinases are a conserved family of enzymes that possess both lipid and protein kinase activity. The PI3Ks are divided into three classes based on their structure and substrate specificity. Class I PI3Ks are heterodimers consisting of a regulatory subunit and a catalytic subunit (p110), and are divided into subclasses IA and IB. The class IA PI3Ks are composed of a p110α, p110β or p110δ catalytic subunit associated with a p85 regulatory subunit, whereas the single class IB member is composed of p110γ and the regulatory protein p101. (Prasad et al. 2003.) Class II PI3Ks have not been reported to be expressed in the myocardium. The functional role of the class IA subgroup consisting of p110α (referred to hereafter as PI3Kα) has so far been characterised in more detail than those consisting of p110β or p110δ. The main downstream effectors of PI3Ks are Akt isoforms. Akt has in turn two major downstream targets, GSK-3β and the mammalian target of rapamycin, mTOR. (Kis et al. 2003, Dorn & Force 2005.)
Both in vitro and in vivo studies have implicated the PI3K-Akt pathway in the regulation of cardiomyocyte growth. Pharmacological inhibition of PI3K, for example,

49
reduces PE or insulin-induced protein synthesis in cultured cardiomyocytes (Schlüter et al. 1999, Pham et al. 2000). Whole-genome knockout of PI3Kα leads to embryonic mortality in vivo, but cardiac-specific over-expression of dominant negative PI3Kα is associated with reduced cardiac growth (Shioi et al. 2000). Furthermore, transgenic mice over-expressing constituvely active PI3Kα develop concentric hypertrophy without transition to maladaptive hypertrophy (Shioi et al. 2000). The findings indicating that PI3Kα is not required for the development of pressure overload hypertrophy nevertheless conflict with these observations (McMullen et al. 2003). Contrarily, PI3Kγ, which is regulated by GPCRs, was shown to affect pressure-overload-induced myocardial remodelling (Patrucco et al. 2004). The phenotype resulting from cardiac-specific Akt over-expression is mostly similar to that of PI3Kα over-expression (Condorelli et al. 2002, Shioi et al. 2002). Akt has also been implicated in cardiomyocyte apoptosis and ischaemia-reperfusion injury, which has been shown to increase Akt activity (Mockridge et al. 2000, Vlahos et al. 2003).
Observations regarding the functional role of the PI3K-Akt pathway have recently been extended by findings concerning the downstream target GSK-3β. Unlike other kinases, GSK-3β is negatively regulated by hypertrophic stimuli and negatively regulates the hypertrophic responses (Antos et al. 2002, Hardt & Sadoshima 2002). GSK-3β regulates ET-1 and beta-adrenergic stimulation-induced cardiomyocyte hypertrophy negatively in vitro and antagonises calcineurin-NFAT signalling (Haq et al. 2000, Morisco et al. 2000, Hardt & Sadoshima 2002). Consistent with these findings, cardiac-specific GSK-3β over-expression antagonised cardiac hypertrophy in response to pressure overload, calcineurin activation or adrenergic stimulation (Antos et al. 2002).
2.4 Cardiac transcription factors
The different cell types of individual organisms share identical genomes but still synthesise a unique set of proteins. This tissue-specific protein synthesis is based on the pattern of gene expression, which is controlled at both the transcriptional and post-transcriptional levels. Transcriptional regulation is coordinated by transcription factors, DNA-binding proteins that interact with specific regulatory regions of individual genes. Accumulating evidence has suggested that transcription factors provide the crucial link between intracellular signal transduction and cardiac-specific gene expression. In this context, cardiac transcription factors have recently been defined as essential transcriptional activator proteins that are predominantly expressed in the myocardium and regulate the expression of cardiac genes encoding structural proteins or regulatory proteins characteristic of cardiomyocytes. (Akazawa & Komuro 2003.)
2.4.1 The GATA family of transcription factors
The transcription factors of the GATA family share three major features in common: they bind to the consensus nucleotide sequence (A/T)GATA(A/G), contain either one or two distinctive DNA-binding zinc finger domains, and are highly conserved between species

50
(Patient & McGhee 2002). GATA factors are found in virtually all types of eukaryotes, including fungi, plants, invertebrates and vertebrates. The vertebrate GATA family includes six proteins, GATA-1-6, all of which have a structure consisting of two adjacent zinc finger domains (Cys-X2-Cys-X17-Cys-X2-Cys) (Molkentin 2000b, Patient & McGhee 2002). These can be classified on the basis of their expression pattern into two subfamilies, GATA-1, -2 and -3 and GATA-4, -5 and -6. While GATA-1,-2 and -3 are predominantly expressed in haematopoietic stem cells, T-lymphocytes, erythroid cells and megakaryotes, in which they have an important regulatory function in differentiation, GATA-4, -5 and -6 are expressed in various mesoderm and endoderm-derived tissues, including the heart. (Molkentin 2000b.)
2.4.1.1 GATA-4
In 1993 two independent groups identified a novel transcription factor containing the highly conserved DNA-binding domain of the GATA transcription factors in the developing heart. This factor was reported to be tissue-specific, developmentally regulated and retinoic acid-inducible and designated GATA-4 (Arceci et al. 1993, Kelley et al. 1993). Cloning and initial characterisation were followed by identification and functional characterisation of the nuclear localisation and transcriptional activation domains. Based on deletion analysis, the C-terminal zinc finger appears to be sufficient for DNA binding, while the N-terminal finger probably affects the stability and specificity of the DNA binding reaction (Yang & Evans 1992, Whyatt et al. 1993, Morrisey et al. 1997, Pikkarainen et al. 2004). The N-terminal part of the protein was also reported to contain two separate transcriptional activation domains, however, which could modulate the transcriptional regulatory function of GATA-4. The C-terminal part, in turn, contains the nuclear localisation sequence adjacent to the C-terminal zinc finger (Morrisey et al. 1997).
GATA-4 is widely expressed during embryonic development. It is found in the heart, ovary, testis, gut and visceral and parietal endoderm of the mouse during embryonic and fetal development (Arceci et al. 1993). Indeed, GATA-4 is considered one of the earliest developmental markers of the precardiac mesoderm, heart and gut (Kelley et al. 1993, Morrisey et al. 1997). Its expression is not restricted to embryonic development, however, but continues postnatally. GATA mRNA has been detected in the heart, testis, and small intestine of adult mice, for instance (Arceci et al. 1993), and GATA-4 can therefore be considered a ubiqitously expressed but tissue-specific transcription factor (Molkentin 2000b).
During embryonic development, GATA-4 mRNA and protein were found to be expressed first in the coelic epithelial cells and in the endocardium, myocardium and embryonic structures containing precardiac mesoderm during heart tube formation (Heikinheimo et al. 1994). Following these observations, inhibition of GATA-4 using an anti-sense strategy was reported to inhibit cardiac muscle cell differentiation in pluripotent embryonal carcinoma cells, implying a functional role for GATA-4 in cardiogenesis (Grepin et al. 1995). GATA-4 did indeed turn out to be critical for cardiac development, since homozygous GATA-4-deficient embryos die within 7-10 days post

51
coitum due to defects in ventral morphogenesis and heart tube formation (Kuo et al. 1997, Molkentin et al. 1997). Subsequent studies using alleles that cause partial loss of GATA-4 function and conditional deletion of GATA-4 have provided further insights regarding its relation to cardiogenesis, suggesting that it is also necessary for the later phases in the development and morphogenesis of the right ventricle (Crispino et al. 2001, Pu et al. 2004, Zeisberg et al. 2005). Mutations in the GATA-4 gene have also been identified as genetic causes of congenital heart disease with atrial and ventricular septal defects (Garg et al. 2003, Okubo et al. 2004).
The relatively tissue-specific expression pattern of GATA-4 led to its identification as a regulator of cardiac-specific gene expression. GATA-4 binding elements and GATA-4-dependent promoter activation have so far been identified in a number of cardiac genes: α-MHC, troponin C and troponin I, ANP, BNP, corin, NCX, A1 adenosine receptor, acetylcholine receptor M2, cardiac-restricted ankyrin repeat protein, MLC 1/3 and calcineurin A (Ip et al. 1994, Thuerauf et al. 1994, McGrew et al. 1996, Durocher et al. 1997, Rosoff & Nathanson 1998, Charron et al. 1999, Cheng et al. 1999, Kuo et al. 1999, Rivkees et al. 1999, Pan et al. 2002, Oka et al. 2005).
Apart from regulating embryonal and baseline cardiac gene expression, GATA-4 is involved in inducible cardiac gene expression in response to hypertrophic stimuli. The first evidence concerning its role in this process was obtained in an aortic constriction model using in vivo gene transfer of an AT1A receptor promoter construct, which showed that GATA-4 and AP-1 binding sites participate in pressure overload-induced AT1A gene expression (Herzig et al. 1997). A similar experimental approach showed that intact GATA-4 binding elements are required for pressure-overload activation of the β-MHC promoter (Hasegawa et al. 1997). Interestingly, mutation of 90 GATA binding sites on the BNP promoter abrogated promoter activation in response to nephrectomy-induced haemodynamic stress (Marttila et al. 2001), suggesting a GATA-4-dependent mechanism in the regulation of stress-induced BNP gene expression. Consistent with this finding, in vitro studies of cultured cardiomyocytes have indicated that PE and isoproterenol-induced human BNP promoter activation requires GATA-binding elements (Thuerauf & Glembotski 1997, He et al. 2002).
A role for GATA-4 in cardiac hypertrophy is further strongly supported by the findings that various hypertrophic stimuli activate GATA-4. GATA-4 DNA-binding activity in cultured cardiomyocytes is increased in response to treatment with ET-1, isoproterenol and PE (Morimoto et al. 2000, Kitta et al. 2001, Morisco et al. 2001, Kerkelä et al. 2002). GATA-4 DNA binding is rapidly up-regulated by arginine-vasopressine (AVP)–induced pressure overload in vivo (Hautala et al. 2001), and although GATA-4 activation in this model was rapid and transient in nature, i.e. observed within minutes, other models have also shown that later phases of hypertrophic transformation may be associated with increased GATA-4 binding. Nephrectomised rats showed increased GATA-4 activity 26-28 h after operation (Marttila et al. 2001), and GATA-4 DNA binding increased coincidently with chronic hypertension in transgenic rats over-expressing the mouse renin gene (Diedrichs et al. 2004). Nevertheless, the necessity for GATA-4 in hypertrophic gene expression is not clear beyond acute haemodynamic overload.
GATA-4 has recently been identified as a nuclear effector of the mechanical stretch-activated hypertrophic programme in vitro (Pikkarainen et al. 2003). Inhibition of GATA-4 activity by adenovirus-mediated gene transfer of GATA-4 anti-sense cDNA attenuated

52
both stretch-induced gene expression and sarcomere reorganisation, and GATA-4 was shown to control hypertrophic gene expression in co-operation with Nkx-2.5 (Pikkarainen et al. 2003). These observations are supported by the anti-hypertrophic effects of GATA-4 anti-sense inhibition in response to PE stimulation (Charron et al. 2001). Furthermore, inhibition by a dominant negative GATA-4-engrailed fusion construct abrogated PE-induced cardiomyocyte hypertrophy (Liang et al. 2001a). Due to the embryonic lethality of GATA-4 disruption and the lack of specific inhibitors, the necessity of GATA-4 for cardiac hypertrophy in vivo is unknown, but it does appear that GATA-4 is at least sufficient to produce hypertrophic responses in vivo, since transgenic mice over-expressing it develop concentric cardiac hypertrophy with morphological, cellular and genetic features (Liang et al. 2001a).
Recent findings have also indicated that the role of GATA-4 as a myocardial survival factor can be extended beyond embryogenesis. Its activity is down-regulated in cultured cardiomyocytes in response to apoptotic stimuli such as treatment with daunorubicin (Suzuki & Evans 2004), and restoration of this activity by adenovirus-mediated gene transfer was able to attenuate the daunorubicin-induced cardiomyocyte apoptosis (Kim et al. 2003). A similar effect was observed in the case of doxorubicin treatment in vitro, and more importantly, mice that were heterozygous for a null allele of the GATA-4 gene showed significantly enhanced cardiotoxic responses after doxorubicin treatment (Aries et al. 2004). Down-regulation of GATA-4 activity was also observed in isolated perfused rat hearts after ischaemia-reperfusion injury, whereas preconditioning was associated with increased GATA-4 binding, implying that GATA-4 may be involved in cardioprotection during ischaemic injury (Suzuki et al. 2004). The mechanism whereby GATA-4 confers anti-apoptotic and cardioprotective effects is not known in detail, although it has been reported that the anti-apoptotic BCL-X gene is regulated by GATA-4 (Aries et al. 2004), and that HGF may be involved in GATA-4 activation (Kitta et al. 2003).
The regulatory mechanisms of GATA-4 activity in the heart have been a subject of intensive research. In terms of hypertrophic stimulation, control at the level of GATA-4 mRNA does not appear to be critical, since GATA-4 mRNA levels remain stable in response to AVP infusion, nephrectomy in vivo and ET-1 treatment in vitro (Hautala et al. 2001, Marttila et al. 2001, Kerkelä et al. 2002). Isoproterenol and PE are able to increase GATA-4 gene expression (Saadane et al. 1999), however, and a tendency for increased GATA-4 mRNA levels has been observed in stretched cardiomyocytes (Pikkarainen et al. 2003). Conversely, the down-regulation of GATA-4 in response to cardiotoxic anthracyclines appears to be due to decreased levels of GATA-4 mRNA and protein (Suzuki & Evans 2004). Nevertheless, accumulating evidence indicates that myocardial GATA-4 is largely controlled by post-transcriptional and post-translational mechanisms, which affect either its DNA-binding activity, transactivation and/or cellular localisation (Pikkarainen et al. 2004). First, GATA-4 protein is subject to phosphorylation, which affects its DNA binding affinity. Increased DNA binding in response to PE, ET-1 and isoproterenol is associated with increased phosphorylation of GATA-4 protein (Morimoto et al. 2000, Charron et al. 2001, Liang et al. 2001b). MAPKs have been suggested as key molecules in inducible GATA-4 phosphorylation (Fig. 4), and seven possible phosphorylation sites for them have been identified in the GATA-4 protein, among which the functional significance of the Ser-105 residue has been demonstrated in several

53
studies (Liang et al. 2001b, Pikkarainen et al. 2004). Mutation of this amino acid is sufficient to reduce GATA-4-mediated transcriptional activation (Liang et al. 2001b). Ser-105 in the GATA-4 protein is sensitive to both p38 MAPK and ERK in vitro, as PE-induced GATA-4 activation is abrogated by inhibition of ERK (Liang et al. 2001b), and p38 MAPK has been shown to phosphorylate Ser-105 directly in pull-down assays with recombinant p38 MAPK proteins (Charron et al. 2001). p38 MAPK and ERK-mediated GATA-4 phosphorylation presumably requires Rho A-related signalling in vitro, since dominant negative forms of p38 MAPK blocked Rho A-induced potentiation of GATA-4 activity (Charron et al. 2001), and Rho kinase inhibition blocked ERK-dependent GATA-4 activation by PE (Yanazume et al. 2002). Furthermore, pharmacological p38 inhibition was sufficient to abrogate ET-1-induced GATA-4 activation in cultured cardiomyocytes (Kerkelä et al. 2002).
While targeted phosphorylation of serine residues affects GATA-4 DNA-binding activity, the phosphorylation of the N-terminal domain by GSK-3β may be related to its subcellular localisation (Pikkarainen et al. 2004). In contrast to serine phosphorylation by p38 MAPK and ERK 1/2, this phosphorylation is associated with decreased transcriptional activity, a fact which is probably related to increased nuclear export of GATA-4 by the exportin Crm1, as inhibition of Crm1 increases basal nuclear GATA-4 and suppresses GSK-3β-induced decreases in nuclear GATA-4 levels (Morisco et al. 2001). In addition, GSK-3β may affect GATA-4 via interaction with NFAT, because it phosphorylates NFAT and enhances NFAT nuclear export (Antos et al. 2002). Finally, GATA-4 protein is also sensitive to other post-translational modifications as well as phosphorylation. It has recently been suggested that acetylation of GATA-4 protein may be involved in the differentiation of embryonic stem cells into cardiac myocytes, by showing that treatment with the histone-deacetylase inhibitor trichostatin A increased the amount of acetylated GATA-4 and its DNA binding (Kawamura et al. 2005). Cardiac hypertrophy in transgenic mice over-expressing histone acetyltransferase p300 is also characterised by increased GATA-4 acetylation and DNA binding (Yanazume et al. 2003).

54
Fig. 4. Regulatory mechanisms and target genes of GATA-4. GATA-4 is subject to both MAPK-mediated phosphorylation and interactions with other transcription factors.
GATA-4 protein is subject to interactions with other transcription factors, and several studies have suggested that functional co-operation may be a prerequisite for the transcriptional effects of GATA-4 (Pikkarainen et al. 2004). This co-operation is mediated by physical interaction with the C-terminal zinc finger of the GATA-4 protein, except in the GATA-4 – friend of GATA 2 (FOG-2) interaction, in which the interacting region is located in the N-terminal zinc finger (Svensson et al. 2000, Pikkarainen et al. 2004). Functional interactions of GATA-4 have so far been described with dHAND, FOG-2, SRF, Nkx-2.5, MEF-2, NFATc4, GATA-6, Tbx-5, Yin Yang 1 and p300 (Lee et al. 1998, Molkentin et al. 1998, Charron et al. 1999, Svensson et al. 1999, Belaguli et al. 2000, Bhalla et al. 2001, Dai & Markham 2001, Dai et al. 2002, Garg et al. 2003), the result being in the majority of cases a synergistic transactivation of the target gene, demonstrated with most cofactors by ANP and BNP promoter activation (Fig. 4). A repressive effect is also possible, however, as with the GATA-4-FOG-2 interaction (Svensson et al. 2000). Although the importance of the GATA-4-cofactor interactions with respect to promoter activation is unequivocal, their pathophysiological significance is less clear. Co-operation between Nkx-2.5 and GATA-4 has recently been suggested as mediating stretch-induced cardiomyocyte hypertrophy and BNP gene expression (Pikkarainen et al. 2003), and synergistic activation of GATA-4 and NFATc4 is thought to be involved in the calcineurin-mediated hypertrophic programme (Molkentin et al. 1998). Finally, given that many GATA-4 cofactors have been suggested as independent regulators of cardiac hypertrophy, synergistic pro-hypertrophic effects are also possible with other cofactors.
GATA-4
ATP
ADP
MAPKs
P
Mechanical and neurohumoral load
ANP, BNP, α-MHC, troponin C, troponin I, corin, Na+/Ca2+-exchanger, A1 adenosine receptor, acetylcholine receptor M2, cardiac-restricted ankyrin repeat protein, myosin light chain, calcineurin
MEF-2
FOG-2
SRF
Nkx-2.5
GATA-6
NFAT
promoter
Target genesGATA-4
ATP
ADP
MAPKs
P
Mechanical and neurohumoral load
ANP, BNP, α-MHC, troponin C, troponin I, corin, Na+/Ca2+-exchanger, A1 adenosine receptor, acetylcholine receptor M2, cardiac-restricted ankyrin repeat protein, myosin light chain, calcineurin
MEF-2
FOG-2FOG-2
SRFSRF
Nkx-2.5Nkx-2.5
GATA-6GATA-6
NFATNFAT
promoter
Target genes

55
2.4.1.2 Other members of the GATA family
The other members of the GATA family expressed in the heart are GATA-5 and GATA-6. GATA-4, GATA-5 and GATA-6 are 85% identical to one another at the amino acid level within the DNA-binding region (Molkentin 2000b).
Like GATA-4, GATA-6 appears to be critical for embryonic development, although its role in cardiac development is poorly understood as null mice die prior to heart induction (Morrisey et al. 1998). Gain-of-function studies have suggested, however, that GATA-6 may affect cardiogenesis (Gove et al. 1997). This notion was also supported by the observations that anti-sense oligonucleotide inhibition of GATA-6 affected the differentiation of a cardiac lineage during embryogenesis (Peterkin et al. 2003, Peterkin et al. 2005). In contrast to GATA-4 and GATA-6, null mutation of GATA-5 does not lead to any obvious cardiac defects, suggesting that GATA-5 is not critical for heart development (Molkentin et al. 2000b).
The role of GATA-5 and GATA-6 in the adult heart is not as well documented as that of GATA-4. In particular, they have not been reported to mediate inducible cardiac gene expression, suggesting that GATA-4 is the major factor bound by the GATA sites of cardiac gene promoters. It is of note, though, that ANP or α-MHC gene expression is not impaired in GATA-4-deficient mice, suggesting that GATA-6 is able to compensate for the lack of GATA-4 under certain conditions (Kuo et al. 1997, Molkentin et al. 1997). It has also been suggested that GATA-6 may regulate gene expression in vascular smooth muscle cells (Molkentin 2000b).
2.4.2 AP-1
AP-1, one of the first mammalian transcription factors to be identified (Angel & Karin 1991), is not a single protein but a complex of heterodimers and homodimers of the leucine zipper proteins Jun (c-Jun, JunB, JunD), Fos (c-fos, FosB, Fra-1 and Fra-2) and ATF (ATF2, ATF3/LRF1, B-ATF, JDP1, JDP2). The Maf proteins (c-Maf, MafB, MafA, MafG/F/K and Nr1) have also been included in the AP-1 family on the grounds of sequence homology. Functionally, c-Jun is the most potent transcriptional activator of the Jun group, while within the Fos group, c-fos and FosB contain transcriptional activation domains and form heterodimers with the Jun group proteins to enhance their transcriptional activity. (Karin et al. 1997, Shaulian & Karin 2002.)
Members of the AP-1 complex identify and bind to the palindromic DNA sequence 5’-TGAGTCA-3’ (Hai & Curran 1991). Although the DNA binding of the AP-1 complex is mediated by the leucine zipper motif; the properties of the individual components of the complex partially determine the nature of the DNA-protein interaction. At the level of DNA binding, AP-1 activity is ubiquitous and found in virtually all types of eukaryotes. (Wisdom 1999.) AP-1 binding sites are abundant in the promoter region of numerous cardiac genes, including the ANP, BNP, α-SkA, ET-1 and AT1A receptor genes (Bishopric et al. 1992, Kovacic-Milivojevic & Gardner 1993, Grepin et al. 1994, Kawana et al. 1995, Herzig et al. 1997).

56
Due to the fact that the AP-1 complex consists of a series of proteins encoded by two multigene proteins, the mechanisms regulating AP-1 activity are complex. They can be classified into four broad categories: first, changes in jun and fos gene transcription and mRNA turnover affect AP-1 activity; second, the regulation may occur through post-translational modification of Jun and Fos proteins; third, it may occur through effects on Jun and Fos protein turnover; and fourth, it may occur through interactions with other transcription factors. (Shaulian & Karin 2002.) The complex mechanisms of regulation are naturally related to the wide array of signal transduction mechanisms affecting AP-1 activity. Within the first and second of the above mentioned categories of AP-1 regulation, MAPKs represent key upstream signalling molecules in many cell types. Members of the MAPK cascade first activate AP-1 by direct phosphorylation of the subunits, so that c-Jun, for instance, is among the primary substrates of JNK and ATF-2 among those of p38 MAPK. Furthermore, ERK and p38 MAPK can potentiate the transcriptional activity of ternary complex factors (TCFs) which bind to the fos promoter, leading to increased fos transcription. (Karin 1995, Shaulian & Karin 2002.) ERK is also known to phosphorylate Fra1 and Fra2 directly (Gruda et al. 1994). A number of other transcription factors have been reported to co-operate with AP-1 in the context of interactions, and an analysis of native promoters has revealed that binding sites for other transcription factors almost invariably exist adjacent to the AP-1 sites. These factors include NFAT, nuclear receptors, ETS binding factors, the Smad family of proteins and NF-κB. These interactions appear to be of particular importance with respect to the specificity of the AP-1 response. (Wisdom 1999.)
AP-1 is activated by a variety of stimuli, which partially resemble those activating MAPK cascades. It is sensitive to cellular stresses, UV irradiation, DNA damage, growth factors, polypeptide hormones, cytoskeletal rearrangements and pro-inflammatory cytokines (Karin et al. 1997, Shaulian & Karin 2002). In the heart, AP-1 DNA binding is increased in response to a number of stimuli, including isoproterenol and angiotensin II infusion, aortic constriction, direct ventricular wall stress and myocardial infarction (Cornelius et al. 1997, Herzig et al. 1997, Shimizu et al. 1998, Takemoto et al. 1999, Fiebeler et al. 2001).
The multiplicity of AP-1 complexes has complicated attempts to determine its functional role. In particular, single gene knock-outs of AP-1 members provide little evidence concerning the role of the entire complex, and the necessity for AP-1 in myocardial remodelling therefore remains essentially unknown (Wisdom 1999). It should be noted, though, that, as mentioned above, AP-1 is sensitive to many stimuli that are critical in the remodelling process, and there are data indicating that AP-1 binding sites are required for inducible activation of the AT1A receptor gene, for instance (Herzig et al. 1997).
2.4.3 NF-κB
NF-κB is a dimeric transcription factor consisting of heterodimers or homodimers of p50, p52, p65 (RelA), c-Rel and RelB proteins. The most common active form of NF-κB is a heterodimer composed of p50 or p52 and RelA. NF-κB activity is controlled by a unique

57
regulatory mechanism, in that NF-κB dimers in their inactive state reside in the cytoplasm and are bound to inhibitory proteins IκB. Upon activation, the N-terminal serine residues of IκB are phosphorylated by IκB kinases, leading to ubiquitination and proteolytic degradation of IκB. This causes the NF-κB to translocate to the nucleus and bind to the promoters of target genes. (Valen et al. 2001.)
NF-κB is involved in immune and inflammatory responses. It is activated by pro-inflammatory cytokines such as TNF-α and IL-1, and its activation appears to be associated with many inflammatory diseases, such as septic shock, acute respiratory distress syndrome and viral diseases (Baeuerle & Baltimore 1996, Purcell & Molkentin 2003). Apart from pro-inflammatory cytokines, NF-κB has been reported to be sensitive to lipopolysaccharide, UV irradiation, phorbol esters, free radicals and oxidative stress (Baeuerle & Baltimore 1996, Valen et al. 2001). NF-κB controls the transcription of a wide spectrum of genes involved in both innate and adaptive immunity, such as chemokines, cytokines (e.g. IL-6 and IL-12), leukocyte adhesion molecules and inflammatory enzymes (such as COX-2 and inducible nitric oxide synthase) (Valen et al. 2001). The cellular consequences of NF-κB are not restricted to the regulation of pro-inflammatory genes, however, but also include apoptotic responses (Chen et al. 1999). Interestingly, a number of both anti-apoptotic and pro-apoptotic genes are controlled by NF-κB. The pro-apoptotic genes include Fas, FasL, caspases 8 and 11 and TNFα, and the anti-apoptotic ones the Bcl-2 family members A1 and Bclx1 and cellular inhibitors of apoptosis (Karin & Lin 2002, Purcell & Molkentin 2003). Consistent with the gene expression profile, both anti-apoptotic and pro-apoptotic effects of NF-κB activation have been reported, depending on the stimulus, cell type and experimental model (Chen et al. 1999). It is significant that at least baseline NF-κB appears to be required for cell survival, as transgenic mice incapable of NF-κB activation die due to excessive liver cell apoptosis (Li et al. 1999, Tanaka et al. 1999).
Given the above cellular functions, it has been suggested that NF-κB may be involved in the pathogenesis of several cardiovascular diseases. It is considered to partially mediate the inflammatory responses of chronic heart failure, based on observations that NF-κB activity and the levels of its target genes are increased in both experimental heart failure models and tissue samples from patients with heart failure or unstable angina (Ritchie 1998, Wong et al. 1998, Lu et al. 2004). Evidence has also accumulated regarding the role of NF-κB in cardiac hypertrophy and ischaemia. Hypertrophic stimuli, including angiotensin II, ET-1 and PE, increase NF-κB transcriptional activity (Fiebeler et al. 2001, Purcell et al. 2001). Over-expression of NF-κB is sufficient to induce hypertrophy and ANP gene expression in cultured cardiomyocytes (Purcell et al. 2001), and it has been suggested that stretch-induced BNP promoter activation may occur through NF-κB activation (Liang & Gardner 1999). Attenuation of cardiomyocyte hypertrophy by the NF-κB inhibitory peptide A20 has also been observed (Cook et al. 2003). These in vitro observations have recently been extended by in vivo studies using genetic and pharmacological approaches to arrest NF-κB activity, showing that both aortic banding-induced hypertrophy and hypertrophy in SHRs can be reduced by NF-κB inhibition (Li et al. 2004, Gupta et al. 2005).
The activation of NF-κB by ischaemia and ischaemia-reperfusion injury is well documented, having been reported both in experimental models and in humans (Valen 2004). In view of its target genes, ischaemic NF-κB activation was originally considered

58
detrimental, an interpretation supported further by the notion that decoy inhibition of NF-κB may reduce ischaemia-reperfusion injury (Morishita et al. 1997, Valen et al. 2001). On the other hand, a positive role for NF-κB has been reported in ischaemic preconditioning, suggesting that, as in the context of apoptosis, NF-κB may have a dual role with both beneficial and detrimental effects (Valen et al. 2001, Valen 2004).
2.4.4 MEF-2
The vertebrate MEF-2 family comprises four isoforms, MEF-2A, MEF-2B, MEF-2C and MEF-2D (Olson et al. 1995). The MEF-2 factors contain a MADS domain with a specific adjacent 29 amino-acid MEF-2 domain, which mediates DNA binding to their cognate DNA sequences CAT(A/T)4TAG/A (Akazawa & Komuro 2003).
MEF-2 factors are widely expressed in different cell types, but specific regulatory functions have been identified predominantly in inflammatory cells, skeletal muscle cells and cardiomyocytes (Han & Molkentin 2000). In the heart, MEF-2-binding sequences have been identified in the promoters of the muscle creatine kinase gene, α-MHC, MLC1/3, MLC2v, α-SkA, SERCA, troponin T, troponin C, troponin I, desmin and dystrophin (Akazawa & Komuro 2003). Cardiac MEF-2 is sensitive to hypertrophic stimulation and partially confers inducible expression of the c-jun gene (Marinissen et al. 1999, Nadruz et al. 2003).
Like GATA-4, MEF-2 appears to be a convergence point for cardiomyocyte signal transduction. It was first reported to be phosphorylated by p38 MAPK in several experimental setups (Han & Molkentin 2000), and ERK5 also phosphorylates MEF-2, a reaction which probably mediates the MEF-2-dependent induction of the c-jun promoter (Kato et al. 1997, Marinissen et al. 1999). Second, MEF-2 is dependent on the PI3K-Akt pathway during IGF-1-induced skeletal muscle differentiation (Tamir & Bengal 2000, Xu & Wu 2000). Third, MEF-2 is a downstream target of calcium-activated signalling, both via direct phosphorylation by CaMKs and via class II histone deacetylases (HDACs) (Lu et al. 2000, McKinsey et al. 2000a, Passier et al. 2000). The class II HDACs are associated with MEF-2, and upon activation, CaMKs phosphorylate the HDACs, causing intracellular chaperones to dissociate the resulting MEF-2-HDACs (McKinsey et al. 2000b). Finally, MEF-2 co-operates functionally with GATA-4 to activate transcription of the ANP, BNP, α-MHC and cardiac α-actin genes (Morin et al. 2000), and protein-protein interactions between MEF-2 and NFAT, MyoD and Smad have been reported (Akazawa & Komuro 2003).
Despite its relatively well-documented activation by hypertrophic stimuli and obvious interactions with other hypertrophy-associated pathways, no definitive mechanistic evidence regarding the role of MEF-2 in cardiovascular pathophysiology exists. It should be noted, however, that several recent studies have provided evidence for HDAC-dependent repression of cardiac hypertrophy, which indirectly supports a role for MEF-2 in the hypertrophic process (Akazawa & Komuro 2003).

59
2.4.5 SRF
The discovery of a serum response element (SRE) in the c-fos promoter led to the purification and cloning of SRF, a 62-67 kDa protein that was able to bind to the core CArG within the element (Prywes & Roeder 1987, Treisman 1987, Boxer et al. 1989). Like MEF-2, SRF belongs to the MADS box family of transcription factors. The MADS box, consisting of a DNA-binding domain, a dimerisation domain and an interface for protein-protein interactions, is located in the N-terminal region of the SRF protein, while the C-terminal part contains a strong transactivation domain with multiple phosphorylation sites (Miano 2003).
Complete disruption of SRF in transgenic mice results in early mortality from gastrulation defects (Arsenian et al. 1998). Cardiac-specific SRF knock-out mice do not develop to term, either, but die of structural defects of the heart and vasculature between embryonic days 10 and 13, indicating that SRF is required for development of the embryonic cardiovascular system (Miano et al. 2004, Parlakian et al. 2004). Its relevance to the postnatal cardiovascular pathophysiology is less clear, although transgenic mice over-expressing mutated SRF seem to develop a phenotype of dilated cardiomyopathy (Zhang et al. 2001). SRF can nevertheless undoubtedly be considered to be among the transcription factors that contribute to inducible cardiac-specific gene expression, since SREs are found in ANP, α-SkA, c-fos and α-MHC promoters, SRF has been shown to contribute to the activation of these genes, and finally, the expression of them is at least partially blunted in SRF-deficient cardiomyocytes (Nelson et al. 2005).

3 Aims of the research
The general aim of this research was to determine the activities and roles of MAPKs and their downstream effector GATA-4 during increased cardiac workload and remodelling.
More specifically, the objectives were:
1. to determine the effect of increased left ventricular wall stress on cardiac transcription factor activities and to study the role of paracrine mechanisms in this process.
2. to study the role of MAPKs in the regulation of the GATA-4 transcription factor during increased wall stress.
3. to evaluate the role of p38 MAPK in the regulation of cardiac transcription factors and cardiac-specific gene expression using an adenovirus-mediated gene transfer approach.
4. to determine the functional role of p38 MAPK in left ventricular remodelling.

4 Materials and methods
4.1 Materials
Bosentan was a generous gift from Dr. Martine Clozel (Actelion, Basel, Switzerland), CV-11974 from Dr. Hajime Toguchi (Takeda Chemical Industries Ltd, Osaka, Japan), SB239063 from Robert N. Willette (GlaxoSmithKline Pharmaceuticals, Philadelphia, USA), and CEP-11004 from Cephalon Inc., West Chester, PA, USA. Other reagents and their suppliers were: hyperfilm MP, [32P]-deoxycytidine-5’-triphosphate (Amersham Life Science, Buckinghamshire, UK), Bio-Rad Protein Assay (Bio-Rad Laboratories Inc., Hercules, CA, USA), bisindolylmaleimide I (Calbiochem, San Diego, CA, USA), anti-caspase-3 antibody, anti-phospho-p44/42 antibody, anti-p38 antibody, anti-p44/42 antibody (Cell Signalling Technology Inc., Hitchin, Hertfordshire, UK), ERK Assay Kit, p38 MAP Kinase Assay Kit, JNK Assay Kit (Cell Signaling Technology, Beverly, MA, USA), anti-phospho-p38 antibody (Chemicon International Inc., Temecula, CA, USA), EnVision Detection Kit system, Ki-67 antibody (DakoCytomation, Denmark), formaldehyde, guanidine isothiocyanate (Fluka Chemie AG, Buchs, Switzerland), PD98059, SB203580 (LC Laboratories, Woburn, MA, USA), ApopTag in situ apoptosis detection kit (Oncor, Gaithersburg, MD, USA), medetomidine hydrochloride, ketamine hydrochloride, atipamezole hydrochloride, xylazine (Orion Pharma Inc, Espoo, Finland), nylon membranes (Osmonics, Westborough, MA, USA), ET-1 (Peninsula Laboratories, Belmont, CA, USA), agarose NA, Quick Prime Kit (Pharmacia, LKB Biotechnology, Uppsala, Sweden), anti-GATA-4 antibody, anti-phospho-Elk-1 antibody, anti-phospho-JNK antibody, anti-JNK antibody, C-kit antibody (Santa Cruz Biotechnology, CA, USA), buprenorphine hydrochloride (Schering-Plough Corporation, Brussels, Belgium), CsCl (Serva Feinchemica GmBh & Co, Heidelberg, Germany), angiotensin II (Sigma Chemicals Co., St Louis, MO, USA), oligonucleotides (Sigma-Genosys, Cambridge, UK), OCT compound (Tissue-Tek, Sakura, Netherlands), U0126, Y-27632 (Tocris Cookson Ltd., Avonmouth, UK), biotinylated lectin GSL 1, HRP-streptavidin (B-1205, Vector Laboratories, Burlingame, CA, USA). Other reagents were from Sigma Chemicals.

62
4.2 Experimental protocols
Table 4. Summary of the experimental protocols.
Study Experimental model Methods I Increased left ventricular wall stress in
isolated perfused rat hearts Electrophoretic mobility shift assay (EMSA) Pharmacological inhibitors RNA isolation and northern blotting
II Increased left ventricular wall stress in isolated perfused rat hearts; mechanical stretch in isolated rat atria
EMSA Pharmacological inhibitors Western blotting Kinase activity assays RNA isolation and northern blotting
III Adenovirus-mediated gene transfer in vivo
Echocardiography DNA microarray RNA isolation, northern blotting and RT-PCR Histology, light microscopy Immunohistochemistry EMSA Western blotting Kinase activity assays
IV Adenovirus-mediated gene transfer in vivo; experimental myocardial infarction in vivo
Echocardiography RNA isolation, northern blotting and RT-PCR Histology, light microscopy and image analysis Immunohistochemistry TUNEL staining X-gal staining Western blotting Kinase activity assays
4.2.1 Experimental animals
Male 8-week-old Sprague-Dawley rats weighing 250-320 g from the Centre for Experimental Animals at the University of Oulu were used. They were housed in plastic cages in a room with controlled 40% humidity and a temperature of 22°C, and a 12-hour environmental light cycle was maintained. All experimental protocols were approved by the Animal Use and Care Committee of the University of Oulu. The investigation conforms to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health.

63
4.2.2 Preparation of isolated perfused rat hearts
The preparation method used in this study was a modification of the previously described experimental setup (Ruskoaho et al. 1986, Thienelt et al. 1997). Briefly, the rats were anaesthetised with carbon dioxide and decapitated. The abdominal cavity was opened, the diaphragm transected and lateral incisions were made on both sides of the rib cage. The heart was cooled with perfusion buffer, and the aorta cannulated above the aortic valve. The heart was then immediately arranged for retrograde perfusion by the Langendorff technique using modified Krebs-Henseleit bicarbonate buffer (pH 7.40) equilibrated with 95% O2-5% CO2 at 37°C. The composition of the buffer was (in mM) 113.8 NaCl, 22.0 NaHCO3, 4.7 KCl, 1.2 KH2PO4, 1.1 MgSO4, 2.5 CaCl2, and 11.0 glucose. The coronary flow rate was gradually increased to 15 mL/min and the heart rate was increased to 15-20% above the spontaneous beating frequency using a Grass stimulator (model S88, Grass Instruments, Quincey, MA, USA). Variations in the perfusion pressure arising from changes in coronary vascular resistance were measured with a pressure transducer (Isotec, Hugo Sachs Elektronik, Germany) situated on a side arm of the aortic cannula. The left ventricular pressure was measured using a fluid-filled balloon connected to a pressure transducer (Isotec, Hugo Sachs Elektronik, Germany). The heart rate was determined from the changes in intraventricular pressure.
Initially, the left ventricular balloon was inserted into the left ventricle through the mitral valve and the heart was unloaded by opening the valve in the cannula of the intraventricular balloon against the air so that the balloon was inflated just enough to obtain a pressure signal to monitor the stability of the preparation. After a period of equilibration under unloaded conditions, the left ventricular balloon was inflated in order to increase the left ventricular wall stress. The valve of the balloon cannula was closed, and the volume of the balloon was gradually increased within 5 minutes to reach a peak systolic pressure of between 130 and 150 mmHg. The end-diastolic pressure was set to between 20-25 mmHg to maximise active pressure generation and the systolic pressure. In the control groups, the perfusion was continued further under unloaded conditions. Analogue signals from the pressure transducers were digitised at a sampling frequency of 125 Hz, recorded and analysed with an IBM PC-compatible computer with PONEMAH data acquisition software (Gould Instrument System Inc, Ohio, USA). The numerical values for wall stress were calculated by deriving the peak systolic circumferential wall stress (σ) from the ventricular pressure measurements, i.e. the intraventricular balloon volume (VB) and the weight of the left ventricle, as described by Strömer et al. (1997). A spherical model was assumed in which the radius of the left ventricle (Ri) could be calculated using the cubic formula Ri =3√VB/[(4/3)·π]. Total left ventricular volume is the sum of VB and the volume of the left ventricular wall [VWall=left ventricular weight/1.05 (specific gravity of myocardium)]. Therefore VB + VWall = (4/3) · π · (Ri + h)3 and h = {3√ (VB + VWall)/ [(4/3)·π]} - Ri , where h = thickness of the left ventricular wall. The left ventricular circumferential wall stress was then derived from Laplace’s law σ = P· [(Ri2/h) / (2Ri + h)], where P = peak systolic pressure.
Depending on the type of experiment, the hearts were perfused under increased wall stress for 10 min, 30 min, or 2 h. The drugs (10 nM CV-11974, 1 μM Bosentan, 10 μM SB239063, 1 μM U0126, 3 μM Y-27632, 90 nM Bisindolylmaleimide I, 100 nM CEP-

64
11004), or vehicle alone, were infused continuously into the aortic cannula in the absence or presence of increased wall stress. ET-1 (30 pM - 1 nM) and angiotensin II (10 nM) were infused in the same manner in the absence of wall stress. At the end of the experiments, the left ventricles were immersed in liquid nitrogen and stored in –70°C until assayed.
4.2.3 Preparation of isolated rat atria
The experiments using isolated rat atrial appendices were performed as described previously (Tavi et al. 1998). Male Sprague-Dawley rats were anaesthetised and their hearts were rapidly removed, as for the isolated perfused rat hearts. The left atrial auricle was attached to one of the four ends of a cross-branch polyethylene adapter and the tissue was placed in a constant-temperature (37°C) organ bath. A tube was attached to the opposite end of the cross-branch adapter, and another tube of smaller diameter was inserted inside the adapter to carry perfusate inflow into the lumen of the auricle. The outflow from the lumen came from one cross-branch of the X-cannula. For atrial stretch, the pressure inside the atrium was increased by raising the height of the outflow tube. The other cross-branch of the X-cannula was connected to a pressure transducer (TCB 100, Millar Instruments, Inc), so that the pressure in the lumen of the auricle could be recorded.
4.2.4 Adenoviral gene transfer in vivo
The recombinant adenoviruses, which were generously supplied by Dr. Veli-Matti Kähäri, University of Turku, Finland, contained the coding regions of constitutively active MKK3b (RAdMKK3bE), MKK6b (RAdMKK6bE), WT p38α (RAdp38α) and WT p38β (RAdp38β) genes driven by the cytomegalovirus immediate early promoter, and had been generated as previously described (Wang et al. 1998). Recombinant replication-deficient adenovirus RAdlacZ, containing the Escherichia coli β-galactosidase (Lac Z) gene was used as a control virus.
The gene transfer protocol was a modification of a previously described experimental procedure (Szatkowski et al. 2001). 8-week-old male SD rats were anaesthetised with medetomidine hydrochloride (250 μg/kg, i.p.) and ketamine hydrochloride (50 mg/kg, i.p.). A left thoracotomy and pericardial incision were performed to expose the heart and single injections of 2-8 x 108 infectious units (pfu) of RAdMKK3bE, RAdMKK6bE, RAdp38α, RAdp38β or RAdlacZ adenovirus in a 100 μl volume were made into the left ventricular free wall using a Hamilton precision syringe. The heart was then rapidly repositioned, the rat was briefly hyperventilated and the incision closed. The anaesthesia was partially antagonised with atipamezole hydrochloride, and buprenorphine hydrochloride was administered for post-operative analgesia. The gene transfer to the hearts with experimental myocardial infarction was performed in a similar manner prior to the ligation of the left anterior descending coronary artery (LAD).

65
4.2.5 Experimental myocardial infarction
Myocardial infarction was produced by ligation of the LAD during medetomidine hydrochloride and ketamine hydrochloride anaesthesia as previously described (Pfeffer et al. 1979). The rat was connected to the respirator through a tracheotomy and ventilated at a rate of 55-60 breaths per minute. A left thoracotomy and pericardial incision were performed and the LAD was ligated about 3 mm from its origin and gene transfer performed as described above when appropriate. After ligation of the LAD, the heart was repositioned in the chest and the incision closed. The anaesthetic effects of the medetomidine were antagonised with atipamezole hydrochloride, and the rats were hydrated with 10 ml physiological saline solution given subcutaneously. Buprenorphine hydrochloride was administered for postoperative analgesia. The sham-operated rats underwent the same surgical procedure without gene transfer or ligation of the LAD.
4.3 Echocardiographic measurements (III, IV)
Transthoracic echocardiography was performed using a commercially available Acuson Ultrasound System (SequoiaTM 512) and a 15-MHz linear transducer (15L8) (Acuson, Mountain View, California, USA). The echocardiographist was blinded to the details of the study. Rats were sedated with ketamine and xylazine and placed in the supine position. Normal body temperature was maintained by means of a warming pad and lamp. A short-axis view of the left ventricle at the level of the papillary muscles was obtained using two-dimensional imaging and a two-dimensionally guided M-mode recording was performed through the anterior and posterior walls of the left ventricle. Left ventricular end-systolic (LVESD) and end-diastolic (LVEDD) dimensions and the thicknesses of the interventricular septum and posterior wall were measured from the M-mode tracings. The fractional shortening (FS) and ejection fraction (EF) were calculated from the M-mode left ventricular dimensions using the following equations: FS (%) = {(LVEDD-LVESD) / LVEDD} x 100, EF (%) = {(LVEDD)3 – (LVESD)3 / LVEDD3} x 100. An average of three measurements of each variable was used for all the calculations. After echocardiography, the animals were sacrificed, the abdominal cavity was opened and the heart removed. The aorta and pulmonary artery were excised and the right ventricle and auricles were removed. All cardiac tissue samples were weighed, frozen in liquid nitrogen and stored at -70°C for further analysis.
4.4 Extraction of cytoplasmic and nuclear protein (I-IV)
In order to extract the cytoplasmic protein, the whole left ventricular tissue was broken and reduced to a powder in liquid nitrogen. The thawed powder was homogenised in a lysis buffer consisting of 20 mmol/L Tris (pH 7.5), 10 mmol/L NaCl, 0.1 mmol/L EDTA, 0.1 mmol/L EGTA, 1 mmol/L β-glycerophosphate, 1 mmol/L Na3VO4, 2 mmol/L benzamidine, 1 mmol/L PMSF, 50 mmol/L NaF, 1 mmol/L DTT and 10 μg/mL each of

66
leupeptin, pepstatin and aprotinin. The resulting tissue homogenates were centrifuged at 2000 rpm for 1 minute at +4°C. The cytosolic fraction was separated out by centrifugation at 12500 rpm for 20 minutes, frozen in liquid nitrogen and stored at –70°C until assayed.
To extract the nuclear protein fraction, the supernatant from the first centrifugation was incubated on ice for 15 minutes, 0.6% NP-40 was added, and the nuclei were pelleted by means of a second centrifugation. The resulting pellet was resuspended in a solution containing 20 mM HEPES (pH 7.9), 0.4 M NaCl, 1 mM EDTA, 1 mM EGTA, 1 mmol/L Na3VO4, 2 mmol/L benzamidine, 1 mmol/L PMSF, 50 mmol/L NaF, 1 mmol/L DTT, 3 ug/mL TPCK, 3 ug/mL TLCK, and 10 μg/mL each of leupeptin, pepstatin and aprotinin. The samples were then incubated for 30 minutes at +4°C, centrifuged and the resulting supernatant frozen in liquid nitrogen and stored at –70°C until assayed. In the alternative nuclear protein extraction protocol (Deryckere & Gannon 1994) described in papers I and II, the tissue was broken as described above and homogenised in a low salt solution consisting of 0.6% NP-40, 150 mM NaCl, 10 mM HEPES pH 7.9, 1 mM EDTA and 0.5 mM PMSF and centrifuged at 2000 rpm for 30 s. The supernatant was then incubated on ice for 4 minutes and centrifuged for 5 min at 5000 rpm. The pellet, consisting of nuclei, was resuspended in a high salt solution (25% glycerol, 20 mM HEPES pH 7.9, 420 mM NaCL, 1.2 mM MgCl2, 0.2 mM EDTA, 0.5 mM dithiotreitol, 0.5 mM PMSF, 2 mM benzamidine and 5 μg each of aprotinin, leupeptin and pepstatin) and incubated on ice for 20 min. Insoluble cellular debris was pelleted by a short centrifugation and the resulting supernatant was divided into aliquots, frozen in liquid nitrogen and stored in at –70°C. All protein concentrations were determined by Bio-Rad Laboratories Protein Assay.
4.5 Western blot analysis and kinase activity assays (II-IV)
For western blot analysis 30 μg of protein was loaded onto a SDS-PAGE column, electrophoresed and transferred to nitrocellulose membranes, which were then blocked in 5% non-fat milk and incubated at +4°C overnight with anti-phospho-p38, anti-phospho-p44/42, anti-phospho-JNK, anti-p38, anti-p44/42, anti-JNK or anti-GATA-4 antibody. On the following day the filters were washed and incubated for 1 hour with an HRP-conjugated anti-rabbit, anti-mouse or anti-goat secondary IgG antibody, and finally the blots were developed with enhanced chemiluminescence reagents and exposed to film for 30 seconds – 10 minutes. The films were scanned and analysed with Quantity One software (Bio-Rad Laboratories, Hercules, CA, USA) for quantitive data analysis.
p38 MAP kinase activity was determined with an immuno complex kinase assay using ATF-2 and Elk-1 as substrates. Cardiac tissue homogenates were clarified by centrifugation, and the supernatants were immunoprecipitated with immobilised phospho-p38 monoclonal antibody. The resulting pellets were washed twice with a buffer consisting of 20 mM Tris (pH 7.5), 10 mM NaCl, 0.1 mM EDTA and 0.1 mM EGTA supplemented with 1 mM β-glycerophosphate, 2 mM dithiothreitol, 1 mM Na3VO4, 10 μg/ml leupeptin, 10 μg/ml aprotinin, 2 μg/ml pepstatin, 2 mM benzamidine, 1 mM phenylmethylsulfonyl fluoride and 50 mM NaF. The pellets were then washed once with

67
a kinase buffer consisting of 25 mM Tris (pH 7.5), 5 mM β-glycerophosphate, 2 mM DTT, 0.1 mM Na3VO4 and 10 mM MgCl2, and finally they were suspended in 40 μl of kinase buffer including 200 μM ATP and 2 μg of ATF-2 or Elk-1 fusion protein. The kinase reaction was continued for 30 minutes at +30°C, and was stopped by placing the samples on ice and adding 20 μl of 3×SDS. The samples were subsequently boiled, microcentrifuged and analysed by western blotting for phospho-Elk-1 or phospho-ATF-2. The assay for measuring ERK activity was similar to the p38 kinase assay, except that the protein was immunoprecipitated with immobilised phospho-p44/42 monoclonal antibody, ELK-1 fusion protein was used as a substrate, and the samples were analysed by western blotting for phospho-ELK-1. For the JNK assay, c-Jun fusion protein was used to pull down active JNK from clarified cardiac tissue homogenates. The pellet was washed twice with lysis buffer and twice with a kinase buffer consisting of 25 mM Tris pH 7.5, 5 mM β-glycerophophate, 2 mM DTT, 0.1 mM Na3VO4 and 10 mM MgCl2. Finally, the pellet was suspended in 40 μl of kinase buffer including 100 μM ATP and the samples were incubated at +30°C for 30 minutes. The kinase reaction was stopped by placing the samples on ice and adding 20 μl of 3×SDS. The samples were then boiled, microcentrifuged, and analysed by western blotting for phospho-c-Jun.
4.6 Gel mobility shift assays (I-III)
Double-stranded oligonucleotides containing GATA or AP-1 binding sequences of the rat BNP promoter, NFAT sequences of the human BNP promoter, the MEF-2 binding sequence of the mouse muscle creatine kinase promoter, the SRF binding sequence of the rat c-fos promoter or oligonucleotides with a NF-κB and Oct-1 consensus binding sequence were labelled with [α-32P]-dCTP using the Klenow enzyme (Hautala et al. 2001). The sequences used for the gel mobility shift assay probes are provided in Table 5.
Table 5. Oligonucleotides for gel mobility shift assay analysis.
Probe Sequence GATA 5’-TGTGTCTGATAAATCAGAGATAAC-CCCACC-3’ AP-1 5’-GGAAGTGTTTTT-GATGAGTCACCCCA-3’ MEF-2 5’-AGCTCGCTCTAAAAATAACCCTGTCCC-3’ SRF 5’-ACAGGATGTCCATATTAGGACATCTGCG-3’ NF-κB 5’- AGTTGAGGGGACTTTCCCAGGCCA-3’ NFAT 5’-AGAGCTATCCTTTTGTTTTCCATCCTG-3’ Oct-1 5’-GATCCGAGCTTCACCTTATTTGCATAAGCGATTGA-3’
Each binding reaction consisted of 15-30 μg of nuclear protein extract, the labelled probe and 2 μg of poly-(dI-dC)(dI-dC) in a buffer containing 10 mM HEPES pH 7.9, 1 mM MgCl2, 50 mM KCl, 1 mM DTT, 0.1 mM EDTA, 10% glycerol, 0.025% NP-40, 0.25 mM PMSF and 1 mM each of aprotinin, leupeptin and pepstatin. The binding reactions were carried out at room temperature for 20 minutes, and the protein-DNA complexes were subsequently separated out by electrophoresis on a 5% polyacrylamide gel in 0.5% Tris-borate-EDTA buffer at 4°C. When appopriate, the DNA binding reactions were pre-

68
incubated for 20 minutes with 1, 10 and 100-mole excesses of non-specific competitor DNAs for competition analysis, or with 1 μg of the antibody indicated for supershift analysis. The non-specific competitor DNAs included double-stranded oligonucleotides containing mutant binding sites for GATA-4, AP-1, SRF, MEF-2, NF-κB and NFAT. After electrophoresis the gels were dried and exposed to PhosphorImager screens (Molecular Dynamics, Sunnyvale, CA, USA), which were scanned using Biorad Molecular Imager FX Pro Plus (Bio-Rad Laboratories, Hercules, CA, USA). All the results were quantified using the Quantity One software.
4.7 Isolation and analysis of RNA (I-IV)
Cytoplasmic RNA was extracted from the ventricular tissue by the guanidine isothiocyanate-CsCl method (Chirgwin et al. 1979). For the northern blot analyses, 20 μg samples of RNA were separated out by electrophoresis and transferred to nylon membranes (Osmonics, Westborough, MA, USA). The PCR-amplified cDNA probes for rat ANP, BNP, c-fos, GATA-4, connective tissue growth factor (CTGF), tissue inhibitor of metalloproteinase-1 (TIMP-1), plasminogen activator inhibitor-1 (PAI-1), and ribosomal 18S RNA were random primer-labelled with [α32P]-dCTP. The membranes were hybridised overnight and exposed to PhosphorImager screens, which were scanned by Molecular Imager FX Pro Plus and quantified using the Quantity One software. The hybridisation signals of the specific mRNAs were normalised to that of 18S RNA in each sample to correct differences in loading and/or transfer.
Bone morphogenetic protein (BMP-2), c-fos, aFGF, bFGF, osteopontin, PDGF-A, TGF-β2 and VEGF-A mRNA levels were analysed by the real-time quantitative reverse transcription-polymerase chain reaction (RT-PCR) method. The first cDNA strand was synthesised from 0.5 μg of RNA, and the reactions were performed using TaqMan chemistry on an ABI 7700 Sequence Detection System (Applied Biosystems). The sequences of the forward and reverse primers and probes for RNA detection are shown in Table 6. The results were normalised to 18S RNA quantified from the same samples.

69
Table 6. Forward and reverse primers used for real time quantitative RT-PCR.
Probe Sense primer Anti-sense primer
Fluorogenic Probe
BMP-2 ACACCGTGCTCAGCTTCCAT GTCGGGAAGTTTTCCCACTCA
ACGAAGAAGCCATCGAGGAACTTTCAGAA
c-fos GGCTGAACCCTTTGATGACTTC GGGCAGTCTCCGAGCCA
TGTTTCCGGCATCATCTAGGC
aFGF ATGGCACCGTGGATGGG TTTCCGCACTGAGCTGCAG
AGGGACAGGAGCGACCAGCACATTC
bFGF CCCGGCCACTTCAAGGAT GATGCGCAGGAAGAAGCC
CCAAGCGGCTCTACTGCAAGAACGG
Osteopontin AATCGCCCCCACAGTCG CCTCAGTCCGTAAGCCAAGC
TGTCCCTGACGGCCGAGGTGA
PDGF-A CGAGCGACTGGCTCGAA GAGTCTATCTCCAAGAGTCGCTGG
TCAGATCCACAGCATCCGGGACC
TGF-β2 ACCTTTTTGCTCCTGCATCTG GTCGAGGGTGCTGCAGGTA
TCCCGGTGGCGCTCAGTCTGT
VEGF-A GATCCGCAGACGTGTAAATGTTC TTAACTCAAGCTGCCTCGCC
TGCAAAAACACAGACTCGCGTTGCA
18S TGGTTGCAAAGCTGAAACTTAAAG AGTCAAATTAAGCCGCAGGC
CCTGGTGGTGCCCTTCCGTCA
4.8 DNA microarrays (III)
RNA (7 µg) was used as a template for synthesising cDNA and for making biotinylated cRNA according to the manufacturer’s instructions (Affymetrix, Santa Clara, CA) (Rysä et al. 2005). The biotinylated cRNA was hybridised to the GeneChip Rat Expression Set 230_2.0 Array, which represents approximately 30,000 rat transcripts, and the arrays were scanned with GeneChip Scanner 3000. The complete data set is available from the NCBI’s Gene Expression Omnibus database and the gene expression profiling data comply with the MIAME standard. Affymetrix CEL files were imported into GeneSpring 7.2 software (Silicon Genetics) and RMA normalization was performed. The genes were defined as differentially expressed if the change was at least 2.0-fold and statistically significant.
4.9 Histological analysis (III, IV)
For histological analyses the hearts were fixed in 10% buffered formalin solution, transversal sections of the left ventricle were embedded in paraffin, and 5-µm sections were cut. These were first stained with haematoxylin and eosin, and then with Masson’s trichrome and Sirius red, to visualise fibrosis. The fibrotic area of the left ventricle and the infarct size were determined from the Masson’s trichrome-stained histological

70
sections using a digital image analysis system (MCID/M4 with software version 3.0, Imaging Research, St. Catharines, Canada).
Endothelial cells were visualised by staining with biotinylated lectin GSL1 (Meoli et al. 2004). After deparaffinisation and incubation with HRP-streptavidin, the peroxidase label was developed using a peroxidase-conjugated EnVision Detection Kit system and the samples were counterstained with haematoxylin. The area covered by microvessels was measured from the lectin-stained sections using the MCID/M4 software. The number of capillaries was measured in five representative high power fields (HPF) (40 x objective) located in the peri-infarct area of each histological section.
In order to detect apoptotic cells, in situ labelling of the 3' ends of the DNA fragments generated by apoptosis-associated endonucleases was performed using a commercially available ApopTag in situ apoptosis detection kit, as previously described (Soini et al. 1996). Tissue sections from hyperplastic lymph nodes were used as positive controls. The apoptotic cells and bodies were counted in 5 HPFs located in the infarcted regions, choosing hot-spot areas in each sample. For detection of caspase-3 positive cells, a specific antibody for cleaved caspase-3 was used. To identify cells undergoing division, immunohistochemical labeling of nuclear Ki-67 antigen was performed by using monoclonal mouse anti-rat Ki-67 antigen antibody. To identify cellular localization of p38, GATA-4, and IL-6, immunohistochemistry by using anti-GATA-4, anti-IL-6 or anti-p38 specific antibodies were performed.
Immunohistochemical staining with a C-kit antibody was used to stain stem-like cells in the myocardium. Briefly, paraffin-embedded sections were deparaffinised in xylene and dehydrated in graded ethanol and incubated with a C-kit antibody. The peroxidase label was developed using a peroxidase-conjugated EnVision Detection Kit system and the samples were counterstained with haematoxylin. The number of c-kit positive stem-like cells in the anterior wall of the left ventricle was counted.
To confirm the efficiency of adenovirus-mediated gene transfer, X-gal staining of the Lac Z -treated hearts was performed. The hearts were rinsed in phosphate-buffered saline (PBS) and fixed in PBS containing 4% paraformaldehyde for 10 min at room temperature, washed twice in 0.15 M sodium phosphate buffer (pH 7.2) for 15 min and incubated with 1 mg/ml X-gal at 37°C for 3 hours. The hearts were photographed, and samples for frozen sections were embedded in OCT compound, frozen and sectioned.
4.10 Statistical analysis
The results are expressed as means ± standard error of the mean (SEM). Student’s t-test was used to compare two groups in terms of statistical significance. One-way analysis of variance (ANOVA) followed by a least significant difference (LSD) post hoc test (II-IV) and Kruskal Wallis test (I) were used to compare multiple groups. The Welch t-test accompanied by assessment of the Benjamini and Hochberg false discovery rate was used to analyse the microarray data. A P value of <0.05 was considered statistically significant.

5 Results
5.1 Activation of cardiac transcription factors by increased wall stress (I, II)
To study the effect of mechanical stress on cardiac transcription factors, isolated perfused rat hearts were subjected to increased wall stress by inflating a fluid-filled balloon in the left ventricle. This resulted in a rapid elevation of left ventricular systolic pressure corresponding to a wall stress of 140-150 kdyn/cm2. Coronary flow and perfusion pressure were maintained at the same level in all the experimental groups, and hearts with flaccid left ventricular balloons served as controls. This approach allows determination of the direct mechanical effects of left ventricular wall stress in the absence of confounding systemic factors.
5.1.1 Wall stress rapidly activates GATA-4 and AP-1 binding
Elevation of wall stress for 30 minutes increased GATA-4 DNA binding 1.7-2.0-fold and AP-1 binding 1.8-fold. The activation of GATA-4 binding appeared to be rapid and transient in nature, since no significant differences were observed after 1 hour or 2 hours of increased wall stress. A significant increase in AP-1 binding was noted at 2 hours. No significant increases in NF-κB, NFATc or Oct-1 binding were observed.
The specificity of the GATA-4 and AP-1 DNA binding reactions were confirmed by supershift and competition analysis. The formation of GATA-4-DNA complexes was inhibited in a dose-dependent manner in the presence of unlabelled self DNA, whereas it remained unaffected by a competitor DNA with a mutant GATA binding site or by the non-related competitor Oct-1. Furthermore, an antibody-induced supershift was observed when DNA binding reactions were pre-incubated with GATA-4 specific IgG antibody, but not with GATA-5 or GATA-6 antibody, suggesting that GATA-4 is the main GATA protein bound by the -90 BNP GATA probe. Similarly, AP-1 binding was attenuated by the unlabelled self probe, but not by the probe with a mutant AP-1 binding site or by Oct-

72
1. The presence of AP-1 components in the complex bound by the oligonucleotide probe was demonstrated by supershift analysis, which showed an antibody-induced supershift brought about by c-fos antibodies.
5.1.2 Activation of cardiac gene expression by left ventricular wall stress
To study the functional significance of transcription factor activation in the isolated heart, left ventricular mRNA levels of BNP and c-fos were measured in hearts stimulated by wall stress. The two-hour left ventricular wall stress resulted in a 1.6-2.0-fold increase in BNP gene expression and a 2.1-fold increase in c-fos gene expression, while a one-hour period of wall stress caused a 1.2-fold increase in the former and a 3.0-fold increase in the latter. Furthermore, left ventricular BNP mRNA levels showed a significant positive correlation with left ventricular developed pressure (R=0.73), suggesting that BNP mRNA levels are dependent on the active generation of an acute increment in left ventricular systolic force and wall stress. In contrast to BNP and c-fos, no significant differences in the levels of GATA-4 mRNA were observed in response to left ventricular wall stress.
5.1.3 Paracrine/autocrine mechanisms of wall stress-induced GATA-4 and AP-1 activation
In order to determine the role of paracrine mechanisms in the activation of GATA-4 and AP-1 transcription factors induced by wall stress, the mixed ETA/ETB receptor antagonist bosentan and the AT1 receptor antagonist CV-11974 were added to the perfusion buffer in the absence and presence of increased wall stress. The doses were chosen based on previous studies employing a similar experimental setup (Magga et al. 1997a). Treatment with either bosentan or CV-11974 had no effect on baseline GATA-4 or AP-1 DNA binding in the absence of wall stress, but treatment with bosentan at a concentration of 1 μM and with 10 nM CV-11974 completely abolished the increase in GATA-4 and AP-1 DNA binding induced by wall stress. The haemodynamic variables, perfusion pressure, left ventricular systolic pressure, left ventricular developed pressure or left ventricular end-diastolic pressure, did not differ between the experimental groups, suggesting that the inhibition of GATA-4 and AP-1 DNA binding activity is not related to secondary haemodynamic effects of bosentan or CV-11974.
The direct role of paracrine/autocrine ET-1 and angiotensin II was further investigated by infusing these at various concentrations in the absence of wall stress. This resulted in a dose-dependent increase in GATA-4 and AP-1 binding in both cases. GATA-4 binding was increased 2.2 fold with 1 nM of ET-1 and 2.7-fold with 10 nM angiotensin II.

73
5.2 Regulation of wall stress-induced GATA-4 activity by p38 MAPK and ERK 1/2 (II)
5.2.1 Activation of p38 MAPK and ERK 1/2 by left ventricular wall stress
The isolated perfused rat heart approach was chosen to determine the role of MAPKs in the regulation of load-induced GATA-4 binding. Isolated perfused rat hearts were first subjected to increased wall stress for 10 minutes and MAPK levels were assessed by western blotting. The increased wall stress resulted in a 2.3-fold increase in phospho-p38 levels, a 1.6-fold increase in phospho-ERK 1/2 levels and a 1.9-fold increase in phospho-JNK levels. No significant differences in total p38, total ERK 1/2 or total JNK were observed.
To study the role of increased local production or release of angiotensin II and ET-1 in conjunction with the wall stress-induced activation of MAPKs, the hearts were perfused for 10 minutes in the presence of 1 μM bosentan and 100 nM CV-11974. Neither bosentan nor CV-11974 had any effect on the wall stress-induced increase in phospho-p38 and phospho-ERK 1/2 levels, suggesting that paracrine ET-1 and angiotensin II are not involved in the stretch-induced activation of MAPKs.
5.2.2 Effect of pharmacological p38 MAPK and ERK 1/2 inhibition on GATA-4 binding
Selective inhibitors of the p38 MAPK, ERK and JNK signalling pathways were used to evaluate the role of MAPKs in stress-induced GATA-4 binding. A second-generation small molecule inhibitor of p38 MAPK, SB239063, was chosen to modulate p38 activity, ERK activity was modulated by a selective MEK 1/2 inhibitor U0126, and JNK activity by a novel MLK inhibitor CEP-11004. The effects of the inhibitors on kinase activities were first verified in western blot and kinase assay analyses. SB239063 at a concentration of 10 μM was able to abrogate the stretch-induced activation of p38 MAPK completely in an ELK-1 based kinase activity assay, the c-Jun based kinase assay of JNK activity similarly showed a marked inhibition of JNK activity by 100 nM CEP-11004, while treatment with U0126 significantly lowered phospho-ERK levels in western blot analysis. The selectivity of the compounds was further confirmed by cross-testing ERK activity in the SB239063-treated hearts and p38 MAPK activity in the U0126-treated hearts, whereupon no effects were observed.
Next, the isolated rat hearts were perfused for 30 minutes in the presence and absence of increased wall stress and continuous infusions of SB239063, U0126 and CEP-11004 at the above-mentioned concentrations were added to the perfusate. The wall stress-induced increase in the DNA binding of GATA-4 was completely abolished by treatment with SB239063 and with U0126, but in contrast to p38 MAPK and ERK inhibition, activation

74
of GATA-4 binding remained unaffected by JNK inhibition. Infusion of either SB239063, U0126 or CEP-11004 had no effect on baseline GATA-4 binding (Fig. 5). These findings indicate that p38 MAPK and ERK activity are required for wall stress-induced GATA-4 activation, whereas induction of JNK is not critical.
The role of p38 MAPK and ERK in the regulation of stretch-induced GATA-4 binding was further examined in isolated rat atrium preparations, by stretching isolated left auricles at 8 cmH2O for 30 minutes, which resulted in a 2.0-fold increase in GATA-4 DNA binding activity. In agreement with the findings in the isolated perfused rat hearts atrial stretch-induced GATA-4 binding was dependent on p38 MAPK and ERK, since the stretch-induced increase was significantly reduced by treatment with the small molecule p38 MAPK inhibitor SB203580 (5 μM) and with the ERK inhibitor PD98059 (5 μM).
Fig. 5. Effect of MAPK inhibitors on left ventricular wall stress-induced activation of GATA-4 binding. Gel mobility shift assays of hearts perfused in the presence of MAPK inhibitors. C indicates control, S indicates increased wall stress. The results are expressed as means±SEM (n=10-13). *P<0.05, ***P<0.001 vs. unstretched control, §§P<0.01 vs. vehicle-infused stretch.
5.2.3 Effect of PKC and Rho kinase inhibition on GATA-4 binding
In view of the previous in vitro findings concerning the upstream kinases of p38 MAPK and ERK, the role of selected upstream kinases in mediating wall stress-induced GATA-4 binding was studied (Kyriakis & Avruch 2001). The involvement of Rho kinase was studied by infusing Y-27632, a selective inhibitor of Rho-dependent kinases, at a concentration of 3 μmol/L during left ventricular wall stress, upon which the wall stress-induced activation of GATA-4 DNA binding was significantly attenuated, suggesting a Rho-dependent upstream mechanism for GATA-4 activation. The baseline GATA-4 binding remained unaffected by Y-27632.
To investigate the role of PKC in stretch-induced GATA-4 binding, the hearts were perfused in the presence of 90 nmol/L of bisindolylmaleimide I (GF-109203X), a potent PKC inhibitor. The stress-induced binding was not affected, although there was a tendency for increased baseline GATA-4 binding. The role of intracellular signalling

75
pathways in the regulation of wall stress–induced GATA-4 binding is summarised in Figure 6.
Fig. 6. Summary of the pathways regulating wall stress-induced GATA-4 binding
5.3 Functional role of p38 MAPK in the intact heart (III)
5.3.1 Activation of p38 MAPK by adenovirus-mediated gene transfer
To gain further insights into the downstream targets and physiological effects of p38 MAPK in the heart, a gene transfer protocol of increased p38 MAPK activity was established. In order to determine the conditions under which maximal p38 MAPK up-regulation is achieved, several combinations of MKK3bE, MKK6bE, WT p38α and WT p38β adenoviruses were first tested. The control animals in all the series of experiments received gene transfer of a replication-deficient adenovirus RAdlacZ at an appropriate concentration. Injection of MKK3bE at 6 x 108 pfu together with 2 x 108 pfu of WT p38α produced the strongest activation of p38 MAPK (Fig. 7). The specificity of MKK3bE and WT p38α gene transfer with respect to p38 MAPK was confirmed by western blot analysis using antibodies against ERK and JNK. Here the levels of phospho-ERK, total ERK, phospho-JNK and total JNK in the hearts injected with MKK3bE + WT p38α were similar to those in the Lac Z -treated hearts.The efficiency of protocol was established by X-gal staining of the Lac Z -injected hearts, which showed a large transmural staining area in the anterior wall of the left ventricle.

76
Baseline cardiac function did not differ between the MKK3bE + WT p38α and Lac Z -treated hearts, since no statistically significant differences in left ventricular fractional shortening, ejection fraction or left ventricular diameter were observed as assessed by echocardiography on day 3 after injection.
Fig. 7. Selective activation of p38 MAPK by adenovirus-mediated gene transfer. Western blot analysis of MAPK levels 3 days after gene transfer. The results are expressed as means±SEM (n=8-9). *P<0.05, **P<0.01 vs. Lac Z.
5.3.2 Up-regulation of cardiac gene expression by p38 MAPK: a DNA microarray analysis
To examine the role of p38 MAPK in cardiac gene expression, the gene expression profiles of hearts over-expressing MKK3bE + WT p38α (n=5 animals/group) were examined by DNA microarray analysis and compared with those of Lac Z –treated animals by screening Affymetrix Rat Expression Set 230_2.0 Arrays obtained 3 days after gene transfer, at which point the maximal p38 MAPK up-regulation was observed.
The microarray analysis identified 264 transcripts that were up-regulated more than 2.0-fold in the hearts over-expressing p38 MAPK. For further analysis of the data, these genes were organised into groups representing their main biological functions: apoptosis, cell adhesion, cell division, cell signalling/communication (subgrouped into hormones and growth factors, intracellular transducers, protein modification and receptors), cell structure/motility, cell/organism defence, channel/transport proteins, inflammatory and immune responses, metabolism (subgrouped into amino acid, carbohydrate, lipid, nucleotide and nucleic acid metabolism), protein synthesis/turnover/post-translational modification, transcription factors, translation factors, unclassified and expressed

77
sequence tags (ESTs) and other unknown transcripts. Of the genes of known biological function, three major groups of p38 MAPK sensitive genes could be distinguished: genes related to cell division (31 genes), cell signalling (28 genes) and inflammatory response (23 genes). In addition, a large number of genes with unknown biological function (69 ESTs and 35 unclassified genes) were differentially expressed in the hearts over-expressing p38 MAPK and the Lac Z -treated hearts (Fig. 8). Notably, only two cardiac genes (for pyruvate dehydrogenase kinase isoenzyme 4 and gap junction membrane channel protein α1) were down-regulated by p38 MAPK over-expression. When the microarray analysis was extended to include genes that were up-regulated 1.5-2.0–fold in hearts with p38 MAPK overexpression, 651 additional transcripts were identified, the majority of which belonged to the groups of unknown function and ESTs.
Fig. 8. Functional classification of p38 MAPK target genes in the left ventricle.
The individual genes that were differentially expressed in the Lac Z and p38 MAPK over-expressing hearts included several novel p38 targets as well as a number previously reported p38-dependent genes. In the cell division category, genes encoding cyclins, kinesins and polo-like kinases etc. were up-regulated. Many of the genes in the cell adhesion and signal transduction category, such as those for osteopontin, CTGF and TGF-β, appeared to be related to myocardial fibrosis, while the inflammatory gene category included several central regulators of both innate and adaptive immunity, such as interleukins. In addition, the microarray analysis identified several transcription factors which have not previously been known as p38 MAPK targets. These included ATF-3, Runx1 and Krox20.

78
5.3.3 Northern blot and RT-PCR analysis of microarray results
To confirm the microarray analysis results regarding p38 MAPK induced gene expression, the expression levels of selected cardiac genes were assessed by RT-PCR and northern blot analysis. Consistent with the microarray data, significant increases in BMP-2, c-fos, bFGF, osteopontin and TGF-β2 mRNA levels upon p38 MAPK over-expression were observed as assessed by RT-PCR. Similarly, northern blot analysis showed a significant up-regulation of ANP, BNP, CTGF, TIMP-1 and PAI-1 gene expression.
5.3.4 Activation of GATA-4 by p38 MAPK over-expression
To evaluate the direct effects of p38 MAPK on GATA-4 activity, nuclear protein extraction and gel mobility shift assays were performed on Lac Z and MKK3bE + WT p38α –treated animals 3 days after gene transfer. Gel mobility shift assays using the -90 BNP GATA-4 probe showed a significant 1.6-fold activation of GATA-4 binding. Consistent with the results obtained with wall stress-stimulated hearts, supershift and competitor analysis showed reduced DNA binding activity with the unlabelled self probe or GATA-4 antibody but unchanged binding with GATA-5 and GATA-6 antibodies and with mutant or non-related probes.
Furthermore, GATA-4 mRNA levels remained stable in the hearts over-expressing p38 MAPK, suggesting that up-regulation of GATA-4 DNA binding is not related to increased production of GATA-4 mRNA or protein.
5.3.5 Activation of other cardiac transcription factors by p38 MAPK
The specificity of p38 MAPK over-expression with respect to GATA-4 was investigated by studying the DNA binding activities of other selected cardiac transcription factors after MKK3bE + WT p38α gene transfer. EMSAs using oligonucleotide probes containing the binding sites for MEF-2, AP-1, NF-κB and SRF were performed, and significant increases in AP-1 (4.5-fold), NF-κB (1.7-fold) and SRF binding (1.4-fold) were observed in response to p38 MAPK over-expression, while the DNA binding of MEF-2 was unaffected (Fig 9).
The specificities of the AP-1, MEF-2, NF-κB and SRF DNA binding reactions were determined in supershift and competition analysis. In all cases the binding was attenuated by unlabelled self DNAs but not by mutant or non-related competitor DNAs. Antibody-induced supershifts were observed for AP-1, MEF-2, NF-κB and SRF, demonstrating that the complexes bound by the oligonucleotide probes contained AP-1, MEF-2, NF-κB and SRF protein components.

79
Fig. 9. p38 MAPK as a convergence point for myocardial signalling. p38 MAPK activates GATA-4, AP-1, NF-κB and SRF, which further transmit the signal to bring about changes in cardiac gene expression.
5.3.6 Function of hearts over-expressing p38 MAPK
The physiological consequences of p38 MAPK over-expression were first investigated by assessing cardiac function by echocardiography 1 week after gene transfer. The parameters of cardiac function did not differ significantly between the hearts injected with Lac Z- and MKK3bE + WT p38α, although a tendency for worsened EF (67% vs. 77%) and FS (32% vs. 41%) was observed in those that received MKK3bE + WT p38α. This was accompanied by a small but significant increase in left ventricular weight vs. body weight (LW/BW) ratio (3.3 vs. 3.0 mg/g), without a significant change in body weight.
5.3.7 Inflammation
To determine the morphological changes caused by p38 MAPK over-expression, histological analysis was performed. The haematoxylin-eosin stained histological sections showed notable anterior wall thickening and a massive infiltration of inflammatory cells into the interstitium of the anterior wall. Morphological analysis showed lymphocytes to be the dominant inflammatory cell type (Fig. 10).

80
5.3.8 Fibrosis
To investigate whether the anterior wall thickening observed upon haematoxylin-eosin staining was due to increased myocardial fibrosis, the histological sections were stained with Sirius Red and Masson’s trichrome. Both showed extensive staining in the injection area, indicating that p38 MAPK over-expression in the normal heart is a cause of myocardial fibrosis.
Fig. 10. Fibrosis and inflammatory cell infiltration in myocardium over-expressing p38 MAPK. Representative histological sections stained with Masson’s trichrome from Lac-Z –treated (left panel) and MKK3bE+ WT p38α –treated (right panel) hearts are shown.
5.3.9 Proliferation
Expression of Ki-67, which is required for cells to progress through the cell cycle and undergo division, is detectable in the G1 phase, increases in the S and G2 phases and continues through mitosis. Ki-67 is considered a specific marker of cellular proliferation, as all cells that express it divide (Yuasa et al. 2004). Since the microarray analysis revealed increased expression of several genes that were associated with proliferation, immunohistochemical Ki-67 staining was performed to study whether increased cell division is observed in response to p38 MAPK over-expression.

81
The Ki-67-stained histological sections of hearts over-expressing p38 MAPK showed a large number of staining-positive cells in the anterior wall, whereas very few Ki-67 positive cells were observed in the Lac Z -treated hearts.
5.4 Role of p38 MAPK in the infarcted heart (IV)
5.4.1 Haemodynamic changes after myocardial infarction
To study the role of myocyte signal transduction pathways and transcription factors after myocardial infarction, the LAD was ligated in a group of Sprague-Dawley rats (Pfeffer et al. 1979). Cardiac function was assessed by echocardiography at 1 day, 2 weeks and 4 weeks after myocardial infarction. Ejection fraction and fractional shortening values decreased progressively and the left ventricle became dilated during the four-week follow-up period (Table 7). Haematoxylin-eosin staining of the myocardial sections showed progressive anterior wall thinning, left ventricular dilatation and posterior wall hypertrophy in the infarcted hearts.
Cardiac gene expression was measured in order to further validate the experimental model. Left ventricular ANP mRNA levels were increased 3.9-fold one day after myocardial infarction and had increased further at 2 and 4 weeks (6.2-fold and 17.0-fold vs. sham-operated rats, respectively). Similarly, myocardial infarction resulted in a 1.7-fold increase in left ventricular BNP gene expression on day 1 and a 1.5-fold increase after 4 weeks. The levels of ANP and BNP mRNA in the right ventricles of the infarcted hearts also increased significantly (9.9-fold and 3.7-fold vs. sham on day 1, respectively).
Table 7. Haemodynamic parameters after myocardial infarction.
Variable Group 1 day 2 weeks 4 weeks Interventricular septum diastole (mm)
Sham AMI
1.9 ± 0.1 1.8 ± 0.1
1.8 ± 0.1 1.3 ± 0.1***
1.8 ± 0.1 1.1 ± 0.1***
Left ventricle diastole (mm)
Sham AMI
7.2 ± 0.1 8.1 ± 0.2***
8.6 ± 0.1 9.7 ± 0.2***
9.1 ± 0.1 11.1 ± 0.2***
Posterior wall diastole (mm)
Sham AMI
1.8 ± 0.1 1.9 ± 0.1
1.8 ± 0.1 1.9 ± 0.1
1.8 ± 0.1 2.0 ± 0.1**
Ejection fraction (%) Sham AMI
83 ± 1 46 ± 4***
77 ± 2 47 ± 3***
75 ± 1 30 ± 3***
Fractional shortening (%) Sham AMI
47 ± 1 21 ± 2***
42 ± 1 21 ± 2***
39 ± 1 13 ± 2***
AMI = acute myocardial infarction. **P<0.01, ***P<0.001 vs. sham.

82
5.4.2 Inactivation of p38 MAPK after myocardial infarction
To analyse the role of MAPKs in post-infarction remodelling, MAPK activities were determined by western blot analysis at several time points. p38, ERK and JNK showed differential activities during post-infarction remodelling. Only p38 MAPK activity was consistently down-regulated (Fig. 11A). The phospho-p38 vs. total p38 ratio had decreased by 76% compared with the sham-operated controls on day 1 after myocardial infarction, and by 43% at 2 weeks, but by four weeks p38 activity had returned to baseline and no statistically significant difference was observed between the sham-operated animals and those with myocardial infarction. The changes in p38 MAPK activity were further investigated in ATF-2 based kinase assays, which showed changes corresponding to the phospho-p38 levels at each time point.
To analyse the upstream mechanisms responsible for the altered p38 MAPK activity, levels of MKK3 were studied in western blot analysis. Consistent with the down-regulation of p38 MAPK activity, phospho-MKK3 levels were reduced after myocardial infarction. Next, regional changes in p38 MAPK activity were studied by performing western blot analyses on protein extracted from the infarcted anterior ventricular wall and non-infarcted posterior wall. Both regions showed decreased p38 MAPK activity 1 day after myocardial infarction, although more pronounced inactivation was observed in the infarcted area.
In contrast to p38 MAPK activity, ERK 1/2 activity remained unaffected 1 day after myocardial infarction and had increased 1.5-fold by 2 weeks. At 4 weeks, the phospho-ERK vs. total ERK levels of the infarcted hearts did not differ significantly from those of the sham-operated animals. The activation of ERK 1/2 was further established in ELK-1-based kinase assays, which showed notable activation 2 weeks after myocardial infarction. Although the phospho-JNK vs. total JNK ratio was increased 3.1-fold on day 1 and had decreased by 37% at 2 weeks, these changes appeared to be a consequence of altered total JNK levels. No statistically significant difference in JNK levels was observed at 4 weeks.
5.4.3 Restoration of p38 MAPK activity by adenovirus-mediated gene transfer
Since post-infarction remodelling was characterised by sustained down-regulation of p38 MAPK activity, a gene transfer protocol was established to restore this activity. The strongest up-regulation of p38 MAPK activity in the normal heart was observed when an adenovirus encoding MKK3bE was co-injected with that encoding WT p38α. This combination was chosen in order to reverse the decreased p38 MAPK levels in the infarcted hearts. MKK3bE at 6 x 108 pfu was co-injected with 2 x 108 pfu of WT p38α into the anterior wall of the left ventricle prior to ligation of the LAD. MAPK levels were assessed by western blotting 3 days after myocardial infarction and gene transfer. Interestingly, the levels of phospho-p38 MAPK in MKK3bE + WT p38α -treated animals with myocardial infarction did not significantly differ from those in the Lac Z -treated

83
animals, indicating that this gene transfer protocol is able to restore p38 MAPK activity completely in the infarcted heart (Fig. 11B). There was no difference in the perioperative mortality between the Lac Z -treated and MKK3bE + WT p38α -treated animals.
Fig. 11. A. Down-regulation of p38 MAPK activity in post-infarction remodelling. B. Rescue of p38 MAPK levels by adenovirus-mediated gene transfer of MKK3bE + WT p38α. Western blot and kinase assay analysis of p38 MAPK levels on day 3 after myocardial infarction and gene transfer. The results are expressed as means±SEM (n=6-8). **P<0.01, ***P<0.001 vs. sham, §P<0.05 vs. Lac Z –injected animals with myocardial infarction.
5.4.4 Rescue of cardiac function in hearts over-expressing p38 MAPK during post-infarction remodelling
The functional consequences of normalised p38 MAPK activity were studied by echocardiography at two time points, 3 days and 2 weeks post infarction. p38 MAPK activity normalisation did not have any apparent effect on cardiac function at 3 days, since EF, FS and left ventricular diameter did not differ significantly between the Lac Z

84
and MKK3bE + WT p38α –treated animals, but the MKK3bE + WT p38α –treated animals showed a significant improvement in cardiac function at 2 weeks (Fig. 12). EF and FS were increased by 50% (66.9±5.5% vs. 44.4±4.0%, and 19.7±2.2% vs. 30.2±2.1%, respectively). The left ventricular diastolic diameter was significantly smaller in the MKK3bE + WT p38α –treated hearts (8.5±0.4 mm vs. 9.5±0.2 mm), indicating that the gene transfer attenuated left ventricular dilatation. The LW/BW ratio was significantly reduced, without a significant difference in the body weight.
Fig. 12. Rescue of cardiac function after restoration of decreased p38 MAPK activity. EF, FS and LW/BW 2 weeks after myocardial infarction and gene transfer. The results are expressed as means±SEM (n=6-8).*P<0.05, ***P<0.001 vs. sham, §§§P<0.001 vs. Lac Z –injected animals with myocardial infarction.
5.4.5 Normalisation of p38 MAPK activity reduces infarct size, apoptosis and fibrosis
To study whether the improved cardiac function in MKK3bE + WT p38α –treated hearts was related to attenuation of the structural remodelling of the heart, histological sections were stained with Masson’s trichrome and Sirius Red. The MKK3bE + WT p38α –treated hearts showed less left ventricular dilatation, anterior wall thinning and posterior wall hypertrophy in these stained sections 2 weeks after myocardial infarction (Fig. 13), and the size of the infarcted area, assessed from left ventricular circumference, was accordingly significantly smaller (26±3% vs. 47±4%). Furthermore, left ventricular fibrosis was significantly attenuated (16±3% vs. 34±8%), as assessed from the positive area in the Masson’s trichrome-stained sections.
The rate of apoptosis was evaluated by TUNEL 3 days and 2 weeks after myocardial infarction. The number of apoptotic cells was significantly reduced in the MKK3bE + WT p38α –treated hearts at 3 days (35 cells vs. 69 cells in Lac Z -treated hearts), while no difference was observed at the later time point. The number of c-kit positive stem-like cells did not differ, either.

85
Fig. 13. Attenuation of left ventricular fibrosis, infarct size and apoptosis by p38 MAPK gene transfer 2 weeks after myocardial infarction. Infarcted and fibrotic areas were assessed from histological sections stained with Masson’s trichrome and the number of apoptotic cells by TUNEL. The results are expressed as means±SEM (n=6-8). ***P<0.001 vs. sham, §P<0.05, §§P<0.01 vs. Lac Z –injected animals with myocardial infarction.
5.4.6 Enhanced coronary angiogenesis in hearts over-expressing p38 MAPK
Since coronary angiogenesis is a critical determinant of post-infarction remodelling (Tabibiazar & Rockson 2001), myocardial sections were stained with Lectin GSL to determine whether MKK3bE + WT p38α gene transfer treatment affected the angiogenic responses after myocardial infarction. The MKK3bE + WT p38α –treated hearts with myocardial infarction had a significantly higher capillary density than the Lac Z-treated hearts (Fig. 14, 2423±107 vs. 1935±86). Furthermore, a notable dilatation of the capillary network was observed and the area covered by microvessels had increased 1.5-fold. A tendency for increased capillary density, although not statistically significant relative to the Lac Z -treated hearts, was observed in the MKK3bE + WT p38α –treated hearts without myocardial infarction.
The angiogenic responses to p38 MAPK over-expression were further investigated by measuring the mRNA levels of selected angiogenic growth factors in MKK3bE + WT p38α –treated hearts. p38 MAPK over-expression increased the levels of bFGF (2.3-fold vs. Lac Z) and PDGF-A mRNA (1.7-fold vs. Lac Z), while those of VEGF remained unchanged.

86
Fig. 14. Enhanced coronary angiogenesis in hearts over-expressing p38 MAPK. Capillary density and area covered by microvessels as assessed from lectin-stained histological sections 2 weeks after myocardial infarction and gene transfer. The results are expressed as means±SEM (n=6-8). *P<0.05, ***P<0.001 vs. sham, §§§P<0.001 vs. LacZ –injected animals with myocardial infarction.
5.5 Altered GATA-4 binding during post-infarction remodelling
5.5.1 Transient inactivation of GATA-4 binding after myocardial infarction
Myocardial GATA-4 DNA binding activity was assessed by EMSA using a 30-bp oligonucleotide probe containing the -90 GATA sites of the rat BNP promoter 1 day, 2 weeks and 4 weeks after myocardial infarction. The DNA binding activity of left ventricular nuclear extracts and the oligonucleotide probe had decreased by 69% on day 1 in the infarcted rat hearts (Fig. 15), but this was followed by a 2.4-fold up-regulation 2 weeks after the myocardial infarction. The binding returned to baseline within 4 weeks of the infarction.
5.5.2 AP-1, NF-κB and SRF binding activities after myocardial infarction
In contrast to GATA-4 DNA binding, myocardial infarction caused a sustained increase in AP-1 DNA binding activity, which had increased significantly after 1 day (6.0-fold vs. sham-operated rats), and remained 4.1-fold higher at 2 weeks and 2.0-fold higher at 4 weeks. Like GATA-4 binding, a 39% decrease in NF-κB binding activity was observed on day 1, a significant increase at 2 weeks (1.7-fold vs. sham) and a return to baseline at 4 weeks. No differences in SRF binding activity were observed during the 4-week follow-up period (Fig. 15).

87
Fig. 15. Transcription factor activities during post-infarction remodelling as assessed by gel mobility shift assays at different time points. The results are expressed as means±SEM (n=6-8). *P<0.05, **P<0.01,***P<0.001 vs. sham.
5.5.3 p38 MAPK-independent regulation of GATA-4 in the infarcted heart
Finally, the role of p38 MAPK in controlling transcription factor activities was studied in the infarcted heart. A gene transfer of MKK3bE at 6 x 108 pfu and WT p38α at 2 x 108 pfu was performed simultaneously with ligation of the LAD, as described above. The control animals received Lac Z gene transfer at 8 x 108 pfu. GATA-4 binding was assessed by EMSA on day 3 after the injection and myocardial infarction. Although the combined administration of MKK3bE and WT p38α was able to normalise the reduction in p38 MAPK activity completely, the reduction in GATA-4 DNA binding remained unaffected (Fig. 16). However, even though MKK3bE + WT p38α gene transfer did not increase GATA-4 activity, it did further potentiate the activation of NF-κB and AP-1 after myocardial infarction.

88
Fig. 16. Effect of p38 MAPK on cardiac transcription factors in the infarcted heart. DNA binding activities of transcription factors as assessed by gel mobility shift assays 3 days after infarction and gene transfer. The results are expressed as means±SEM (n=6-8). *P<0.05, ***P<0.001 vs. sham, §P<0.05 vs. Lac Z –injected animals with myocardial infarction.

6 Discussion
6.1 Transcription factor activities during wall stress and remodelling
In order to undergo structural remodelling, the individual myocytes of the heart alter their gene and protein expression pattern under the control of cardiac transcription factors, which are essential regulators of inducible gene expression (Akazawa & Komuro 2003). The aim here was to study cardiac transcription factor activities, with special emphasis on GATA-4, in two experimental setups: perfused rat hearts stimulated by wall stress and hearts subjected to experimental myocardial infarction.
Previous in vitro studies have demonstrated that GATA-4 is activated by GPCR agonists (Morimoto et al. 2000, Kitta et al. 2001, Morisco et al. 2001, Kerkelä et al. 2002). GATA-4 activity is sensitive to AVP-induced pressure overload in vivo (Hautala et al. 2001), and both nephrectomised rats and rats that over-express the mouse renin gene exhibit an increase in this activity (Marttila et al. 2001, Diedrichs et al. 2004). The systemic responses evoked by these stimuli in addition to increased blood pressure are diverse, however, and it is difficult to separate the contributions of mechanical and hormonal factors to the models. The present results indicate that mechanical stress per se rapidly activates GATA-4 and AP-1 transcription factors, and that this effect is dependent on both angiotensin II and ET-1, since activation was completely blocked by their receptor antagonists. It thus appears that increased wall stress first stimulates ET-1 production, or more likely, considering the rapid time-course, it stimulates the release of ET-1 from cardiac stores. Angiotensin II may also stimulate ET production and release, which would explain the mutual requirement of both ET-1 and angiotensin II (McClellan et al. 1994). The role of ET-1 and angiotensin II in regulating GATA-4 activity in the isolated heart is further strengthened by the observation that both of them were able to activate GATA-4 in the absence of wall stress. Interestingly, the paracrine signalling mechanisms mediating GATA-4 and AP-1 activation seem to differ between the pressure-overload models and the stretch model used in here. The time-course and increase in GATA-4 activation reported in AVP-infused rats resembled that observed here, but simultaneous AP-1 activation was absent and GATA-4 activation was unaffected by treatment with an AT1 receptor antagonist (Hautala et al. 2001). These differences may be

90
due to the systemic effects of AVP infusion, as discussed above, and to the fact that direct mechanical left ventricular wall stress may trigger different signalling pathways from pressure overload.
It is interesting that, as a stimulus, left ventricular wall stress appears to show specificity with respect to its transcriptional targets. GATA-4 and AP-1 were rapidly activated, but no change was observed in NF-κB and NFAT activities. This is of particular significance considering that NF-κB and NFAT are activated by hypertrophic stimuli in many other models and have both been suggested as essential mediators of the hypertrophic response. The selective activation of GATA-4 and AP-1 further emphasises their role as potential mediators of mechanical stress-induced hypertrophy and heart failure.
To gain further insights into the regulation of GATA-4 under pathophysiological conditions, GATA-4 activity was studied in a model of experimental myocardial infarction. In contrast to increased wall stress, myocardial infarction caused rapid inactivation of GATA-4, which was followed by a corresponding activation during the later phases of post-infarction remodelling. Interestingly, the inactivation of GATA-4 activity was observed at an early point in time post infarction, which is generally associated with significant haemodynamic stress. Thus it appears that GATA-4 is differentially regulated in the normal and the infarcted heart. In support of these findings, reversible ischaemia-reperfusion injury in vitro has recently been shown to down-regulate GATA-4 activity (Suzuki et al. 2004), an effect that does not seem to be restricted to ischaemic injury, since treatment of cultured cardiomyocytes with cardiotoxic anthracyclines such as daunorubicin and doxorubin has been shown to reduce GATA-4 DNA binding activity (Kim et al. 2003, Aries et al. 2004). GATA-4 depletion has recently been identified as an early aspect of the cardiotoxic effect of doxorubicin in vivo as well (Aries et al. 2004). In these studies GATA-4 down-regulation was associated with enhanced cardiomyocyte apoptosis, thereby extending the role of GATA-4 as a cardiac survival factor beyond embryogenesis. The functional significance of the early GATA-4 down-regulation in post-infarction remodelling remains to be studied, but in view of the findings discussed above, it is intriguing to speculate that it could be related to cardiomyocyte survival and apoptotic cell death. The late activation of GATA-4 may also be of functional significance, as the echocardiographic measurements showed significant posterior wall hypertrophy at these time points.
6.2 The role of p38 MAPK in the regulation of GATA-4
GATA-4 protein contains at least 7 potential sites for serine phosphorylation by MAPKs, and in vitro evidence exists from prior studies suggesting that MAPKs are able to control GATA-4 activity under certain experimental conditions (Pikkarainen et al. 2004). The role of MAPKs as regulators of GATA-4 in the adult heart was established here using two alternative experimental approaches.
In Paper II, isolated perfused rat hearts were subjected to increased wall stress in the presence of selective MAPK inhibitors. The activation of GATA-4 binding was preceded by activation of the MAPKs, p38, ERK and JNK, in agreement with previous

91
observations (Takeishi et al. 2001). Interestingly, the wall stress-induced activation of GATA-4 was completely abolished in the presence of either a p38 MAPK or an ERK inhibitor, indicating that the action of both p38 MAPK and ERK is required for activation. These results were confirmed in the isolated rat atria, which showed a similar dependence of stretch-induced GATA-4 binding on ERK and p38 MAPK. These findings are consistent with the fact that PE-stimulated GATA-4 binding in cultured cardiomyocytes is sensitive to ERK inhibition and ET-1-induced binding to p38 MAPK inhibition (Liang et al. 2001b, Kerkelä et al. 2002). On the other hand, ERK inhibition reduced baseline GATA-4 activity but did not affect ET-1-induced activity in cultured cardiomyocytes (Kerkelä et al. 2002).
Several possible explanations at the molecular level may account for the simultaneous requirement of both p38 MAPK and ERK in stretch-induced GATA-4 binding. First, it is likely that mechanical stress is a more complex stimulus than treatment with GPCR agonists, leading to the activation of a more diverse array of intracellular signalling pathways. Second, as mentioned above, GATA-4 protein contains multiple phosphorylation sites for MAPKs. p38 MAPK and ERK may phosphorylate different serine residues, all of which may be required for the stretch-induced activation. Third, it is possible that ERK and p38 MAPK may phosphorylate the same serine residues, such as serine-105, but that the action of both is required to reach a sufficient amount of phosphorylation. Considering the somewhat opposed effects of ERK and p38 MAPK in cardiovascular pathophysiology, the fact that their simultaneous action was required for the full stretch response is of particular interest. The present findings support the role of GATA-4 as a convergence point in signal transduction and imply that p38 MAPK/ERK-mediated activation of GATA-4 could be involved in both beneficial and harmful processes in cardiovascular diseases.
The connection between GATA-4 and p38 MAPK was further investigated in Paper III using adenovirus-mediated p38 MAPK over-expression. Interestingly, this experimental setup served to verify the p38 MAPK dependence of GATA-4. Over-expression of p38 MAPK resulted in an activation of GATA-4 which was quantitatively comparable to that observed in response to increased wall stress or AVP infusion in vivo. It is likely that the activation of GATA-4 is a consequence of p38 MAPK-mediated phosphorylation, since its mRNA levels remained unchanged in the hearts over-expressing p38 MAPK. The results detailed in Paper III nevertheless indicate, consistent with previous studies, that the activating effect of p38 MAPK is not specific to GATA-4, but that a number of other cardiac transcription factors are activated as well (Kyriakis & Avruch 2001). It is therefore not possible to distinguish the role of the p38 MAPK-GATA-4 pathway in cardiac gene expression in this setup. Nevertheless, of the known GATA-4 target genes at least ANP and BNP were up-regulated in response to p38 MAPK over-expression, suggesting that the p38 MAPK-GATA-4 pathway is of functional significance at the level of gene expression. It should also be noted that the ability of p38 MAPK to activate other transcription factors may be dependent on the conditions: p38 MAPK over-expression activated NF-κB, but NF-κB activation was absent in the wall stress-stimulated hearts in spite of simultanous p38 MAPK activation.
Finally, the interaction of p38 MAPK with GATA-4 was studied in the infarcted heart. This experimental approach further highlighted the complexity of the mechanisms regulating GATA-4 in vivo, as GATA-4 did not respond to p38 MAPK over-expression in

92
this case. Several underlying molecular mechanisms may account for this. Other MAPKs may contribute to GATA-4 signalling in the infarcted heart, the translocation of GATA-4 protein may be altered in the infarcted myocardium, or the levels of GATA-4 protein may be down-regulated, as in anthracycline-treated cardiomyocytes (Aries et al. 2004). Also, GATA-4 regulation in the infarcted myocardium may be dominated by interactions with other transcription factors, such as Nkx-2.5, and other post-translational modifications beside MAPK-mediated phosphorylation, so that p38 MAPK fails to up-regulate GATA-4. Interestingly, it seems that there also is a disconnection between p38 and NF-κB, SRF, and AP-1 in the infarcted heart, because AP-1 and NF-κb were activated and SRF remained unaffected at the post-infarction time points at which p38 MAPK was down-regulated. On the other hand, even though p38 MAPK is not required for the activation of AP-1 and NF-κB, they were further activated by p38 MAPK over-expression in the infarcted heart.
6.3 Other mechanisms of GATA-4 regulation
In vivo mechanisms other than MAPK-mediated phosphorylation of GATA-4 remain largely unknown, and the upstream mechanisms that link GATA-4 and MAPKs to extracellular stimuli are not well characterised.
In vitro, activation of GATA-4 by both p38 and ERK appears to be at least partially dependent on Rho signalling, since dominant negative forms of p38 attenuate the Rho A-induced potentiation of GATA-4 activity, and ERK-dependent GATA-4 activation by PE requires Rho kinase (Charron et al. 2001, Yanazume et al. 2002). The role of two selected upstream pathways, PKC and Rho kinase, was studied here in isolated rat hearts, where the stretch-induced GATA-4 binding was inhibited by the Rho kinase inhibitor Y-27632, suggesting that Rho kinase may be the upstream kinase activating p38 MAPK and ERK. On the other hand, GATA-4 binding was not influenced by pharmacological PKC inhibition, suggesting that PKC is not among the upstream pathways of GATA-4. Importantly, the present results do not exclude the possible involvement of interactions and other post-translational mechanisms of GATA-4 regulation in vivo. Notably, p38 and ERK were required to confer the full stretch response of GATA-4, as were ET-1 and angiotensin II. Despite this, ET-1 and angiotensin II receptor antagonists did not abrogate the stretch-induced activation of p38 MAPK and ERK. This evidence taken together suggests that alternative intracellular pathways or mechanisms connecting GATA-4 with ETA/B and AT1 receptors are likely to exist, and alternative pathways also appear to control GATA-4 activity in the infarcted myocardium. Interactions with other transcription factors and co-factors may also affect GATA-4 activity under these conditions. These mechanisms represent logical targets for future investigations.
6.4 The role of p38 MAPK in cardiac gene expression
Even though p38 MAPK is a highly conserved kinase expressed by virtually all eukaryotes, the global gene expression pattern that is dependent on p38 MAPK has

93
remained unknown. In view of findings regarding the ability of p38 MAPK to activate a variety of transcription factors, it was hypothesised that p38 MAPK may represent an essential regulatory convergence point in cardiac gene expression.
Local adenovirus-mediated over-expression of p38 MAPK provides a valuable tool for studying its direct effects on molecular events such as cardiac gene expression. This is of particular importance because transgenic animals over-expressing p38 MAPK exhibit a phenotype of dilated cardiomyopathy which makes it difficult to distinguish the direct effects of p38 MAPK from secondary haemodynamic changes (Liao et al. 2001). The gene expression profile was analysed here at a time point when p38 MAPK was maximally up-regulated without significant haemodynamic or structural changes, whereas previous comprehensive p38 MAPK-related microarray analyses had only been performed in cultured cardiomyocytes and transformed lymphoma cells treated with pharmacological p38 MAPK inhibitors (Lin et al. 2004, Engel et al. 2005). Pharmacological p38 MAPK inhibitors may also have systemic and haemodynamic effects in vivo, and it is difficult to confirm their specificity with respect to a single protein kinase molecule.
DNA microarray analysis identified 264 transcripts that were up-regulated more than 2-fold in the left ventricle over-expressing p38 MAPK relative to Lac Z –injected hearts. When the genes were classified into subgroups representing their biological functions, three groups appeared to dominate the analysis: cell division (31 genes), cell signalling (28 genes) and genes related to an inflammatory response (23 genes). It thus appears that the gene expression profile controlled by p38 MAPK in the heart correlates very well with the biological functions that have generally been connected with p38 MAPK in different cell types. p38 MAPK responds strongly to pro-inflammatory stimuli and is involved in the pathogenesis of inflammatory diseases such as arthritis, septic shock and chronic obstructive pulmonary disease (Kyriakis & Avruch 2001, Saklatvala 2004). Second, p38 MAPK is by definition a mitogen-activated protein kinase that controls processes related to cell cycle and division (Kyriakis & Avruch 2001). In agreement with this, its over-expression activated a number of central cell division genes such as cyclins and kinesins. Third, as a convergence point of signal transduction, p38 MAPK affects the levels of expression of a number of other signal transduction molecules. It is thus plausible that the collective significance of these findings can be extended beyond the cardiovascular system. As the pattern of p38 MAPK-dependent genes was a conserved rather than a cardiac-restricted one, it is likely that these results can be considered when studying the role of p38 MAPK and its inhibition in inflammatory diseases, cancer cells and other disease processes.
The microarray analysis of hearts over-expressing p38 MAPK revealed a large number of genes of unknown function and expressed sequence tags. When the microarray analysis was extended to include genes that were up-regulated 1.5-2.0–fold by p38 MAPK, the majority of the additional genes belonged to these groups. This is of particular interest with respect to future studies, because it suggests indirectly that p38 MAPK may have many cellular functions which are currently unknown.

94
6.5 The dual role of p38 MAPK in normal and infarcted hearts
Among the key findings presented here is the unique functional role of p38 MAPK in the adult myocardium. p38 MAPK is revealed as a context-dependent, dualistic regulator of myocardial remodelling (Fig. 17) that is able to affect nearly all the pathophysiological processes that are significant in this remodelling: apoptosis, angiogenesis, fibrosis, inflammation and cell proliferation.
The functional role of p38 MAPK was determined in the normal heart in the work described in Paper III, where the levels of p38 MAPK were found to be increased by the adenovirus-mediated gene transfer of MKK3bE and WT p38α and the pathophysiological effects were assessed by echocardiography and histological analysis. The latter yielded three major findings: a massive infiltration of inflammatory cells, fibrosis and a significant increase in Ki-67-positive cells undergoing proliferation.
In view of the findings regarding p38 MAPK-induced gene expression, it is likely that the inflammatory response is a direct consequence of the increased expression of pro-inflammatory molecules, which attract the inflammatory cells to invade the affected myocardium. Furthermore, the increased cellular proliferation may be related to the inflammatory response, since the majority of the Ki-67 positive cells appeared to belong to inflammatory cell types. Even though it has been suggested that p38 MAPK may be involved in cardiomyocyte proliferation (Engel et al. 2005), a loss of cardiomyocytes rather than a proliferation was observed in the hearts over-expressing p38 MAPK. Nevertheless, the histological sections showed a notable thickening of the anterior wall due to increased myocardial fibrosis. Whether the fibrosis is also related to the inflammatory response remains to be elucidated, but it should be noted that the DNA microarray showed an up-regulation of many fibrosis-associated genes, suggesting that p38 MAPK directly affects fibrosis. This is also supported by observations in transgenic gain-of-function studies pointing to increased fibrosis in response to MKK3 (Liao et al. 2001). The present results are also quite consistent with transgenic animal studies with respect to inflammation, since MKK6bE transgenic animals showed increased plasma levels of TNF-α and IL-6 (Li et al. 2005).
p38 MAPK has also been linked to the regulation of cardiac contractility, as it has been thought to confer a negative inotropic effect on cultured cardiomyocytes (Liao et al. 2002, Chen et al. 2003). Interestingly, despite the massive inflammation and fibrosis, the hearts over-expressing p38 MAPK did not show impaired function as assessed by echocardiography. This finding does not support the hypothesis that p38 MAPK may be a mediator of a negative inotropic effect; on the contrary, it suggests that p38 MAPK has no significant role in vivo as a direct regulator of cardiac contractility.
The role of p38 MAPK in post-infarction remodelling was established in Paper IV, where western blot analysis revealed that, unlike reversible ischaemia, post-infarction remodelling was characterised by a sustained down-regulation of p38 MAPK activity. This down-regulation was unique in nature with respect to other MAPKs, since ERK and JNK showed activation rather than inactivation, but it is consistent with those heart failure studies that report decreased p38 MAPK activity (Lemke et al. 2001, Communal et al. 2002, Takeishi et al. 2002). In the light of the results of Paper IV, it appears that decreased p38 predisposes the subject to adverse post-infarction remodelling and thus

95
represents a causative factor in the pathogenesis of heart failure. When p38 MAPK levels were restored by means of adenoviral gene transfer, both the morphological and the functional features of post-infarction heart failure were attenuated. At the functional level, the infarcted hearts with normalised p38 MAPK activity showed significant improvements in ejection fraction and fractional shortening and less left ventricular dilatation, while histological analysis showed the thinning of the anterior wall, hypertrophy of the posterior wall and infarct size to have significantly decreased. Collectively, these findings indicate that normalised p38 activity after myocardial infarction protects the heart from adverse remodelling and the development of heart failure.
The mechanistic studies of infarcted hearts treated with p38 MAPK over-expression revealed two potential mechanisms whereby p38 MAPK may confer protection from adverse remodelling. At an early time point post infarction, the hearts over-expressing p38 MAPK showed significantly less apoptosis than those treated with the Lac Z control virus. This suggests that p38 MAPK protects the myocytes from programmed cell death after infarction and is thereby able to reduce the infarct size. Although the first in vitro studies favoured a pro-apoptotic effect of p38 MAPK (Wang et al. 1998), later in vivo studies have indicated that p38 MAPK may be anti-apoptotic in the heart (Martindale et al. 2005), a view with which the present findings are in agreement. Angiogenesis, another integral mechanism of post-infarction remodelling, may also explain the p38 MAPK-mediated cardioprotection, as the p38 MAPK-treated hearts exhibited increased capillary density and microvessel enlargement relative to the Lac Z -treated hearts. Although no definitive previous evidence exists for a role for p38 MAPK in angiogenesis, this may be mainly a direct angiogenic effect of p38 MAPK. Previous work has shown that VEGF and angiopoietin exert their angiogenic functions partially via p38 MAPK, and p38 MAPK inhibition has been shown to be anti-angiogenic under certain experimental conditions (Rousseau et al. 1997, Jackson et al. 1998, Harfouche et al. 2003). More importantly, p38 MAPK activated angiogenic growth factor production and a tendency for increased capillary density was found in the normal heart. In contrast to angiogenesis, the attenuation of fibrosis and improved cardiac function are likely to be secondary consequences of the decrease in infarct size, considering the pro-fibrotic effect of p38 MAPK in the normal heart and the lack of effect on baseline cardiac contractility.
The above results raise the question of the molecular mechanism behind the somewhat discrepant findings in normal and infarcted hearts. The controversial results reported in prior studies should first be noted in this context. Protection from ischaemia-reperfusion injury has been observed in MKK6 over-expressing and in dominant-negative p38α and MKK6 transgenic mice (Kaiser et al. 2004, Martindale et al. 2005). Over-expression of constitutively active MKK3 or MKK6 leads to increased interstitial fibrosis in transgenic animals, but increased fibrosis is also observed in cardiac-specific dominant-negative p38α, MKK3 and MKK6 transgenic mice in response to hypertrophic stimulation (Liao et al. 2001, Braz et al. 2003, Nishida et al. 2004). Inhibition of p38 MAPK activity during ischaemia-reperfusion in vitro enhances post-ischaemic recovery of cardiac function (Ma et al. 1999, Barancik et al. 2000, Schneider et al. 2001), but conversely, p38 MAPK appears to mediate ischaemic preconditioning (Ravingerova et al. 2003). Taken these observations together with the present results, p38 MAPK can be considered a highly context-dependent kinase: it can be beneficial or detrimental, anti-apoptotic or pro-

96
apoptotic, and either promote or attenuate fibrosis depending on the pathophysiological conditions (Fig. 17). Theoretically, this is supported by the conserved nature of p38 MAPK, as a high degree of context-dependent versatility is required to be able to regulate central cellular processes in response to diverse stimuli in virtually all eukaryotes from yeasts to mammalian cardiomyocytes. Furthermore, the conditions at both the physiological and molecular level differ fundamentally between the infarcted myocardium and the normal heart, as massive cell death leads to alterations in loading conditions, changes in the extracellular matrix and an altered balance of paracrine and hormonal factors, all of which may direct the kinase activity to different cellular functions. Second, the nuclear effectors of p38 MAPK appeared to be partly different between the normal and infarcted heart, since GATA-4 was p38 MAPK-independent in the infarcted myocardium. Third, myocardial infarction is known to alter the activities of multiple signal transduction pathways, and as a convergence point of signalling, p38 MAPK activation may affect many other signalling pathways. It is therefore possible that p38 MAPK over-expression may alter the overall balance of kinase activity in different ways in the normal and infarcted myocardium, leading to different responses at the physiological level. Fourth, the effects of p38 MAPK over-expression in the normal heart cannot simply be labelled as harmful: in view of prior data concerning cardiac inflammation and cellular proliferation, the release of cytokines and cell cycle promoting factors can be beneficial under certain conditions (Nian et al. 2004). Finally, one more aspect should be noted: p38 MAPK activity is reduced in the infarcted heart and gene transfer returns it to the normal level, whereas in the normal heart p38 MAPK activity is increased above the baseline levels. In view of the central and conserved position of p38 MAPK, it is possible that the maintenance of normal p38 activity is critical, while an alteration in the balance in either direction causes detrimental effects. This point of view is also supported by the controversial results obtained with transgenic over-expression and dominant-negative models.
Current heart failure drug therapies are mainly targeted against receptors, and it is likely that they affect the systemic responses to the disease process rather than the cellular pathophysiological mechanisms involved. The normalisation of p38 MAPK activity would represent a potential cardiac gene therapy approach targeted against a conserved intracellular signalling pathway, and a novel therapeutic approach targeted at the intracellular mechanism of the disease process. As such, it would also affect the fundamental cellular processes that cause the transition from myocardial infarction to a failing heart: cell death, lack of vascularisation and fibrosis. Although a therapeutic potential with respect to remodelling has also been attributed to small molecule inhibitors of p38 MAPK in other studies (See et al. 2004, Liu et al. 2005), the present results may still not be at variance with these observations, for while myocardial p38 is down-regulated in the failing heart, vascular p38 MAP kinase is known to be activated, and the beneficial effects of the inhibitors may therefore be related to the systemic responses (Widder et al. 2004). The timing of p38 inhibitor administration in the previous studies was also different from that employed here, and the present results do not exclude the potential benefits of late p38 MAPK inhibition (See et al. 2004, Liu et al. 2005). This would be comparable to ACE inhibitor treatment, which is beneficial only beyond the acute phase (Swedberg et al. 1992). Taken together, the present results indicate that p38 MAPK is a central regulator of myocardial remodelling and a potential novel target for

97
therapeutic approaches. The context-dependence of p38 MAPK function should nevertheless be considered when interpreting these results in terms of therapeutic potential.
Fig. 17. Summary of the dual role of p38 MAPK in the normal and infarcted heart.

7 Summary and conclusions
The aim of this work was to determine the activities, role and interaction of MAPKs and their nuclear downstream effector GATA-4 during increased wall stress and post-infarction remodelling, representing two central stimuli of heart failure.
1. To study the transcription factor activities in response to increased workload, isolated perfused rat hearts were subjected to an acute increase in active left ventricular wall stress. The DNA binding activities of GATA-4 and AP-1 transcription factors were rapidly activated. Pharmacological inhibition of both ETA/B and AT1 receptors abolished the activation of GATA-4 binding, indicating that the action of both ET-1 and angiotensin II is required to induce the transcriptional response to increased wall stress.
2. The model of increased wall stress in isolated hearts was chosen to determine the role of MAPKs in stretch-induced GATA-4 binding. Increased wall stress rapidly activated all MAPKs, i.e. p38 MAPK, ERK and JNK. Inhibition of p38 MAPK by the selective small molecule inhibitor SB239063 and inhibition of the ERK cascade by the MEK 1/2 inhibitor U0126 abrogated the stress-induced GATA-4 activation, while inhibition of JNK had no effect. These results indicate that both ERK and p38 MAPK are involved in the regulation of wall stress-induced GATA-4 binding.
3. To gain further insights into the role of p38 MAPK as a regulator of cardiac transcription and gene expression, a gene transfer protocol of increased p38 MAPK activity was established. Adenovirus-mediated gene transfer of the constitutively active upstream kinase MKK3bE and WT p38α selectively and efficiently increased p38 MAPK activity in the left ventricle, followed by activation of multiple cardiac transcription factors, including GATA-4, and by up-regulation of cardiac gene expression. To identify the p38 MAPK-dependent cardiac genes, the gene expression profiles of p38 MAPK-treated and Lac Z-treated hearts were compared in a DNA microarray analysis. The microarray identified 264 genes that were up-regulated more than 2.0-fold by p38 MAPK, most of them belonging functionally to the genes controlling cellular proliferation, inflammation and signal transduction. Consistent with the gene expression profile, p38 MAPK over-expression caused myocardial inflammation, fibrosis and cellular proliferation.

99
4. To assess the role of MAPKs in post-infarction remodelling, rats were subjected to experimental myocardial infarction by ligating the LAD. Myocardial infarction caused a sustained down-regulation of p38 MAPK activity, which was reversed using adenovirus-mediated gene transfer of MKK3bE and WT p38α. The normalisation of p38 MAPK activity attenuated post-infarction remodelling by reducing the infarct size and improving cardiac function, as assessed by histological analysis and echocardiography. The main mechanisms underlying this p38 MAPK-mediated cardioprotection may involve cardiomyocyte apoptosis and increased coronary angiogenesis. These findings indicate collectively that reduced p38 MAPK activity predisposes a subject to adverse post-infarction remodelling, and that restoration of p38 MAPK may represent a potential novel therapeutic approach to the treatment of heart failure.
5. To study the activities and regulation of cardiac transcription factors during post-infarction remodelling, rats were subjected to experimental myocardial infarction. These experiments revealed that GATA-4 is differentially regulated in the normal and the infarcted heart. It was rapidly inactivated after myocardial infarction, but was activated in the later phases of remodelling. In contrast, AP-1 and NF-κB were consistently activated in the infarcted heart. In contrast to the situation in the normal heart, GATA-4 was not controlled by p38 MAPK in the infarcted heart.

References
Abbate A, Bussani R, Biondi-Zoccai GG, Rossiello R, Silvestri F, Baldi F, Biasucci LM & Baldi A (2002) Persistent infarct-related artery occlusion is associated with an increased myocardial apoptosis at postmortem examination in humans late after an acute myocardial infarction. Circulation 106: 1051-1054.
Abdellatif M, Packer SE, Michael LH, Zhang D, Charng MJ & Schneider MD (1998) A Ras-dependent pathway regulates RNA polymerase II phosphorylation in cardiac myocytes: implications for cardiac hypertrophy. Mol Cell Biol 18: 6729-6736.
Abe K, Shimokawa H, Morikawa K, Uwatoku T, Oi K, Matsumoto Y, Hattori T, Nakashima Y, Kaibuchi K, Sueishi K & Takeshit A (2004) Long-term treatment with a Rho-kinase inhibitor improves monocrotaline-induced fatal pulmonary hypertension in rats. Circ Res 94: 385-393.
Aikawa R, Nagai T, Kudoh S, Zou Y, Tanaka M, Tamura M, Akazawa H, Takano H, Nagai R & Komuro I (2002) Integrins play a critical role in mechanical stress-induced p38 MAPK activation. Hypertension 39: 233-238.
Akazawa H & Komuro I (2003) Roles of cardiac transcription factors in cardiac hypertrophy. Circ Res 92: 1079-1088.
Akhter SA, Luttrell LM, Rockman HA, Iaccarino G, Lefkowitz RJ & Koch WJ (1998) Targeting the receptor-Gq interface to inhibit in vivo pressure overload myocardial hypertrophy. Science 280: 574-577.
Angel P & Karin M (1991) The role of Jun, Fos and the AP-1 complex in cell-proliferation and transformation. Biochim Biophys Acta 1072: 129-157.
Angoulvant D, Fazel S & Li RK (2004) Neovascularization derived from cell transplantation in ischemic myocardium. Mol Cell Biochem 264: 133-142.
Antos CL, McKinsey TA, Frey N, Kutschke W, McAnally J, Shelton JM, Richardson JA, Hill JA & Olson EN (2002) Activated glycogen synthase-3 beta suppresses cardiac hypertrophy in vivo. Proc Natl Acad Sci U S A 99: 907-912.
Arai H, Hori S, Aramori I, Ohkubo H & Nakanishi S (1990) Cloning and expression of a cDNA encoding an endothelin receptor. Nature 348: 730-732.
Arceci RJ, King AA, Simon MC, Orkin SH & Wilson DB (1993) Mouse GATA-4: a retinoic acid-inducible GATA-binding transcription factor expressed in endodermally derived tissues and heart. Mol Cell Biol 13: 2235-2246.
Aries A, Paradis P, Lefebvre C, Schwartz RJ & Nemer M (2004) Essential role of GATA-4 in cell survival and drug-induced cardiotoxicity. Proc Natl Acad Sci U S A 101: 6975-6980.
Arsenian S, Weinhold B, Oelgeschlager M, Ruther U & Nordheim A (1998) Serum response factor is essential for mesoderm formation during mouse embryogenesis. EMBO J 17: 6289-6299.

101
Atlas SA, Kleinert HD, Camargo MJ, Januszewicz A, Sealey JE, Laragh JH, Schilling JW, Lewicki JA, Johnson LK & Maack T (1984) Purification, sequencing and synthesis of natriuretic and vasoactive rat atrial peptide. Nature 309: 717-719.
Babbitt CJ, Shai SY, Harpf AE, Pham CG & Ross RS (2002) Modulation of integrins and integrin signaling molecules in the pressure-loaded murine ventricle. Histochem Cell Biol 118: 431-439.
Bader M, Peters J, Baltatu O, Muller DN, Luft FC & Ganten D (2001) Tissue renin-angiotensin systems: new insights from experimental animal models in hypertension research. J Mol Med 79: 76-102.
Baeuerle PA & Baltimore D (1996) NF-kappa B: ten years after. Cell 87: 13-20. Baines CP & Molkentin JD (2005) STRESS signaling pathways that modulate cardiac myocyte
apoptosis. J Mol Cell Cardiol 38: 47-62. Baldi A, Abbate A, Bussani R, Patti G, Melfi R, Angelini A, Dobrina A, Rossiello R, Silvestri F,
Baldi F & Di Sciascio G (2002) Apoptosis and post-infarction left ventricular remodeling. J Mol Cell Cardiol 34: 165-174.
Banai S, Jaklitsch MT, Shou M, Lazarous DF, Scheinowitz M, Biro S, Epstein SE & Unger EF (1994) Angiogenic-induced enhancement of collateral blood flow to ischemic myocardium by vascular endothelial growth factor in dogs. Circulation 89: 2183-2189.
Barancik M, Htun P, Strohm C, Kilian S & Schaper W (2000) Inhibition of the cardiac p38-MAPK pathway by SB203580 delays ischemic cell death. J Cardiovasc Pharmacol 35: 474-483.
Bayer AL, Heidkamp MC, Patel N, Porter M, Engman S & Samarel AM (2003) Alterations in protein kinase C isoenzyme expression and autophosphorylation during the progression of pressure overload-induced left ventricular hypertrophy. Mol Cell Biochem 242: 145-152.
Behr TM, Nerurkar SS, Nelson AH, Coatney RW, Woods TN, Sulpizio A, Chandra S, Brooks DP, Kumar S, Lee JC, Ohlstein EH, Angermann CE, Adams JL, Sisko J, Sackner-Bernstein JD & Willette RN (2001) Hypertensive end-organ damage and premature mortality are p38 mitogen-activated protein kinase-dependent in a rat model of cardiac hypertrophy and dysfunction. Circulation 104: 1292-1298.
Belaguli NS, Sepulveda JL, Nigam V, Charron F, Nemer M & Schwartz RJ (2000) Cardiac tissue enriched factors serum response factor and GATA-4 are mutual coregulators. Mol Cell Biol 20: 7550-7558.
Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K, Leri A, Kajstura J, Nadal-Ginard B & Anversa P (2003) Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell 114: 763-776.
Bhalla SS, Robitaille L & Nemer M (2001) Cooperative activation by GATA-4 and YY1 of the cardiac B-type natriuretic peptide promoter. J Biol Chem 276: 11439-11445.
Bing OH (1994) Hypothesis: apoptosis may be a mechanism for the transition to heart failure with chronic pressure overload. J Mol Cell Cardiol 26: 943-948.
Bishopric NH, Jayasena V & Webster KA (1992) Positive regulation of the skeletal alpha-actin gene by Fos and Jun in cardiac myocytes. J Biol Chem 267: 25535-25540.
Bogoyevitch MA, Gillespie-Brown J, Ketterman AJ, Fuller SJ, Ben-Levy R, Ashworth A, Marshall CJ & Sugden PH (1996) Stimulation of the stress-activated mitogen-activated protein kinase subfamilies in perfused heart. p38/RK mitogen-activated protein kinases and c-Jun N-terminal kinases are activated by ischemia/reperfusion. Circ Res 79: 162-173.
Bogoyevitch MA, Ketterman AJ & Sugden PH (1995) Cellular stresses differentially activate c-Jun N-terminal protein kinases and extracellular signal-regulated protein kinases in cultured ventricular myocytes. J Biol Chem 270: 29710-29717.
Bohm M, Gierschik P, Knorr A, Larisch K, Weismann K & Erdmann E (1992) Desensitization of adenylate cyclase and increase of Gi alpha in cardiac hypertrophy due to acquired hypertension. Hypertension 20: 103-112.

102
Boknik P, Heinroth-Hoffmann I, Kirchhefer U, Knapp J, Linck B, Luss H, Muller T, Schmitz W, Brodde O & Neumann J (2001) Enhanced protein phosphorylation in hypertensive hypertrophy. Cardiovasc Res 51: 717-728.
Boulton TG, Nye SH, Robbins DJ, Ip NY, Radziejewska E, Morgenbesser SD, DePinho RA, Panayotatos N, Cobb MH & Yancopoulos GD (1991) ERKs: a family of protein-serine/threonine kinases that are activated and tyrosine phosphorylated in response to insulin and NGF. Cell 65: 663-675.
Bourassa MG, Gurne O, Bangdiwala SI, Ghali JK, Young JB, Rousseau M, Johnstone DE & Yusuf S (1993) Natural history and patterns of current practice in heart failure. The Studies of Left Ventricular Dysfunction (SOLVD) Investigators. J Am Coll Card 22 14A-19A.
Bowman JC, Steinberg SF, Jiang T, Geenen DL, Fishman GI & Buttrick PM (1997) Expression of protein kinase C beta in the heart causes hypertrophy in adult mice and sudden death in neonates. J Clin Invest 100: 2189-2195.
Boxer LM, Prywes R, Roeder RG & Kedes L (1989) The sarcomeric actin CArG-binding factor is indistinguishable from the c-fos serum response factor. Mol Cell Biol 9: 515-522.
Braz JC, Bueno OF, De Windt LJ & Molkentin JD (2002) PKC alpha regulates the hypertrophic growth of cardiomyocytes through extracellular signal-regulated kinase1/2 (ERK1/2). Journal Cell Biol 156: 905-919.
Braz JC, Bueno OF, Liang Q, Wilkins BJ, Dai YS, Parsons S, Braunwart J, Glascock BJ, Klevitsky R, Kimball TF, Hewett TE & Molkentin JD (2003) Targeted inhibition of p38 MAPK promotes hypertrophic cardiomyopathy through upregulation of calcineurin-NFAT signaling. J Clin Invest 111: 1475-1486.
Braz JC, Gregory K, Pathak A, Zhao W, Sahin B, Klevitsky R, Kimball TF, Lorenz JN, Nairn AC, Liggett SB, Bodi I, Wang S, Schwartz A, Lakatta EG, DePaoli-Roach AA, Robbins J, Hewett TE, Bibb JA, Westfall MV, Kranias EG & Molkentin JD (2004) PKC-alpha regulates cardiac contractility and propensity toward heart failure. Nat Med 10: 248-254.
Brilla CG, Pick R, Tan LB, Janicki JS & Weber KT (1990) Remodeling of the rat right and left ventricles in experimental hypertension. Circ Res 67: 1355-1364.
Brilla CG, Zhou G, Matsubara L & Weber KT (1994) Collagen metabolism in cultured adult rat cardiac fibroblasts: response to angiotensin II and aldosterone. J Mol Cell Cardiol 26: 809-820.
Brown RD, Ambler SK, Mitchell MD & Long CS (2005) The cardiac fibroblast: therapeutic target in myocardial remodeling and failure. Annu Rev Pharmacol Toxicol 45: 657-687.
Bueno OF, De Windt LJ, Lim HW, Tymitz KM, Witt SA, Kimball TR & Molkentin JD (2001) The dual-specificity phosphatase MKP-1 limits the cardiac hypertrophic response in vitro and in vivo. Circ Res 88: 88-96.
Bueno OF, De Windt LJ, Tymitz KM, Witt SA, Kimball TR, Klevitsky R, Hewett TE, Jones SP, Lefer DJ, Peng CF, Kitsis RN & Molkentin JD (2000) The MEK1-ERK1/2 signaling pathway promotes compensated cardiac hypertrophy in transgenic mice. EMBO J 19: 6341-6350.
Bueno OF & Molkentin JD (2002) Involvement of extracellular signal-regulated kinases 1/2 in cardiac hypertrophy and cell death. Circ Res 91: 776-781.
Bueno OF, van Rooij E, Molkentin JD, Doevendans PA & De Windt LJ (2002) Calcineurin and hypertrophic heart disease: novel insights and remaining questions. Cardiovasc Res 53: 806-821.
Calderone A, Thaik CM, Takahashi N, Chang DL & Colucci WS (1998) Nitric oxide, atrial natriuretic peptide, and cyclic GMP inhibit the growth-promoting effects of norepinephrine in cardiac myocytes and fibroblasts. J Clin Invest 101: 812-818.
Calderone A, Takahashi N, Izzo NJ, Thaik CM & Colucci WS (1995) Pressure- and volume-induced left ventricular hypertrophies are associated with distinct myocyte phenotypes and differential induction of peptide growth factor mRNAs. Circulation 92: 2385-2390.

103
Campbell SE, Korecky B & Rakusan K (1991) Remodeling of myocyte dimensions in hypertrophic and atrophic rat hearts. Circ Res 68: 984-996.
Campbell SE, Rakusan K & Gerdes AM (1989) Change in cardiac myocyte size distribution in aortic-constricted neonatal rats. Basic Res Cardiol 84: 247-258.
Charron F, Paradis P, Bronchain O, Nemer G & Nemer M (1999) Cooperative interaction between GATA-4 and GATA-6 regulates myocardial gene expression. Mol Cell Biol 19: 4355-4365.
Charron F, Tsimiklis G, Arcand M, Robitaille L, Liang Q, Molkentin JD, Meloche S & Nemer M (2001) Tissue-specific GATA factors are transcriptional effectors of the small GTPase RhoA. Genes Dev 15: 2702-2719.
Chatterjee S, Stewart AS, Bish LT, Jayasankar V, Kim EM, Pirolli T, Burdick J, Woo YJ, Gardner TJ & Sweeney HL (2002) Viral gene transfer of the antiapoptotic factor Bcl-2 protects against chronic postischemic heart failure. Circulation 106: I212-I217.
Chen F, Castranova V, Shi X & Demers LM (1999) New insights into the role of nuclear factor-kappaB, a ubiquitous transcription factor in the initiation of diseases. Clin Chem 45: 7-17.
Chen HH & Burnett JC (1998) C-type natriuretic peptide: the endothelial component of the natriuretic peptide system. J Cardiovasc Pharmacol 32: S22-S28.
Chen Y, Rajashree R, Liu Q & Hofmann P (2003) Acute p38 MAPK activation decreases force development in ventricular myocytes. Am J Physiol Heart Circ Physiol 285(6): H2578-H2586.
Cheng G, Hagen TP, Dawson ML, Barnes KV & Menick DR (1999) The role of GATA, CArG, E-box, and a novel element in the regulation of cardiac expression of the Na+-Ca2+ exchanger gene. J Biol Chem 274: 12819-12826.
Chiloeches A, Paterson HF, Marais R, Clerk A, Marshall CJ & Sugden PH (1999) Regulation of Ras.GTP loading and Ras-Raf association in neonatal rat ventricular myocytes by G protein-coupled receptor agonists and phorbol ester. Activation of the extracellular signal-regulated kinase cascade by phorbol ester is mediated by Ras. J Biol Chem 274: 19762-19770.
Chirgwin JM, Przybyla AE, MacDonald RJ & Rutter WJ (1979) Isolation of biologically active ribonucleic acid from sources enriched in ribonuclease. Biochemistry 18: 5294-5299.
Choukroun G, Hajjar R, Fry S, del Monte F, Haq S, Guerrero JL, Picard M, Rosenzweig A & Force T (1999) Regulation of cardiac hypertrophy in vivo by the stress-activated protein kinases/c-Jun NH(2)-terminal kinases. J Clin Invest 104: 391-398.
Chusho H, Tamura N, Ogawa Y, Yasoda A, Suda M, Miyazawa T, Nakamura K, Nakao K, Kurihara T, Komatsu Y, Itoh H, Tanaka K, Saito Y, Katsuki M & Nakao K (2001) Dwarfism and early death in mice lacking C-type natriuretic peptide. Proc Natl Acad Sci U S A 98: 4016-4021.
Clerk A & Sugden PH (2000) Small guanine nucleotide-binding proteins and myocardial hypertrophy. Circ Res 86: 1019-1023.
Clerk A, Pham FH, Fuller SJ, Sahai E, Aktories K, Marais R, Marshall C & Sugden PH (2001) Regulation of mitogen-activated protein kinases in cardiac myocytes through the small G protein Rac1. Mol Cell Biol 21: 1173-1184.
Clerk A, Michael A & Sugden PH (1998) Stimulation of the p38 mitogen-activated protein kinase pathway in neonatal rat ventricular myocytes by the G protein-coupled receptor agonists, endothelin-1 and phenylephrine: a role in cardiac myocyte hypertrophy? J Cell Biol 142: 523-535.
Cleutjens JP, Kandala JC, Guarda E, Guntaka RV & Weber KT (1995) Regulation of collagen degradation in the rat myocardium after infarction. J Mol Cell Cardiol 27: 1281-1292.
Clipstone NA & Crabtree GR (1992) Identification of calcineurin as a key signalling enzyme in T-lymphocyte activation. Nature 357: 695-697.
Colomer JM, Mao L, Rockman HA & Means AR (2003) Pressure overload selectively up-regulates Ca2+/calmodulin-dependent protein kinase II in vivo. Mol Endocrinol 17: 183-192.

104
Communal C, Colucci WS, Remondino A, Sawyer DB, Port JD, Wichman SE, Bristow MR & Singh K (2002) Reciprocal modulation of mitogen-activated protein kinases and mitogen-activated protein kinase phosphatase 1 and 2 in failing human myocardium. J Card Fail 8: 86-92.
Condorelli G, Morisco C, Stassi G, Notte A, Farina F, Sgaramella G, de Rienzo A, Roncarati R, Trimarco B & Lembo G (1999) Increased cardiomyocyte apoptosis and changes in proapoptotic and antiapoptotic genes bax and bcl-2 during left ventricular adaptations to chronic pressure overload in the rat. Circulation 99: 3071-3078.
Condorelli G, Drusco A, Stassi G, Bellacosa A, Roncarati R, Iaccarino G, Russo MA, Gu Y, Dalton N, Chung C, Latronico MV, Napoli C, Sadoshima J, Croce CM & Ross J,Jr (2002) Akt induces enhanced myocardial contractility and cell size in vivo in transgenic mice. Proc Natl Acad Sci U S A 99: 12333-12338.
Cook SA, Novikov MS, Ahn Y, Matsui T & Rosenzweig A (2003) A20 is dynamically regulated in the heart and inhibits the hypertrophic response. Circulation 108: 664-667.
Cook SA, Sugden PH & Clerk A (1999) Activation of c-Jun N-terminal kinases and p38-mitogen-activated protein kinases in human heart failure secondary to ischaemic heart disease. J Mol Cell Cardiol 31: 1429-1434.
Cooper JA, Bowen-Pope DF, Raines E, Ross R & Hunter T (1982) Similar effects of platelet-derived growth factor and epidermal growth factor on the phosphorylation of tyrosine in cellular proteins. Cell 31: 263-273.
Cornelius T, Holmer SR, Muller FU, Riegger GA & Schunkert H (1997) Regulation of the rat atrial natriuretic peptide gene after acute imposition of left ventricular pressure overload. Hypertension 30: 1348-1355.
Crispino JD, Lodish MB, Thurberg BL, Litovsky SH, Collins T, Molkentin JD & Orkin SH (2001) Proper coronary vascular development and heart morphogenesis depend on interaction of GATA-4 with FOG cofactors. Genes Dev 15: 839-844.
Dagnino L, Lavigne JP & Nemer M (1992) Increased transcripts for B-type natriuretic peptide in spontaneously hypertensive rats. Quantitative polymerase chain reaction for atrial and brain natriuretic peptide transcripts. Hypertension 20: 690-700.
Dai YS, Cserjesi P, Markham BE & Molkentin JD (2002) The transcription factors GATA4 and dHAND physically interact to synergistically activate cardiac gene expression through a p300-dependent mechanism. J Biol Chem 277: 24390-24398.
Dai YS & Markham BE (2001) p300 Functions as a coactivator of transcription factor GATA-4. J Biol Chem 276: 37178-37185.
D'Angelo DD, Sakata Y, Lorenz JN, Boivin GP, Walsh RA, Liggett SB & Dorn GW,2nd (1997) Transgenic Galphaq overexpression induces cardiac contractile failure in mice. Proc Natl Acad Sci U S A 94: 8121-8126.
de Bold AJ, Borenstein HB, Veress AT & Sonnenberg H (1981) A rapid and potent natriuretic response to intravenous injection of atrial myocardial extract in rats. Life Sci 28: 89-94.
de Bold AJ, Bruneau BG & Kuroski de Bold ML (1996) Mechanical and neuroendocrine regulation of the endocrine heart. Cardiovasc Res 31: 7-18.
Degousee N, Martindale J, Stefanski E, Cieslak M, Lindsay TF, Fish JE, Marsden PA, Thuerauf DJ, Glembotski CC & Rubin BB (2003) MAP kinase kinase 6-p38 MAP kinase signaling cascade regulates cyclooxygenase-2 expression in cardiac myocytes in vitro and in vivo. Circ Res 92: 757-764.
Deryckere F & Gannon F (1994) A one-hour minipreparation technique for extraction of DNA-binding proteins from animal tissues. BioTechniques 16: 405.
Deten A, Volz HC, Briest W & Zimmer HG (2002) Cardiac cytokine expression is upregulated in the acute phase after myocardial infarction. Experimental studies in rats. Cardiovasc Res 55: 329-340.

105
Diedrichs H, Mei C, Frank KF, Boelck B & Schwinger RH (2004) Calcineurin independent development of myocardial hypertrophy in transgenic rats overexpressing the mouse renin gene, TGR(mREN2)27. J Mol Med 82: 688-695.
Dimmeler S, Zeiher AM & Schneider MD (2005) Unchain my heart: the scientific foundations of cardiac repair. J Clin Invest 115: 572-583.
Disatnik MH, Buraggi G & Mochly-Rosen D (1994) Localization of protein kinase C isozymes in cardiac myocytes. Exp Cell Res 210: 287-297.
Domingos PP, Fonseca PM, Nadruz W,Jr & Franchini KG (2002) Load-induced focal adhesion kinase activation in the myocardium: role of stretch and contractile activity. Am J Physiol Heart Circ Physiol 282: H556-H564.
Dorn GW,2nd & Force T (2005) Protein kinase cascades in the regulation of cardiac hypertrophy. J Clin Invest 115: 527-537.
Dorn GW,2nd, Robbins J & Sugden PH (2003) Phenotyping hypertrophy: eschew obfuscation. Circ Res 92: 1171-1175.
Durocher D, Charron F, Warren R, Schwartz RJ & Nemer M (1997) The cardiac transcription factors Nkx2-5 and GATA-4 are mutual cofactors. EMBO J 16: 5687-5696.
Eldar-Finkelman H, Seger R, Vandenheede JR & Krebs EG (1995) Inactivation of glycogen synthase kinase-3 by epidermal growth factor is mediated by mitogen-activated protein kinase/p90 ribosomal protein S6 kinase signaling pathway in NIH/3T3 cells. J Biol Chem 270: 987-990.
Engel D, Peshock R, Armstong RC, Sivasubramanian N & Mann DL (2004) Cardiac myocyte apoptosis provokes adverse cardiac remodeling in transgenic mice with targeted TNF overexpression. Am J Physiol Heart Circ Physiol 287: H1303-H1311.
Engel FB, Schebesta M, Duong MT, Lu G, Ren S, Madwed JB, Jiang H, Wang Y & Keating MT (2005) p38 MAP kinase inhibition enables proliferation of adult mammalian cardiomyocytes. Genes Dev 19: 1175-1187.
Esposito G, Prasad SV, Rapacciuolo A, Mao L, Koch WJ & Rockman HA (2001) Cardiac overexpression of a G(q) inhibitor blocks induction of extracellular signal-regulated kinase and c-Jun NH(2)-terminal kinase activity in in vivo pressure overload. Circulation 103: 1453-1458.
Fiebeler A, Schmidt F, Muller DN, Park JK, Dechend R, Bieringer M, Shagdarsuren E, Breu V, Haller H & Luft FC (2001) Mineralocorticoid receptor affects AP-1 and nuclear factor-kappab activation in angiotensin II-induced cardiac injury. Hypertension 37: 787-793.
Fischer TA, Ludwig S, Flory E, Gambaryan S, Singh K, Finn P, Pfeffer MA, Kelly RA & Pfeffer JM (2001) Activation of cardiac c-Jun NH(2)-terminal kinases and p38-mitogen-activated protein kinases with abrupt changes in hemodynamic load. Hypertension 37: 1222-1228.
Flanagan MF, Fujii AM, Colan SD, Flanagan RG & Lock JE (1991) Myocardial angiogenesis and coronary perfusion in left ventricular pressure-overload hypertrophy in the young lamb. Evidence for inhibition with chronic protamine administration. Circ Res 68: 1458-1470.
Flesch M, Margulies KB, Mochmann HC, Engel D, Sivasubramanian N & Mann DL (2001) Differential regulation of mitogen-activated protein kinases in the failing human heart in response to mechanical unloading. Circulation 104: 2273-2276.
Fliss H & Gattinger D (1996) Apoptosis in ischemic and reperfused rat myocardium. Circ Res 79: 949-956.
Force T, Michael A, Kilter H & Haq S (2002) Stretch-activated pathways and left ventricular remodeling. J Card Fail 8: S351-S358.
Fortuno MA, Ravassa S, Fortuno A, Zalba G & Diez J (2001) Cardiomyocyte apoptotic cell death in arterial hypertension: mechanisms and potential management. Hypertension 38: 1406-1412.
Francis GS (2001) Pathophysiology of chronic heart failure. Am J Med 110: 37S-46S. Frey N, McKinsey TA & Olson EN (2000) Decoding calcium signals involved in cardiac growth
and function. Nat Med 6: 1221-1227.

106
Frödin M & Gammeltoft S (1999) Role and regulation of 90 kDa ribosomal S6 kinase (RSK) in signal transduction. Mol Cell Endocrinol 151: 65-77.
Fuchs S, Baffour R, Zhou YF, Shou M, Pierre A, Tio FO, Weissman NJ, Leon MB, Epstein SE & Kornowski R (2001) Transendocardial delivery of autologous bone marrow enhances collateral perfusion and regional function in pigs with chronic experimental myocardial ischemia. J Am Coll Cardiol 37: 1726-1732.
Fukuda S, Yoshii S, Kaga S, Matsumoto M, Kugiyama K & Maulik N (2004) Angiogenic strategy for human ischemic heart disease: brief overview. Mol Cell Biochem 264: 143-149.
Fuller SJ, Davies EL, Gillespie-Brown J, Sun H & Tonks NK (1997) Mitogen-activated protein kinase phosphatase 1 inhibits the stimulation of gene expression by hypertrophic agonists in cardiac myocytes. Biochem J 323: 313-319.
Fuller SJ, Gillespie-Brown J & Sugden PH (1998) Oncogenic src, raf, and ras stimulate a hypertrophic pattern of gene expression and increase cell size in neonatal rat ventricular myocytes. J Biol Chem 273: 18146-18152.
Galaria II, Fegley AJ, Nicholl SM, Roztocil E & Davies MG (2004) Differential regulation of ERK1/2 and p38(MAPK) by components of the Rho signaling pathway during sphingosine-1-phosphate-induced smooth muscle cell migration. J Surg Res 122: 173-179.
Gallo KA & Johnson GL (2002) Mixed-lineage kinase control of JNK and p38 MAPK pathways. Nat Rev Mol Cell Biol 3: 663-672.
Gardner DG (2003) Natriuretic peptides: markers or modulators of cardiac hypertrophy? Trends Endocrinol Metab 14: 411-416.
Gardner DG, Deschepper CF, Ganong WF, Hane S, Fiddes J, Baxter JD & Lewicki J (1986) Extra-atrial expression of the gene for atrial natriuretic factor. Proc Natl Acad Sci U S A 83: 6697-6701.
Garg V, Kathiriya IS, Barnes R, Schluterman MK, King IN, Butler CA, Rothrock CR, Eapen RS, Hirayama-Yamada K, Joo K, Matsuoka R, Cohen JC & Srivastava D (2003) GATA4 mutations cause human congenital heart defects and reveal an interaction with TBX5. Nature 424: 443-447.
Garrington TP & Johnson GL (1999) Organization and regulation of mitogen-activated protein kinase signaling pathways. Curr Opin Cell Biol 11: 211-218.
Gavin JB, Maxwell L & Edgar SG (1998) Microvascular involvement in cardiac pathology. J Mol Cell Cardiol 30: 2531-2540.
Geng YJ, Ishikawa Y, Vatner DE, Wagner TE, Bishop SP, Vatner SF & Homcy CJ (1999) Apoptosis of cardiac myocytes in Gsalpha transgenic mice. Circ Res 84: 34-42.
Gerdes AM, Campbell SE & Hilbelink DR (1988) Structural remodeling of cardiac myocytes in rats with arteriovenous fistulas. Lab Invest 59: 857-861.
Gillespie-Brown J, Fuller SJ, Bogoyevitch MA, Cowley S & Sugden PH (1995) The mitogen-activated protein kinase kinase MEK1 stimulates a pattern of gene expression typical of the hypertrophic phenotype in rat ventricular cardiomyocytes. J Biol Chem 270: 28092-28096.
Glennon PE, Kaddoura S, Sale EM, Sale GJ, Fuller SJ & Sugden PH (1996) Depletion of mitogen-activated protein kinase using an antisense oligodeoxynucleotide approach downregulates the phenylephrine-induced hypertrophic response in rat cardiac myocytes. Circ Res 78: 954-961.
Gove C, Walmsley M, Nijjar S, Bertwistle D, Guille M, Partington G, Bomford A & Patient R (1997) Over-expression of GATA-6 in Xenopus embryos blocks differentiation of heart precursors. EMBO J 16: 355-368.
Gottlieb RA, Burleson KO, Kloner RA, Babior BM & Engler RL (1994) Reperfusion injury induces apoptosis in rabbit cardiomyocytes. J Clin Invest 94: 1621-1628.
Grepin C, Dagnino L, Robitaille L, Haberstroh L, Antakly T & Nemer M (1994) A hormone-encoding gene identifies a pathway for cardiac but not skeletal muscle gene transcription. Mol Cell Biol 14: 3115-3129.

107
Grepin C, Robitaille L, Antakly T & Nemer M (1995) Inhibition of transcription factor GATA-4 expression blocks in vitro cardiac muscle differentiation. Mol Cell Biol 15: 4095-4102.
Grossman W, Jones D & McLaurin LP (1975) Wall stress and patterns of hypertrophy in the human left ventricle. J Clin Invest 56: 56-64.
Gruda MC, Kovary K, Metz R & Bravo R (1994) Regulation of Fra-1 and Fra-2 phosphorylation differs during the cell cycle of fibroblasts and phosphorylation in vitro by MAP kinase affects DNA binding activity. Oncogene 9: 2537-2547.
Gruver CL, DeMayo F, Goldstein MA & Means AR (1993) Targeted developmental overexpression of calmodulin induces proliferative and hypertrophic growth of cardiomyocytes in transgenic mice. Endocrinology 133: 376-388.
Guarda E, Katwa LC, Myers PR, Tyagi SC & Weber KT (1993) Effects of endothelins on collagen turnover in cardiac fibroblasts. Cardiovasc Res 27: 2130-2134.
Gudi SR, Lee AA, Clark CB & Frangos JA (1998) Equibiaxial strain and strain rate stimulate early activation of G proteins in cardiac fibroblasts. Am J Physiol 274: C1424-C1428.
Gunther S & Grossman W (1979) Determinants of ventricular function in pressure-overload hypertrophy in man. Circulation 59: 679-688.
Gupta S, Young D & Sen S (2005) Inhibition of NF-kappaB induces regression of cardiac hypertrophy, independent of blood pressure control, in spontaneously hypertensive rats. Am J Physiol Heart Circ Physiol 289: H20-H29.
Hagemann D, Bohlender J, Hoch B, Krause EG & Karczewski P (2001) Expression of Ca2+/calmodulin-dependent protein kinase II delta-subunit isoforms in rats with hypertensive cardiac hypertrophy. Mol Cell Biochem 220: 69-76.
Hai T & Curran T (1991) Cross-family dimerization of transcription factors Fos/Jun and ATF/CREB alters DNA binding specificity. Proc Natl Acad Sci U S A 88: 3720-3724.
Hamet P, Richard L, Dam TV, Teiger E, Orlov SN, Gaboury L, Gossard F & Tremblay J (1995) Apoptosis in target organs of hypertension. Hypertension 26: 642-648.
Han J, Lee JD, Bibbs L & Ulevitch RJ (1994) A MAP kinase targeted by endotoxin and hyperosmolarity in mammalian cells. Science 265: 808-811.
Han J & Molkentin JD (2000) Regulation of MEF2 by p38 MAPK and its implication in cardiomyocyte biology. Trends Cardiovasc Med 10: 19-22.
Haq S, Choukroun G, Kang ZB, Ranu H, Matsui T, Rosenzweig A, Molkentin JD, Alessandrini A, Woodgett J, Hajjar R, Michael A & Force T (2000) Glycogen synthase kinase-3beta is a negative regulator of cardiomyocyte hypertrophy. J Cell Biol 151: 117-130.
Haq S, Choukroun G, Lim H, Tymitz KM, del Monte F, Gwathmey J, Grazette L, Michael A, Hajjar R, Force T & Molkentin JD (2001) Differential activation of signal transduction pathways in human hearts with hypertrophy versus advanced heart failure. Circulation 103: 670-677.
Harada K, Komuro I, Shiojima I, Hayashi D, Kudoh S, Mizuno T, Kijima K, Matsubara H, Sugaya T, Murakami K & Yazaki Y (1998a) Pressure overload induces cardiac hypertrophy in angiotensin II type 1A receptor knockout mice. Circulation 97: 1952-1959.
Harada K, Komuro I, Zou Y, Kudoh S, Kijima K, Matsubara H, Sugaya T, Murakami K & Yazaki Y (1998b) Acute pressure overload could induce hypertrophic responses in the heart of angiotensin II type 1a knockout mice. Circ Res 82: 779-785.
Hardt SE & Sadoshima J (2002) Glycogen synthase kinase-3beta: a novel regulator of cardiac hypertrophy and development. Circ Res 90: 1055-1063.
Harfouche R, Gratton JP, Yancopoulos GD, Noseda M, Karsan A & Hussain SN (2003) Angiopoietin-1 activates both anti- and proapoptotic mitogen-activated protein kinases. FASEB J 17: 1523-1525.

108
Hariawala MD, Horowitz JR, Esakof D, Sheriff DD, Walter DH, Keyt B, Isner JM & Symes JF (1996) VEGF improves myocardial blood flow but produces EDRF-mediated hypotension in porcine hearts. J Surg Res 63: 77-82.
Hasegawa K, Lee SJ, Jobe SM, Markham BE & Kitsis RN (1997) cis-Acting sequences that mediate induction of beta-myosin heavy chain gene expression during left ventricular hypertrophy due to aortic constriction. Circulation 96: 3943-3953.
Hattori T, Shimokawa H, Higashi M, Hiroki J, Mukai Y, Tsutsui H, Kaibuchi K & Takeshita A (2004) Long-term inhibition of Rho-kinase suppresses left ventricular remodeling after myocardial infarction in mice. Circulation 109: 2234-2239.
Hautala N, Tokola H, Luodonpaa M, Puhakka J, Romppanen H, Vuolteenaho O & Ruskoaho H (2001) Pressure overload increases GATA4 binding activity via endothelin-1. Circulation 103: 730-735.
He H, Li HL, Lin A & Gottlieb RA (1999) Activation of the JNK pathway is important for cardiomyocyte death in response to simulated ischemia. Cell Death Differ 6: 987-991.
He Q, Mendez M & LaPointe MC (2002) Regulation of the human brain natriuretic peptide gene by GATA-4. Am J Physiol Endocrinol Metab 283: E50-E57.
Hedman M, Hartikainen J, Syvanne M, Stjernvall J, Hedman A, Kivela A, Vanninen E, Mussalo H, Kauppila E, Simula S, Narvanen O, Rantala A, Peuhkurinen K, Nieminen MS, Laakso M & Yla-Herttuala S (2003) Safety and feasibility of catheter-based local intracoronary vascular endothelial growth factor gene transfer in the prevention of postangioplasty and in-stent restenosis and in the treatment of chronic myocardial ischemia: phase II results of the Kuopio Angiogenesis Trial (KAT). Circulation 107: 2677-2683.
Heikinheimo M, Scandrett JM & Wilson DB (1994) Localization of transcription factor GATA-4 to regions of the mouse embryo involved in cardiac development. Dev Biol 164: 361-373.
Henry TD, Annex BH, McKendall GR, Azrin MA, Lopez JJ, Giordano FJ, Shah PK, Willerson JT, Benza RL, Berman DS, Gibson CM, Bajamonde A, Rundle AC, Fine J, McCluskey ER & VIVA Investigators. (2003) The VIVA trial: Vascular endothelial growth factor in Ischemia for Vascular Angiogenesis. Circulation 107: 1359-1365.
Herzig TC, Jobe SM, Aoki H, Molkentin JD, Cowley AW,Jr, Izumo S & Markham BE (1997) Angiotensin II type1a receptor gene expression in the heart: AP-1 and GATA-4 participate in the response to pressure overload. Proc Acad Natl Sci U S A 94: 7543-7548.
Higashi M, Shimokawa H, Hattori T, Hiroki J, Mukai Y, Morikawa K, Ichiki T, Takahashi S & Takeshita A (2003) Long-term inhibition of Rho-kinase suppresses angiotensin II-induced cardiovascular hypertrophy in rats in vivo: effect on endothelial NAD(P)H oxidase system. Circ Res 93: 767-775.
Higuchi Y, McTiernan CF, Frye CB, McGowan BS, Chan TO & Feldman AM (2004) Tumor necrosis factor receptors 1 and 2 differentially regulate survival, cardiac dysfunction, and remodeling in transgenic mice with tumor necrosis factor-alpha-induced cardiomyopathy. Circulation 109: 1892-1897.
Hill JA (2003) Electrical remodeling in cardiac hypertrophy. Trends Cardiovasc Med 13: 316-322. Hines WA, Thorburn J & Thorburn A (1999) Cell density and contraction regulate p38 MAP
kinase-dependent responses in neonatal rat cardiac myocytes. Am J Physiol 277: H331-H341. Honing ML, Smits P, Morrison PJ, Burnett JC,Jr & Rabelink TJ (2001) C-type natriuretic peptide-
induced vasodilation is dependent on hyperpolarization in human forearm resistance vessels. Hypertension 37: 1179-1183.
Horio T, Nishikimi T, Yoshihara F, Matsuo H, Takishita S & Kangawa K (2000) Inhibitory regulation of hypertrophy by endogenous atrial natriuretic peptide in cultured cardiac myocytes. Hypertension 35: 19-24.

109
Hreniuk D, Garay M, Gaarde W, Monia BP, McKay RA & Cioffi CL (2001) Inhibition of c-Jun N-terminal kinase 1, but not c-Jun N-terminal kinase 2, suppresses apoptosis induced by ischemia/reoxygenation in rat cardiac myocytes. Mol Pharmacol 59: 867-874.
Hu H & Sachs F (1997) Stretch-activated ion channels in the heart. J Mol Cell Cardiol 29: 1511-1523.
Hunter JJ, Tanaka N, Rockman HA, Ross J,Jr & Chien KR (1995) Ventricular expression of a MLC-2v-ras fusion gene induces cardiac hypertrophy and selective diastolic dysfunction in transgenic mice. J Biol Chem 270: 23173-23178.
Hutchins GM & Bulkley BH (1978) Infarct expansion versus extension: two different complications of acute myocardial infarction. Am J Cardiol 41: 1127-1132.
Ip HS, Wilson DB, Heikinheimo M, Tang Z, Ting CN, Simon MC, Leiden JM & Parmacek MS (1994) The GATA-4 transcription factor transactivates the cardiac muscle-specific troponin C promoter-enhancer in nonmuscle cells. Mol Cell Biol 14: 7517-7526.
Irwin MW, Mak S, Mann DL, Qu R, Penninger JM, Yan A, Dawood F, Wen WH, Shou Z & Liu P (1999) Tissue expression and immunolocalization of tumor necrosis factor-alpha in postinfarction dysfunctional myocardium. Circulation 99: 1492-1498.
Ishikawa T, Yanagisawa M, Kimura S, Goto K & Masaki T (1988a) Positive chronotropic effects of endothelin, a novel endothelium-derived vasoconstrictor peptide. Pflugers Arch 413: 108-110.
Ishikawa T, Yanagisawa M, Kimura S, Goto K & Masaki T (1988b) Positive inotropic action of novel vasoconstrictor peptide endothelin on guinea pig atria. Am J Physiol 255: H970-H973.
Ito H, Hiroe M, Hirata Y, Fujisaki H, Adachi S, Akimoto H, Ohta Y & Marumo F (1994) Endothelin ETA receptor antagonist blocks cardiac hypertrophy provoked by hemodynamic overload. Circulation 89: 2198-2203.
Ito H, Tomooka T, Sakai N, Yu H, Higashino Y, Fujii K, Masuyama T, Kitabatake A & Minamino T (1992) Lack of myocardial perfusion immediately after successful thrombolysis. A predictor of poor recovery of left ventricular function in anterior myocardial infarction. Circulation 85: 1699-1705.
Itoh G, Tamura J, Suzuki M, Suzuki Y, Ikeda H, Koike M, Nomura M, Jie T & Ito K (1995) DNA fragmentation of human infarcted myocardial cells demonstrated by the nick end labeling method and DNA agarose gel electrophoresis. Am J Pathol 146: 1325-1331.
Iwase M, Bishop SP, Uechi M, Vatner DE, Shannon RP, Kudej RK, Wight DC, Wagner TE, Ishikawa Y, Homcy CJ & Vatner SF (1996) Adverse effects of chronic endogenous sympathetic drive induced by cardiac GS alpha overexpression. Circ Res 78: 517-524.
Jackson JR, Bolognese B, Hillegass L, Kassis S, Adams J, Griswold DE & Winkler JD (1998) Pharmacological effects of SB 220025, a selective inhibitor of P38 mitogen-activated protein kinase, in angiogenesis and chronic inflammatory disease models. Journal Pharmacol Exp Ther 284: 687-692.
Jessup M & Brozena S (2003) Heart failure. New Engl J Med 348: 2007-2018. John SW, Veress AT, Honrath U, Chong CK, Peng L, Smithies O & Sonnenberg H (1996) Blood
pressure and fluid-electrolyte balance in mice with reduced or absent ANP. Am J Physiol 271: R109-R114.
Ju H, Zhao S, Tappia PS, Panagia V & Dixon IM (1998) Expression of Gq alpha and PLC-beta in scar and border tissue in heart failure due to myocardial infarction. Circulation 97: 892-899.
Kacimi R & Gerdes AM (2003) Alterations in G protein and MAP kinase signaling pathways during cardiac remodeling in hypertension and heart failure. Hypertension 41: 968-977.
Kaiser RA, Bueno OF, Lips DJ, Doevendans PA, Jones F, Kimball TF & Molkentin JD (2004) Targeted inhibition of p38 mitogen-activated protein kinase antagonizes cardiac injury and cell death following ischemia-reperfusion in vivo. J Biol Chem 279: 15524-15530.

110
Kaiser RA, Liang Q, Bueno OF, Huang Y, Lackey T, Klevitsky R, Hewett TE & Molkentin JD (2005) Genetic inhibition or activation of JNK1/2 protects the myocardium from ischemia-reperfusion-induced cell death in vivo. J Biol Chem 280: 32602-32608.
Kajstura J, Cheng W, Reiss K, Clark WA, Sonnenblick EH, Krajewski S, Reed JC, Olivetti G & Anversa P (1996) Apoptotic and necrotic myocyte cell deaths are independent contributing variables of infarct size in rats. Lab Invest 74: 86-107.
Kajstura J, Leri A, Finato N, Di Loreto C, Beltrami CA & Anversa P (1998) Myocyte proliferation in end-stage cardiac failure in humans. Proc Natl Acad Sci U S A 95: 8801-8805.
Kamihata H, Matsubara H, Nishiue T, Fujiyama S, Tsutsumi Y, Ozono R, Masaki H, Mori Y, Iba O, Tateishi E, Kosaki A, Shintani S, Murohara T, Imaizumi T & Iwasaka T (2001) Implantation of bone marrow mononuclear cells into ischemic myocardium enhances collateral perfusion and regional function via side supply of angioblasts, angiogenic ligands, and cytokines. Circulation 104: 1046-1052.
Karin M (1995) The regulation of AP-1 activity by mitogen-activated protein kinases. J Biol Chem 270: 16483-16486.
Karin M & Lin A (2002) NF-kappaB at the crossroads of life and death. Nat Immunol 3: 221-227. Karin M, Liu Z & Zandi E (1997) AP-1 function and regulation. Curr Opin Cell Biol 9: 240-246. Kariya K, Karns LR & Simpson PC (1991) Expression of a constitutively activated mutant of the
beta-isozyme of protein kinase C in cardiac myocytes stimulates the promoter of the beta-myosin heavy chain isogene. J Biol Chem 266: 10023-10026.
Kass DA, Bronzwaer JG & Paulus WJ (2004) What mechanisms underlie diastolic dysfunction in heart failure? Circ Res 94: 1533-1542.
Kato Y, Kravchenko VV, Tapping RI, Han J, Ulevitch RJ & Lee JD (1997) BMK1/ERK5 regulates serum-induced early gene expression through transcription factor MEF2C. EMBO J 16: 7054-7066.
Kawamoto A, Gwon HC, Iwaguro H, Yamaguchi JI, Uchida S, Masuda H, Silver M, Ma H, Kearney M, Isner JM & Asahara T (2001) Therapeutic potential of ex vivo expanded endothelial progenitor cells for myocardial ischemia. Circulation 103: 634-637.
Kawamoto A, Tkebuchava T, Yamaguchi J, Nishimura H, Yoon YS, Milliken C, Uchida S, Masuo O, Iwaguro H, Ma H, Hanley A, Silver M, Kearney M, Losordo DW, Isner JM & Asahara T (2003) Intramyocardial transplantation of autologous endothelial progenitor cells for therapeutic neovascularization of myocardial ischemia. Circulation 107: 461-468.
Kawamura T, Ono K, Morimoto T, Wada H, Hirai M, Hidaka K, Morisaki T, Heike T, Nakahata T, Kita T & Hasegawa K (2005) Acetylation of GATA-4 is involved in the differentiation of embryonic stem cells into cardiac myocytes. J Biol Chem 280: 19682-19688.
Kawana M, Lee ME, Quertermous EE & Quertermous T (1995) Cooperative interaction of GATA-2 and AP1 regulates transcription of the endothelin-1 gene. Mol Cell Biol 15: 4225-4231
Kelley C, Blumberg H, Zon LI & Evans T (1993) GATA-4 is a novel transcription factor expressed in endocardium of the developing heart. Development 118: 817-827.
Kerkelä R, Pikkarainen S, Majalahti-Palviainen T, Tokola H & Ruskoaho H (2002) Distinct roles of mitogen-activated protein kinase pathways in GATA-4 transcription factor-mediated regulation of B-type natriuretic peptide gene. J Biol Chem 277: 13752-13760.
Khasar SG, Lin YH, Martin A, Dadgar J, McMahon T, Wang D, Hundle B, Aley KO, Isenberg W, McCarter G, Green PG, Hodge CW, Levine JD & Messing RO (1999) A novel nociceptor signaling pathway revealed in protein kinase C epsilon mutant mice. Neuron 24: 253-260.
Kim S & Iwao H (2000) Molecular and cellular mechanisms of angiotensin II-mediated cardiovascular and renal diseases. Pharmacol Rev 52: 11-34.
Kim Y, Ma AG, Kitta K, Fitch SN, Ikeda T, Ihara Y, Simon AR, Evans T & Suzuki YJ (2003) Anthracycline-induced suppression of GATA-4 transcription factor: implication in the regulation of cardiac myocyte apoptosis. Mol Pharmacol 63: 368-377.

111
Kis A, Yellon DM & Baxter GF (2003) Second window of protection following myocardial preconditioning: an essential role for PI3 kinase and p70S6 kinase. J Mol Cell Cardiol 35: 1063-1071.
Kitta K, Clement SA, Remeika J, Blumberg JB & Suzuki YJ (2001) Endothelin-1 induces phosphorylation of GATA-4 transcription factor in the HL-1 atrial-muscle cell line. Biochem J 359: 375-380.
Kitta K, Day RM, Kim Y, Torregroza I, Evans T & Suzuki YJ (2003) Hepatocyte growth factor induces GATA-4 phosphorylation and cell survival in cardiac muscle cells. J Biol Chem 278: 4705-4712.
Knöll R, Hoshijima M & Chien K (2003) Cardiac mechanotransduction and implications for heart disease. J Mol Med 81: 750-756.
Kobayashi T, Miyauchi T, Sakai S, Kobayashi M, Yamaguchi I, Goto K & Sugishita Y (1999) Expression of endothelin-1, ETA and ETB receptors, and ECE and distribution of endothelin-1 in failing rat heart. Am J Physiol 276: H1197-H1206.
Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff D, Wang J, Homma S, Edwards NM & Itescu S (2001) Neovascularization of ischemic myocardium by human bone-marrow-derived angioblasts prevents cardiomyocyte apoptosis, reduces remodeling and improves cardiac function. Nat Med 7: 430-436.
Komatsu Y, Nakao K, Suga S, Ogawa Y, Mukoyama M, Arai H, Shirakami G, Hosoda K, Nakagawa O & Hama N (1991) C-type natriuretic peptide (CNP) in rats and humans. Endocrinology 129: 1104-1106.
Komuro I, Kaida T, Shibazaki Y, Kurabayashi M, Katoh Y, Hoh E, Takaku F & Yazaki Y (1990) Stretching cardiac myocytes stimulates protooncogene expression. J Biol Chem 265: 3595-3598.
Komuro I, Kudo S, Yamazaki T, Zou Y, Shiojima I & Yazaki Y (1996) Mechanical stretch activates the stress-activated protein kinases in cardiac myocytes. FASEB J 10: 631-636.
Kovacic-Milivojevic B & Gardner DG (1993) Regulation of the human atrial natriuretic peptide gene in atrial cardiocytes by the transcription factor AP-1. Am J Hypertens 6: 258-263.
Kudoh S, Komuro I, Hiroi Y, Zou Y, Harada K, Sugaya T, Takekoshi N, Murakami K, Kadowaki T & Yazaki Y (1998) Mechanical stretch induces hypertrophic responses in cardiac myocytes of angiotensin II type 1a receptor knockout mice. J Biol Chem 273: 24037-24043.
Kudoh S, Komuro I, Mizuno T, Yamazaki T, Zou Y, Shiojima I, Takekoshi N & Yazaki Y (1997) Angiotensin II stimulates c-Jun NH2-terminal kinase in cultured cardiac myocytes of neonatal rats. Circ Res 80: 139-146.
Kuhn M (2005) Cardiac and intestinal natriuretic peptides: insights from genetically modified mice. Peptides 26: 1078-1085.
Kuo CT, Morrisey EE, Anandappa R, Sigrist K, Lu MM, Parmacek MS, Soudais C & Leiden JM (1997) GATA4 transcription factor is required for ventral morphogenesis and heart tube formation. Genes Dev 11: 1048-1060.
Kuo H, Chen J, Ruiz-Lozano P, Zou Y, Nemer M & Chien KR (1999) Control of segmental expression of the cardiac-restricted ankyrin repeat protein gene by distinct regulatory pathways in murine cardiogenesis. Development 126: 4223-4234.
Kuwahara K, Saito Y, Nakagawa O, Kishimoto I, Harada M, Ogawa E, Miyamoto Y, Hamanaka I, Kajiyama N, Takahashi N, Izumi T, Kawakami R, Tamura N, Ogawa Y & Nakao K (1999) The effects of the selective ROCK inhibitor, Y27632, on ET-1-induced hypertrophic response in neonatal rat cardiac myocytes--possible involvement of Rho/ROCK pathway in cardiac muscle cell hypertrophy. FEBS Lett 452: 314-318.
Kyriakis JM & Avruch J (2001) Mammalian mitogen-activated protein kinase signal transduction pathways activated by stress and inflammation. Physiol Rev 81: 807-869.

112
Kyriakis JM & Avruch J (1990) pp54 microtubule-associated protein 2 kinase. A novel serine/threonine kinase regulated by phosphorylation and stimulated by poly-L-lysine. J Biol Chem 265: 17355-17363.
Laham RJ, Sellke FW, Edelman ER, Pearlman JD, Ware JA, Brown DL, Gold JP & Simons M (1999) Local perivascular delivery of basic fibroblast growth factor in patients undergoing coronary bypass surgery: results of a phase I randomized, double-blind, placebo-controlled trial. Circulation 100: 1865-1871.
Laufs U, Kilter H, Konkol C, Wassmann S, Bohm M & Nickenig G (2002) Impact of HMG CoA reductase inhibition on small GTPases in the heart. Cardiovasc Res 53: 911-920.
Lee Y, Shioi T, Kasahara H, Jobe SM, Wiese RJ, Markham BE & Izumo S (1998) The cardiac tissue-restricted homeobox protein Csx/Nkx2.5 physically associates with the zinc finger protein GATA4 and cooperatively activates atrial natriuretic factor gene expression. Mol Cell Biol 18: 3120-3129.
Lemke LE, Bloem LJ, Fouts R, Esterman M, Sandusky G & Vlahos CJ (2001) Decreased p38 MAPK activity in end-stage failing human myocardium: p38 MAPK alpha is the predominant isoform expressed in human heart. J Mol Cell Cardiol 33: 1527-1540.
Lerman A, Edwards BS, Hallett JW, Heublein DM, Sandberg SM & Burnett JC,Jr (1991) Circulating and tissue endothelin immunoreactivity in advanced atherosclerosis. The N Engl J Med 325: 997-1001.
Levin ER, Gardner DG & Samson WK (1998) Natriuretic peptides. N Engl J Med 339: 321-328. Levy D, Larson MG, Vasan RS, Kannel WB & Ho KK (1996) The progression from hypertension
to congestive heart failure. JAMA 275: 1557-1562. Li M, Georgakopoulos D, Lu G, Hester L, Kass DA, Hasday J & Wang Y (2005) p38 MAP kinase
mediates inflammatory cytokine induction in cardiomyocytes and extracellular matrix remodeling in heart. Circulation 111: 2494-2502.
Li Q, Van Antwerp D, Mercurio F, Lee KF & Verma IM (1999) Severe liver degeneration in mice lacking the IkappaB kinase 2 gene. Science 284: 321-325.
Li WG, Zaheer A, Coppey L & Oskarsson HJ (1998) Activation of JNK in the remote myocardium after large myocardial infarction in rats. Biochem Biophys Res Commun 246: 816-820.
Li Y, Ha T, Gao X, Kelley J, Williams DL, Browder IW, Kao RL & Li C (2004) NF-kappaB activation is required for the development of cardiac hypertrophy in vivo. Am J Physiol Heart Circ Physiol 287: H1712-H1720.
Li Y, Takemura G, Kosai K, Yuge K, Nagano S, Esaki M, Goto K, Takahashi T, Hayakawa K, Koda M, Kawase Y, Maruyama R, Okada H, Minatoguchi S, Mizuguchi H, Fujiwara T & Fujiwara H (2003) Postinfarction treatment with an adenoviral vector expressing hepatocyte growth factor relieves chronic left ventricular remodeling and dysfunction in mice. Circulation 107: 2499-2506.
Liang F, Wu J, Garami M & Gardner DG (1997) Mechanical strain increases expression of the brain natriuretic peptide gene in rat cardiac myocytes. J Biol Chem 272: 28050-28056.
Liang F & Gardner DG (1999) Mechanical strain activates BNP gene transcription through a p38/NF-kappaB-dependent mechanism. J Clin Invest 104: 1603-1612.
Liang F, Lu S & Gardner DG (2000) Endothelin-dependent and -independent components of strain-activated brain natriuretic peptide gene transcription require extracellular signal regulated kinase and p38 mitogen-activated protein kinase. Hypertension 35: 188-192.
Liang Q, Bueno OF, Wilkins BJ, Kuan CY, Xia Y & Molkentin JD (2003) c-Jun N-terminal kinases (JNK) antagonize cardiac growth through cross-talk with calcineurin-NFAT signaling. EMBO J 22: 5079-5089.
Liang Q, De Windt LJ, Witt SA, Kimball TR, Markham BE & Molkentin JD (2001a) The transcription factors GATA4 and GATA6 regulate cardiomyocyte hypertrophy in vitro and in vivo. J Biol Chem 276: 30245-30253.

113
Liang Q & Molkentin JD (2003) Redefining the roles of p38 and JNK signalling in cardiac hypertrophy: dichotomy between cultured myocytes and animal models. J Mol Cell Cardiol 35: 1385-1394.
Liang Q, Wiese RJ, Bueno OF, Dai YS, Markham BE & Molkentin JD (2001b) The transcription factor GATA4 is activated by extracellular signal-regulated kinase 1- and 2-mediated phosphorylation of serine 105 in cardiomyocytes. Mol Cell Biol 21: 7460-7469.
Liao P, Georgakopoulos D, Kovacs A, Zheng M, Lerner D, Pu H, Saffitz J, Chien K, Xiao RP, Kass DA & Wang Y (2001) The in vivo role of p38 MAP kinases in cardiac remodeling and restrictive cardiomyopathy. Proc Natl Acad Sci U S A 98: 12283-12288.
Liao P, Wang SQ, Wang S, Zheng M, Zheng M, Zhang SJ, Cheng H, Wang Y & Xiao RP (2002) p38 Mitogen-activated protein kinase mediates a negative inotropic effect in cardiac myocytes. Circ Res 90: 190-196.
Liew CC & Dzau VJ (2004) Molecular genetics and genomics of heart failure. Nat Rev Genet 5: 811-825.
Lin Z, Crockett DK, Jenson SD, Lim MS & Elenitoba-Johnson KS (2004) Quantitative proteomic and transcriptional analysis of the response to the p38 mitogen-activated protein kinase inhibitor SB203580 in transformed follicular lymphoma cells. Mol Cell Proteomics 3: 820-833.
Lips DJ, deWindt LJ, van Kraaij DJ & Doevendans PA (2003) Molecular determinants of myocardial hypertrophy and failure: alternative pathways for beneficial and maladaptive hypertrophy. Eur Heart J 24: 883-896.
Liu J, Farmer JD,Jr, Lane WS, Friedman J, Weissman I & Schreiber SL (1991) Calcineurin is a common target of cyclophilin-cyclosporin A and FKBP-FK506 complexes. Cell 66: 807-815.
Liu YH, Wang D, Rhaleb NE, Yang XP, Xu J, Sankey SS, Rudolph AE & Carretero OA (2005) Inhibition of p38 mitogen-activated protein kinase protects the heart against cardiac remodeling in mice with heart failure resulting from myocardial infarction. J Card Fail 11: 74-81.
Lombes M, Oblin ME, Gasc JM, Baulieu EE, Farman N & Bonvalet JP (1992) Immunohistochemical and biochemical evidence for a cardiovascular mineralocorticoid receptor. Circ Res 71: 503-510.
Lorell BH & Carabello BA (2000) Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 102: 470-479.
Lu J, McKinsey TA, Zhang CL & Olson EN (2000) Regulation of skeletal myogenesis by association of the MEF2 transcription factor with class II histone deacetylases. Mol Cell 6: 233-244.
Lu L, Chen SS, Zhang JQ, Ramires FJ & Sun Y (2004) Activation of nuclear factor-kappaB and its proinflammatory mediator cascade in the infarcted rat heart. Biochem Biophys Res Commun 321: 879-885.
Lüscher TF & Barton M (2000) Endothelins and endothelin receptor antagonists: therapeutic considerations for a novel class of cardiovascular drugs. Circulation 102: 2434-2440.
Ma XL, Kumar S, Gao F, Louden CS, Lopez BL, Christopher TA, Wang C, Lee JC, Feuerstein GZ & Yue TL (1999) Inhibition of p38 mitogen-activated protein kinase decreases cardiomyocyte apoptosis and improves cardiac function after myocardial ischemia and reperfusion. Circulation 99: 1685-1691.
MacCumber MW, Ross CA, Glaser BM & Snyder SH (1989) Endothelin: visualization of mRNAs by in situ hybridization provides evidence for local action. Proc Natl Acad Sci U S A 86: 7285-7289.
Mack CA, Patel SR, Schwarz EA, Zanzonico P, Hahn RT, Ilercil A, Devereux RB, Goldsmith SJ, Christian TF, Sanborn TA, Kovesdi I, Hackett N, Isom OW, Crystal RG & Rosengart TK (1998) Biologic bypass with the use of adenovirus-mediated gene transfer of the complementary deoxyribonucleic acid for vascular endothelial growth factor 121 improves myocardial perfusion and function in the ischemic porcine heart. J Thorac Cardiovasc Surg 115: 168-77.

114
Mackay K & Mochly-Rosen D (2001) Localization, anchoring, and functions of protein kinase C isozymes in the heart. J Mol Cell Cardiol 33: 1301-1307.
Magga J, Marttila M, Mantymaa P, Vuolteenaho O & Ruskoaho H (1994) Brain natriuretic peptide in plasma, atria, and ventricles of vasopressin- and phenylephrine-infused conscious rats. Endocrinology 134: 2505-2515.
Magga J, Vuolteenaho O, Marttila M & Ruskoaho H (1997a) Endothelin-1 is involved in stretch-induced early activation of B-type natriuretic peptide gene expression in atrial but not in ventricular myocytes: acute effects of mixed ET(A)/ET(B) and AT1 receptor antagonists in vivo and in vitro. Circulation 96: 3053-3062.
Magga J, Vuolteenaho O, Tokola H, Marttila M & Ruskoaho H (1997b) Involvement of transcriptional and posttranscriptional mechanisms in cardiac overload-induced increase of B-type natriuretic peptide gene expression. Circ Res 81: 694-702.
Malhotra A, Kang BP, Opawumi D, Belizaire W & Meggs LG (2001) Molecular biology of protein kinase C signaling in cardiac myocytes. Mol Cell Biochem 225: 97-107.
Mann DL (2003) Stress-activated cytokines and the heart: from adaptation to maladaptation. Annu Rev Physiol 65: 81-101.
Marinissen MJ, Chiariello M, Pallante M & Gutkind JS (1999) A network of mitogen-activated protein kinases links G protein-coupled receptors to the c-jun promoter: a role for c-Jun NH2-terminal kinase, p38s, and extracellular signal-regulated kinase 5. Mol Cell Biol 19: 4289-4301.
Martindale JJ, Wall JA, Martinez-Longoria DM, Aryal P, Rockman HA, Guo Y, Bolli R & Glembotski CC (2005) Overexpression of mitogen-activated protein kinase kinase 6 in the heart improves functional recovery from ischemia in vitro and protects against myocardial infarction in vivo. J Biol Chem 280: 669-676.
Marttila M, Hautala N, Paradis P, Toth M, Vuolteenaho O, Nemer M & Ruskoaho H (2001) GATA4 mediates activation of the B-type natriuretic peptide gene expression in response to hemodynamic stress. Endocrinology 142: 4693-4700.
Marzo KP, Frey MJ, Wilson JR, Liang BT, Manning DR, Lanoce V & Molinoff PB (1991) Beta-adrenergic receptor-G protein-adenylate cyclase complex in experimental canine congestive heart failure produced by rapid ventricular pacing. Circulation research 69: 1546-1556.
McGrew MJ, Bogdanova N, Hasegawa K, Hughes SH, Kitsis RN & Rosenthal N (1996) Distinct gene expression patterns in skeletal and cardiac muscle are dependent on common regulatory sequences in the MLC1/3 locus. Mol Cell Biol 16: 4524-4534.
McKinsey TA, Zhang CL, Lu J & Olson EN (2000a) Signal-dependent nuclear export of a histone deacetylase regulates muscle differentiation. Nature 408: 106-111.
McKinsey TA, Zhang CL & Olson EN (2000b) Activation of the myocyte enhancer factor-2 transcription factor by calcium/calmodulin-dependent protein kinase-stimulated binding of 14-3-3 to histone deacetylase 5. Proc Natl Acad Sci U S A 97: 14400-14405.
McClellan G, Weisberg A, Rose D & Winegrad S (1994) Endothelial cell storage and release of endothelin as a cardioregulatory mechanism. Circ Res 75: 85-96.
McMullen JR, Shioi T, Zhang L, Tarnavski O, Sherwood MC, Kang PM & Izumo S (2003) Phosphoinositide 3-kinase(p110alpha) plays a critical role for the induction of physiological, but not pathological, cardiac hypertrophy. Proc Natl Acad Sci U S A 100: 12355-12360
Meerson FZ (1961) On the mechanism of compensatory hyperfunction and insufficiency of the heart. Cor Vasa (3): 161-177.
Meoli DF, Sadeghi MM, Krassilnikova S, Bourke BN, Giordano FJ, Dione DP, Su H, Edwards DS, Liu S, Harris TD, Madri JA, Zaret BL & Sinusas AJ (2004) Noninvasive imaging of myocardial angiogenesis following experimental myocardial infarction. J Clin Invest 113: 1684-1691.
Miano JM (2003) Serum response factor: toggling between disparate programs of gene expression. J Mol Cell Cardiol 35: 577-593.

115
Miano JM, Ramanan N, Georger MA, de Mesy Bentley KL, Emerson RL, Balza RO,Jr, Xiao Q, Weiler H, Ginty DD & Misra RP (2004) Restricted inactivation of serum response factor to the cardiovascular system. Proc Natl Acad Sci U S A 101: 17132-17137.
Michel MC, Li Y & Heusch G (2001) Mitogen-activated protein kinases in the heart. Naunyn-Schmiedebergs Arch Pharmacol 363: 245-266.
Minamino T, Yujiri T, Terada N, Taffet GE, Michael LH, Johnson GL & Schneider MD (2002) MEKK1 is essential for cardiac hypertrophy and dysfunction induced by Gq. Proc Natl Acad Sci U S A 99: 3866-3871.
Miyagawa S, Sawa Y, Taketani S, Kawaguchi N, Nakamura T, Matsuura N & Matsuda H (2002) Myocardial regeneration therapy for heart failure: hepatocyte growth factor enhances the effect of cellular cardiomyoplasty. Circulation 105: 2556-2561.
Mizukami Y & Yoshida K (1997) Mitogen-activated protein kinase translocates to the nucleus during ischaemia and is activated during reperfusion. Biochem J 323: 785-790.
Mizuno Y, Yoshimura M, Yasue H, Sakamoto T, Ogawa H, Kugiyama K, Harada E, Nakayama M, Nakamura S, Ito T, Shimasaki Y, Saito Y & Nakao K (2001) Aldosterone production is activated in failing ventricle in humans. Circulation 103: 72-77.
Mockridge JW, Marber MS & Heads RJ (2000) Activation of Akt during simulated ischemia/reperfusion in cardiac myocytes. Biochem Biophys Res Commun 270: 947-952.
Molkentin JD (2000a) Calcineurin and beyond: cardiac hypertrophic signaling. Circ Res 87: 731-738.
Molkentin JD (2000b) The zinc finger-containing transcription factors GATA-4, -5, and -6. Ubiquitously expressed regulators of tissue-specific gene expression. J Biol Chem 275: 38949-38952.
Molkentin JD & Dorn II GW (2001) Cytoplasmic signaling pathways that regulate cardiac hypertrophy. Annu Rev Physiol 63: 391-426.
Molkentin JD, Lin Q, Duncan SA & Olson EN (1997) Requirement of the transcription factor GATA4 for heart tube formation and ventral morphogenesis. Genes Dev 11: 1061-1072.
Molkentin JD, Lu JR, Antos CL, Markham B, Richardson J, Robbins J, Grant SR & Olson EN (1998) A calcineurin-dependent transcriptional pathway for cardiac hypertrophy. Cell 93: 215-228.
Molkentin JD, Tymitz KM, Richardson JA & Olson EN (2000) Abnormalities of the genitourinary tract in female mice lacking GATA5. Mol Cell Biol 20: 5256-5260.
Montessuit C, Rosenblatt-Velin N, Papageorgiou I, Campos L, Pellieux C, Palma T & Lerch R (2004) Regulation of glucose transporter expression in cardiac myocytes: p38 MAPK is a strong inducer of GLUT4. Cardiovasc Res 64: 94-104.
Morimoto T, Hasegawa K, Kaburagi S, Kakita T, Wada H, Yanazume T & Sasayama S (2000) Phosphorylation of GATA-4 is involved in alpha 1-adrenergic agonist-responsive transcription of the endothelin-1 gene in cardiac myocytes. J Biol Chem 275: 13721-13726.
Morin S, Charron F, Robitaille L & Nemer M (2000) GATA-dependent recruitment of MEF2 proteins to target promoters. EMBO J 19: 2046-2055.
Morisco C, Seta K, Hardt SE, Lee Y, Vatner SF & Sadoshima J (2001) Glycogen synthase kinase 3beta regulates GATA4 in cardiac myocytes. J Biol Chem 276: 28586-28597.
Morisco C, Zebrowski D, Condorelli G, Tsichlis P, Vatner SF & Sadoshima J (2000) The Akt-glycogen synthase kinase 3beta pathway regulates transcription of atrial natriuretic factor induced by beta-adrenergic receptor stimulation in cardiac myocytes. J Biol Chem 275: 14466-14475.
Morishita R, Sugimoto T, Aoki M, Kida I, Tomita N, Moriguchi A, Maeda K, Sawa Y, Kaneda Y, Higaki J & Ogihara T (1997) In vivo transfection of cis element "decoy" against nuclear factor-kappaB binding site prevents myocardial infarction. Nat Med 3: 894-899.

116
Morita H, Seidman J & Seidman CE (2005) Genetic causes of human heart failure. J Clin Invest 115: 518-526.
Morrisey EE, Ip HS, Tang Z & Parmacek MS (1997) GATA-4 activates transcription via two novel domains that are conserved within the GATA-4/5/6 subfamily. J Biol Chem 272: 8515-8524.
Morrisey EE, Tang Z, Sigrist K, Lu MM, Jiang F, Ip HS & Parmacek MS (1998) GATA6 regulates HNF4 and is required for differentiation of visceral endoderm in the mouse embryo. Genes Dev 12: 3579-3590.
Murriel CL, Churchill E, Inagaki K, Szweda LI & Mochly-Rosen D (2004) Protein kinase Cdelta activation induces apoptosis in response to cardiac ischemia and reperfusion damage: a mechanism involving BAD and the mitochondria. J Biol Chem 279: 47985-47991.
Nadruz W, Kobarg CB, Constancio SS, Corat PD & Franchini KG (2003) Load-induced transcriptional activation of c-jun in rat myocardium: regulation by myocyte enhancer factor 2. Circ Res 92: 243-251.
Nakagawa O, Ogawa Y, Itoh H, Suga S, Komatsu Y, Kishimoto I, Nishino K, Yoshimasa T & Nakao K (1995) Rapid transcriptional activation and early mRNA turnover of brain natriuretic peptide in cardiocyte hypertrophy. Evidence for brain natriuretic peptide as an "emergency" cardiac hormone against ventricular overload. J Clin Invest 96: 1280-1287.
Nakano K, Corin WJ, Spann JF,Jr, Biederman RW, Denslow S & Carabello BA (1989) Abnormal subendocardial blood flow in pressure overload hypertrophy is associated with pacing-induced subendocardial dysfunction. Circ Res 65: 1555-1564.
Nakao K, Ogawa Y, Suga S & Imura H (1992) Molecular biology and biochemistry of the natriuretic peptide system. II: Natriuretic peptide receptors. J Hypertens 10: 1111-1114.
Narula J, Haider N, Virmani R, DiSalvo TG, Kolodgie FD, Hajjar RJ, Schmidt U, Semigran MJ, Dec GW & Khaw BA (1996) Apoptosis in myocytes in end-stage heart failure. N Engl J Med 335: 1182-1189.
Nelson TJ, Balza R,Jr, Xiao Q & Misra RP (2005) SRF-dependent gene expression in isolated cardiomyocytes: regulation of genes involved in cardiac hypertrophy. J Mol Cell Cardiol 39: 479-489.
Nemoto S, Sheng Z & Lin A (1998) Opposing effects of Jun kinase and p38 mitogen-activated protein kinases on cardiomyocyte hypertrophy. Mol Cell Biol 18: 3518-3526.
Netticadan T, Temsah RM, Kawabata K & Dhalla NS (2000) Sarcoplasmic reticulum Ca(2+)/Calmodulin-dependent protein kinase is altered in heart failure. Circ Res 86: 596-605.
Neumann J, Schmitz W, Scholz H, von Meyerinck L, Doring V & Kalmar P (1988) Increase in myocardial Gi-proteins in heart failure. Lancet 2: 936-937.
Nian M, Lee P, Khaper N & Liu P (2004) Inflammatory cytokines and postmyocardial infarction remodeling. Circ Res 94: 1543-1553.
Nishida K, Yamaguchi O, Hirotani S, Hikoso S, Higuchi Y, Watanabe T, Takeda T, Osuka S, Morita T, Kondoh G, Uno Y, Kashiwase K, Taniike M, Nakai A, Matsumura Y, Miyazaki J, Sudo T, Hongo K, Kusakari Y, Kurihara S, Chien KR, Takeda J, Hori M & Otsu K (2004) p38alpha mitogen-activated protein kinase plays a critical role in cardiomyocyte survival but not in cardiac hypertrophic growth in response to pressure overload. Mol Cell Biol 24: 10611-10620.
Ogawa Y, Itoh H, Tamura N, Suga S, Yoshimasa T, Uehira M, Matsuda S, Shiono S, Nishimoto H & Nakao K (1994) Molecular cloning of the complementary DNA and gene that encode mouse brain natriuretic peptide and generation of transgenic mice that overexpress the brain natriuretic peptide gene. J Clin Invest 93: 1911-1921.
Oh H, Bradfute SB, Gallardo TD, Nakamura T, Gaussin V, Mishina Y, Pocius J, Michael LH, Behringer RR, Garry DJ, Entman ML & Schneider MD (2003) Cardiac progenitor cells from adult myocardium: homing, differentiation, and fusion after infarction. Proc Natl Acad Sci U S A 100: 12313-12318.

117
Oka T, Dai YS & Molkentin JD (2005) Regulation of calcineurin through transcriptional induction of the calcineurin A beta promoter in vitro and in vivo. Mol Cell Biol 25: 6649-6659.
Okubo A, Miyoshi O, Baba K, Takagi M, Tsukamoto K, Kinoshita A, Yoshiura K, Kishino T, Ohta T, Niikawa N & Matsumoto N (2004) A novel GATA4 mutation completely segregated with atrial septal defect in a large Japanese family. J Med Genet 41: e97.
Olivetti G, Abbi R, Quaini F, Kajstura J, Cheng W, Nitahara JA, Quaini E, Di Loreto C, Beltrami CA, Krajewski S, Reed JC & Anversa P (1997) Apoptosis in the failing human heart. N Engl J Med 336: 1131-1141.
Olson EN, Perry M & Schulz RA (1995) Regulation of muscle differentiation by the MEF2 family of MADS box transcription factors. Dev Biol 172: 2-14
Omura T, Yoshiyama M, Shimada T, Shimizu N, Kim S, Iwao H, Takeuchi K & Yoshikawa J (1999) Activation of mitogen-activated protein kinases in in vivo ischemia/reperfused myocardium in rats. J Mol Cell Cardiol 31: 1269-1279.
Ono K, Matsumori A, Shioi T, Furukawa Y & Sasayama S (1998) Cytokine gene expression after myocardial infarction in rat hearts: possible implication in left ventricular remodeling. Circulation 98: 149-156.
Oskarsson HJ, Coppey L, Weiss RM & Li WG (2000) Antioxidants attenuate myocyte apoptosis in the remote non-infarcted myocardium following large myocardial infarction. Cardiovasc Res 45: 679-687.
Pan J, Hinzmann B, Yan W, Wu F, Morser J & Wu Q (2002) Genomic structures of the human and murine corin genes and functional GATA elements in their promoters. J Biol Chem 277: 38390-38398.
Parlakian A, Tuil D, Hamard G, Tavernier G, Hentzen D, Concordet JP, Paulin D, Li Z & Daegelen D (2004) Targeted inactivation of serum response factor in the developing heart results in myocardial defects and embryonic lethality. Mol Cell Biol 24: 5281-5289.
Passier R, Zeng H, Frey N, Naya FJ, Nicol RL, McKinsey TA, Overbeek P, Richardson JA, Grant SR & Olson EN (2000) CaM kinase signaling induces cardiac hypertrophy and activates the MEF2 transcription factor in vivo. J Clin Invest 105: 1395-1406.
Patient RK & McGhee JD (2002) The GATA family (vertebrates and invertebrates). Curr Opin Gen Dev 12: 416-422.
Patrucco E, Notte A, Barberis L, Selvetella G, Maffei A, Brancaccio M, Marengo S, Russo G, Azzolino O, Rybalkin SD, Silengo L, Altruda F, Wetzker R, Wymann MP, Lembo G & Hirsch E (2004) PI3Kgamma modulates the cardiac response to chronic pressure overload by distinct kinase-dependent and -independent effects. Cell 118: 375-387.
Pellieux C, Sauthier T, Aubert JF, Brunner HR & Pedrazzini T (2000) Angiotensin II-induced cardiac hypertrophy is associated with different mitogen-activated protein kinase activation in normotensive and hypertensive mice. J Hypertens 18: 1307-1317.
Peterkin T, Gibson A, Loose M & Patient R (2005) The roles of GATA-4, -5 and -6 in vertebrate heart development. Semin Cell Dev Biol 16: 83-94.
Peterkin T, Gibson A & Patient R (2003) GATA-6 maintains BMP-4 and Nkx2 expression during cardiomyocyte precursor maturation. EMBO J 22: 4260-4273.
Petrich BG, Eloff BC, Lerner DL, Kovacs A, Saffitz JE, Rosenbaum DS & Wang Y (2004) Targeted activation of c-Jun N-terminal kinase in vivo induces restrictive cardiomyopathy and conduction defects. J Biol Chem 279: 15330-15338.
Pfeffer MA & Braunwald E (1990) Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 81: 1161-1172.
Pfeffer MA, Pfeffer JM, Fishbein MC, Fletcher PJ, Spadaro J, Kloner RA & Braunwald E (1979) Myocardial infarct size and ventricular function in rats. Circ. Res. 13: 293-316.
Pham FH, Sugden PH & Clerk A (2000) Regulation of protein kinase B and 4E-BP1 by oxidative stress in cardiac myocytes. Circ Res 86: 1252-1258.

118
Pieruzzi F, Abassi ZA & Keiser HR (1995) Expression of renin-angiotensin system components in the heart, kidneys, and lungs of rats with experimental heart failure. Circulation 92: 3105-3112.
Pikkarainen S, Tokola H, Kerkelä R & Ruskoaho H (2004) GATA transcription factors in the developing and adult heart. Cardiovasc Res 63: 196-207.
Pikkarainen S, Tokola H, Majalahti-Palviainen T, Kerkelä R, Hautala N, Bhalla SS, Charron F, Nemer M, Vuolteenaho O & Ruskoaho H (2003) GATA-4 is a nuclear mediator of mechanical stretch-activated hypertrophic program. J Biol Chem 278: 23807-23816.
Ping P (2003) A new chapter in cardiac PKC signaling studies: searching for isoform-specific molecular targets. Focus on: "isoenzyme-selective regulation of SERCA2 gene expression by protein kinase C in neonatal rat ventricular myocytes". Am J Physiol Cell Physiol 285: C19-C21.
Post GR, Goldstein D, Thuerauf DJ, Glembotski CC & Brown JH (1996) Dissociation of p44 and p42 mitogen-activated protein kinase activation from receptor-induced hypertrophy in neonatal rat ventricular myocytes. J Biol Chem 271: 8452-8457.
Pracyk JB, Tanaka K, Hegland DD, Kim KS, Sethi R, Rovira II, Blazina DR, Lee L, Bruder JT, Kovesdi I, Goldshmidt-Clermont PJ, Irani K & Finkel T (1998) A requirement for the rac1 GTPase in the signal transduction pathway leading to cardiac myocyte hypertrophy. J Clin Invest 102: 929-937.
Prasad SV, Perrino C & Rockman HA (2003) Role of phosphoinositide 3-kinase in cardiac function and heart failure. Trends Cardiovasc Med 13: 206-212.
Prywes R & Roeder RG (1987) Purification of the c-fos enhancer-binding protein. Mol Cell Biol 7: 3482-3489.
Pu WT, Ishiwata T, Juraszek AL, Ma Q & Izumo S (2004) GATA4 is a dosage-sensitive regulator of cardiac morphogenesis. Dev Biol 275: 235-244.
Purcell NH & Molkentin JD (2003) Is nuclear factor kappaB an attractive therapeutic target for treating cardiac hypertrophy? Circulation 108: 638-640.
Purcell NH, Tang G, Yu C, Mercurio F, DiDonato JA & Lin A (2001) Activation of NF-kappa B is required for hypertrophic growth of primary rat neonatal ventricular cardiomyocytes. Proc Natl Acad Sci U S A 98: 6668-6673.
Qiu Y, Ping P, Tang XL, Manchikalapudi S, Rizvi A, Zhang J, Takano H, Wu WJ, Teschner S & Bolli R (1998) Direct evidence that protein kinase C plays an essential role in the development of late preconditioning against myocardial stunning in conscious rabbits and that epsilon is the isoform involved. J Clin Invest 101: 2182-2198.
Rajanayagam MA, Shou M, Thirumurti V, Lazarous DF, Quyyumi AA, Goncalves L, Stiber J, Epstein SE & Unger EF (2000) Intracoronary basic fibroblast growth factor enhances myocardial collateral perfusion in dogs. J Am Coll Cardiol 35: 519-526.
Rakusan K, Flanagan MF, Geva T, Southern J & Van Praagh R (1992) Morphometry of human coronary capillaries during normal growth and the effect of age in left ventricular pressure-overload hypertrophy. Circulation 86: 38-46.
Ramirez MT, Sah VP, Zhao XL, Hunter JJ, Chien KR & Brown JH (1997) The MEKK-JNK pathway is stimulated by alpha1-adrenergic receptor and ras activation and is associated with in vitro and in vivo cardiac hypertrophy. J Biol Chem 272: 14057-14061.
Rapacciuolo A, Esposito G, Caron K, Mao L, Thomas SA & Rockman HA (2001) Important role of endogenous norepinephrine and epinephrine in the development of in vivo pressure-overload cardiac hypertrophy. J Am Coll Cardiol 38: 876-882.
Ravingerova T, Barancik M & Strniskova M (2003) Mitogen-activated protein kinases: a new therapeutic target in cardiac pathology. Mol Cell Biochem 247: 127-138.
Ray LB & Sturgill TW (1988) Insulin-stimulated microtubule-associated protein kinase is phosphorylated on tyrosine and threonine in vivo. Proc Natl Acad Sci U S A 85: 3753-3757.

119
Remme WJ, Swedberg K & Task Force for the Diagnosis and Treatment of Chronic Heart Failure, European Society of Cardiology. (2001) Guidelines for the diagnosis and treatment of chronic heart failure. Eur Heart J 22: 1527-1560.
Remondino A, Kwon SH, Communal C, Pimentel DR, Sawyer DB, Singh K & Colucci WS (2003) Beta-adrenergic receptor-stimulated apoptosis in cardiac myocytes is mediated by reactive oxygen species/c-Jun NH2-terminal kinase-dependent activation of the mitochondrial pathway. Circ Res 92: 136-138.
Remuzzi G, Perico N & Benigni A (2002) New therapeutics that antagonize endothelin: promises and frustrations. Nat Rev Drug Discov 1: 986-1001.
Ritchie ME (1998) Nuclear factor-kappaB is selectively and markedly activated in humans with unstable angina pectoris. Circulation 98: 1707-1713.
Rivkees SA, Chen M, Kulkarni J, Browne J & Zhao Z (1999) Characterization of the murine A1 adenosine receptor promoter, potent regulation by GATA-4 and Nkx2.5. J Biol Chem 274: 14204-14209.
Rockman HA, Koch WJ & Lefkowitz RJ (2002) Seven-transmembrane-spanning receptors and heart function. Nature 415: 206-212.
Roman BB, Geenen DL, Leitges M & Buttrick PM (2001) PKC-beta is not necessary for cardiac hypertrophy. Am J Physiol Heart Circ Physiol 280: H2264-H2270.
Rosoff ML & Nathanson NM (1998) GATA factor-dependent regulation of cardiac m2 muscarinic acetylcholine gene transcription. J Biol Chem 273: 9124-9129.
Ross RS, Pham C, Shai SY, Goldhaber JI, Fenczik C, Glembotski CC, Ginsberg MH & Loftus JC (1998) Beta1 integrins participate in the hypertrophic response of rat ventricular myocytes. Circ Res 82: 1160-1172.
Rousseau S, Houle F, Landry J & Huot J (1997) p38 MAP kinase activation by vascular endothelial growth factor mediates actin reorganization and cell migration in human endothelial cells. Oncogene 15: 2169-2177.
Ruskoaho H (2003) Cardiac hormones as diagnostic tools in heart failure. Endocr Rev 24: 341-356. Ruskoaho H (1992) Atrial natriuretic peptide: synthesis, release, and metabolism. Pharmacol Rev
44: 479-602. Ruskoaho H, Tholken H & Lang RE (1986) Increase in atrial pressure releases atrial natriuretic
peptide from isolated perfused rat hearts. Pflugers Arch 407: 170-174. Ruwhof C & van der Laarse A (2000) Mechanical stress-induced cardiac hypertrophy: mechanisms
and signal transduction pathways. Cardiovasc Res 47: 23-37. Rysä J, Leskinen H, Ilves M & Ruskoaho H (2005) Distinct upregulation of extracellular matrix
genes in transition from hypertrophy to hypertensive heart failure. Hypertension 45: 927-933. Saadane N, Alpert L & Chalifour LE (1999) Expression of immediate early genes, GATA-4, and
Nkx-2.5 in adrenergic-induced cardiac hypertrophy and during regression in adult mice. Br J Pharmacol 127: 1165-1176.
Sadoshima J, Xu Y, Slayter HS & Izumo S (1993) Autocrine release of angiotensin II mediates stretch-induced hypertrophy of cardiac myocytes in vitro. Cell 75: 977-984.
Sadoshima J & Izumo S (1997) The cellular and molecular response of cardiac myocytes to mechanical stress. Annu Rev Physiol 59: 551-571.
Sadoshima J, Takahashi T, Jahn L & Izumo S (1992) Roles of mechano-sensitive ion channels, cytoskeleton, and contractile activity in stretch-induced immediate-early gene expression and hypertrophy of cardiac myocytes. Proc Natl Acad Sci U S A 89: 9905-9909.
Sadoshima J, Montagne O, Wang Q, Yang G, Warden J, Liu J, Takagi G, Karoor V, Hong C, Johnson GL, Vatner DE & Vatner SF (2002) The MEKK1-JNK pathway plays a protective role in pressure overload but does not mediate cardiac hypertrophy. J Clin Invest 110: 271-279.

120
Sah VP, Hoshijima M, Chien KR & Brown JH (1996) Rho is required for Galphaq and alpha1-adrenergic receptor signaling in cardiomyocytes. Dissociation of Ras and Rho pathways. J Biol Chem 271: 31185-31190.
Sah VP, Minamisawa S, Tam SP, Wu TH, Dorn GW,2nd, Ross J,Jr, Chien KR & Brown JH (1999) Cardiac-specific overexpression of RhoA results in sinus and atrioventricular nodal dysfunction and contractile failure. J Clin Invest 103: 1627-1634.
Sakai S, Miyauchi T, Kobayashi M, Yamaguchi I, Goto K & Sugishita Y (1996a) Inhibition of myocardial endothelin pathway improves long-term survival in heart failure. Nature 384: 353-355.
Sakai S, Miyauchi T, Sakurai T, Kasuya Y, Ihara M, Yamaguchi I, Goto K & Sugishita Y (1996b) Endogenous endothelin-1 participates in the maintenance of cardiac function in rats with congestive heart failure. Marked increase in endothelin-1 production in the failing heart. Circulation 93: 1214-1222.
Sakata Y, Hoit BD, Liggett SB, Walsh RA & Dorn GW,2nd (1998) Decompensation of pressure-overload hypertrophy in G alpha q-overexpressing mice. Circulation 97: 1488-1495.
Saklatvala J (2004) The p38 MAP kinase pathway as a therapeutic target in inflammatory disease. Curr Opin Pharmacol 4(4): 372-377.
Sakurai T, Yanagisawa M, Takuwa Y, Miyazaki H, Kimura S, Goto K & Masaki T (1990) Cloning of a cDNA encoding a non-isopeptide-selective subtype of the endothelin receptor. Nature 348: 732-735.
Sam F, Sawyer DB, Chang DL, Eberli FR, Ngoy S, Jain M, Amin J, Apstein CS & Colucci WS (2000) Progressive left ventricular remodeling and apoptosis late after myocardial infarction in mouse heart. Am J Physiol Heart Circ Physiol 279: H422-H428.
Saraste A, Pulkki K, Kallajoki M, Henriksen K, Parvinen M & Voipio-Pulkki LM (1997) Apoptosis in human acute myocardial infarction. Circulation 95: 320-323.
Sato M, Cordis GA, Maulik N & Das DK (2000) SAPKs regulation of ischemic preconditioning. Am J Physiol Heart Circ Physiol 279: H901-H907.
Schaper W & Ito WD (1996) Molecular mechanisms of coronary collateral vessel growth. Circ Res 79: 911-919.
Schlüter KD, Simm A, Schafer M, Taimor G & Piper HM (1999) Early response kinase and PI 3-kinase activation in adult cardiomyocytes and their role in hypertrophy. Am J Physiol 276: H1655-H1663.
Schnabel P & Bohm M (1996) Heterotrimeric G proteins in heart disease. Cell Signal 8: 413-423. Schneider S, Chen W, Hou J, Steenbergen C & Murphy E (2001) Inhibition of p38 MAPK
alpha/beta reduces ischemic injury and does not block protective effects of preconditioning. Am J Physiol Heart Circ Physiol 280: H499-H508.
Schreiber SS, Oratz M, Evans CD, Gueyikian I & Rothschild MA (1970) Myosin, myoglobin, and collagen synthesis in acute cardiac overload. Am J Physiol 219: 481-486.
Schrier RW & Abraham WT (1999) Hormones and hemodynamics in heart failure. N Engl J Med 341: 577-585.
Scotland RS, Ahluwalia A & Hobbs AJ (2005) C-type natriuretic peptide in vascular physiology and disease. Pharmacol Ther 105: 85-93.
Scott BA, Lawrence B, Nguyen HH & Meyer WJ (1987) Aldosterone and dexamethasone binding in human arterial smooth muscle cells. J Hypertens 5: 739-744.
See F, Thomas W, Way K, Tzanidis A, Kompa A, Lewis D, Itescu S & Krum H (2004) p38 mitogen-activated protein kinase inhibition improves cardiac function and attenuates left ventricular remodeling following myocardial infarction in the rat. J Am Coll Cardiol 44: 1679-1689.
Shaulian E & Karin M (2002) AP-1 as a regulator of cell life and death. Nat Cell Biol 4: E131-E136.

121
Shimizu N, Yoshiyama M, Omura T, Hanatani A, Kim S, Takeuchi K, Iwao H & Yoshikawa J (1998) Activation of mitogen-activated protein kinases and activator protein-1 in myocardial infarction in rats. Cardiovasc Res 38: 116-124.
Shioi T, Kang PM, Douglas PS, Hampe J, Yballe CM, Lawitts J, Cantley LC & Izumo S (2000) The conserved phosphoinositide 3-kinase pathway determines heart size in mice. EMBO J 19: 2537-2548.
Shioi T, McMullen JR, Kang PM, Douglas PS, Obata T, Franke TF, Cantley LC & Izumo S (2002) Akt/protein kinase B promotes organ growth in transgenic mice. Mol Cell Biol 22: 2799-2809.
Shiojima I, Sato K, Izumiya Y, Schiekofer S, Ito M, Liao R, Colucci WS & Walsh K (2005) Disruption of coordinated cardiac hypertrophy and angiogenesis contributes to the transition to heart failure. J Clin Invest 115: 2108-2118.
Silvestre JS, Heymes C, Oubenaissa A, Robert V, Aupetit-Faisant B, Carayon A, Swynghedauw B & Delcayre C (1999) Activation of cardiac aldosterone production in rat myocardial infarction: effect of angiotensin II receptor blockade and role in cardiac fibrosis. Circulation 99: 2694-2701.
Simonis G, Honold J, Schwarz K, Braun MU & Strasser RH (2002) Regulation of the isozymes of protein kinase C in the surviving rat myocardium after myocardial infarction: distinct modulation for PKC-alpha and for PKC-delta. Basic Res Cardiol 97: 223-231.
Simons M, Bonow RO, Chronos NA, Cohen DJ, Giordano FJ, Hammond HK, Laham RJ, Li W, Pike M, Sellke FW, Stegmann TJ, Udelson JE & Rosengart TK (2000) Clinical trials in coronary angiogenesis: issues, problems, consensus: An expert panel summary. Circulation 102: 73-86.
Soini Y, Virkajarvi N, Lehto VP & Paakko P (1996) Hepatocellular carcinomas with a high proliferation index and a low degree of apoptosis and necrosis are associated with a shortened survival. Br J Cancer 73: 1025-1030.
Steinhelper ME, Cochrane KL & Field LJ (1990) Hypotension in transgenic mice expressing atrial natriuretic factor fusion genes. Hypertension 16: 301-307.
Strait JB,3rd, Martin JL, Bayer A, Mestril R, Eble DM & Samarel AM (2001) Role of protein kinase C-epsilon in hypertrophy of cultured neonatal rat ventricular myocytes. Am J Physiol Heart Circ Physiol 280: H756-H766.
Strauer BE (1990) Significance of coronary circulation in hypertensive heart disease for development and prevention of heart failure. Am J Cardiol 65: 34G-41G.
Strauer BE, Schwartzkopff B, Motz W & Vogt M (1991) Coronary vascular changes in the progression and regression of hypertensive heart disease. J Cardiovasc Pharmacol 18: S20-S27.
Strohm C, Barancik T, Bruhl ML, Kilian SA & Schaper W (2000) Inhibition of the ER-kinase cascade by PD98059 and UO126 counteracts ischemic preconditioning in pig myocardium. J Cardiovasc Pharmacol 36: 218-229.
Strömer H, Cittadini A, Szymanska G, Apstein CS & Morgan JP (1997) Validation of different methods to compare isovolumic cardiac function in isolated hearts of varying sizes. Am J Physiol 272: H501-H510.
Sudoh T, Kangawa K, Minamino N & Matsuo H (1988) A new natriuretic peptide in porcine brain. Nature 332: 78-81.
Sudoh T, Minamino N, Kangawa K & Matsuo H (1990) C-type natriuretic peptide (CNP): a new member of natriuretic peptide family identified in porcine brain. Biochem Biophys Res Commun 168: 863-870.
Sugden PH (2003) Ras, Akt, and mechanotransduction in the cardiac myocyte. Circ Res 93: 1179-1192.
Sugden PH & Clerk A (1998a) Cellular mechanisms of cardiac hypertrophy. J Mol Med 76: 725-746.

122
Sugden PH & Clerk A (1998b) "Stress-responsive" mitogen-activated protein kinases (c-Jun N-terminal kinases and p38 mitogen-activated protein kinases) in the myocardium. Circ Res 83: 345-352
Sugden PH & Clerk A (2000) Activation of the small GTP-binding protein Ras in the heart by hypertrophic agonists. Trends Cardiovasc Med 10: 1-8.
Sugden PH & Clerk A (1998c) Regulation of mitogen-activated protein kinase cascades in the heart. Adv Enzyme Regul 38: 87-98.
Suo M, Hautala N, Foldes G, Szokodi I, Toth M, Leskinen H, Uusimaa P, Vuolteenaho O, Nemer M & Ruskoaho H (2002) Posttranscriptional control of BNP gene expression in angiotensin II-induced hypertension. Hypertension 39: 803-808.
Sussman MA, Welch S, Walker A, Klevitsky R, Hewett TE, Price RL, Schaefer E & Yager K (2000) Altered focal adhesion regulation correlates with cardiomyopathy in mice expressing constitutively active rac1. J Clin Invest 105: 875-886.
Sutton MG & Sharpe N (2000) Left ventricular remodeling after myocardial infarction: pathophysiology and therapy. Circulation 101: 2981-2988.
Suzuki G, Morita H, Mishima T, Sharov VG, Todor A, Tanhehco EJ, Rudolph AE, McMahon EG, Goldstein S & Sabbah HN (2002) Effects of long-term monotherapy with eplerenone, a novel aldosterone blocker, on progression of left ventricular dysfunction and remodeling in dogs with heart failure. Circulation 106: 2967-2972.
Suzuki K, Murtuza B, Smolenski RT, Sammut IA, Suzuki N, Kaneda Y & Yacoub MH (2001) Cell transplantation for the treatment of acute myocardial infarction using vascular endothelial growth factor-expressing skeletal myoblasts. Circulation 104: I207-12.
Suzuki T, Kumazaki T & Mitsui Y (1993) Endothelin-1 is produced and secreted by neonatal rat cardiac myocytes in vitro. Biochem Biophys Res Commun 191: 823-830.
Suzuki YJ & Evans T (2004) Regulation of cardiac myocyte apoptosis by the GATA-4 transcription factor. Life Sci 74: 1829-1838.
Suzuki YJ, Nagase H, Day RM & Das DK (2004) GATA-4 regulation of myocardial survival in the preconditioned heart. J Mol Cell Cardiol 37: 1195-1203.
Svensson EC, Huggins GS, Dardik FB, Polk CE & Leiden JM (2000) A functionally conserved N-terminal domain of the friend of GATA-2 (FOG-2) protein represses GATA4-dependent transcription. J Biol Chem 275: 20762-20769.
Svensson EC, Tufts RL, Polk CE & Leiden JM (1999) Molecular cloning of FOG-2: a modulator of transcription factor GATA-4 in cardiomyocytes. Proc Natl Acad Sci U S A 96: 956-961.
Svoboda P, Teisinger J, Novotny J, Bourova L, Drmota T, Hejnova L, Moravcova Z, Lisy V, Rudajev V, Stohr J, Vokurkova A, Svandova I & Durchankova D (2004) Biochemistry of transmembrane signaling mediated by trimeric G proteins. Physiol Res 53: S141-S152.
Swedberg K, Held P, Kjekshus J, Rasmussen K, Ryden L & Wedel H (1992) Effects of the early administration of enalapril on mortality in patients with acute myocardial infarction. Results of the Cooperative New Scandinavian Enalapril Survival Study II (CONSENSUS II). N Engl J Med 327: 678-684.
Swynghedauw B (1999) Molecular mechanisms of myocardial remodeling. Physiol Rev 79: 215-262.
Szatkowski ML, Westfall MV, Gomez CA, Wahr PA, Michele DE, DelloRusso C, Turner II, Hong KE, Albayya FP & Metzger JM (2001) In vivo acceleration of heart relaxation performance by parvalbumin gene delivery. J Clin Invest 107: 191-198.
Tabibiazar R & Rockson SG (2001) Angiogenesis and the ischaemic heart. Eur Heart J 22: 903-918.
Takeda Y, Yoneda T, Demura M, Miyamori I & Mabuchi H (2000) Cardiac aldosterone production in genetically hypertensive rats. Hypertension 36: 495-500.

123
Takeishi Y, Huang Q, Abe J, Che W, Lee JD, Kawakatsu H, Hoit BD, Berk BC & Walsh RA (2002) Activation of mitogen-activated protein kinases and p90 ribosomal S6 kinase in failing human hearts with dilated cardiomyopathy. Cardiovasc Res 53: 131-137.
Takeishi Y, Huang Q, Abe J, Glassman M, Che W, Lee JD, Kawakatsu H, Lawrence EG, Hoit BD, Berk BC & Walsh RA (2001) Src and multiple MAP kinase activation in cardiac hypertrophy and congestive heart failure under chronic pressure-overload: comparison with acute mechanical stretch. J Mol Cell Cardiol 33: 1637-1648.
Takeishi Y, Ping P, Bolli R, Kirkpatrick DL, Hoit BD & Walsh RA (2000) Transgenic overexpression of constitutively active protein kinase C epsilon causes concentric cardiac hypertrophy. Circ Res 86: 1218-1223.
Takemoto Y, Yoshiyama M, Takeuchi K, Omura T, Komatsu R, Izumi Y, Kim S & Yoshikawa J (1999) Increased JNK, AP-1 and NF-kappa B DNA binding activities in isoproterenol-induced cardiac remodeling. J Mol Cell Cardiol 31: 2017-2030.
Takemura G & Fujiwara H (2004) Role of apoptosis in remodeling after myocardial infarction. Pharmacol Ther 104: 1-16.
Tamir Y & Bengal E (2000) Phosphoinositide 3-kinase induces the transcriptional activity of MEF2 proteins during muscle differentiation. J Biol Chem 275: 34424-34432.
Tamura K, Umemura S, Nyui N, Hibi K, Ishigami T, Kihara M, Toya Y & Ishii M (1998) Activation of angiotensinogen gene in cardiac myocytes by angiotensin II and mechanical stretch. Am J Physiol 275: R1-R9.
Tamura N, Ogawa Y, Chusho H, Nakamura K, Nakao K, Suda M, Kasahara M, Hashimoto R, Katsuura G, Mukoyama M, Itoh H, Saito Y, Tanaka I, Otani H & Katsuki M (2000) Cardiac fibrosis in mice lacking brain natriuretic peptide. Proc Natl Acad Sci U S A 97: 4239-4244.
Tanaka M, Fuentes ME, Yamaguchi K, Durnin MH, Dalrymple SA, Hardy KL & Goeddel DV (1999) Embryonic lethality, liver degeneration, and impaired NF-kappa B activation in IKK-beta-deficient mice. Immunity 10: 421-429.
Tavi P, Han C & Weckstrom M (1998) Mechanisms of stretch-induced changes in [Ca2+]i in rat atrial myocytes: role of increased troponin C affinity and stretch-activated ion channels. Circ Res 83: 1165-1177.
Teerlink JR (2002) Reversal of left ventricular remodeling: role of the endothelin pathway. J Card Fail 8: S494-S499.
Teiger E, Than VD, Richard L, Wisnewsky C, Tea BS, Gaboury L, Tremblay J, Schwartz K & Hamet P (1996) Apoptosis in pressure overload-induced heart hypertrophy in the rat. J Clin Invest 97: 2891-2897.
Tenhunen O, Szokodi I & Ruskoaho H (2005) Posttranscriptional activation of BNP gene expression in response to increased left ventricular wall stress: role of calcineurin and PKC. Regul Pept 128: 187-196.
Theodosiou A & Ashworth A (2002) MAP kinase phosphatases. Genome Biol 3: REVIEWS3009. Thienelt CD, Weinberg EO, Bartunek J & Lorell BH (1997) Load-induced growth responses in
isolated adult rat hearts. Role of the AT1 receptor. Circulation 95: 2677-2683. Thorburn A, Thorburn J, Chen SY, Powers S, Shubeita HE, Feramisco JR & Chien KR (1993)
HRas-dependent pathways can activate morphological and genetic markers of cardiac muscle cell hypertrophy. J Biol Chem 268: 2244-2249.
Thuerauf DJ, Arnold ND, Zechner D, Hanford DS, DeMartin KM, McDonough PM, Prywes R & Glembotski CC (1998) p38 Mitogen-activated protein kinase mediates the transcriptional induction of the atrial natriuretic factor gene through a serum response element. A potential role for the transcription factor ATF6. J Biol Chem 273: 20636-20643. T
Thuerauf DJ & Glembotski CC (1997) Differential effects of protein kinase C, Ras, and Raf-1 kinase on the induction of the cardiac B-type natriuretic peptide gene through a critical promoter-proximal M-CAT element. J Biol Chem 272: 7464-7472.

124
Thuerauf DJ, Hanford DS & Glembotski CC (1994) Regulation of rat brain natriuretic peptide transcription. A potential role for GATA-related transcription factors in myocardial cell gene expression. J Biol Chem 269: 17772-17775
Tokola H, Hautala N, Marttila M, Magga J, Pikkarainen S, Kerkelä R, Vuolteenaho O & Ruskoaho H (2001) Mechanical load-induced alterations in B-type natriuretic peptide gene expression. Can J Physiol Pharmacol 79: 646-653.
Torre-Amione G (2005) Immune activation in chronic heart failure. Am J Cardiol 95: 3C-8C; discussion 38C-40C.
Torsoni AS, Fonseca PM, Crosara-Alberto DP & Franchini KG (2003) Early activation of p160ROCK by pressure overload in rat heart. Am J Physiol Cell Physiol 284: C1411-C1419.
Treisman R (1987) Identification and purification of a polypeptide that binds to the c-fos serum response element. EMBO J 6: 2711-2717.
Tsuruda T, Boerrigter G, Huntley BK, Noser JA, Cataliotti A, Costello-Boerrigter LC, Chen HH & Burnett JC,Jr (2002) Brain natriuretic Peptide is produced in cardiac fibroblasts and induces matrix metalloproteinases. Circ Res 91: 1127-1134.
Unger T, Chung O, Csikos T, Culman J, Gallinat S, Gohlke P, Hohle S, Meffert S, Stoll M, Stroth U & Zhu YZ (1996) Angiotensin receptors. J Hypertens 14: S95-S103.
Urbanek K, Quaini F, Tasca G, Torella D, Castaldo C, Nadal-Ginard B, Leri A, Kajstura J, Quaini E & Anversa P (2003) Intense myocyte formation from cardiac stem cells in human cardiac hypertrophy. Proc Natl Acad Sci U S A 100: 10440-10445.
Urbanek K, Torella D, Sheikh F, De Angelis A, Nurzynska D, Silvestri F, Beltrami CA, Bussani R, Beltrami AP, Quaini F, Bolli R, Leri A, Kajstura J & Anversa P (2005) Myocardial regeneration by activation of multipotent cardiac stem cells in ischemic heart failure. Proc Natl Acad Sci U S A 102: 8692-8697.
Valen G (2004) Signal transduction through nuclear factor kappa B in ischemia-reperfusion and heart failure. Basic Res Cardiol 99: 1-7.
Valen G, Yan ZQ & Hansson GK (2001) Nuclear factor kappa-B and the heart. J Am Coll Card 38: 307-314.
Vega RB, Bassel-Duby R & Olson EN (2003) Control of cardiac growth and function by calcineurin signaling. J Biol Chem 278: 36981-36984.
Vlahos CJ, McDowell SA & Clerk A (2003) Kinases as therapeutic targets for heart failure. Nat Rev Drug Discov 2: 99-113.
Volders PG, Willems IE, Cleutjens JP, Arends JW, Havenith MG & Daemen MJ (1993) Interstitial collagen is increased in the non-infarcted human myocardium after myocardial infarction. J Mol Cell Cardiol 25: 1317-1323.
Wakasaki H, Koya D, Schoen FJ, Jirousek MR, Ways DK, Hoit BD, Walsh RA & King GL (1997) Targeted overexpression of protein kinase C beta2 isoform in myocardium causes cardiomyopathy. Proc Natl Acad Sci U S A 94: 9320-9325.
Wang Y, Huang S, Sah VP, Ross J,Jr, Brown JH, Han J & Chien KR (1998) Cardiac muscle cell hypertrophy and apoptosis induced by distinct members of the p38 mitogen-activated protein kinase family. J Biol Chem 273: 2161-2168.
Wencker D, Chandra M, Nguyen K, Miao W, Garantziotis S, Factor SM, Shirani J, Armstrong RC & Kitsis RN (2003) A mechanistic role for cardiac myocyte apoptosis in heart failure. J Clin Invest 111: 1497-1504.
Whyatt DJ, deBoer E & Grosveld F (1993) The two zinc finger-like domains of GATA-1 have different DNA binding specificities. EMBO J 12: 4993-5005.
Widder J, Behr T, Fraccarollo D, Hu K, Galuppo P, Tas P, Angermann CE, Ertl G & Bauersachs J (2004) Vascular endothelial dysfunction and superoxide anion production in heart failure are p38 MAP kinase-dependent. Cardiovasc Res 63: 161-167.

125
Wilkins BJ & Molkentin JD (2004) Calcium-calcineurin signaling in the regulation of cardiac hypertrophy. Biochem Biophys Res Commun 322: 1178-1191.
Wilson EM, Diwan A, Spinale FG & Mann DL (2004) Duality of innate stress responses in cardiac injury, repair, and remodeling. J Mol Cell Cardiol 37: 801-811.
Wisdom R (1999) AP-1: one switch for many signals. Exp Cell Res 53: 180-185. Wong SC, Fukuchi M, Melnyk P, Rodger I & Giaid A (1998) Induction of cyclooxygenase-2 and
activation of nuclear factor-kappaB in myocardium of patients with congestive heart failure. Circulation 98: 100-103.
Xu L, Kappler CS & Menick DR (2005) The role of p38 in the regulation of Na+-Ca2+ exchanger expression in adult cardiomyocytes. J Mol Cell Cardiol 38: 735-743.
Xu Q & Wu Z (2000) The insulin-like growth factor-phosphatidylinositol 3-kinase-Akt signaling pathway regulates myogenin expression in normal myogenic cells but not in rhabdomyosarcoma-derived RD cells. J Biol Chem 275: 36750-36757.
Yamada K & Yoshida S (1991) Role of endogenous endothelin in renal function during altered sodium balance. J Cardiovasc Pharmacol 17: S290-S292.
Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, Yazaki Y, Goto K & Masaki T (1988) A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature 332: 411-415.
Yanazume T, Hasegawa K, Morimoto T, Kawamura T, Wada H, Matsumori A, Kawase Y, Hirai M & Kita T (2003) Cardiac p300 is involved in myocyte growth with decompensated heart failure. Mol Cell Biol 23: 3593-3606.
Yanazume T, Hasegawa K, Wada H, Morimoto T, Abe M, Kawamura T & Sasayama S (2002) Rho/ROCK pathway contributes to the activation of extracellular signal-regulated kinase/GATA-4 during myocardial cell hypertrophy. J Biol Chem 277: 8618-8625.
Yang HY & Evans T (1992) Distinct roles for the two cGATA-1 finger domains. Mol Cell Biol 12: 4562-4570.
Yau TM, Fung K, Weisel RD, Fujii T, Mickle DA & Li RK (2001) Enhanced myocardial angiogenesis by gene transfer with transplanted cells. Circulation 104: I218-I222.
Yin T, Sandhu G, Wolfgang CD, Burrier A, Webb RL, Rigel DF, Hai T & Whelan J (1997) Tissue-specific pattern of stress kinase activation in ischemic/reperfused heart and kidney. J Biol Chem 272: 19943-19950.
Ylä-Herttuala S & Alitalo K (2003) Gene transfer as a tool to induce therapeutic vascular growth. Nat Med 9: 694-701.
Yorikane R, Sakai S, Miyauchi T, Sakurai T, Sugishita Y & Goto K (1993) Increased production of endothelin-1 in the hypertrophied rat heart due to pressure overload. FEBS Lett 332: 31-34.
Young M, Head G & Funder J (1995) Determinants of cardiac fibrosis in experimental hypermineralocorticoid states. Am J Physiol 269: E657-E662.
Yuasa S, Fukuda K, Tomita Y, Fujita J, Ieda M, Tahara S, Itabashi Y, Yagi T, Kawagushi H, Hisaka Y & Ogawa S (2004) Cardiomyocytes undergo cells division following myocardial infaction is a spatially and temporally restricted event in rats. Mol Cell Biochem 259:177-181.
Yue TL, Gu JL, Wang C, Reith AD, Lee JC, Mirabile RC, Kreutz R, Wang Y, Maleeff B, Parsons AA & Ohlstein EH (2000a) Extracellular signal-regulated kinase plays an essential role in hypertrophic agonists, endothelin-1 and phenylephrine-induced cardiomyocyte hypertrophy. J Biol Chem 275: 37895-37901.
Yue TL, Wang C, Gu JL, Ma XL, Kumar S, Lee JC, Feuerstein GZ, Thomas H, Maleeff B & Ohlstein EH (2000b) Inhibition of extracellular signal-regulated kinase enhances Ischemia/Reoxygenation-induced apoptosis in cultured cardiac myocytes and exaggerates reperfusion injury in isolated perfused heart. Circ Res 86: 692-699.

126
Zechner D, Thuerauf DJ, Hanford DS, McDonough PM & Glembotski CC (1997) A role for the p38 mitogen-activated protein kinase pathway in myocardial cell growth, sarcomeric organization, and cardiac-specific gene expression. J Cell Biol 139: 115-127.
Zeisberg EM, Ma Q, Juraszek AL, Moses K, Schwartz RJ, Izumo S & Pu WT (2005) Morphogenesis of the right ventricle requires myocardial expression of Gata4. J Clin Invest 115: 1522-1531.
Zhang GX, Kimura S, Nishiyama A, Shokoji T, Rahman M, Yao L, Nagai Y, Fujisawa Y, Miyatake A & Abe Y (2005) Cardiac oxidative stress in acute and chronic isoproterenol-infused rats. Cardiovasc Res 65: 230-238.
Zhang GX, Kimura S, Nishiyama A, Shokoji T, Rahman M & Abe Y (2004) ROS during the acute phase of Ang II hypertension participates in cardiovascular MAPK activation but not vasoconstriction. Hypertension 43: 117-124.
Zhang T & Brown JH (2004) Role of Ca2+/calmodulin-dependent protein kinase II in cardiac hypertrophy and heart failure. Cardiovasc Res 63: 476-486.
Zhang T, Johnson EN, Gu Y, Morissette MR, Sah VP, Gigena MS, Belke DD, Dillmann WH, Rogers TB, Schulman H, Ross J,Jr & Brown JH (2002) The cardiac-specific nuclear delta(B) isoform of Ca2+/calmodulin-dependent protein kinase II induces hypertrophy and dilated cardiomyopathy associated with increased protein phosphatase 2A activity. J Biol Chem 277: 1261-1267.
Zhang X, Azhar G, Chai J, Sheridan P, Nagano K, Brown T, Yang J, Khrapko K, Borras AM, Lawitts J, Misra RP & Wei JY (2001) Cardiomyopathy in transgenic mice with cardiac-specific overexpression of serum response factor. Am J Physiol Heart Circ Physiol 280: H1782-H1792.
Zhou G, Bao ZQ & Dixon JE (1995) Components of a new human protein kinase signal transduction pathway. J Biol Chem 270: 12665-12669.
Zou Y, Komuro I, Yamazaki T, Aikawa R, Kudoh S, Shiojima I, Hiroi Y, Mizuno T & Yazaki Y (1996) Protein kinase C, but not tyrosine kinases or Ras, plays a critical role in angiotensin II-induced activation of Raf-1 kinase and extracellular signal-regulated protein kinases in cardiac myocytes. J Biol Chem 271: 33592-33597.

Original papers
I Hautala N, Tenhunen O, Szokodi I & Ruskoaho H (2002) Direct left ventricular wall stretch activates GATA4 binding in perfused rat heart: involvement of autocrine/paracrine pathways. Pflugers Arch 443: 362-369. Reprinted with permission of Springer-Verlag from Pflugers Arch, copyright 2002.
II Tenhunen O, Sarman B, Kerkelä R, Szokodi I, Papp L, Toth M & Ruskoaho H (2004) Mitogen-activated protein kinases p38 and ERK 1/2 mediate the wall stress-induced activation of GATA-4 binding in adult heart. J Biol Chem 279: 24852-24860. Reprinted with permission of ASBMB Journals from J Biol Chem, copyright 2004.
III Tenhunen O, Rysä J, Ilves M, Ruskoaho H & Leskinen H (2006) Identification of cell cycle regulatory and inflammatory genes as predominant targets of p38 MAPK in the heart. Circ Res, in press. Reprinted with permission of Lippincott Williams & Wilkins from Circ Res, copyright 2006.
IV Tenhunen O, Soini Y, Ilves M, Rysä J, Tuukkanen J, Serpi R, Pennanen H, Ruskoaho H & Leskinen H (2006) p38 kinase rescues failing myocardium after myocardial infarction: evidence for angiogenic and anti-apoptotic mechanisms. FASEB J, in press. Reprinted with permission of The Federation of American Societies for Experimental Biology from FASEB J, copyright 2006.
Original publications are not included in the electronic version of the dissertation.


A C T A U N I V E R S I T A T I S O U L U E N S I S
Distributed byOULU UNIVERSITY LIBRARY
P.O. Box 7500, FI-90014University of Oulu, Finland
Book orders:OULU UNIVERSITY PRESSP.O. Box 8200, FI-90014University of Oulu, Finland
S E R I E S D M E D I C A
874. Sorppanen, Sanna (2006) Kliinisen radiografiatieteen tutkimuskohde.Käsiteanalyyttinen tutkimus kliinisen radiografiatieteen tutkimuskohdettamäärittävistä käsitteistä ja käsitteiden välisistä yhteyksistä
875. Erola, Tuomo (2006) Deep brain stimulation of the subthalamic nucleus inParkinson's disease. A clinical study
876. Mäkinen, Tiina M. (2006) Human cold exposure, adaptation and performance in anorthern climate
877. Autio, Reijo (2006) MRI of herniated nucleus pulposus. Correlation with clinicalfindings, determinants of spontaneous resorption and effects of anti-inflammatorytreatments on spontaneous resorption
878. Laurila, Jouko (2006) Surgically treated acute acalculous cholecystitis in criticallyill patients
879. Pakkanen, Outi (2006) Assembly and secretion of recombinant human collagensand gelatins in the yeast Pichia pastoris, and generation and analysis of knock-outmice for collagen prolyl 4-hydroxylase type I
880. Neubauer, Antje (2006) Expression and analysis of recombinant human collagenprolyl 4-hydroxylase in E. coli and optimization of expression
881. Koivula, Marja-Kaisa (2006) Autoantibodies binding citrullinated type I and IIcollagens in rheumatoid arthritis
882. Kervinen, Marko (2006) Membranous core domain of Complex I andmitochondrial disease modeling
883. Rytkönen, Jani (2006) Effect of heat denaturation of bovine milk beta-lactoglobulinon its epithelial transport and allergenicity
884. Erkinaro, Tiina (2006) Fetal and placental haemodynamic responses tohypoxaemia, maternal hypotension and vasopressor therapy in a chronic sheepmodel
885. Lähdesmäki, Raija (2006) Sex chromosomes in human tooth root growth.Radiographic studies on 47,XYY males, 46,XY females, 47,XXY males and 45,X/46,XX females
886. Rauvala, Marita (2006) Matrix metalloproteinases -2 and -9 and tissue inhibitorsof metalloproteinases -1 and -2 in gynaecological cancers
887. Kiviniemi, Antti (2006) Measurement of cardiac vagal outflow by beat-to-beat R-Rinterval dynamics
D888etukansi.fm Page 2 Tuesday, September 12, 2006 12:45 PM

ABCDEFG
UNIVERS ITY OF OULU P .O . Box 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
EDITORIAL SECRETARY
Professor Mikko Siponen
Professor Harri Mantila
Professor Juha Kostamovaara
Professor Olli Vuolteenaho
Senior Assistant Timo Latomaa
Communications Officer Elna Stjerna
Senior Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publication Editor Kirsti Nurkkala
ISBN 951-42-8192-6 (Paperback)ISBN 951-42-8193-4 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
OULU 2006
D 888
Olli Tenhunen
MITOGEN-ACTIVATED PROTEIN KINASES AND TRANSCRIPTION FACTORS DURING INCREASED CARDIAC WORKLOAD AND REMODELLING
FACULTY OF MEDICINE, DEPARTMENT OF PHARMACOLOGY AND TOXICOLOGY, BIOCENTER OULU,UNIVERSITY OF OULU
D 888
AC
TA O
lli TenhunenD888etukansi.fm Page 1 Tuesday, September 12, 2006 12:45 PM