Embed Size (px)
Citation preview

Integrated Systems and Technologies
Sentinel Lymph Node Biopsy Revisited: Ultrasound-GuidedPhotoacoustic Detection of Micrometastases UsingMolecularly Targeted Plasmonic Nanosensors
Geoffrey P. Luke1,2, Jeffrey N. Myers3, Stanislav Y. Emelianov1,2,4, and Konstantin V. Sokolov2,4
AbstractMetastases rather than primary tumors are responsible for killingmost patients with cancer. Cancer cells often
invade regional lymph nodes (LN) before colonizing other parts of the body. However, due to the low sensitivityand specificity of current imaging methods to detect localized nodal spread, an invasive surgical procedure—sentinel LN biopsy—is generally used to identify metastatic cancer cells. Here, we introduce a new approach formore sensitive in vivo detection of LN micrometastases, based on the use of ultrasound-guided spectroscopicphotoacoustic (sPA) imaging ofmolecularly activated plasmonic nanosensors (MAPS). Using ametastaticmurinemodel of oral squamous cell carcinoma, we showed that MAPS targeted to the epidermal growth factor receptorshifted their optical absorption spectrum to the red-near-infrared region after specific interactions with nodalmetastatic cells, enabling their noninvasive detection by sPA. Notably, LN metastases as small as 50 mm weredetected at centimeter-depth range with high sensitivity and specificity. Large sPA signals appeared inmetastaticLNwithin 30minutes of MAPS injection, in support of the clinical utility of this method. Our findings offer a rapidand effective tool to noninvasively identify micrometastases as an alternate to sentinal node biopsy analysis.Cancer Res; 74(19); 5397–408. �2014 AACR.
IntroductionAccurate detection of regional lymph node (LN) metastases
is a critical step in staging, prognosis, and development of atreatment plan for patients with cancer (1–3). Lymphaticmapping with sentinel LN (SLN) biopsy has been introducedas an alternative to elective LN dissection and has gained rapidacceptance because it allows improved accuracy anddecreased patient morbidity for regional cancer staging(4, 5). However, SLN biopsy still has major limitations. Theprocedure requires two or more injections of radionuclidetracers followed by an invasive surgical procedure associatedwith removal of one or more LNs identified as SLNs withassociated risks of short- and long-term morbidity and up to 2weeks of waiting for full histopathology evaluation (6, 7). In
addition, the detection limits for pathologic identification ofmetastatic cells remain subject to the skill and patience of thepathologist. In fact, LNmetastases go undetected in up to 9% ofpatients with melanoma, allowing the disease to spreaduntreated (8). Therefore, there is a definite and urgent clinicalneed for an imaging technique that is widely available, isnoninvasive and simple to perform, is safe, and can reliablydetect and adequately diagnose LN micrometastases in realtime.
Ahost of imagingmodalities have been tested in animals andpatients in attempts to improve the accuracy and safety of SLNbiopsy (9–14). For example, ultrasound imaging has been usedto detect changes in LN size, shape, and blood flow, which areassociated with metastasis (10). In addition, ultrasound imag-ing ofmicrobubbles and fluorescence imaging of dye have beenproposed as an approach to guide SLN biopsy (14, 15). Positronemission tomography (PET) has showed limited sensitivity indetection of metastatic deposits and has been able to reliablydetect metastases only with sizes greater than 80 mm3 (11).Magnetic resonance imaging (MRI) of systemically injectedsuperparamagnetic iron oxide nanoparticles has been shownto indirectly indicate potential presence of metastasis bydetecting a disrupted drainage in metastatic LNs (16). There-fore, although these imaging approaches have shown potentialin providing usefulmorphologic and functional information, todate, none have demonstrated sufficient sensitivity and spec-ificity to replace the current invasive SLN procedure (11, 12).
Photoacoustic imaging has recently been introduced as amodality that can improve the detection threshold and sen-sitivity of radiographic imaging modalities (17–22). It is an
1Department of Electrical and Computer Engineering, The University ofTexas at Austin, Austin, Texas. 2Department of Biomedical Engineering,The University of Texas at Austin, Austin, Texas. 3Department of Head andNeck Surgery, The University of Texas MD Anderson Cancer Center,Houston, Texas. 4Department of Imaging Physics, The University of TexasMD Anderson Cancer Center, Houston, Texas.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Authors: Stanislav Y. Emelianov, The University of Texasat Austin, 107 West Dean Keeton Street, Austin, TX 78712. Phone: 512-471-1733; Fax: 512-471-0616; E-mail: [email protected]; andKon-stantin V. Sokolov, The University of Texas MD Anderson Cancer Center,1515 Holcombe Boulevard, Houston, TX 77030. Phone: 713-745-0620;Fax: 713-563-2986; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-14-0796
�2014 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 5397
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

emerging hybrid imaging technique that combines the highcontrast and sensitivity of optical imaging with the excellentdepth resolution of ultrasound imaging. Images are acquiredby detecting broadband ultrasoundwaves that propagate fromsites of optical absorption after the tissue is irradiated with ananosecond pulsed laser. Previous studies have shown thatphotoacoustic imaging can accurately track intradermallyinjected dyes or nanoparticles for localization of LNs withhigh sensitivity (23, 24). However, even though theseapproaches eliminate the use of radioactive compounds, theystill require surgical removal and histopathologic evaluation ofthe SLNs and they do not provide information about themetastatic state of the SLN.
To address the need for molecular-specific detection ofmicrometastasis with enhanced specificity and sensitivity, wedeveloped a novel method based on spectroscopic photoa-coustic (sPA) imaging with molecularly activated plasmonicnanosensors (MAPS). The MAPS (Fig. 1A) consisted of 40-nmspherical gold nanoparticles (AuNPs) targeted to the epider-mal growth factor receptor (EGFR), a molecular target asso-ciated with carcinogenesis in many cancers, including lung,oral cavity, and cervix (25), through directional conjugationwith anti-EGFR monoclonal antibodies and polyethylene gly-col (PEG; refs. 26, 27). Here, we show that MAPS can be used inin vivo applications where nonspecific signal due to delivery ofa contrast agent hinders the ability to visualize the underlying
500 550 600 650 700 7500
0.2
0.4
0.6
0.8
1
Wavelength (nm)
Sca
tterin
g in
tens
ity (a
.u.)
CellsDeliveryInteraction
A B
C D E
F G H
50 nm
Gold nanoparticle
Heterofunctionallinker
PEG-SH
Targeting antibody
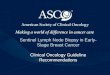
Figure 1. The effect of plasmon resonance coupling inmolecular-specific imaging of EGFR-expressing cancer cells. A, a schematic of the EGFR-targetedMAPS;relative dimensions of antibody molecules and a gold nanoparticle (AuNPs) are preserved. B, hyperspectral dark-field microscopy was used to obtain opticalspectra from unlabeled cells (blue), MAPS dispersed in extracellular space (green) and cells labeled with MAPS (violet). Dark-field optical images (C, D, and E;scale bar, 10mm)and cartoon (F, G, andH) show cancer cells in the absence of gold nanoparticles (C and F); cells in the presence of nonspecificAuNPs (D andG);and cells labeledwithMAPS (EandH).Unlabeled cells havea characteristic bluishwhite appearance due to intrinsic light scattering properties (C)while a greenishhaze is evident in the presence of nonspecific AuNPs that strongly scatter green light (D). Molecular-specific interactions between MAPS and EGFR-overexpressing cancer cells lead to receptor-mediated endocytosis that results in plasmon resonance coupling between MAPS and the associated strongchanges in their optical properties (E). The colored stars in C–E identify the regions from which the same-color spectral curves are displayed in B.
Luke et al.
Cancer Res; 74(19) October 1, 2014 Cancer Research5398
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

molecular expressions. In an orthotopic nude mouse model ofsquamous cell carcinoma of the oral cavity (SCCOC) thatdevelops LN micrometastases (28), we show that a singleperitumoral injection of MAPS followed by sPA imaging issufficient to detect micrometastases as small as 50 mm in size.Molecular-specific interactions between the EGFR-targetedMAPS and tumor cells lead to a dramatic change in thespectroscopic signal ofMAPS in sPA imaging that enables highlysensitivedetectionofmicrometastasis. Thus, the combinationoftraditional ultrasound imaging to provide guidance and ana-tomic information with sPA MAPS-based detection of cancercells provides an integrated technique for the detection of smallmicrometastases with high sensitivity and specificity. Ourmeth-odhas a great potential for clinical translationbecause it is basedon a combination of a well-established ultrasound imaging andemerging clinically translatable sPA imaging and MAPS. Thispowerful combination can provide dramatic improvement inthe clinical staging, prognosis, and therapeutic planning forpatients with cancer with metastatic disease.
Materials and MethodsNanoparticle synthesisMolecular-targeted AuNPs were synthesized as previously
described (26). First, 40-nm spherical AuNPs were preparedby heating 100 mL of a 0.01% (w/v) water solution ofchloroauric acid (HAuCl4; Sigma-Aldrich) to boiling, andrapidly adding 4 mL of a 1% (w/v) solution of sodium citrate.Then, anti-EGFR or anti-RG16 monoclonal antibodies (cloneC225 or RG16; Sigma-Aldrich) were attached to the AuNPsusing directional conjugation chemistry that uses a carbo-hydrate chain on the Fc portion of the antibody leavingantigen binding sites on the Fab moiety available for target-ing (26). Briefly, antibodies at 1 mg/mL in 40 mmol/L HEPESbuffer, pH 7.5 and 100 mmol/L sodium periodate (NaIO4;Sigma-Aldrich) were mixed at 10:1 (v/v) ratio, respectively,and were incubated for 30 minutes in dark at room tem-perature to oxidize hydroxyl groups of the carbohydratechain in the Fc antibody regions. Then, approximately100-fold molar excess of a heterofunctional hydrazide--PEG–dithiol linker (dithiolaromatic–PEG6k–CONHNH2;SensoPath Technologies) was added to the oxidized anti-bodies for 1 hour. The hydrazide portion of the linker reactswith aldehydes on antibody molecules to form a stablelinkage. The antibody–linker complexes were purified usinga 100,000 Da molecular weight cutoff centrifugal filter (Milli-pore). After purification, the modified antibodies were resus-pended in 40 mmol/L HEPES (pH 7.4) at concentration of 0.1mg/mL and were mixed with prepared AuNPs at 1:10 anti-body:nanoparticle (v/v) ratio for 20 minutes at room tem-perature. During this step, a stable bond is formed betweenthe gold surface and the linker's thiol groups. Subsequently,10�5 mol/L 1� phosphate-buffered saline (PBS) solutionof methoxy-poly(ethylene-glycol)thiol (mPEG-SH; 14 kD;Shearwater Polymers) was added at ca. 1:10 mPEG-SH tonanoparticle ratio (v/v) for 20 minutes to passivate thesurface of nanoparticle conjugates that is not covered byantibodies (Fig. 1A). The final conjugates were washed using
centrifugation (4,000 rpm, 30 minutes) and were resus-pended in 1� PBS at concentration of ca. 1 � 1012 nano-particles/mL.
Animal studiesAll animal studieswere approved by the Institutional Animal
Care and Use Committee at The University of Texas at Austin(Austin, TX). Balb/c nudemice of 2 months of age were used inthis study (Charles River Laboratories). The primary tumorswere initiated with a submucosal injection of 300,000 FaDu-Luciferase cells suspended in 30 mL of DMEM media into thetongue. The FaDu cells (ATCC, 2009) are a primary humansquamous cell carcinoma of the pharynx cell line that werevalidated at the Fragment Analysis Facility at Johns HopkinsUniversity (Baltimore, MD) via short-tandem repeat profilingon January 20, 2011. The cells were passaged for fewer than 6months before these studies. The tumors were allowed to growto 3 to 4 mm in diameter before the imaging experiments wereperformed. At this point, 82% of the inoculatedmice developedmicrometastases in the cervical LNs.
During ultrasound and photoacoustic imaging, the micewere anesthetized with isoflurane (1.5%, 0.5 L/min O2). Heartrate, respiration rate, and body temperature were monitoredusing a heated electrocardiogram pad. The mice were imagedbefore the injection of nanoparticles. Forty microliters ofsterile-filtered nanoparticle solution was injected peritumo-rally immediately after the first imaging session while themicewere still under anesthesia. The total injected dose was 1.6pmol of nanoparticles that is equivalent to 40 mg of gold.Imaging was performed continuously for 2 hours followingthe injection of nanoparticles.
Following the ultrasound and photoacoustic imaging, thebioluminescent cancer cells in the mice were imaged using anIVIS Spectrum (PerkinElmer). Once anesthetized with isoflur-ane, the mice were injected with 100 mL of RediJect D-Luciferin(PerkinElmer). Bioluminescence imagingwas performed for 10to 15 minutes following the injection. Then, mice were eutha-nized by an overdose of isoflurane and cervical dislocation.Bioluminescence imaging was performed to guide the resec-tion of the primary tumor and metastases. The primary tumorand cervical LNs were fixed in 10% formalin for 24 hours and,then, were transferred to 70% ethanol. Samples were thenembedded in paraffin for histologic analysis.
Photoacoustic and ultrasound imagingA Vevo LAZR high frequency ultrasound and photoacoustic
imaging system (VisualSonics) equipped with a linear arraytransducer (LZ-550, 40 MHz center frequency) was used toacquire all photoacoustic and ultrasound images. The co-registered spatial dimensions of the collected ultrasound andphotoacoustic images were 14 mm (width) by 15 mm (depth).Ultrasound and photoacoustic images at each optical wave-length covering three-dimensional (3D) volumes surroundingthe cervical LNs were acquired by scanning the ultrasoundtransducer in the elevational direction with a step size of 76mm. The laser was tuned to optical wavelengths of 680, 700, 720,740, 760, 780, 800, 820, 840, and 860 nm. Laser fluences,measured by a Nova II power meter with a PE50BB sensor
Molecular Photoacoustic Imaging of LN Metastases
www.aacrjournals.org Cancer Res; 74(19) October 1, 2014 5399
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

Figure 2. Generation of sPA images. A, in each 2D plane photoacoustic images are acquired using excitation wavelengths spanning 680 to 860 nm in steps of20 nm. B, each pixel is compared with hemoglobin and activated MAPS; the dashed lines represent the expected spectra, while the colored boxes arerepresentative measured photoacoustic signals. Spectral unmixing is performed using a least squares method (29). An example of spectral unmixing of aseries of photoacoustic images is shown in C–H. Photoacoustic images acquired at 680 nm (C) and 860 nm (D) show the raw photoacoustic signal. E–G, thespectra derived from three pixels (denoted by orange, red, and blue stars, for E, F, and G, respectively) of the photoacoustic images acquired at 10wavelengths, including the images from C and D, exhibit distinct spectral signatures that correlate well with the spectra of hemoglobin or MAPS. The pixelcontaining signal correlating to the MAPS spectrum steadily increases in amplitude over time (E), while the signals corresponding to blood remain relativelyconstant (F and G). H, after spectral unmixing, the different absorbers are clearly distinguished as either blood (red/blue) or activated MAPS (yellow).Scale bars, 1 mm. PA, photoacoustic.
Luke et al.
Cancer Res; 74(19) October 1, 2014 Cancer Research5400
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

(Ophir), were 10 to 20mJ/cm2; all laser energies were below theAmerican National Standards Institute (ANSI) safe exposurelevel for human skin. Photoacoustic images were averagedeight times, thus suppressing uncorrelated noise. Each photo-acoustic image was normalized by the measured fluence tocorrect for the pulse-to-pulse laser energy variations.To resolve different types of optical absorbers, we developed
an ultrasound-guided sPA imaging algorithm. We restrictedour analysis to three predominant absorbers: oxygenatedhemoglobin (HbO2), deoxygenated hemoglobin (Hb), and acti-vated MAPS. The ultrasound image was used to automaticallysegment themouse to remove photoacoustic imaging artifactson the surface of the skin. The relative contributions ofHbO2,
Hb, andMAPS to the overall photoacoustic signal in each pixelwas determined using a previously developed linear leastsquares method (29). Pixels containing negative concentra-tions (an artifact arising from noise or the presence of absor-bers other thanHbO2, Hb, and MAPS) were not displayed. Theoxygen saturation of hemoglobin (SO2) was computed as theratio of HbO2 concentration to total hemoglobin concentra-tion. The sPAHb signal was defined as the total hemoglobinconcentration while the sPAMAPS signal was defined as theconcentration of activated MAPS. sPA images were displayedusing yellow color for activated sPAMAPS and blue/red colorsfor sPAHb with SO2 varying from 60% (blue) to 100% (red). Therange from 100% to 60% was chosen because it represents
A B C
D
E
F G
Primary tumorPrimary tumor(tongue)
Metastases
SLN
Metastasis
SO
2
100%
60%
sPA
MA
PS
Max
Min
US
0 dB
–50 dB
EGFR-MAPS EGFR-MAPSRG16-AuNPs
, P = 0.006
, P = 0.005
Tumor+ Tumor+ Tumor–
1.5
1.0
sPA
MA
PS
sig
nal (
a.u.
)
0.5
Figure 3. In vivo imaging of LN micrometastases. A, 3D ultrasound image of a mouse with an overlaid cartoon of the primary tumor in the tongue andmicrometastases in the cervical lymph nodes. Inset, a 2D cross-section of the ultrasound image with a LN seen as the dark, hypoechoic bean-shaped region.B, a representative bioluminescence image confirms the presence of FaDu cells in the primary tumor and in the lymphatic system. Representativeoverlaid ultrasound (US) and sPA images of a tumor-bearing mouse with a LNmetastasis 2 hours after a peritumoral injection of either EGFR-targetedMAPS(C) or control RG16-conjugated AuNPs (D) and a normal mouse (E) 2 hours after a submucosal injection of EGFR-targeted MAPS. Hemoglobin (sPAHb) isdepicted in red–blue, as determined by the oxygen saturation, while the presence of cancer cells labeled with MAPS (sPAMAPS) is depicted in yellow(see an arrow pointing to a micrometastasis in C); the anatomic location of a cervical LN is outlined by a dashed white line. Note the strong sPAMAPS signalin tumor-bearing mice injected with EGFR-targeted MAPS. F, the LNs were split into three categories for analysis: (i) LNs containing metastases inmice injectedwith EGFR-targetedMAPS (N¼ 7), (ii) LNs in tumor-bearingmice injectedwith RG16-conjugated AuNPs (N¼ 7), and (iii) LNswithoutmetastasisin mice with or without a primary tumor injected with EGFR-targeted MAPS (N¼ 8). The total signal of activated MAPS was used as indicator of metastases.The metastatic LNs in tumor-bearing mice exhibit a statistically significant increase in the sPAMAPS signal. The P values are from a Mann–Whitney Utest and error bars correspond to one standard deviation. G, a 3D reconstruction of the ultrasound images with the SLN volume segmented from the2D ultrasound images (cyan), with the overlaid 3D sPA image showing the volumetric distribution of the sPAMAPS signal. All scale bars, 1 mm.
Molecular Photoacoustic Imaging of LN Metastases
www.aacrjournals.org Cancer Res; 74(19) October 1, 2014 5401
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

normal physiologic extremes of blood oxygen saturation (e.g.,arterial and venous blood). Pixels below 60% SO2 were coloredblue. The intensity of the sPA signal was determined from theaverage photoacoustic signal.
The SLNswere identified andmanually segmented using the3-D visualization of ultrasound data. Only the signal inside orwithin 100 mm of the LNs was considered. The estimatedconcentrations were filtered with a 5 � 5 � 5 voxel medianfilter to suppress physiologic motion. The ratio between theresidual of the least squares approximation and the averageconcentration was used as a threshold to discard pixels whosespectra did not correlate strongly with the analyzed absorbers.In general, most pixels were retained during this operation.Wenoticed that this step mainly led to a suppression of the signalgenerated at the surface of the skin (because melanin was notincluded in spectral analysis). Finally, the total signal stem-ming from the activated MAPS was summed throughout eachnode to be used as an indicator of metastasis.
Histology and optical imagingFormalin-fixed, paraffin-embedded samples were sliced in
100-mm levels. The samples were stained using hematoxylinand eosin (H&E) stain to show tissue morphology and silverstain to detect gold and anti-EGFR rabbit polyclonal anti-bodies (Sigma HPA018530) for molecular-specific identifi-cation of EGFR(þ) metastatic cells. A Leica DMI 3000Bmicroscope coupled to a DFC 290 camera was used torecord color images.
Dark-field and hyperspectral imaging were performed on aLeica DM 6000 microscope with a 20� objective and xenonlamp. Hyperspectral imaging was carried out with PARISSsystem (Lightform, Inc.) attached to the Leica DM 6000 micro-scope. The system was calibrated using a multi-ion discharge
lamp (MIDL) with known emission spectrum. To normalizescattering spectra with the incident lamp spectrum, a spec-trum of the excitation xenon lamp was acquired using aLabsphere Spectralon calibrated scattering substrate.
Statistical analysisA Lilliefors test was used to determine that the sPAMAPS
signal in the LNs did not follow a normal distribution. Anonparametric Mann–Whitney U test was used to test thenull hypothesis that the sPAMAPS signal in metastatic nodeswas not significantly greater than the controls. All LNs frommice injected with EGFR-targetedMAPSwere used to evaluatethe sensitivity and specificity of the imaging technique. Areceive operator characteristic (ROC) curve constructed fromthe sPAMAPS signal was used to determine the threshold forsensitivity and specificity.
ResultsThree distinct states can be encountered in vivo after
injection of MAPS (Fig 1A): (i) cells with no MAPS present atthe site of interest, (ii) no interactions between cells anddelivered MAPS due to the lack of a molecular biomarker ofinterest, and (iii) molecular-specific interactions between cellsand targeted MAPS. Hyperspectral and dark-field opticalmicroscopy of cell cultures simulating these three states (Fig.1) show that delivery ofMAPS increases optical absorption andscattering in the wavelength range near nanoparticle plasmonresonance peak (Fig. 1B and D), while molecular-specificinteractions between MAPS and EGFR-expressing cancer cellsare associated with plasmon resonance coupling, resulting instriking optical changes including red spectral shift in excess of100 nmand broadening of nanoparticle extinction spectra (Fig.1B and E). This sensing method is unique among optical
SLN
SLNA B C
D
Figure 4. Spatial correlationbetween sPAMAPS signal andbioluminescence. A and B,photograph with overlaidbioluminescence image showing asmall metastasis at the edge of theLN. C, ultrasound image showingthe imaging plane depicted in D. E,an ultrasound image of the planedepicted inDandoverlaid sPAMAPS
signal shows twomicrometastasesthat generated thebioluminescence signal and a thirdthat was undetected bybioluminescence.
Luke et al.
Cancer Res; 74(19) October 1, 2014 Cancer Research5402
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

activatable imaging agents, which typically rely on enzymaticcleavage for activation and, therefore, are mostly limited todetection of various proteinases (13).To establish the utility of MAPS in vivo, we performed sPA
imaging with MAPS for noninvasive detection of micrometas-tases in the lymphatics of the orthotopic nudemouse model ofSCCOC (28). Either EGFR-targeted MAPS or control AuNPsconjugated with a nonspecific RG16 monoclonal antibodywere injected peritumorally and were allowed to drain to thecervical LNs of tumor-bearing mice. In clinical practice, a
similar injection of radionuclide tracers is routinely performedto identify the location of LNs; however, it does not allow for thedetection of cancer cells. The RG16 antibody acts as a non-specific control because it targets heavy chains of rabbit IgG/IgM/IgA, which are not present in mouse or FaDu cells. Theinjected dose was approximately 1.6 pmol, which is signifi-cantly less than a dose of AuNPs with any reported cytotoxicityin vivo (30). The cervical LNs, the site ofmicrometastatic foci inthis mouse model (28), were identified using ultrasoundimaging.
25
45
65
85
105
125
Time after injection (m
in)
Before injection
A
G
F
E
D
C
B
Metastatic nodeNormal node
LN SLN
Figure 5. Kinetics of MAPSinteraction with micrometastasis.Combined ultrasound and sPAimage of a 2D cross-sectioncontaining two LNs (center), and4� enlarged sPA images of aregion on the border of the left LN(left) and right LN (right; A) before,25 (B), 45 (C), 65 (D), 85 (E), 105 (F),and 125 (G) minutes after theinjection of MAPS. The steadilygrowing region of activated MAPSin the right LN indicates that MAPSare gradually being delivered toand are interacting with cancercells on the border of the LN. Scalebars, 1 mm.
Molecular Photoacoustic Imaging of LN Metastases
www.aacrjournals.org Cancer Res; 74(19) October 1, 2014 5403
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

To differentiate cancer cells labeled with MAPS from thebackground, we implemented an image analysis algorithm tospectroscopically resolve the twomajor contributors to photo-acoustic signal in our studies—hemoglobin (sPAHb) andMAPS-labeled cancer cells (sPAMAPS)—in the red-near-infrared(NIR) wavelength region (Fig. 2). The relative contributions ofsPAHb and sPAMAPS to the overall photoacoustic signal weredetermined via a linear least squares method (29). The SO2, ascalculated by the ratio between the concentration of oxygen-ated hemoglobin and total hemoglobin, was used to assign acolor to the sPAHb signal. No significant changes in the red-NIRphotoacoustic signal intensity from LNs were evident in con-trol groups for several hours following injection ofMAPSdue tolow absorption of noninteracting MAPS in this spectral regionand no apparent changes in blood flow. In contrast, a strongincrease in the photoacoustic signal was observed in LNsharboring metastases less than 2 hours after administrationof MAPS (Fig. 2).
Overlaid ultrasound and sPA images of cervical LNs(Fig. 3C–E) depicting the anatomy (gray) and contributionsfrom sPAHb (blue/red) and sPAMAPS (yellow) 2 hours afterthe peritumoral injection of MAPS show the ability of ourmethod to detect micrometastases in the lymphatics withhigh spatial resolution. LNs are identifiable by a dark bean-shaped region in the ultrasound images (outlined usingwhite dashed line); the hypoechoic contrast is typical forLNs in ultrasound imaging (see an example in Supplemen-tary Fig. S1; ref. 31). The injection of EGFR-targeted MAPSleads to a strong increase in the sPAMAPS signal from the LNs
with micrometastases (Fig. 3C). A 3D reconstruction of theultrasound/sPA images shows that the sPAMAPS signal isconstrained to a small region on the edge of the LN (Fig. 3G),which is consistent with the location of metastases observedin this mouse model. Furthermore, there was excellentcorrelation between the spatial location of the sPAMAPS
signal and the in situ bioluminescence signal from meta-static cells (Fig. 4).
Overall, tumor-bearing mice injected with EGFR-targetedMAPS exhibit a statistically significant increase in sPAMAPS
signal from metastatic LNs (N ¼ 7 nodes) over LNs of controlmice injected with RG16-conjugated AuNPs (N¼ 7 nodes; P¼0.006) and either LNs of normal mice (N¼ 5 nodes) or healthyLNs in tumor-bearing mice (N¼ 3 nodes) injected with EGFR-targetedMAPS (totalN¼ 8 nodes; P¼ 0.005; Fig. 3F). Statisticalanalysis of the data results in a sensitivity of 100% and aspecificity of 87.5% of our method in detection of LN micro-metastasis. The results show that our method is able to detectmetastases as small as 50 mm (which was determined bymeasuring the longest diameter of the metastasis across allhistology slices), which corresponds to approximately 30 cells(if we assume a spherical metastasis and cell diameter of 15mm). The single false-positive came from a LN in a tumor-bearing mouse with a confirmed metastasis in the contralat-eral cervical LN. Given the fact that bilateral LN metastasesdeveloped in a large portion of mice in this study (21% ofmetastatic mice), it is possible that MAPS are more sensitivethan the validation using histology (the current gold standard)and this false-positive represents an occult metastasis.
A
D
G
B
E
H
C
F
I
Metastatic mouseEGFR-targeted MAPS
Metastatic mouseRG16-conjugated AuNPs
Non–tumor-bearing mouseEGFR-targeted MAPS
Figure 6. Histologic evaluation ofexcised LNs. A andB, H&E stainingof LNs from mice with positivebioluminescent signal in LNsshows the subcapsular formationof micrometastases (dashed redoutline) near an afferent lymphvessel. C, the morphology of a LNfrom a normal mouse is shown forreference. D and E, at highmagnification, the irregular shapeand large nuclei indicate presenceof cancer cells in H&E sections. F, anormal population of lymphaticcells is seen in normal mice.Immunohistochemical stainingshows elevated expression ofEGFR in the micrometastases(G and H) and negligible EGFRexpression in normal nodes (I).Scale bars, 200 mm (A–C) and100 mm (D–I).
Luke et al.
Cancer Res; 74(19) October 1, 2014 Cancer Research5404
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

Continuous sPA imaging of cervical LNs immediately fol-lowing MAPS injection shows progressive labeling of cancercells over the course of 2 hours, indicating quick delivery anduptake of the nanoparticles (Fig. 5). A steady increase insPAMAPS signal amplitude and volume is seen in a smalllocalized region on the border of the LN. The vasculature thatis visible throughout the rest of the image experiences littlevariation over the same timescale. The contrast generated byMAPS generally tended to plateau after 2 to 3 hours. Thisindicates that the optimal time point to perform imagingoccurs in the first few hours after the injection. Furthermore,the 2-hour timescale is consistent with nanoparticle drainagethrough the lymphatics observed in vivo (32, 33) and cellularuptake of MAPS observed in vitro (34). Taken together, theseobservations provide additional support to the conclusion thatthe highly localized signal is due to tumor cell–mediatedactivation of MAPS.H&E staining (Fig. 6A–F) confirmed the presence of the
metastases that were indicated by the bioluminescenceimaging and were detected by sPA imaging of MAPS. Themetastases had a tendency to form in the subcapsular regionof the node near the afferent lymphatic vessel or within the
vessel itself. This trend is in excellent correlation with theregions of elevated sPAMAPS and bioluminescence signal(Figs. 3, 4, and 6). Immunohistochemistry confirmed theoverexpression of EGFR in the micrometastases (Fig. 6G–I).Furthermore, hyperspectral dark-field reflectance opticalmicroscopy of the excised tissue slices showed strong label-ing of tumor cells and plasmon resonance coupling betweenMAPS at the location of the micrometastases (Fig. 7). Nosuch signal was observed in the metastatic mice injectedwith RG16-conjugated AuNPs. These results further indicatethat activation of MAPS is specific to EGFR overexpressingcells.
DiscussionMolecular-specific imaging of small cellular clusters in vivo
at substantial depth remains a great challenge in modernbiology andmedicine (35). Attempts have beenmade to extendvirtually every biomedical imaging modality, including PET(36), MRI (37), ultrasound imaging (38, 39), optical imaging(40), and photoacoustic imaging (21, 22), to localize molecularexpressions in vivo. Nevertheless, accurate measurements of
Metastatic mouse
EGFR-targeted MAPS
Metastatic mouse
RG16-conjugated AuNPs
A B
C D
400
800
Peak w
aveleng
th (n
m)
Scatteringintensity (a.u.)
Min Max
Figure 7. Optical hyperspectralmicroscopy of specificnanoparticle uptake and plasmonresonance coupling of MAPS. H&Estains of metastases (dashed redoutline) in mice injected with eitherEGFR-targetedMAPS (A) or RG16-targeted AuNPs (B). C and D, dark-field reflectance hyperspectralmicroscopy of adjacent tissueslices shows tumor cell uptake ofEGFR-targeted MAPS andplasmon resonance couplingbetween theMAPS as evident froma strong red-NIR shift in theirplasmon resonances, with noplasmon resonance couplingobserved after the injection ofRG16-targeted AuNPs. The colorin C and D indicates thewavelength of peak scatteringintensity, while the brightnessindicates the magnitude ofscattering; the range of colors isdepicted in the color bar. Scalebars, 100 mm.
Molecular Photoacoustic Imaging of LN Metastases
www.aacrjournals.org Cancer Res; 74(19) October 1, 2014 5405
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

molecular expressions in a tissue remain a difficult task.Indeed, it is commonly assumed that the presence of a molec-ularly targeted contrast agent correlates to the level of expres-sion of the targeted molecule. What this assumption fails toconsider is that delivery of a contrast agent to a site of interestand interaction between the agent and its target are twoindependent events. Therefore, passive accumulation of acontrast agent in a tissue (e.g., via the enhanced permeabilityand retention effect in tumors; ref. 41) leads to decreasedspecificity in molecular sensing (35, 42).
Advanced optical imaging techniques, such as F€orster Res-onance Energy Transfer (43) or fluorescent imaging usingactivatable probes (13), are able to provide a much morespecific visualization of molecular expressions. However, thesemethods suffer from low penetration depth (less than onemillimeter in the ballistic regime of photon transport) or poorresolution and sensitivity at greater depths (40). Furthermore,fluorescent probes are prone to photobleaching. All of thesefactors severely limit clinical applicability of optical techniquesfor molecular detection of diseases, including micrometas-tases. Photoacoustic imaging addresses these limitationsby combining the high contrast of optical imaging with theexcellent resolution of ultrasound imaging at depths up to 5 cm(20–22, 44). In addition, plasmonic nanoparticles characterizedby enhanced optical absorption and photostability providestrong contrast in photoacoustic imaging (19, 44, 45). However,previous efforts to combine plasmonic nanoparticles with invivo photoacoustic imaging have not addressed the fundamen-tal challenge in specificity that most other molecular imagingmodalities suffer from: nanoparticles that have interacted witha molecule of interest cannot be differentiated from those thathave simply been delivered to the region.
Our approach based on nanoscale interactions betweencells and MAPS provides a straightforward mechanism todecouple nanoparticle delivery from molecular interactions(Supplementary Fig. S2). Our results show an excellentability to detect small colonies of cancerous cells. Indeed,the 100% sensitivity and 87.5% specificity of sPA imaging ofMAPS are significantly better than the results obtained usingother noninvasive imaging modalities (46). For example,PET, while more sensitive than many other radiographicmodalities, has 50% sensitivity and 87% specificity in detec-tion of impalpable cervical metastases in human patientswith oral cancer (47). Demonstrated here is the capacity todetect metastatic tumors consisting of just few tens ofmalignant cells deep inside tissue.
The translation of this technique to the clinic will requireboth a clinical imaging system and a clinically approvedcontrast agent. The clinical imaging systemmust be developedto image tissues at 3 to 5 cm depth. This could be achieved bycombining a clinically relevant lower frequency ultrasoundtransducer (e.g., 10 MHz center frequency) with a tunable lasersource in the red-NIR spectral region that provides sufficientpulse power at clinically save irradiation levels; this combina-tion will achieve light penetration in tissue and propagation ofacoustic waves that are appropriate for LN imaging inmultipleanatomic locations including LNs associated with oral and
breast cancers. In general, we do not expect the approach todepend on the location of the primary tumor or its proximityto the SLN. What is important is that the primary tumor needsto be accessible for an injection of the MAPS and the LNs mustbe accessible for photoacoustic imaging (i.e., they must bewithin a few centimeters of a handheld or endoscopic imagingprobe).We expect that the sensitivity of our imagingmethod inthe clinic will be primarily limited by the ability to deliver lightdeep in tissue. In addition, while the dose of gold used in thisstudy is well below any previously reported toxicity threshold(30), gold nanoparticles are not yet accepted for widespreadclinical use. One of the concerns associated with gold nano-particles is potential long-term toxicity because particles largerthan 5 to 6 nm are not easily cleared from the body. Previousstudies have shown that nanoparticles with sizes below ca.6 nm can undergo efficient clearance through urine and feces(48–50). Therefore, scaling down the MAPS to 5 nm is a viablepath toward clinical acceptance. Because the MAPS are deliv-ered through the lymphatics, the short half-life of small par-ticles in the bloodstream will not affect our technology asopposed to applications requiring systemic delivery wheresmall particles can undergo quick renal clearance. Overall, theclinical translation of the developed method is possible andanticipated.
Disclosure of Potential Conflicts of InterestS.Y. Emelianov and K.V. Sokolov have ownership interest in and are con-
sultants/advisory boardmembers for NanoHybrids, Inc. No potential conflicts ofinterest were disclosed by the other authors.
Authors' ContributionsConception and design: G.P. Luke, J.N. Myers, S.Y. Emelianov, K.V. SokolovDevelopment of methodology: G.P. Luke, S.Y. Emelianov, K.V. SokolovAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): G.P. LukeAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): G.P. Luke, J.N. Myers, S.Y. Emelianov, K.V. SokolovWriting, review, and/or revision of the manuscript: G.P. Luke, J.N. Myers,S.Y. Emelianov, K.V. SokolovAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): S.Y. Emelianov, K.V. SokolovStudy supervision: S.Y. Emelianov, K.V. Sokolov
AcknowledgmentsThe authors thank Dr. Aristarchos Papagiannaros of the University of
Texas MD Anderson Cancer Center for his help with nanoparticle conjuga-tion, tumor inoculation, and histology in preliminary studies, Dr. PratixaJoshi, Dr. Justina Tam, and Mr. Chun-Hsien Wu of The University of Texas atAustin for their assistance with nanosphere synthesis and antibody conju-gation, Dr. Timothy Larson at The University of Texas at Austin for his helpwith optical microscopy and hyperspectral image processing of cell cultures,Ms. Sally Amen of the University of Texas at Austin for consulting on thestatistical analysis, and Mrs. Nancy Wick Otto of the University of Texas MDAnderson Cancer Center Science Park for her expertise on immunohis-tochemistry optimization and processing.
Grant SupportThe work was supported, in part, by grants from the NIH (R01EB008101 and
F31CA168168).The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisementin accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received March 19, 2014; revised June 13, 2014; accepted July 23, 2014;published OnlineFirst August 8, 2014.
Luke et al.
Cancer Res; 74(19) October 1, 2014 Cancer Research5406
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

References1. Gershenwald JE, Thompson W, Mansfield PF, Lee JE, Colome MI,
Tseng C-H, et al. Multi-institutional melanoma lymphatic mappingexperience: the prognostic value of sentinel lymph node status in612 stage I or II melanoma patients. J Clin Oncol 1999;17:976.
2. Stoeckli SJ, Steinert H, Pfaltz M, Schmid S. Sentinel lymph nodeevaluation in squamous cell carcinoma of the head and neck. Otolar-yngol Head Neck Surg 2001;125:221–6.
3. Veronesi U, Paganelli G, Galimberti V, Viale G, Zurrida S, Bedoni M,et al. Sentinel-node biopsy to avoid axillary dissection in breast cancerwith clinically negative lymph-nodes. Lancet 1997;349:1864–7.
4. Bergkvist L, Frisell J. Multicentre validation study of sentinel nodebiopsy for staging in breast cancer. Br J Surg 2005;92:1221–4.
5. Ronka R, Smitten K, Sintonen H, Kotomaki T, Krogerus L, Leppanen E,et al. The impact of sentinel node biopsy and axillary staging strategyon hospital costs. Ann Oncol 2004;15:88–94.
6. Goldberg J, Riedel E, MorrowM, Van Zee K.Morbidity of sentinel nodebiopsy: relationship between number of excised lymph nodes andpatient perceptions of lymphedema. Ann Surg Oncol 2011;18:2866–72.
7. Langer I, Guller U, Berclaz G, Koechli OR, Schaer G, Fehr MK, et al.Morbidity of sentinel lymph node biopsy (SLN) alone versus SLN andcompletion axillary lymph node dissection after breast cancer surgery:a prospective swiss multicenter study on 659 patients. Ann Surg2007;245:452–61.
8. Scoggins CR, Martin RC, Ross MI, Edwards MJ, Reintgen DS, UristMM, et al. Factors associated with false-negative sentinel lymph nodebiopsy in melanoma patients. Ann Surg Oncol 2010;17:709–17.
9. Cohen SM, Fishinghawk BG, Cohen MS. Translational imaging oflymphatics in cancer. Adv Drug Deliv Rev 2011;63:956–62.
10. Wunderbaldinger P. Problems and prospects of modern lymph nodeimaging. Eur J Radiol 2006;58:325–37.
11. Wagner JD, Schauwecker DS, Davidson D, Wenck S, Jung SH,Hutchins G. FDG-PET sensitivity for melanoma lymph node metas-tases is dependent on tumor volume. J Surg Oncol 2001;77:237–42.
12. vanderHoeven JJ,HoekstraOS,ComansEF, Pijpers R, BoomRP, vanGeldere D, et al. Determinants of diagnostic performance of [F-18]Fluorodeoxyglucose positron emission tomography for axillarystaging in breast cancer. Ann Surg 2002;236:619–24.
13. Savariar EN, Felsen CN, Nashi N, Jiang T, Ellies LG, Steinbach P, et al.Real-time in vivo molecular detection of primary tumors and metas-tases with ratiometric activatable cell-penetrating peptides. CancerRes 2013;73:855–64.
14. Kim S, Lim YT, Soltesz EG, DeGrand AM, Lee J, Nakayama A, et al.Near-infrared fluorescent type II quantumdots for sentinel lymph nodemapping. Nat Biotechnol 2004;22:93–7.
15. Goldberg BB, Merton DA, Liu J-B, Thakur M, Murphy GF, NeedlemanL, et al. Sentinel lymph nodes in a swine model with melanoma:contrast-enhanced lymphatic US1. Radiology 2004;230:727–34.
16. Harisinghani MG, Barentsz J, Hahn PF, Deserno WM, Tabatabaei S,vande Kaa CH, et al. Noninvasive detection of clinically occultlymph-node metastases in prostate cancer. N Engl J Med 2003;348:2491–9.
17. Zhang HF, Maslov K, Stoica G, Wang LV. Functional photoacousticmicroscopy for high-resolution and noninvasive in vivo imaging. NatBiotechnol 2006;24:848–51.
18. Eghtedari M, Oraevsky A, Copland JA, Kotov NA, Conjusteau A,Motamedi M. High sensitivity of in vivo detection of gold nanorodsusing a laser optoacoustic imaging system. Nano Lett 2007;7:1914–8.
19. Luke GP, Yeager D, Emelianov SY. Biomedical applications of photo-acoustic imaging with exogenous contrast agents. Ann Biomed Eng2012;40:422–37.
20. Diebold GJ, Khan MI, Park SM. Photoacoustic "signatures" of partic-ulate matter: optical production of acoustic monopole radiation.Science 1990;250:101–4.
21. Wang LV, Hu S. Photoacoustic tomography: in vivo imaging fromorganelles to organs. Science 2012;335:1458–62.
22. Beard P. Biomedical photoacoustic imaging. Interface Focus 2011;1:602–31.
23. Song KH, Stein EW, Margenthaler JA, Wang LV. Noninvasive photo-acoustic identification of sentinel lymph nodes containing methyleneblue in vivo in a rat model. J Biomed Opt 2008;13:054033–6.
24. Song KH, Kim C, Cobley CM, Xia Y, Wang LV. Near-infrared goldnanocages as a new class of tracers for photoacoustic sentinel lymphnode mapping on a rat model. Nano Lett 2008;9:183–8.
25. Barnes CJ, Kumar R. Biology of the epidermal growth factor receptorfamily. Cancer Treat Res 2004;119:1–13.
26. Kumar S, Aaron J, Sokolov K. Directional conjugation of antibodies tonanoparticles for synthesis of multiplexed optical contrast agents withboth delivery and targeting moieties. Nat Protoc 2008;3:314–20.
27. Niidome T, Yamagata M, Okamoto Y, Akiyama Y, Takahashi H,Kawano T, et al. PEG-modified gold nanorods with a stealth characterfor in vivo applications. J Control Release 2006;114:343–7.
28. Myers JN, Holsinger FC, Jasser SA, Bekele BN, Fidler IJ. An orthotopicnude mouse model of oral tongue squamous cell carcinoma. ClinCancer Res 2002;8:293–8.
29. Kim S, Chen Y-S, Luke GP, Emelianov SY. In vivo three-dimensionalspectroscopic photoacoustic imaging for monitoring nanoparticledelivery. Biomed Opt Express 2011;2:2540–50.
30. KhlebtsovN,DykmanL.Biodistribution and toxicity of engineeredgoldnanoparticles: a review of in vitro and in vivo studies. Chem Soc Rev2011;40:1647–71.
31. Richards PS, Peacock TE. The role of ultrasound in the detection ofcervical lymph node metastases in clinically N0 squamous cell carci-noma of the head and neck. Cancer Imaging 2007;7:167–78.
32. Cai X, Li W, Kim CH, Yuan Y, Wang LV, Xia Y. In vivo quantitativeevaluation of the transport kinetics of gold nanocages in a lymphaticsystem by noninvasive photoacoustic tomography. ACS Nano2011;5:9658–67.
33. LukeGP, BashyamA,HomanKA,Makhija S,ChenY-S, Emelianov SY.Silica-coated gold nanoplates as stable photoacoustic contrastagents for sentinel lymph node imaging. Nanotechnology 2013;24:455101.
34. Aaron J, Travis K, Harrison N, Sokolov K. Dynamic imaging of molec-ular assemblies in live cells based on nanoparticle plasmon resonancecoupling. Nano Lett 2009;9:3612–8.
35. Weissleder R. Molecular imaging in cancer. Science 2006;312:1168–71.
36. Gambhir SS. Molecular imaging of cancer with positron emissiontomography. Nat Rev Cancer 2002;2:683–93.
37. Lee J-H, Huh Y-M, Jun Y-W, Seo J-W, Jang J-T, Song H-T, et al.Artificially engineered magnetic nanoparticles for ultra-sensitivemolecular imaging. Nat Med 2006;13:95–9.
38. Kaufmann BA, Lindner JR. Molecular imaging with targeted contrastultrasound. Curr Opin Biotechnol 2007;18:11–6.
39. Foster FS, Pavlin CJ, Harasiewicz KA, Christopher DA, Turnbull DH.Advances in ultrasound biomicroscopy. Ultrasound Med Biol2000;26:1–27.
40. Weissleder R, Ntziachristos V. Shedding light onto live moleculartargets. Nat Med 2003;9:123–8.
41. Maeda H. The enhanced permeability and retention (EPR) effect intumor vasculature: the key role of tumor-selective macromoleculardrug targeting. Adv Enzyme Regul 2001;41:189–207.
42. Massoud TF, Gambhir SS.Molecular imaging in living subjects: seeingfundamental biological processes in a new light. Gen Dev 2003;17:545–80.
43. Jares-Erijman EA, Jovin TM. FRET imaging. Nat Biotechnol 2003;21:1387–95.
44. Emelianov SY, Li P-C, O'Donnell M. Photoacoustics for molecularimaging and therapy. Physics Today 2008:34–9.
45. JainPK, LeeKS, El-Sayed IH, El-SayedMA.Calculated absorption andscattering properties of gold nanoparticles of different size, shape, andcomposition: applications in biological imaging and biomedicine.J Phys Chem B 2006;110:7238–48.
46. Stuckensen T, Kov�acs AF, Adams S, Baum RP. Staging of the neck inpatients with oral cavity squamous cell carcinomas: a prospectivecomparison of PET, ultrasound, CT and MRI. J Craniomaxillofac Surg2000;28:319–24.
www.aacrjournals.org Cancer Res; 74(19) October 1, 2014 5407
Molecular Photoacoustic Imaging of LN Metastases
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

47. Kyzas PA, Evangelou E, Denaxa-Kyza D, Ioannidis JP. 18F-fluoro-deoxyglucose positron emission tomography to evaluate cervicalnode metastases in patients with head and neck squamous cellcarcinoma: a meta-analysis. J Natl Cancer Inst 2008;100:712–20.
48. Choi HS, Liu W, Misra P, Tanaka E, Zimmer JP, Ipe BI, et al. Renalclearance of quantum dots. Nat Biotechnol 2007;25:1165–70.
49. Schipper ML, Iyer G, Koh AL, Cheng Z, Ebenstein Y, Aharoni A, et al.Particle size, surface coating, and PEGylation influence the biodistri-bution of quantum dots in living mice. Small 2009;5:126–34.
50. Park J-H, Gu L, Von Maltzahn G, Ruoslahti E, Bhatia SN, Sailor MJ.Biodegradable luminescent porous silicon nanoparticles for in vivoapplications. Nat Mater 2009;8:331–6.
Cancer Res; 74(19) October 1, 2014 Cancer Research5408
Luke et al.
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796

2014;74:5397-5408. Published OnlineFirst August 8, 2014.Cancer Res Geoffrey P. Luke, Jeffrey N. Myers, Stanislav Y. Emelianov, et al. Targeted Plasmonic NanosensorsPhotoacoustic Detection of Micrometastases Using Molecularly Sentinel Lymph Node Biopsy Revisited: Ultrasound-Guided
Updated version
10.1158/0008-5472.CAN-14-0796doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2014/08/16/0008-5472.CAN-14-0796.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/74/19/5397.full#ref-list-1
This article cites 49 articles, 7 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/74/19/5397.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/74/19/5397To request permission to re-use all or part of this article, use this link
on September 24, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 8, 2014; DOI: 10.1158/0008-5472.CAN-14-0796