Embed Size (px)
DESCRIPTION
Sierra Sacramento Valley Medicine is the official journal of the Sierra Sacramento Valley Medical Society (SSVMS) and promotes the history, art, and science of medicine, the protection of public health and the well-being of patients.
Citation preview

Sierra Sacramento Valley
MEDICINE
September/October 2015
Serving the counties of El Dorado, Sacramento and Yolo


September/October 2015 1
A collection of prosthetic eyes was recently donated to our Museum of Medical History, which prompted Curator Dr. Bob LaPerriere to look into the history of fitting and fabricating these glass ocular replacements. The glass eyes in our museum are made of cryolite glass, a special soft, and easy-to-form or to blow, glass. This glass is non-toxic, is very compatible with human tissue, and was developed in Lauscha, Germany. Most prosthetic eyes now fitted in the U.S. are made of acrylic plastic and are custom-molded to accurately fit the patient’s anatomy. Dr. LaPerriere’s article begins on page 18.
3 PRESIDENT’S MESSAGE Mental Health Advocacy
Jason Bynum, MD
4 EDITOR’S MESSAGE Comfort Foods
Nathan Hitzeman, MD
5 Crisis in the Emergency Department
Aileen Wetzel, Executive Director
10 Volunteering in Sierra Leone During Ebola
Eileen Barrett, MD
12 Irma West – Memories of an Early Woman Doctor
Jack Ostrich, MD
16 BOOK REVIEW Being Mortal
18 Eyes on the Past
Bob LaPerriere, MD
Sierra Sacramento Valley
MEDICINE
Volume 66/Number 5
Official publication of the Sierra Sacramento Valley Medical Society
5380 Elvas Avenue Sacramento, CA 95819 916.452.2671916.452.2690 [email protected]
We welcome articles from our readers by email, facsimile or mail to the Editorial Committee at the address below. Authors will be able to review articles before publication. Letters may be published in a future issue; send emails to e.LetterSSV [email protected] or to the author.
All articles are copyrighted for publication in this magazine and on the Society’s website. Contact the medical society for permission to reprint.
Visit Our Medical History Museum 5380 Elvas Ave. Sacramento Open free to the public 9 am–4 pm M–F, except holidays.
SSV Medicine is online at www.ssvms.org/Publications/SSVMedicine.aspx
21 Memorable Experiences from Sutter Memorial
26 Moving Toward Universal Health Care
Glennah Trochet, MD
28 New Med School in Town
Bob LaPerriere, MD
29 On Box-Making
Caroline Giroux, MD
30 Bioelectrical Medicine
Kent Perryman, Ph.D.
34 Board Briefs
35 Welcome New Members
35 Classified Advertising

2 Sierra Sacramento Valley Medicine
Sierra Sacramento Valley
MEDICINEThe Mission of the Sierra Sacramento Valley Medical Society is to bring together physicians from all modes of practice to promote the art and science of quality medical care and to enhance the physical and mental health of our entire community.
2015 Officers & Board of DirectorsJason Bynum, MD, PresidentThomas Ormiston, MD, President-ElectJosé A. Arévalo, MD, Immediate Past President
District 1Seth Thomas, MDDistrict 2Laurie Gregg, MDVijay Khatri, MDChristian Serdahl, MDDistrict 3Ruenell Adams Jacobs, MDDistrict 4Russell Jacoby, MD
2014 CMA DelegationDistrict 1Reinhardt Hilzinger, MDDistrict 2Lydia Wytrzes, MDDistrict 3Katherine Gillogley, MDDistrict 4Russell Jacoby, MDDistrict 5Maynard Johnston, MDDistrict 6Marcia Gollober, MDAt-LargeAlicia Abels, MD José A. Arévalo, MDJason Bynum, MDAdam Dougherty, MD Alan Ertle, MD Richard Gray, MDKaren Hopp, MDRichard Jones, MDCharles McDonnell, MDJanet O’Brien, MDThomas Ormiston, MD Richard Pan, MD, Senator Margaret Parsons, MDAnthony Russell, MDKuldip Sandhu, MDJames Sehr, MD
CMA TrusteesDistrict XIBarbara Arnold, MD Douglas Brosnan, MD
CMA Imm. Past PresidentRichard Thorp, MD
AMA DelegationBarbara Arnold, MD Richard Thorp, MD
Editorial CommitteeNate Hitzeman, MD, Editor/ChairJohn Paul Aboubechara, MS IIISean Deane, MDAdam Doughtery, MDAnn Gerhardt, MDSandra Hand, MDAlbert Kahane, MDRobert LaPerriere, MD John Loofbourow, MD
Executive Director Aileen WetzelManaging Editor Nan Nichols CrussellWebmaster Melissa DarlingGraphic Design Planet Kelly
Sierra Sacramento Valley Medicine, the official journal of the Sierra Sacramento Valley Medical Society, is a forum for discussion and debate of news, official policy and diverse opinions about professional practice issues and ideas, as well as information about members’ personal interests.
Advertising rates and information sent upon request. Acceptance of advertising in Sierra Sacramento Valley Medicine in no way constitutes approval or endorsement by the Sierra Sacramento Valley Medical Society of products or services advertised. Sierra Sacramento Valley Medicine and the Sierra Sacramento Valley Medical Society reserve the right to reject any advertising.
Opinions expressed by authors are their own, and not necessarily those of Sierra Sacramento Valley Medicine or the Sierra Sacramento Valley Medical Society. Sierra Sacramento Valley Medicine reserves the right to edit all contributions for clarity and length, as well as to reject any material submitted. Not responsible for unsolicited manuscripts. ©2015 Sierra Sacramento Valley Medical Society
SIERRA SACRAMENTO VALLEy MEDICINE (ISSN 0886 2826) is published bi-monthly by the Sierra Sacramento Valley Medical Society, 5380 Elvas Ave., Sacramento, CA 95819. Subscriptions are $26.00 per year. Periodicals postage paid at Sacramento, CA and additional mailing offices. Correspondence should be addressed to Sierra Sacramento Valley Medicine, 5380 Elvas Ave., Sacramento, CA 95819-2396. Telephone (916) 452-2671. Postmaster: Send address changes to Sierra Sacramento Valley Medicine, 5380 Elvas Ave., Sacramento, CA 95819-2396.
District 1Kevin Elliott, MDDistrict 2Don Wreden, MDDistrict 3Ruenell Adams Jacobs, MDDistrict 4Courtney LaCaze-Adams, MDDistrict 5Robert Madrigal, MDDistrict 6Rajan Merchant, MDAt-LargeNatasha Bir, MDHelen Biren, MDSean Deane, MDKevin Jones, DOThomas Kaniff, MDVijay Khatri, MDSandra Mendez, MDArmine Sarchisian, MDVacantVacantVacantVacantVacantVacant VacantVacant
George Meyer, MD John Ostrich, MDGerald Rogan, MDGlennah Trochet, MDLee Welter, MDGilbert Wright, MD
District 5Steven Kelly-Reif, MDRajiv Misquitta, MDSadha Tivakaran, MDJohn Wiesenfarth, MDEric Williams, MDDistrict 6Kieu-Loan Luc, DO

September/October 2015 3
Mental Health Advocacy
IT HAS BEEN A VERY EXCITING and busy past couple of months at the medical society, and this has played out to be the year of mental health advocacy. While this has been purely coincidental with my presidency, the mental health crisis has truly come to a head, predominantly due to the massive influx of patients into our local emergency rooms. Physicians are encouraged to visit the SSVMS website, www.ssvms.org, to download a recently-published white paper on the subject. Several SSVMS members have worked very hard on this, and we are truly proud of their efforts.
I have been involved for quite some time with the Lanterman Petris Short Act (LPS) Reform Task Force. As a child psychiatrist, I have shared with the task force my concerns about involuntary holds of minors. My colleagues in other parts of the state tell me that the vast majority of adolescent patients brought to inpatient psychiatric facilities are brought in voluntarily by their parents or guardians.
In our region, however, we have a very different process. At the inpatient psychiatric hospital where I work, 100 percent of the adolescents who are admitted arrive on involuntary holds. Here’s the problem: Frequently, a teen will tell a teacher or school counselor about emotional struggles that are leading to concerns for suicide. Law enforce-ment is then called, the minor is placed on a 5150, and taken to the emergency room.
Ultimately, they come to me, or to a facility like mine, and I am frequently the first phone call the parents or legal guardians receive. Not only is this a concern for me professionally and ethically, but I am also the parent of two boys. I would be quite upset if I were unable to find where my child was taken, if he were ever placed on an involuntary hold.
As a child psychiatrist, the best part of my job is working within the framework of a family in which the patient is a minor. Informed consent, decision making about safety, and alternatives to hospitalization, are all part of the process in working with families. Doesn’t a legal guardian have the right to provide an alternative to hospitalization? I have sent hundreds of kids home when the family is able to provide me with a rational safety plan, is committed to outpatient treatment, and where there is not a concern for neglect or abuse. This is a tough debate. On one hand, is parental consent the best decision for the child? While on the other, is the presumed 100 percent failsafe protection a hospitalization can provide best for the minor?
I base much of my family-oriented approach on two points. First, a legal hearing should be in place if my opinion is different from the legal guardians who are presumed to have capacity. In other states, this is how it is handled. If I differ strongly from the decision of parents, an emergent Child Protective Services worker would be called and a midnight order obtained from the on-call civil judge.
Second, I believe the assumption that my ability to keep their child safer in the hospital than at home with 24/7 monitoring is faulty. Psychiatric hospitals are more acute in their pathology than ever before, and a reasonable alternative should be considered.
In addition to the white paper, I have prepared a resolution for the 2015 CMA House of Delegates calling on our professional organization to increase lobbying efforts to modernize our procedures for involuntary holds. I invite interested readers to contact me with your thoughts on this important issue.
By Jason Bynum, MD
PrESIDENT’S MESSAGE
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

4 Sierra Sacramento Valley Medicine
EDITOr’S MESSAGE
Comfort Foods
IT’S DANGEROUS TO WRITE “hangry” - hungry and angry, but here goes. It’s a Friday afternoon, and I’m in one of those rare hunger spirals where none of the usual foods sounds good. But with an exciting platter of topics in this issue, I’ve secured a napkin around my neck and am rubbing my utensils together. Let’s dive in!
For the appetizer, let’s enjoy Dr. Bob LaPerriere’s history lesson on fake and prosthetic eyes. For a family of ocularists to have produced this lasting collection of teaching tools is remarkable, and I’m glad UCSF has recently resurrected them. I suspect a few of the ones on the cover were used in the banquet scene in Indiana Jones and the Temple of Doom.
Several cultures enjoy eating eyeballs. Boiled sheep’s head with the eyeballs in place (but, of course, without the brains!) is a delicacy in Iceland and Norway. A raw, and most assuredly chewy, eye ball is served in some sushi restaurants in Japan. Of course, no traditional Asian soups are complete without fish heads, as my Indonesian-born wife tells me. We have a bag of deep-fried, salty-sweet little anchovies at home that we sprinkle on steamed rice. The kids think the little eyes are cute!
Some of you may enjoy grocery shopping for your food. I like my local Safeway because they always play obscure 80s songs like “Africa” by Toto. The periphery is supposed to be healthiest, and I admit to sampling and then repackaging grapes to remove the bad ones and pay less.
During my late night runs to Safeway or any-time-of-day treks to Walmart for cheap produce, I encounter some of the mentally disturbed folks addressed in Aileen Wetzel’s condensed version of the recent SSVMS white paper on the mental health crisis in our emergency departments. These are not just those people seemingly talking to the themselves
on their cell phone ear pieces (which makes us all look psychotic), but the ones directing traffic, cussing, with that psychotic stare, self medicating with alcohol or drugs or huffing Freon, or quietly drowning in their depression. Who knew “need for a spit net” would become a check off box in our EDs! We need to do something about this epidemic. This paper is a momentous step in the process.
Many of us would consider a colleague “out of their gourd” to take the health risk to volunteer in Ebola-stricken countries, but guest writer Eileen Barrett, MD, inspires us with her recent volunteerism there. Dr. Glennah Trochet writes about expanding care for the undocumented. If everyone deserves nutritious food, doesn’t everyone deserve basic health care? There is enough to go around. Let’s have more chairs at our health care table.
Let’s loosen the belt a notch as you sip your overpriced iced cappuccino from Starbucks, and take a moment to reminisce about the closing of Sutter Memorial Hospital. I want to go back in time and have a Sutter Memorial patient meal in the 1930s. I bet it was gourmet and served on shiny metal platters. What happened to hospital food between then and now? Who is responsible for this debacle? I hold you, cardiologists, partly responsible with your low-salt, low-flavor propaganda. Bring back the good hospital food!
Lastly, read about inspiring SSVMS member Dr. Irma West. We all need to find out what she eats so we can live such a long and productive life. Three cheers to you, Dr. West! Ok, now I’m getting some lunch, and trying to figure out how to connect Kent Perryman’s piece on Deep Brain Stimulation to food. If not successful, I implore you, Dear Reader, to do so in your Letters to the Editor. Thanks for dining with us!
By Nathan Hitzeman, MD
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

September/October 2015 5
Crisis in the Emergency Departmentremoving Barriers to Timely and Appropriate Mental Health Treatment
THE SYSTEM OF MENTAL health care is fundamentally broken in Sacramento County. Every month over 1,600 children and adults experiencing a mental health crisis end up in one of the Sacramento region’s hospital emergency departments (ED) – a number that continues to rise.
These patients are frequently “boarded” in the ED, oftentimes for days, until inpatient psychiatric beds become available and the transfer process is completed. This influx of patients has strained the region’s EDs, resulting in extended wait times for patients experiencing medical and/or psychiatric emergencies. This process results in the delivery of suboptimal quality of care for patients, ED overcrowding, as well as increased lengths of stay and higher risks of adverse outcomes for all ED patients.
Bearing witness to these worsening trends, the Sierra Sacramento Valley Medical Society (SSVMS) has developed a white paper, Crisis in the Emergency Department: Removing Barriers to Timely and Appropriate Mental Health Treatment, with the goal of assessing the historical events leading up to this mental health care delivery crisis. SSVMS proposes three elements of a broader collaborative strategy among regional stakeholders with the goal of increasing care coordination for individuals experiencing a mental health crisis. The SSVMS Board of Directors adopted the recommendations set forth in the white paper in July 2015.
Since 1960, SSVMS has convened an
Emergency Care Committee (ECC) that includes medical directors of the EDs from all 12 hospitals in the Sacramento region. The ECC meets bimonthly and studies issues related to emergency care services and facilities, trauma, patient transport and triage, disaster preparedness and on-call issues within the region. In recent years, members of the ECC have reported a significant increase in the number of patients presenting to the region’s EDs with mental health issues.
Sacramento County has seen increased utilization of the ED and inpatient services for psychiatric care as evidenced by data gathered from the California Office of Statewide Health Planning and Development (See Exhibit 1).
The reasons for ED overcrowding in Sacramento by individuals experiencing a mental health crisis are multifactorial. A significant driver of higher ED utilization was the closure of half of the inpatient psychiatric beds at the Sacramento County Mental Health Treatment Center (SCMHTC), and the county’s only Crisis Stabilization Unit (CSU) in 2009.
At that time, SCMHTC was averaging over 100 hospitalized patients a day, and the CSU was experiencing over 6,800 adult crisis visits a year. The county’s CSU served as a 23-hour observation unit to determine whether patients needed hospitalization and intensive care. Due to the loss of this intermediate facility, the county had less capacity to prevent unnecessary admissions.
As a result of these closures, patients would
By Aileen Wetzel, Executive Director
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

6 Sierra Sacramento Valley Medicine
board longer in the EDs while waiting for beds that were in high demand, leading to the delay of needed specialized psychiatric care. Data collected by the California Office of Statewide Health Planning and Development highlight the effect of these closures, showing a doubling of the number of ED encounters discharged to inpatient psychiatric care facilities between 2009 and 2013.
The impact of these events on the health care delivery system in Sacramento is staggering. It is estimated that more than 1,600 visits per month to hospital EDs are by individuals seeking mental health treatment. A 2012 study reported that the average wait time for adult patients with a primary psychiatric diagnosis in the ED, from the decision to admit until placement into an inpatient psychiatric bed, was over 10 hours. In
2013, the average length of stay, from admission to discharge, for individuals seeking mental health evaluations in the EDs was 19.5 hours.
There are increased costs associated with ED boarding, including costs for law enforcement, for the extra time spent in the EDs waiting on patients placed on 5150 holds to be assessed; increased nursing and security staffing; and costs associated with unnecessary diagnostic and laboratory tests required by inpatient psychiatric treatment programs prior to accepting a patient from the ED for admission and transfer. The average cost to board a psychiatric patient has been estimated at $2,264. The ED is just not conducive to the healing of patients with mental health needs.
In October 2014, a regional Mental Health Improvement Coalition was convened by Valley

September/October 2015 7
There is a
lack of effec-
tive coordi-
nation and
commu-
nication
between
health care
providers
of mental
health
patients...
Vision, a local not-for-profit company. The coalition includes leaders from each of the region’s health systems, SSVMS, the Hospital Council of Northern and Central California, Sacramento Metro Fire, the Sierra Health Foundation and other stakeholders. Since late 2014, the coalition has worked collaboratively with Sacramento County leadership to support a framework for rebalancing the continuum of behavioral health services.
Areas of agreement include the step-wise re-opening of the crisis stabilization unit (CSU), the opening of an urgent care center to deliver behavioral health services, implementing medical clearance protocol, transparency and cooperation on the application of SB 82 funds, and an open discussion of geographically-dispersed crisis stabilization services, including placement of psychiatric health facilities or PHFs, crisis residential beds, urgent care and other services.
With the coalition’s support, the Sacramento County Board of Supervisors at its June 16, 2015, budget hearing, unanimously approved spending $13.7 million for three 15-bed crisis residential facilities, 20 subacute beds, re-opening and expanding the county CSU, and pharmaceutical supplies. The total includes $5.7 million in SB 82 funds from the state. This is a great step forward.
The coalition stakeholders continue to work with Sacramento County to rebalance the mental health system toward greater access to appropriate crisis stabilization services, and to reduce the use of hospital EDs for psychiatric emergencies. The proposed solutions set forth in Crisis in the Emergency Department are not intended to replace or usurp the work and recommendations of the coalition. Rather, the solutions are offered to complement the county’s strategy and to ensure that patients have access to quality medical care in the most appropriate setting.
SSVMS proposes three overarching recommendations to improve the quality of care for patients experiencing mental health crises, aimed at providing better access to the right care at the right time.
Recommendation 1: Implement an electronic Health Information Exchange (HIE) in the Sacramento region to help coordinate care of patients seeking emergency psychiatric services.
There is a lack of effective coordination and communication between health care providers of mental health patients in the Sacramento region. The proposed benefits of HIE technology include more efficient hospital workflows with readily-available patient health data, increased cost-effectiveness, overall improved quality of health care delivery, patient safety, and better informed clinical decision making.
SSVMS’ white paper includes a case study, as well as a discussion of HIE best practices. We recommend that Sacramento region hospitals, health systems, and ancillary psychiatric care providers implement a regional HIE network that actively encourages case management of patients at high risk of presenting to the ED with a mental health crisis. Furthermore, interoperability of patient data exchange should include outpatient providers, hospitals, skilled nursing facilities, and residential care facilities, among others. Incorporation of HIE throughout a broad spectrum of care facilities will strengthen the health safety net of these vulnerable populations.
Recommendation 2: Standardize the medical clearance process across all EDs and inpatient psychiatric treatment programs to facilitate the timely transfer of patients to appropriate treatment centers.
To facilitate medical clearance, SSVMS brought together specialists in the fields of emergency medicine and psychiatry to develop a standardized medical clearance form, which includes a series of questions under the acronym SMART. Adoption of the SMART Medical Clearance Form by each of the Sacramento region’s EDs, as well as by all inpatient psychiatric facilities, would vastly expedite the transfer process of mental health patients to an appropriate inpatient treatment program, reduce costly and unnecessary

8 Sierra Sacramento Valley Medicine
diagnostic tests, and ensure that patients receive timely treatment.
The success of a standardized medical clearance protocol is dependent on regional adoption. Standardization of the medical clearance process helps promote patient safety by ensuring that all ED physicians in the region are performing the same evaluation that is thoughtful, patient specific and evidence-based.
As discussed in the white paper, the region’s health systems and inpatient psychiatric treatment facilities are evaluating the SMART form. We anticipate that the process will be implemented on a region-wide basis before the end of 2015.
Recommendation 3: Establish dedicated psychiatric emergency services (PES) to ensure that patients experiencing a mental health crisis receive the right care at the right time.
Many proposed solutions to ED overcrowding have focused solely on increasing available inpatient psychiatric beds, rather than considering alternative designs that provide access to care and may reduce the need for hospitalization. Best practices and evidence-based programs may provide an option to reducing the cost of services and lessening the need for costly inpatient hospitalizations. An example of this type of a system is a dedicated Psychiatric Emergency Service (PES).
PES is a stand-alone ED specifically for patients experiencing a mental health crisis. As a dedicated psychiatric ED, a PES accepts patients who are either transferred from a regular ED, taken there directly by ambulance or law enforcement, or who walk in.
Regular EDs are not conducive to healing for mental health patients. Additionally, the ED is not secure, presents special risks for suicidal patients, and increases the risk for elopements. The PES, on the other hand, provides a more comfortable, calm environment for patients as they are evaluated. In addition to crisis stabilization, PES would provide case management programs, medication evaluation and management, and referral to community services.
Rather than immediate admission to an inpatient psychiatric facility, patients are under treatment for up to 24 hours in a PES, and only then is a decision made for discharge or transfer to an appropriate setting. This extended period provides enough time for the unit’s prompt interventions to effect patient improvement and healing, which can result in far less need for hospitalizations in the majority of individuals.
SSVMS’ white paper discusses the benefits of a regional PES, including patient access to crisis intervention services, reduced inpatient hospitalizations and reduced ED overcrowding.
Visit www.ssvms.org to download a copy of Crisis in the Emergency Department.
916-808-1591TripleR.org
Locations in Midtown, North Sacramentoand Greenhaven
Licensed by theState of California,Dept. of Social Services
Heart and Soul in Dementia CareTriple-R Adult Day Program
Providing your patients a safe and enriching place to spend the day,
while giving family caregivers respite.
OLDER ADULT SERVICES
AS A PHYSICIAN, you probably know bett er than anyone else how quickly a disability can strike and not only delay your dreams, but also leave you unable to provide for your family. Whether it is a heart att ack, stroke, car accident or fall off a ladder, any of these things can aff ect your ability to perform your medical specialty.
That’s why the SSVMS/CMA sponsors a Group Long-Term Disability program underwritt en by New York Life Insurance Company:
• Benefi ts not tied to a practice, giving you more fl exibility with potential career changes
• Benefi t payments that are 100% TAX-FREE — when you pay premiums yourself
• High monthly benefi ts up to $10,000
• Protection in your medical specialty for the fi rst 10 years of disability
With this critical protection, you’ll have one less thing to worry about until
your return.
69960 Sierra Sacramento (9/15)Full Size: 8.5" x 11" Bleed: 8.75" x 11.25" Live: 7.5" x 10"Folds to: NA Perf: NAColors: BW Stock: NA Postage: NA Misc: NAM
ERCER
SPONSORED BY:
69960, 70834 (1/15) Copyright 2015 Mercer LLC. All rights reserved.
Mercer Health & Benefits Insurance Services LLC • CA Ins. Lic. #0G39709777 South Figueroa Street, Los Angeles, CA 90017 • 800-842-3761
[email protected] • www.CountyCMAMemberInsurance.com
UNDERWRITTEN BY:
New York Life Insurance CompanyNew York, NY 10010 on Policy Form GMR
LEARN MORE ABOUT THIS VALUABLE PLAN TODAY!——————————————————
Call Mercer for free information, including features, costs, eligibility, renewability, limitations and exclusions at:
800.842.3761——————————————————
OR SCAN TO LEARN MORE!
THE PBEGIN
We work to protect you.
YOU WORK TO PROTECT YOUR PATIENTS.
69960 SSVMS LTD Ad 9-15.indd 1 8/3/15 11:14 AM

September/October 2015 9
AS A PHYSICIAN, you probably know bett er than anyone else how quickly a disability can strike and not only delay your dreams, but also leave you unable to provide for your family. Whether it is a heart att ack, stroke, car accident or fall off a ladder, any of these things can aff ect your ability to perform your medical specialty.
That’s why the SSVMS/CMA sponsors a Group Long-Term Disability program underwritt en by New York Life Insurance Company:
• Benefi ts not tied to a practice, giving you more fl exibility with potential career changes
• Benefi t payments that are 100% TAX-FREE — when you pay premiums yourself
• High monthly benefi ts up to $10,000
• Protection in your medical specialty for the fi rst 10 years of disability
With this critical protection, you’ll have one less thing to worry about until
your return.
69960 Sierra Sacramento (9/15)Full Size: 8.5" x 11" Bleed: 8.75" x 11.25" Live: 7.5" x 10"Folds to: NA Perf: NAColors: BW Stock: NA Postage: NA Misc: NAM
ERCER
SPONSORED BY:
69960, 70834 (1/15) Copyright 2015 Mercer LLC. All rights reserved.
Mercer Health & Benefits Insurance Services LLC • CA Ins. Lic. #0G39709777 South Figueroa Street, Los Angeles, CA 90017 • 800-842-3761
[email protected] • www.CountyCMAMemberInsurance.com
UNDERWRITTEN BY:
New York Life Insurance CompanyNew York, NY 10010 on Policy Form GMR
LEARN MORE ABOUT THIS VALUABLE PLAN TODAY!——————————————————
Call Mercer for free information, including features, costs, eligibility, renewability, limitations and exclusions at:
800.842.3761——————————————————
OR SCAN TO LEARN MORE!
THE PBEGIN
We work to protect you.
YOU WORK TO PROTECT YOUR PATIENTS.
69960 SSVMS LTD Ad 9-15.indd 1 8/3/15 11:14 AM

10 Sierra Sacramento Valley Medicine
LIKE MANY OTHERS, I applied as a volunteer physician in West Africa when news broke of the dire health care worker shortages in the coun-tries affected by Ebola. As a general internist, I’ve always taken care of complicated patients, and as a hospitalist, my patients have often been critically ill. Having worked in remote and underserved areas, both domestically and abroad, I thought I could offer skills that could be of use. And, unlike many other physicians, I was at a point in my career and in my family life where I could take six weeks to do humanitarian relief work.
My application was accepted and, within a month, I was deployed to Sierra Leone. Before leaving, colleagues and friends asked many questions about what the work would be like, and many asked why I volunteered. The first question was both easy and impossible to answer because I applied to work as a doctor in an Ebola Treatment Unit, but didn’t know in which country I’d be working, under what conditions, and what were basic logistics of medical care. The second question was difficult to answer because my thoughts and emotions were intertwined − because the world has forgotten them; because I was trained to do this; because I took an oath when I became a doctor; because a lot of people who want to help can’t, but I can; because there is a moral imperative to relieve suffering; because I believe in the effectiveness of personal protective equipment (PPE) and am not afraid. Each of these replies was true, but they seemed incomplete, and I left unable to provide a clear answer.
Once arriving in Sierra Leone, training was comprehensive and well-organized. All
volunteer health care workers receive intensive and extensive standardized training, including on the epidemiology of Ebola, the medical care of patients, and the safe use of PPE. After a week of training, health care workers were sent to the field.
It is difficult to describe work in an Ebola-affected country to people who have never traveled in a devastatingly poor area or have never practiced medicine in an exceedingly underserved setting, because they have so little context for the daily challenges. For example, despite Sierra Leoneans’ being generally friendly and warm, this highly contagious and morbid disease resulted in people being wary of casual contact (including handshakes) and fearful of hospitals, churches, and schools. And although much has been written about how physically demanding it is to wear full PPE in un-air-conditioned and stifling Treatment Units, it’s not often said that the health care available is not medically complex, but is exceedingly difficult to provide.
Critical shortages of basic medications and supplies, such as IV tubing, electrolytes, anti-diarrheals, antibiotics, and anti-emetics, complicate the care of suffering and dying patients. Open burning of trash, including Ebola-infected medical waste, hospitals powered by local generators and without running water when the generator is off, and maternal deaths were the norm. But despite these conditions and pervasive grief, the heroic commitment and dedication of so many Sierra Leonean nationals and of fellow international volunteers offers the immeasurable balm of inspiration, solace, and hope.
Volunteering in Sierra Leone During Ebola
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].
By Eileen Barrett, MD

September/October 2015 11
The Ebola crisis has taught us many lessons: health crises cross borders; poverty begets grave inequalities; all countries need a robust public health infrastructure; and scrupulous infection control saves lives. One lesson not often verbalized is that physicians who offer their expertise and compassion where there is need are awarded the invaluable and life-changing experience of being a part of something bigger than themselves. This provides a profound and nearly indescribable sense of meaning that all of us can experience when we serve in any way. I can now say I went to Sierra Leone because to be a physician is to have the ability to relieve suffering. And I would do it again for the patients and also for myself, that I would again be so moved by the compassion and heroism of my colleagues.
NOTE: Dr. Eileen Barrett is a friend of Dr. George Meyer, who serves on our Editorial Committee.
Dr. Barrett’s friend and colleague, Allendre Lindor, above, is shown in full personal protec-tive equipment in Sierra Leone. At left is the Ebola Treatment Unit where Dr. Barrett volunteered.

12 Sierra Sacramento Valley Medicine
Irma West – Memories of an Early Woman Doctor
IRMA WEST, MD, RECENTLY wrote down her “Memories” to share. They take the reader from her childhood in Canada to college in Oregon, then to medical school in Philadelphia and finally to a long and successful career as a public health doctor in California. In retirement, she became a very active member of SSVMS and helped to improve our medical museum. This brief article is based on her “Memories,” as well as a personal interview in early July.
There was no clock in the upstairs bedroom in the little house where Irma Marie Calvert was born, so she is not sure of her exact time of birth, but knows it was around midnight on December 31, 1917. She suspects, however, that her father told the town clerk in Hespeler, Ontario, that she was definitely born prior to the stroke of midnight, so she qualified as a tax deduction for that entire year.
Hespeler has since ceased to exist as an independent town. It merged with neighboring Galt to form the city of Cambridge, Ontario, about 40 miles west of Toronto. The name Hespeler lives on as a line of hockey equipment, and Galt, California, was so named by a Canadian immigrant, farmer John McFarland, who came to California from Galt, Ontario.
Irma’s family also emigrated to the USA when she was 12 years old. Even then, she says, she wanted to be a physician.
“[A medical career] was a dream on the back burner. The family moved to Bremerton, Washington, and I graduated in 1940 from Willamette University in Salem, Oregon, where I majored in chemistry and took pre-med courses, just in case.”
After college, she passed a science-based
Federal Civil Service exam and was given a job at the Moffett Field research facility as a “computer.” The facility was run by the National Advisory Committee for Aeronautics (NACA) that had been founded in 1915, and in 1958 it morphed into NASA.
At Moffett, Irma and lots of other scientifically-inclined young women were tasked to process an immense amount of data derived from aeronautical wind tunnel tests. She earned $1,800 a year and reports that she was able to live comfortably on that salary.
She sought acceptance to medical school and was eligible to enter the University of Oregon School of Medicine, but was told that they were under orders to admit only men, due to the demands of the military which did not allow any female physicians in field hospitals. Female nurses were common in those settings, but not female doctors. So she went to Philadelphia to begin medical studies at Woman’s Medical College. Because of Federal anti-discrimination rulings in the 1970s, Woman’s Medical College merged with Hahnemann Medical College and both schools are now part of Drexel University College of Medicine.
Upon entering her clinical years of medical school, Irma confronted two immediate prob-lems, the first being a positive TB skin test, and also a positive throat swab for beta hemolytic strep. No student was allowed to do any clinical work until she had no evidence of infectious disease. Irma recalled having had scrofula (mycobacterial cervical adenitis) as a child, but she had no signs of strep pharyngitis. A thorough exam revealed no findings of TB,
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].
By Jack Ostrich, MD

September/October 2015 13
and she was given a supply of penicillin, then very scarce on the home front, and injected herself several times a day for three weeks. Her follow-up culture was negative, but she recalls that her post-antibiotic colitis took quite a while to resolve.
She and a friend earned some money working as attendants at Norristown State Hospital (originally called the “State Lunatic Hospital at Norristown”). The place housed about 3,000 mentally ill patients, and skilled medical care was minimal.
“Twice a week, a group of patients was lined up for shock therapy...and only one improved. She had classic catatonic schizophrenia and I had been feeding her by tube. After shock treatment, she looked at me and spoke for the first time in years asking where she was and why.”
And in the hospital basement there were...”contraptions that looked like iron lungs, but were ovens in which...patients with CNS syphilis were secured and sedated for heat treatments. Their rectal temperatures were held at 106 degrees for four hours. The treatment was based on observations that syphilitic patients seemed to improve after malarial fevers...” (Note: This observation resulted in the 1927 Nobel Prize for Medicine being awarded to Julius Wagner-Jauregg, an Austrian physician who applied “pyrotherapy” to a wide variety of illnesses.)
After medical school, Irma returned to California to serve an internship at St. Joseph’s Hospital in San Francisco where she was the only female intern. She was housed in a private hospital room with her own shower and was paid $100 a month. She married the chief resident at St. Joseph’s, and the couple moved to Santa Rosa where Irma worked at Sonoma State Hospital as a staff physician. She gave birth to a son, her only child, and she was divorced soon thereafter.
She then moved to the Bay Area and got a job with the State Department of Public Health, then completed her Master’s degree in Public Health at UC Berkeley. She recalls her interview for her job with the State of California:
“When I was interviewed for my position, I was asked if I intended to marry again and have more children! The attitude (then) toward woman doctors was that there must be something wrong with them...(they were) unattractive, or worse, and unable to find men who would marry them. I set out to be well groomed and stylishly-dressed. As a result, I received many comments about not looking like a typical woman doctor.”
Not long after she began her work, she and several colleagues contracted brucellosis. All recovered without incident. Then came news of multiple cases of pulmonary tuberculosis among workers at a diatomaceous earth quarry in Santa Barbara County. Biopsies revealed not just routine TB, but rather silicotuberculosis. The two mining companies denied that silica dust was contributing to the illnesses and refused to allow Irma and her
Dr. Irma West, above, receives a Certificate of Appreciation from the California Highway Patrol. Below is Dr. West at her gradua-tion from medical school.

14 Sierra Sacramento Valley Medicine
staff to inspect the properties. An article entitled “Death By Dust”
appeared in a national magazine, accompanied by surreptitiously-obtained aerial photographs of the quarries and factories. The problem was referred to the USPHS, but little was done except to urge the workers to wear protective clothing and filtration masks.
And if brucellosis and silicosis were not enough, poisonings of farm workers and aerial crop dusting pilots, due to organophosphate pesticides, were becoming epidemic in California. So Irma and her crew went off to educate the doctors in agricultural areas on how to recognize and handle organophosphate toxicity. She writes :
“It was a hard sell to (convince) physicians...to give toxic doses of atropine to save a life.”
The information that the public health personnel gathered prompted the development
of a new generation of crop duster aircraft. The open cockpits were replaced by positive pressurized pilot compartments, and the chemicals were stored under and behind the pilot, not in the front of the plane. The Grumman “Ag Cat” was the first such plane taking to the air in 1957, and is still in use today. Organophosphates continue to be used around the world, but much more restrictively than in the twentieth century.
In 1968, Irma was the lead author for a paper published in JAMA (July 29, 1968; vol 204, pp 266-271) which studied 1,024 single vehicle accidents in California. Of that number, there were 871 driver deaths, and the assumption of law enforcement and medical authorities, prior to Irma’s study, was that the majority of those deaths were due to “natural” causes or perhaps carbon monoxide leaking into the passenger compartment. Toxicology studies, however, revealed no carbon monoxide or illicit drug involvement. Rather, it was found that of the 871 dead drivers, 648 had an average blood alcohol level of 0.19mg/100 ml. The paper sparked a long-needed national discussion about drunk driving.
Now, based here in Sacramento, she received a call from a local doctor who said he had two patients who were seriously ill with lead poisoning, and both of them worked at the same car battery recycling operation in West Sacramento. One even had a gingival “lead line,” something Irma had never seen before.
She visited the plant, not far from where Raley Field now stands, on Riske Lane (“Well named,” comments Irma). The air was heavy with fumes as the poorly-ventilated furnaces melted the batteries to recover the lead. The owner was straightaway served with papers to cease all operations, and arrangements were made to test all employees for lead toxicity. The papers were cosigned by Irma and an engineer at the local State Industrial Safety Office (now Cal/OSHA). Their individual office addresses were included as well.
Not long after he had been served, the owner of the plant came armed to the engineer’s office and held a gun to the man’s head, threatening
Dr. Irma West in retirement, today.

September/October 2015 15
to kill him. He was disarmed without anyone being harmed, and in the meantime, Irma was warned that she might also be in danger, so she and her staff evacuated their offices until it could be proven that there was no one else on the prowl. Subsequently, the gun-toting owner of the recycling plant was found to have a very high blood lead level, and he successfully pleaded “temporary insanity” due to plumbism.
Dr. West retired in 1980. She then became very involved with the Sacramento Historic City Cemetery and was a member of the Old City Cemetery Committee at its inception and for many decades after. She has assisted in cataloging the burial sites of the tens of thousands of souls who rest there. When she and other fellow volunteers began their work, the 49 acres were overgrown with weeds and nondescript brush and shrubbery; and many of the gravestones were in poor repair, toppled or vandalized. She has been the only person to intensively research the lives and practices of
over 50 early Sacramento physicians who lie at rest there. She also conducted the “Medical Bag” tours at the cemetery for many years. Of the 17 Sacramento physicians who died in the great cholera epidemic of 1850, only one grave site is certain. The 800-1,000 citizens who also perished were buried in sites unknown to us today.
And, in addition to her work at the cemetery, Irma became very (very) active at the Medical Society, greatly helping to improve the medical museum, as well as serving as a docent and museum tour guide. She has written at least 22 articles, mostly regarding local medical history, for this magazine. Her pamphlet entitled, “Cholera and Other Plagues of the Gold Rush,” was published by the Sacramento Historical Society. It is worthwhile, pleasant and easy reading for anyone with interest in that period of our state’s history.
Certified Public Accountants | Business Consultants
Every patient is different. So is every medical group. That’s why we provide you with customized solutions designed to help solve your unique business, financial, and operational challenges.
Find out what providers across the nation already know: that the right assurance, tax, and consulting firm is one that understands your industry. And offers candid insight to help you meet the needs of your patients. Put our expertise to work for you.
WWW.MOSSADAMS.COM/MEDGROUPS
Your patients get personal care. Shouldn’t your business?

16 Sierra Sacramento Valley Medicine
Being MortalMedicine and What Matters in the End, by Atul Gawande, MD. Publisher Metropolitan Books, ISBN-13: 978-0805095159
YOU WILL DIE. I WILL DIE. We all will die.Given current trends in this country, you
and I may die a prolonged death in the hospital or nursing home, on dialysis, or after courses of surgeries, chemotherapy, and radiation that may harm as well as help. As physicians, we encounter frailty and mortality on a regular basis. So why do we need a book about it?
Yes, a quarter of Medicare dollars are spent on the last year of life, and mostly on the last weeks of life. Yes, we do not educate medical students adequately on the limitations of medicine, and how to guide patients through their inevitable demise. Yes, we do too many costly inventions with somewhat dubious long term benefits.
So what does East Coast surgeon Dr. Atul Gawande tell us that is new in this book?
I must confess that I am a big Atul Gawande fan, having read his New Yorker essays over the past decade speaking to geographic disparities in health care, waste in medicine, the power of checklists, achieving one’s personal best, targeting the “hot spotter” high utilizers in the revolving EDs, and more recently, the overkill we do in pathologizing what could be indolent cancers and processes.
Being Mortal seems a culmination of Gawande’s journey as writer, public health researcher, and physician; accordingly, this book does not disappoint. As a surgeon, Gawande does not talk in the abstract. He’s analytical and concrete. He even includes two simple hand-drawn graphs early on in the text to contrast the precipitous death of our ancestors with the slow sinusoidal death of modern day. He likes to dissect to the root causes of problems.
He also has an appreciation for the history of medicine and the art of healing. He brings a cultural sensitivity as a second generation Indian American, and he radiates the intellect of a Harvard professor.
Most importantly, he teaches by examples. Many examples. Through Being Mortal, we hear about his friends, patients, his daughter’s piano teacher, and ultimately his father struggling with their declining health and inevitable death. He weaves these examples into the framework of a history lesson on how society has dealt with the aged over the past century, from almshouses in the early 1900s, to the rise of hospitals and skilled nursing facilities in the mid-1900s post-war economic boom, to a counterculture of assisted-living experiments in the 1980s that sought to return some measure of independence to their clients – some having stayed true to their original vision, and many more now commercialized, diluted, or perverted.
Gawande also shows us that surgeons and humility need not be mutually exclusive. He examines his own naivety about end-of-life discussions. He recounts his missteps with patients. There is no one-size-fits-all. He is reflective and intense in wanting to get better at this. He interviews geriatricians, patients, and community activists to see how docs can engage more effectively with their patients.
Gawande brings up all of these issues without finger pointing. He acknowledges the complexities of deciding on how much care to seek for our loved ones. He also acknowledges the absurdity of our broken system with humor. He muses that if there were an implantable “automatic defrailer” device that could reduce
Reviewed By Nate Hitzeman, MD
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].
BOOk rEVIEW

September/October 2015 17
end-of-life discussions with patients and their families, I know I have made missteps, and I have already found these four questions extremely helpful. Within days of reading this book, this approach helped me uncover that a middle-aged lady with metastatic lung cancer who kept returning to the ED was most fearful of falling at home and not of dying. Our focus became that. When rounding with the residents on a young man dying from an untreatable GI malignancy, it became clear that he wanted a feeding tube to allow him to go on a two-week road trip he had been planning for a long time with an old friend. After that, he wanted to pursue hospice. That road trip became our goal.
Gawande quotes a palliative care specialist as saying, “A family meeting is a procedure, and it requires no less skill than performing an operation.” Many other pearls abound in this book. If you are talking more than 50 percent of the visit, you are talking too much. Don’t take away hope, but bring up the elephant in the room when it is clear a patient is dying. A good way to do this is by pushing the computer screen aside for a moment, looking right at the patient and family, and saying “I’m worried about you. I’m very worried” and then let the pregnant pause deliver the insight to them and follow their lead.
Two doctors from different hospitals I have talked to recently about this book independently declared, “This book should be required reading in every medical school.” I have to agree. I think you will, too, after reading Being Mortal. I hope it touches you deeply, makes you question your own habits and approaches, and most importantly, motivates you to appreciate every fleeting moment of the rest of your life and the undying spirit of family.
Books and their wisdom are immortal. Pass this gift on to others.
the need for higher level care placement by 40 percent – similar to the effect of having outpatient multidisciplinary geriatric teams – “we’d be clamoring for it. We wouldn’t care if doctors had to open up your chest and plug the thing into your heart.”
So why are only 300 residents a year becoming geriatricians? Why are geriatric departments being shut down? All this in a country where our elderly population is going to double between the years 2010 and 2030? Bonkers!
Gawande is not overly sentimental, and he lets the experiences speak for themselves. But there are moments in this book that will jerk your tears and make you reflect on your loved ones who have passed or almost passed. As he details his father’s slow demise with cancer, I found myself thinking of my own father’s near death at Kaiser South San Francisco three years ago. Heart attack, atrial fibrillation, on pressors and BiPap, cath lab one hour away at the downtown facility. I would have done anything at that moment for a chance to pull him through, whatever the cost! I wanted everything done! He got great care, not perfect care (can it ever be so to a physician family member?), but great, and he pulled through.
I contrast this with my yearly trips to Nicaragua where many of the dying people just straight up don’t get advanced treatments because they aren’t available or are too expensive. This is rationing, and developed countries are eventually going to feel it more as our proverbial medical snake-on-the-staff swallows more of the GDP pie.
If you take away nothing else from Gawande’s book, remember these four questions to ask your patients and loved ones who are ill: “What is your understanding of the situation and its potential outcomes? What are your fears and what are your hopes? What are the trade-offs you are willing to make and not willing to make? And what is the course of action that best serves this understanding?” A condensed version of this is, “If time becomes short, what is most important to you?”
As a family physician who has had many
“For human beings, life is meaningful because it is a story.” – Atul Gawande, MD

18 Sierra Sacramento Valley Medicine
Eyes on the PastFrom Study Sets to Prosthetic Eyes
OFTEN, TALKS I GIVE TO service organizations have bonuses. At a recent talk on “Gold Rush Medicine” I gave to a Rotary Club, I met Phil Danz, a retired ocularist, a specialist with a 48-year history of fitting and fabricating prosthetic eyes. In addition, he has a related family history going back generations. He recently donated a collection of prosthetic eyes to our Museum of Medical History.
The glass eyes in our museum are made of cryolite glass, a special soft, and easy-to-form or to blow, glass. This glass is non-toxic, is very compatible with human tissue, and was developed in Lauscha, Germany, as the special sands required are found in that area. Others tried, but were not able to replicate the cryolite. After WWII, acrylic material became available. It was moldable, lighter weight, and easier to fabricate accurately and is now the preferred material in most of the world. Most prosthetic eyes now fitted in the U.S. are made of acrylic plastic and are custom-molded to accurately fit the patient’s anatomy.
A prosthesis may be required due to an injury to the eye that then becomes atrophied and unsightly, in which case a thin scleral shell prosthesis is used. Or, if the eye was surgically removed (enucleated), an ocular implant inserted to mimic the volume of the lost eyeball would be used.
The eyes are retained in the socket by the fitting of the glass eye into the natural eye cul
de sac (the conjunctival lining of the eyeball which allows eye movement or motility). This space, and the pressure from the eyelids, keep the prosthesis in place.
Phil’s family dates back to Lauscha, Germany, and has been involved with artificial eyes for eight generations. He is related to Ludwig Müller-Uri, who invented the German method of manufacture that became globally
preeminent for about 130 years, starting in the 1830s. His family also started the fitting of glass eyes for humans in Germany in the 1830s.
Another part of the story involves a rare kit of 123 custom glass eye specimens
that replicate eye diseases, made by Phil’s great uncle, Amandus Müller, in the 1880s. The kit contains blown glass eye pathology specimens used as teaching aides for German and European medical schools. Phil recalled that his grandmother, Anna Müller Reichart, who gave him the kit when she was 83, mentioned that only a limited number of kits were made, and it is possible that Phil’s is the only complete one remaining. The kit was given to his grandmother by Amandus Müller and reflects the history of eye pathology at that time.
Phil had donated the rare kit to UCSF in 1963, but it garnered little attention until recently, when the UCSF archivists discovered the kit in the basement of the library. Robert S. Sherins, MD, an alumnus of the UCSF School of Medicine, Class of 1963 and retired
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].
By Bob LaPerriere, MD
“Get thee glass eyes, and like a scurvy politician seem to
see the things thou dost not.”
— Shakespeare, King Lear, Act 4, Scene 5

September/October 2015 19
ocular surgeon, was asked to examine the kit. He discovered that most of the specimens represented traumatic injuries in younger patients, an indication that most patients did not live long enough to develop degenerative diseases.
The best examples were chosen for his UCSF lecture, manuscript and an exhibit honoring the Danz family for their contributions over eight generations. The exhibit, “Origin, History, Science and Art of the Ocular Prosthesis,” began May 28th, 2015 at the UCSF library, and is currently featured as part of the 150th Anniversary of UCSF. It is open to the public.
For more information about glass-blown products from Lauscha, go to: http://bit.ly/ 1K7OjLy
For more about Prosthetic Artists (formerly Phillip A. Danz and Associates), go to: www.phildanzeyes.com.
references
Our thanks to Dr. Robert Sherins and the University of California San Francisco for the content and sharing of the next three sites.
To view the UCSF lecture/video about the set of glass eyes go to: http://bit.ly/1KVQF5Z
To review a blog with further information on “History, Science, and Art of Ocular Prosthetics” Lecture and Reception at UCSF go to: http://bit.ly/1KVQF5Z
To view the PDF of the entire publication by Dr. Sherins go to: http://bit.ly/1gKfSU8
Prosthetic eyes, circa 1930, donated by Phil Danz.
| bloodsource.org | not-for-profit since 1948
Be a Source of Hope
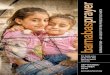
Jacqueline DeGracia, shown with her mother Leticia, needed plasma-based medicine to survive Kawasaki disease.
There’s more ways than ever to help patients in need – introducing source plasma. Source plasma donation, a type of blood donation dedicated for further development into lifesaving plasma-based medicines, is needed for patients with immune deficiencies, neurological diseases, blood disorders, and more. Learn more about donating source plasma by calling 866.822.5663 or visiting bloodsource.org/sourceplasma.
Together, we do save lives.

Exclusive Dinner and Presentation for Sacramento Area Physicians
The Anatomy of a Lawsuit and How to Mitigate Risk
The Cooperative of American Physicians, Inc. (CAP) is proud to join the Sierra Sacramento Valley Medical Society (SSVMS) in hosting a series of free, no-obligation risk management presentations designed to help physicians run safer, more successful practices. Our first presentation, The Anatomy of a Lawsuit and How to Mitigate Risk, will offer practical tips to help physicians reduce the chances of being named in a malpractice lawsuit and maintain positive doctor-patient relationships. You will also learn from examples of past cases the do’s and don’ts of a lawsuit, and how to best prepare yourself if faced with a lawsuit. We hope you will join us at The Citizen Hotel for a dining experience that celebrates the flavors of California’s Central Valley.
Join Us: Thursday, September 17, 2015
The Citizen Hotel 926 J Street Sacramento, CA 95814
Time: 6:00 p.m. — Registration and Cocktails
6:30 p.m. — Dinner and Program
Cost and Parking: Complimentary
To RSVP or For More Information:
Space is limited and reservations are required. To RSVP, contact Elizabeth Gomez at
213-473-8729 or [email protected] by September 11.
For more information about CAP, contact
Gary Homer at 916-409-0405 or email [email protected].
About SSVMS:
The Sierra Sacramento Valley Medical Society is dedicated to bringing together physicians from all modes of practice to promote the art and science of quality medical care and to enhance the physical and mental health of our entire community.
About CAP:
The Cooperative of American Physicians, Inc. was established in 1975 by a group of California physicians to manage the escalating cost of medical professional liability coverage. Two years later, CAP formed the Mutual Protection Trust (MPT), which has earned an A+ (Superior) rating from A.M. Best since 2006. CAP now supports nearly 12,000 of California’s finest physicians through offices in Los Angeles, San Diego, Orange County, Sacramento, and Palo Alto.
Susan Schmid, Esq., Managing Attorney, Schmid & Voiles, ABOTA member.
Susan Jones, BA, LVN, CPHRM CAP Senior Risk Management & Patient Safety Specialist
Presenters

September/October 2015 21
Background: Sutter Memorial Hospital in Sacramento officially closed its doors on August 8, as services are being consolidated to the Midtown Sutter Medical Center Campus. Many of our society members have delivered their own babies there, or the babies of their patients. We have also published a few stories in past SSV Medicine issues about artificial valve innovations and cardiovascular advances that have been pioneered at Sutter Memorial. From Sutter’s website: www.suttermedicalcenter.org/spiritualcare/history.html:
“The first satellite hospital in California, Sutter Memorial Hospital, opened in 1937. It was the first hospital in California to utilize isolation techniques and multiple nurseries for infants. Today, the 346-bed specialty medical center is known for its cardiovascular services, transplants and women’s and children’s specialty services.”
Commentary from some of our members follows:
We pioneered one of the first acute child psychiatric units in the USA. We started as a section of the pediatric medical floor. One of our first successes was a young boy admitted for asthma. He was very anxious and afraid to be any distance from his respirator. We integrated him into our program and he was able to overcome his anxiety and his asthma stabilized. −James Margolis, MD
Surpassing my many anesthesiology adventures at Sutter Memorial Hospital was the birth and neonatal care of my triplet grandchildren there. Our family appreciates the skilled and caring attention they received. Now young teens, the Paron triplets have no apparent deficits from their early birth and intensive care, and they continue to thrive. −Lee O. Welter, MD
My memories include being part of the team that developed the first neonatal ECMO (Extracorporeal Membrane Oxygenation) program in all of Northern California, and performing the first patient cannulation in 1987 in the NICU at Sutter Memorial Hospital. Development and growth of the Neonatal and Pediatric Surgical Programs at Sutter Memorial Hospital. The Neonatologists at Sutter Memorial Hospital, under the direction of Dr. Andrew Wertz, developed the ALS Program whereby critically ill neonates were able to be stabilized and transported by a specially-trained team of nurses and respiratory therapists to the NICU from their delivering hospital without the need for physician presence. This model was subsequently adopted by many, and now virtually all NICUs statewide and even beyond. −Clifford Marr, MD
I delivered both my children there. I also had the privilege of working with one of the
Memorable Experiences from Sutter Memorial
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

22 Sierra Sacramento Valley Medicine
Photos from Sutter Memorial Hospital in the 1940s and 1950s show off their modern radiol-ogy, surgery and maternity depart-ments.
finest group of Labor and Delivery nurses and OBGYNs/Perinatologists when I was in private practice. The level of patient care and compassion from everyone was amazing. It is truly the most baby friendly and highest quality newborn and maternal care I have experienced. It would be truly exciting to match that level
of care to a brand new facility when the new medical campus opens. −Hui Cheong, MD
I’ve worked at Sutter Memorial intermittently over the past 13 years as a family medicine resident and attending, seeing adults and infants, and delivering babies. Most memorable to me are the following: the bucolic drive down
H street (often in a hurry to get to deliveries), the great nursing staff, a special care nursery which had the smallest babies I have ever seen and amazing outcomes nonetheless, the old buildings with an odd layout and series of zigzags to get from one end to another, finding various branches and leaves smothering my car after a Fall shift (huge trees!), and the rewarding meals at nearby Sellands and Café Rolle when sustenance was needed. Middle-of-the-night deliveries in a haze of caffeine, much needed nursing station gossip, and convoluted baby daddy scenarios that made my brain hurt. Postpartum hemorrhages flowing like the Ganges that we were able to quell through great teamwork. Dr. Wertz and his little AM radio listening to sports updates while charting in the NICU. An insanely-small Emergency Department that seemed to work miracles and have staff that had been there for decades (think Overlook hotel in The Shining). Helping hold my first daughter down on the table while they

September/October 2015 23
Sutter Memorial Hospital had a long tradition of being Sacramento’s baby hospital. Over 346,500 babies were delivered there from 1937 to present day.
attempted a spinal tap. Helping hold my second daughter down while they placed stitches on her head. Faces, names, lives, deaths, storms, quiet between the storms, consulting with colleagues, messy doctors’ lounge with the TV on too loud, overall warmth and caring and community! Much will be gained and much will be lost with the move of this hospital. −Nathan Hitzeman, MD
With the closing of Sutter Memorial Hospital, there are years of memories that will be indelible from an obstetrical standpoint. Since opening in 1937, over 340,000 babies have been delivered there. I have been privileged to be a part of the obstetrical staff for over 35 years. In the late 1960s, my former partner in practice, Erwin Eichhorn, MD, was passionate in his desire for family-centered care. He fought hard to allow fathers in the labor and delivery room to support their wives in this incredible life-altering experience. Now, of course, it is standard practice.
In 1974, the NICU was headed by Dr. Andrew Wertz who revolutionized the care of premature and ill newborns at birth. Perinatal obstetrical services became a reality in the early 1980s, in large part due to Dr. Jack Schneider. In the mid 1980s, Dr. Michael Plummer headed the outstanding obstetrical anesthesia department which offered epidural services 24 hours a day, 7 days a week. In the late 1980s, as OB-GYN chairman at the time, I helped develop a system of 24/7 obstetrical care for the many patients who came to Sutter with no prior prenatal care (aka “no doc” patients).
I personally cared for three patients who suffered amniotic fluid emboli (80 percent fatal in most cases). By the grace of God and the superb nursing and staff, all three
patients survived along with their babies. In my 35 years of practice, I have had the pleasure to have delivered successive generations of babies within the same families. Due to Sutter’s excellent reputation for nearly 80 years, many in the community can say with pride, “I was born at Sutter Memorial Hospital.” −Stephen Hiuga, MD

Contact SSVMS TODAY to Access These MEMBER ONLY BENEFITS
(916) 452-2671
PUBLICATIONS
BENEFIT RESOURCE Reimbursement Helpline FREE assistance with contracting or reimbursement
CMA’s Center for Economic Services (CES) www.cmanet.org/ces | 800.401.5911 | [email protected]
Legal Services CMA On-Call, California Physician’s Legal Handbook (CPLH) and more...
CMA’s Center for Legal Affairs www.cmanet.org/resources/legal-assistance [email protected]
Insurance Services Life, Disability, Long Term Care, Medical/Dental, Workers’ Comp, and more...
Mercer Health & Benefits Insurance Services LLC Cmacounty/[email protected] www.countyCMAmemberinsurance.com
Travel Accident and Travel Assistance Policies This is a free benefit for all SSVMS members.
Prudential Travel Accident Policy & AXA Travel Assistance Program http://tinyurl.com/SSVMS-travel-policy
ICD-10-CM Training Deeply discounted rates on several ICD-10 solutions, including ICD-10 Code Set Boot Camps
AAPC www.cmanet.org/aapc
Mobile Physician Websites Save up to $1,000 on unique website packages
MAYACO Marketing & Internet www.mayaco.com/physicians
Auto/Homeowners Insurance Save up to 10% on insurance services
Mercury Insurance Group www.mercuryinsurance.com/cma
Car Rental Save up to 25% - Members-only coupon codes required
Avis or Hertz www.cmanet.org/groupdiscounts
CME Certification Services Discounted CME Certification for members
CMA’s Institute for Medical Quality (IMQ)
Financial Services Up to $2,400 in savings on banking services
Union Bank
Health Information Technology Free secure messaging application
DocBookMD www.docbookmd.com/physicians/
HIPAA Compliance Toolkit Various discounts; see website for details
PrivaPlan Associates, Inc www.privaplan.com
Magazine Subscriptions 50% off all subscriptions
Subscription Services, Inc
Medical ID’s 24-hour emergency identification and family notification services
MedicAlert www.cmanet.org/groupdiscounts
Medical Waste Management Save 30% or more on medical waste management and regulatory compliance services
EnviroMerica www.cmanet.org/groupdiscounts www.enviromerica.com
Office supplies, facility, technology, furniture, custom printing and more… Save up to 80%
StaplesAdvantage www.cmanet.org/groupdiscounts
Physician Laboratory Accreditation 15% off lab accreditation programs and services Members only coupon code required
COLA www.cmanet.org/groupdiscounts
Security Prescription Products 15% off tamper-resistant security subscription pads
RxSecurity www.rxsecurity.com/cma-order
[email protected] | (916) 452-2671
CMA Publications www.cmanet.org/news-and-events/publications
CMA Alert e-newsletter CMA Practice Resources
CMA Resource Library & Store www.cmanet.org/resource-library/list?category=publications
Advance Health Care Directive Kit California Physician's Legal Handbook Closing a Medical Practice Do Not Resuscitate Form HIPAA Compliance Online Toolkit Managed Care Contracting Toolkit Model Medical Staff Bylaws Patient-Physician Arbitration Agreements Physician Orders for Life Sustaining Treatment Kit
SSVMS Publications www.ssvms.org/publications.aspx
Sierra Sacramento Valley Medicine (bi-monthly magazine) Medical Society News (monthly e-Bulletin)

September/October 2015 25
The Sierra Sacramento Valley Medical Society Alliance would like to thank the following generous donors to the Community Endowment Fund. The $11,300 raised will help support programs promoting the health of our region's citizens.
PLATINUM LEVEL Dr. Nick and Kim Maje�ch Dr. Dennis and Nancy Marks Amy Wandel, MD Dr. Gordon and Merrily Wong GOLD LEVEL Dr. Jim and Barbara Andras Donis Eichhorn George Lian, MD SILVER LEVEL Karen Banker Marla Bommer Dr. Walt and Joan Brainerd Paula Cameto Celeste Chin Dr. Jose and Anita Cueto David F. Dozier Jr., MD Dr. Daniel and Carla Flamm Francine Gallawa, MD Drs. Michael and Katherine Gillogley Henry Go, MD
Kathy Greenhalgh Dr. Julian and Diane Holt Dr. Pei‐Hsiu and Alice Huang Dr. Forrest and Pat Junod Suzanne Kilmer, MD Dr. Douglas and Kathryn Kindall Scarlet LaRue, MD Evie Lieb Jerilyn Marr Dr. Del and Linda Meyer Dr. Allen and Glenda Morris Mary Ann H. Murray Robert G. Myers, MD Anh H. Nguyen, MD Dr. Russ and Ingrid Niles Frank Palumbo, MD Ann Parsons Gail Pirie, MD Dr. Hal and Donna Renollet Joan Rice Shelly Schermer Roy Schutzengel, MD Lisa Smith
Mary Sterner‐Sosa, MD Stewart Teal, MD Dr. William and Kathryn Ve�er Ka�e White Deborah Wills Dr. John and Karen Young BRONZE LEVEL Dr. Sallie and Jess Adams Renee Anderson Dr. and Mrs. John M. Babich Carol Bargar E. Lawrence Bingham, MD Peter Carruth, MD Dr. Sco�e and Cat Dogge� Erla Goller Donald Hopkins, MD Marni E. Kaplan Mary Lee Moritz Dr. Jim and Carolyn Reece Mary Lou Trowbridge Susan Vogel Peter Wu, MD

26 Sierra Sacramento Valley Medicine
REGARDLESS OF OUR VIEWS on the subject, we can all agree that the cost of medical care in the United States keeps many people from obtain-ing the health services they need. Although we are all affected, those without health insurance bear the brunt of this cost. The Affordable Care Act specifically excludes undocumented resi-dents of the United States from its benefits. In California there have been efforts to remedy this. At the California Senate Health Committee hearing, held on April 15, 2015 on SB 4, several stories of undocumented residents were heard.
One 27-year-old woman told how, when she was seven years old, her mother went into a coma and was hospitalized. The diagnosis was type 2 diabetes. Her mother refused to get medical care after that because of the cost to her family. Her mother died last year.
Another undocumented young woman told the committee that her mother has said that when she dies, her daughter can sell all her possessions to bury her without going into debt. But if she goes to the doctor when she is sick, she will bury her family in debt. Fortunately, there are efforts in California to expand health care to all.
The second half of June 2015 was a remarkable time for those who advocate for universal health care in the United States, and gave hope to the people who testified at the April hearing, that things might improve.
At the federal level, the Supreme Court affirmed the Affordable Care Act (ACA) and subsidies for those who buy health insurance
on the exchanges, whether they are set up by the federal government or by a state.
At the California State level, SB4, also known as Health4All, was passed by the Senate. Although the bill had been reduced from its initial ambitious version of including all undocumented residents of California in the benefits of the ACA (price tag $400 million), to covering all children up to the age of 19 regardless of legal status (price tag $40 million), the Governor’s signature on the budget affirmed the view that we are all healthier when everyone has access to health care, regardless of legal status.
At the local level, the Sacramento Board of Supervisors voted on June 16 to reverse their policy of not serving undocumented residents of Sacramento, and to create a health care program for adults between the ages of 19 and 64, regardless of legal status. This came during the budget hearings in which the Board unanimously approved the program. In addition, they approved funding to reduce infant mortality among African-Americans, which is more than twice that of any other race or ethnicity, and funding to reinstitute a functional mental health program in the county.
The meeting was very well attended, with demonstrators in front of the building for “All Lives Matter.” The audience was very supportive of these budget augmentations, and there was celebratory applause when the Board vote was done.
The good news does not end here. The
By Glennah Trochet, MD, former Sacramento County Public Health Officer
Moving Toward Universal Health CareCalifornia Senate Passes SB4, Also known as Health4All
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

September/October 2015 27
State of California runs a program for medically indigent adults in 35 small, rural counties. This County Medical Services Program (CMSP) is the equivalent of the County Medically Indigent Services Program (CMISP), run by Sacramento and other large counties. For years they have excluded undocumented residents from these services. The Board that governs this program voted on June 25 to include undocumented residents in the CMSP program. With one stroke of the pen, 35 additional counties have a policy change!
SPIrIT Program Will Be keyAll this good news is very encouraging.
However, policy changes must be effectively implemented or they become only symbols without substance. For example, the program to help undocumented adult residents of Sacramento is modest. Initially it will serve a maximum of 3,000 individuals and will rely on the only county clinic still in operation to provide primary care. Specialty care is still to be defined. The SSVMS SPIRIT program will be key to providing specialty care for this population.
The Sacramento Physicians’ Initiative to Reach out, Innovate and Teach (SPIRIT) Program, a collaboration of the medical society and health systems, currently provides donated surgical services to undocumented immigrants and is collaborating with Sacramento County to expand the specialty services offered.
At a meeting for stakeholders that took place on June 24, it was clear that much still needs to be worked out. However, the principle that everyone in Sacramento should have access to health care, regardless of legal status, has once again been endorsed by our elected officials.
Here are a few details that still need work: There is no program for undocumented residents over the age of 64. Many undocumented adults
are seen in community clinics and by physicians in their offices, and it is the desire of those who advocated for the program that these providers also have access to a network of specialists. How this would happen has not been determined. Stakeholders will need to remain vigilant to ensure that this program is successful and has continued support from the Board of Supervisors.
I am not as familiar with the initial steps to implement services at the state level, but I’m sure that the details will be just as important to ensure that there is real access for the target population.
reference
Video of CA State Health Committee hearing, April 15, 2015 http://calchannel.granicus.com/MediaPlayer.php?view_id=&clip_id=2746&meta_id=64581
Physicians Nurse Practitioners ~ Physician Assistants
Locum Tenens ~ Permanent Placement
S.S.V.M.S.12-11-13
Tracy Zweig AssociatesA R E G I S T R Y & P L A C E M E N T F I R M
Voice: 800-919-9141 or 805-641-9141FAX : 805-641-9143
INC.

28 Sierra Sacramento Valley Medicine
College of PharmacyCALIFORNIA NORTHSTATE University’s (CNU) College of Pharmacy was launched in Rancho Cordova in 2007 after some concerned pharmacists, physicians and other financial sponsors pooled together a capital fund for establishing a pharmacy college in response to an anticipated shortage of pharmacists. In 2011, it acquired the former AAA call center in Elk Grove and moved in three years later. It currently has over 450 students and 70 faculty and staff.
CNU’s College of Pharmacy was the concept of two pharmacists from Kaiser. One of the pharmacists, Alvin Cheung, is the President of California Northstate, which was financed by private capital and professionally accredited in 2013. A total of 379 students have graduated so far, and pass rates on licensure exams have been high. Ninety-two percent of graduates in the class of 2014 are employed full-time.
CNU recently acquired an adjacent building which is largely leased for the next five years, but the remaining available space will be used for the benefit of students.
College Of Health SciencesCalifornia Northstate University’s College
of Health Sciences has been in the planning stage for several years. This past May, the program received Western Association of Schools and Colleges (WASC) accreditation. The College is designed to prepare students for medical, pharmacy, dental, and other graduate professional health care schools and has a planned class size of up to 200 students. The Dean, Rose Leigh Vines, has a doctorate in anatomy from California State University, Sacramento, and prior to retirement, taught there for over three decades.
College of MedicineThe CNU Board of Trustees approved plans
for a medical school in 2010. After a whirlwind
of preparation and capital raising, the College of Medicine attained applicant school status with the Liaison Committee on Medical Education (LCME) in 2011. The Founding Dean, Dr. Joe Silva, is a former Dean of the University of California Davis Medical School. The facility, staff and curriculum were ready for acceptance of their first class as early as 2011, but the accreditation process is slow, at best.
In June 2013, the LCME, which oversees accreditation, eliminated a standard that could have had the effect of a near impossibility for a privately-funded medical school to be approved. With that obstacle lifted, and after multiple sessions of document review, the accreditation body completed a site visit in January of this year. The College of Medicine then received preliminary accreditation in June.
The first class will be about 60 students this fall, with a goal of controlled growth over time. The curriculum for the first two years, which will integrate science and classroom study with clinical medicine, will be followed by clinical rotations at area hospitals, doctor offices and clinics. The concept is to provide cost-effective, quality education by working with community partners to offer clinical training, rather than building a new medical center. The school will also bring together pharmacy and medical students for inter-professional education.
California Northstate is the nation’s first for-profit traditional medical school created from “scratch.” Despite concern by some about for-profit medical schools, there is tremendous support from the community and the medical colleagues for Northstate, especially with its focus on primary care.
If you are interested in opportunites at Northstate, contact Dean Silva directly by email at [email protected].
By Bob LaPerriere, MD
New Med School in Town
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].

September/October 2015 29
Memories of odd schools, these bodies, cold and rigidMy white coat was for days the chosen territory of formaldehydeThe interview needs dissection So needs, we’re so told, our every action Our Hippocrates’ oath is shaken By the rolling of boulders from Adminland We’ve just entered the torture chamber93011, 90899C, 99214… To figure out which lucky number to pick Make sure you count the “bullet” points, quick In this gun culture, my hands shake, uneasy About being the target of invisible auditors, Almighty… Queen Mother Likes to keep her MDs Even buzzier than can beNow our charts must justify the time for vitalsThe signs of life or the signs of declining healthI feel like shouting, “Let me through, the SySTEM needs to breathe… I am a doctor!” I want to help people Where is the way to this safe temple? I am not a very skilled acrobat To satisfy the fancies of bureaucratsNot enough that our brains are useless without companies’ seal of approvalFor diagnostic tests, medication choices or doses… I am so appalled! “Beware, these codes will expire July 1st, please use more granular ones” Not sure why, some words just make my teeth grind moreAnd July 1st is tomorrow, with my documentation habits in goreBut hey, by the way Also… Canada Day! O! Beloved universal health care, with not as many bullet points... or wounds!
On Box-MakingBy Caroline Giroux, MD
“Add-on psychotherapy”: scroll down very far, click a check box “Interactive Complexity”: (implicit…) but you still have to click! Check another box 95510, one note if a patient is dysregulated And then a separate one… when crisis has finally dissipated A manager told me that an MD Is now a glorified secretary From eight to five, the flat screen eats me aliveWhat about all this wisdom, in my soft drive?Better set the chicken timer for med management Drrrrrrriiiiiiinnnnng! Now time to set it for psychotherapy, No more medical questions allowed, sorry Scrutiny is this insidious shadow upon us, dictating without trustWill our skills disintegrate, to the stage of dust?I hate moving, I hate packing Boxes segregate my treasures, I always forget where all went Patients have so many beautiful complexities But how to intervene when our thinking is in chronic agranulocytosis Remember? I once studied for many years to become a doctor I believed in the path of recovery through relationship Have I espoused a now sinking ship?This trusting, continuous process is hard to decorticateyet I hope impossible to desecrate Remember: I am not a box-filler, I am doctorWith growing knowledge, competency made of aware ignoranceAlready tired of this click-click-click danceAnd whose 10 min each visit it would take extra to be a coder Could be used in a way much better…

30 Sierra Sacramento Valley Medicine
Bioelectrical Medicine Deep brain stimulation is used to treat some movement disorders such as Parkinson’s disease and Tourette’s Syndrome, as well as some mood disorders and cluster headaches.
BIOELECTRICAL MEDICINE IS increasingly being employed as electricity-based therapy to treat neurological and psychiatric disorders. Utilizing stereotactic and imaging procedures, subcortical regions of the brain, including neuronal pathways and nuclei, can be targeted with implantable electrodes. The application of electrical currents to these electrodes is used to functionally interrupt pathological impulses, as well as to control the release of neuro-trans-mitters associated with movement, mood and headache disorders. This bioelectrical medical technique is commonly referred to as deep brain stimulation (DBS). A brief history and review of DBS techniques will be covered as well as examples of using this electricity-based therapy to treat Parkinson’s disease, Tourette syndrome, depression and headache.
Early HistoryDuring the fourth century AD, the ancient
Romans reportedly applied electric eels to the scalp as a treatment for headache. Electric fish were also used to treat seizures, depression and pain up until the eighteenth century in Europe. Later, during the nineteenth century, Giovanai Aldini, nephew of Luigi Galvani, promoted the use of applying electricity directly to the cortical surface for treating neuropsychiatric disorders.
Many animal studies were also conducted during this time with stimulating currents to the central nervous system (CNS) that aided early neuroscientists in understanding the functional role that many cortical surface areas played in behavior. These discoveries enabled investigators to electrically conform the motor topography of the human brain when the cortical dura matter
was exposed through accident and disease. More accurate findings of the human
cortical topology came about with the notable studies of Wilder Penfield in the early twentieth century. Penfield’s electrical cortical stimulation provided an accurate representation of many motoric and sensory brain functions that led to the cortical homunculus, which neurosurgeons currently rely on during treatment procedures.
Deep Brain Stimulation (DBS)Early investigational procedures employed
to treat psychiatric and headache disorders lesioned various brain structures. Surgical procedures, such as lobotomy, transorbital leucotomy and stereotactic lesioning, were utilized in the mid-twentieth century to disconnect communication between various regions of the central nervous system. More medically-effective psychopharmacological therapies eventually replaced these surgical procedures for managing psychiatric and neurological disorders.
Deep brain stimulation was originally termed neuromodulation by Norm Shealy in 1967 as a method to treat cancer pain using the first dorsal column stimulator. Neuromodulation was first described as a physiological process whereby neurons could be electrically excited to release multiple neurotransmitters such as acetylcholine, norepinephrine, dopamine and serotonin.
DBS came into its own with the evolution of functional neurosurgical techniques that included neural stimulation and stereotactic localization of subcortical structures in the thalamus and cerebellar nuclei. With the advent
Comments or letters, which may be published in a future issue, should be sent to the author’s email or to e.LetterSSV [email protected].
By Kent Perryman, Ph.D.

September/October 2015 31
of the first human stereotactic atlas by Ernst Spiegel and Henry Wycis in 1947, precise coordinates for subcortical nuclei could be localized.
Initially, electrical stimulation of these sites was employed to confirm accurate localization prior to lesions. It was soon realized that the electrical stimulation could also be used as a therapeutic method itself, not only as a neuromodulator, but also to restore normal neuronal activity. Consequently, the evolution from lesional to stimulating functional neurosurgery had occurred. Also, the major safety of DBS led to a gradual abandonment of lesional techniques.
DBS Surgical Procedure The DBS surgical procedure begins with
MRI or CT imaging for stereotactic localization of stimulus sites in the thalamus, subthalamic nucleus (STN) or globus pallidus (GP) in the case of Parkinson’s disease (PD). The DBS System consists of electrodes, an extension cord, and an implantable pulse generator (IPG) including battery.
The IPG is a programmable digital device the size of a stopwatch used to deliver electrical stimulation. The electrode component is a thin wire insulated along the shaft with some bare exposed wire at the tip for current propagation. The electrode is inserted into a stereotactically-mounted guide tube and lowered to the precise target site. In some instances a bipolar (two adjacent electrodes) stimulation procedure must be employed to restrict current spread.
The distribution of the stimulus current field is crucial in controlling neuronal activation of minuscule fiber tracts or nuclei. The guide tube is then retracted leaving the electrode to be cemented to the cranium for attachment of the extension cord. In some instances, multiple electrodes are placed in the thalamus, subthalamic nucleus (STN) or the globus pallidus (GP) in the case of Parkinson’s disease (PD).
The extension cord is composed of multiple insulated wires that are passed under the scalp, neck and shoulder and connected to the IPG.
The IPG is normally implanted under the skin near the clavicle. Sometimes there may be complications such as bleeding within the brain, brain edema, mild disorientation and sleepiness following surgery.
Following implantation, the next step is selecting appropriate stimulation parameters to provide the maximum therapeutic benefit. Finding the optimal voltage, pulse width and frequency is a process of trial and error to assess the clinical benefit. In some instances, computer models have been employed to determine optimal stimulation parameters
Insertion of electrode during surgery using a stereotactic frame.

32 Sierra Sacramento Valley Medicine
based on electrode location using MRI and CT images.
Short duration pulses are normally employed to reduce charge injection and increase the therapeutic window with non-damaging stimu-lation. Some examples of stimulus parameters include frequencies of 0-15 HZ, pulse widths of 60-450 microseconds and voltages up to 10.5 volts. Some short-term adverse effects of DBS are paresthesias, headache, dysarthria, paresis, gait disturbances and ataxia. These adverse effects can usually be managed by adjusting the stimulation parameters.
Therapeutic Brain StimulationParkinson’s disease (PD). Medtronic was
one of the first manufactures to develop neural stimulators for French neurosurgeons to treat movement disorders in 1987. Canada, Europe and Australia approved the use of Medtronic’s IPG for movement disorders in 1993. The United States Food and Drug Administration approved DBS of thalamic nuclei for
PD-related tremors in 1997, followed in 2003 for the subthalamic nucleus (STN) and globus pallidus (GP).
PD is a neurodegenerative disease character-ized by symptoms of rigidity, tremor, bradykine-sia and postural instability. DBS is only recom-mended for patients with medically-refractory PD who demonstrate no symptoms of cognitive impairment. The STN is currently the optimal stimulation target for reducing the occurrence of movement disorders. The patient is still required, in most instances, to maintain a schedule of medications at a reduced dosage. Most patients with PD who have undergone DBS experience an improved quality of life with a reduction of dyskinesias.
Tourette’s Syndrome (TS). Tourette’s, which is characterized by multiple motor tics, is observed more frequently in pediatric populations and generally disappears by adulthood. DBS is not recommended as a functional neurosurgical treatment for child- ren, and consequently is reserved only for
intractable TS adult patients. There are multiple effective DBS target sites in the thalamus, including the centromedian (CM) as well as the globus pallidus (GP). TS patients receiving DBS have a 37-82 percent favorable response rate with sustained tic reduction for up to 10 years following surgery.
Obsessive Compulsive Disorder (OCD). OCD is characterized by time-consuming intrusive thoughts (obsessions) and compulsions that interfere with the individual’s level of social and occupational functioning. OCD affects approximately 1-2 percent of the population with 40 percent of those re- sponding unfavorably to
Reconstruction of DBS electrodes implanted in the substantia nigra and subthalamic necleus.

September/October 2015 33
pharmacological interven-tions. DBS that targets ventral capsule/ventral striatum area results in a favorable response rate of 62 percent for those intractable OCD patients.
Bipolar Affective Disorder (BD). BD is characterized by distinct periods of mania offset by periods of depression. DBS-targeted regions of the subcallosal cingulate demonstrate a favorable response rate of 92 percent for manic symptoms and 58 percent for the depression component in patients with medically-intractable BD. Favorable outcome measures have also been associated with DBS treatments for unipolar depression.
Cluster Headaches (CL). Cluster headaches are characterized by recurrent, severe headaches on one side of the head; typically around the eye. CL is assigned to primary headache disorders known as trigeminal autonomic cephalalgias (TACs). DBS intervention for drug-resistant CL, targets the ipsilateral hypothalamus. A limited number of patients have benefited from DBS treatments for 2-22 months post procedure.
ConclusionMany of these neurological
and psychiatric disorders may share common neural circuits, which benefit from the administration of electrical excitation. Targeting one or more neuronal regions may trigger multiple neurons in adjacent pathways underlying these disorders. The therapeutic effects of DBS may originate from its rebalancing of damaged neuronal circuits that entails the encouragement of alternate pathways in the CNS.
An attractive feature of DBS is its reversible nature, unlike previous lesional procedures that were once employed by the medical community. However, an objective and statistically-valid assessment of long-term results is impossible due to medically-ethical concerns. DBS treatments cannot be statistically evaluated in a controlled, double-blind procedure as required
for scientific validation. Therefore, treatment concerns must rely on employing the DBS procedure when other methods of treatment goals cannot be achieved.
references
Altinay, M, Estemalik, E, Malone Jr, DA. A Comprehensive Review of the Use of Deep Brain Stimulation (DBS) in Treatment of Psychiatric and Headache Disorders. www.medscape.com/viewarticla/841638-print
Kern, DS, Kumar, R. Deep Brain Stimulation. T. Neurol., 2007; Vol13(5): 237-252.
Sironi, VA. Origin and Evolution of Deep Brain Stimulation. Front. Integr. Neurosci., 2011; Vol 5(42): 1-11.
Kelly Rackham[916] 616 [email protected]
KKelly Rackhaelly Rackhamm
P L A N E T E L L YD E S I G N / M A R K E T I N G

34 Sierra Sacramento Valley Medicine
July 13, 2015The Board:
Approved the SSVMS white paper, “Crisis in the Emergency Department: Removing Barriers to Timely and Appropriate Mental Health Treatment” and the following three recommendations contained in the paper to improve the quality of care for patients experiencing mental crisis: 1) Implement an electronic Health Information Exchange (HIE) in the Sacramento region to help coordinate care of patients seeking emergency psychiatric services; 2) Standardize the medical clearance process across all emergency departments and inpatient psychiatric treatment programs to facilitate the timely transfer of patients to appropriate treatment centers; 3) Establish dedicated psychiatric emergency services (PES) to maximally dis-impact the region’s EDs and ensure that patients experiencing a mental health crisis receive the right care at the right time.
Approved the endorsement of Ruth Haskins, MD for 2016 CMA President-Elect.
Approved the 2015 Second Quarter Financial Statements.
Approved the following changes in the SSVMS Delegation to the CMA: 1) Move Alan Ertle, MD, who previously occupied the now eliminated Delegate At-Large Office 22 to the currently vacant Delegate At-Large Office 11; 2) Move Adam Doughtery, MD, who previously occupied the now eliminated Resident Delegate At-Large Office 23 to the currently vacant Alternate-Delegate Office 15; 3) Accept the resignations from Pat Samuelson, MD, Alternate-Delegate Office 14 and Olivia Kasirye, MD, Alternate-Delegate Office 16.
Approved to continue to support the mission of the California Public Protection and Physician Health, (CPPPH), which is dedicated to public safety and the health and well-being of California physicians, and to provide use of the SSVMS conference room and publication of CPPPH events.
Approved the 2015 Board of Directors reapportionment that the composition of the Board remain unchanged due to the May 1, 2015 reapportionment in accordance with SSVMS Bylaws, Article VII, Section 1(d).
Approved the Membership Reports for June 22, 2015 and July 13, 2015 as follows:
For Active Membership — Jeannette K. Berrong, DO; John Marshellito B. Canio, MD; William K. Chen, MD; Priya D. Chib, MD; Jenny Chou, MD; Gaurang Desai, MD; Rino H. Dizon, DO; Caroline Giroux, MD; Elilta M. Hagos, MD; Donald W. Hause, MD; Mary E. Horner, MD; Veeraparn Kanchananakhin, MD; Bernard K. Kao, MD; Nhein Le, DO; Judeth K. McGann, MD; Janice A. Santos Cortes, MD; Diane B. Saeed, MD; Andrés F. Sciolla, MD; Sheetal D. Sran, MD; Christopher W. Swales, MD; Nabin Timilsina, MD; Steven J. Wright, DO.
For Resident/Fellow Active Membership — Allison M. Aul, MD; Silen Bun, MD; Melissa Joy Chen, MD; Fayha Lakhani, DO; David D. Lee, DO; Ron Martin Garcia Menorca, MD; Ashley Montross, DO; Rashida Parween, DO; Augustine M. Saiz, Jr., MD.
For Reinstatement to Active Membership — George T. Bolton, MD; Roderick G.S. Sanden, MD; John J. Tiedeken, MD.
For Retired Membership — Nicholas D. Simopoulos, MD.
Termination of Membership for Nonpayment of Dues — Theresa D. Marsh, MD; Dan Nadler, MD; Zack M. I. Nakao, DO; Daniel A. Poon, MD.
For Resignation — Daren Danielson, MD (relocated to Minnesota); Edward A. Panacek, MD (relocated to Alabama); Robert Suskind, MD (relocated to San Bernardino).
Transferred Membership — Catherine V. Carroll, MD (to San Diego); Theodore M. Geissler, MD (to Fresno)
Deceased: Neil C. Andrews, MD (June 6, 2015)
Board Briefs

September/October 2015 35
Welcome New MembersThe following applications have been received by the Sierra Sacramento Valley Medical Society. Information pertinent to consideration of any applicant for membership should be communicated to the Society. — Rajiv Misquitta, MD, Secretary.
Allison M. Aul, MD, Obstetrics & Gynecology, University of Wisconsin Medical School – 2015, UC Davis Medical Center, 4860 y Street, Ste. 2500, Sacramento, 95817
Jeanette k. Berrong, DO, Family Medicine, Western University of Health Sciences College of Osteopathic Medicine – 2001, Dignity Health Medical Group – Woodland Clinic, 632 W. Gibson Road, Woodland, 95695
Silen Bun, MD, Family Medicine, UC Davis School of Medicine – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
John Marshellito B. Canio, MD, Internal Medicine, Howard University College of Medicine – 1994, Capitol Gastroenterology Consultants Medical Group, Inc., 6555 Coyle Avenue, Suite 330, Carmichael, 95608
Melissa J. Chen, MD, Obstetrics & Gynecology, Northwest University Feinberg School of Medicine – 2010, UC Davis Medical Center (Resident/Fellow Program), 4860 y Street, #2500, Sacramento 95817
William k. Chen, MD, Internal Medicine, College of Physicians and Surgeons of Columbia University – 1983, Mercy Medical Group, 6555 Coyle Avenue, Carmichael, 95608
Priya D. Chib, MD, Pediatrics, Ross University School of Medicine – 2005, Dignity Health Medical Group – Woodland Clinic, 632 W. Gibson Road, Woodland, 95695
Jenny Chou, MD, Ophthalmology, David Geffen School of Medicine at UCLA – 2004, Dignity Health Medical Group – Woodland Clinic, 1321 Cottonwood Street, Woodland, 95695
Gaurang N. Desai, MD, Neonatology, Gujarat University, B.J. Medical College – 1986, Mercy Medical Group, 6501 Coyle Avenue, Carmichael, 95608
rino H. Dizon, DO, Family Medicine, Midwestern University Chicago College of Osteopathic Medicine – 2008, The Permanente Medical Group, 1650 Response Road, Sacramento, 95815
Caroline Giroux, MD, Psychiatry, University of Montreal Facility of Medicine – 2000, UC Davis, 2230 Stockton Blvd., Sacramento, 95817
Elilta M. Hagos, MD, Family Medicine, St. George’s University School of Medicine – 2008, Dignity Health Medical Group – Woodland Clinic, 2330 W. Covell Blvd., Davis, 95616
Donald W. Hause, MD, Plastic Surgery, Baylor College of Medicine – 1986, Cosmetic Surgery Center of Sacramento, 705 University Avenue, Sacramento, 95825
Mary E. Horner, MD, Dermatology, UC Davis School of Medicine – 2011, Dermatology Consultants of Sacramento, 5340 Elvas Avenue, #600, Sacramento, 95819
Bernard k. kao, MD, Neonatology, Saint Louis University School of Medicine – 1998, Mercy Medical Group, 6501 Coyle Avenue, Carmichael, 95608
Veeraparn kanchananakhin, MD, Pediatrics, Chiang Mai University (Thailand) – 1997, Dignity Health Medical Group – Woodland Clinic, 2330 W. Covell Blvd., Davis, 95616
Fayha Lakhani, DO, Family Medicine, Touro University College of Osteopathic Medicine – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
Nhein Le, DO, Family Medicine, Ohio University College of Osteopathic Medicine – 2007, Dignity Health Medical Group – Woodland Clinic, 1207 Fairchild Court, Woodland, 95695
David D. Lee, DO, Family Medicine, Western University of Health Sciences – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
Judeth k. McGann, MD, Pediatrics, Albany Medical College – 1993, Dignity Health Medical Group – Woodland Clinic, 632 W. Gibson Road, Woodland, 95695
ron Martin Garcia Menorca, MD, Family Medicine, University of Rochester School of Medicine – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
Ashley Montross, DO, Family Medicine, Touro University College of Osteopathic Medicine – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
rashida Parween, DO, Family Medicine, Touro University, Nevada – 2015, Sutter Health Family Medicine Residency Program, 1201 Alhambra Blvd., Sacramento, 95816
Diane B. Saeed, MD, Neonatology, UCLA School of Medicine – 1986, Mercy Medical Group, 6501 Coyle Avenue, Carmichael, 95608
Augustine Mark Saiz, Jr., MD, University of Wisconsin Medical School – 2015, UC Davis Medical Center, 4860 y Street, Ste. 3800, Sacramento, 95817
Janice A. Santos Cortes, MD, Urology, University of Puerto Rico – 2004, Dignity Health Medical Group – Woodland Clinic, 2440 W. Covell Blvd., Davis, 95616
Andrés F. Sciolla, MD, Psychiatry, University of Chile, School of Medicine – 1983, UC Davis, 2230 Stockton Blvd., Sacramento 95817
Sheetal D. Sran, MD, Pediatrics, Government Medical College Patiala – 2006, Dignity Health Medical Group – Woodland Clinic, 632 W. Gibson Road, Woodland, 95695
Christopher W. Swales, MD, Family Medicine, St. George’s University School of Medicine – 2010, Dignity Health Medical Group – Woodland Clinic, 2330 W. Covell Blvd., Davis, 95616
Nabin Timilsina, MD, Internal Medicine, Magadh University Nalanda Medical College – 2001, Dignity Health Medical Group – Woodland Clinic, 1325 Cottonwood Street, Woodland, 95695
Steven J. Wright, DO, Otolaryngology, Touro University College of Osteopathic Medicine – 2006, Dignity Health Medical Group – Woodland Clinic, 1321 Cottonwood Street, Woodland, 95695
CLASSIFIED ADVErTISING
PHYSICIANS FOr JUDICIAL rEVIEW COMMITTEES
The Institute for Medical Quality (IMQ) is seeking primary care physicians, board certified in either Family Practice or Internal Medicine, to serve on Judicial Review Committees (JRC) for the California Department of Corrections and Rehabilitation (CDCR). These review committees hear evidence regarding the quality of care provided by a CDCR physician. Interested physicians must be available to serve for 5 consecutive days, once or twice per year. Hearings will be scheduled in various geographic locations in California, most probably in Sacramento, Los Angeles, and San Diego.
IMQ physicians credentialed to serve on JRC panels will be employed as Special Consultants to the State, and will be afforded civil liability protection to the same extent as any Special Consultant. Physicians will be paid on an hourly basis and reimbursed travel expenses. Please contact Leslie Anne Iacopi ([email protected]) if interested.

36 Sierra Sacramento Valley Medicine
• Fast, accurate claims payments• Free eReferrals and online doctor-patient communications• Experienced RN case management for complex, time-intensive cases• Deep discounts on EPM and EHR solutions to help you meet the federal mandate• Easy preventive care and disease management reminders for patients• Extensive health resources that boost patient engagement• High consumer awareness that builds practice volume
At Hill Physicians, we continue to improve upon coordinated care, with remarkable results. We provide the tools and support that practices need to be financially successful and improve the coordinated care experience for their patients. Our advantages include:
That’s why 3,800 independent primary care physicians, specialists and healthcare professionals have joined Hill. Feel confident in the future of your practice and your patients by affiliating with Hill Physicians Medical Group.
Hill Physicians’ 3,800 healthcare providers accept HMOs and many PPOs from Aetna, Anthem Blue Cross, Blue Shield, CIGNA, Easy Choice, Health Net, Humana, SCAN, San Francisco Health Plan, United Healthcare WEST and Western Health Advantage. Medicare Advantage plans in all regions. Medi-Cal in some regions for physicians who opt-in.
Sunita Jain, M.D.Hill Physicians provider since 2003.
Uses Ascender preventive care reminders, RelayHealth online communication tools and Hill EHR for a comprehensive solution to patient care, practice management and ePrescribing.
Confidence
For more about the advantages of affiliating, visit HillPhysicians.com/JoinUs.
The feeling you have when you are affiliated with Hill Physicians.

Success.
Free Risk Management Dinner Presentations!
Since 1977, the Cooperative of American Physicians
(CAP) has provided superior medical professional liability
coverage and valuable risk and practice management
programs to California’s finest physicians through its
Mutual Protection Trust (MPT).
As a physician-directed organization, we understand the
realities of running a medical practice these days, and are
committed to supporting you with a range of programs
and services that no other professional liability company
offers. These include a 24-hour early intervention
program, HR support, EHR consultation, a HIPAA hotline,
and a robust group purchasing program, to name a few.
It’s what Sierra Sacramento Valley’s finest physicians strive for. . .and what CAP can help you achieve.
800-252-7706 | www.CAPphysicians.com
CAP is proud to join the Sierra Sacramento Valley Medical Society (SSVMS) in hosting a series of free, no-obligation risk management presentations designed to help physicians run safer, more successful medical practices.
These informative presentations will conveniently be held at three
select dining locations. We encourage you to attend any or all.
For more information or to reserve your spot, please call
(213) 473-8729 or email [email protected].
Times, locations, and further details can be found on the
SSVMS website at www.SSVMS.org/events.
September 17 Anatomy of a Lawsuit and How to Mitigate Risk
October 20 Avoiding Lawsuits: The Role Your Staff Plays
December 10 Protecting Your Online Reputation

© 2015 NORCAL Mutual Insurance Company. * Based on 2014 data.
Proud to be endorsed by the Sierra Sacramento Val ley Medical Society
GUIDEGUARDADVOCATE
844.4NORCAL | CA.NORCALMUTUAL.COM
MEDICAL PROFESSIONAL LIABILITY INSURANCE
CALIFORNIA PHYSICIANS DESERVE
Your Guide: Awarding more than 35,000 CME certificates in 2014*
Your Guard: Resolving 89%* of claims without indemnity payments
Your Advocate: Largest contributor to the No On 46 coalition
Our heart beats in California ... and has for almost 4 decades. Talk to a NORCAL Mutual agent/broker today.