Embed Size (px)
Citation preview

Laurent Brochard
Toronto
Laurent Brochard
Toronto
Separation fromMechanical Ventilation

Conflicts of interest
• Our clinical research laboratory has received research grantsand/or equipment for clinical research projects from the following companies: – Covidien (PAV+)
– Dräger (SmartCare)
– General Electric (FRC)
– Philips (NIV-sleep)
– Fisher Paykel (High flow)
– Maquet (NAVA)

Weaning from mechanical ventilation.
Three groups
• 1) Simple Weaning (first trial)
– Early detection
• 2) Difficult Weaning (more than 1 attempt, up to one
week)
– Reasons for failure
• 3) Prolonged Weaning (more than 1 week or than
three attemps)
– Global managementBoles JM. ERJ 2007

5955
43
3026
39 39 40
14
6
18
30
0
20
40
60
80
FUNK et al. PEÑUELAS et al. SELLARES et al. TONNELIER et al.
Proportion of patients in
each group (%)
Re-intubation rate (%)
ICU Mortality (%)
Simple weaning Difficult weaning Prolonged weaning
37
13
01
711
2
22
13
42
18
0
10
20
30
40
50
FUNK et al. PEÑUELAS et al. SELLARES et al. TONNELIER et al.
1310
1 0
710
19
95
16
33
24
0
10
20
30
40
50
FUNK et al. PEÑUELAS et al. SELLARES et al. TONNELIER et al.

WIND new classification
Beduneau G et al AJRCCM 2016

WIND new classification /
Mortality
6%
17% 29%
Beduneau G et al AJRCCM 2016

Beduneau G et al AJRCCM 2016

Ely E.W. et coll. N Engl J Med 1996; 335: 1864-9
• Intervention Group
1) A daily screening of respiratory function (by the respiratory therapists of the unit)
PaO2/FIO2 > 200
PEEP< 5 cm H2O
Adequate cough
f/VT < 105 c/min
No vasopressor agents or sedatives
2) A 2-hour trial of spontaneous breathing
3) Notification of the physician of the successful results
Identifying patients capable of breathing spontaneously
and duration of mechanical ventilation
Pa
tien
ts R
ecei
vin
g M
ech
an
ical
Ven
tila
tion
(%
)
Days after Succesful Screening
SIMV

Imsand et al. Anesthesiology 1994

Imsand et al. Anesthesiology 1994


Weaning with Pressure Support Ventilation
Brochard AJRCCM 1994 Esteban NEJM 1995

Weaning with Pressure Support Ventilation
Good ? Bad ?
•RR < 35 breaths/min•RR ≤ 25 breaths/min
Brochard AJRCCM 1994 Esteban NEJM 1995

0
2
4
6
8
10
12
14
16
18
0:00 0:28 0:57 1:26 1:55 2:24 2:52
PS
level cm
H2O
)
Time (h:min)
ObservationMaintain
Adaptation
PS min
« Epreuve de VS automatisée»
EXTUBATION
Reduction of ¨PSV
Message: « separation from ventilator »
PEEP 5 cmH2O
Weaning with «SmartCare »

2014

Weaning…
…Screening & Tests

Tobin M J et al. Am Rev Respir Dis 1986;134:1111-8

A place forf/Vt?

The «Spontaneous Breathing Trial»:
T-piece, Low PS, CPAP…
Screening Test or Diagnostic
Tool?

Straus C, et al. AJRCCM 1998;157:23-30
Total
E
R

n Failure,
2hr
Ext Reint Succ Ext,
48hr
2 hr
T-piece
246 22%
(54/246)
192 36 63%
(156/246)
2 hr
PSV 7
238 14%
(33/238)
205 38 70%
(167/238)
P 0.03 ns ns ns
Esteban A, et al. AJRCCM 1997;156:459-65
TEST: T-piece or PSV?


Mahul et al Crit Care AJRCCM 2016
Spontaneous breathing trial and post-extubation work of breathing in
morbidly obese critically ill patients

Physiological Measures of Patient Respiratory Effort Among
Different Spontaneous Breathing Trial Techniques: A Systematic
Review and Physiological Meta-Analysis
Sklar M et al submitted
0.4
0.6
0.8
1.0
1.2
1.4
PSV vs. E
xtub
ation
PSV vs. T
-Piece
PSV vs. P
SV/C
PAP0
PSV vs. C
PAP
CPAP vs. E
xtub
ation
CPAP vs. T
-Piece
CPAP vs. P
SV/C
PAP0
PSV0/
CPAP0
vs. E
xtub
ation
PSV0/
CPAP0
vs. T
-Piece
T-Piece
vs. E
xtub
ation
Ratio
of
me
an
s (
95
% C
I)
Measurement
WOB
PTP
RSBI
n=239

Weaning difficulties…
…Medical issues

Kress, JP. et al. N Engl J Med 2000; 342:1471-1477
Sedation
Daily interruption of sedation

Girard et al. Lancet 2008
Sedation


Patient with COPD repeatedly failing weaning
Lemaire et al, Anesthesiology 1988
Weaning-induced Pulmonary Edema

Succès Echec
0
500
1000
1500
2000
2500
BN
P,
pg
/mL
Mekontso Dessap et al, ICM 2007
BNP & WEANING PREDICTION
Success Failure

FLUID BALANCE AND EXTUBATION FAILURE
Frutos-Vivar F, Chest 2006

%

AJRCCM 2012
□ Usual
■ BNP
*p<0.05 between usual weaning and BNP-guided weaning
**p<0.01 between usual weaning and BNP-guided weaning


ICU-acquired
paresis
no ICUAP
Duration
of MV after
awakening
1.0
.80
.60
.40
.20
0.0
03
69
1215
1821
2427
30
Dependent variable
Independent variables (multivariate analysis)
Duration of MV after awakening
ICU-acquired paresis OR 2.4 (1.4 - 4.2)
COPD OR 2.6 (1.5 - 4.5)
P = 0.01
De Jonghe et al., Intensive Care Med 2004

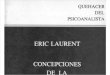
Levine S et al. N Engl J Med 2008;358:1327-1335
Comparison of Representative Case and Control Diaphragm-Biopsy Specimens with Respect to Fiber Size

47
47
41
3934
30
27
21
4744
3228
22
18 15 1313
13
11
11
11
11
11
10
-30%
-20%
-10%
0%
+10%
+20%
+30%
1 2 3 4 5 6 7 8
Day of Study
Cha
nge
in
dia
ph
ragm
th
ickne
ss o
ve
r tim
e (
% o
f b
ase
line
)
Group: Diaphragm Thickness Change
>10% loss on or before day 8
<10% change on or before day 8
>10% gain on or before day 8
Goligher E et al. 2015 Am J Respir Crit Care Med

0
10
20
30
40
50
60
0 5 10 15 20 25 30 35
MR
C s
core
Ptr,stim (cm H2O)
Dres M et al AJRCCM 2016
76 patients at their first weaning attempt:
63% had diaphragm dysfunction, 34% had limb muscle weakness and 21% had both

DiehlDiehl J-L, et al.J-L, et al.AmAm JJ Respir Crit Care MedRespir Crit Care Med 1999; 159:383-3881999; 159:383-388
Effects of tracheostomy on work of breathing


Weaning…
…and the decision to
extubate

0 10 20 30 40 50
Daley
Demling-T
Rady
Engoren
Demling-GS
Tahvanainen
Epstein
Lee
Esteban
Esteban
Esteban
Vallverdú
Failure
Success
% Mortality for Extubation Failure Patients

0
2
4
6
8
10
12
J-1 J0 J1 J2 J3
SOFA score
Success
FailurePlanned extubation
‡
§§
§
‡ §
‡ ‡
NS
Day-1 Day0 Day1 Day2 Day3
Thille AW et al CCM


Weaning winning strategies
• Systematic screening
• Weaning test (safety) T-piece, low PS,
no PEEP
• Sedation management
• Fluid overload (BNP), weakness
(prevention)
• Automated weaning