-
7/24/2019 Sepsis - Infeksi App Antibiotika
1/26
Sepsis Infection:
The Appropriate Antibiotics
Dr. Veronica Wiwing, SpMK
-
7/24/2019 Sepsis - Infeksi App Antibiotika
2/26
Introduction
Causes of death (RSCM, 2010)
1) SIRS & MODS 47.05%
2) Inhalation Injury 39.70%
3) Shock 30.90%
4) ARDS 26.5
5) Sepsis 23.5%
-
7/24/2019 Sepsis - Infeksi App Antibiotika
3/26
Introduction
Sepsis @ causa Infection
1) Contributing factors
a) Predisposing:
b) Precipitating: Immunocompromise2) Port dentree
a) Wound infection
b) Bacterial translocation
c) Instrumentation
-
7/24/2019 Sepsis - Infeksi App Antibiotika
4/26
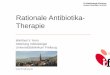
The concept of SIRS & MODS
SIRS
Infection
BacterimiaViremia
Parasytemia
Fungemia
T r a u m a
B u r n
Ischemia
Pancreatitis
Sepsis
Diagram: the concept of SIRS and sepsis
Baue, AE, Faist, E, Fry, ED. Multiple organ failure,
pathophysiology, prevention, and therapy. New York : Springer,
2000.
-
7/24/2019 Sepsis - Infeksi App Antibiotika
5/26
The concept of SIRS & MODS
SIRSsystemic Inflammatory response syndrome
SepsisSIRS due to objective (laboratory evidenced)
of infection: bacteremia (toxemia)
MODS
multi system organ dysfunction syndrome(previously: multiple
organ failure)
2 or more organs involved
Baue, AE, Faist, E, Fry, ED. Multiple organ failure,
pathophysiology, prevention, and therapy. New York : Springer,
2000.
-
7/24/2019 Sepsis - Infeksi App Antibiotika
6/26
The concept of SIRS & MODS
Shocklack of perfusion
Septic shocksepsiswith hypotension despite adequate
fluid resuscitation
Severe Sepsissepsisassociated with organ dysfunction
Baue, AE, Faist, E, Fry, ED. Multiple organ failure,
pathophysiology, prevention, and therapy. New York : Springer,
2000.
-
7/24/2019 Sepsis - Infeksi App Antibiotika
7/26
Predisposing
Precipitating
Local effect of Anti
Inflammatory response
Localeffect of Pro
Inflammatory response
Cardiovascular
compromised
Equal CARS-SIRS
Homeostasis Apoptosis
SIRS Predominant SIRS Predominant
Organ
dysfunction CARS Dominant
immune
Suppression
C H A O SCARS Compensatory Anti-inflammatory Response Syndrome
MARS Mixed Antagonistic Response Syndrome
Pro Inflammatory response
enter the systemiccirculation
Anti Inflammatory response
enter the systemiccirculation
SIRS Predominant
Systemic Response
CARS
MARS
SIRS
Diagram the cascade of SIRS
-
7/24/2019 Sepsis - Infeksi App Antibiotika
8/26
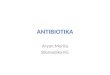
Exaggerated response
Tissue injury SIRS
Immunere
sponsetoinjury
time
recruitmentneutrophil
arachidonic acid production
free radicals
anti-inflammatorypro-inflammatory
compensation
3-5 days
5-21 days
The diagram of the nature of SIRSwith the host immune response
to injury point of view
The concept of SIRS & MODS
(ARDS)
32 days
CARS
immunosuppressive
-
7/24/2019 Sepsis - Infeksi App Antibiotika
9/26
The concept of SIRS & MODS
Predisposing factors:
Host / Injury ex : burns devastating injury /
Management (early, advanced)
Precipitating factors (Initiation):
Epithelial damage:
Endothelial (capillary permeability)
Mucosa (disrupted airway mucosa, gut mucosal
disruption, acute tubular necrosis, etc)
Skin-soft tissue necrosis: eschar
-
7/24/2019 Sepsis - Infeksi App Antibiotika
10/26
-
7/24/2019 Sepsis - Infeksi App Antibiotika
11/26
Infection @ causa burns injury
Host defence Immunosuppresion
Epithelial damage
Port dentre:
Wound infection
Bacterial translocation
Instrumentation
Defenceaggressor homeostasis
-
7/24/2019 Sepsis - Infeksi App Antibiotika
12/26
Bacterial Translocation
Splanchnic hypoperfusion lead to ischaemic and
mucosal disruption (epithelialdamage) Altered gut mucosal and
intraluminal environment due
to:
Fasting the injured pts
The use of Antacids The use of certain Antimicrobial
-
7/24/2019 Sepsis - Infeksi App Antibiotika
13/26
Instrumentation
Disobeyed a and antiseptic handling in procedure of
insertion and maintenance of: Endotracheal tube, tracheostomy
tube, suction catheter,
etc
IV lines, CVP lines, syringes
Indwelling catheter Wound management
-
7/24/2019 Sepsis - Infeksi App Antibiotika
14/26
Wound infection
Non vital tissue (eschar)
Tissue perfusion Wound degradation
Microorganism: >105/mm3, virulence
Pro-inflammatory Mediators
Immune system suppression
-
7/24/2019 Sepsis - Infeksi App Antibiotika
15/26
1. Prevention the development
2. Breaking the cascade
In dealing with SIRS, sepsis and MODS, the treatment
should be:
Listen to what the cells say
The strategy
The management
-
7/24/2019 Sepsis - Infeksi App Antibiotika
16/26
The management
Bacterial translocation
The fluid resuscitation:
Adequate volume replacement regarding ischaemic
time (gut mocosa: 4 hrs) Peripheral vasodilator (low dose
dopamine)
Gut resuscitation:
No fasting but early enteral nutrition (when the gutworks: use
it! to feed the gut rather than to feed the
body) No antacids and H2antagonist
No local antibiotics, no an-aerob antibiotics
No prophylactic antibiotic is needed
-
7/24/2019 Sepsis - Infeksi App Antibiotika
17/26
The management
Instrumentation
Aseptic procedure supported with appropriate antiseptic
Everything is single use only No prophylactic antibiotic is
needed
-
7/24/2019 Sepsis - Infeksi App Antibiotika
18/26
The management
Wound infection
Wound cleaning with dressing
moist dressing for 48 hrs (prevent the wounddegradation)
Early excision:
Tangential excision (necrotomy) followed by
(immediate) skin grafting
-
7/24/2019 Sepsis - Infeksi App Antibiotika
19/26
The management
Wound infection (cont)
Haemodynamic stability Limitations:
Manpower (skill), Facilities, donor
Impending SIRS & MODS
The needs for supportive antibiotics
Problems:
-
7/24/2019 Sepsis - Infeksi App Antibiotika
20/26
The use of antimicrobial
The rational use of antibiotics:
Standard : class I level of evidence
Guidelines : class II level of evidence
Options : class III level of evidence
-
7/24/2019 Sepsis - Infeksi App Antibiotika
21/26
The use of antimicrobialGuidelines
Systemic and topical antibiotics:
Sterile wound
48hr 5 - 7 day
Gram positive mo Gram negative mo
The wound colonization
Shock phase Second phaseImmune-compromize
-
7/24/2019 Sepsis - Infeksi App Antibiotika
22/26
The use of antimicrobialGuidelines
Systemic and topical antibiotics should be avoided :
Antibiotic which is cyto-toxic (visceral organs and
wounds) Antibiotic interfering the gut normal flora balance.
Potent antibiotic killing commensal non patogen
bacteria.
Refer to general guidelines.
-
7/24/2019 Sepsis - Infeksi App Antibiotika
23/26
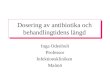
Amos F, Grochowski J, Tongol MAS. MIMS antimicrobial guides
Indonesia.Singapore: MediMedia Asia. PTE.Ltd.; I(1); 2002
Burns
Common pathogen:
Streptococcus
pyogenes
Enterobacter sp
Staphylococcus
aureusPseudomonas
aurugenosa
Enterococcus sp
Aeromonas
Vancomycin 1g IV bid
&
Amikacin 10mg/kg IV initial,
& 7.5mg/kg IV bid
Piperacillin or 4g IV qid
Ceftazidim 500mg-2g IV 8-12hror
Meropenem (single) 500mg-1g IV tid
Imipenem (single) 500mg-1g tid-qid
Common pathogen:
Streptococcus sp
Topical antibioticswith oral:Silver nitrate 0.5% Moist dressing
2hr
Mafenide acetate cr apply 2-3 times/day
Silver sulfadiazine 1%cr apply 2-3 times/day
Fusidic acid 2% cr/oint apply 2 times/day
Mupirocin 2% cr apply 2 times/day
Penicillins:
Penicillin V 1-2g/day PO devided
dose qid
Penicillin G 2-3 MU IV / 4hr
Macrolides:
Erythromycin 1-2g/day PO devided
dose qid
Wound
sepsis
Cellulitis
-
7/24/2019 Sepsis - Infeksi App Antibiotika
24/26
The use of antimicrobialGuidelines
Systemic antibiotics:
Sterile wound
48hr 5 - 7 day
Gram positive mo Gram negative mo
Penicillin (V or G)
Penicillinase resistant
Vancomycin
Avoids:
Carbapenem
ImipenemAminoglycosides
According to mo
succeptibility
No antibiotics
-
7/24/2019 Sepsis - Infeksi App Antibiotika
25/26
Conclusion(s)
Guideline for using antibiotic in burns
Effectiveness, non toxic to visceral organs as well aswound
No ideal antibiotic
The use of antibiotic
is a kind of supportive treatment; accomplishment oftreatment
sequence
refer to: 1) indication, 2) timing, & 3) clinical
condition
supported by a wound biopsy (culture &
resistance,histopathology exam)
should be individual and very selective
Use your judgment
-
7/24/2019 Sepsis - Infeksi App Antibiotika
26/26
26
How to manage
this Infection ??