Embed Size (px)
Citation preview
Sepsis Prevention Strategies: Stopping the Progression of Hospital Acquired Infections
Kristen Luttenberger RN, MSN, CCRN-CMC, PCCN, APNC
http://www.milkproduction.com/ImageVaultFiles/id_916/cf_4/st_edited/QTjFNqf6BJdhn5Cs7vaE.jpg
…..insufficient perfusion of cells and vital organs, causing tissue hypoxia which results in cellular, metabolic, and hemodynamic derangements
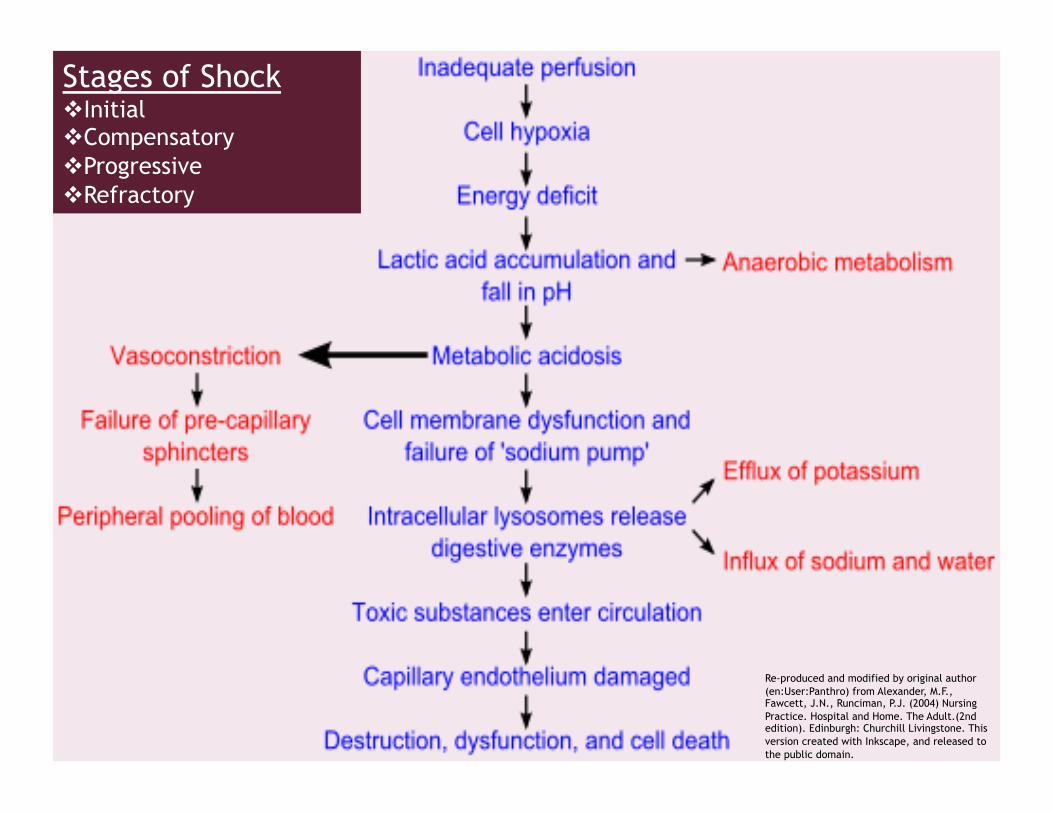
Re-produced and modified by original author (en:User:Panthro) from Alexander, M.F., Fawcett, J.N., Runciman, P.J. (2004) Nursing Practice. Hospital and Home. The Adult.(2nd edition). Edinburgh: Churchill Livingstone. This version created with Inkscape, and released to the public domain.
Stages of Shock Initial Compensatory Progressive Refractory
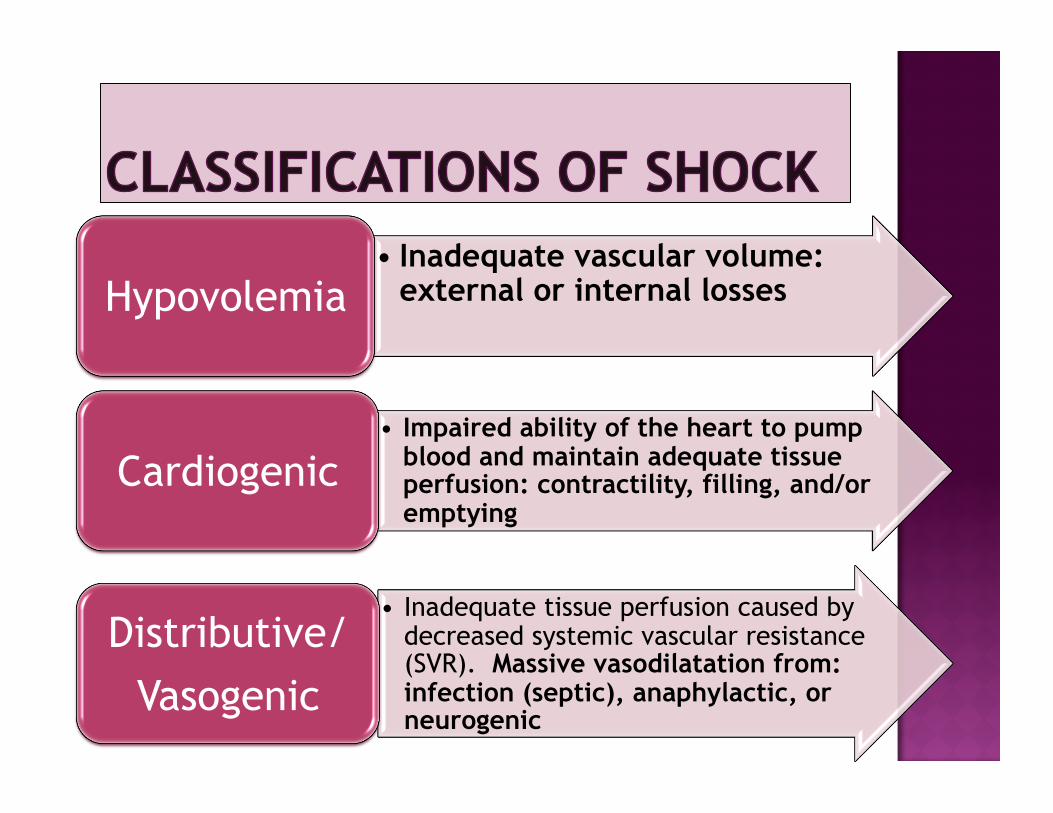
• Inadequate vascular volume: external or internal losses Hypovolemia
• Impaired ability of the heart to pump blood and maintain adequate tissue perfusion: contractility, filling, and/or emptying
Cardiogenic
• Inadequate tissue perfusion caused by decreased systemic vascular resistance (SVR). Massive vasodilatation from: infection (septic), anaphylactic, or neurogenic
Distributive/ Vasogenic
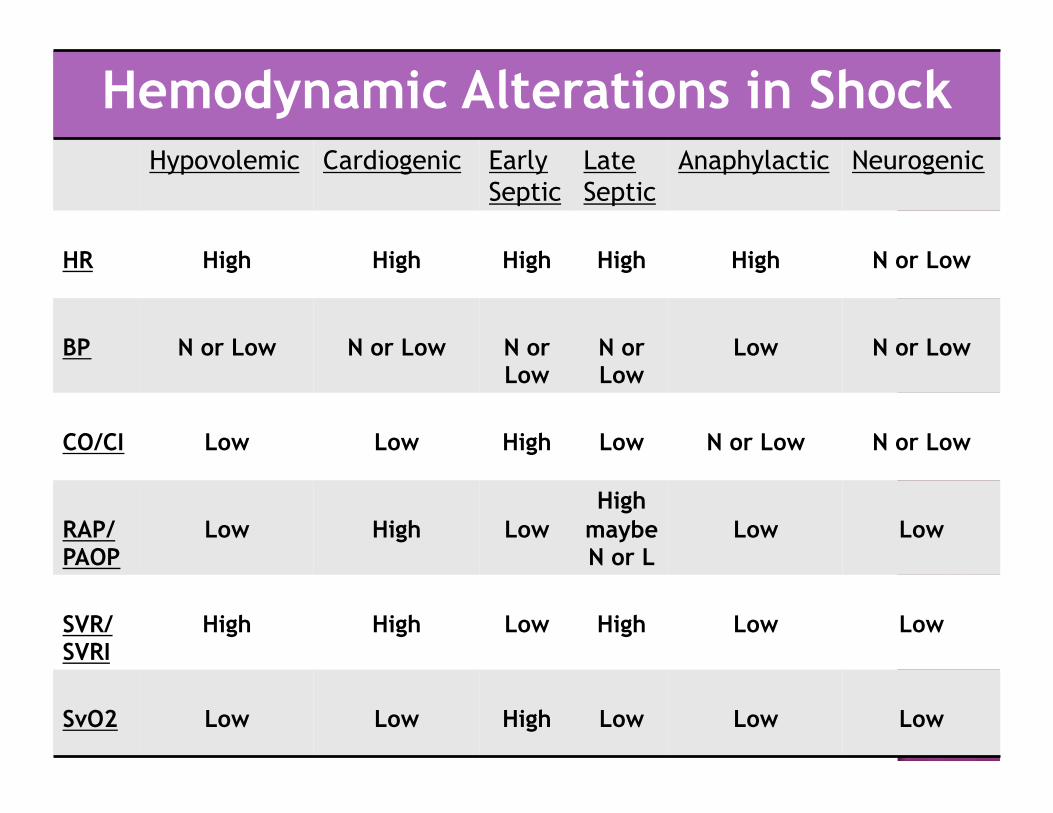
Hemodynamic Alterations in Shock Hypovolemic Cardiogenic Early
Septic Late Septic
Anaphylactic Neurogenic
HR High High High High High N or Low
BP N or Low N or Low N or Low
N or Low
Low N or Low
CO/CI Low Low High Low N or Low N or Low
RAP/ PAOP
Low High Low High
maybe N or L
Low Low
SVR/ SVRI
High High Low High Low Low
SvO2 Low Low High Low Low Low
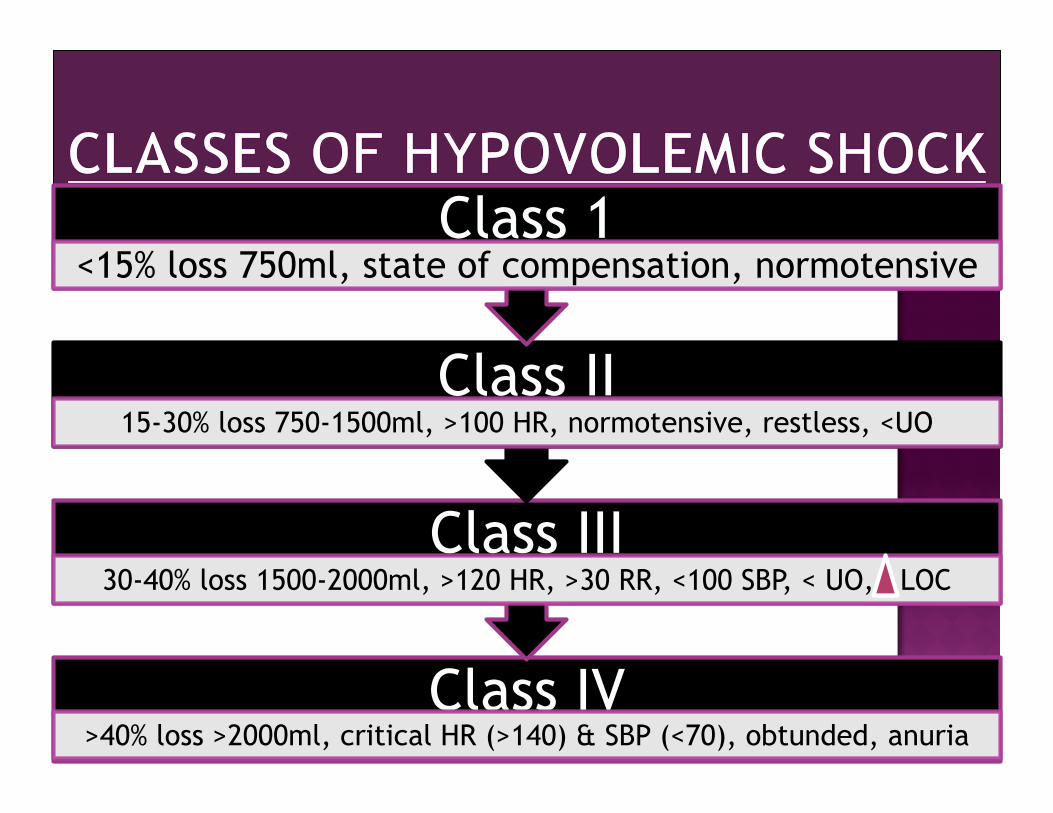
Class IV >40% loss >2000ml, critical HR (>140) & SBP (<70), obtunded, anuria
Class III 30-40% loss 1500-2000ml, >120 HR, >30 RR, <100 SBP, < UO, LOC
Class II 15-30% loss 750-1500ml, >100 HR, normotensive, restless, <UO
Class 1 <15% loss 750ml, state of compensation, normotensive
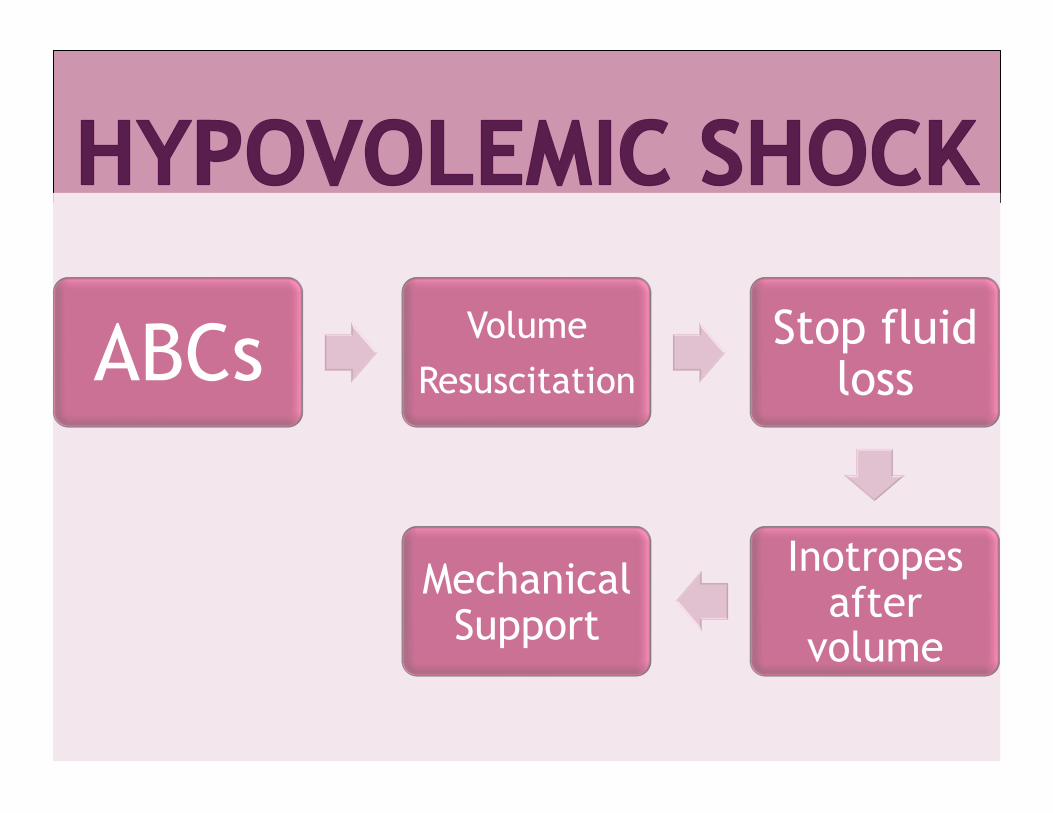
ABCs Volume Resuscitation
Stop fluid loss
Inotropes after
volume
Mechanical Support
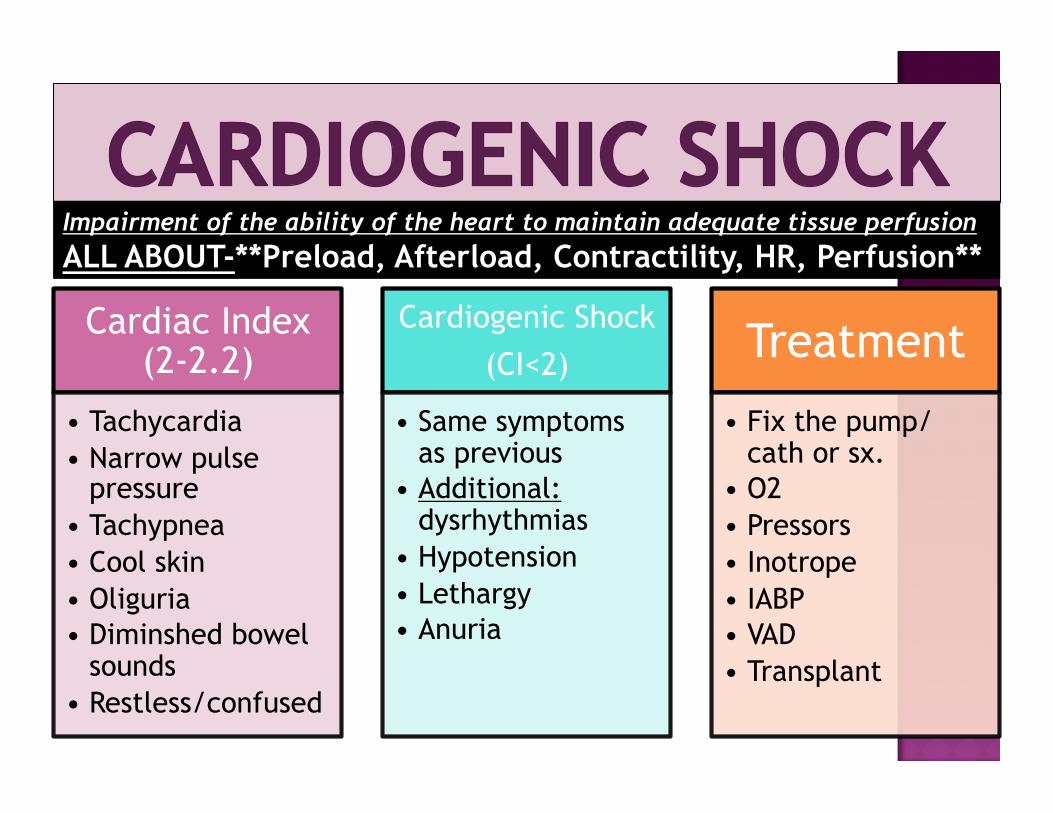
Cardiac Index (2-2.2)
• Tachycardia • Narrow pulse
pressure • Tachypnea • Cool skin • Oliguria • Diminshed bowel
sounds • Restless/confused
Cardiogenic Shock (CI<2)
• Same symptoms as previous
• Additional: dysrhythmias
• Hypotension • Lethargy • Anuria
Treatment
• Fix the pump/cath or sx.
• O2 • Pressors • Inotrope • IABP • VAD • Transplant
Impairment of the ability of the heart to maintain adequate tissue perfusion ALL ABOUT-**Preload, Afterload, Contractility, HR, Perfusion**
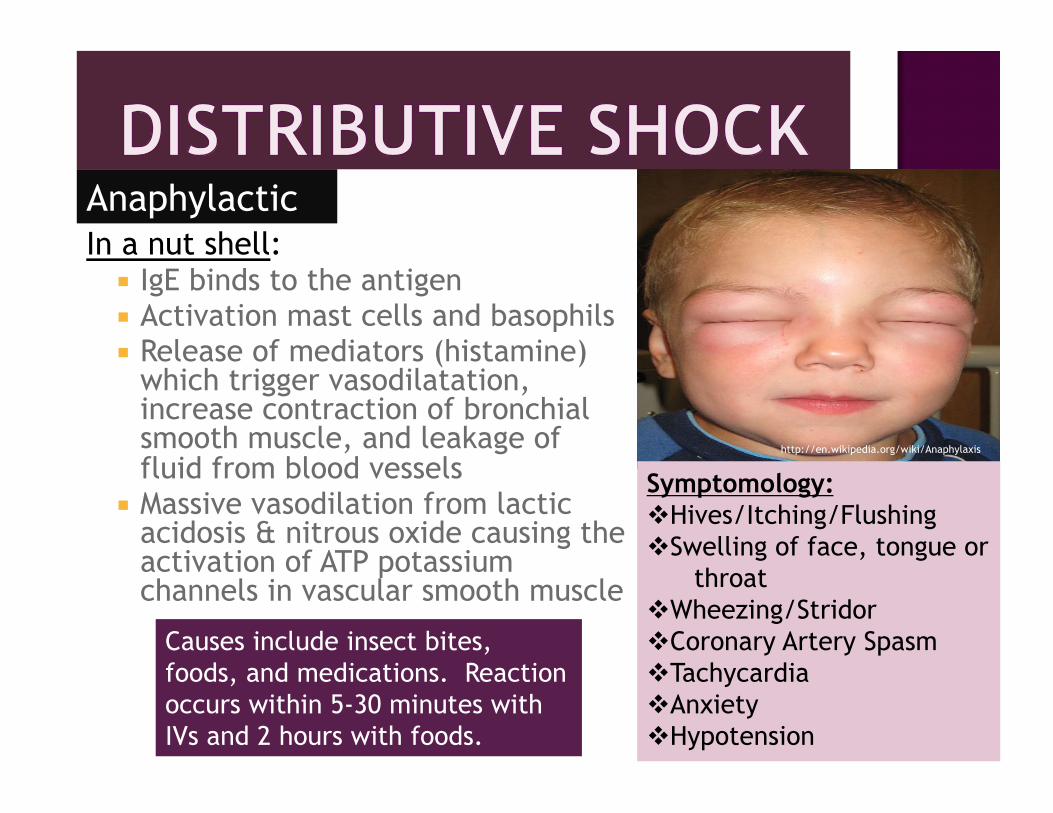
In a nut shell: IgE binds to the antigen Activation mast cells and basophils Release of mediators (histamine)
which trigger vasodilatation, increase contraction of bronchial smooth muscle, and leakage of fluid from blood vessels
Massive vasodilation from lactic acidosis & nitrous oxide causing the activation of ATP potassium channels in vascular smooth muscle
Anaphylactic
Symptomology: Hives/Itching/Flushing Swelling of face, tongue or
throat Wheezing/Stridor Coronary Artery Spasm Tachycardia Anxiety Hypotension
Causes include insect bites, foods, and medications. Reaction occurs within 5-30 minutes with IVs and 2 hours with foods.
http://en.wikipedia.org/wiki/Anaphylaxis
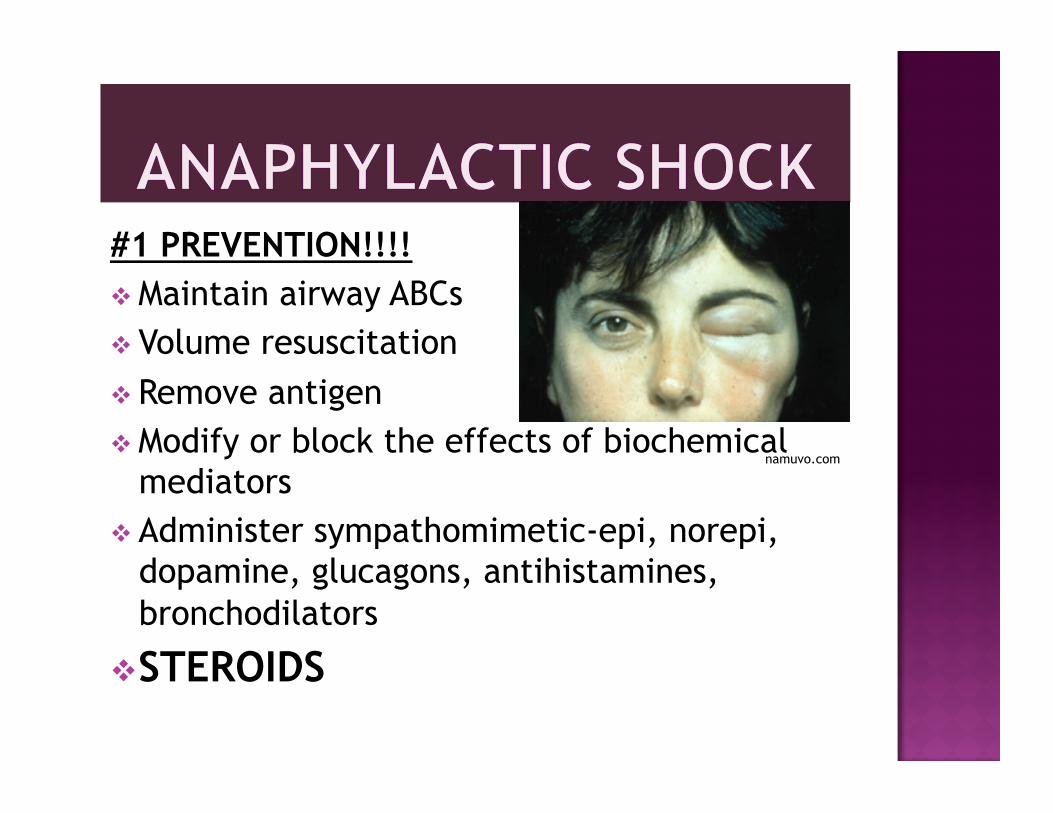
#1 PREVENTION!!!! Maintain airway ABCs Volume resuscitation Remove antigen Modify or block the effects of biochemical
mediators Administer sympathomimetic-epi, norepi,
dopamine, glucagons, antihistamines, bronchodilators
STEROIDS
namuvo.com
uic.edu
1 2
3
4
5
6
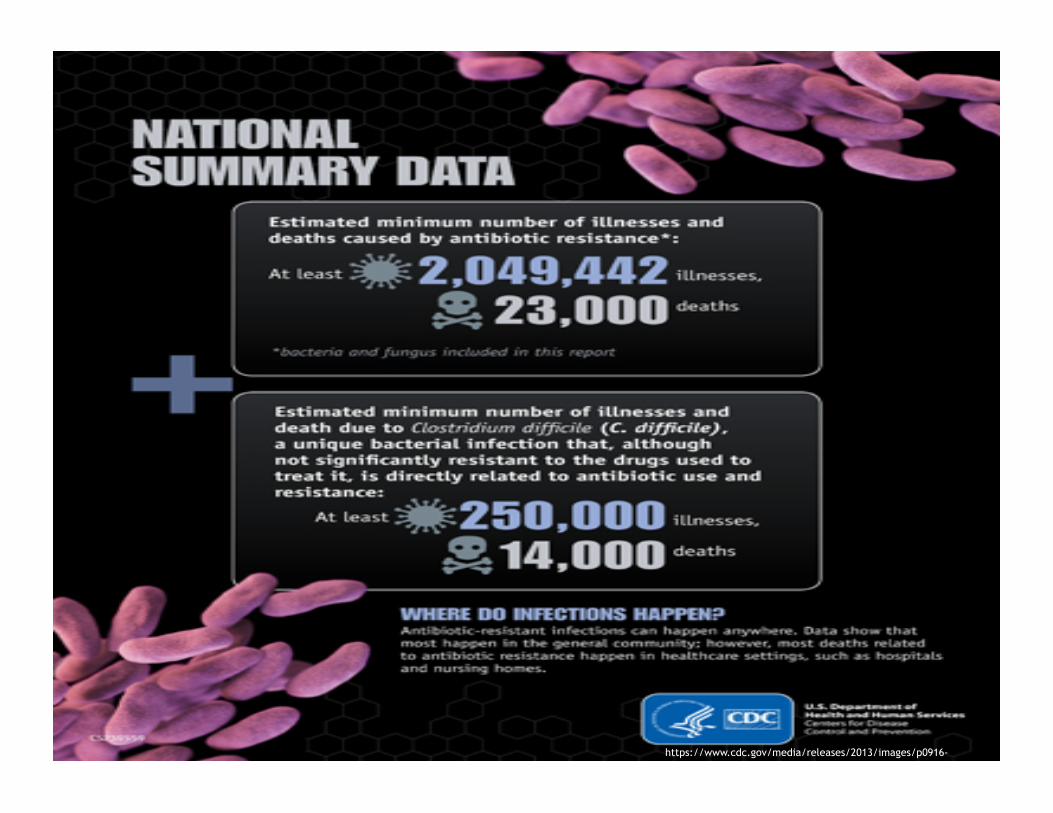
https://www.cdc.gov/media/releases/2013/images/p0916-untreatable.jpg

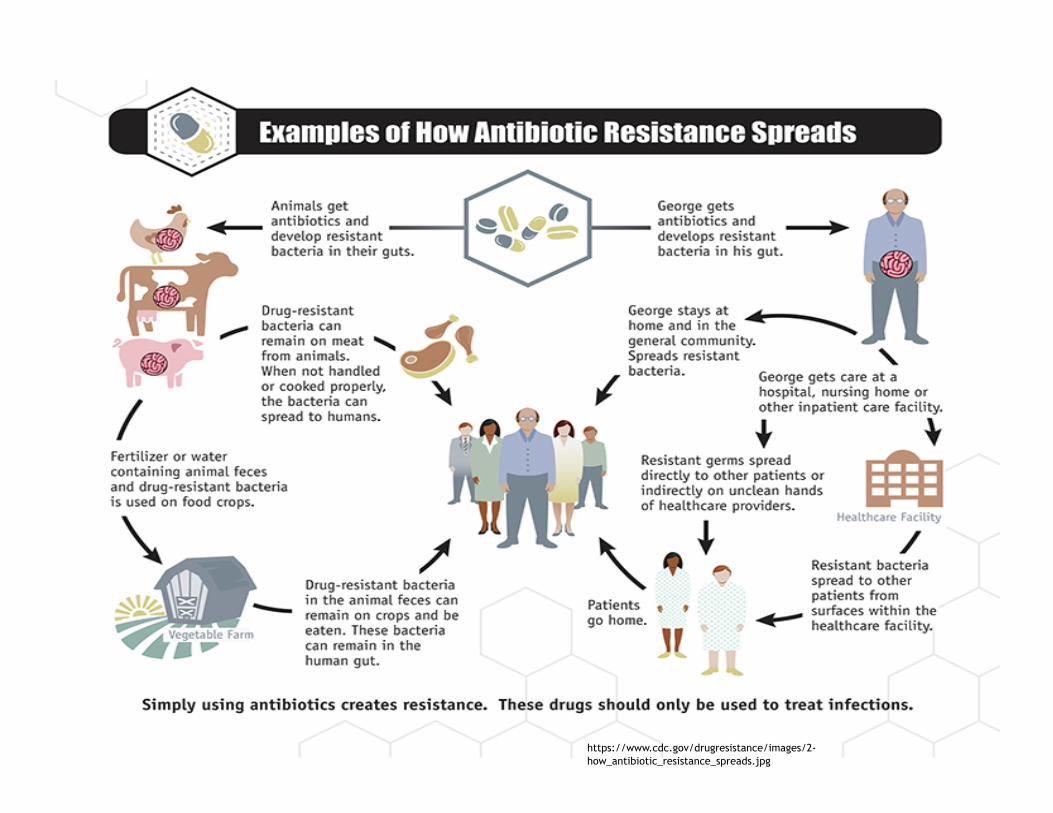
https://www.cdc.gov/drugresistance/images/2-how_antibiotic_resistance_spreads.jpg
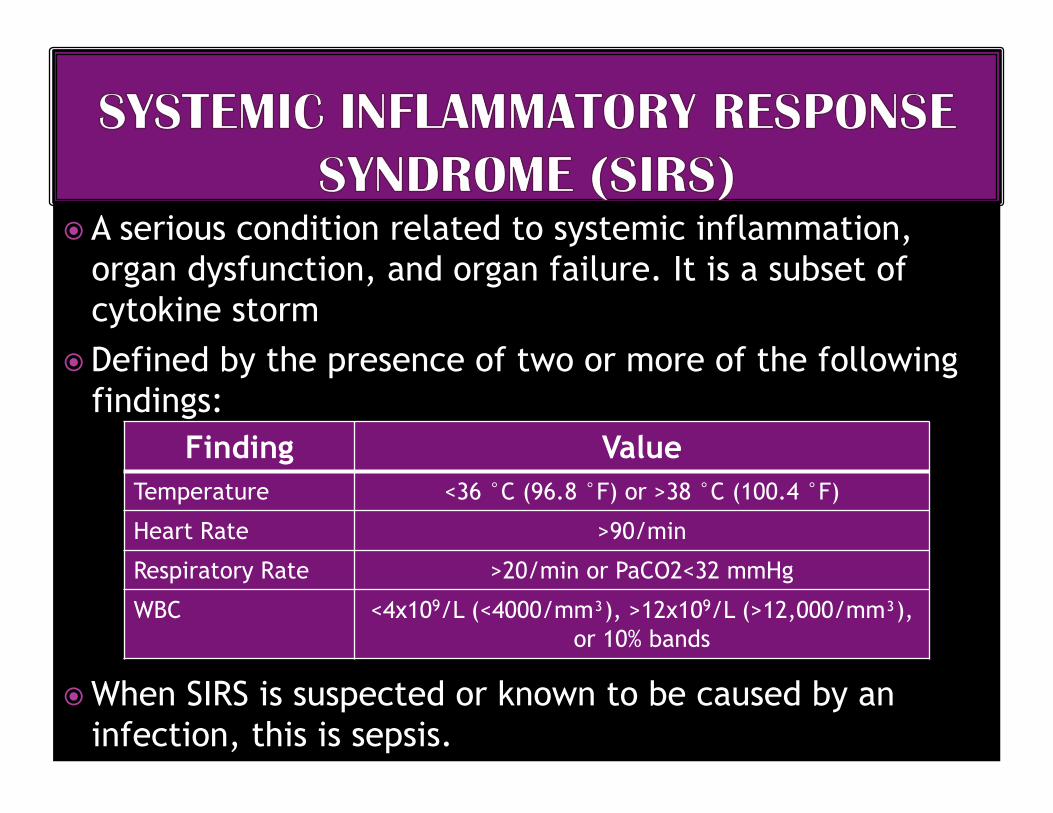
A serious condition related to systemic inflammation, organ dysfunction, and organ failure. It is a subset of cytokine storm
Defined by the presence of two or more of the following findings:
When SIRS is suspected or known to be caused by an infection, this is sepsis.
Finding Value Temperature <36 °C (96.8 °F) or >38 °C (100.4 °F)
Heart Rate >90/min
Respiratory Rate >20/min or PaCO2<32 mmHg
WBC <4x109/L (<4000/mm³), >12x109/L (>12,000/mm³), or 10% bands
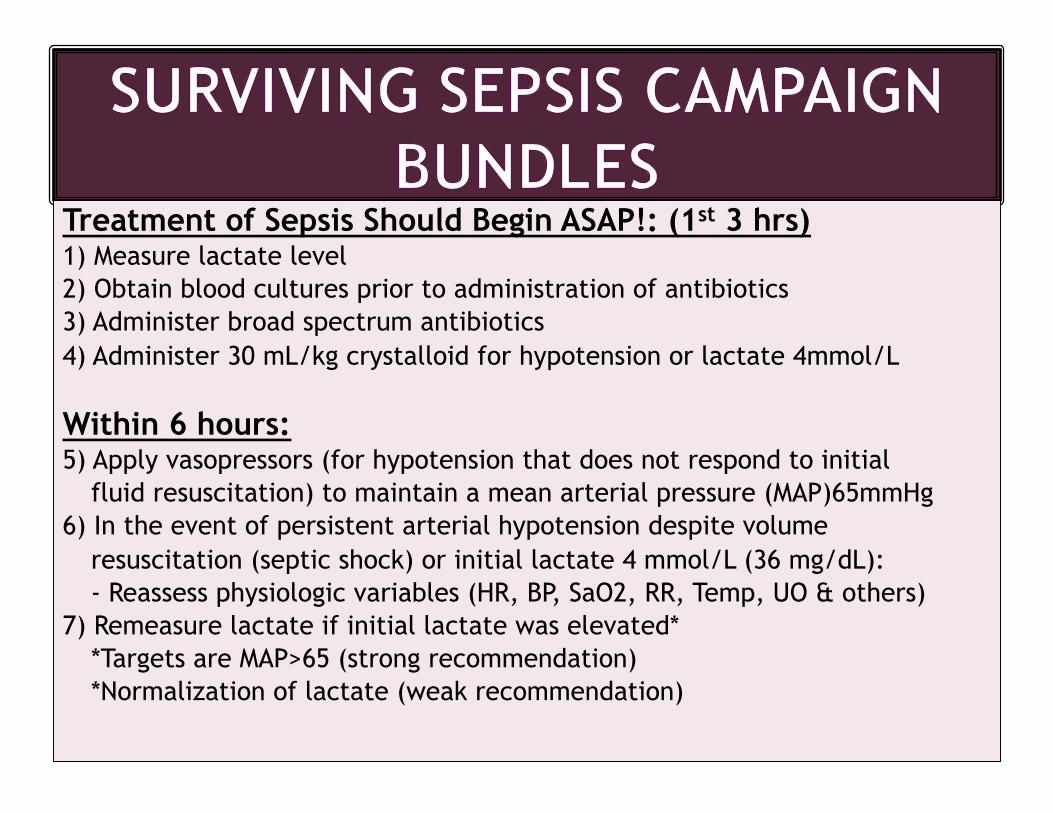
Treatment of Sepsis Should Begin ASAP!: (1st 3 hrs) 1) Measure lactate level 2) Obtain blood cultures prior to administration of antibiotics 3) Administer broad spectrum antibiotics 4) Administer 30 mL/kg crystalloid for hypotension or lactate 4mmol/L
Within 6 hours: 5) Apply vasopressors (for hypotension that does not respond to initial
fluid resuscitation) to maintain a mean arterial pressure (MAP)65mmHg 6) In the event of persistent arterial hypotension despite volume
resuscitation (septic shock) or initial lactate 4 mmol/L (36 mg/dL): - Reassess physiologic variables (HR, BP, SaO2, RR, Temp, UO & others)
7) Remeasure lactate if initial lactate was elevated* *Targets are MAP>65 (strong recommendation) *Normalization of lactate (weak recommendation)
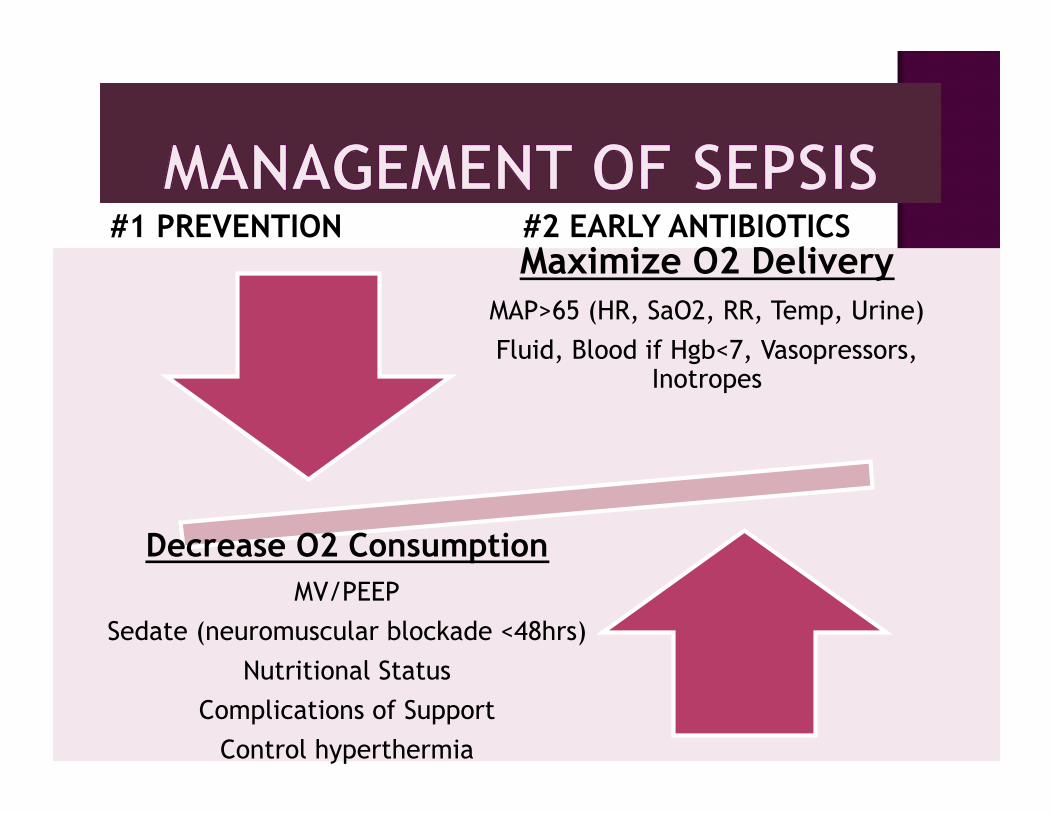
Maximize O2 Delivery MAP>65 (HR, SaO2, RR, Temp, Urine) Fluid, Blood if Hgb<7, Vasopressors,
Inotropes
Decrease O2 Consumption MV/PEEP
Sedate (neuromuscular blockade <48hrs) Nutritional Status
Complications of Support Control hyperthermia
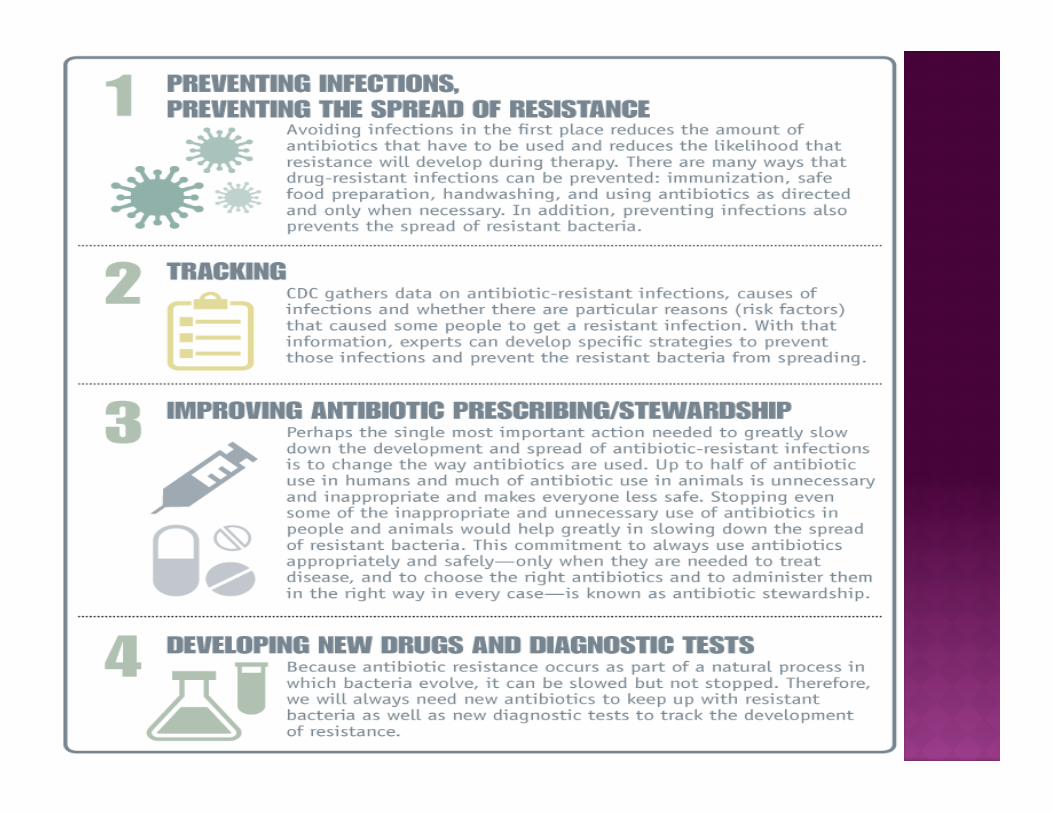
#1 PREVENTION #2 EARLY ANTIBIOTICS
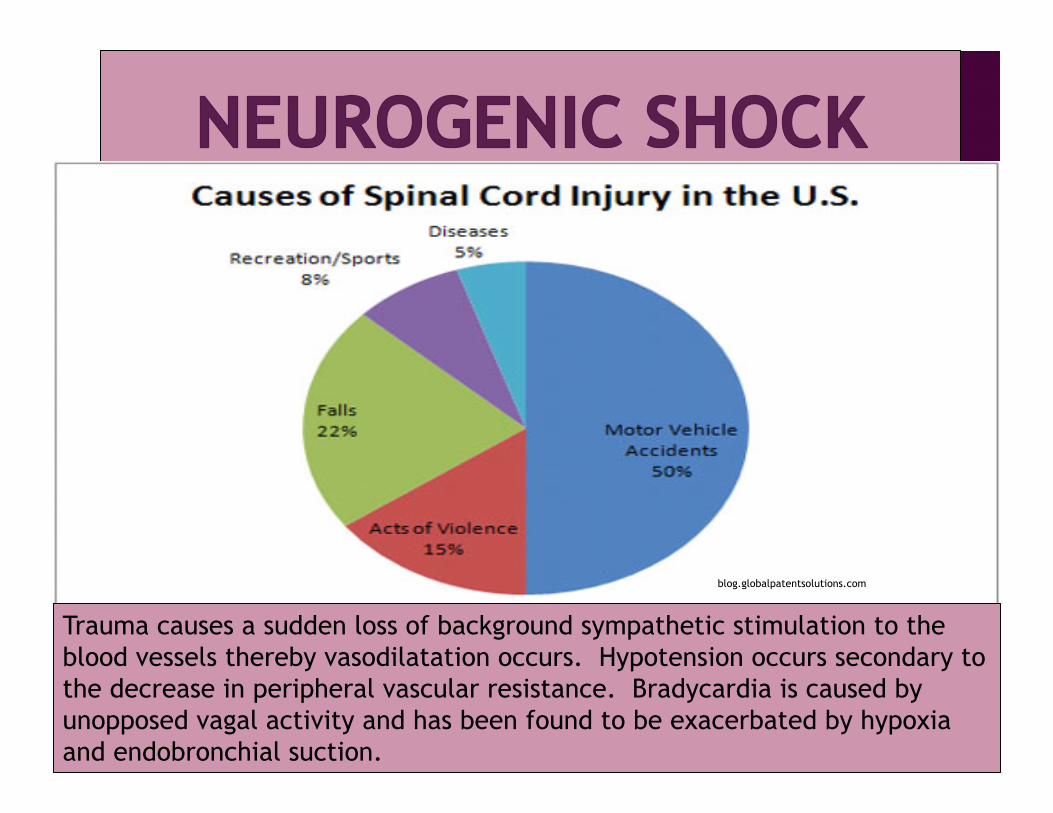
Trauma causes a sudden loss of background sympathetic stimulation to the blood vessels thereby vasodilatation occurs. Hypotension occurs secondary to the decrease in peripheral vascular resistance. Bradycardia is caused by unopposed vagal activity and has been found to be exacerbated by hypoxia and endobronchial suction.
blog.globalpatentsolutions.com
Neurogenic: ABCs Spinal Cord Immobilization Warming Measures Maintain MAP (Fluids, pressors, Dopa) Maintain HR (Atropine, PPM) Prevent venous stasis Volume Replacement Monitor for complications of shock STEROIDS?? topnews.net.nz