Embed Size (px)
Citation preview

Sensory stimulation and Snoezelen in the management of people with cognitive impairment
Dr Lesley CollierSenior Lecturer



What do we mean by sensory stimulation and Snoezelen
Snoezelen Sensory stimulation

Development of sensory stimulation and Snoezelen
Key areas of practice
• Learning disabilities (Autism, Downs syndrome)
• Older persons mental health (Dementia, depression)
• Acute mental health settings (Stress management, Schizophrenia)
• Palliative care (pain management, end of life care)
• Maternity care (pain management, stress management)
• Neurology (acquired brain injury, sensory retraining)

Problems identified
• Poor concentration
• Restlessness / wandering
• Shouting
• Aggressive behaviour
• Severe disorientation
• Unable to engage in purposeful activity
• General mood disturbance
• Anxiety
• Inability to follow simple instructions
• Severe memory loss
• Loss of social skills
• Physical faility

Sensory challenges
Person
Sensory processing
Just right challenge
Environmental demand
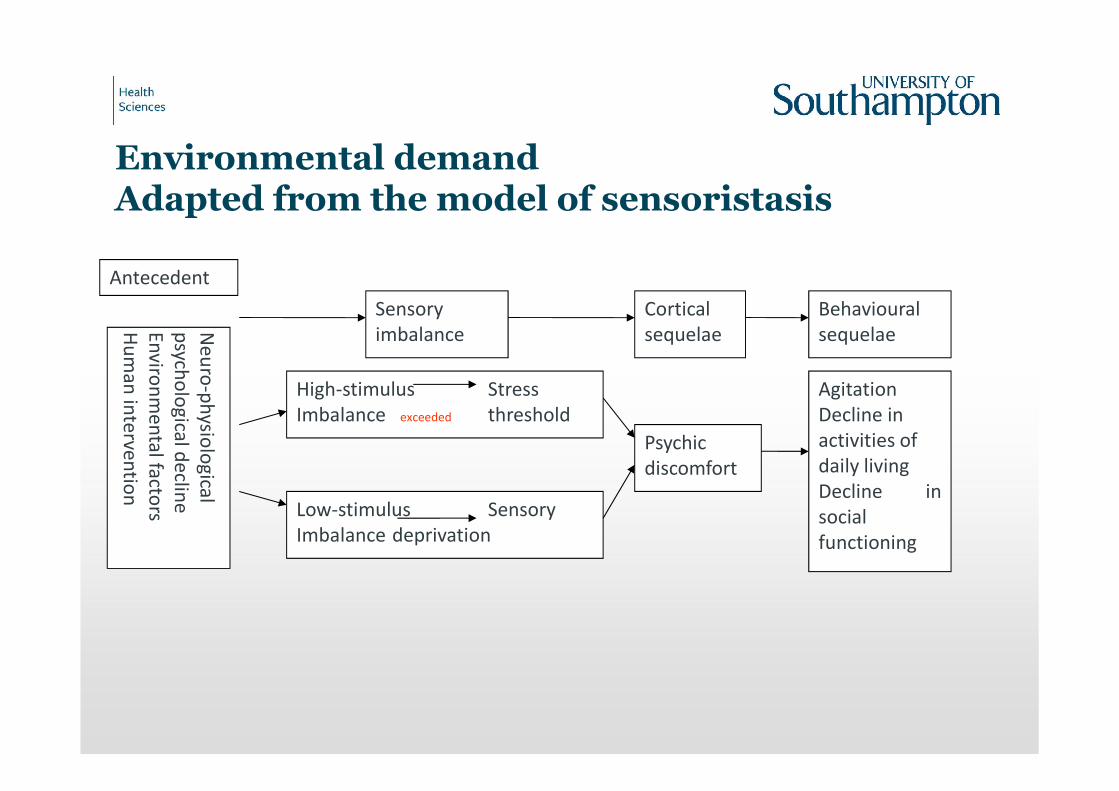
Environmental demandAdapted from the model of sensoristasis
Sensoryimbalance
Corticalsequelae
Behaviouralsequelae
Low-stimulus SensoryImbalance deprivation
Psychicdiscomfort
AgitationDecline in activities of daily livingDecline insocialfunctioning
High-stimulus StressImbalance exceeded threshold
Antecedent
Neu
ro-p
hysio
logical
psych
olo
gicaldeclin
eEn
viron
men
talfactors
Hu
man
interven
tion

Tenets of the model
• An imbalance may occur as a result of neurophysiological or environmental factors
• Too much high-stimulus activity can result in stress threshold being exceeded
• This will occur at a lower level if activity is unpleasant or processing is too fast.
• Too lower stimulus activity may lead to sensory deprivation.

Looking at skill levels
Sensory level
Perception Skill acquisition
(Normal development)
(Cognitive impairment / decline)

Sensory integration is critical for human development and function
Sensory intake
Sensory integration
Planning and
organisation of behaviour
Adaptive behaviour
and learning
Feedback
Attention
Arousal
Sensory modalities
Motivation and drive

Five basic assumptions
Potential for neuroplasticity
Interaction between higher order (cortical) and lower order (subcortical ) areas to modulate sensory input
Neurophysiological development of sensory integration follows a sequential pattern
Adaptive response – ability to adjust performance according to environmental demand
Presence of inner drive to meet and master a challenge

FlowCsikszentmihalyi, 1975
High cognitivedemand
LowCognitivedemand
Ch
allenge
Low Skills High
Anxiety
Flow
ApathyBoredom

The model of sensory processingDunn, 2002
Sensory processing patterns are based on how the nervous system reacts to input and how the person responds to that input.
Nervous system thresholds – thresholds for responding along a continuum based on sensory preference
Self regulation strategies - active management of sensory input

Patterns of sensory processing assessed by the Sensory Profile
Responding strategies
Threshold / reactivity Passive Active
High threshold with low reactivity
Low registration (Bystander)
Does not notice sensory events or is slow to respond
Sensory seeking (Seeker)
Looks for sensory experiences
Low threshold with high reactivity
Sensory sensitivity (Sensor)
Readily notices sensory stimuli, may be distracted by them
Sensory avoider (Avoider)
Deliberately acts to reduce or prevent exposure to sensory stimuli

The sensory tool box
• Sight - visual
• Sound - Auditory
• Touch - Somatosensory / vibration
• Taste - Gustatory and texture
• Smell - Olfactory
• Movement - Vestibular / proprioception

The use of multisensory approaches to improve function performance of people with moderate to severe dementia.
Dr Lesley Collier

Research questions
• To what extent do MSEs influence functional performance compared with a control activity (gardening)?
• To what extent are mood and behaviour affected by MSEs compared with the control activity group?
• To what extent is the sensory profile of the individual associated with the response to the MSE?

Randomised, single blind, repeated measures design
Baseline Intervention (sessions 1 to 12) Follow up
Pilot and Recruitment
Baseline assessment
SMMSE
GBS
Sensory profile
PAL
Randomised to:
MSE or
Gardening
Pre-session assessment
AMPS motor
AMPS process
NRS
Post-session assessment
AMPS motor
AMPS process
NRS
1/12 after Session 12
AMPS motor
AMPS process
NRS

Assessment of Motor and Process Skills (AMPS) Fisher 2003
• Standardised observational assessment of functional performance
• Motor and Process skills in ADL performance
• Uses Rasch analysis to adjust for skill complexity, rater severity and task difficulty
• Sensitive to change
• Significant change ≥0.5 logits

Baseline data: Recruitment sites
Recruitment sites MSE Gardening
NHS ward Assessment ward
NHS ward Continuing care
Day Hospital
Private Nursing Home
5 (29%)
6 (35%)
4 (23%)
2 (12%)
4 (31%)
4 (31%)
4 (31%)
1 (8%)
χ2(3, N = 30) = 0.6, p = 1.0

Baseline to last treatment session
• Both Motor and Process scores improved by the interventions
• No group differences
• Scores equally improved for MSE and gardening
Baseline Last tmt session
Baseline Last tmt session
MSE
Gardening-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
Motor Process
MSE
Gardening

Mean delta AMPS motor scores
-1
-0.5
0
0.5
1
1.5
2
2.5
3
3.5
4
1 2 3 4 5 6 7 8 9 10 11 12
Sessions
AM
PS
delt
a s
co
ress
MSE group
Gardening group

Mean delta AMPS process scores
-1
-0.5
0
0.5
1
1.5
2
1 2 3 4 5 6 7 8 9 10 11 12
Sessions
AM
PS
delt
a s
co
res
MSE group
Gardening group

Percentage improvers
6 7 %
4 5 % 4 7 %
3 0 %
0
10
20
30
40
50
60
70
80
Motor Process
Perc
en
tag
eMSE
Gardening
Motor scores t(30) = 2.28, p = .030Process scores, ns differences
p < .05

Baseline to last treatment session
• NRS scores improved (reduced) by the interventions
• No group differences
• Scores equally improved for MSE and gardening
Before
After
MSE
Gardening
0
5
10
15
20
25
30
35
40
NR
S M
ea
n
sc
ore
MSE
Gardening

Sensory stimulation and Snoezelen in the management of people with dementia
Dr Lesley CollierSenior Lecturer

What do we mean by sensory stimulation and Snoezelen
Snoezelen Sensory stimulation

Sensory challenges experienced by people with dementia
Person with
dementia
Sensory processing
Just right challenge
Environmental demand

Assessment tools to assess sensory needs
• Adult sensory profile (Brown & Dunn)
• Sensory profiling tool (Rompa)
• The Pool Activity Levels occupational Profiling Tool
(Pool, 2012)

Adult sensory profile

The model of sensory processingDunn, 2002
Sensory processing patterns are based on how the nervous system reacts to input and how the person responds to that input.
Nervous system thresholds – thresholds for responding along a continuum based on sensory preference
Self regulation strategies - active management of sensory input

Patterns of sensory processing assessed by the Sensory Profile
Responding strategies
Threshold / reactivity Passive Active
High threshold with low reactivity
Low registration (Bystander)
Does not notice sensory events or is slow to respond
Sensory seeking (Seeker)
Looks for sensory experiences
Low threshold with high reactivity
Sensory sensitivity (Sensor)
Readily notices sensory stimuli, may be distracted by them
Sensory avoider (Avoider)
Deliberately acts to reduce or prevent exposure to sensory stimuli

The sensory profiling tool


Implementing the Pool Activity Level Occupational Profiling Tool
• Life History Profile
• A Checklist of how the person carries out everyday tasks
• Activity Profile which assists the translation of understanding into practice
• Individual Action Plans for personal ADL
• Outcome Sheet for recording results

The Pal
Planned
• Complete activity• Search for objects• Follow simple instruction• Can use memory prompts
Exploratory
• Complete familiar task• Concerned about the effect of doing the task• May not have an end result in mind• Need activity broken down into steps
Sensory
• No thoughts regarding the purpose of the task• Concerned with sensation• One step at a time• Verbal and non-verbal direction
Planned
• No aware of the environment• Movement is in response to stimulus• Can only process one sensation at a time• Communication is predominately non-verbal

The sensory tool box
• Sight - visual
• Sound - Auditory
• Touch - Somatosensory / vibration
• Taste - Gustatory and texture
• Smell - Olfactory
• Movement - Vestibular / proprioception

Analysing the Snoezelen environment
• Intensity
• Amount
• Consistency
• Any competing stimuli
• Familiarity
• Level of arousal
• Environmental cues

Organising a session
• Identifying focus for the session based on assessment outcomes
• Techniques for specific needs
• Timing and the therapeutic intervention
• Measuring outcome
• Reflection on the session

Using the PAL to guide the session
Positioning of objects – eye line, direct contact, one sense at a time
Verbal directions – Allow time to settle and explore, guide movements, reinforce response with verbal and non-verbal cues
Directions – Breakdown to one step at a time, session length approximately 10 minutes, one to one sessions, end session by gradually increasing light
Activity characteristics – To arouse conscious awareness of self and immediate environment

Achieving sensory modulation within session
Balance of excitation & inhibition
Excitation – over-response eg. release phenomena in brain injury & stroke.
Inhibition – under-response, fail to notice stimulation eg. Neglect
Role of feedback system to regulate balance

Arousal & alerting systemsSensory system Arousal / alerting
descriptorsDiscriminating/ mapping descriptors
For all systems Unpredictable –unfamiliar, cannot anticipate the sensory experience
Predictable – familiar, can anticipate what will happen next
Somatosensory Light touchPain – sharp, pinchTemperature Small surface contact
Pressure touchLong duration stimuliLarge body surface contact
Vestibular Head position changeSpeed changeDirection changeRotary head movement
Linear head movement –rocking, bouncingRepetitive

Arousal & alerting systems
Sensory system
Arousal / alerting descriptors
Discriminating/ mapping descriptors
Proprioception Quick stretch – brisk tapping Sustained tension –constant action on muscles, heavy objects
Visual High intensity – bright visual stimulusHigh contrast – difference between stimulus & environmentVariable – changing characteristics
Pressure touchLong duration stimuliLarge body surface contact
Auditory Variable – changing characteristicsHigh intensity – loudCompetitive – conflicting sound
Linear head movement –rocking, bouncingRepetitive
Olfactory / gustatory
Strong intensity Mild intensity

Incorporating sensory qualities into integrated therapy programmes
Visual
Arousal
• High intensity – to increase arousal & attention
• High contrast – to enhance location & attention
• Variability – Maintain alertness & attention
Discrimination
• Low intensity – generate searching behaviours
• Low contrast –discrimination
• Competitive – increase tolerance and inhibitory response

Auditory
Arousal
• Variable – maintain arousal or interest in the task
• High intensity – Alerting, location
Discrimination
• Rhythmic – predictable / organising / orientation
• Constant – Environmental orientation
• Competitive – Orientation & tolerance

Olfactory / Gustatory
Arousal
• Strong intensity - arousal
Discriminatory
• Noncompetitive – focus attention
• Low intensity – generate searching behaviour
• Mild intensity –recognition & memory

Sensory magic
Reduce agitation / education / increase arousal...Sensory Magic offers the individual a safe sensory environment which is structured and predictable. The sensory room can be set according to each individual’s needs and preferences, so that each and every time the experience is identical, providing continuity and stability. In this way, anxiety levels are kept to a minimum. The MSE can be subtly and slowly altered over time to introduce new colours, images and sounds at the individual’s own pace.
• www.rompa.com/sensorymagic

Simon
• 67 year old man with Alzheimer’s disease and attempted insulin overdose
• Sensory seeker using the Sensory Profile
• Sensory level using the PAL
• Graded introduction
• Sensory package for use at home

Claire
• 80 year old woman with vascular dementia and R CVA
• Sensory sensitive using the Sensory Profile
• Exploratory using the PAL
• Graded exposure and relaxation techniques
• Sensory soothing kit

Research• Burns, I., Cox, H., & Plant, H. (2000). Leisure or therapeutics? Snoezelen and the care of older persons
with dementia. Int.J.Nurs.Pract., 6, 118-126.
• Baker, R., Bell, S., Baker, E., et al. (2001). Randomised controlled trial of the effects of multi-sensory stimulation (MSS) for people with dementia. BJClinPysch 40, 81-96.
• Chung, J. C., Lai, C. K., Chung, P. M., & French, H. P. (2002). Snoezelen for dementia. Cochrane.Database.Syst.Rev., CD003152.
• Schofield, P. (2002). Evaluating Snoezelen for relaxation within chronic pain management. Br.J.Nurs., 11, 812-821.
• Staal, J., Pinkney, L., & Roane, D. (2003). Assessment of Stimulus Preferences in Multi-sensory Environment Therapy for Older People with Dementia. British Journal of Occupational Therapy, 66,542-550.
• Heyn, P. (2003). The effect of a multisensory exercise program on engagement, behavior, and selected physiological indexes in persons with dementia. Americal Journal of Alzheimer's disease and Other Dementias, 18, 247-251.
• Baillon, S., Van Diepen, E., Prettyman, R., et al. (2004). A comparison of the effects of Snoezelen and reminiscence therapy on the agitated behaviour of patients with dementia. Int.J.Geriatr.Psychiatry, 19, 1047-1052
• Ball, J. & Haight, B. K. (2005). Creating a multisensory environment for dementia: the goals of a Snoezelen room. J.Gerontol.Nurs., 31, 4-10.

Research cont.• Baillon, S., Van Diepen, E., Prettyman, R., et al. (2004). A comparison of the effects of Snoezelen and
reminiscence therapy on the agitated behaviour of patients with dementia. Int.J.Geriatr.Psychiatry, 19, 1047-1052
• van Weert, J. C., van Dulmen, A. M., Spreeuwenberg, P. M., Bensing, J. M., & Ribbe, M. W. (2005). The effects of the implementation of snoezelen on the quality of working life in psychogeriatric care. Int.Psychogeriatr., 17, 407-427.
• Ball, J. & Haight, B. K. (2005). Creating a multisensory environment for dementia: the goals of a Snoezelen room. J.Gerontol.Nurs., 31, 4-10.
• Staal, J. (2007). The Effects of Snoezelen (Multi-sensory Behavior Therapy) and Psychiatric Care on Agitation, Apathy, and Activities of Daily Living in Dementia Patients on a Short Term Geriatric Psychiatric Inpatient Unit. Journal of Psychiatry in Medicine, 37, 357-370.
• Collier, L., McPherson, K., Ellis-Hill, C., Staal, J., & Bucks, R. (2010). Multisensory Stimulation to Improve Functional Performance in Moderate to Severe Dementia-Interim Results. American Journal of Alzheimers Disease and Other Dementias, 25, 698-703.
• Klages, K., Zecevic, A., Orange, J. B., & Hobson, S. (2011). Potential of Snoezelen room multisensory stimulation to improve balance in individuals with dementia: a feasibility randomized controlled trial.
Clin.Rehabil., 25, 607-616.52

Thank you for listening
Dr Lesley Collier
Centre for Innovation and Leadership
Faculty of Health Sciences
University of Southampton
SO17 1BJ









![G ARTICLE IN PRESS - Snoezelen Multi-Sensory Environments...multi-sensory therapy is beneficial for people with sensory and learning disabilities [9]. Moffat et al. revealed positive](https://img.pdfslide.us/doc/110x75/5fe8d0c61e886b29082f1769/g-article-in-press-snoezelen-multi-sensory-environments-multi-sensory-therapy.jpg)