Embed Size (px)
Citation preview
SEPSIS 2020: HOW IS OUR VISION
R. Phillip Dellinger MD, MSc, MCCMProfessor of Medicine and Distinguished ScholarCooper Medical School of Rowan UniversityDirector Cooper Research InstituteSenior Critical Care AttendingCamden NJ USA
Objectives
2
Fluid Rx Septic Shock
ESRD and CHF
Vitamin C,Thiamineand (Steroids)
Dobutamine inSeptic Shock
( )

No Conflicts of Interest

4
Fluid Rx Septic Shock
ESRD and CHF
30 ml/kg crystalloid first 3 hrs
5
Surviving Sepsis Campaign

End Stage Renal Disease on Dialysis
Compensated Congestive Heart failure
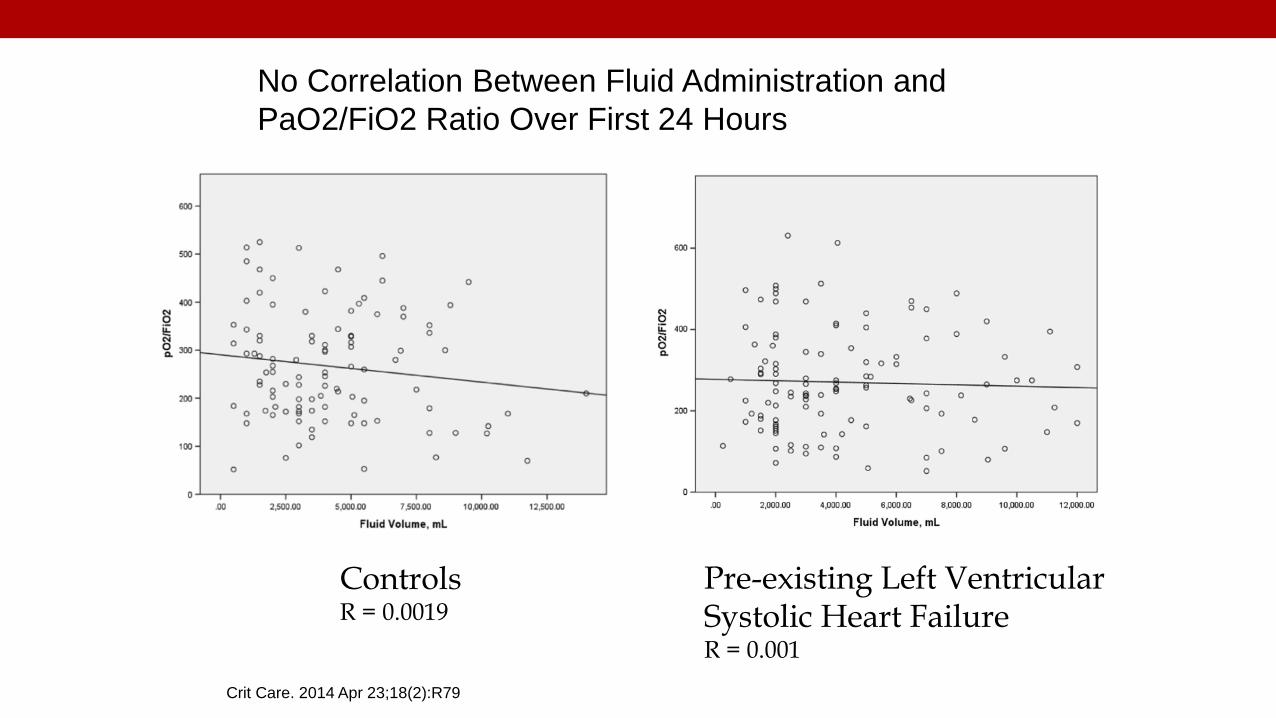
Crit Care. 2014 Apr 23;18(2):R79
No Correlation Between Fluid Administration and PaO2/FiO2 Ratio Over First 24 Hours
ControlsR = 0.0019
Pre-existing Left Ventricular Systolic Heart FailureR = 0.001


Liu et al Am J Respir Crit Care Med 2016; 193(11):1264–1270
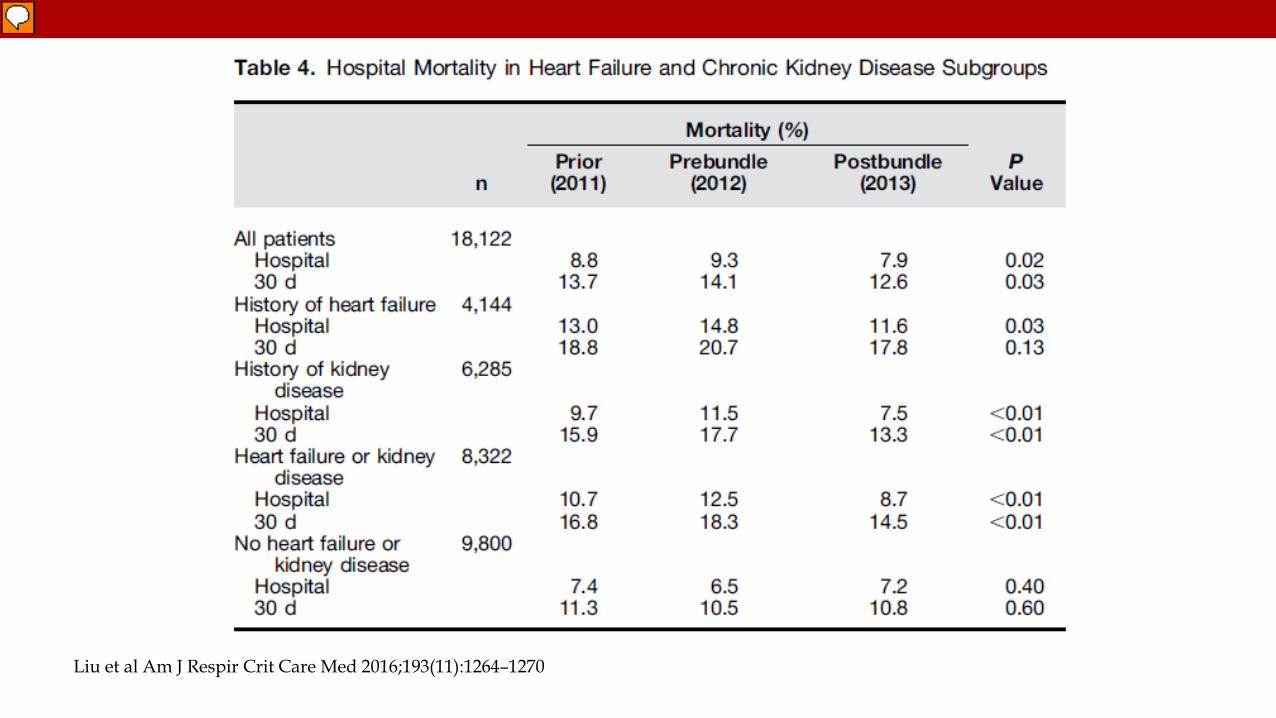
Liu et al Am J Respir Crit Care Med 2016;193(11):1264–1270
Chest. 2019 Oct 14. pii: S0012-3692(19)34013-9. doi: 10.1016/j.chest.2019.09.029
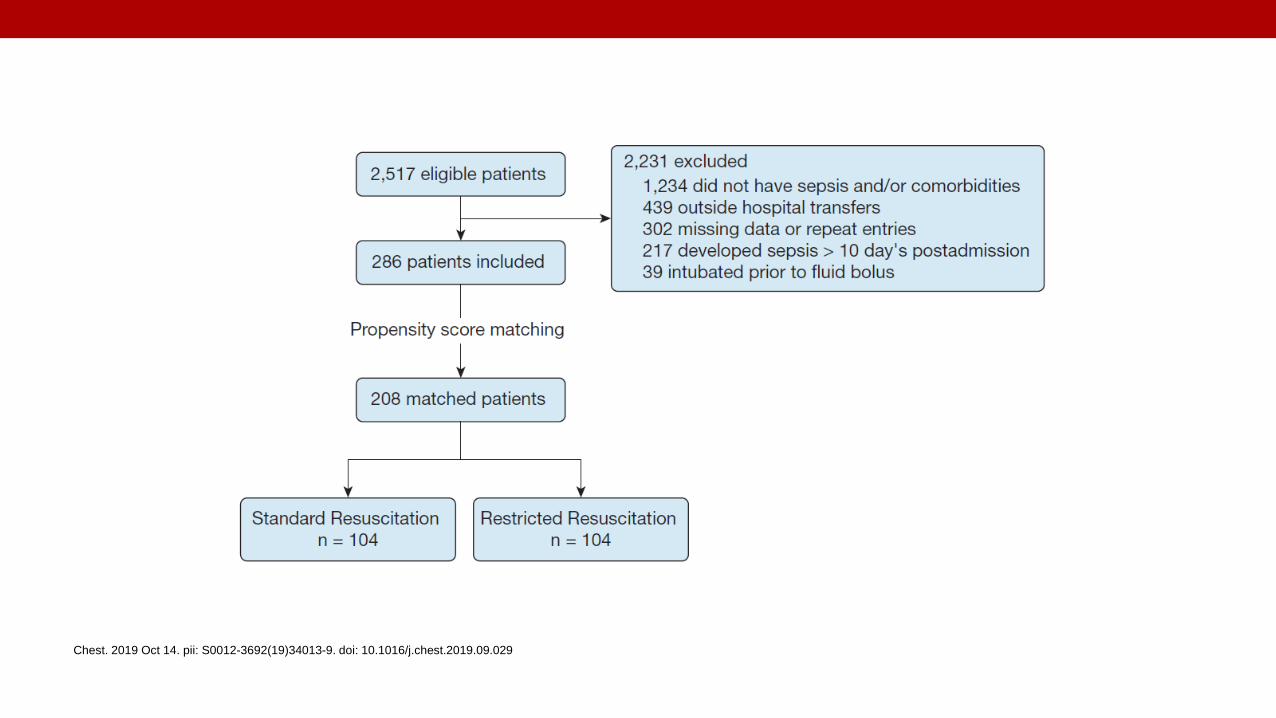
Chest. 2019 Oct 14. pii: S0012-3692(19)34013-9. doi: 10.1016/j.chest.2019.09.029
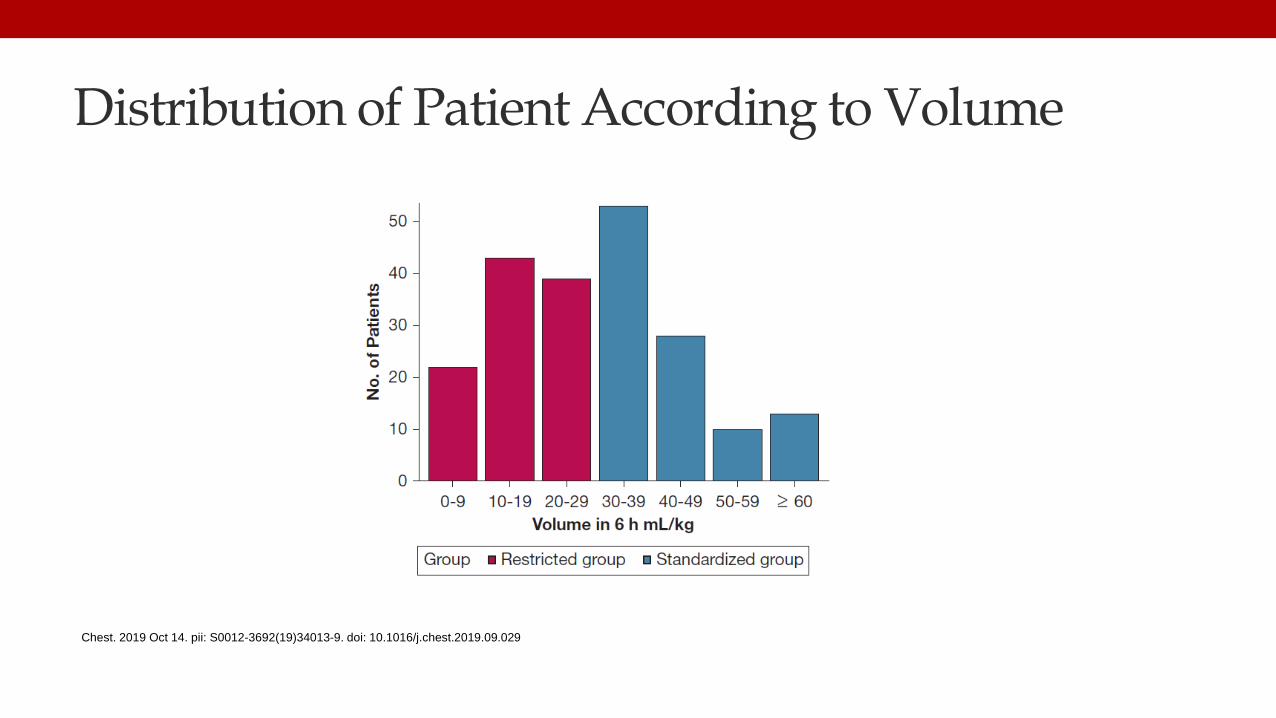
Distribution of Patient According to Volume
Chest. 2019 Oct 14. pii: S0012-3692(19)34013-9. doi: 10.1016/j.chest.2019.09.029
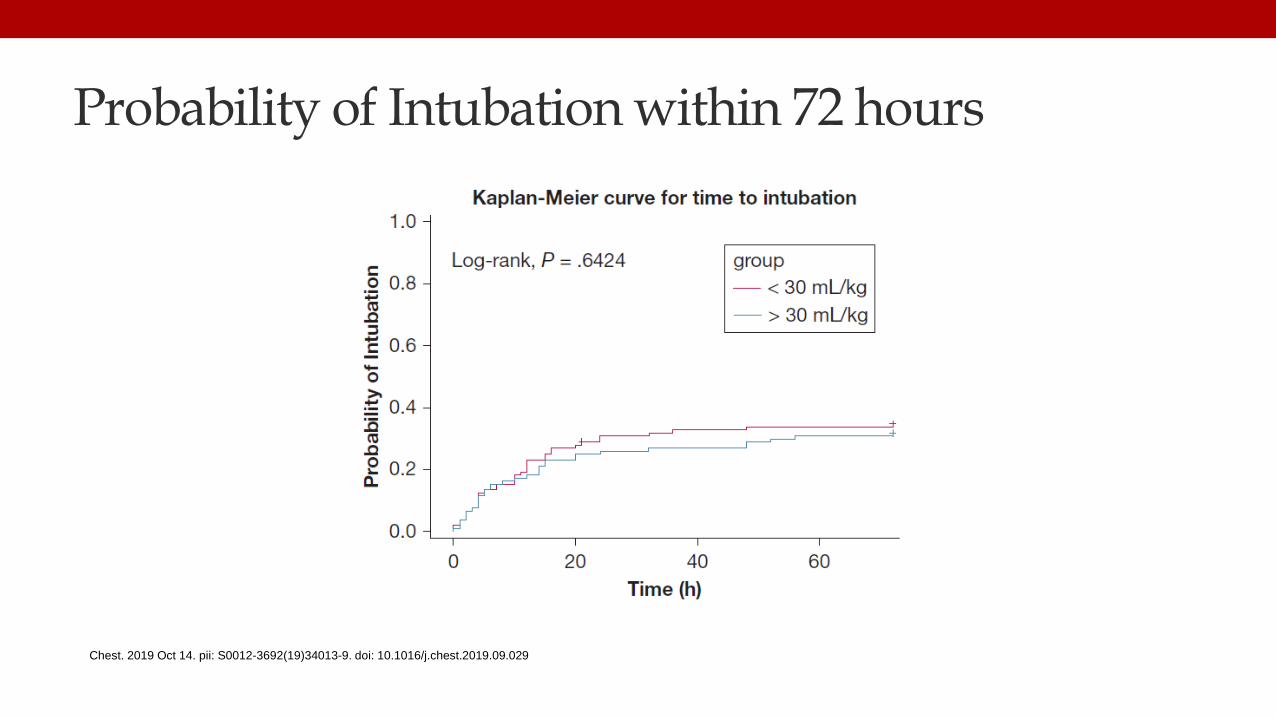
Probability of Intubation within 72 hours
Chest. 2019 Oct 14. pii: S0012-3692(19)34013-9. doi: 10.1016/j.chest.2019.09.029

17
Vitamin C, Thiamine and (Steroids)
( )
• Anti-oxidant• Reduced endothelial permeability• Improved microvascular function• Attenuated cellular apoptosis• Reduction of inflammatory mediators• Maintaining vascular vasopressor responsiveness?
Vitamin C
• Essential for generation of glutathione, an important antioxidant• Essential for aerobic respiration• Extreme thiamine deficiency syndrome, beri beri, has many of the
same characteristics of septic shock
Thiamine
Shin TG et al. J Clin Med 2019 8, 102; doi:10.3390/jcm8010102
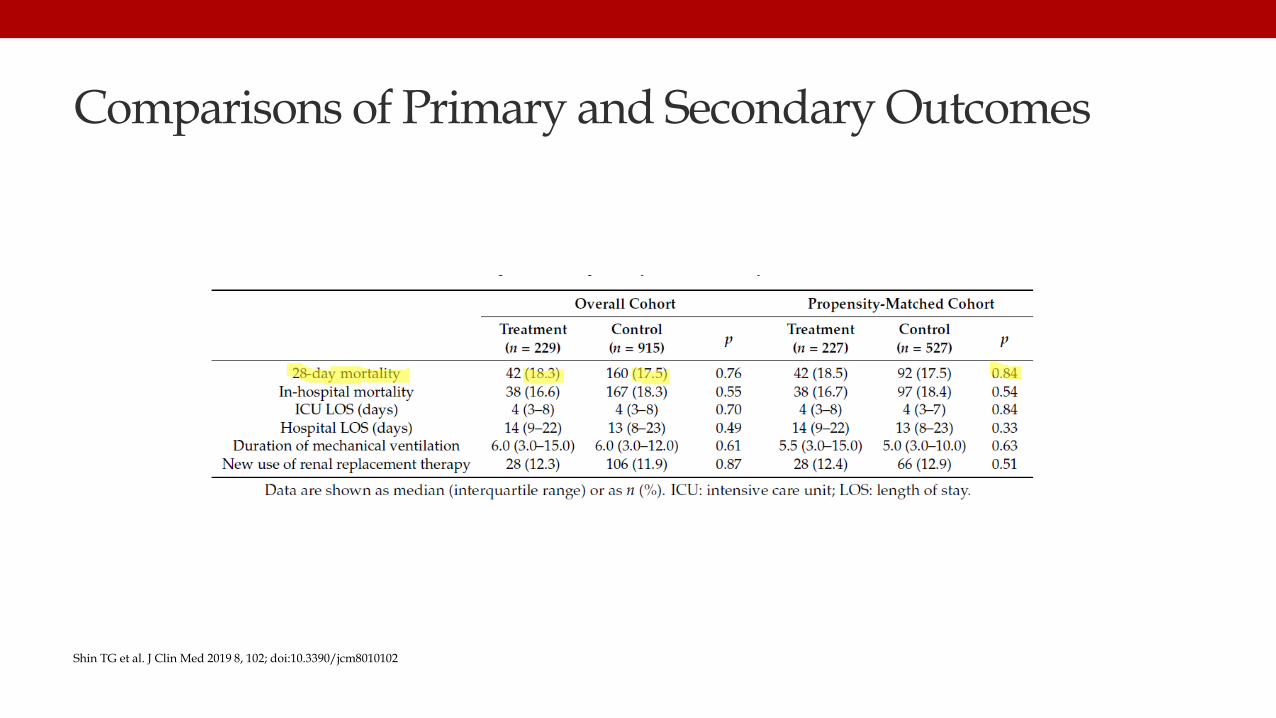
Comparisons of Primary and Secondary Outcomes
Shin TG et al. J Clin Med 2019 8, 102; doi:10.3390/jcm8010102
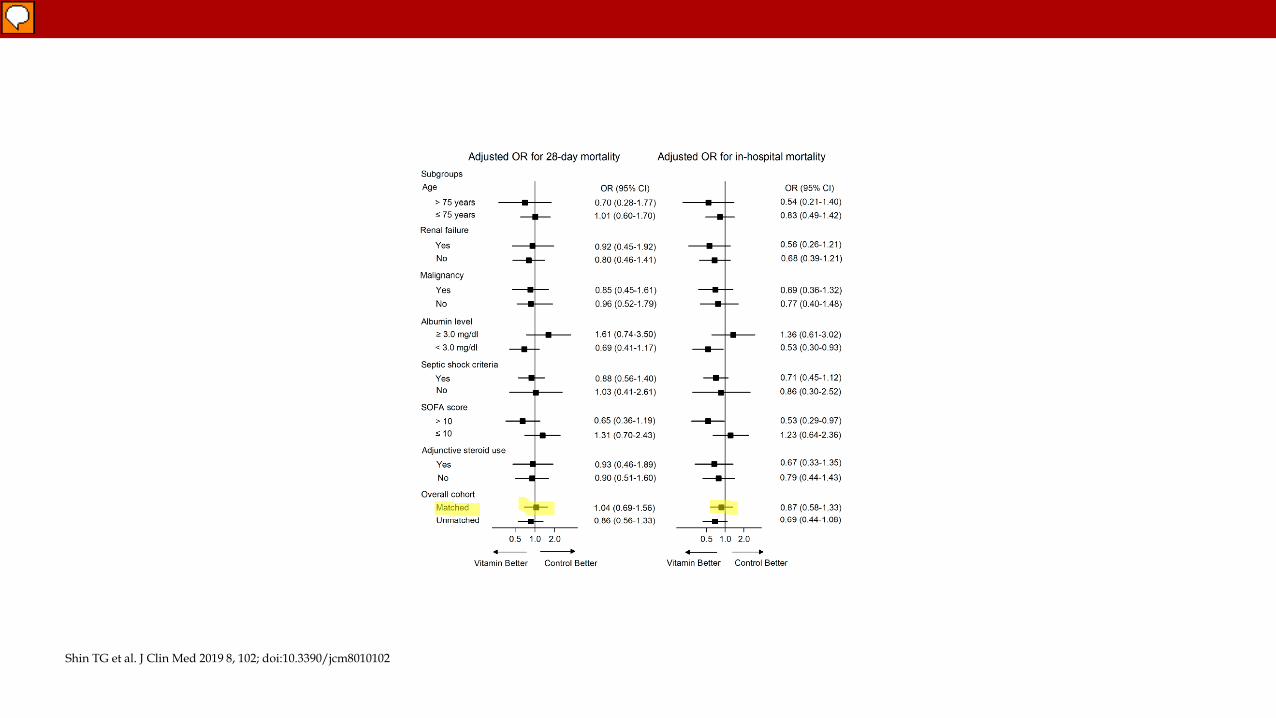
Shin TG et al. J Clin Med 2019 8, 102; doi:10.3390/jcm8010102
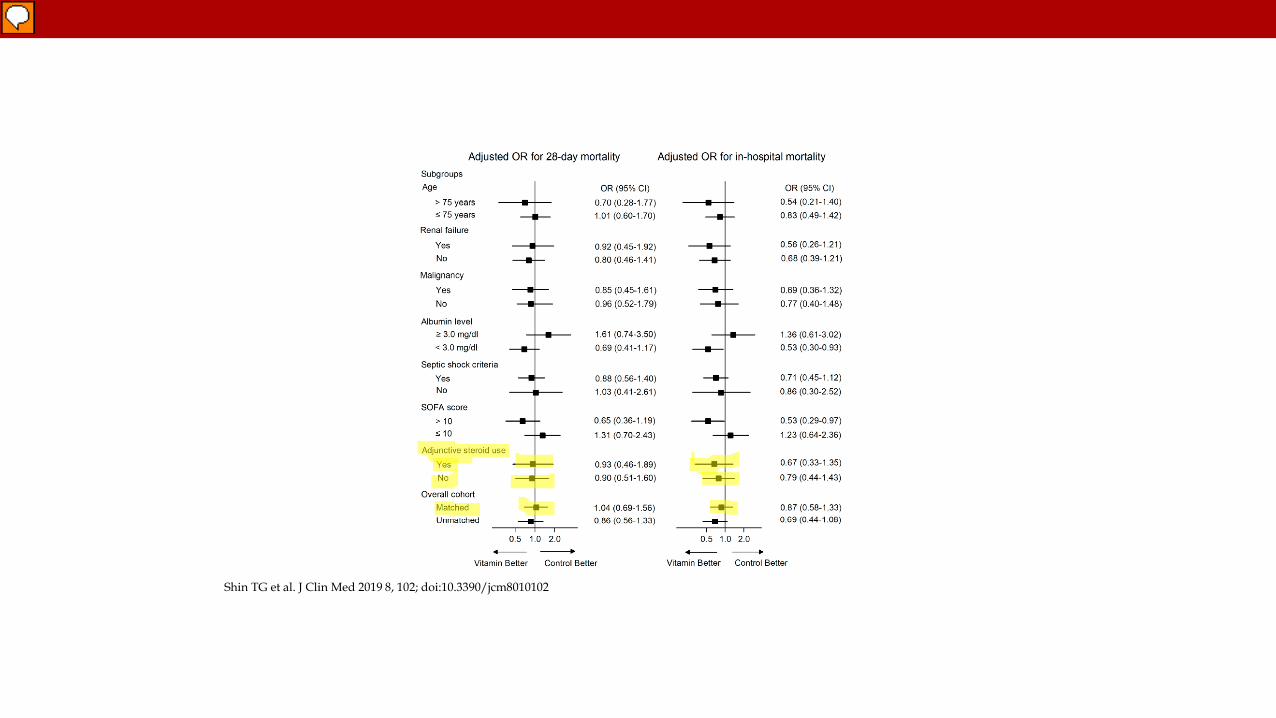
Shin TG et al. J Clin Med 2019 8, 102; doi:10.3390/jcm8010102
Mitchell AB et al. The American Journal of Medicine. 2019
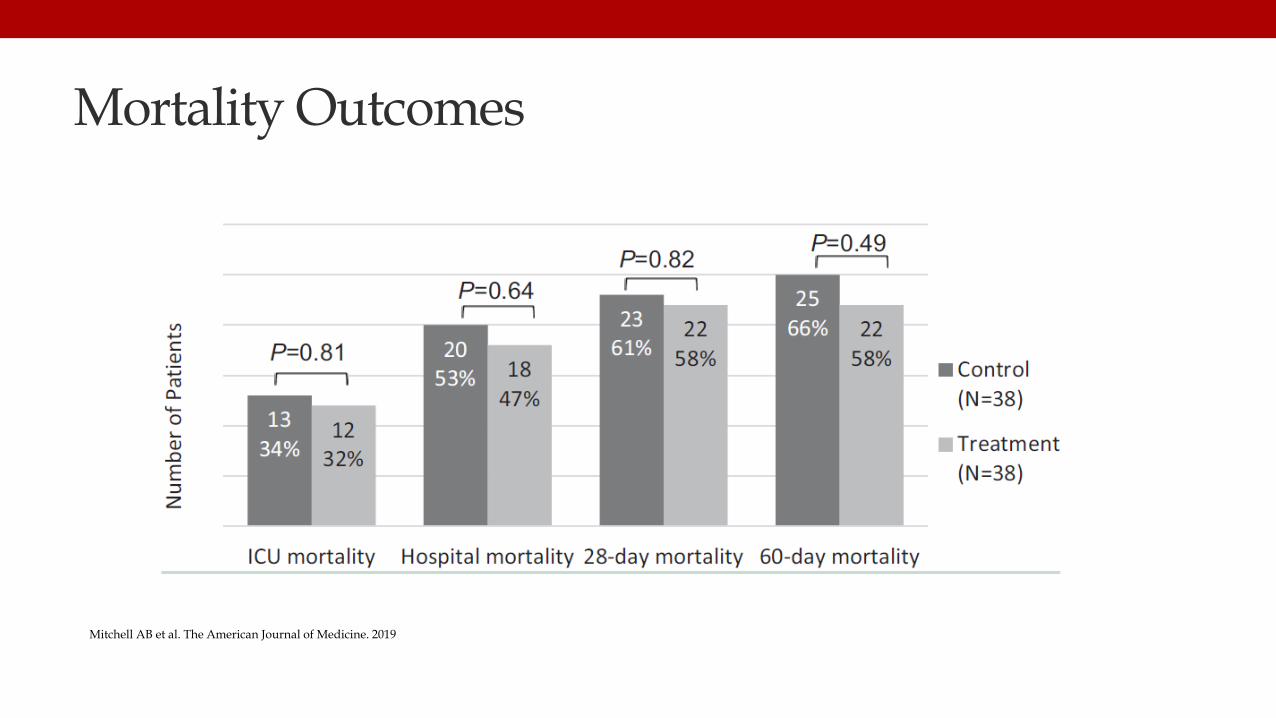
Mortality Outcomes
Mitchell AB et al. The American Journal of Medicine. 2019
Ahn JH et al. J Thorac Dis 2019; 11(4):1562-1570.
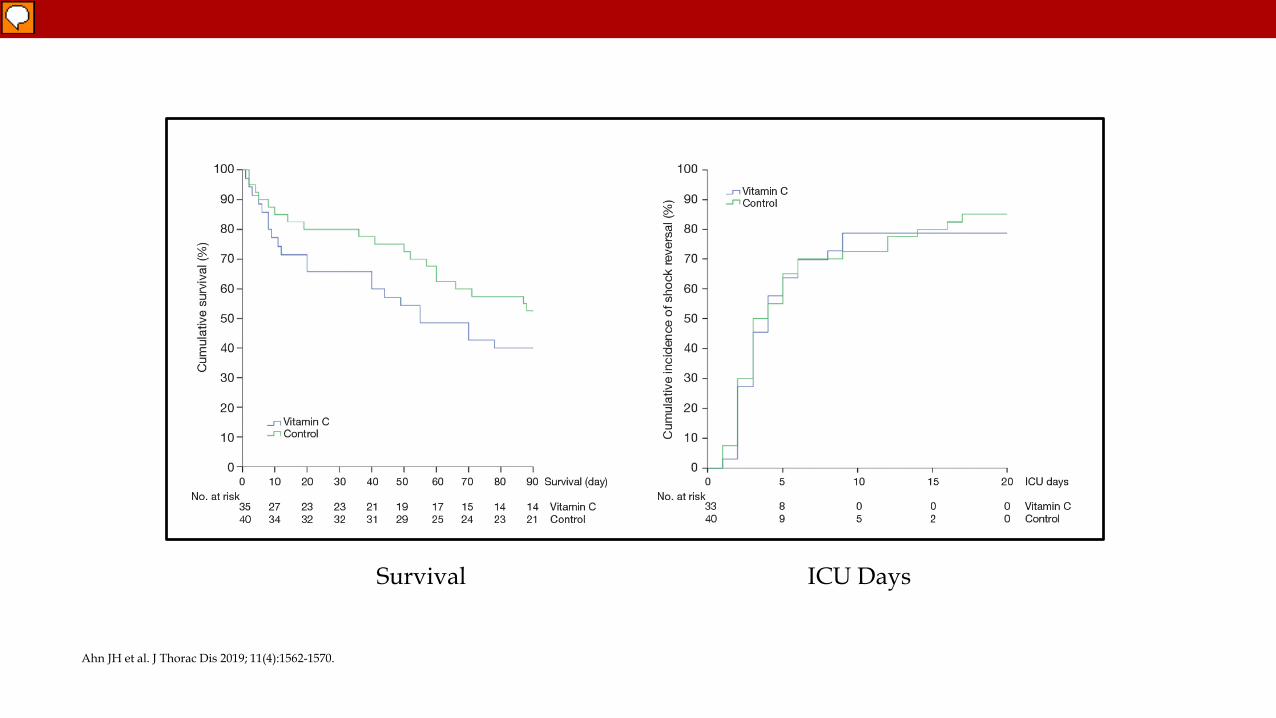
Ahn JH et al. J Thorac Dis 2019; 11(4):1562-1570.
Survival ICU Days
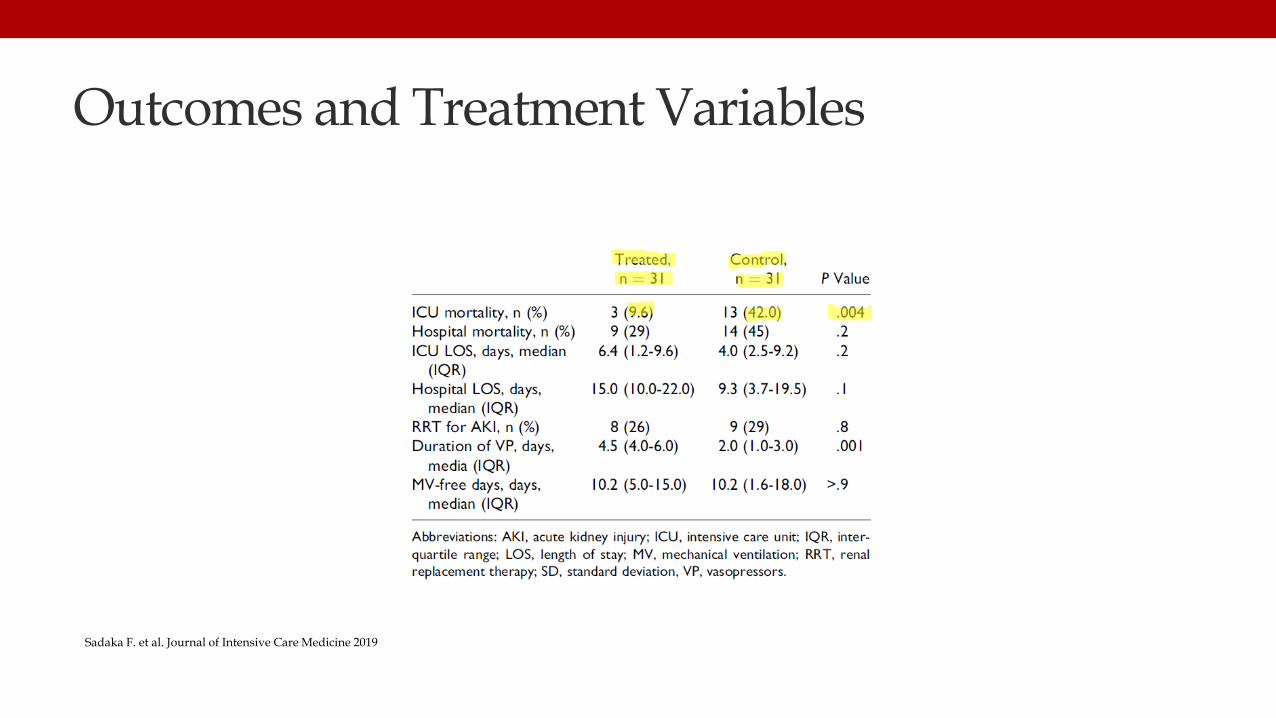
Outcomes and Treatment Variables
Sadaka F. et al. Journal of Intensive Care Medicine 2019

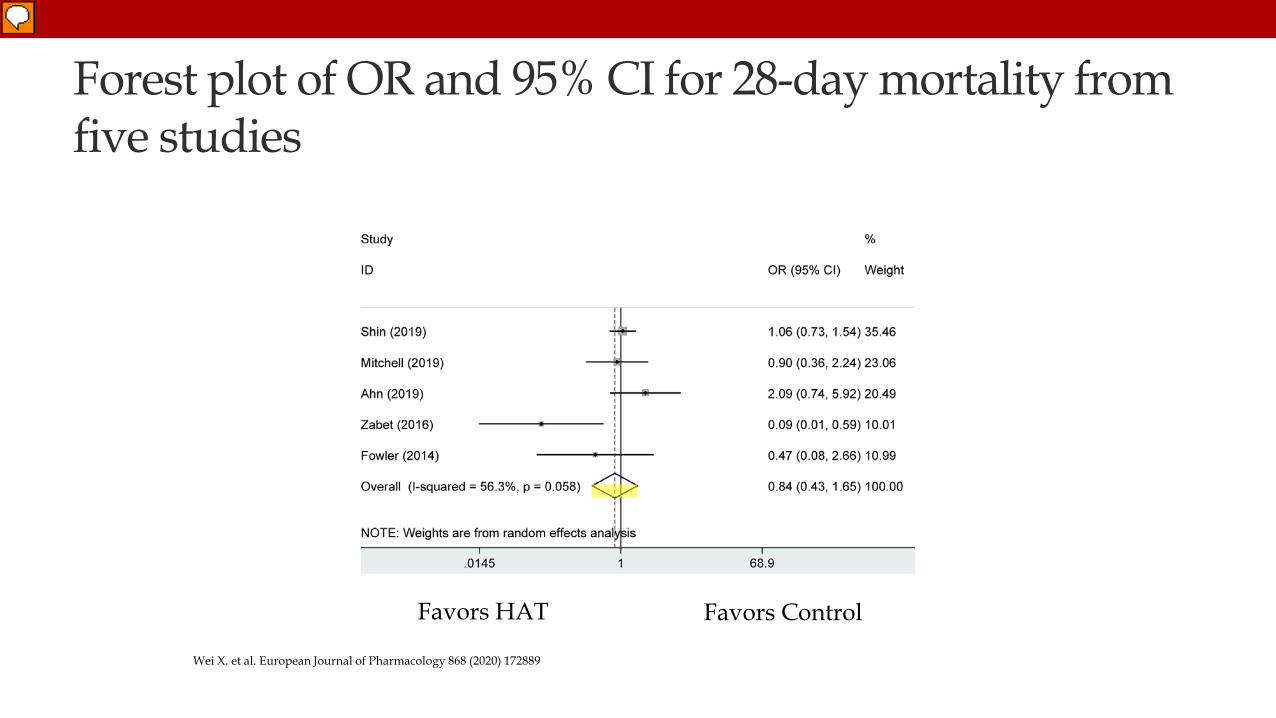
Forest plot of OR and 95% CI for 28-day mortality from five studies
Wei X. et al. European Journal of Pharmacology 868 (2020) 172889
Favors HAT Favors Control
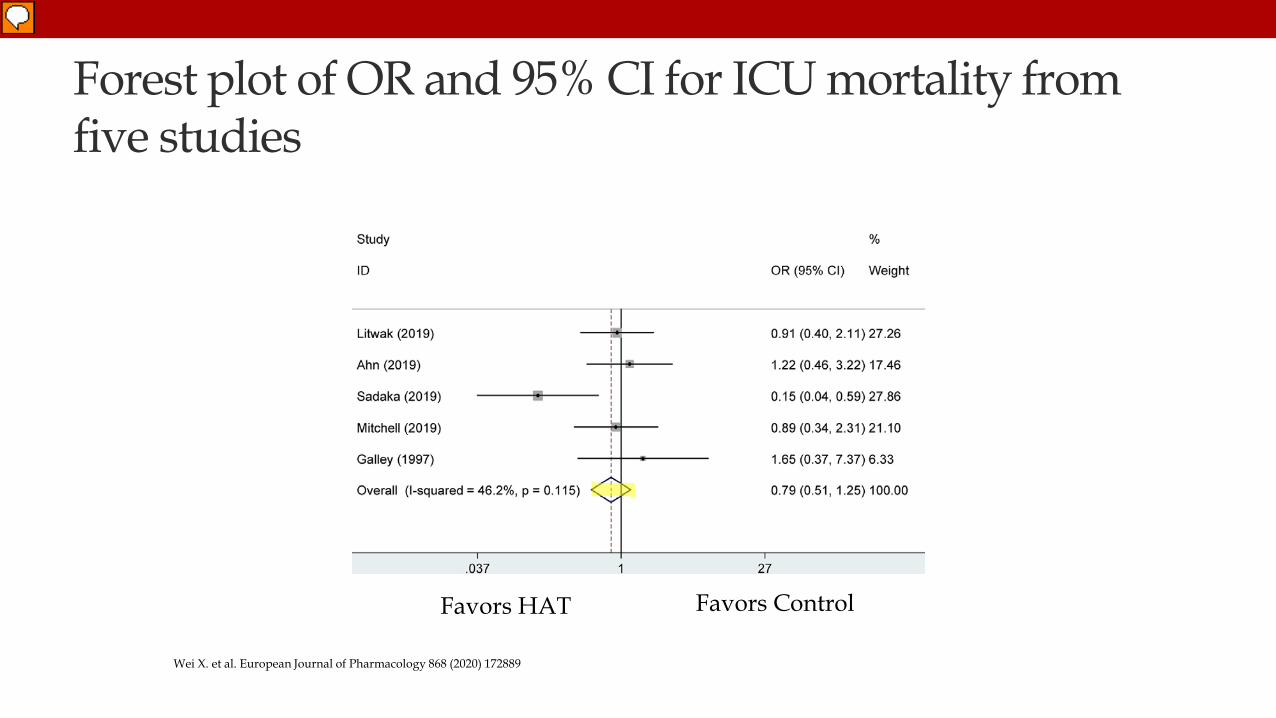
Forest plot of OR and 95% CI for ICU mortality from five studies
Wei X. et al. European Journal of Pharmacology 868 (2020) 172889
Favors HAT Favors Control
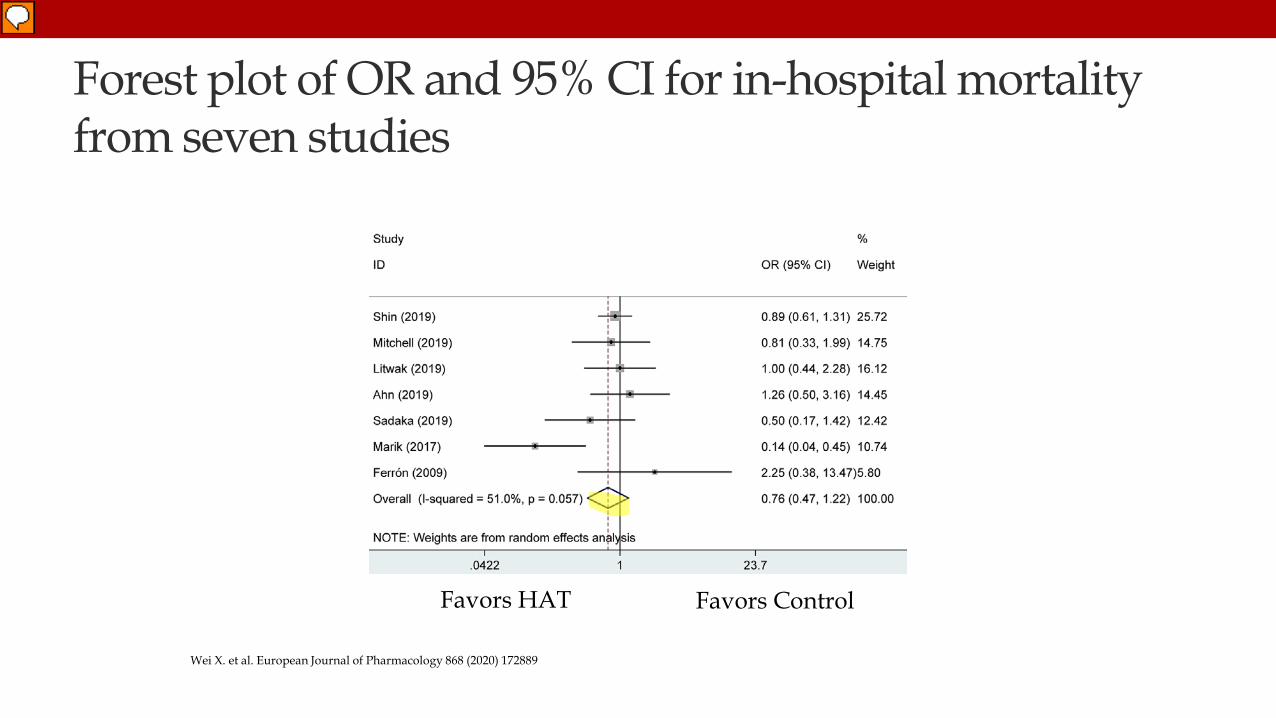
Forest plot of OR and 95% CI for in-hospital mortality from seven studies
Wei X. et al. European Journal of Pharmacology 868 (2020) 172889
Favors HAT Favors Control
Fowler AA. et al. JAMA 2019. 322 (13) :1261-1270. doi: 10.1001/jama.2019.11825.

Fowler AA. et al. JAMA 2019. 322 (13) :1261-1270. doi: 10.1001/jama.2019.11825.
Primary Endpoint Change in Modified Sequential Organ Failure Assessment Score from Baseline to 96 Hours.
• Vitamin C – 9.8 to 6.8
• Placebo – 10.3 to 6.8
• P = 0.86
Fowler AA. et al. JAMA 2019. 322 (13) :1261-1270. doi: 10.1001/jama.2019.11825.
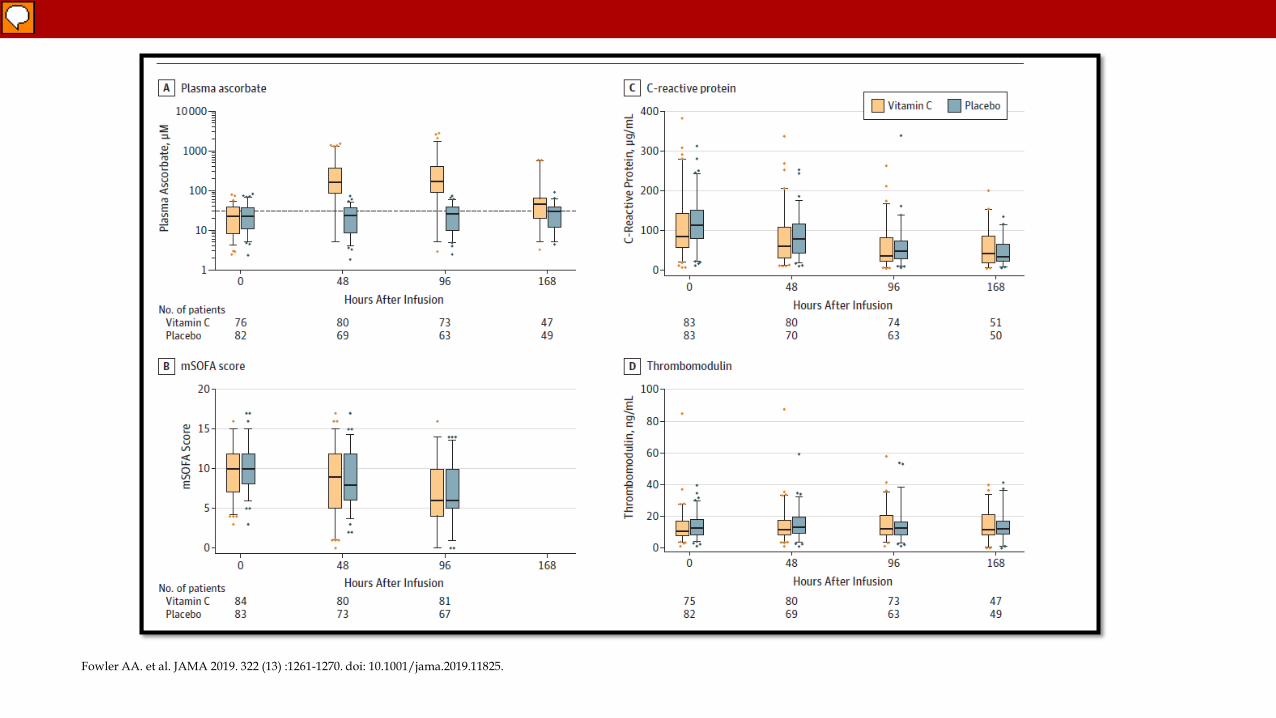
Fowler AA. et al. JAMA 2019. 322 (13) :1261-1270. doi: 10.1001/jama.2019.11825.
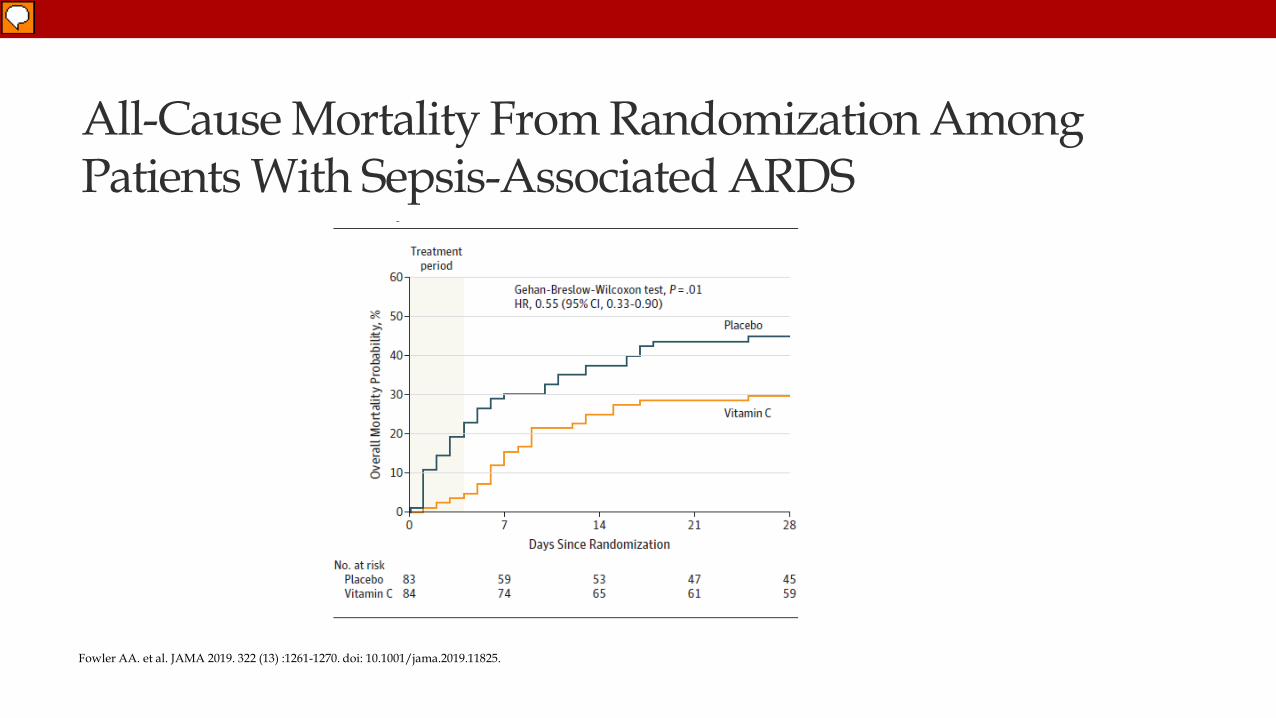
All-Cause Mortality From Randomization Among Patients With Sepsis-Associated ARDS
Fowler AA. et al. JAMA 2019. 322 (13) :1261-1270. doi: 10.1001/jama.2019.11825.
Fujii T et al. JAMA January 17, 2020. doi: 10.1001/jama.2019.22176
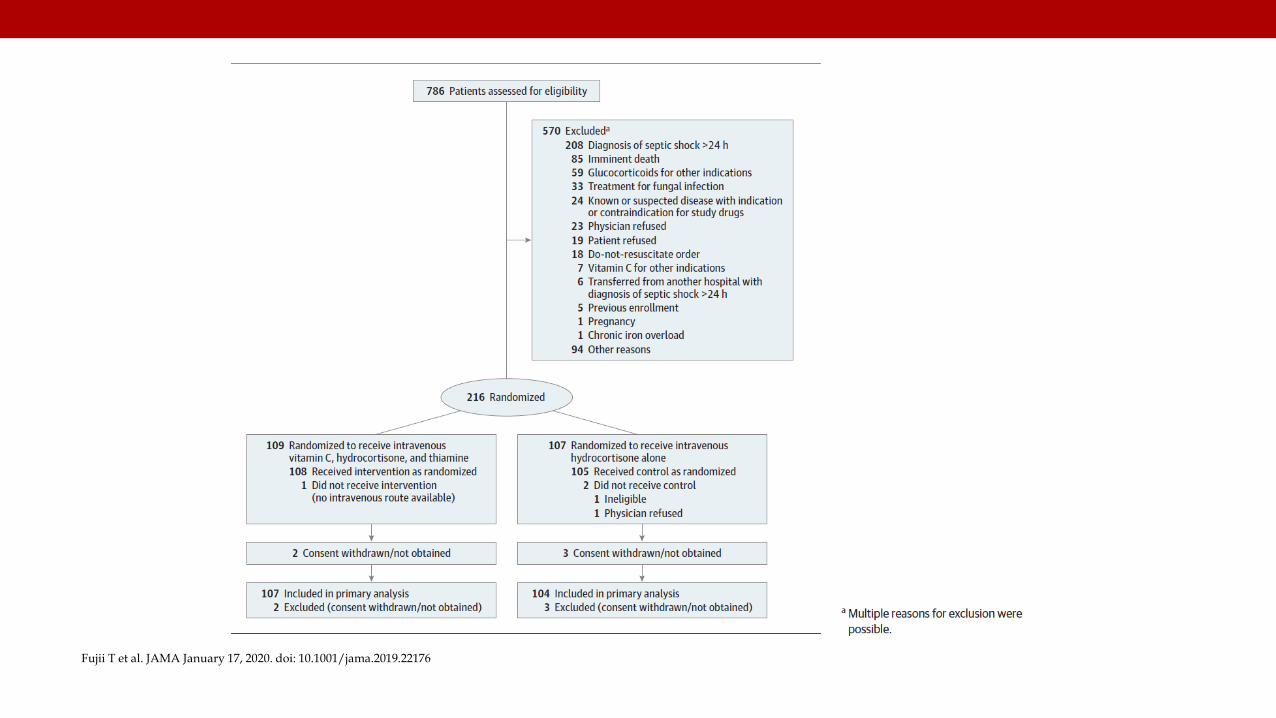
Fujii T et al. JAMA January 17, 2020. doi: 10.1001/jama.2019.22176
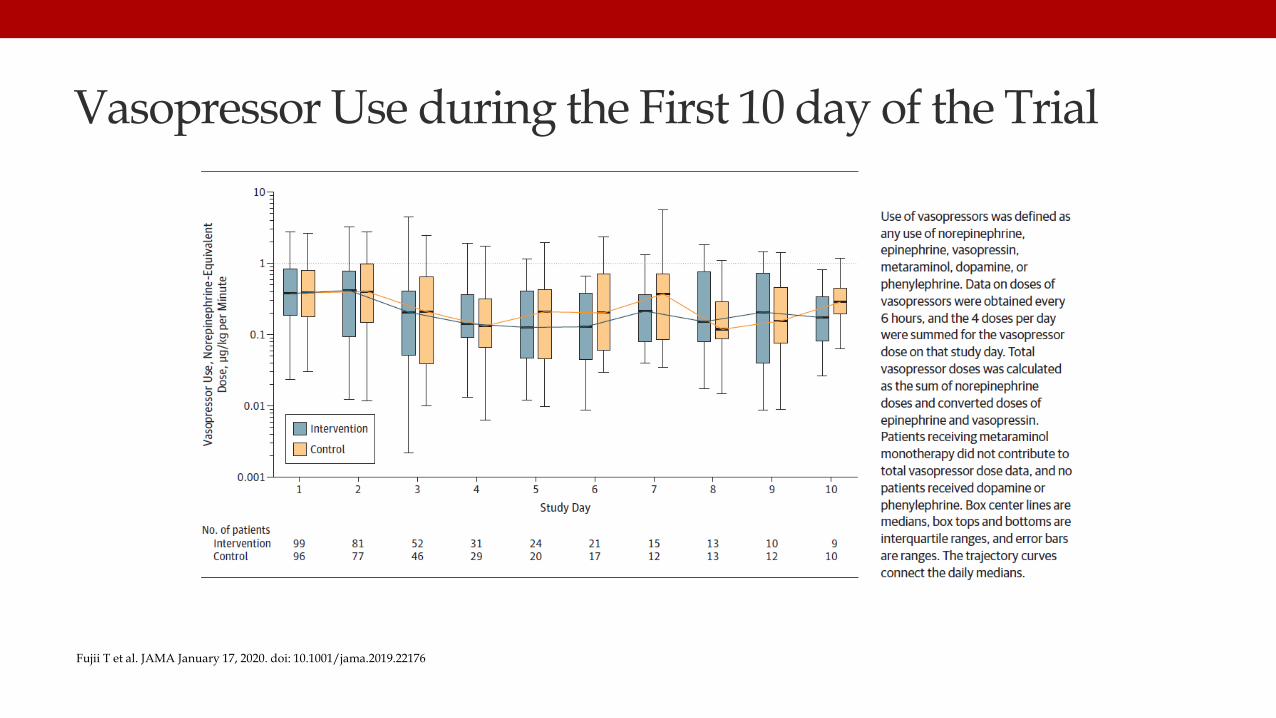
Vasopressor Use during the First 10 day of the Trial
Fujii T et al. JAMA January 17, 2020. doi: 10.1001/jama.2019.22176
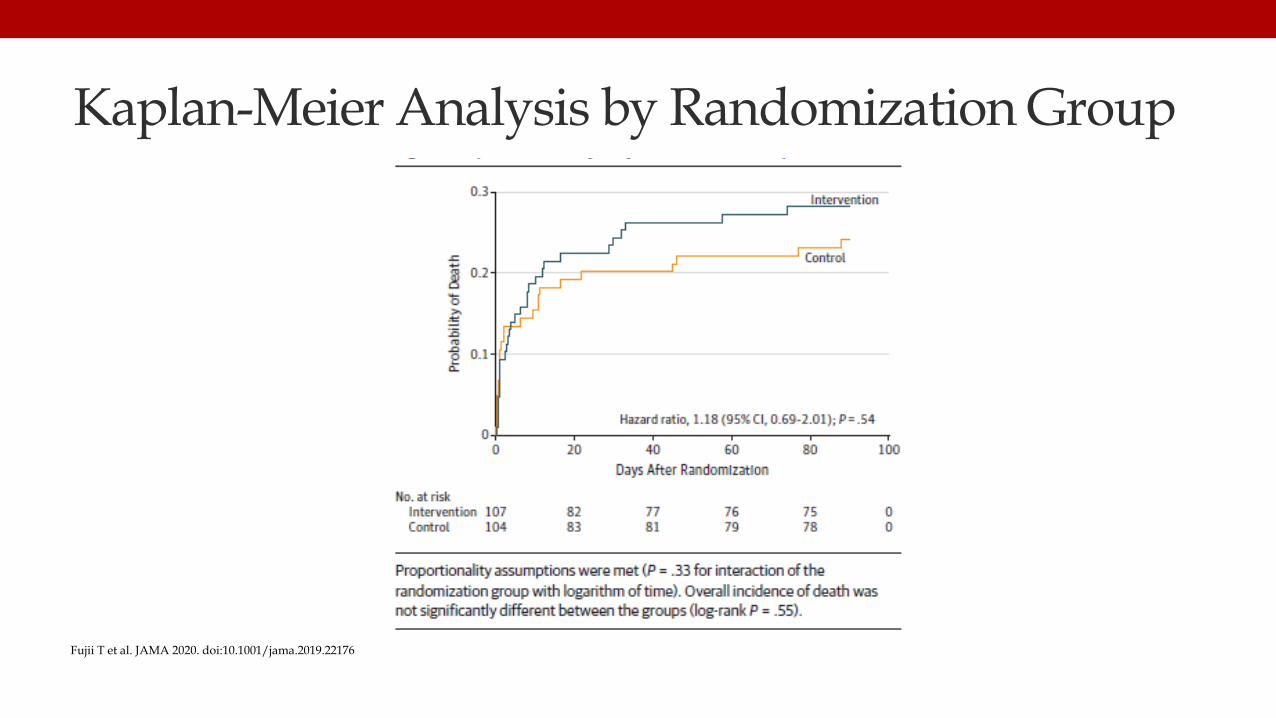
Kaplan-Meier Analysis by Randomization Group
Fujii T et al. JAMA 2020. doi:10.1001/jama.2019.22176
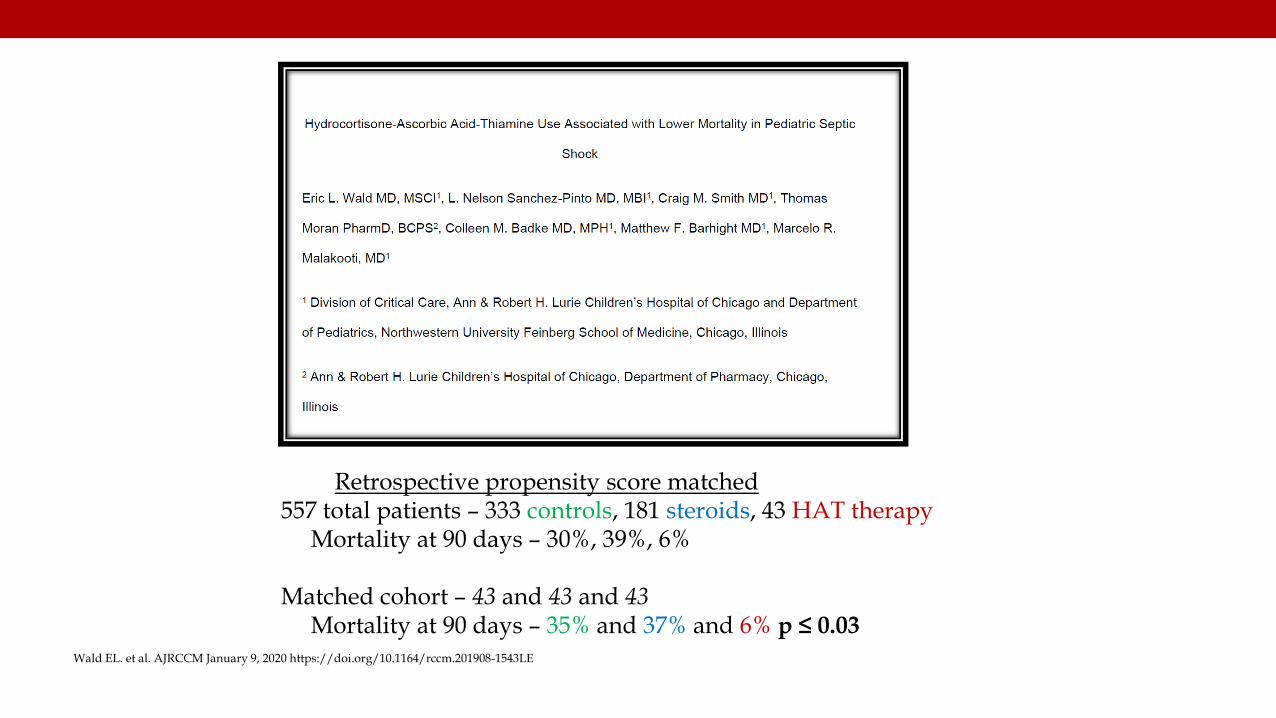
Wald EL. et al. AJRCCM January 9, 2020 https://doi.org/10.1164/rccm.201908-1543LE
Retrospective propensity score matched557 total patients – 333 controls, 181 steroids, 43 HAT therapy
Mortality at 90 days – 30%, 39%, 6%
Matched cohort – 43 and 43 and 43Mortality at 90 days – 35% and 37% and 6% p ≤ 0.03

48
Dobutamine inSeptic Shock
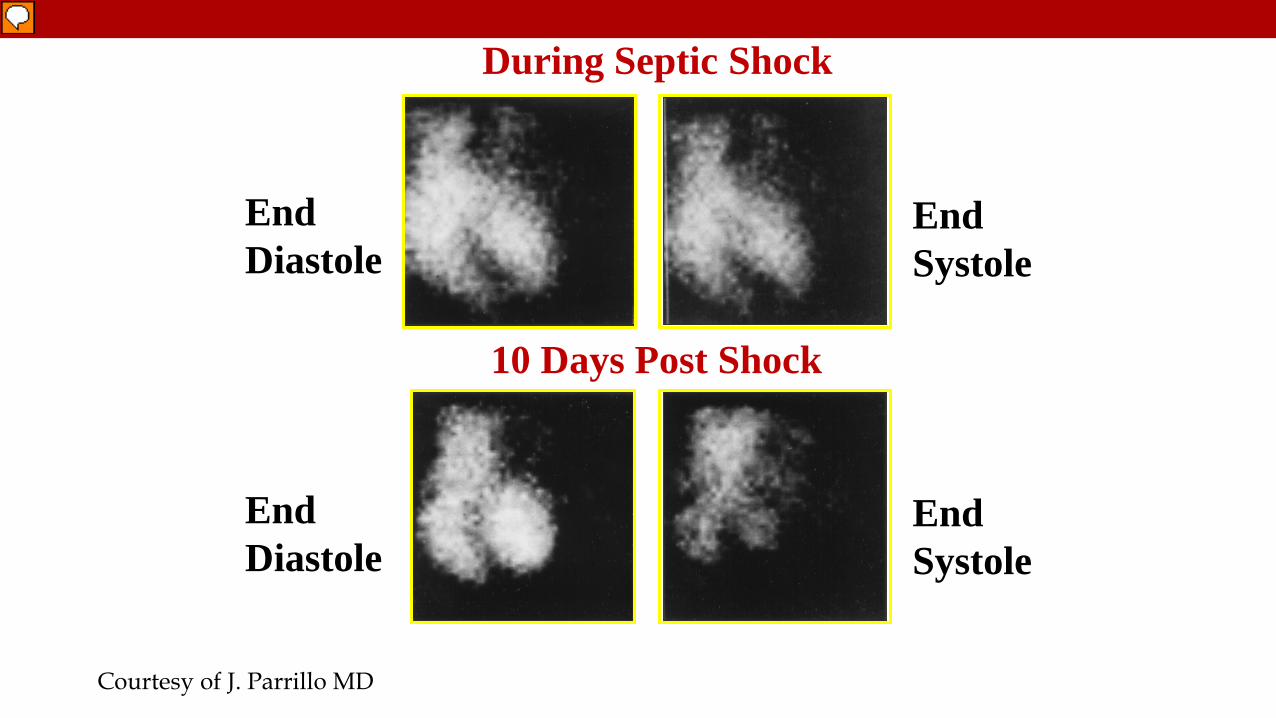
During Septic Shock
10 Days Post Shock
EndDiastole
EndSystole
EndDiastole
EndSystole
Courtesy of J. Parrillo MD
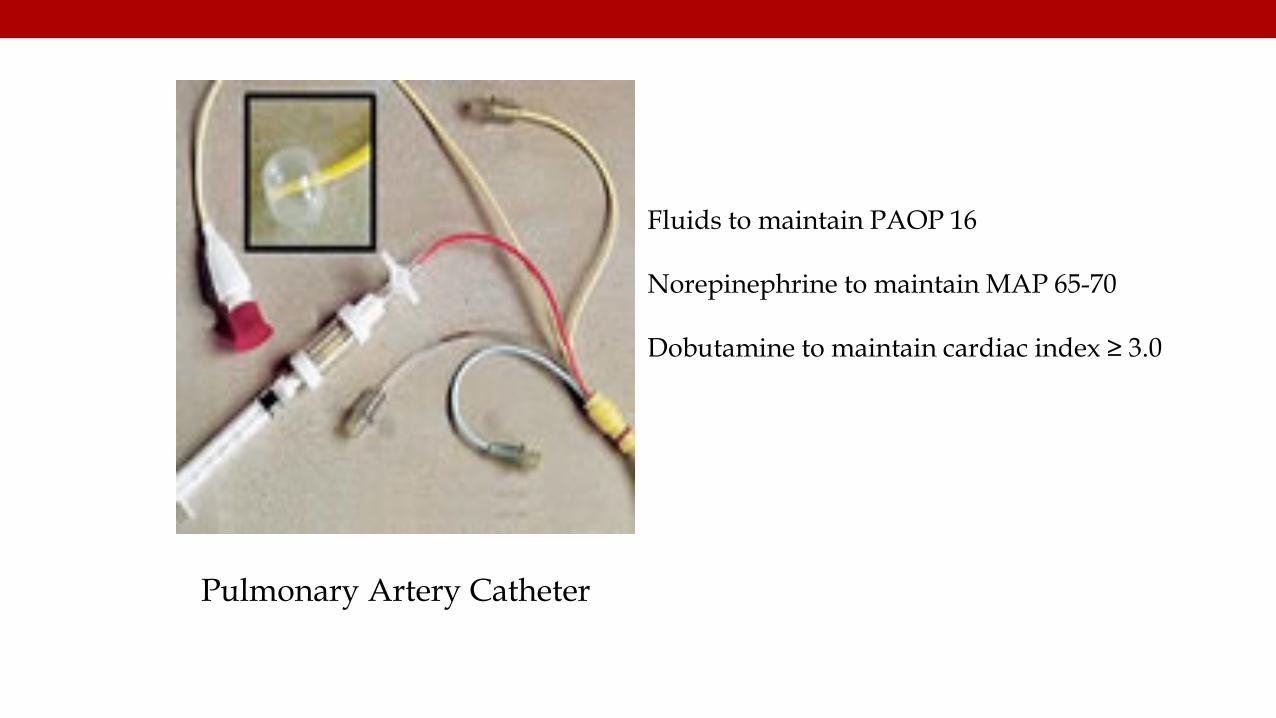
Pulmonary Artery Catheter
Fluids to maintain PAOP 16
Norepinephrine to maintain MAP 65-70
Dobutamine to maintain cardiac index ≥ 3.0
• We suggest using dobutamine in patients who show evidence of persistent hypoperfusion despite adequate fluid loading and use of vasopressor agents.
(Weak recommendation, low quality of evidence)
51
2016
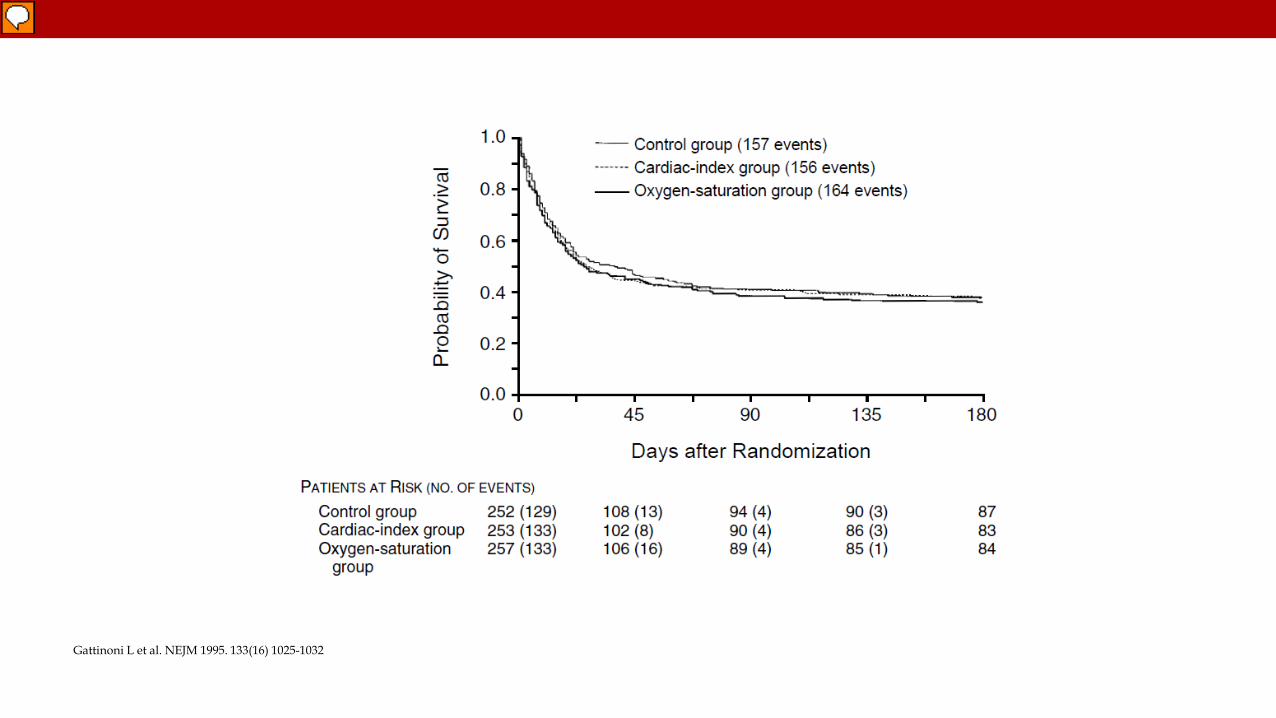
Gattinoni L et al. NEJM 1995. 133(16) 1025-1032
Hayes MA et al. NEJM 1994. 33-(24)
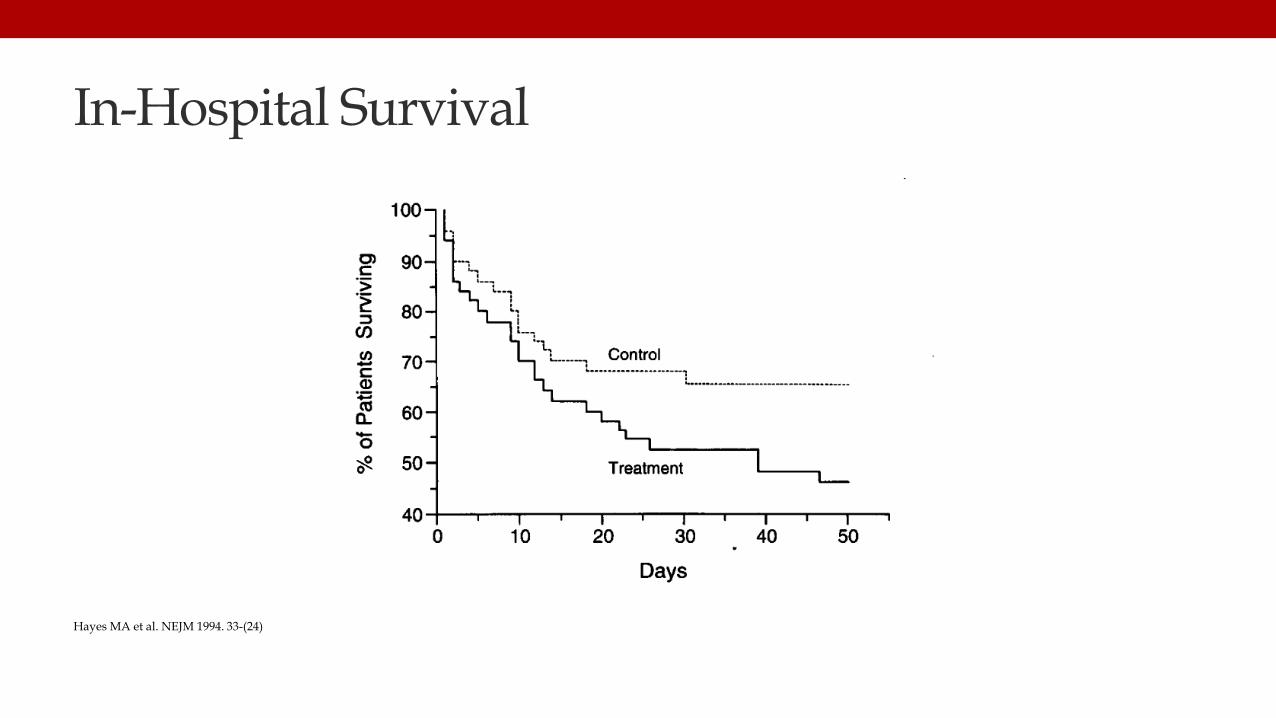
In-Hospital Survival
Hayes MA et al. NEJM 1994. 33-(24)
Gordan AC. et al. NEJM 2016. 375(17) 16-38-1648
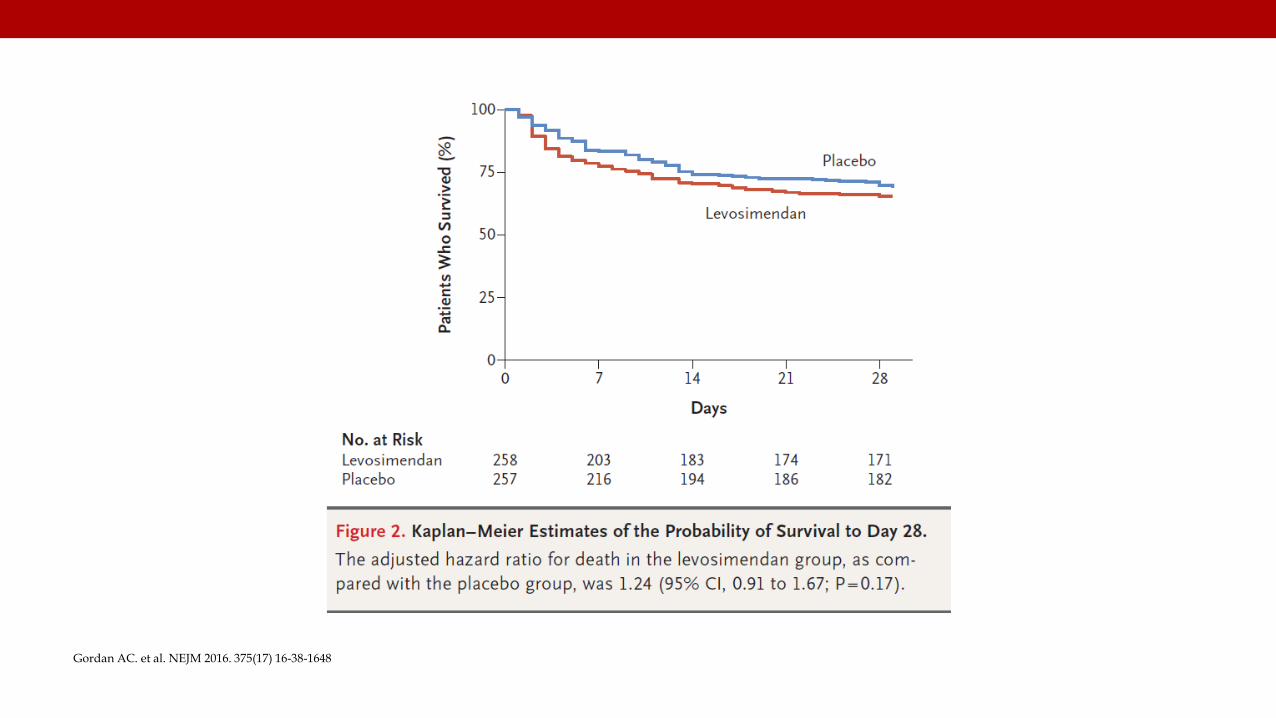
Gordan AC. et al. NEJM 2016. 375(17) 16-38-1648
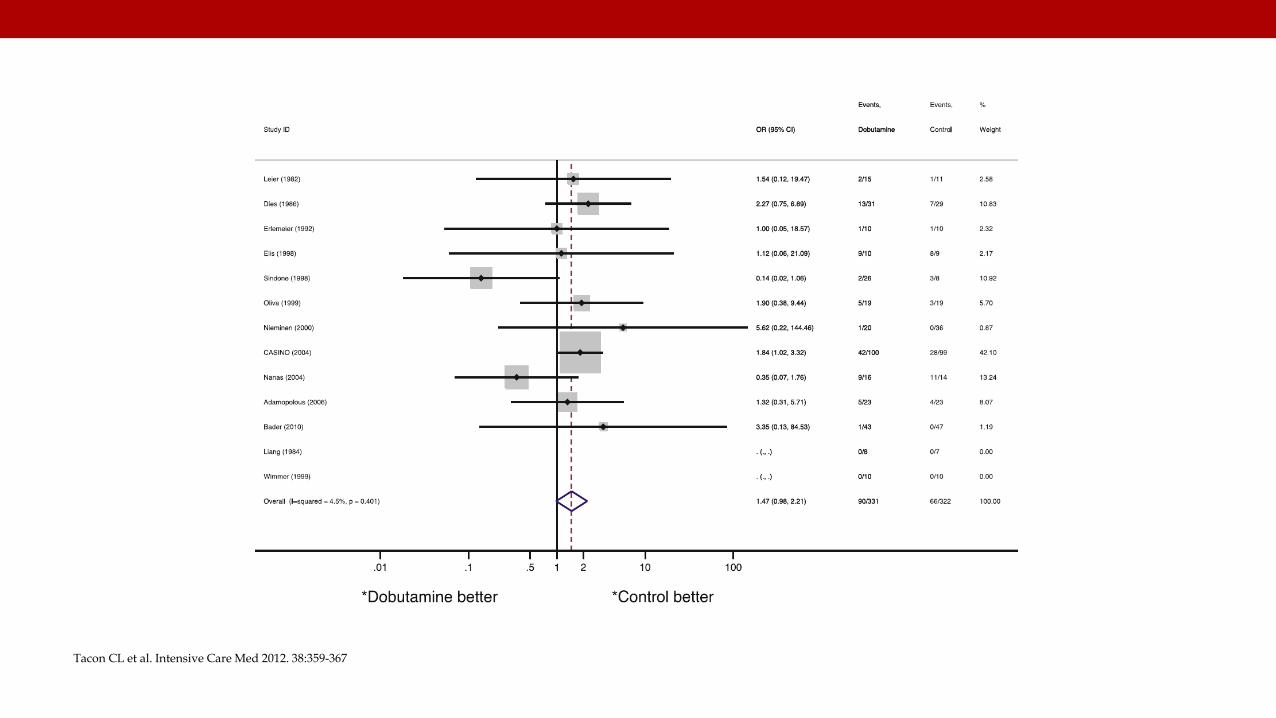
Tacon CL et al. Intensive Care Med 2012. 38:359-367
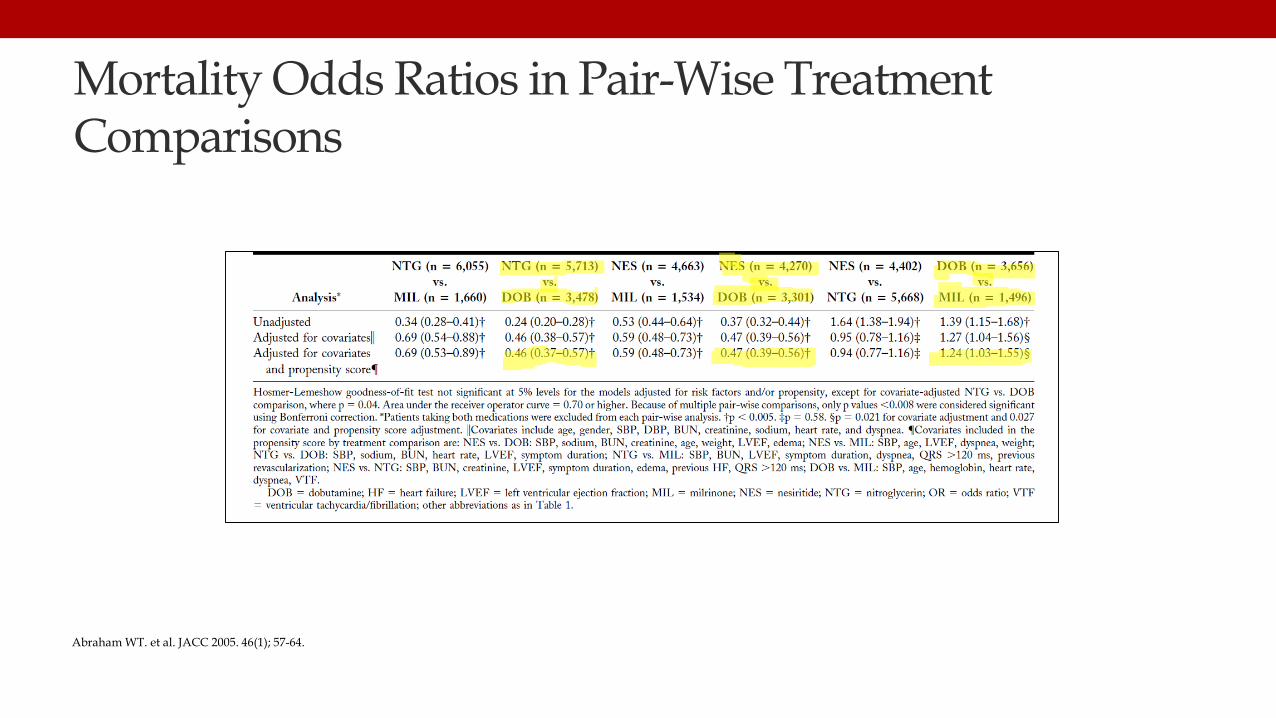
Mortality Odds Ratios in Pair-Wise Treatment Comparisons
Abraham WT. et al. JACC 2005. 46(1); 57-64.
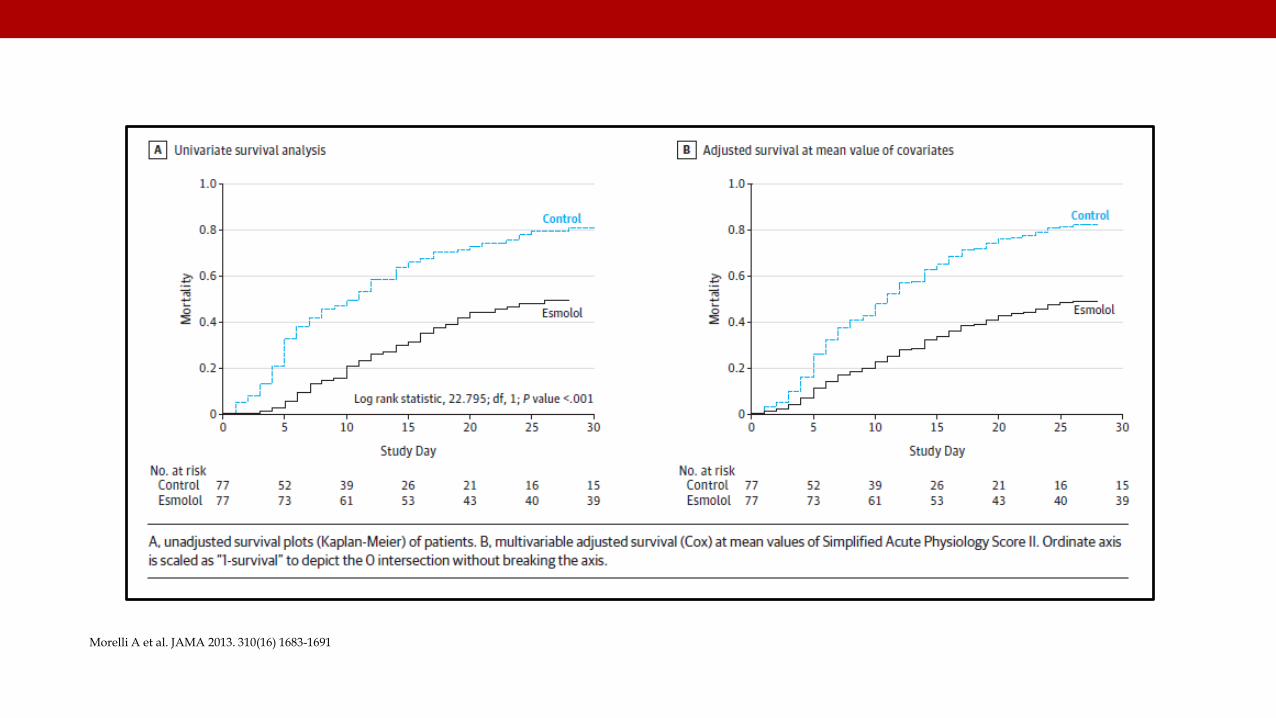
Morelli A et al. JAMA 2013. 310(16) 1683-1691
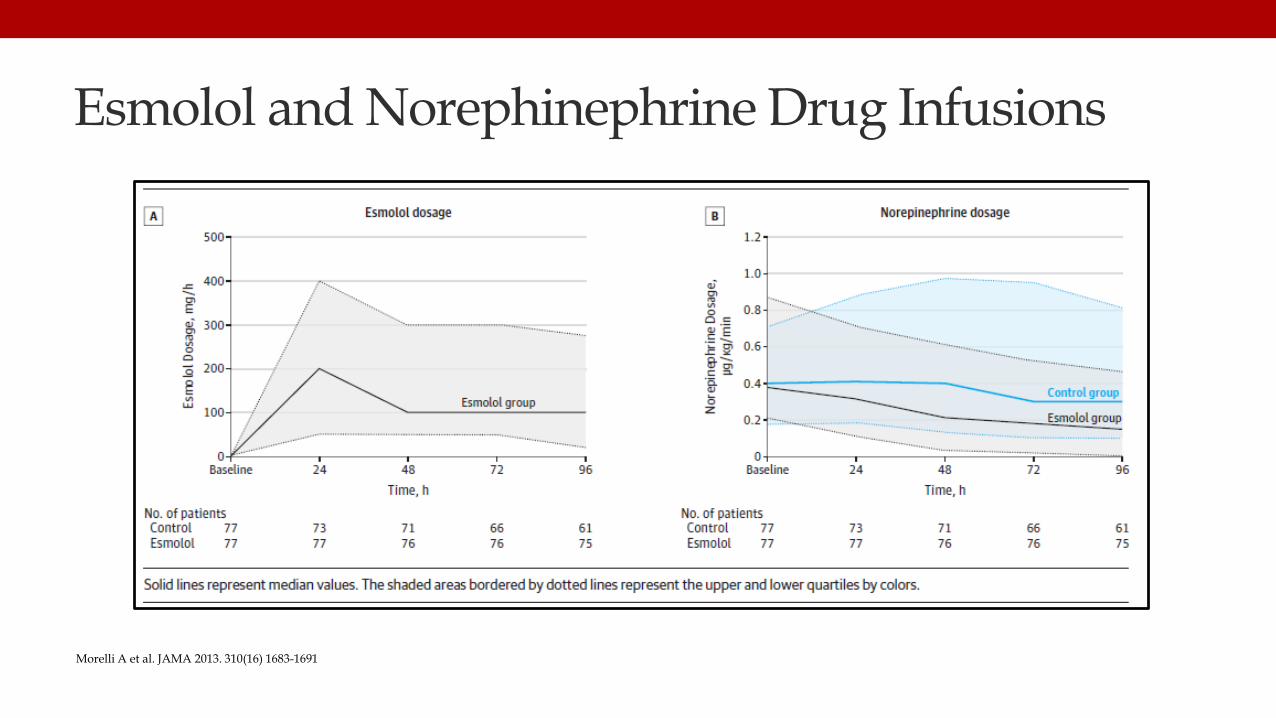
Esmolol and Norephinephrine Drug Infusions
Morelli A et al. JAMA 2013. 310(16) 1683-1691
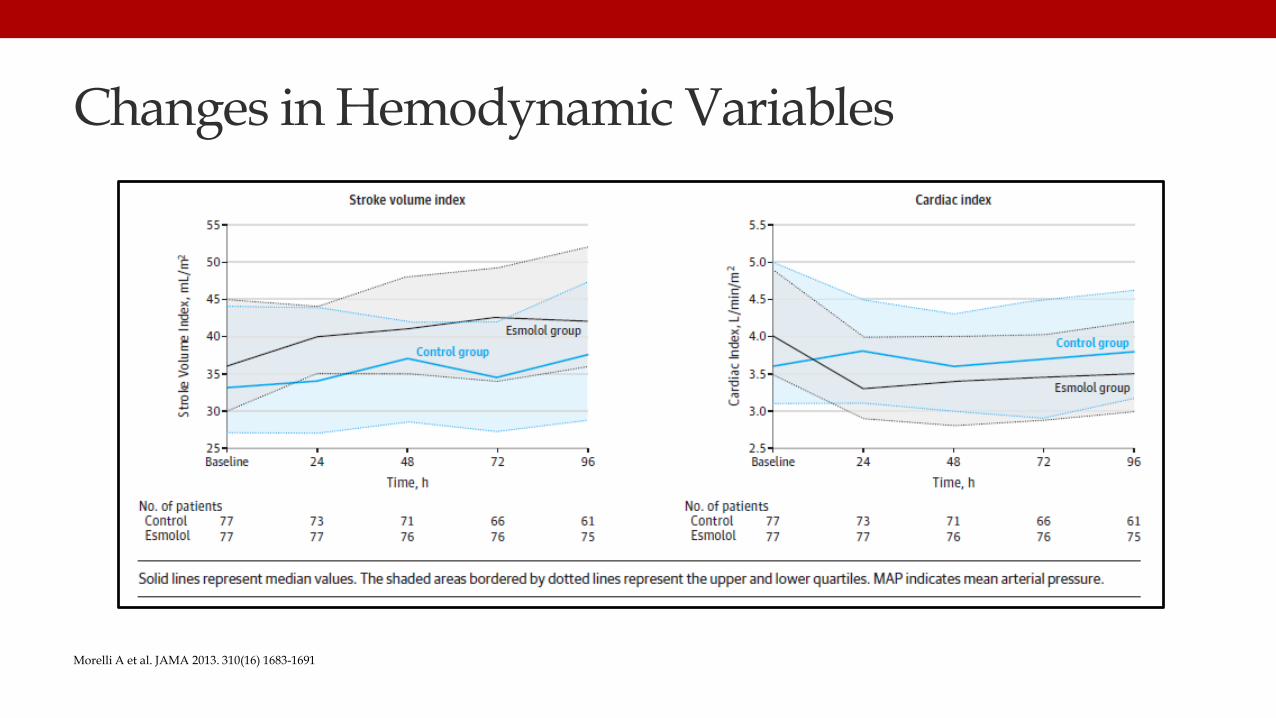
Changes in Hemodynamic Variables
Morelli A et al. JAMA 2013. 310(16) 1683-1691
Morelli A et al. JAMA 2013. 310(16) 1683-1691
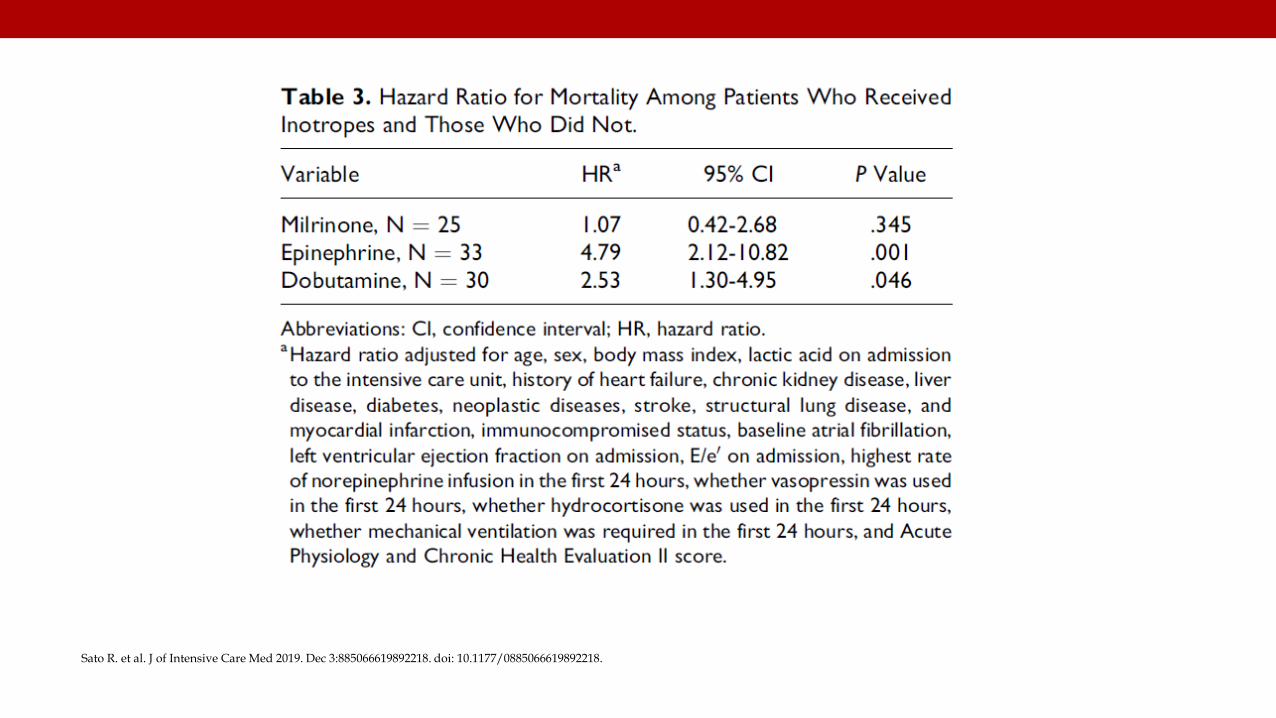
Sato R. et al. J of Intensive Care Med 2019. Dec 3:885066619892218. doi: 10.1177/0885066619892218.
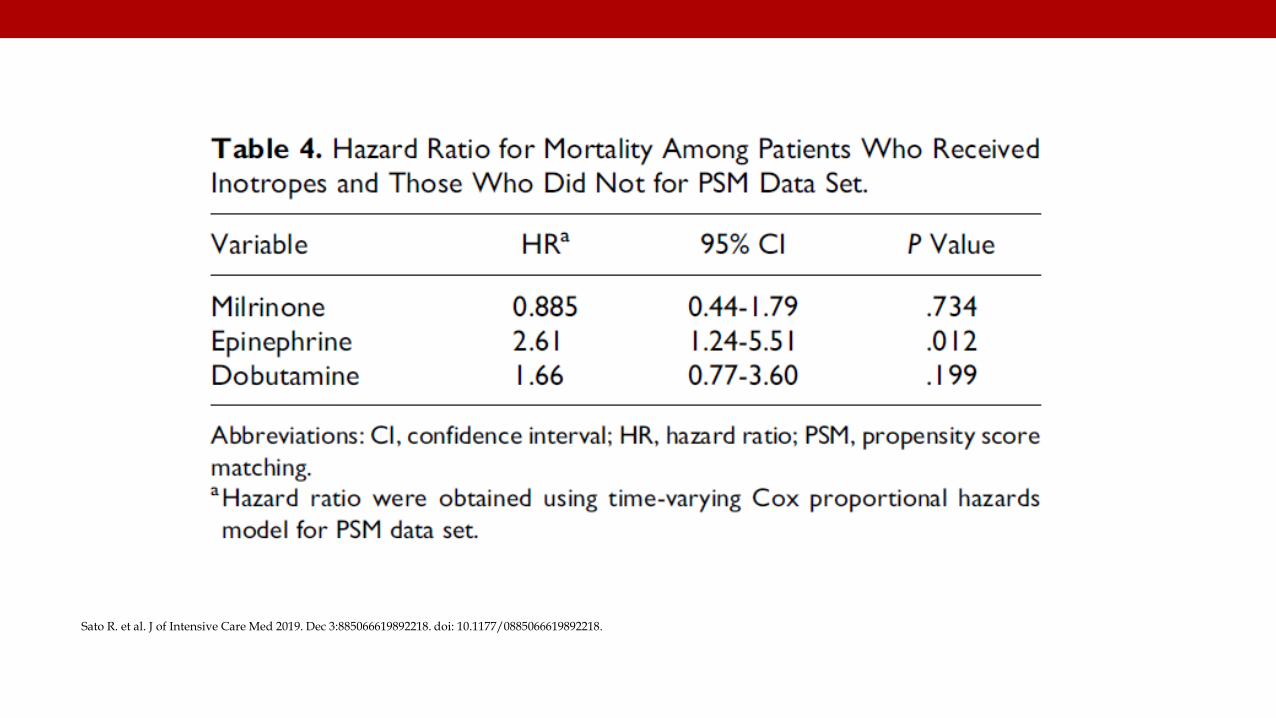
Sato R. et al. J of Intensive Care Med 2019. Dec 3:885066619892218. doi: 10.1177/0885066619892218.
• We suggest using dobutamine in patients who show evidence of persistent hypoperfusion despite adequate fluid loading and use of vasopressor agents.
(Weak recommendation, low quality of evidence)
69
2016
Summary
70
Fluid Rx Septic Shock
ESRD and CHF
Vitamin C,Thiamineand (Steroids)
Dobutamine inSeptic Shock
( )
Thank you