Embed Size (px)
Citation preview

Special Educational
Needs and Disabilities
Needs Assessment
Cornwall & Isles of Scilly
18/12/18 V0.9 Final

JSNA Special Education Needs and Disabilities 2
18/12/18 V 0.9 Final
Current Document Status
Version 0.8
Approving body SEND Board
Date Date of formal approval (if applicable)
Responsible officer
Review date
Location
Insert web address where document can be accessed.
Version History
Date Version Author/Editor Comments
08/06/2016
0.1
Linda Howarth
Working Draft
28/09/2016
0.2
Linda Howarth
Updated data
15/10/2017
0.5
Brian O’Neill
Update for SEND performance board
30/05/2018
0.7
Julie Moseley
Update from partners
07/09/2018
0.8
Brian O’Neill
Sign off changes from partners
18/12/2018
0.9
Brian O’Neill
Final amendments
Comprehensive Impact Assessment Record
Date Type of assessment conducted
Stage/level completed (where applicable)
Summary of actions taken decisions made
Completed by
Impact Assessment review date
Insert Date
Initial / Full
Complete
NFA
Insert officer name
Insert date
Document retention
Document retention period E.g. 5 years in hard and electronic copies.

JSNA Special Education Needs and Disabilities 3
18/12/18 V 0.9 Final
Joint Strategic Needs Assessment Special Educational Needs and Disability
Executive Summary 6
Recommendations 10
Scope 12
Purpose of Cornwall and the Isles of Scilly special education needs
and disabilities joint strategic needs assessment
Context for the JSNA
National Context 13
Definition of special educataional needs and disabilities 16 Special educational needs 16
Disability 17
What’s happening in Cornwall and the Isles of Scilly? 19 Cornwall context 20
Isles of Scilly context 20
Clinical commissioning group 21
Population profile 21
Trend overview (0-25) 21
Number of children and young people by age (0-25) 21
Births 22
Migration 24
Total number of pupils 25
Prevalence of SEND in Cornwall and the Isles of Scilly 26
Limiting long-term health problems and disabilities 26
Disability Living Allowance (DLA) 26
Prevalence estimates 29
Prevalence of SEN in Cornwall and the Isles of Scilly 29
Types of special educational need 31
Specific learning difficulty 31
Moderate learning difficulty 31
Profound and multiple learning difficulty 32
Social, emotional and mental health difficulties 32
Speech, language and communication needs 33
Hearing impairment 34
Visual impairment 35
Multi-sensory impairment 35
Autistic spectrum disorder 36
Other difficulty/disability 37
Educational attainment 37
Elective home education 42
Absences and exclusions from education 43
Youth offending 43

JSNA Special Education Needs and Disabilities 4
18/12/18 V 0.9 Final
NEET 44
Vulnerable children 45
Children on a child protection plan 46
Continuing care needs 47
Prevalence of children with SEN in areas of higher deprivation 47
Disability by ethnicity (aged 0-15), Census 2011 48
School census ethnicity – Cornwall state-funded primary, secondary and special
schools 48
SEND prevalence and language 48
SEND prevalence and gender and age 49
SEND prevalence and religion 50
SEND prevalence and gender reassignment 50
Health determinants 51
Older mothers 51
Young mothers 51
Smoking during pregnancy 52
Maternal diet 53
Maternal obesity 53
Low birth weight 53
Gestational age 54
Screening and immunisation 55
Antenatal and new-born screening 55
Child health records department 56
Vaccinations 57
Information from the health visitor needs assessment 58
Injuries to children and young people 59
Child poverty 61
Service provision – health 61
Health visiting 62
Community paediatrics 63
Speech and language 63
Community therapy department 64
CAMHS 64
Transition to adult mental health services 65
Special parenting service 67
Autistic spectrum disorder assessment team 67
Service provision – local authority 68
Transport 68
Equipment 69
Reccomendations 70

JSNA Special Education Needs and Disabilities 5
18/12/18 V 0.9 Final
Appendices 71
Appendix 1 Legislative and policy context Appendix 2 Risk Factors
Appendix 3 Population projections
Appendix 4 DLA claimants Appendix 5 Trends in types of SEND Appendix 6 Absenteeism and exclusions
Appendix 7 Prevalence of SEND by deprivation Appendix 8 SEND and ethnicity
Appendix 9 Prevalence of SEND by gender, age and religion

JSNA Special Education Needs and Disabilities 6
18/12/18 V 0.9 Final
Executive summary

JSNA Special Education Needs and Disabilities 7
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 8
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 9
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 10
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 11
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 12
18/12/18 V 0.9 Final
Scope
Purpose of Cornwall and the Isles of Scilly’s special
education needs and disabilities joint strategic needs
assessment
This needs assessment focuses on those children and young people in
Cornwall and the Isles of Scilly with an identified special educational need,
including those who have an education, health and care (EHC) plan, and
the families/carers of all the children and young people.
Children and young people with special educational needs and/or
disabilities (SEND) are a diverse group; Part 3 of the Children and
Families Act (2014)1 sets out the need for agencies and families to work
together, to ensure that children and young people receive support that
is timely and proportionate to their need.
This needs assessment aims to collate and analyse both national and local
information and data on the needs of children and young people with
SEND, to create a more comprehensive picture to support effective
activity to meet needs in Cornwall and the Isles of Scilly.
Context for the JSNA
The purpose of this needs analysis is to bring together and analyse all the
available relevant health, education and care data about children and
young people in Cornwall and the Isles of Scilly who are aged 0-25 and
have SEND.
The Joint Strategic Needs Assessment (JSNA) informs understanding of
needs in Cornwall and the Isles of Scilly. This document will inform joint
strategic decisions, defining priorities and the allocation of resources to
make the greatest impact.
In Cornwall the SEND JSNA is a key resource that informs the Cornwall
area self- evaluation for special educational needs and disability. The self-
evaluation is annually updated with the identified priorities for
development being considered by the multi- agency SEND Board, and
addressed in Cornwall’s SEND Strategy. This process enables partners
collectively to agree priorities and deliver change. Both the SEND self-
evaluation and the SEND Strategy are available on the Cornwall Council
website.
1 Children and Families Act (2014) http://www.legislation.gov.uk/ukpga/2014/6/contents/enacted

JSNA Special Education Needs and Disabilities 13
18/12/18 V 0.9 Final
In the Isles of Scilly the JSNA feeds into the SEND Programme Board, and
raises key issues for consideration.
The main objectives of this needs assessment are:
To provide an understanding of the education, health and social
care needs of children and young people with SEND, at local authority level and across Cornwall and the Isles of Scilly;
To understand both current and projected needs for the next 5
years;
To understand the prevalence of specific disabilities/needs;
To raise key issues for consideration by Cornwall’s SEND Board, and
the Isles of Scilly SEND Programme Board.
National Context
Key Messages from the Children and Families Act, 2014
Children, young people and their families must be involved
in discussions and decisions about their care and
education.
Local authorities, health and care services are required to
co-operate and jointly commission the services needed.
There must be a local offer, which must be kept under review.
There must be clear information about available services.
Statements of special educational need were replaced by
education, health and care plans (EHC plans), which cover
ages 0-25.

JSNA Special Education Needs and Disabilities 14
18/12/18 V 0.9 Final
What do families tell us?
The 2018 SEND survey followed up on the 2016 survey in order to get an
up-to-date summary of people’s views, and measure change to date.
There was a significant increase in the number of respondents in 2018
compared with 2016. Respondents represented a wide range of special
educational needs, and came from a wide geographic spread of the
county.
A total of 566 people took part in the surveys or young people’s
engagement activities:
53 (30 in 2016) young people completed the young people’s
survey, and 115 took part in engagement sessions: one in a special
school, and three in local FE colleges.
398 (200 in 2016) people completed the surveys.
141 (100 in 2016) parents or carers, or family members and children
responded to the survey. For 59% of the respondents, their child’s educational needs included autism.
Key messages from the 2018 Cornwall survey of the views of families:
54% of families rate the current provision as good or very
good – this is up from 41% in 2016.
60% agreed that there were some high quality services –
this is up from 56% in 2016.
69% agreed that families are recognised as key partners,
making a difference to arrangements for children and
young people – in 2016 this figure was 24%.
77% of respondents agreed that there is much more to be
done to improve services and processes about SEND.
70% felt that outcomes for the children and young people
with the most complex needs need to be clearer in EHC
plans.
The importance of ease of access to information about meeting individual needs, and what support children, young people and their families can expect.
For the Isles of Scilly the Parent Carer Forum is the forum
that represents families; their views have not been canvassed
recently.

JSNA Special Education Needs and Disabilities 15
18/12/18 V 0.9 Final
115 young people took part in group engagement sessions about ‘Feeling
included in trips, clubs and activities’ and ‘Getting ready for adulthood’.
There was some positive feedback that the young people really enjoyed
having the opportunity to raise their thoughts and ideas for improvement.
Young people told us they feel happy and included at college: ‘I feel
included when the lessons include teamwork’, ‘I really enjoy college’, ‘I
feel happy in class’.
Based on feedback from young people, more resources will be developed to support inclusion of children and young people on school and college trips.
The feedback from young people will be used to develop resources to prepare young people for adulthood from an early age.

JSNA Special Education Needs and Disabilities 16
18/12/18 V 0.9 Final
Definitions of special educational needs and disability
Special Educational Needs (SEN)
Special educational needs are defined in the Special educational needs
and disability code of practice: 0 to 25 years, 20152 as follows:
A child or young person has SEN if they have a learning difficulty or a
disability which calls for special educational provision to be made for him
or her.
A child of compulsory school age or a young person has a learning
difficulty or a disability if he or she:
• has a significantly greater difficulty in learning than the majority
of others of the same age, or
• has a disability which prevents or hinders him or her from making
use of facilities of a kind generally provided for others of the same
age in mainstream schools or mainstream post-16 institutions.
Special Educational Provision means:
• For children aged two or more - educational or training provision
that is additional to or different from that made generally for
other children or young people of the same age by mainstream
schools, maintained nursery schools, mainstream post-16
institutions or by relevant early years providers.
• For a child under two years of age - educational provision of any
kind.
Paragraphs 6.27 – 6.35 of the 0-25 SEND Code of Practice3 expand on
this definition setting out four specific areas of SEN:
Communication and interaction – for example, where children
and young people have speech, language and communication
difficulties which make it difficult for them to make sense of
language or to understand how to communicate effectively and
appropriately with others.
2 Department for Education, Special educational needs and disability code of practice: 0 to 25 years,
January 2015, p15-16 3 Department for Education, Special educational needs and disability code of practice: 0 to 25 years,
January 2015, p15-16

JSNA Special Education Needs and Disabilities 17
18/12/18 V 0.9 Final
Cognition and learning – for example, where children and young
people learn at a slower pace than others their age, have difficulty in
understanding parts of the curriculum, have difficulties with
organisation and memory skills, or have a specific difficulty affecting
one particular part of their learning performance such as in literacy
or numeracy.
Social, emotional and mental health difficulties – for example,
where children and young people have difficulty in managing their
relationships with other people, are withdrawn, or if they behave in
ways that may hinder their and other children’s learning or that
have an impact on their health and wellbeing.
Sensory and/or physical needs – for example, children and
young people with visual and/or hearing impairments, or a physical
need that means they must have additional ongoing support and
equipment.
Many children and young people may have SEN across more than one of these areas.
National reporting is against a defined set of primary needs at a more
detailed level than these four areas of SEN.
Disability Children and young people who have SEN may also have a disability.
Disability has been defined by a number of statutory organisations but
there is no one commonly agreed definition. The SEND Code of practice
utilises the Equality Act 20104 definition which defines disability as follows:
A person is disabled, if he or she has a physical or mental impairment that
has a ‘substantial’ and ‘long-term’ negative effect on his or her ability to do
normal daily activities:
• ‘substantial’ is more than minor or trivial - e.g. it takes much
longer than it usually would to complete a daily task like
getting dressed
• ‘long-term’ means 12 months or more - e.g. a breathing
condition that develops as a result of a lung infection.
4 Equality Act 2010 http://www.legislation.gov.uk/ukpga/2010/15/section/6 - accessed May 2017

JSNA Special Education Needs and Disabilities 18
18/12/18 V 0.9 Final
In health, the definition of disability used is usually that of the World
Health Organisation (WHO)5 where it is explained that disability is an
umbrella term, covering impairments, activity limitations, and
participation restrictions, and is not simply a health problem. Specifically
it is stated that:
Disability is an umbrella term, covering impairments, activity limitations,
and participation restrictions:
• An impairment is a problem in body function or structure;
• An activity limitation is a difficulty encountered by an individual
in executing a task or action; • A participation restriction is a problem experienced by
an individual in involvement in life situations.
The risk factors associated with childhood disability are described in appendix 2.
5 WHO http://www.who.int/topics/disabilities/en/

JSNA Special Education Needs and Disabilities 19
18/12/18 V 0.9 Final
What’s happening in Cornwall and the Isles of Scilly?
Key messages:
The geographical location of Cornwall and the Isles of
Scilly impacts on access to services and provision that
would be more readily available in parts of the country
with a higher population density
A high proportion of children and young people have their
needs met by mainstream schools and settings
Cornwall is a low-funded local authority, ranked 144th out of
150 per person for high needs block funding
The Ofsted and CQC area SEND inspection of Cornwall in 2017
found that ‘leaders are ambitious to improve action for
children and young people who have SEND and are delivering
improvements despite reducing resources and increasing
demand for services’. It also found that plans are in place to
improve autistic spectrum disorder provision, awareness and
assessment; CAMHS arrangements; children with SEND who
are electively educated at home; occupational therapy
provision; opportunities for supported employment; and
schools’ approaches to meeting needs at SEN Support
The Isles of Scilly are similarly disadvantaged in terms of access to
medical services. Families report that consultations with mainland
professionals frequently involve overnight stays and relatively
complex travel arrangements.
The islands have one school for students aged 3-16. The school is
committed to meeting the needs of all the children in the locality in the
knowledge that any appropriate mainland provision would require a
residential setting.

JSNA Special Education Needs and Disabilities 20
18/12/18 V 0.9 Final
Cornwall context
The population of Cornwall has been growing steadily since the 1960s.
Current estimates suggest that Cornwall’s population stands at around
553,687 and it is estimated to reach 635,900 by 20376, an increase of
82,213 (14.8%). This growth is predicted to be driven by migration,
largely due to more people moving in, but also importantly due to a
decline in the number of people leaving Cornwall.
A statistical summary for Cornwall and the Isles of Scilly with population
projections is provided later in this document.
Isles of Scilly context The Isles of Scilly comprise over 200 granite islands scattered across 200
km², set out in the Atlantic some 45 km south-west of Land’s End. Five
islands are permanently inhabited (St Mary’s, St Agnes, St Martin’s,
Tresco and Bryher) and each of these has their own unique character and
distinct identity. The occupied islands cover a total area of just over 14
km².7
The Islands support a resident population of around 2,3248. The
population of the islands declined in the 1980s, but has been slowly
increasing since then, with nearly all of the growth being on St Mary’s.
It is estimated that 1,758 live on St Mary’s, 210 on Tresco, 150 on St
Martin’s and 206 on Bryher and St Agnes. Population projections for
Scilly suggest an overall decline in population over the next 20 years with
estimates predicting a population of 2,122 by 2037 – a decline of 200
(8.7%).
The Council of the Isles of Scilly is an independent unitary authority and
oversees the administration of services. However, due to efficiencies a
number of services are jointly commissioned with Cornwall Council and
delivered by Cornwall Foundation Trust.
62014-based subnational population projections and 2015 Mid Year Population Estimates, Population
Estimates Unit, ONS 7 Natural England: National Character: Area Profile 158 Isles of Scilly,
publications.naturalengland.org.uk/file/6631520605306880 8 2015 mid-year population estimates, Population Estimates Unit, ONS

JSNA Special Education Needs and Disabilities 21
18/12/18 V 0.9 Final
Clinical Commissioning Group
Clinical commissioning groups (CCGs) have responsibility for
commissioning health services. Within Cornwall and the Isles of Scilly
there is one CCG, NHS Kernow.
Population profile
Trend overview (0-25)
The 0-25 year old group is expected to increase by nearly 14% by 2030,
which equates to an additional 20,500 children and young people. A
number of these children and young people will have additional and special
needs that require support9.
Historically Cornwall has experienced high levels of outward migration of
people between the ages of 16-24. However, the expansion in the higher
education infrastructure and better employment prospects has led to a
reduction in the number of young people leaving Cornwall and increasingly
greater numbers of young people moving to Cornwall. These trends are
neither fixed nor guaranteed, and are fragile but account in some part for
the increase in cohorts aged 16-24 since 2001.
Details of the population projections to 2030 can be found in appendix 3.
Number of children and young people by age (0-25)
In 2016 there were 148,926 children and young people aged 0-25 living in
Cornwall and the Isles of Scilly. Cornwall and the Isles of Scilly have a
lower proportion of children and young people than the average for
England; overall 27% of the population of Cornwall and the Isles of Scilly is
aged 0-25 compared with 30% in England.
9 ONS Migration Tool 2005-15. Migration Statistics Unit ©Crown Copyright 25th August 2016, and
Cornwall Small Area Population Projections, Edge Analysis

JSNA Special Education Needs and Disabilities 22
18/12/18 V 0.9 Final
Figure 3: 0-25 Age Structure for Cornwall and Isles of Scilly, and England, 2016 Mid-Year Estimates, ONS
Births The number of births has grown steadily in Cornwall and the Isles of Scilly
since 2001 with 4,463 live births in 2001 compared with 5,447 in 2014,
almost 1,000 higher.
However, there were reductions in both 2015 (to 5,417) and 2016 (to
5,313), with a further reduction in 2017 to 5,162.
6 4 2 0 2 4 6
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
Cornwall & IoS Males England Males Cornwall & IoS Females England Females

23 JSNA Special Education Needs and Disabilities
18/12/18 V 0.9 Final
Figure 4. Births and Females of Childbearing Age (Cornwall) 1981-2031
The chart above reflects national patterns, which saw an overall fall in birth
rates during the 1990s due to declining fertility among women in their
twenties. In contrast, the overall rise in births since 2001 has been driven
by a faster increase in birth rates for women in their thirties and forties
(continuing the long-term trend that started in the late 1970s) and
increasing births among women in their 20s.
Older and younger parents are more at risk of complications that can result
in childhood disability. Babies born to women under 20 are more at risk of
poor nutrition and poor placental transfer of food and oxygen, whereas
those born to older mothers are more likely to have chromosomal
abnormalities.
The trend in Cornwall and the Isles of Scilly shows that the actual numbers
of births to women aged 20 to 24 has decreased between 2011 and 2016
by more than 26%; births to 35 to 39 year olds increased between 2009
and 2016 by 11%, with all other age groups remaining fairly static. The
most recent data shows that women over the age of 40 represent 3.8% of
all births in Cornwall and the Isles of Scilly10
The following chart shows the rate of live births in Cornwall and the Isles of
Scilly by age of birth mother (per 1,000 women).
10South West Clinical Network Maternity Dashboard (2018) Online
0
1
2
3
4
5
6
7
80
85
90
95
100
105
110
115
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
2013
2015
2017
2019
2021
2023
2025
2027
2029
2031
Th
ou
san
ds
Th
ou
san
ds
Females aged 15-49 Births
Projected figures 2018 - 31

JSNA Special Education Needs and Disabilities 24
18/12/18 V 0.9 Final
Figure 5. Live birth rates by age per 1,000 women
Migration
According to the 2011 census11 21,205 persons, of whom 2,642 were aged
1-15, moved into Cornwall and the Isles of Scilly from other areas; 14,321
persons moved out, 1,431 of whom were 1-15 years old. Overall, this
migration resulted in 6,884 more persons in Cornwall and the Isles of
Scilly. Movement within Cornwall and the Isles of Scilly accounted for
43,263 persons, of whom 8,252 were in the 1-15 year old bracket.
11
www.nomisweb.co.uk
45+
40-44
35-39
2009
2010
2011
2012
2013
2014
2015
2016
30-34
25-29
20-24
<20
0 20 40 60 80 100 120 140

JSNA Special Education Needs and Disabilities 25
18/12/18 V 0.9 Final
Migration of people into and out of Cornwall
Total number of pupils
The total number of pupils in schools in Cornwall and the Isles of Scilly are shown below:
Total Pupils in Cornwall and the Isles of Scilly12
2011 2012 2013 2014 2015 2016 2017
Cornwall 72,374 72,399 72,550 72,708 72,927 73,508 74,193
Isles of Scilly 274 277 273 274 274 279 266
NOTE: Includes maintained and direct grant nursery schools, maintained primary and secondary schools, city technology colleges, university technology colleges, studio schools, primary and secondary academies including free schools, special schools, special
academies including free schools, pupil referral units, alternative provision academies
including free schools and independent schools.
There are also children and young people who are electively educated at
home. At the beginning of 2018, 1,077 children and young people were being educated at home; 52 (4.8%) of these had an Education Health Care
plan in place.
On the Isles of Scilly, there are fewer than five pupils who are electively educated at home; none have been identified with SEND.
12
Department for Education https://www.gov.uk/government/collections/statistics-special-educational-
needs-sen

JSNA Special Education Needs and Disabilities 26
18/12/18 V 0.9 Final
Prevalence of SEND in Cornwall and the Isles of Scilly There are a number of different sources available to estimate the number
of children with special educational needs and disabilities. These include
pupils with special educational needs (SEN), children who had limiting long
term illness at the time of the 2011 Census, and those receiving Disability
Living Allowance (DLA), alongside various prevalence estimates.
There is no gold standard disability data source and no single definitive
measure of disability or chronic illnesses. Estimates of disability prevalence
and chronic illness vary between surveys according to the definitions of
disability that are used.
The various sources provide a very wide range of estimates, and children
and young people with SEND are not one group within the population – for
example, not all SEN children have disabilities and not all children with
disabilities will have SEN.
Limiting long term health problems and disabilities
The 2011 Census asked the question ‘Are your day-to-day activities limited
because of a health problem or disability which has lasted, or is expected
to last, at least 12 months?’ Responses were for all members of the
household. This is a very broad definition and is likely to include some,
but not all children, with special educational needs as well as those with
disabilities.
In 2011 there were 6,945 children and young people aged (0-24) whose
day to day activities were reported to be limited by a long-term health
problem or disability in Cornwall. This represents 4.9% of the 0-24 year
old population, which was higher than the regional and national average of
4.3%13.
Disability Living Allowance
To qualify for DLA, a child must have walking difficulties or physical or
mental disability sufficiently severe to need a lot more help or supervision
than other children of the same age with activities such as washing,
dressing or communicating. In order to determine whether a child is
eligible to receive DLA, they must have an assessment of their disability or
a statement from their GP14. These are quite stringent criteria, and it is
13
2011 Census © ONS 14
Gov.uk (2016) Disability Living Allowance (DLA) for children, Available:

JSNA Special Education Needs and Disabilities 27
18/12/18 V 0.9 Final
likely that some children who fail to qualify for DLA might still have special
educational needs. It is also likely that some families who would be eligible
for DLA may not be claiming it. This means that DLA only provides a
partial picture of children with special educational needs and disabilities.
In February 2015, there were 4,570 children and young people aged 0-24
claiming DLA in Cornwall15. This represents 3.1% of the 0-24 year old
population16.
The number of children and young people receiving DLA in Cornwall
increased by nearly 300 people or 6.1% between February 2012 and
February 2015, but reduced again in February 2016. During the same
period, the total 0-24 year old population in Cornwall increased at a
much slower rate, of 2.1% or 3,100 people17.
The following diagram breaks down the number of children and young
people receiving DLA by condition. It shows that learning difficulties is
the most common condition accounting for 44% of claimants.
https://www.gov.uk/disability-living- allowance-children/eligibility 15
Disability living allowance by disabling condition, DWP, [NOMIS 2016] 16
2014 Mid-Year Population Estimates © ONS 17
2012 and 2014 Mid-Year Population Estimates © ONS

JSNA Special Education Needs and Disabilities 28
18/12/18 V 0.9 Final
Disability Living Allowance is a benefit paid by the Department for Work
and Pensions to people aged under 65years ‘With a physical or mental
disability or both or with a disability that is severe enough to require help
caring or have walking difficulties’.
Disability Living Allowance is paid whether or not the person is in
employment. In Cornwall in February 2017 there were 24,290 people
claiming disability living allowance, 4,570 (19%) were in the age group 0-
24 years.
Further information about DLA claimants can be found in appendix 4.

JSNA Special Education Needs and Disabilities 29
18/12/18 V 0.9 Final
Prevalence estimates
Population forecasts over the next 20 years based on Office of National
Statistics projections can be used as a rough proxy for increases in the
disabled population, although they do not take into account higher survival
rates of babies and children with congenital anomalies, trauma or illness; a
trend towards more high risk pregnancies; and also more rigorous
diagnosis.
The number of children with disability may be expected to rise from 5,927
in 2013 to 6,486 in 2021, due to population increase alone, assuming
prevalence remains constant.
Prevalence of SEN in Cornwall and the Isles of Scilly
Children and young people identified by their educational setting as having
special educational needs are described as being at SEN Support. A small
proportion of children and young people have more complex special
educational needs. Upon request an education, health and care needs
assessment can be undertaken that may result in an education, health and
care plan being issued.
Before September 2014 pupils with complex needs could have a statement
of special educational need. After this date, education, health and care
(EHC) plans were introduced nationally. All statements were replaced by
EHC plans by April 2018. Therefore between these two dates, both types of
arrangement were in place for children and young people with complex
needs.
In 2017 there were 74,193 pupils in Cornwall. The percentage of pupils in
2017 who had an EHC plan was 2.4%18. The percentage of pupils in the
Isles of Scilly who have an EHC plan was 3.4%. For comparison, the
percentage for England was 2.8%, and for the South West was 2.7%.
Cornwall is slightly lower than both England and the South West, whereas
the Isles of Scilly are higher than both. However, small numbers of pupils
with EHC plans on the Isles of Scilly means that a change of one child can
make a big difference to the percentage.
Trends in numbers of children and young people with statements of SEN
and EHC plans are generally understood to be associated with changes in
18
Local Authority Interactive Tool https://www.gov.uk/government/publications/local-authority-
interactive-tool-lait

JSNA Special Education Needs and Disabilities 30
18/12/18 V 0.9 Final
legislation rather than changes in need of the population. However, for
completeness, details of changes in numbers of children and young people
with statements and EHC plans are shown in appendix 5.

JSNA Special Education Needs and Disabilities 31
18/12/18 V 0.9 Final
Types of special educational needs
In addition to the four main areas of special educational needs as set out in
the SEND Code of Practice 2015, national government collects data relating
to individual children and young people’s primary need. For a large
proportion of individuals, a primary need cannot reflect the full range of
needs that an individual has.
There are 449,905 (5.2%) of pupils in England with a learning difficulty.
For Cornwall, this figure is 3,671 (4.9%). Four types of learning difficulty
are recognised; these are specific, moderate, severe, and profound and
multiple learning difficulty.
Specific learning difficulty
In England as a whole, 32.6% of pupils with a learning difficulty have a
specific learning difficulty (SpLD), with the majority (84,143) attending
state-funded secondary schools, 61,123 attending state-funded primary
schools, and 1,607 attending state-funded special schools.
In Cornwall, 1,188 pupils have a SpLD as their primary need. This is
32.4% of all pupils with a learning difficulty, and 1.6% of all pupils.
On the Isles of Scilly the numbers are small so it is difficult to draw any
conclusions. However, there are 17 children identified as having a learning
difficulty, all of whom attend state-funded mainstream school. Children
identified as having a specific learning difficulty make up the majority of
children and young people with recognised learning difficulties (65%) – the
remainder have moderate learning difficulties. Pupils with a specific
learning difficulty make up 4.1% of all pupils on the Isles of Scilly.
Moderate learning difficulty Pupils with moderate learning difficulty (MLD) make up the largest
percentage of pupils with a learning difficulty in England; this is 259,713
(57.7%) pupils.
MLD also makes up the majority of pupils with a learning difficulty in
Cornwall. There are 2,071 pupils with MLD. This is 56.4% of all pupils
with an identified learning difficulty, and 2.8% of all pupils.
On the Isles of Scilly, six (35%) pupils with an identified learning difficulty
have a moderate learning difficulty. This is 2.3% of all pupils.

JSNA Special Education Needs and Disabilities 32
18/12/18 V 0.9 Final
Profound and multiple learning difficulty In England 10,981 (2.4%) of pupils with a learning difficulty have a
profound and multiple learning difficulty (PMLD). The majority (8,774)
attend state-funded special schools, although there are 1,783 attending
state-funded primary schools, and 424 attending state-funded secondary
schools.
In Cornwall there are 88 pupils with PMLD. This is 2.4% of all pupils with
an identified learning difficulty, and 0.1% of all pupils.
Number and percentage of pupils with learning disability/learning
difficulty 201719
Specific
Learning Difficulty
Moderate
Learning Difficulty
Severe
Learning Difficulty
Profound &
Multiple Learning
Difficulty
Number % Number % Number % Number %
STATE-FUNDED PRIMARY SCHOOLS
ENGLAND 62,123 9.7 147,684 23.3 4,346 0.7 1,783 0.3
SOUTH WEST 7,188 11.7 12,336 20.1 484 0.8 189 0.3
Cornwall 454 8.4 1,172 21.7 131 2.4 20 0.4
Isles of Scilly 0 0 0 0 0 0 0 0
STATE-FUNDED SECONDARY SCHOOLS
ENGLAND 84,143 21.1 95,738 24.0 2,020 0.5 424 0.1
SOUTH WEST 10,284 25.7 6,232 17.0 219 0.5 18 0.0
Cornwall 734 19.7 889 23.9 65 1.7 4 0.1
Isles of Scilly 11 26.8 6 14.6 0 0 0 0
STATE-FUNDED SPECIAL SCHOOLS
ENGLAND 1,607 1.4 16,291 14.5 25,972 23.2 8,774 7.8
SOUTH WEST 90 1.0 1,252 14.1 2,324 26.2 725 8.2
Cornwall 0 0 10 2.7 128 35.0 64 17.5
Isles of Scilly 0 0 0 0 0 0 0 0
Cornwall has particularly high percentages of children and young people
who have severe learning difficulty identified as their primary need.
Social, emotional and mental health difficulties
In England there are 186,793 (2.2% of all pupils, and 15% of all pupils
with an identified SEN) pupils with social, emotional and mental health
difficulties. The majority of these pupils attend state-funded schools;
99,475 (53.3%) attend primary schools and 73,325 (39.3%) secondary
19
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 33
18/12/18 V 0.9 Final
schools. There are also 13,993 (7.5%) pupils with these difficulties who
attend state-funded special schools.
1,857 (2.5% of all pupils, and 18.6% of all pupils with an identified SEN)
pupils within Cornwall have a social, emotional and/or mental health
difficulty as their primary need; this is a higher rate than both the South
West and England. Four pupils (1.1%) attend special schools, whilst the
figure is 12.5% in England. This may be a consequence of the types of
state-funded special schools in Cornwall. In Cornwall 1,038 (19.2%)
attend primary schools, and 815 (21.9%) secondary schools. On the Isles
of Scilly, three pupils were identified as having social, emotional and
mental health difficulties in 2017.
It should be noted that social, emotional and mental health difficulties was
added as a new type of classification in 2015; the previous classification of
behaviour, emotional and social development was removed. Behavioural,
emotional and social development and social, emotional and mental health
are not strictly equivalent descriptors.
Number and percentage of pupils with social, emotional and
mental health difficulties 20172021
ENGLAND SOUTH WEST Cornwall IoS
No % No % No % No %
STATE-FUNDED PRIMARY
SCHOOLS
99,475 15.7 11,517 18.8 1,038 19.2 0 0.0
STATE-FUNDED SECONDARY SCHOOLS
73,325 18.4 8,121 20.3 815 21.9 3 7.3
STATE-FUNDED SPECIAL SCHOOLS
13,993 12.5 1,302 14.7 4 1.1 0 0.0
Speech, language and communication needs
In England 234,076 (2.7%) of pupils have a speech, language and/or
communication need. Over 75% of these children, 183,769 (78.5%),
attend state-funded primary schools, 43,143 (18.4%) state-funded
secondary schools, with a further 7,164 (3.1%) attending special schools.
Within Cornwall, 1,850 pupils (2.5% of all pupils, and 18.6% of all pupils
with an identified SEN) have speech, language and communication needs
listed as their primary need; this is slightly lower than the regional and
national average. Eleven pupils on the Isles of Scilly have been identified
20
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen 21
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 34
18/12/18 V 0.9 Final
as having speech, language and communication needs.
Number and percentage of pupils with speech, language
and communication needs 201721
ENGLAND SOUTH WEST Cornwall IoS
No % No % No
% No %
STATE-FUNDED
PRIMARY SCHOOLS 183,769 29.0 17,259 28.1 1,487 27.5 0 0.0
STATE-FUNDED SECONDARY SCHOOLS
43,143 10.8 4,334 10.8 395 10.6 11 26.8
STATE-FUNDED
SPECIAL SCHOOLS 7,164 6.4 509 5.7 20 5.5 0 0.0
Hearing impairment
The number of pupils with a hearing impairment in England is 21,167,
0.2% of the population. The majority of these pupils attend state-funded
schools; 10,665 (50.4%) attend primary schools, and 9,096 (43.0%)
secondary schools. There are a further 1,406 (6.6%) pupils with a hearing
impairment attending special schools.
In state-funded schools within Cornwall 158 pupils have a hearing
impairment as their primary need, whilst there is one attending a special
school. At 0.3% those attending special schools and 1.8% attending
secondary schools are below the national average. However, primary
schools at 1.7% are in line with both the South West (1.6%) and England
(1.7%). There are no pupils on the Isles of Scilly with an identified hearing
impairment.
Number and percentage of pupils with hearing impairment 201722
ENGLAND SOUTH WEST Cornwall IoS
Number % Number % Number % Number %
STATE-FUNDED
PRIMARY SCHOOLS 10,665 1.7 999 1.6 91 1.7 0 0.0
STATE-FUNDED SECONDARY SCHOOLS
9,096 2.3 891 2.2 66 1.8 0 0.0
STATE-FUNDED SPECIAL SCHOOLS
1,406 1.3 99 1.1 1 0.3 0 0.0
22
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 35
18/12/18 V 0.9 Final
Visual impairment
In England 0.1% (11,889) of pupils have a visual impairment. The
majority of these pupils attend state-funded schools; 5,904 (49.7%) attend
primary schools and 5,225 (43.9%) secondary schools, with a further 760
(6.4%) attending special schools.
In Cornwall 86 pupils who have a significant visual impairment attend
state-funded schools; as a percentage it is in line with the national
average. 51 (0.9%) pupils attend primary schools, and 35 (0.9%)
secondary schools. There are no pupils attending special schools. There
are no pupils on the Isles of Scilly who have visual impairment.
Number and percentage of pupils with visual impairment 201722
ENGLAND SOUTH WEST
T
Cornwall IoS
Number % Number % Number % Number %
STATE-FUNDED
PRIMARY SCHOOLS 5,904 0.9 535 0.9 51 0.9 0 0.0
STATE-FUNDED SECONDARY SCHOOLS
5,225 1.3 423 1.1 35 0.9 0 0.0
STATE-FUNDED SPECIAL SCHOOLS
760 0.7 32 0.4 0 0.0 0 0.0
Multi-sensory impairment
In England 0.03% (2,719) of pupils have a multi-sensory impairment.
66.8% of these pupils (1,815) attend state-funded primary schools, 635
(23.4%) state-funded secondary schools, with a further 269 (9.9%)
attending special schools.
In Cornwall 48 pupils have a multi-sensory impairment as their primary
need, with a slightly higher than national percentage attending primary
schools. At 0.7% those attending primary schools are higher than the
regional and national average. There are no pupils on the Isles of Scilly
who have multi-sensory impairment.

JSNA Special Education Needs and Disabilities 36
18/12/18 V 0.9 Final
Autistic spectrum disorder
Within Cornwall there are 792 pupils recognised has having autistic
spectrum disorder as their primary need; again, as a percentage of pupils
within the region, this is higher than both the South West and England,
particularly those attending special schools. 332 (6.1%) pupils attend
primary schools, and 339 (9.1%) secondary schools, both of which are
comparable to the national average. 121 (33.1%) with autistic spectrum
disorder attend special schools, which is substantially higher than both
England (26.9%) and the South West (23.3%). This increased percentage
may be a reflection of the availability of state-funded special schools in
Cornwall. There are four pupils on the Isles of Scilly who are identified as
having an autistic spectrum disorder.
Number and percentage of pupils with autistic spectrum disorder 201724
ENGLAND SOUTH WEST Cornwall IoS
No % No % No % No %
STATE-FUNDED PRIMARY
SCHOOLS 42,494 6.7 3,287 5.4 332 6.1 0 0.0
STATE-FUNDED
SECONDARY SCHOOLS 35,706 8.9 3,475 8.7 339 9.1 4 9.8
STATE-FUNDED SPECIAL
SCHOOLS 30,203 26.9 2,069 23.3 121 33.1 0 0.0
23
Special educational needs in Cornwall January 2017 Government
Statistics https://www.gov.uk/government/collections/statistics-special-educational-needs-sen
24
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen
Number and percentage of pupils with multi-sensory impairment 201723
ENGLAND SOUTH WEST
T
Cornwall IoS Numbe
r % Number % Number % Number %
STATE-FUNDED PRIMARY SCHOOLS
1,815 0.3 223 0.4 39 0.7 0 0.0
STATE-FUNDED
SECONDARY SCHOOLS 635 0.2 80 0.2 8 0.2 0 0.0
STATE-FUNDED SPECIAL SCHOOLS
230 0.2 21 0.2 1 0.3 0 0.0

JSNA Special Education Needs and Disabilities 37
18/12/18 V 0.9 Final
Other difficulty/disability
443 pupils in Cornwall do not fall within the above categories and are
placed in the other difficulty/disability category. These pupils all attend
state-funded mainstream schools. These values are slightly lower than
national and South West values.
Number and percentage of pupils with other difficulty/disability 201725
ENGLAND SOUTH WEST Cornwall IoS
Number % Number % Number % Number %
STATE-FUNDED
PRIMARY SCHOOLS 26,601 4.2 2,793 4.6 216 4.0 0 0.0
STATE-FUNDED
SECONDARY SCHOOLS 26,081 6.5 2,800 7.0 224 6.0 4 9.8
STATE-FUNDED
SPECIAL SCHOOLS 1,660 1.5 231 2.6 0 0.0 0 0.0
Educational attainment
Children with a low level of educational attainment are almost five times as
likely to be in poverty now and 11 times as likely to be severely materially
deprived in the future as those with a high level of education2628.
The following information gives a summary of the headline performance
measures for 2017. It includes all stages in education from early years
through to Key Stage 4 (KS4). The data comes from the Local Authority
Interactive Tool (LAIT), National Statistics, and Department for Education
(DfE) publications, such as Assessing Schools’ Performance.
The early years foundation stage profile (EYFSP) is a teacher assessment of
children’s development at the end of the academic year in which the child
turns five.
25
Special educational needs in Cornwall January 2017 Government Statistics https://www.gov.uk/government/collections/statistics-special-educational-needs-sen 26
Intergenerational transmission of disadvantage in the UK & EU
http://www.ons.gov.uk/ons/rel/household- income/intergenerational-transmission-of-poverty-in-the-uk---eu/2014/blank.html#tab-1--Key-points

JSNA Special Education Needs and Disabilities 38
18/12/18 V 0.9 Final
Achievement in EYFSP teacher assessments by SEN provision, 2017
A good level of development
England
Cornwall
Isles of Scilly
% achieving % achieving % achieving
All 71 69 -
No SEN 76 73 -
SEN Support 27 24 -
EHC plan 4 - -
It is recognised in Cornwall that outcomes for a good level of development
for children with SEN Support who do not have an EHC assessment are currently 3% lower than national. Our target is to be at least in line with
national outcomes and to move from a quartile band of C on the current LAIT to band A or B.
The phonics (word reading skills) screening check shows the percentage of
children meeting the expected standard for all children in year 1.
Achievement of expected standards in the year 1 phonics test, 2017
A good level of development
England
Cornwall
Isles of Scilly
% achieving % achieving % achieving
All 81 78.8 -
No SEN 87 84.3 -
SEN Support 47 39.9 -
EHC plan 18 17.1 -
In Cornwall, the percentage of pupils achieving the expected standards in
phonics has fallen from the previous reported year year and is now below
the national average for all pupils. The numbers are too small for the Isles
of Scilly for the data to be available.
Pupils take standardised tests in year 2 – this is the end of Key Stage 1.
The percentages of pupils achieving the expected standards are shown in
the following table.

JSNA Special Education Needs and Disabilities 39
18/12/18 V 0.9 Final
Percentage of pupils achieving the expected standards at KS1, 2017
Reading Writing Maths
England
Cornwall
IoS
England
Cornwall
IoS
England
Cornwall
IoS
All 76 74.2 - 68 65.1 - 75 71.2 -
No SEN 84 81.2 - 77 72.0 - 83 78.3 -
SEN Support 34 26.2 - 23 17.7 - 35 28.4 -
SEN statement or EHC plan
14 18.5 - 9 8.7 - 14 14.1 -
In Cornwall the percentage of all pupils achieving the expected standard in
reading, writing and maths is below the national average. The
performance in reading of pupils with a statement or EHC plan is better
than the national average, whilst the performance in writing and maths of
pupils with a statement or EHC plan is close to the national average. The
attainment of SEN Support in Key Stage 1 remains an area for
development.
There is no data for the Isles of Scilly due to the small numbers.
In terms of progress, this is measured by how much progress pupils make
in reading writing and maths between the end of Key Stage 1 and the end
of Key Stage 2, compared with pupils across England who had similar
results at the end of Key Stage 1.
Progress score for Cornwall from KS1 to KS2, 2017
Reading Writing Maths
All -0.09 0.01 -1.02 No SEN 0.22 0.64 -0.76
SEN Support -1.52 -3.13 -2.36 SEN statement or EHC plan
-3.00 -4.48 -4.00
A score above zero means that pupils have made more progress on
average, than pupils across England who got similar results at the end of
KS1. A score below zero means that pupils made less progress. A
negative score does not mean that pupils have made no progress.
The DfE ranks the performance of all local authorities. Upper quartile
banding (A and B) is better than national average, C is equivalent to
national average, and D is below national average.

JSNA Special Education Needs and Disabilities 40
18/12/18 V 0.9 Final
DfE performance score for Cornwall from KS1 to KS2, 2017
Reading Writing Maths
No SEN C C D SEN Support B C C SEN statement or EHC plan
C C D
The progress of SEN pupils is similar to the progress of SEN pupils
nationally. There are two areas of note: the progress of pupils with SEN
support in reading, which is ranked in quartile B; and the progress in
maths of pupils with an EHC plan, which is in the lowest quartile (D).
Attainment in mathematics is a priority area for development for pupils
with and without special educational needs in Cornwall and in the
neighbouring local authorities. Action is being taken through support from
School Effectiveness Cornwall for identified schools, and School
Improvement Fund bids through the Cornwall and East Devon Maths Hub –
a joint bid with Devon LA – and a Cornwall bid specifically targeted upon
SEN students’ progress in mathematics.
Percentage of pupils achieving the expected standards at KS2, 2017
Reading Writing Maths
England
Cornwall
IoS
England
Cornwall
IoS
Englan
d
Cornwall
IoS
All 71 71.8 82 76 76 41 75 71.5 71
No SEN 80 79.2 - 86 85.3 - 83 79.5 -
SEN Support 37 36.2 - 34 31.2 - 41 33.5 -
SEN statement
or EHC plan 15 18.9 - 13 11.5 - 15 12.3 -
In Cornwall performance data is in line with national outcomes for reading
and writing. The percentage of pupils achieving the expected standard in
maths is below the national average. SEN Support is below national
average, but has improved since 2016. The performance in reading of
pupils with an EHC plan is a strength in Cornwall.
The data for the Isles of Scilly is too limited to draw meaningful conclusions.
A new secondary school accountability system was implemented in 2016. Progress 8 measures the progress a pupil makes from the end of KS2 to
the end of KS4. However, due to the limited number of entries for some pupils with SEN, the Progress 8 measure does not reflect the full KS4

JSNA Special Education Needs and Disabilities 41
18/12/18 V 0.9 Final
population.
At KS4 there is significant variation in the number of qualifications pupils
with SEN are entered for. The number of entries for SEN Support pupils
has risen, although the number of entries for pupils on EHC plans remains
similar to 2016.
Average Progress 8 scores for pupils with no identified SEN ranks Cornwall
74 in the national ranking of all local authorities (quartile banding C).
Average Progress 8 scores for pupils at SEN Support are 82 (quartile
banding C). For pupils with an EHC plan, Cornwall’s rank is 61 (quartile
banding B), above average.
Average Progress 8 scores at KS 4, 2017
P8 English Maths
England Cornwall IoS England Cornwall IoS England Cornwall IoS
All 0 -0.03 -0.57 -0.03 -0.14 - -0.02 -0.11 -
No SEN 0.07 0.06 -0.53 -0.07 0.06 - 0.04 -0.05 -
SEN Support -0.43 -0.46 - -0.03 -0.45 - -0.02 -0.44 -
SEN statement or
EHC plan -1.04 -0.98 - -0.03 -0.99 - -0.02 -0.69 -
Attainment 8 measures the average achievement of pupils in up to eight
qualifications: English and maths (double weighted), three subjects fulfilling
the EBacc criteria, and a further three qualifications (open element).
Average Progress 8 scores at KS 4, 2017
P8 English Maths
England Cornwall IoS England Cornwall IoS England Cornwall IoS
All 0 -0.03 -0.57 -0.03 -0.14 - -0.02 -0.11 -
No SEN 0.07 0.06 -0.53 -0.07 0.06 - 0.04 -0.05 -
SEN Support -0.43 -0.46 - -0.03 -0.45 - -0.02 -0.44 -
SEN statement or
EHC plan -1.04 -0.98 - -0.03 -0.99 - -0.02 -0.69 -
SEN Support pupils do not do quite as well as the national average,
although the difference is not large. Pupils with a statement or EHC plan

JSNA Special Education Needs and Disabilities 42
18/12/18 V 0.9 Final
perform in line with the national average.
Average Attainment 8 scores for pupils in Cornwall with no SEN ranks
Cornwall 85 out of all local authorities (quartile banding C). Average
Attainment 8 scores for pupils with SEN Support is ranked 82 (quartile
banding C), whereas for pupils with a statement or EHC plan, Cornwall is
ranked 61 (quartile banding B).
The attainment summary shows that the percentage of 5 year olds who
finish the foundation stage at a good level of development is below
national average for all measures and standards of achievement. As a
population they continue to be below the national average level at KS1 in
phonics and the standardised tests in year 2.
However, by the end of KS2 Cornwall performance has caught up, and
overall performance is at, or above national standards in reading and
writing. Attainment of SEN Support pupils in reading, writing and maths
has improved now quartile C.
Standards and progress in maths remains an area of focus for Cornwall’s
Primary Schools for all pupils. This is the one area where pupil progress is
in the lowest quartile nationally for SEN Support pupils.
Progress and attainment in Cornwall’s secondary schools is similar to 2016
in terms of national rankings. Pupils with an EHC plan perform the best,
being in the upper quartiles for all local authorities for both progress and
attainment.
Elective home education
In May 2018 there were 1,077 pupils in Cornwall who are electively
educated at home (source: Capita One). Of these, 52 (4.8%) have an
education, health and care plan, although there are no SEN Support
figures. This percentage is higher than those not electively educated at
home (2.4%).
Of the pupils electively educated at home with an EHC plan, the largest
group is those with an autistic spectrum disorder (24, 46%).

JSNA Special Education Needs and Disabilities 43
18/12/18 V 0.9 Final
Absences and exclusions from education
Persistent absentees are defined as having an overall absence rate of
around 15% or more. This equates to 56 or more sessions of absence
(authorised and unauthorised) during the year for pupils aged between 5
and 14, and 46 or more sessions of absence (authorised and unauthorised)
during the year for pupils aged 15.
Absenteeism (both authorised and unauthorised) in Cornwall in 2013/1427
is in line with the South West and England, where all have a persistent
absenteeism percentage of 2.6%. The Isles of Scilly have a persistent
absenteeism percentage of 2.5%. The most noticeable percentage
difference is in those with SEN with a statement where it is 9.1% in
Cornwall as opposed to 11.0% in England. The numbers of pupils on the
Isles of Scilly are too small to be able to draw meaningful conclusions. It
should be noted that the data for absenteeism is old, and may not reflect
the current situation.
In terms of exclusions, the most recent data from the DfE school census for
the academic year 2016/17 shows that in Cornwall there were 84
permanent exclusions, with 48 (57%) of these being pupils with identified
SEN. Twenty (24%) of these exclusions were for pupils with social,
emotional and mental health difficulties.
The most recent data shows that since September 2017, 64 permanent
exclusions have been recorded, with 27 (42%) pupils having an identified
SEN, and six with no SEN, no permanently excluded pupil had an EHC
plan.
There were 3,165 fixed term exclusions in Cornwall, of which 1,956 (62%)
related to pupils with an identified SEN. Of those fixed term exclusions,
the largest percentage was for pupils with social, emotional and mental
health difficulties (1,016, 32%).
Youth offending
A significant proportion of detained children and young people (under age
19) have special educational needs; a Ministry of Justice document in 2014
stated that approximately 18% of those in custody have a statement of
special educational need compared to 3% of children and young people
overall in England. Over 60% of children and young people in custody
27
Department for Education https://www.gov.uk/government/publications/sen-absences-and-
exclusions-additional- analysis

JSNA Special Education Needs and Disabilities 44
18/12/18 V 0.9 Final
have speech, language and communication needs28. To address these
needs the Special Educational Needs and Disability (Detained Persons)
Regulations 201529 build on the structure and principles set out primarily
in sections 70 to 75 of the Children and Families Act 2014.
The assessment tool for young offenders is AssetPlus. This assessment tool
looks at all needs and will trigger a referral to the nurses for a
Comprehensive Health Assessment. It is relatively new, so there is limited
data available. In Cornwall there are currently 260 assessments on
AssetPlus. Of these, 74 (28%) are recorded as having SEND
characteristics. However, the belief within the service is that this figure is
much higher.
Young people within the Youth Offending Service (YOS) have good access
to autism spectrum disorder (ASD) assessment, with a fast-track
arrangement ensuring they are all offered a referral within three months.
This service is currently only offered for under 16s, but the aim is to
include those who are 16+.
The screening includes physical health, mental health (including attention
deficit hyperactivity disorder (ADHD) etc.), traumatic brain injury
screening and an early help assessment initially and can then do further
assessments for SALT/communication, ASD, learning disability (LD) and
educational needs. As the data is limited, trend cannot be commented on
with any certainty. However, anecdotally, the belief is that there are a
high number of young people within the YOS who have speech, language
and communication difficulties.
NEET
Young people Not in Education, Employment or Training (NEET) cover the
age group 16-24; available statistics however cover the 16-18 age group.
In 2016 the Local Authority Interactive Tool30 showed that in Cornwall,
90% of KS4 students with EHC plans (including those attending special
schools) went on to or remained in education, employment or training.
This figure is in line with the England and South West average, which are
also 90%. The percentage of KS4 students in Cornwall with SEN Support
who went on to, or remained in education, employment or training
(including those attending special schools) was 87%. This is slightly below
28Ministry of Justice
29Government Legislation http://www.legislation.gov.uk/uksi/2015/62/contents/made
30Local Authority Interactive Tool https://www.gov.uk/government/publications/local-authority-
interactive-tool-lait

JSNA Special Education Needs and Disabilities 45
18/12/18 V 0.9 Final
England (88%), the South West (89%) and statistical neighbours (88.5%).
There were no figures available for the Isles of Scilly.
In year 12, the percentage of students with SEND who were also NEET fell
from 8.1% of the cohort in October 2017, to 5.6% of the cohort in
December. For those in year 14 with SEND who were also NEET, the
percentage rose over the same three month period from 9.8% to 13.2%31.
The Cornwall 2017/18 transitions data dashboard showed that in December
2017 for years 12-14 (aged 16-18), there were 639 young people with
SEND, with 62 (9.7%) of these being NEET. This is higher than the figure
for young people who have no identified SEND (4.4%).
Employability is a focus for Cornwall Council’s Preparing for Adulthood
work. The challenges that have to be overcome are the relatively high
proportion of small and medium sized enterprises in the Duchy and the
geographical challenges that the area presents. To address these
challenges there is an established Enterprise Adviser network, including a
specific appointment to work with special schools and area resource bases.
The successful Ambitions bid will fund Disability Access, and support posts
to work with employers and to increase opportunities. DfE funding for
Cornwall and the Isles of Scilly will be used to appoint a supported
internship coordinator to build and support a network that will extend
provision into ‘hard to reach’ areas.
Vulnerable children
Matched Capita and Mosaic data from spring 2018 shows that there were
2,668 children and young people who had an EHC plan in place. Of these,
102 children and young people were also in care, 925 identified as children
in need, and 24 had a child protection plan in place. This is shown in the
chart below.
31
CSW Group https://cswgroup.co.uk

JSNA Special Education Needs and Disabilities 46
18/12/18 V 0.9 Final
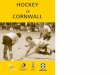
Chart showing the percentage of children and young people with EHC plans, and
those who are also identified as children in care, children in need, or the subject
of a child protection plan. Source: Children and Family Services
The most recent data for children in care who also have SEND is for the
spring term 2018. The total number of children and young people in care
in Cornwall from age 2 to the end of year 13 is 509. Of these children and
young people, there are 102 who have an EHC plan. The most commonly
identified primary need is social, emotional and mental health difficulty,
with 74 (63%) of children and young people having this as their primary
need. The numbers for the Isles of Scilly are too small to draw any
conclusions.
The total number of children and young people in care with an EHC plan is
23.0%. The equivalent national percentage is 26.7%.
Children on a child protection plan
As at 31st March 2018 there were 2,989 children in Cornwall identified as
children in need and 395 who were the subject of a child protection plan.
On the Isles of Scilly, Children’s Social Care work with many of the families
identified with SEND as they meet the local threshold of ‘Child in Need’. A
system of short break budgets supports families of children with disability
to access services and resources on the islands and mainland.
102, 4%
925, 35%
24, 1%
1617, 60%
children in care
children in need
child protection plan
EHC plan with no socialcare involvement

JSNA Special Education Needs and Disabilities 47
18/12/18 V 0.9 Final
Continuing care needs
In Cornwall there are around 40 children under 18 at any point in time with
Continuing Care packages. There are, however, far more children and
young people with high level needs who access targeted services.
Prevalence of children with SEN in areas of higher
deprivation
In the January 2017 Cornwall school census, 9,605 (13%) of school
children have an identified SEN. Of those children, 7,766 (81%) are from
the most deprived areas in Cornwall. In England, 889 (11%) of those
within the most deprived areas are in the most deprived 0-10% of LSOAs
(rank 1-3284). In the most deprived areas, 14% of children and young
people have an identified SEN, whereas for non-deprived areas, it is 11%.
Therefore, children and young people from deprived areas are more likely
to be identified as having SEN.
Of primary school children, 5,426 (13%) have SEN, of which 81% (4,418)
are within the most deprived areas in Cornwall. Of those in the most
deprived areas, 12% live in the most deprived decile for England.
Of secondary school pupils, 3,719 (13%) have SEN, of which 80% (2,967)
are within the most deprived areas in Cornwall. 11% of those within the
most deprived areas for Cornwall are also live in the most deprived decile
for England.
The Isles of Scilly are in the seventh decile nationally i.e. they are in the
30-40% least deprived LSOAs in England. They have 121 pupils with no
identified SEN; 27 at SEN support (10.4%); and 12 (4.4%) with either a
statement of educational need or an EHC plan.
A more detailed description of the prevalence of SEND in areas of
deprivation is given in appendix 7.
It should be noted that data from the school census has not been verified.

JSNA Special Education Needs and Disabilities 48
18/12/18 V 0.9 Final
Disability by ethnicity (aged 0-15), Census 201132 The child (0-18 years of age) population of Cornwall and the Isles of Scilly
is predominantly white with only 1.8% from the combined ethnic minority
groups.33
School Census ethnicity - Cornwall state-funded primary,
secondary and special schools
The comparison between 2011 and 2017 data, based on information
collected in the school census by local authority, shows that the number of
pupils in school within Cornwall has not changed significantly34, although
the number of pupils has increased in 2017. The percentage of white
pupils has decreased slightly, whilst ethnic minorities have increased.
Despite this increase, only 4.3% of pupils in Cornwall are from an ethnic
minority – this is an increase from 3.4% in 2011.
On the Isles of Scilly, 5.5% of pupils identify themselves as belonging to an
ethnic minority. However, the numbers are small, so it is difficult to draw
conclusions.
In Cornwall 14.5% of pupils have SEND. The majority are white (96.4% of
all children with SEND). This represents 14.5% of white pupils in Cornwall.
The proportion of pupils from an ethnic minority who also have SEND is
similar to the white population.
For a more detailed breakdown of prevalence of SEND by ethnic group, see
appendix 8.
SEND prevalence and language
The Special Educational Needs and Disability code of practice: 0 to 25 years
(January 2015)35 states – “Identifying and assessing SEN for young
children whose first language is not English requires particular care. Early
years practitioners should look carefully at all aspects of a child’s learning
and development to establish whether any delay is related to learning
English as an additional language or if it arises from SEN or disability.
32
Census 2011 https://www.nomisweb.co.uk/census/2011/lc3205ew 33
https://www.nomisweb.co.uk/census/2011/data_finder 34
National Statistics – Department of Education https://www.gov.uk/government/statistics 35
Department for Education, Special educational needs and disability code of practice: 0 to 25 years, January 2015 5.30

JSNA Special Education Needs and Disabilities 49
18/12/18 V 0.9 Final
Difficulties related solely to learning English as an additional language are
not SEN.” It is widely recognised that it can sometimes be very difficult to
recognise clearly the difference between the need for English as an
additional language (EAL) support and the need for SEN support.
There is a very small percentage (2.3%) of pupils in Cornwall whose first
language is not English. This percentage has risen, only slightly, from
1.7% over the past three years. Although small, there may be a wide
range of languages to consider.
86% of all primary and secondary school children with English as an
additional language have no SEN. A very high percentage (90.5%) of
pupils with English as a second language come from a black and minority
ethnic background and 37.9% are in the 30% most deprived areas.
For further information about SEND prevalence and language, see appendix
8.
SEND prevalence and gender and age
In terms of SEN, there are more males than females. 12% of boys are
identified as having an SEN, and 5% of girls. Boys make up 70% of those
identified with SEN. There are approximately three times as many boys
with EHC plans, and around 70% of pupils at special schools are boys36.
On the Isles of Scilly the large majority of EHC plans that are in place are
for boys.
Nationally, over all ages there are slightly more (51.5%) females with long
term health problems or disabilities37. Within Cornwall this percentage
changes; in the 0 to 15 year category with 51.4% male and 50.5% in the
16 to 24 age group.
There are more children in the 0 to 15 year age group with long term
health problems or a disability, 51.4% of whom are males. Overall there
are 8.8% males in the 0 to 15 year age group and 5% in the 16 to 24 year
group. 16.2% of females overall with long term health problems or a
disability are in the 0 to 15 year age group, with 9.5% in the 16 to 24 year
group.
36
Gender and education: the evidence on pupils in England
http://webarchive.nationalarchives.gov.uk/20090108131527/http://www.dcsf.gov.uk/research/data/uploadfiles/RTP01 -07.pdf 37
Long Term Health or Disability https://www.nomisweb.co.uk/census/2011/lc3302ew

JSNA Special Education Needs and Disabilities 50
18/12/18 V 0.9 Final
SEND prevalence and religion38
For information on SEND prevalence and religion, see appendix 9
SEND prevalence and gender reassignment
There are no local figures on gender variance and gender reassignment.
38
Census 2011 https://www.nomisweb.co.uk/census/2011/lc3207ew

JSNA Special Education Needs and Disabilities 51
18/12/18 V 0.9 Final
Health determinants
Older mothers
The trend in Cornwall and the Isles of Scilly shows that the actual numbers
of births to older mothers has increased between 2009 and 2016,
particularly in 35 to 39 year olds where it had increased by 11%. This
trend is seen nationally. As women get older this is an increased risk of
pregnancy-related complications and health problems both to mothers and
babies. There is an increased chance of having a baby with a congenital
abnormality. Women over the age of 40 represent 3.8% of all births in
Cornwall and the Isles of Scilly39. This is slightly lower than England
(4.3%) and the South West (4.2%). Age of carer will therefore need
consideration as a child’s support needs increase with age.
Young mothers Around 60% of babies who are subject to SCR (serious case reviews) are
born to mothers under the age of 21.
Babies born to mothers under the age of 21 have a 56% higher risk of
infant mortality and are at 3 times the risk of SUDI (sudden unexpected
death of an infant). They are also twice as likely to attend hospital with an
illness, accident or injury and have a 21% higher chance of a low birth
weight or premature birth which rises to 95% for subsequent children.
Premature babies are at increased risk of neurodevelopment impairments,
respiratory and gastrointestinal complications.
Cornwall and the Isles of Scilly have a slightly higher percentage of babies
born to mothers under the age of 20 (3.6%) compared with England
(3.2%) and the South West (3.0%).
39
South West Clinical Network Maternity Dashboard (2018) Online:
https://maternitydashboard.swscn.org.uk/

JSNA Special Education Needs and Disabilities 52
18/12/18 V 0.9 Final
Smoking during pregnancy
Babies from deprived backgrounds are more likely to be born to mothers
who smoke, and to have much greater exposure to second-hand smoke in
childhood40.
Smoking remains one of the few modifiable risk factors in pregnancy. It
can cause complications during labour and an increased risk of
miscarriage, premature birth, stillbirth, low birthweight and sudden
unexpected death in infancy, and placental complications that could lead to
disabilities41.
Children may also suffer from on-going health risks such as symptoms of
asthma and problems of ear, nose and throat if growing up in a home
where there are smokers.
Data from NHS Digital42 shows that 13.3% of women were smoking at the
time of delivery in 2017/18.
Known smokers at time of delivery
Total Maternities Known Smokers
England South
West* CIoS** England
South
West* CIoS**
2009/10 647,378 57,185 5,181 90,908 8,069 809
14.0% 14.1% 15.6%
2010/11 659,067 58,640 5,422 89,036 7,860 776
13.5% 13.4% 14.3%
2011/12 665,081 59,512 5,659 87,731 7,884 776
13.2% 13.2% 13.7%
2012/13 657,551 58,588 5,514 83,506 7,817 759
12.7% 13.3% 13.8%
2013/14 632,956 16,742 5,394 75,913 2,150 733
12.0% 12.8% 13.6%
2014/15 622,643 15,958 5,129 70,879 1,957 711
11.4% 12.3% 13.9%
2015/16 631,225 32,50
5 5,186 67,195 3,821 688
10.6% 11.8% 13.3%
2016/17 619,234 31,95
3 5,017 65,02
3 3,761 644
10.5% 11.8% 12.8%
2017/18 602,499 32,36
7 4,980 64,11
4 3,628 660
10.6% 11.2% 13.3% * South West becomes Devon, Cornwall & Isles of Scilly from 2013
**Cornwall & Isles of Scilly becomes NHS Kernow from 2013 Data from NHS Digital
40
Statistics on Women's Smoking Status at Time of Delivery, HSCIC 41
NICE, 2010, P22 42
NHS Digital (2017) Statistics on women’s smoking at time of delivery Online:
https://digital.nhs.uk/catalogue/PUB24222

JSNA Special Education Needs and Disabilities 53
18/12/18 V 0.9 Final
Maternal diet
Maternal diet plays an important role in the antenatal development of the
child. The ingestion of certain foods and supplements can offer benefits
to an unborn child. Folic acid has been identified as reducing the
incidence of major birth defects including spina bifida. All women are
recommended to supplement their diet with folic acid before pregnancy
and this dosage is increased if women have a BMI over 35, are epileptic
or have had a previous affected baby. However, as the cost of folic acid
over the counter is less than that of a prescription, it is not known how
many women actually purchase and use folic acid supplements.
Maternal obesity
Women who are obese when they become pregnant face an increased risk
of complications during pregnancy and childbirth. These include the risk of
impaired glucose tolerance, gestational diabetes, miscarriage, pre-
eclampsia, thromboembolism and maternal death (Centre for Maternal
and Child Enquiries and the Royal College of Obstetricians and
Gynaecologists 2010)43. Children of obese parents are also more likely to
be obese themselves.
Data for Cornwall and the Isles of Scilly from the Maternity Services
Statistics (2018) indicates that 22.9% of mothers are obese at the time of
booking their pregnancy leading to a higher risk of complications at birth.
Low birth weight
Low birth weight is closely associated with foetal and neonatal mortality
and morbidity, inhibited growth and cognitive development and chronic
diseases later in life. A baby’s low weight at birth is either the result of
preterm birth (before 37 weeks of gestation) or due to restricted foetal
(intrauterine) growth. Low birth weight has been defined by the World
Health Organisation (WHO) as weight at birth of less than 2,500 grams44.
Very low birthweight is defined as weight at birth less than 1,500 grams45.
43
Centre for Maternal and Child Enquiries and Royal College of Obstetricians and Gynaecologists (2010)
Joint Guideline: Management of Women with Obesity in Pregnancy. Online 44
NHS Digital (2017) Statistics on women’s smoking at time of delivery Online:
https://digital.nhs.uk/catalogue/PUB24222 45
UNICEF and WHO, 2004, p.21

JSNA Special Education Needs and Disabilities 54
18/12/18 V 0.9 Final
The main risk factors for low birth weight are nutritional status of the
mother, smoking in pregnancy, substance misuse, low uptake of prenatal
care and psycho- social factors causing stress and depression46
The rate of low birth weights across Cornwall and the Isles of Scilly over
the last 10 years has been generally below national rates, and largely in
line with rates in the South West47. This suggests that this is not a
particular factor for SEND in Cornwall and the Isles of Scilly.
Gestational age
The World Health Organization (WHO) defines prematurity as babies born
before 37 weeks from the first day of the last menstrual period48.
Premature babies are at increased risk of neurodevelopment impairments,
respiratory and gastrointestinal complications. The EPICure studies looked
at premature babies born in hospitals throughout England in 1995 and
2006, and found that 80% of babies born under 26 weeks gestation had
some form of impairment49.
Survival rates of pre-term babies have improved in recent years. The
EPICure study looked at survival rates and ongoing illnesses or
complications affecting babies born extremely prematurely (between 22
and 26 weeks of pregnancy) in England in 2006 and 199550. Their main
finding was that when comparing survival-to-discharge rates (meaning
babies were eventually thought to be well enough to leave hospital)
between 1995 and 2006, there was an increase from 40% in 1995 to 53%
in 2006. However, there was no difference in the level of ongoing illnesses
or disabilities affecting these surviving babies, i.e. more preterm babies
are surviving to be discharged from hospital with no increase in the
numbers with illness or disability.
46
NICE 2003 47
Fingertips tool https://fingertips.phe.org.uk/profile-group/child-health/profile/child-health-pregnancy 48
World Health Organisation (2013) Preterm births, Available:
http://www.who.int/mediacentre/factsheets/fs363/en/ 49
EPICure studies. BMJ 2012 50
Costeloe KL, Hennessy EM, Haider S, et al. Short term outcomes after extreme preterm birth in
England: comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ. Published online December 4 2012

JSNA Special Education Needs and Disabilities 55
18/12/18 V 0.9 Final
Screening and immunisation
Antenatal and new-born screening
Screening is a way of identifying apparently healthy people who may have an increased risk of a particular condition. The NHS offers a range of
screening tests to pregnant women and their children.
This image explains how the screening process can be compared to putting people through a sieve
The sieve represents the screening test and most people pass through it. This means they have a low chance of having the condition screened for.
The people left in the sieve have a higher chance of having the condition. A
further investigation is then offered to them. Identification through this process can show that they have the condition screened for. The person
may need further confirmatory diagnostic tests.

JSNA Special Education Needs and Disabilities 56
18/12/18 V 0.9 Final
The UK National Screening Committee (UK NSC) currently recommends the offer of:
Antenatal screening:
Sickle cell and thalassaemia
Fetal anomaly (T21, T18, T13 & fetal anomaly ultrasound)
Infectious diseases (hepatitis B, HIV, syphilis)
New-born screening:
Newborn blood spot
Newborn and infant physical examination
Newborn hearing screening
Antenatal and neonatal screening programmes work well at a population
level with a high degree of offer to the population with quality monitoring
and appropriate failsafe programmes. They will generate referral into other
programmes for a small number of people including diagnosis and care.
They are not designed to report on outcomes.
Data for 2017/18 from Public Health England51 shows that population
coverage of the programmes in Cornwall is good, with all but one
programme meeting acceptable levels of coverage. The only one where
coverage was not as expected is for the new- born physical examination
(90.8% target 95%).
Child health records department
The Child Health Information Service (CHIS) works closely with the
screening team to ensure at all children who live in Cornwall receive their
new-born blood spot screening according to the national guidelines. CHIS
records the screening results that have been emailed by the laboratories in
Bristol onto the child’s health record. In addition to the screening team,
CHIS also monitors the child health system failsafe and the national
failsafe to ensure that children are not missed.
51
Public Health England (2018) NHS screening programmes: KPI reports 2017 to 2018. Online:
www.gov.uk/government/publications/nhs-screening-programmes-kpi-reports-2017-to-2018

JSNA Special Education Needs and Disabilities 57
18/12/18 V 0.9 Final
Vaccinations
One thing that can help protect all children from ill health is ensuring that
they are vaccinated against infectious diseases. Vaccines work by making
our bodies produce antibodies that fight diseases, they do this without
infection. When a child who has been vaccinated comes in contact with a
disease their body will already be able to fight off an infection as they will
be able to quickly produce antibodies52.
It is important to ensure that as many children as possible are vaccinated
in order to prevent illness in children who cannot be vaccinated; this is
called “herd immunity”.53 Usually 95% of the child population need to be
vaccinated to protect against disease in the wider population.
A vaccination programme that protects children against 13 diseases is
offered during childhood. Some vaccinations require multiple doses to be
affective against specific diseases.
Evidence summarised by NICE (2016)54,55,56,57 show that children and young
people with risk factors associated with child poverty may also be at risk of
not being fully immunised, these children include:
• Looked after children
• Children with physical or learning disabilities
• Children of teenage or lone parents
• Younger children from large families
• Vulnerable children, such as those whose families are
travellers, asylum seekers or are homeless
• Those who have missed previous vaccinations (whether as
a result of parental choice or otherwise)
• Those not registered with a GP
• Children who are hospitalised or have a chronic illness
• Those from some minority ethnic groups
• Those from non-English speaking families
52
NHS Choices (2018) How vaccines work. Online: www.nhs.uk/conditions/vaccinations/how-vaccines-
work/ 53
NICE (2016) Quality standard topic: Vaccine uptake in under 19s. Online:
www.nice.org.uk/guidance/qs145/documents/briefing-paper 54
Department of Health (2005) Vaccination services: reducing inequalities in uptake. London:
Department of Health 55
Hill CM, Mather M, Goddard J (2003) Cross sectional survey of meningococcal C immunisation in
children looked after by local authorities and those living at home. BMJ 326: 364–5 56
Peckham C, Bedford H, Seturia Y et al. (1989) The Peckham report – national immunisation study: factors influencing immunisation uptake in childhood. London: Action Research for the Crippled Child 57
Samad L, Tate AR, Dezateux C et al. (2006) Differences in risk factors for partial and no immunisation
in the first year of life: prospective cohort study. BMJ 332: 1312–3

JSNA Special Education Needs and Disabilities 58
18/12/18 V 0.9 Final
Unfortunately, data is not available that tells us about which groups are missing out on vaccinations in Cornwall and the Isles of Scilly.
Information from the health visitor needs assessment (2018) The 2018 health visitor needs assessment58 reported on the three
questions that are asked in the early help assessment that are relevant
to this needs assessment. The three questions were about children with
special educational/medical needs; speech and language delay; and
developmental delay (other than speech and language).
Children from the health visitor survey identified with the following needs
2015/16 2016/17 2017/18 Number % Number % Number % Children with
special educational/ medical needs
0 0 328 1.6 417 2.4
Speech and language
delay
236 1.1 913 4.3 1,086 6.1
Developmental
delay (other than speech
and language)
533 2.5 1,028 4.9 1,155 6.5
Children from the most deprived LSOAs in Cornwall identified
with the following needs
Number % Number % Number % Children with special
educational/ medical needs
0 0 35 2.4 42 3.4
Speech and
language delay
19 1.3 76 5.2 100 8.0
Developmental delay (other than speech and language)
53 3.6 100 6.8 110 8.8
This table shows that children from the most deprived decile have higher
percentages of children with special educational/medical needs; speech
and language delay; and developmental delay other than speech and
language.
58
Public Health, Cornwall Council (2018) Health visiting needs assessment: 0-5 healthy child
programme

JSNA Special Education Needs and Disabilities 59
18/12/18 V 0.9 Final
Injuries to children and young people
Injuries to children and young people can lead to ongoing medical
problems and special educational needs.
Accidental injuries are a major health problem throughout the United
Kingdom59 and one of the most common causes of death in children
over one year of age. Every year they leave many children and young
people permanently disabled or disfigured.
Those most at risk from a home accident are the 0-4 years age group.
Falls account for the majority of non-fatal accidents while the highest
numbers of deaths are due to fire. Most of these accidents are
preventable through increased awareness, improvements in the home
environment and greater product safety.
A&E attendances of children (0-4 years)60
England South West
Cornwall and IoS
2010/11 483.9 413.7 398.8
2011/12 510.8 427.0 420.3
2012/13 534.9 437.3 413.5
2013/14 525.6 431.7 400.6
2014/15 540.5 446.2 423.5
2015/16 588.1 469.3 458.2
2016/17 601.8 477.2 520.7
Attendances at A&E have been increasing – this is a national and regional
trend. However, the increase may be due to parents finding it difficult to
get appointments at their GP, so they take their child to A&E departments
as an alternative.
Hospital admissions have been dropping steadily since 2010. Admissions in
the 0-14 year age group have reduced by 21% and 15-24 years by 27%.
Cornwall and the Isles of Scilly are similar to both national and the South
West.
59
The Royal Society for the Prevention of Accidents http://www.rospa.com/home-safety/advice/child-
safety/accidents- to-children/ 60
Hospital admissions http://www.localhealth.org.uk/#l=en;v=map7

JSNA Special Education Needs and Disabilities 60
18/12/18 V 0.9 Final
Hospital admissions caused by injuries in children61
0-14 years 15-24 years
England South West
Cornwall and Ios
England South West
Cornwall and IoS
2010/11 115.2 109.7 131.9 154.2 162.1 209.2
2011/12 118.2 114.9 116.1 144.7 152.7 188.5
2012/13 103.8 103.9 105.5 130.7 144.2 166.2
2013/14 112.2 110.6 103.7 136.7 147.0 153.4
2014/15 109.6 111.1 114.4 131.7 145.0 125.4
2015/16 104.2 105.0 101.0 134.1 153.2 139.7
2016/17 101.5 104.3 101.8 129.2 147.9 137.0
Further information about injuries to children and young people can be
found in the health visitor needs assessment62.
61
Public Health, Cornwall Council (2018) Health visiting needs assessment: 0-5 healthy child
programme 62
Public Health, Cornwall Council (2018) Health visiting needs assessment: 0-5 healthy child
programme

JSNA Special Education Needs and Disabilities 61
18/12/18 V 0.9 Final
Child poverty Children growing up in poverty experience many disadvantages, which
accumulate across the life cycle. An evidence review by Professor
Bradshaw63 and colleagues finds the following detrimental outcomes for
children to be associated with child poverty:
mortality, morbidity, fatal accidents, mental illness, suicide, child
abuse (but not sexual abuse), teenage pregnancy, poor housing
conditions, homelessness, low educational attainment and smoking
(mainly after childhood).
Research carried out by the Children’s Society estimates that 4 in every 10
disabled children in the UK live in poverty. This compares to 3 in 10 across
all children in the UK and shows that disabled children are more likely to
live in poverty and experience the associated problems than their peers64.
If a child has a disability both parents are less likely to work, leading to
higher incidence of poverty.
Service provision - health
There are five main providers of children and young people’s health
services in Cornwall and the Isles of Scilly:
Cornwall Partnership NHS Foundation Trust provides child and
adolescent mental health services and specialist children’s services,
including speech and language therapy, community nursing services
and learning disability services.
The Royal Cornwall Hospitals Trust, Plymouth Hospitals NHS Trust
and North Devon District Hospital provide acute care and general
hospital services as well as community paediatrics, and some
community services.
Peninsula Community Health provides services including specialist
dentistry; district nursing services and physiotherapy for 16+.
Further details can be found in Supporting Educational Achievement (2017)65.
63
Bradshaw (2011) The well-being of children in the UK 64
Children’s Society (2011) 4 in every 10 Disabled children living in poverty 65
Newman S, Corlett E, Lewis j, and O’Neill B (2017) Supporting Educational Achievement – the health
contribution for children and young people aged 0-25 years with special educational needs and disabilities

JSNA Special Education Needs and Disabilities 62
18/12/18 V 0.9 Final
Children and young people’s needs66 are met from a whole range of NHS
services; some are universally available such as GPs and health visiting
services, and some are more specialised and need an assessment or
referral from a health or social care professional to access.
In Cornwall there are a range of specialist services to meet the health
needs of children and young people with:
physical or sensory difficulties
developmental delay or impairment
maintaining a healthy weight
speech, language and communication needs
difficulties with eating, drinking and swallowing
epilepsy
diabetes
mental health issues
complex and technology dependent health care needs life limiting/ life threatening conditions
The majority of children with SEND receive the support to meet their health
needs locally. However, occasionally, due to the complexity of a child or
young person’s health need, they have to be referred to highly specialised
services based outside Cornwall and the Isles of Scilly.
For under 18s there is an assessment process called Children’s Continuing
Care which may indicate that more than one agency i.e. health, social care
or education need to be involved in the care. For young people over the
age of 18 there is a similar process called NHS Continuing Health Care.
The following services assess and diagnose children with additional health
and development need, disability or lifelong conditions and therefore
demand on these services are an indication of levels of need in the system.
Health visiting
The health visitors keep children with SEND on their caseload until the child
is five. Each health visitor has children on their caseload with complex
needs. A mandatory field in the database ensures that the needs of these
children are recorded to ensure their needs are addressed.
66
https://www.supportincornwall.org.uk/kb5/cornwall/directory/localoffer.page?localofferchannel=8

JSNA Special Education Needs and Disabilities 63
18/12/18 V 0.9 Final
Community paediatrics
The overall aim of the service is to provide a consultant-led locality-based
community child health service for children and young people who are
vulnerable due to disease, disability or disadvantage. With a particular
emphasis on improving access to health services for those vulnerable
groups of children and young people who are traditionally difficult to
engage, the service aims to deliver high quality, safe, flexible and holistic
care.
The types of conditions that are managed include: physical disabilities;
children at high risk of developmental problems (e.g. as a result of
premature birth or acquired brain injury); children with delayed milestones
(e.g. speech, motor, social communication or play) who are not yet at
school; developmental co-ordination disorder (dyspraxia); hearing or
visual impairment; social communication difficulties; concerns about
attention and hyperactivity; development and learning assessment in pre-
school children; and in patients with known learning difficulties for
investigation of a possible underlying cause.
Speech and language
Speech and language therapy supports children and young people in
Cornwall aged 0- 19 years who have difficulties with communication, or
with eating, drinking and swallowing. This can include children/young
people with delay in learning to talk, speech sound production difficulties,
learning difficulties, cleft palate, stammering, selective mutism, autism,
hearing impairment and physical disabilities.
Data from the speech and language department shows that the current
caseload (May 2018) comprises 2,486 children and young people. This
number has remained largely similar over recent years. Most of these
children and young people, by the fact that they have a communication
need, will be on the SEND continuum.
Speech and language therapists (SLTs) aim to help to develop the skills of
parents/carers and other people who support the child in their everyday
environments. This ensures that therapy can be non-intrusive, practical and
most effective for the child/young person.
Available data suggests that the number of children and young people
requiring alternative and augmentative communication (AAC) is increasing.

JSNA Special Education Needs and Disabilities 64
18/12/18 V 0.9 Final
Community Therapy Services
The Children’s Community Therapy Service (CCTS) and Community
Paediatrics work in partnership within the department of Community Child
Health at the Royal Cornwall Hospital NHS Trust, delivering Occupational
Therapy, and Physiotherapy treatment, to children and young people who
present with, or are being investigated for, neurological, neuro-
developmental, neuro-muscular conditions, atypical development and/or
disabilities.
There are occupational therapists (OTs) who assess the needs of children
and young people, aged from 5 years to 17 years 11 months, with
disabilities at home, school, and in respite settings. The OT’s role is to
enable children and young people to become as independent as possible in
daily living activities, and help find solutions to any barriers which are
preventing this.
CAMHS
Child and adolescent mental health services (CAMHS)67 helps children
and young people deal with emotional, behavioural or mental health
issues, including:
Emotional problems e.g. anxiety, depression, anger, mood
swings, low self- esteem.
Behaviour problems e.g. violence, destructiveness, self-harm,
hyper-activity, over-sexualisation and obsession.
Relationship problems, including difficulties in the family, with
friends or colleagues, in school or the community, as well as
difficulties associated with attachment and loss.
Problems with development or disability e.g. bed-wetting and
difficulties with eating, sleeping or talking.
Emotional problems linked to physical health issues e.g.
difficulties with taking medication as prescribed by a doctor.
NHS England has made a commitment that by 2020/21, there will be a
significant expansion in access to high-quality mental health care for
children and young people.
67CAMHS

JSNA Special Education Needs and Disabilities 65
18/12/18 V 0.9 Final
At least 70,000 additional children and young people each year across
England will receive evidence-based treatment – representing an increase
in access to NHS-funded community services to meet the needs of at least
35% of those with diagnosable mental health conditions.
NHS England has set targets regarding the percentage of children and
young people accessing NHS funded mental health services within 28 days
of referral. For 2018/19 this is 32% of the children with specialist mental
health service needs rising to 38% in 2022. The proportion of children and
young people receiving an assessment following acceptance of a referral
into specialist mental health services (CAMHS) is on an upward trend rising
with an average of 73.1% seen within 28 days between April and July
2018. There has been an 8% reduction in 28 day waiting breaches.
Transition to adult mental health services
Mental health services for teenagers are split between child and adolescent
mental health services (CAMHS) and adult mental health services (AMHS).
According to the TRACK study (2015)68 the time point when a young
person transfers to AMHS can lie between the ages of 16 and 18 years. As
adult services focus on severe mental illness, young people with other
ongoing mental health disorders, such as emotional, neurodevelopmental
(e.g. autism spectrum disorder, attention-deficit hyperactivity disorder
(ADHD)) or emerging personality disorders can fall through the CAMHS-
AMHS gap. There is concern that these young people have poor outcomes
(e.g. increased rates of attendance at accident and emergency
departments, employment problems, contact with criminal justice and
social care systems).They may present to adult services later, when in
crisis or having developed severe and enduring mental health problems.
In Cornwall and the Isles of Scilly there was not an organised system for
transition to adult services that worked in harmony with families and other
agencies.
Data tells us the number of young people who transfer to adult services but
this does not give a picture of the transition. The TRACK study found that
the most common outcomes were discharge to a general practitioner and
ongoing care with CAMHS with little indication of use of third sector
68
Islam Z et al (2015) Mind how you cross the gap! Outcomes for young people who failed to make
the transition from child to adult services : the TRACK study. BJPsych Blletin, 1-8

JSNA Special Education Needs and Disabilities 66
18/12/18 V 0.9 Final
organisations. Most of these young people had emotional/neurotic
disorders and neurodevelopmental disorders.
The clinical implications out of this study identified that GPs and CAMHS are
left with the responsibility for the continuing care of young people for
whom no adult mental health service could be identified. GPs may not be
able to offer the skilled ongoing care that these young people need.
NHS commissioning incentives have prompted a transition refresh project.
A checklist of timelines, who to speak to, and when to start has been
developed in conjunction with services and families.
The process will start at 17 with a referral to adult services and self-
assessment to understand what a young person’s transition goals are. At
17½ there will be a joint meeting with CAMHS and adult mental health
services, usually at school. Six months after transition another survey is
sent out to see if their transition goals have been met. Some goals e.g.
going to university may not be met but will be outlined at the meeting,
making the team around them aware of what is in their best interest.
A transitions webpage has been developed with a guide on where to go for
help. There will also be a second level for professionals with more detailed
information to help avoid unnecessary incorrect referrals.
Schools are keen to act as hubs for the transition meetings. The schools
have spent more time than any other agency with the young person. If
schools act as hubs they will be automatically included in the transition
process.
Transition generally happens at the wrong time for young people. For
health services this happens at 18 and can cause considerable stress.
CAMHS children services are pretty inclusive whereas adult services have a
narrower focus which causes anxiety about access to services. There are
no adult autism or ADHD services. The project is also looking for a better
connection with primary care to assist coordination of care and reduce
stress that may lead to a demand for adult services later on with the
development of mental health issues.

JSNA Special Education Needs and Disabilities 67
18/12/18 V 0.9 Final
Special parenting service
The special parenting service (SPS) supports parents who have mild to
borderline learning disability. The service is provided by a range of
professionals who work with families to improve parenting skills. Their role
is to help parents understand the needs of their children, and in particular,
how to keep their children safe; set routines for their baby or child; how to
manage their child’s behaviour; and how to access further support and
help.
The following chart shows the number of referrals to the SPS for three
complete years, and the referrals to date for this year.
Autistic spectrum disorder assessment team
The autistic spectrum disorder assessment team (ASDAT) is offered by
Cornwall Partnership Foundation Trust. It is a diagnostic service for
children and young people aged between 5½ and 16, who have complex
social and communication difficulties.
The ASDAT team is made up of the following disciplines: child and
adolescent psychiatry; child psychology; occupational therapy; and
speech and language therapy.
As of March 2018, data from ASDAT showed that there were 659 children
and young people who are waiting for an assessment for autism using
the ASDAT pathway (0-18). The waiting time for under 5s is 173 days
and for older children and young people it is 257 days. The ASDAT team
received 1237 referrals (approximately 65 per month) for the period
January 2017 to July 2018.
1st April - 31st March referrals
80
95 4
0
87 7
3 20
40
43 2
6 6 8 0
2018 current year
No of under 25s referred
Total number of SPS referrals

JSNA Special Education Needs and Disabilities 68
18/12/18 V 0.9 Final
Service provision - Local authority
Cornwall’s Local Offer and the Isles of Scilly’s Local Offer are the key
sources of up-to- date information about provision available to meet
SEND in our area.69,70
There are many different services that meet the needs of children and
young people; just some of the services provided by the local authority
and health include:
Schools
Speech and language therapy
Early years settings
Health visiting
Occupational therapy
Physiotherapy
Cognition and learning advice
Teachers of the deaf and the visually impaired
Social care
Child and adolescent mental health services
Special schools
The vast majority of children with SEND receive the support they need
locally, however, occasionally, due to complexity a child or young person
accesses highly specialised services based outside Cornwall and the Isles
of Scilly.
Transport
School Transport71 is generally limited to those children attending their
designated school or nearest school with a place available and when one of
the following apply:
The school is more than two miles from the home address for pupils under
69
https://www.supportincornwall.org.uk/kb5/cornwall/directory/site.page?id=aq6QKb5BEPE 70
http://www.scilly.gov.uk/childrens-services/isles-scilly-local-offer
71
Cornwall Council School Transport http://www.cornwall.gov.uk/schooltransport

JSNA Special Education Needs and Disabilities 69
18/12/18 V 0.9 Final
the age of eight, and more than three miles for pupils over the age of
eight;
The pupil is unable to walk to school by reason of their special
educational need, disability or mobility problem;
The nature of the route is deemed by the Local Authority as being
unsuitable for pedestrian use.
Decisions are made on an individual basis for children and young people
with SEND. Some parents are happy to transport their child themselves,
and receive a mileage allowance for this – this is usually the most cost-
effective way of transporting children. However, other parents prefer to
have their child transported to school.
If possible, children will be grouped into the same transport. However, this
is often not possible, and there are lots of single-occupancy vehicles.
Some children and young people with less complex needs can be funded to
use public transport.
Some children and young people require a trained passenger assistant (PA)
to help manage their needs during the journey. PAs are usually provided
by the taxi companies that are used, although they can be provided by
schools, agencies, or the parents themselves.
An increasing number of transport providers have CCTV installed in their
vehicles. Any safeguarding issues are picked up by the Local Authority
Designated Officer (LADO).
Transport needs are not routinely reviewed, and changes often only
become apparent following an incident. Inclusion of a routine review would
be a better option, and aim for independence.
Data from the Transport Services Team shows that the cost of transport is
high. In 2017/18, there were 811 children and young people with SEND
under the age of 16, for whom transport has been provided at a cost of
approximately £5M. There were 316 young people with SEND over the age
of 16, for whom transport was provided at a cost of approximately £1.5M.
The overall budget for transport for 2017/18 was £13M, although this was
overspent by approximately £2.5M.
Equipment
There is a joint equipment store between education, health and social services. School are expected to provide certain items of equipment.

JSNA Special Education Needs and Disabilities 70
18/12/18 V 0.9 Final
Recommendations
Key issues Actions & recommendations
1. Outcome from the JSNA The Special Educational Needs and Disability Board and relevant partners work collaboratively to address the specific recommendations that
follow. 2. Data sharing Information collection and analysis within and
between services in relation to SEN needs to be
improved further.
3. Clarity and consistency about identification of SEN
A range of activity is required to improve accuracy and timeliness of identification of SEN.
4. Increasing demand. Predicted increases in SEND should be incorporated into forward planning of children’s
and adult’s services.
5. Transition to adult based services still requires further
improvement.
Transition between children and adult services requires continued focussed activity.
6. The level of health protection through
immunisations and screening needs further clarification.
Establish data to analyse the rate of immunisation uptake for those infants, children and young
people with a disability compared to the wider population and understand the reasons for any variance.
7. Wider determinants of
health in relation to SEND and access to services needs further research.
Further research is needed on lifestyle behaviours of children and young people with disabilities and how this impacts on their needs.
Further research is needed on housing and families with disabilities particularly those which require adaptations or have specific housing requirements.
8. Access and equity of services
Services are generally distributed well across Cornwall. However, these will need to be mapped to understand whether they are truly accessible and meeting local needs and informing planning for future demands.
9. Cornwall’s current education performance by children and young people with SEN is not in the top quartile nationally
Focussed activity by all partners, across the full
age range, to reduce the gaps in achievement between children and young people with and
without SEN in Cornwall, and the performance of pupils with SEN in Cornwall in comparison children and young people with SEN in other parts of the
country.

JSNA Special Education Needs and Disabilities 71
18/12/18 V 0.9 Final
Appendix 1 – Legislative and policy context
Improving the educational, health and wellbeing outcomes for children and
young people with special educational needs and disabilities has been a
focus for successive governments. This has been illustrated by a growing
body of evidence and government policies, such as:
Local area SEND inspection framework 201672
A new inspection framework for SEND (special educational needs and/or
disability) was published in April 2016. Local areas (including local
authorities, clinical commissioning groups, Public Health, the NHS, schools,
and other providers) will be inspected at least once every five years jointly
by Ofsted and the Care Quality Commission. Inspections assess how well
the local area as a whole is meeting the needs of children and young
people aged 0 to 25 with SEND.
SEND Code of Practice January 201573
The SEND Code of Practice provides statutory guidance on duties, policies
and procedures relating to Part 3 of the Children and Families Act 2014
and associated regulations across England.
72
Local area SEND inspection: framework https://www.gov.uk/government/publications/local-area-
send-inspection- framework 73 Statutory Guidance - SEND code of practice: 0 to 25 years
https://www.gov.uk/government/publications/send-code-of-practice-0-to-25
Key Messages
There is a wide range of legislation creating powers and
duties in relation to children and young people with
additional needs.
All public bodies have statutory duties to have due regard
for those with disabilities. All organisations (voluntary or
commissioned) working within this sector must be clear in
terms of the extent to which they promote disabled
children's human rights and give due regard through
services delivered.

JSNA Special Education Needs and Disabilities 72
18/12/18 V 0.9 Final
Children and Families Act 201474 Part 3: Children and young
people with special educational needs and disabilities
The Children and Families Act 2014 provided for an overhaul of the system
for identifying children and young people in England with special
educational needs (SEN), assessing their needs and making provision for
them. It places a specific duty on local authorities to identify all children in
their area who have SEN or disabilities.
The Act introduces Education Health and Care assessments and plans
which replace statutory assessments and statements of special
educational need. Many of the legal requirements for EHC assessments
and plans are the same or similar to those required for statements.
There are also some significant differences, including:
EHC plans do not necessarily cease when a young person leaves
school and can be maintained when a young person is in college,
undertaking an apprenticeship, or not in education, employment or
training;
EHC plans can be maintained up to the age of 25;
There are enforceable elements of health and social care that must be
recorded in EHC Plans.
The overarching aim is to give families and young people a greater
involvement in decisions about their support and to encourage social
care, education and health services to work together more closely.
Local authorities must pay particular attention to:
the views, wishes and feelings of children and their parents, and young people;
the importance of them participating as fully as possible in decision-
making and providing the information and support to enable them to
do so; and
supporting children and young people’s development and helping
them to achieve the best possible educational and other
outcomes.
74
http://www.legislation.gov.uk/ukpga/2014/6/contents/enacted

JSNA Special Education Needs and Disabilities 73
18/12/18 V 0.9 Final
As part of the changes local authorities are required to publish a ‘local
offer’ setting out what support is available to young people with SEN and
families with children who have disabilities or SEN. The local offer also
explains how families can request personal budgets, make complaints
and access more specialist help.
The Act also sets out requirements for all Early Years providers to have
arrangements in place to support children with SEN or disabilities75. Every
local authority must also have a SEN inclusion fund to support early
years providers in meeting the needs of individual children with SEN.
A more comprehensive summary of the legislation is available from the
Council for Disabled Children76.
Special Educational Needs and Disability Regulations 201477
These Regulations set out the detailed requirements on local authorities for
assessing children and young people’s education, health and care needs
and where necessary drawing up Education, Health and Care plans. They
set out requirements on schools for identifying and supporting children and
young people with special educational needs and also the arrangements
for resolving disagreements, including mediation and appeals to an
independent tribunal where parents or young people do not agree with
decisions made by their local authority.
They also set out the way in which local authorities and health bodies
should review support for children and young people with SEND and how
local authorities and schools must publish information concerning the
support which is available.
75Early years: guide to the 0 to 25 SEND code of practice, Advice for early years providers that are
funded by the local authority.
_Code_of_Practice_-_02Sept14.pdf 76
Children and Families Act http://www.councilfordisabledchildren.org.uk/resources/summary-of-the-children-and- families-act 77
The Special Educational Needs and Disability Regulations 2014
http://www.legislation.gov.uk/uksi/2014/1530/pdfs/uksi_20141530_en.pdf

JSNA Special Education Needs and Disabilities 74
18/12/18 V 0.9 Final
Special Educational Needs (Personal Budgets) Regulations
201478
These regulations provide a framework as to how local authorities can
assign personal budgets to young people with SEND or their families. This
applies to the use of personal budgets for children and young people with
SEND who have an EHC plan and the regulations set out the criteria and
detailed provision for the use of personal budgets, including direct
payments for special educational provision.
The Care Act 201479 The Care Act 2014 sets out carers' legal rights to assessment and support.
It came into force in April 2015. The Care Act relates mostly to adult carers
– people aged 18 and over who are caring for another adult. However, the
Act also contains new rules about working with young carers or adult
carers of disabled children to plan an effective and timely move to adult
care and support.
The Act says adult social services need to be involved in planning the
support a young carer may need once they reach 18. This also applies to
adult carers of children where it appears likely that the adult carer will
have needs for support after the child turns 18.
The Breaks for Carers of Disabled Children Regulations 201180
In order to meet the requirements of the regulations, Local Authorities
must have regard to the needs of carers in respect of their capacity to care
for, or continue to care for, their disabled child, and must provide a range
of services designed to meet this need. The following summarises the key
duties introduced under these regulations:
Duty to make provision
Local authorities must take into account the needs of carers who
would be unable to continue caring for their child unless breaks from
caring were given; or who would be able to give more effective care
78
The Special Educational Needs (Personal Budgets) Regulations 2014
http://www.legislation.gov.uk/ukdsi/2014/9780111114056 79
Care Act 2014 http://www.legislation.gov.uk/ukpga/2014/23/contents/enacted 80
http://www.legislation.gov.uk/uksi/2011/707/made

JSNA Special Education Needs and Disabilities 75
18/12/18 V 0.9 Final
if breaks were given to allow them to, for example, attend
educational classes or work, meet the needs of other children in the
family, or carry out necessary day-to-day tasks in the household.
Types of services which must be provided
Local Authorities must, so far as is reasonably practicable, provide a
range of services sufficient to meet the needs of carers to care, or
care more effectively, including:
Day care in the child’s own home or elsewhere
Overnight care in the child’s own home or elsewhere
Educational or leisure activities for children outside their own
homes
Services in the evenings, at weekends and during school holidays
Short breaks services statement Local Authorities must prepare a statement for carers in their area
setting out the range of services available;
any eligibility criteria for these services; and
how the range of services is designed to meet the needs of carers
Equality Act 201081
The Equality Act 2010 replaced various anti-discrimination laws (for
example the Disability Discrimination Act and the Race Relations
Amendment Act) with a single Act. It simplified the legislation, removing
inconsistencies and making it easier for people to understand and comply
with it. It also strengthened the law in important ways to help tackle
discrimination and inequality.
The Act introduced new public sector equality duties for organisations such
as county and district councils and the NHS. Organisations that perform
‘public functions’ are also covered by these duties to:
eliminate unlawful discrimination, harassment or victimisation
advance equality of opportunity between people who share
a protected characteristic, and those who do not
foster good relations between people who share a protected
characteristic, and those who do not.
81
http://www.legislation.gov.uk/ukpga/2010/15/contents

JSNA Special Education Needs and Disabilities 76
18/12/18 V 0.9 Final
Special Educational Needs and Disability Act 200182
The Disability Discrimination Act (DDA) 1995 legislated that it is against the
law for goods, services and facility providers to discriminate against
disabled people by treating them less favourably due to their disability. If
someone is adamant that this sort of discrimination is justified, they would
be required to show why such action should be regarded as reasonable.
The DDA 1995 did not, however, extend as far as encompassing education
providers. The Special Educational Needs and Disability Act 2001 was
created in order to tackle discrimination in this sphere and extend the DDA
1995.
Under the Special Educational Needs and Disability Act 2001, schools,
colleges, universities, adult education providers, statutory youth services
and local education authorities were required to make the same sort of
reasonable adjustments for disabled people as stipulated in the DDA 1995.
The aim of including these groups, organisations and bodies in the Act was
to ensure that disabled people were offered the same opportunities and
choices as those in mainstream society. It was also designed to make sure
that where possible, disabled people have the right to be able to work at
their fullest capacity and have the chance to fulfil their potential.
Education Act 200183
The Education Act makes provision about education, childcare,
apprenticeships and training, schools and the school workforce, institutions
within the further education sector and Academies; to abolish the General
Teaching Council for England, the Training and Development Agency for
Schools, the School Support Staff Negotiating Body, the Qualifications and
Curriculum Development Agency and the Young People’s Learning Agency
for England; to make provision about the Office of Qualifications and
Examinations Regulation and the Chief Executive of Skills Funding; to make
provision about student loans and fees; and for connected purposes. This
Act included criteria for statements of special educational need, although
statements were replaced with education, health and care (EHC) plans
from September 2014, the criteria for assessment remains unchanged.
82
http://www.legislation.gov.uk/ukpga/2001/10/contents 83
Government Legislation http://www.legislation.gov.uk/ukpga/2011/21/introduction/enacted

JSNA Special Education Needs and Disabilities 77
18/12/18 V 0.9 Final
Human Rights Act (HRA) 199884
In the UK, human rights are protected by the Human Rights Act 1998. The
Act came into full force on 2 October 2000 and gives effect to the human rights set out in the European Convention on Human Rights (ECHR).
Under the Human Rights Act, everyone is entitled to expect that the
government, and all public agencies and organisations should have respect
for their basic human rights. If they consider that their rights have been
ignored, they can bring a case in the UK courts to challenge an action or a
decision by any public authority on the grounds that it interferes with their
rights.85
NOTE: The Disability Discrimination Act is no longer in use - it is now
known as the Equality Act 2010. From 1 October 2010, the Equality Act
replaced most of the Disability Discrimination Act (DDA). However, the
Disability Equality Duty in the DDA continues to apply.
NICE (National Institute for Clinical Excellence)86
The National Institute for Clinical Excellence provides national guidance and
advice to improve outcomes for people using the NHS and other public
health and social care services. As part of its suite of products, NICE
produces guidelines. These are evidence-based recommendations for health
and care in England and set out the care and services suitable for most
people with a specific condition or need, and people in particular
circumstances or settings.
In the last few years NICE have released the following guidance
documents relevant to children and young people with disability and
special educational needs:
NG62 Cerebral palsy in under 25s: assessment and management, Jan 2017
QS140 Transition from children’s to adults’ services, Dec 16 NG61 End of life care for infants, children and young people with life-
limiting conditions: planning and management, Dec 16 QS128 Early years: promoting health and wellbeing in under 5s, Aug 2016 NG43 Transition from children’s to adults’ services for young people
using health or social care services, Feb16
84Human Rights Act 1998 http://www.legislation.gov.uk/ukpga/1998/42/schedule/1
85"A Guide to the Human Rights Act 1998: Questions and Answers" (PDF). JUSTICE. December
2000. https://web.archive.org/web/20020312081934/86
National Institute for Clinical Excellence https://www.nice.org.uk/

JSNA Special Education Needs and Disabilities 78
18/12/18 V 0.9 Final
QS102 Bipolar disorder, psychosis and schizophrenia in children and young people, Oct 15
NG1 Gastro-oesophageal reflux disease in children and young people: diagnosis and management, Jan 15
QS51 Autism, Jan 14
QS48 Depression in children and young people, Sept 13
CG170 Management of autism in children and young people, Aug 13
QS39 Attention deficit hyperactivity disorder, July 13
GDG Challenging behaviour and learning disabilities, May 13
CG158 Conduct disorder in children and young people, Mar 13
QS27 The epilepsies in children and young people, Feb 13
CG155 Psychosis and schizophrenia in children and young people, Jan 13
(Updated Oct 15)
PH20&40 Social and emotional wellbeing in early years (PH40) and in
secondary education, Oct 12
CG145 Spasticity in children and young people, Jul 12 (Updated Nov16)
CG128 Autism in children and young people, Sept 11 (NICE 2013)
Throughout all of these there is strong focus on: access to services;
accurate diagnosis and its clear documentation and communication; annual
specialist reviews; comprehensive treatment options (including non-
pharmacological and non-surgical); a ‘life-course’ perspective to
management; child-focused planning with involvement of parents and
carers; addressing the social, physical and psychosocial environments; and
transition to adult services and adult life.
Safeguarding in schools
The Department for Education’s report Keeping Children Safe in Education
July 2015 is statutory guidance issued the Education Act 2002, the
Education (Independent School Standards) Regulations 2014 and the
Education (Non-Maintained Special Schools) (England) Regulations 2011.
This guidance contains information on what schools and colleges should do
and sets out the legal duties with which schools and colleges must comply
and should be read alongside statutory guidance Working Together to
Safeguard Children 2015 and departmental advice What to do if you are
worried a child is being abused 2015. The designated safeguarding lead
should be alert to the specific needs of children, those in need, those with
special educational needs and young carers.

JSNA Special Education Needs and Disabilities 79
18/12/18 V 0.9 Final
Appendix 2 – Risk factors associated with childhood disability
There can be many reasons for disability or developmental delay. These
can begin anytime during the developmental period and whilst many begin
before a baby is born, some can happen after birth because of injury,
infection, or other factors.
Factors known to influence disability or developmental delay amongst
children include genetics; parental health and behaviours (such as
smoking and drinking) during pregnancy; complications during birth;
infections the mother might have during pregnancy or the baby might have
very early in life; and exposure of the mother or child to high levels of
environmental toxins, such as lead.
For some developmental disabilities, such as foetal alcohol syndrome,
which is caused by drinking alcohol during pregnancy, we know the cause.
But for most, we don’t87.
The following provide examples of known specific risks:
Before birth
Before birth the health of a baby is significantly influenced by the health
and well- being of their mother88. Prenatal risk factors include:
Preconception factors – relate predominantly to genetic conditions or
syndromes such as Down’s syndrome and fragile X syndrome – around
one in every 1,000 babies born in the UK will have Down’s syndrome89.
Older and younger parents are more at risk of complications that can
result in their child experiencing a disability. Those under 20 are more
at risk of poor nutrition and poor placental transfer of food and oxygen,
whereas those who have children later are more likely to suffer from
chromosomal abnormalities90.
Maternal physical injury – injury or impact to the mother’s abdomen
87
Developmental Disabilities, National Center on Birth Defects and Developmental Disabilities, Centers
for Disease Control and Prevention [Accessed January 2017]
https://www.cdc.gov/ncbddd/developmentaldisabilities/facts.html 88
M. Marmot, 'Fair Society, Healthy Lives. The Marmot Review', Strategic review of health inequalities in England post - 2010 (2010).
89 http://www.cdc.gov/ncbddd/birthdefects/downsyndrome.html
90 Blomberg M, Tyrberg RB and Kjølhede P. Impact of maternal age on obstetric and neonatal
outcome with emphasis on primiparous adolescents and older women: a Swedish Medical Birth Register Study. BMJ Open 2014; 4:e005840

JSNA Special Education Needs and Disabilities 80
18/12/18 V 0.9 Final
during pregnancy can result in disabilities when the child is born.
Infections – a number of viral and sexual infectious diseases suffered by
mothers during pregnancy can cross the placental barrier and cause
disabilities including: toxoplasmosis, herpes, gonorrhoea, chlamydia,
invasive Group B strep, listeria infection or bacterial infections.
Exposure to toxins – foetuses being exposed to drugs and/or
alcohol,91,92radiation, certain prescription drugs, and environmental
pollutants can cause birth defects.
Maternal chronic illness – conditions such as asthma, diabetes,
epilepsy, cancer, hypertensive disorders (e.g. pre-eclampsia and
eclampsia), phenylketonuria, sickle cell anaemia, systemic lupus
erythematosus, thalassaemia, and thyroid problems can all result in
complications in pregnancy and pose a threat to the unborn baby.
Maternal nutritional deficiencies – deficiencies in key vitamins and
minerals can lead to disabilities, for example hydrocephalus and
spina-bifida.
Incompatible blood type – when a mother’s blood type is different to the
baby’s, there is risk that the mother’s body forms antibodies that can
attack the baby’s blood causing disabilities, such as cerebral palsy and
deafness.
At the time of birth
The process of labour and delivery can also present complications. The
following sets out the potential risks of difficulty in delivery:
Premature birth and/or low birth weight babies – babies who are
born early and/or have a low birth weight have an increased
risk of health and developmental problems.93,94,95,96 Premature
91
NICE. Antenatal care CG62. London: National Institute for Health and clinical Excellence 2008.
Available from: https://www.nice.org.uk/guidance/cg62 92
NICE. Pregnancy and complex social factors: A model for service provision for pregnant women with complex social factors CG110. London: National Institute for Health and clinical Excellence 2010. Available from: https://www.nice.org.uk/guidance/cg110 93
deRegnier RA. Neurophysiologic evaluation of brain function in extremely premature newborn infants. Seminars in Perinatology. 2008; 32:2–10. 94
Zwicker JG, Harris SR. Quality of life of formerly preterm and very low birth weight infants from preschool age to adulthood: A systematic review. Pediatrics. 2008; 121: e366–e376. 95
MacDonald H. Perinatal Care at the Threshold of Viability. Pediatrics. 2002; 110: 5. 96
Hack M, Klein NK, Taylor HG. Long-term developmental outcomes of low birth weight infants. Future
of Children. 1995; 5:176 –96

JSNA Special Education Needs and Disabilities 81
18/12/18 V 0.9 Final
birth and low birth weight can be caused by maternal lifestyle
choices, for example smoking97 or poor nutrition. However, for
the majority of women who have preterm births, the causes are
unclear98.
Birth trauma – such as breech presentation, operative vaginal
delivery or small maternal size and maternal pelvic anomalies
that may contribute towards temporary stoppage of oxygen
supply to the brain of the baby or damages nervous tissues.
Multiple births – have a higher rate of obstetrical complications
during the pregnancy and at time of delivery, resulting in
higher risks of serious health problems99.
Post birth
In the days and weeks following birth, there are common conditions that, if
left untreated, can lead to an infant developing a disability or SEN:
Untreated new-born jaundice (high levels of bilirubin in the
blood during the first few days after birth) – can cause a type
of brain damage known as kernicterus. This can result in
involuntary and uncontrolled movements (athetoid cerebral
palsy), hearing loss and improper development of tooth
enamel.
Hypoglycaemia (low blood glucose) – which if severe or prolonged
may result in a risk of seizures and serious brain injury.
Over the longer term risks linked to disability and SEN are much the same
as the wider population including:
Accident or injury – including falls, poisoning, suffocation
and road traffic accidents. Evidence suggests these to be
closely linked with social deprivation100.
97Larsen, L.G. et al. Stereologic examination of placentas from mothers who smoke during pregnancy.
Am J Obstet & Gynecol. 2002; 186: 531-53798
Bull, J et al (2003) Prevention of low birth weight: assessing the effectiveness of smoking cessation and nutritional interventions. Evidence Briefing July 2003 Health Development Agency
99Improving outcomes for fertility patients: multiple births 2015, Human Fertilisation and Embryology
Authority, 100
WHO. World report on child injury prevention. WHO. 2008. Available at http://apps.who.int/iris/bitstream/10665/43851/1/9789241563574_eng.pdf – accessed May 2017

JSNA Special Education Needs and Disabilities 82
18/12/18 V 0.9 Final
Infectious diseases – lack of immunisation increases the risks
associated with infectious diseases such as mumps,
meningitis or measles all of which can cause disability101.
Malnutrition – nutrition and disability are intimately linked:
malnutrition can directly cause or contribute to disability and
disability to malnutrition. Malnutrition as a result of a poor
diet is rare in the UK, however, nutritional deficiencies can
result in a variety of physical and mental disabilities including
growth deficiencies, bone malformation and blindness102.
National estimates vary from 10% (Emerson, E. and Hatton, C. 2005); 7%
(Office National Statistics 2004103); 3% OPCS (1989) and 1.2% (estimate
of young people with severe disabilities, DCSF 2007).
The Office of National Statistics report suggested a 62% increase in the
number of disabled children between 1975 and 2002, in part due to
medical advances and increased diagnosis and reporting; this is an
ongoing trend. The vast majority of families (98%) care for their children
at home. Those children and their families have needs that are various and
wide-ranging.
101
WHO. 2011. World Report on Disability. Ibid. 102
Groce.N, et. al., Stronger Together: Nutrition-Disability Links and Synergies (Briefing Note), UNICEF,
https://www.unicef.org/disabilities/files/Stronger-Together_Nutrition_Disability_Groce_Challenger_Kerac.pdf - accessed May2017 103
The Health of Children and young people, Chapter 10,: Disability, March 2004, ONS

JSNA Special Education Needs and Disabilities 83
18/12/18 V 0.9 Final
Appendix 3 – population projections
Population projections for the 0-25 age group The following maps introduce the scale of forecasted population change
across Cornwall. It utilises population projections commissioned by
Cornwall Council from Edge Analytics (POPGROUP) which incorporate the
Council’s housing growth targets set out within the Local Plan.

JSNA Special Education Needs and Disabilities 84
18/12/18 V 0.9 Final

JSNA Special Education Needs and Disabilities 85
18/12/18 V 0.9 Final
The population projections show that there is expected to be an increase in
the population of children and young people in the Falmouth area as a
result of the presence of the university. There is also expected to be an
increase in the Roseland.
There are few special schools in Cornwall and the Isles of Scilly, so children
and young people tend to travel large distances to access the school that is
most suitable for their needs. Therefore, local population changes are
unlikely to impact on the numbers of children and young people attending
special schools.

JSNA Special Education Needs and Disabilities 86
18/12/18 V 0.9 Final
2015 2020 2025
Cornwall [M]
Cornwall [F]
Cornwall [M]
Cornwall [F]
Cornwall [M]
Cornwall [F]
0-4 15,022 14,257 0-4 15,109 14,298 0-4 15,637 14,797 5-9 15,048 14,279 5-9 16,367 15,414 5-9 16,414 15,429
10-14 14,432 13,575 10-14 16,147 15,289 10-14 17,427 16,383 15-19 16,180 15,354 15-19 15,105 14,147 15-19 16,890 15,892 20-24 15,599 14,897 20-24 15,750 14,867 20-24 14,779 13,903 25-29 13,810 13,307 25-29 15,267 14,442 25-29 15,190 14,119 30-34 13,417 14,178 30-34 14,173 14,498 30-34 15,412 15,344 35-39 13,596 14,410 35-39 14,246 15,530 35-39 14,987 15,862 40-44 15,819 17,582 40-44 14,427 15,528 40-44 15,159 16,705 45-49 18,377 20,313 45-49 16,460 18,489 45-49 15,053 16,439 50-54 19,280 20,354 50-54 19,102 21,253 50-54 17,169 19,382 55-59 18,087 19,687 55-59 20,071 21,480 55-59 19,946 22,348 60-64 17,682 19,213 60-64 18,841 20,470 60-64 21,017 22,505 65-69 20,776 21,881 65-69 17,861 19,337 65-69 19,182 20,690 70-74 15,318 16,526 70-74 19,501 20,849 70-74 16,981 18,546 75-79 10,926 12,301 75-79 13,491 14,967 75-79 17,348 18,997 80-84 7,590 9,502 80-84 8,685 10,527 80-84 10,993 12,993
85+ 5,982 10,991 85+ 7,404 11,703 85+ 9,280 13,420
266,941 282,607 278,007 293,088 288,864 303,754

JSNA Special Education Needs and Disabilities 87
18/12/18 V 0.9 Final
Appendix 4 – further details about Disability Living Allowance
The main categories for claimants for Disability Living Allowance (DLA) are
shown in the following charts.
Disability Living Allowance in 0-24 years for conditions that have risen since 2011
Disability Living Allowance 0-24 years 2,500
2,000
1,500
Emotional and Behavioural disorder
Hyperkinetic syndrome
Learning Difficulties
Mental Health
Nervous system
1,000
500
0
Disability Living Allowance 0-24 years - rising
2,000 EmotionalandBehaviouraldisorder
Hyperkinetci syndrome
Unknown
1,500 LearningDi iculties
1,000
500
0

JSNA Special Education Needs and Disabilities 88
18/12/18 V 0.9 Final
The following table shows the comparison between DLA claimants in
2012 and 2017. The greatest change was in emotional and behavioural
disorder.
DLA benefit claimants 0-24 Comparison104
Category Feb 2012 Feb 2017 Difference
+/-
Alcohol and drug abuse 0 0 0
Chronic fatigue 40 20 -20
Circulatory 70 40 -30
Diabetes 200 160 -40
Disease 240 160 -80
Emotional and behavioural disorder 210 590 380
Frailty 0 0 0
Hyperkinetic syndrome 480 380 -10
Learning difficulties 2110
2,00
0
-
110 Mental health 340 130 -210 Multi system disorders 0 0 0
Multiple allergy syndromes 10 0 -10
Musculoskeletal 230 180 -50
Nervous system 610 410 -
200 Respiratory 50 20 -30
Sensory loss 220 170 -50
Terminal illness 10 0 -10
Trauma 40 20 -20
Unknown 110 270 160
Urinary system 30 20 -10
TOTAL* 5,00
0
4,99
0
-10
*Figures are rounded
104
Disability living allowance by disabling condition, DWP, [NOMIS 2016]

JSNA Special Education Needs and Disabilities 89
18/12/18 V 0.9 Final
Appendix 5 – trends in numbers of children and young people who have SEND
Pupils with or without statements of special educational needs (SEN) or education,
health and care (EHC) plans (January each year) 2007-17105
Total pupils
Pupils with statements Pupils without statements
ENG SW C’wall ENG % SW % C’wall % ENG % SW % C’wall %
2007 8,167,715 771,615 74,983 232,760 2.8 20,820 2.7 2,060 2.7
2008 8,121,955 767,260 74,250 227,315 2.8 20,620 2.7 2,063 2.8
2009 8,092,280 762,685 73,178 225,400 2.8 20,565 2.7 2,032 2.8 1,447,205 17.9 130,345 17.1 12,027 16.4
2010 8,098,360 759,470 72,648 223,945 2.8 20,580 2.7 2,130 2.9 1,481,035 18.3 132,535 17.5 12,585 17.3
2011 8,123,865 759,690 72,374 224,210 2.8 20,470 2.7 2,023 2.8 1,449,685 17.8 131,975 17.4 13,007 18.0
2012 8,178,200 761,960 72,399 226,125 2.8 20,710 2.7 2,054 2.8 1,392,215 17.0 128,825 16.9 12,179 16.8
2013 8,249,810 764,655 72,550 229,390 2.8 20,885 2.7 2,051 2.8 1,316,220 16.0 122,085 16.0 11,688 16.1
2014 8,331,385 768,995 72,708 232,190 2.8 21,285 2.8 2,035 2.8 1,260,760 15.1 120,285 15.6 11,010 15.1
2015 8,438,145 775,755 72,927 236,165 2.8 21,580 2.8 1,948 2.7 1,065,280 12.6 104,110 13.4 9,110 12.5
Pupils with or without statements of special educational needs106
As can be seen from the table below Cornwall has been in line with national
and regional numbers during the 2011 to 2017 period. Both specific and
moderate learning difficulties showed a decrease in the number of pupils
up to 2014 and there has been a substantial increase since. In both the
severe learning, and profound and multiple learning difficulty categories
there has been a steady increase during this time period. In 2017, there
were 266 pupils on the Isles of Scilly. Of these, 32 (12.0%) had SEN but
no EHC plan, and a further nine (3.4%) had EHC plans.
However, the small numbers on the Isles of Scilly make it difficult to draw
conclusions.
Number of pupils with learning difficulties107
105
Special educational needs in Cornwall January 2017 Government Statistics https://www.gov.uk/government/collections/statistics-special-educational-needs-sen 106
Special educational needs in Cornwall January 2017 Government statistics

JSNA Special Education Needs and Disabilities 90
18/12/18 V 0.9 Final
2017 2016 2015 2014 2013 2012 2011
Specific Learning Difficulty
ENGLAND 147,873 151,153 135,505 67,555 70,655 74,575 78,135
SOUTH WEST 17,562 17,919 16,060 6,490 6,825 7,060 7,340
Cornwall 1,188 1,314 1,370 55
5
588 683 70
8 Isles of Scilly 1
1
1
3
12 X X 3 X
Moderate Learning Difficulty
ENGLAND 259,713 273,627 241,125 129,830 138,350 149,520 160,750
SOUTH WEST 19,820 21,398 17,385 7,865 8,210 8,980 9,525
Cornwall 2,071 2,183 1,867 860
958 1,065 1,142
Isles of Scilly 6 5 7 4 3 5 9
Severe Learning Difficulty
ENGLAND 32,338 32,304 32,090 31,040 30,440 29,935 29,270
SOUTH WEST 3,027 3,088 3,035 2,920 2,855 2,800 2,700
Cornwall 324
344
334 327
308 282 277 Isles of Scilly 0 0 0 0 0 0 0
Profound & Multiple Learning Difficulty
ENGLAND 10,981 10,914 10,910 10,590 10,525 10,255 9,895
SOUTH WEST 932
952
970 940
955 940 895 Cornwall 8
8 80
68 70
61 64 62 Isles of Scilly 0 X X X X 0 0
X – Numbers redacted
In the table below it shows there were decreases in the number of pupils
with social, emotional and behavioural difficulty between 2010 and 2014.
Cornwall is very much in line with the national and regional trend, with a
decrease from 1,492 in 2011 to 1,213 in 2014 and then an increase up to
1,771 in 2017. The numbers for the Isles of Scilly are too small to give
meaningful information about trends.
Number of pupils with social, emotional and mental health difficulties106
2017 2016 2015 2014 2013 2012 2011
ENGLAND 186,793 184,930 169,110 138,655 143,050 151,150 158,015
SOUTH WEST 20,940 20,221 17,370 13,090 13,085 13,485 13,785
Cornwall 1,857 1,771 1,535 1,213 1,363 1,400 1,492
Isles of Scilly 3 5 5 X X X 4
The table below shows the steady increase from 2011 to 2017 in the
107
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 91
18/12/18 V 0.9 Final
number of pupils with speech, language and communication needs.
Cornwall is in line with the national and regional figures having
increased from 1,191 to 1,902. Whilst the numbers of pupils on the
Isles of Scilly with speech, language and communication needs are too
small to draw firm conclusions, there is a suggestion that the numbers
may be increasing, with 11 pupils having been identified in 2017.
Number of pupils with speech, language and communication
needs108
2017 2016 2015 2014 2013 2012 2011
ENGLAND 234,076 221,456 190,475 138,905 132,205 125,635 120,610
SOUTH WEST 22,102 20,921 17,655 12,610 12,135 11,760 11,605
Cornwall 1,902 1,850 1,653 1,231 1,270 1,286 1,191
Isles of Scilly 11 5 5 4 4 X 0
X – Numbers redacted
The table below shows the increase from 2010 to 2017 in Cornwall from 106 to 158; this is in line with national and regional numbers. Since 2012,
there have been no pupils on the Isles of Scilly who have a hearing
impairment.
Number of pupils with hearing impairment107
2017 2016 2015 2014 2013 2012 2011
ENGLAND 21,167 20,499 19,350 16,470 16,270 16,135 15,980
SOUTH WEST 1,989 1,967 1,855 1,455 1,410 1,390 1,330
Cornwall 158 150 157 132 130 120 109
Isles of Scilly 0 0 0 0 0 0 X
X – Numbers redacted
The table below shows that within Cornwall and the South West the
numbers of pupils with visual impairment was steadily declining from 2010
but has increased over the last two years. The national figures, however,
show a steady increase. There have been no pupils on the Isles of Scilly
since 2011 with visual impairment.
Number of pupils with visual impairment107
108
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 92
18/12/18 V 0.9 Final
2017 2016 2015 2014 2013 2012 2011
ENGLAND 11,889 11,592 10,840 9,115 9,070 8,900 8,775
SOUTH WEST 990 959 875 730 700 755 770
Cornwall 86 86 84 61 67 68 70
Isles of Scilly 0 0 0 0 0 0 0
The number of pupils with multi-sensory impairments has increased substantially over the six year period shown in the table below. Cornwall
has been in line with the national and regional increases.
Number of pupils with multi-sensory impairment109108
2017 2016 2015 2014 2013 2012 2011
ENGLAND 2,719 2,302 1,845 1,115 1,025 965 935
SOUTH WEST 326 309 275 125 110 90 80
Cornwall 47 42 37 16 17 17 3
Isles of Scilly 0 0 0 0 0 0 0
The table below shows how the number of pupils with a physical disability
has increased steadily from 2010 to 2016 with England and the South
West. This has not been the pattern within Cornwall where it decreased in
2013 to 258 and is increasing slightly to 283 in 2016.
Number of pupils with a physical disability108
2017 2016 2015 2014 2013 2012 2011
ENGLAND 33,686 32,897 30,790 26,760 26,685 26,620 26,970
SOUTH WEST 3,263 3,202 2,945 2,560 2,525 2,545 2,595
Cornwall 292 283 277 265 258 282 297
Isles of Scilly 2 2 X X 0 0 0
X – Numbers have been redacted
The table below shows there have been substantial increases in the number
of pupils with Autistic Spectrum Disorder in the 2010 to 2017 timescale. In
line with the national and regional trend, Cornwall has increased from 549
to 792.
Number of pupils with autistic spectrum disorder108
109
Special educational needs in Cornwall January 2017 Government Statistics
https://www.gov.uk/government/collections/statistics-special-educational-needs-sen

JSNA Special Education Needs and Disabilities 93
18/12/18 V 0.9 Final
2017 2016 2015 2014 2013 2012 2011
ENGLAND 108,403 100,012 90,775 76,015 70,780 66,200 61,575
SOUTH WEST 8,831 8,272 7,665 6,400 5,985 5,610 5,240
Cornwall 792 779 751 703 636 583 557
Isles of Scilly 4 4 4 5 3 3 X
X – Numbers have been redacted
The table below shows the number of pupils with other difficulties or disability. The number of pupils has increased from 2011 to 2017;
however, this has not been a steady increase.
Number of pupils with other difficulty/disability108
2017 2016 2015 2014 2013 2012 2011
ENGLAND 54,342 55,196 50,210 29,040 29,020 29,485 30,475
SOUTH WEST 5,824 5,932 4,965 2,605 2,580 2,700 2,685
Cornwall 440 443 397 231 256 287 312
Isles of Scilly 4 4 4 4 3 0 X

JSNA Special Education Needs and Disabilities 94
18/12/18 V 0.9 Final
Appendix 6 – absenteeism and exclusions
Absence rates and pupils defined as persistent absentees by special educational needs 2013/14110
England South
West Cornwall IoS
No
Identified SEN
Number of pupil enrolments 5,221,040
492,130
50,363
199
Sessions missed due to overall absence (%)
4.1 4.2 4.3 4.6
Percentage defined as persistent absentees (%)
2.6 2.6 2.6 2.5
SEN
without a statement
Number of pupil enrolments 1,100,02
5
103,90
5
10,23
3
22
Sessions missed due to
overall absence (%) 6.1 6.0 6.0 6.1
Percentage defined as persistent absentees (%)
7.0 6.7 6.4 0
School
Action
Number of pupil enrolments 683,11
5
68,89
0
6,70
0
12
Sessions missed due to overall absence (%)
5.7 5.7 5.8 6.0
Percentage defined as persistent absentees (%)
5.9 5.8 5.6 0
School Action Plus
Number of pupil enrolments 416,90
5
35,01
5
3,53
3
10
Sessions missed due to
overall absence (%) 6.7 6.7 6.5 6.4
Percentage defined as
persistent absentees (%) 8.8 8.5 7.8 0
SEN with
a statement
Number of pupil enrolments 188,66
5
17,70
5
1,83
0
5
Sessions missed due to overall absence (%)
7.5 7.4 6.6 3.8
Percentage defined as persistent absentees (%)
11.0 10.7 9.1 0
All pupils
Number of pupil enrolments 6,554,005
617,345
62,715
225
Sessions missed due to overall absence (%)
4.5 4.6 4.7 4.8
Percentage defined as
persistent absentees (%) 3.6 3.5 3.4 2.2
School Census 2014
The number of excluded pupils by SEN stage is expressed as a percentage
of the total number of all pupils of the same SEN stage at the time of the
January 2014 School Census. For fixed period exclusions, pupils' SEN
status at the time of their most recent fixed period or permanent
exclusion, the number is expressed as a percentage of the number
(headcount) of all pupils of the same SEN stage. Permanent exclusions,
SEN is recorded at the time of exclusion.
The percentage of fixed period exclusions and pupils receiving at least one
fixed-term exclusion, as a percentage of the school population is
110
Department for Education https://www.gov.uk/government/publications/sen-absences-and-
exclusions-additional- analysis

JSNA Special Education Needs and Disabilities 95
18/12/18 V 0.9 Final
considerably lower in Cornwall in comparison with both the South West
and England. However, the percentage receiving a permanent exclusion is
slightly higher than both the regional and national average.
Permanent and fixed-term exclusions by special educational needs 2013/14111
England South West
Cornwall IoS
No
identified SEN
Number of pupil enrolments 6,298,520 578,840 57,480 235
Number of fixed period exclusions as a percentage of school population (%)
1.73 1.63 1.09 X
Percentage receiving at least one fixed term exclusion (%)
1.08 1.00 0.71 X
Percentage receiving a permanent exclusion (%)
0.03 0.03 0.03 0
SEN without a statement
(6)
Number of pupil enrolments 1,181,310 110,850 10,691 33
Number of fixed period exclusions as a percentage of school population (%)
10.79 10.52 6.61 0
Percentage receiving at least one fixed term exclusion (%)
5.17 5.07 3.88 0
Percentage receiving a permanent exclusion (%)
0.25 0.27 0.33 0
School Action
Number of pupil enrolments 724,690 73,190 7,023 18
Number of fixed period exclusions as a percentage of school population (%)
7.17 6.97 4.19 0
Percentage receiving at least one fixed term exclusion (%)
3.78 3.74 2.69 0
Percentage receiving a permanent exclusion (%)
0.13 0.15 0.17 0
School Action Plus
Number of pupil enrolments 456,620 37,670 3,668 15
Number of fixed period exclusions as a percentage of school population (%)
16.53 17.43 11.26 0
Percentage receiving at least one fixed term exclusion (%)
7.38 7.67 6.16 0
Percentage receiving a permanent exclusion (%)
0.43 0.50 0.63 0
SEN with a statement
Number of pupil enrolments 218,480 20,130 1,998 6
Number of fixed period exclusions as a percentage of school population (%)
15.19 19.12 11.41 0
Percentage receiving at least one fixed term exclusion (%)
6.42 7.74 5.66 0
Percentage receiving a permanent exclusion (%)
0.15 0.19 0.35 0
All pupils
Number of pupil enrolments 7,698,310 709,830 70,170 270
Number of fixed period exclusions as a percentage of school population (%)
3.50 3.51 2.23 X
Percentage receiving at least one fixed term exclusion (%)
1.86 1.83 1.33 X
Percentage receiving a permanent exclusion (%)
0.06 0.07 0.09 0
School Census 2014 Further information is available in the "Guide to absence statistics". X = redacted
111
Department for Education https://www.gov.uk/government/publications/sen-absences-and-
exclusions-additional- analysis

JSNA Special Education Needs and Disabilities 96
18/12/18 V 0.9 Final
Appendix 7 – prevalence of SEND in areas of higher deprivation
Children with SEN in primary schools in Cornwall
2015 IMD Decile
No SEN School Support (K)
% School Suppor
t
SEN stateme
nt or EHC plan
% with stateme
nt or EHCP
All SEN
% of
all SEN
Total NOR
Mo
st
Dep
riv
ed
of
LS
OA
s i
n
En
gla
nd
0 - 10% (rank 1 - 3284)
2,319 459 10 53 8 512 9 2,831
10 - 20% (rank 3285 - 6568)
3,408 554 12 67 11 621 11 4,029
20 - 30% (rank 6569 - 9853)
5,788 818 17 110 17 928 17 6,716
30 - 40% (rank 9854 - 13137)
10,046 1,245 26 162 26 1,410 26 11,456
40 - 50% (rank 13138 - 16422)
6,929 837 17 110 17 947 17 7,876
Least
Dep
riv
ed
of
LS
OA
s i
n
En
gla
nd
40 - 50% (rank 16423 - 19706)
4,002 407 8 51 8 458 8 4,460
30 - 40% (rank 19707 - 22990)
2,722 242 5 49 5 291 5 3,013
20 - 30% (rank 22991 - 26275)
1,861 202 4 30 4 232 4 2,093
10 - 20% (rank 26276 - 29559)
X X 0 X 0 X 0 278
0 - 10% (rank 29560 - 32844)
X X 0 X 0 X 0 5
Grand Total
37332
4,790
100
635
100
5,426
100
42757
DfE Schools Census Spring 2017 Pupils Single or Main dual Registered. Includes
ARB/CDC Pupils Data supplied by Education, Health and Social Care, Cornwall Council X – numbers redacted to avoid disclosure, including by subtraction
Children with SEN in secondary schools in Cornwall
2015 IMD Decile
No SEN School
Support (K)
% School
Support
SEN statemen t or EHC
plan
% with statemen t or EHCP
All SEN
% of all SEN
Total NOR
Most
Deprived o
f
LSO
As in E
ngla
nd
0 - 10% (rank 1 - 3284)
1,432 271 9 55 8 326 9 1,758
10 - 20% (rank 3285 - 6568)
2,050 352 12 79 11 431 12 2,481
20 - 30% (rank 6569 - 9853)
3,847 541 18 107 15 648 17 4,495
30 - 40% (rank 9854 - 13137)
6,799 719 24 177 25 896 24 7,695
40 - 50% (rank 13138 - 16422)
5,137 537 18 129 18 666 18 5,803
Least
Deprived o
f
LSO
As in E
ngla
nd
40 - 50% (rank 16423 - 19706)
2,751 253 8 69 10 322 9 3,073
30 - 40% (rank 19707 - 22990)
1,841 212 7 52 9 264 7 2,105
20 - 30% (rank 22991 - 26275)
1,204 121 4 27 4 148 4 1,352
10 - 20% (rank 26276 - 29559)
X X 0 3 0 X 0 184
0 - 10% (rank 29560 - 32844)
X X 0 0 0 X 0 X
Grand Total 25231 3,013 100 698 100 3,719 100 28949

JSNA Special Education Needs and Disabilities 97
18/12/18 V 0.9 Final
Appendix 8 – SEND and ethnicity
Data is from the 2011 Census.
0-18 year old ethnicity
Ethnic group/age
Age
0 - 2
Age
3 - 4
Age
5-7
Age
8-9
Age
10-11
Age
12-14
Age
15-16
Age
17-18 Total
All Ethnic Groups
16,385
10,961
15,698
10,342
11,325
18,559
12,071
8,468 103,809
White: Total
16,037
10,724
15,400
10,179
11,141
18,245
11,869
8,337 101,932
White: English/ Welsh/ Scottish/ Northern Irish/ British
15,438
10,369
14,921
9,890
10,834
17,781
11,572
8,127
98,932
White: Irish
61
45
70
38
50
56
48
38 406
White: Other White
538
310
409
251
257
408
249
172 2,594
Mixed/multiple ethnic group
119
70
100
60
77
118
71
47
662
Asian/Asian British
118
105
109
63
70
113
97
57 732
Black/African/ Caribbean/Black British
63
40
43
28
23
52
14
20
283
Other ethnic group
48
22
46
12
14
31
20
7 200

JSNA Special Education Needs and Disabilities 98
18/12/18 V 0.9 Final
Pupils by ethnic group
2011 2012 2013 2014 2015 2016 2017
White 60,905 60,590 60,695 60,583 60,347 60,526 61,444
White British 59,366 59,023 59,090 58,843 58,524 58,582 59,397
Irish 102 111 110 103 116 112 120
Traveller Of Irish Heritage 12 11 4 15 13 13 9
Gypsy/ Roma 124 119 113 123 115 113 128
Any Other White Background 1,293 1,322 1,375 1,498 1,579 1,706 1,790
Mixed 925 1,025 1,100 1,206 1,285 1,362 1,408
White And Black Caribbean 217 234 237 249 264 276 290
White And Black African 85 108 127 135 143 167 170
White And Asian 297 314 335 378 421 450 459
Any Other Mixed Background 324 368 398 444 457 469 489
Asian 165 350 300 262 232 228 217
Indian 30 38 36 38 40 40 44
Pakistani 11 13 13 12 7 7 14
Bangladeshi 42 48 52 54 49 45 45
Any Other Asian Background 84 252 200 161 136 136 114
Black 55 55 60 65 62 62 53
Caribbean 7 8 8 5 10 7 10
African 20 23 27 35 31 34 30
Any Other Black Background 26 27 23 24 21 21 13
Chinese 70 80 95 91 90 89 100
Any Other Ethnic Group 125 135 140 145 157 165 212
Classified 62,245 62,240 62,385 62,362 62,173 62,432 63,434
Unclassified 773 711 758 660 659 730 756
All pupils 63,019 62,955 63,150 63,018 62,832 63,162 64,190
Pupils by ethnic group extracted from School Census
*number sufficiently small to warrant redaction
Of the 219 pupils on the Isles of Scilly in 2017, 214 had their ethnic group
classified. The majority of pupils identified themselves as white (207, 94.5%). For the remaining pupils, numbers were too small to be identified
separately.

JSNA Special Education Needs and Disabilities 99
18/12/18 V 0.9 Final
Note: 0-15 is the only age category available *number sufficiently small to warrant redaction
Ethnic Group
Day-to-day activities - %
Cornwall South West England and Wales
Limited
a lot (%)
Limited
a little (%)
Not
limited (%)
Limited
a lot (%)
Limited
a little (%)
Not
limited (%)
Limited
a lot (%)
Limited
a little (%)
Not
limited (%)
All categories 1.57 2.49 95.94 1.45 2.27 96.28 1.56 2.22 96.23
White 1.59 2.51 95.90 1.45 2.29 96.25 1.56 2.29 96.15
Mixed/multiple ethnic
group 0.95 2.26 96.80 1.39 2.33 96.28 1.62 2.32 96.06
Asian/Asian British 0.70 0.87 98.43 1.20 1.48 97.32 1.48 1.75 96.76
Black/African/Caribbean
/Black British 3.85 0.96 95.19 1.72 1.97 96.31 1.58 1.94 96.48
Other ethnic group 0.61 2.44 96.95 1.31 1.53 97.17 1.58 1.86 96.56
4.1% of children in the 0-15 year old age group in Cornwall have limited
day-to-day activities, 1.57% of whom are limited a lot – 1.56% of these
are white. In the mixed/multiple ethnic group 0.95% and 0.7% of Asians
are limited a lot. Although there are only 104 in the
Black/African/Caribbean/Black British group, the percentage (3.9%) is
higher than in other ethnic groups.
Ethnic Group
Day-to-day activities
Long-term
health problem
or disability
Limited a lot Limited a little Not limited
All categories: Ethnic group 89,941 1,415 2,239 86,287
White 87,413 1,390 2,191 83,832
Mixed/multiple ethnic group 1,685 16 38 1,631
Asian/Asian British 575 4 5 566
Black/African/Caribbean/Black British 104 4 1 99
Other ethnic group 164 1 4 159

JSNA Special Education Needs and Disabilities 100
18/12/18 V 0.9 Final
Pupils with SEN in Cornwall
No SEN
School
Support
(K)
State-
mented (S)
Education,
Health &
Care Plan
(EHCP)
With Stat (S)
or Educ,
Health &
Care Plan (E)
Total NOR
White 49631 6817 1075 536 1611 58043
White British 48014 6620 1059 518 1577 56195
Irish 95 8 X X 5 108
Traveller Of Irish Heritage X X X X X 15
Gypsy/ Roma 78 X X X X 111
Any Other White Background 1430 158 12 14 26 1614
Mixed 1154 140 18 6 24 1316
White And Black Caribbean 218 43 X X 6 267
White And Black African 145 X X X X 164
White And Asian 398 32 X X 5 433
Any Other Mixed Background 393 47 X X 12 452
Asian 200 17 3 1 4 221
Indian X X X X X 40
Pakistani X X X X X X
Bangladeshi 42 X X X X 47
Any Other Asian Background 118 X X X X 130
Black 55 2 0 1 1 58
Caribbean 6 0 0 0 0 6
African X X X X X 34
Any Other Black Background X X X X X 18
Chinese 76 X X X X 85
Any Other Ethnic Group 124 X X X X 158
Classified 51159 6989 1097 546 1643 59773
Unclassified 589 88 13 6 19 696
All pupils 51748 7077 1110 552 1662 60469

JSNA Special Education Needs and Disabilities 101
18/12/18 V 0.9 Final
SEND prevalence and language
Number and percentage of pupils by first language112
First language
known/ believed to
be
2014 2015 2016 2017
ENG SW C’wall ENG SW C’wall ENG SW C’wall ENG SW C’wall
Other than
English
No 1,123,195 35,685 1,210 1,185,960 39,303 1,307 1,249,070 43,478 1,439 1,306,829 47,052 1,545
% 16.6% 5.6% 1.9% 17.3% 6.1% 2.1% 18.0% 6.7% 2.3% 18.5% 7.1% 2.4%
English No 5,634,120 605,155 61,874 5,658,801 606,724 61,914 5,687,573 608,923 62,081 5,732,647 612,971 62,631
% 83.2% 94.3% 98.1% 82.5% 93.8% 97.9% 81.8% 93.2% 97.6% 81.3% 92.8% 97.6%
Un classified No 14,325 720 8 13,923 645 45 14,099 757 94 11,889 761 14
% 0.2% 0.1% 0.0% 0.2% 0.1% 0.1% 0.2% 0.1% 0.1% 0.2% 0.11% 0.0%
Total 6,771,630 641,560 63,090 6,858,684 646,672 63,266 6,950,742 653,158 63,614 7,051,365 660,784 64,190
There were 219 pupils on the Isles of Scilly, all of whom had English as
their first language.
English as an additional language (EAL)
Pupils Total
% of
Total
Head
count
Fem
ale
Ma
le
No
SE
N
SE
N:
SE
N S
up
port
SE
N:
Sch
oo
l A
cti
on
SE
N:
Sch
oo
l A
cti
on
Plu
s
SE
N:
Sta
tem
en
t o
r E
HC
Pla
n
Free
Sch
ool
Meals
Free
Sch
ool
Meals
ov
er
6
In t
he 3
0%
mo
st D
ep
riv
ed
Area
s
In C
are
Ad
op
ted
Fro
m C
are
Bla
ck
& M
inorit
y E
thn
ic
Gy
psy
, R
om
a a
nd
Tra
vell
er
Servic
e C
hil
dren
Primary School 911 2.3% 436 475 782 86 23 11 9 42 92 338 0 0 815 0 12
Secondary School 527 1.8% 267 260 455 35 25 6 6 21 55 207 <5 <5 487 0 5
Produced by the Directorate Support Team (Data and Statistics), Cornwall Council using CAPITA One Database January 2015 School Census
Gypsy Roma and Traveller Children
Children who are from Gypsy Traveller families may have specific
educational and social needs relating to their interrupted learning113. Gypsy
Traveller pupils are more likely to be identified as having special
112Department for Education https://www.gov.uk/government/collections/statistics-school-and-pupil-
numbers 113
Chimat

JSNA Special Education Needs and Disabilities 102
18/12/18 V 0.9 Final
educational needs (SEN). This may be the result of families lacking
information or experiencing problems accessing appropriate health care, or
schools failing to respond appropriately to cultural difference. Gypsy
Travellers have significantly poorer health than other UK-resident English-
speaking ethnic minorities and economically disadvantaged white UK
residents. They also have one of the highest maternal death rates in the
UK.
The number of traveller and gypsy pupils has changed only slightly since
2010.
Traveller and Gypsy families in Cornwall114
2011 2012 2013 2014 2015 2016 2017
Traveller Of Irish Heritage 12 11 * 15 13 13 9
Gypsy/ Roma 124 119 11
3
12
3
11
5
11
3
12
8
*number sufficiently small to warrant redaction
There were no Traveller or Gypsy families on the Isles of Scilly in 2017.
ONS analysis, based on data from the 2011 Census, exploring the
characteristics115 of the Gypsy and Irish Traveller community, identified
that they had the highest proportion with no qualifications of any ethnic
group (60%) – almost three times higher than for England and Wales as a
whole (23%). Gypsy or Irish Traveller ethnic group was among the
highest providers of unpaid care in England and Wales at 11 per cent (10
per cent for England and Wales as a whole) and provided the highest
proportion of people providing 50 hours or more of unpaid care at 4 per
cent (compared to 2 per cent for England and Wales as a whole).
According to the census 47% of 16-24 year olds had no educational
qualifications. Four per cent of Gypsy or Irish Travellers who spoke a main
language other than English could not speak English well or at all – double
the proportion for the whole of England and Wales.
114
National Statistics – Department of Education https://www.gov.uk/government/statistics 115
What does the 2011 Census tell us about the characteristics of Gypsy or Irish travellers in England
and Wales? http://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/whatdoesthe2011censustellu saboutthecharacteristicsofgypsyoririshtravellersinenglandandwales/2014-01-21

JSNA Special Education Needs and Disabilities 103
18/12/18 V 0.9 Final
Appendix 9 – prevalence of SEND by gender, age and religion
The information in this section is from the 2011 Census.
Long-term health problem or disability by gender
All persons Males Females
Age 0 to 15 89,764 46,163 43,601
Age 16 to 24 51,498 26,023 25,475
All categories: Age 523,432 253,965 269,467
Long term health or disability
Day-to-day activities
Long-term health problem
or disability
Limited a lot Limited a little Not limited
All categories: Age 523,432 49,392 59,352 414,688
Age 0 to 15 89,764 1,408 2,234 86,122
Age 16 to 24 51,498 1,251 2,052 48,195
Male 253,965 23,035 27,408 203,522
- Age 0 to 15 46,163 903 1,389 43,871
- Age 16 to 24 26,023 670 1,001 24,352
Female 269,467 26,357 31,944 211,166
- Age 0 to 15 43,601 505 845 42,251
- Age 16 to 24 25,475 581 1,051 23,843
Long-term health problem or disability by gender
All persons Males Females
Age 0 to 15 89,764 46,163 43,601
Age 16 to 24 51,498 26,023 25,475
All categories: Age 523,432 253,965 269,467

JSNA Special Education Needs and Disabilities 104
18/12/18 V 0.9 Final
In Cornwall 3654 (4.1%) of children with long term health problems or
disability in the 0-15 year old age group have limited day-to-day activities,
1.6% of which are limited a lot. Only 0.8% identify themselves as
Christian, with many not identifying a religious preference.
Data for the Isles of Scilly is insufficiently detailed to allow analysis by
religion.
Note: 0-15 is the only age category available
*number sufficiently small to warrant redaction
Religious group
Day-to-day activities
Long-term
health problem
or disability
Limited a lot Limited a little Not limited
All categories: Religion 89,941 1,415 2,239 86,287
Christian 43,466 695 1,060 41,711
Buddhist 171 1 2 168
Hindu 110 2 1 107
Jewish 53 0 4 49
Muslim 210 2 3 205
Sikh 16 0 0 16
Other religion 240 2 11 227

JSNA Special Education Needs and Disabilities 105
18/12/18 V 0.9 Final
Author/s
Rebecca Cohen
Julie Moseley
Linda Howarth
Brian O’Neill
If you would like this information
in another format or language please contact:
Cornwall Council
County Hall Treyew Road
Truro TR1 3AY
Telephone: 0300 1234 100
Email: [email protected]
www.cornwall.gov.uk