Embed Size (px)
Citation preview

Sensible. Simple. Effective.Reaching out to more patients.
DEVELOPING A PERIOPERATIVESLEEP MANAGEMENT PROGRAM

REASONS TO INTEGRATE A PERIOPERATIVE APNEA PROGRAM
Increasing Prevalence of Apnea
4% -Estimated prevalence of OSA in middle-aged men.
24% -Percent of U.S. men suffer from some form of sleep disordered breathing (SDB).
ASA Practice Guidelines
Joint Commission Focus
Reimbursement Changes
Reduce Liability Claims
Improving Patient Care
Reduce Adverse Events, Decreasing:
o Hospital Re-admissions
o Extended PACU stays
o Unanticipated ICU admissions
New England Journal of Medicine. 1993; 328; 1230-1235.ASA Task Force. Anesthesiology 2006; 104:1081–93.

REASONS FOR APNEA SCREENING
Undiagnosed Apnea Patients Pose the Highest Risk
Known apneics make up a small portion of the population undergoing surgery.
Over 28 million Americans suffer from OSA, 20 million going undiagnosed & untreated.
Research shows preoperative identification of OSA & use of perioperative precautionary measures improves patient outcomes.
Finkel, et. al. Sleep Review July-Aug 2006. Gupta, et. al.. Mayo Clinic Proc. 2001; 76:897-905. Moos, et. al. ANAA Journal. June 2005. Vol 3, No 3.ASA Task Force. Anesthesiology 2006; 104:1081–93.
SCREENING IDENTIFIES PATIENTS THAT WOULD NOT SEEK TREATMENT OTHERWISE.

A combination of factors
put apnea patients at
higher risk, including:
• Lingering anesthetics
• Amount/type of pain
medications used
• Decreased monitoring
• Marked REM rebound
APNEA, ANESTHESIA & PAIN MANAGEMENT
Finkel, et. al. Sleep Review July-Aug 2006. Gupta, et. al.. Mayo Clinic Proc. 2001; 76:897-905. Moos, et. al. ANAA Journal. June 2005. Vol 3, No 3.ASA Task Force. Anesthesiology 2006; 104:1081–93.
Anesthetics & Pain Medications Depress the Central Nervous
System
Decreased Muscle Tone
Obstructive Apnea Events
Light, Erratic Breathing
Central Apnea EventsHypoxemia
Respiratory Failure
Diminished Arousal Response
HypoxemiaRespiratory Failure

FINANCIAL RISK REDUCTION
Implementing a Perioperative Apnea Management Program Prevents or Reduces Risk of:
Never Events
o Waived Fees
o Possible Remunerative or Punitive Repercussions
Non-payment for Unexpected Medical Events
o National movement to stop paying for these types of events
CMS Recovery Audits

COST BENEFIT- CASE STUDY FINDINGS
Candidates for Monitoring a Year 20,000 patients
Post-operative Respiratory Failure Rate 17 per 1000
Number Patients at Risk 340 patients
Additional Length of Stay (Days) 9.08
Hospital Cost per Day $1,900
Additional Cost for Patients at Risk $5,865,680
Success of Orders with C02 Monitoring 30%
Savings with Monitoring $1 ,759,704
Capital Costs ( 100 @ $1,000/device) $100,000
Depreciation (5 year straight line) $60,000
Savings $1,723,104
Spin Off PSG Charges (244 * $2,500) $612,000
Costs PSG + Interpretation $165,920
Gross Revenue (PSG + Hospital Savings) $1,889,624
DME Spin Off if Available (Gross Revenue) S 170,000
Example Case Study Findings
-Savings on at-risk patients
-Increased revenue through PSG & DME

SAVING MONEY & INCREASING OPPORTUNITIES
Case Study Findings: At Risk Patients = Greater Costs for Hospitals
Not Identifying at Risk Patients?
Deduct from Your Bottom Line.*From a Patient Pool of 20,000:
o 340 Patients -
At Risk Of Post-operative Respiratory Failure
o 9 Additional Days -
Spent In Hospital By At-risk Patients on Average
o $1,900 –
Hospital Cost Per Day
= $5,865,680
Total Additional Costs
Case Study Findings

SAVING MONEY & INCREASING OPPORTUNITIES
Case Study Findings: Monitoring Saves Money & Creates Opportunity
Saving Money
o $1,759,704 - Amount Saved with Objective Screening in Case Study
Opportunity through the Sleep Lab & DMEo +$446,080 -
Gross margin for additional PSG testing (to confirm & initiate therapy) brought on by patients identified during pre-operative screening.
o +$170,000 -
Net Revenue for DME

PROBLEMS WITH COMMON SCREENING METHODS
o Subjective
o Simplistic stratification i.e. high or low risk
o Not specific i.e. high # of false-positives - Leads to unnecessary testing or delayed surgery
o Cannot indicate type/severity of SDB
QuestionnairesIn-lab Polysomnography (PSG)
o Costly
o Impractical for ScreeningPopulation is too large – Would delay surgery
o Can Take Days or Weeks to Receive Results
o Higher refusal/drop-out rates
Guidelines for the Perioperative Management of Patients with Obstructive Sleep Apnea. Anesthesiology 2006; 104:1081–93.STOP Questionnaire; A Tool to Screen Patients for Obstructive Sleep Apnea. Chung, et. al.. Finkel, et. al.. Sleep Review July-Aug 2006. Magalang, et. al. Chest 2003; 124; 1694-1701

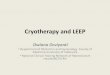
META-ANALYSIS OF OSA QUESTIONNAIRES
Study Pooled Study n FN Rate
Ease of Use, 0-3
Test Accuracy, by Diagnostic Odds
Ratio (DOR)*Summary
Recommendations
ASA Checklist 117 0.123 - 0.279 1 Poor No preoperative value, unacceptable FN rate
BMI alone 406 0.228 - 0.298 0 Poor No preoperative value, unacceptable FN rate
Epworth Sleepiness Scale 46 0.714 1 Poor Unacceptable FN rate
STOP Questionnaire 177 0.205 - 0.344 1 Poor No preoperative value,
unacceptable FN rate
STOP-BANG 177 0.0 - 0.164 2 Average-ExcellentExcellent screening test for severe OSA, unacceptable FN rate for Dx of OSA
*DOR combines data on sensitivity and specificity to give an indication of a test’s ability to rule in or rule out a condition.
Screening Test Reliability & Summary Recommendations for Preoperative Use
Many of the most
commonly used
preoperative
screening
questionnaires are
considered to have
poor accuracy.
Derived from Ramachandran, et. Al. Anesthesiology, V 110, No 4, Apr 2009

THE S.O.S. APPROACH
Subjective Screen
Use questionnaire (e.g. STOP; STOP-BANG; Berlin) to screen everyone
o The population at risk is often large and will often include many patients with low risk.
A much smaller subgroup with very high risk will require pre-op intervention.
Objective Screen
Oximetry (e.g. SatScreen) devices are widely used because of affordability, high predictive value, & minimal patient impact.
o Identifies the high risk subgroup.
“S.O.S.”Subjective Objective Screening
Research shows a combination approach can be the most feasible & effective method
Hwang, et. al. Chest 2008; 133; 1128-1134.

Patents
High resolution oximetry with
Digital pattern analysis & recognition
SatScreen
Oximetry screening
FDA cleared acquisition, analysis & reporting software
Patient Safety Connection Center
Oximetry & HST software management platform
PATIENT SAFETY, INCTECHNOLOGY
BREAKTHROUGHS

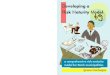
WHY SATSCREEN?
Accurate & Cost-Effective
Results in Minutes
Easy to Read –Green to red indices for important information
Indicates Arousal Failure & Hypoventilation Syndromes-These patients are at higher risk of post-op respiratory failure
Highlights Frequency of Events & Severity of O2 Desaturations
Most oximetry
software only
report raw data,
ODI & O2 ranges.
Bloch. Chest 2003; 124; 1628-1630. ASA Task Force. Anesthesiology 2006; 104:1081–93.
Madani. Advance for Respiratory Care and Sleep Medicine. Posted on January 7, 2009.

GET STARTED
Define your protocol for at risk patients Determine your Screening Protocol
o Gather your team & assign responsibilities
Practice Guidelineso If patient is identified as at risk, follow ASA guidelines or
preferred protocol
Develop discharge instructions / plan
Questions?
We want to help you make your organization’s OSA screening program a success.
Please contact us at:
1-888-666-0635