-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
1/10
The Bacterial Etiology of DestructivePeriodontal Disease:
Current Concepts*3 ~ t ~ ~ l n dSocr-ansky and Ann e D.
Haffajee
T H E I N T E R P R E T A T I O N O F DIAGNOS TIC TESTS for the
detection of subgingival bacterialspecies is dependent on knowledge
of the microbial etiology of destructive periodontaldiseases.
Specific etiologic agents of these diseases have been sought for ov
er 1 00 years;however, the complexity of the microbiota, an
incomplete understanding of the biologyof periodontal diseases, and
technical problems have handicapped this search. Nonethe-less, a
number of possible pathogens have been suggested on the basis of
their associationwith disease, animal pathogenicity, and virulence
factors. The immunological responseof the host to a species and the
relation of successful therapy to the elimination of thespecies
have also been used to support or refute suspected periodontal
pathogens. Currentdata suggest that pathogens are necessary but not
sufficient for disease activity to occur.Factors which influence
activity include susceptibility of the individual host and
thepresence of interacting bacterial species which facilitate or
impede disease progression.Recent studies have attempted to
distinguish virulent and avirulent clonal types of sus-pected
pathogenic species and seek transmission of genetic elements needed
for patho-genic species to cause disease. Finally, the local
environment of the periodontal pocketmay be important in the
regulation of expression of virulence factors by pathogenicspecies.
Thus, in order that disease result from a pathogen, 1) it must be a
virulent clonaltype; 2) it must possess the chromosomal and
extra-chromosomal genetic factors toinitiate disease; 3) the host
must be susceptible to this pathogen; 4) the pathogen mustbe in
numbers sufficient to exceed the threshold for that host; 5 ) it
must be located atthe right place; 6) other bacterial species must
foster, or at least not inhibit, the process;and 7) the local
environment must be one which is conducive to the expression of
thespecies' virulence properties. J Periodontol 1992;
63.322-331.Key Words: Periodontal diseasesletiology; periodontal
diseasesimicrobiology; periodon-tal diseaseslpathogenesis.
Before beginning a discussion of current concepts of
thebacterial etiology of destructive periodontal diseases, it
isworth asking whether such knowledge would improve theprevention
and treatment of these diseases. Specific an-swers to this question
will be provided, at least in part, byDr. Listgarten in the next
presentation. However, perspec-tive may be gained by analogy to the
success of medicalmicrobiology in determining not only the etiology
of manyinfectious diseases, but in designing diagnostic tests
fortheir causative agents and, eventually, better methods fortheir
control. We note their success but may fail to appre-ciate the time
needed for its fruition. Lung infections serveas a useful example.
In 1882, Koch' published a paperdescribing the etiologic agent of
tuberculosis. Within oneyear, 26 papers were published telling him
why he waswrong.2 Criticisms started with concerns about
fundamentalbiology, suggesting that there were no such things as
bac-Wepartment of Periodontology, Forsyth Dental Center, Boston MA
.
teria or that there was only one species of bacteria wimany
different forms. Critics went on to criticize his staing and
microscopy techniques, animal model systems, dividual specific
findings, and his interpretations of thofindings. In 1883, Koch
published a specific rebuttal each of his critic^. This rebuttal
demo nstrated the raprate of publication in that era and Koch's
desire and abilito unmercifully flay his critics. (The tone of his
responwould be unthinkable in the current era of peer reviewKoch
was clearly correct. However, it is worth noting thspecific
treatments based o n this knowledge were not avaable for close to
40 years. Over the next 10 0 years, addtional etiologic agents of
lung infections were discoveresome as recently as 1977, when the
causative agent of Lgionnai re ' s di sease was dis~overed. '~~as
knowledge specific etiology of lung infection been useful?
Withosuch knowledge, physicians might have difficulty in indvidual
cases, in distinguishing between diseases such tuberculosis,
pneumococcal pneumonia, coccidiomycos
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
2/10
Volume 63Number 4 SOCRANSKY,HAFFAJEE100 YEARS OF PERIODONTAL
MICROBIOLOGY
SPECIFIC NON-SPECIFIC- ;* SPECIFIC---- -- J\-____Y--Fusrfoimis
Ius~formisv Streptococc~v
SprochetesTAmoebaT
M~xednfectionF~~osplrochetal. ? yrrlgivalisM~xednteclion ?
!nt~i!nedjaBlack ptgmented TBacferotdcs C rectusB forsyfhusSpmchete
VANUGv
A V ~ S C O S ~ ~ ST- 7- - -- - --
1890 1900 1910 1920 1930 1940 1930 1960 1970 1980 1990
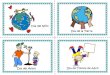
Figure I . D~ ag ram f some of the highlights of the past 100
years of th erearch for the etlolo g~c gents of destructive penodon
tal diseases.
and Legionnaire's disease. More importantly, the optimumspecific
therapy for each disease might not be employed.The point of this
introduction is to illustrate that it takestime to determine the
etiologic agents of diseases affectinga given organ system. It
takes additional time to developappropriate diagnostic tests for
those agents. Finally, it takeseven more time, sometimes decades in
the example citedabove, before specific therapies based on
knowledge ofspecific etiology can be developed. In the field of
perio-dontology, we are fortunate in some ways and unfortunatein
others. We are fortunate in that we can draw on theexperiences of
physicians who designed and implementeddiagnostic tests useful for
other organ systems; and we canemploy newly developed technologies
for the rapid iden-tification and enumeration of microbial species.
We areunfortunate in that we have a rather complex problem
inetiology to unravel. Furthermore, we have a tradition ofnon-use
of laboratory diagnostic tests to overcome. Clini-cians have
treated periodontal diseases more or less suc-cessfully for over
100 years without benefit of diagn ostictests for the detection and
identification of subgingival bac-terial species. They are
naturally somewhat skeptical of theneed for such tests. However,
when such tests can be dem-onstrated to increase the precision and
reliability of peri-odontal disease control, their ultimate
acceptance is highlyprobable.100 Years of Periodontal
MicrobiologyFigure 1 presents a diagram of some of the highlights
ofthe past 100 years of the search for the etiologic agents
ofdestructive periodontal diseases. The papers describing eachof
the pathogens or pathogen complexes have been re-viewed elsewh
ere.' Obv iously not all of the significantfindings have been
included, but enough to provide an ap-preciation that the search
has been long, that numerousagents have been suggested, and that
uncertainty has beena hallmark of this search. The time line is
divided into threephases: an initial phase where specificity in the
etiology ofdisease was the prominent concept; a period of
disillusion-ment in which non-specificity in bacterial etiology (or
lackof a role for bacteria) was dominant; and a return to the
concept of specificity in the etiology of periodontal disein the
1970s. Around the turn of the century, investigatwere proposing
poss ible e t iologic roles for fus iformamoebae, spirochetes, and
streptococci. Even though spcific etiology fell out of fashion at
approximately 193mixed infections continued to be studied and
specific mcrobial complexes suggested. In the mid-1960s, it was
sgested that a specific spirochete m ight be the cau se of
acnecrotizing ulcerative gingivitis on the basis of observilarge
numbers of this organism in sections of lesions of td i ~ e a s e .
~ , ~n the same decade, a possible role was sugested for
Actinomyces viscosus in the etiology of peodontal disease largely
on the basis of the pathogenicitythis species in hamster and rat
mod el system .^ Specificreturned as a fundamental concept of the
etiology of peodontal diseases after studies of localized juvenile
peodon titis implicated Actinobacillus actinomycetemcomitaas a
possible pathogen in this disease."-" Soo n thereaftPolphyromotzas
gingivalis was suggested to be importain adult periodontitis.12-l6
In more recent years, additiospecies have been suggested as
discussed below. Th e mapoint of Figure 1 is that, over the years,
numerous "patogens" have been proposed, but their role in disease
hnot been made entirely clear. This suggests that there habeen
problems associated with the search for etiologic ageas outlined
below.The Complexity of the ProblemThe difficulties encountered in
determining the etiologagents of destructive periodontal diseases
have been dcussed at length.'7,'8 In brief, investigators have been
hanicapped by the dual problems of technical difficulty ainadequate
understanding of the biology of destructive peodontal d iseases.
Techn ical difficulties start with the takiof plaque samples.
Obtaining precise, "uncontaminated"samples from the correct
location in a pocket at a stage active disease has been extremely
challenging . Even if susamples were obtained, the investigator
would be facwith discriminating the pathogen(s) from among the 300
400 candidate species encountered in subgingival plaquMaking
matters worse, many plaque isolates are difficuto grow and maintain
and even when this is possible, theare often problems in taxonomy
and identification.
While the technical problems are forbidding, lack ofclear
understanding of disease pathogenesis has been evmore troublesome.
Most difficulties in this area result fromisclassification of
disease type and status. Clearly, theare multiple destructive
periodontal diseases. Combinisubjects representing two or more
disease types into a singgroup diminishes the likelihood of
discriminating the pato g e n ( ~ )rom other species. In addition,
an individual mighave disease due to different species at different
sites. It also conceivable that a site could exhibit consecutive
epsodes of disease each due to different species. Failure recognize
such occurrences may obscure detection of patogenic species.
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
3/10
32 4 CURRENT CONCEPTS OF BACTERIAL ETIOLOGYMultiple d iseases
with multiple etiologies are not the onlyproblem of
misclassification faced by the investigator. De-structive
periodontal diseases leave an historical record oftheir progress in
terms of attachment and bone loss, pocketformation, and recession.
Even the causative organisms mayremain in periodontal pockets,
albeit in lower numbers,long past the time in which the disease wa
s active. E pisodicdisease will be discussed at greater length by
Drs. Jeffcoatand Goodson; however, taking samples from sites (or
sub-jects) which are in remission and interpreting them as ifthey
were obtained from sites undergoing active destructioncould lead to
erroneous conclusions.Another difficulty associated with attempts
to defineperiodontal pathogens is the possibility that some of thes
~s pe ct ed athogens may result from, rather than cause,
thediseases. Thus, disease caused by a pathogen at a site
changesthe environment at that site, quite possibly favoring
themultiplication of species which are favored by the new
en-vironment. These "opportunistic" species may be re-covered from
the site and assumed to be the cause of theobserved pathology. This
problem is particularly relevantsince most studies in this field
may be considered retro-spective case control studies, wher e sam
ples are taken fromcases and controls after disease has taken
place. Prospectivestudies should diminish this concern to some
extent.It is likely that a subset of the periodontal lesions
weobserve result from two or more species acting in concertto cause
disease. These mixed infections create another de-gree of
complexity for the research worker. The number ofpossib!e co mbina
tions of two, three, o r more species thatwould have to be
evaluated for their role in disease makes
detection of such mixtures in clinical material more
difficultthan defining the role of single species.It is clear that
suspected periodontal pathogens can bedetected in low numbers in
healthy subjects or in healthysites in diseased subject s. This
"carrier state" could rep-resent a long lag phase prior to
detection of disease or itcould represent a true carrier state in
which that site mightnever show disease. The carrier state has been
recognizedfor medically-important bacteria for decades. The
presenceof the carrier state complicates analysis, since it
providessamples from sites of non-disease which harbor the
samepathogens as sites of disease. Detection of pathogens inhealthy
sites could also be explained by differences in clonaltype. There
are data to indicate that strains of the samesubgingival species
exhibit different pathogenicity in ani-mal model Failure to
distinguish virulent fromavirulent clonal types would impair our
ability to distin-guish pathogenic species. This area will be
amplified ingreater detail below.The Approach to Determining
Etiologic AgentsThe complexity of the problem outlined above
requires theformulation of strategies for distinguishing
periodontalpathogens. The classic approach to this problem has
beento use the criteria known as Koch's postulates. These are:
J PeriodonApril 1992 (Suppleme1) the agent must be isolated from
every case of diseas2) the agent must not be recovered from cases
of othforms of disease or non-pathogenically; and 3) after isoltion
and repeated growth in pure culture the pathogen muinduce disease
in experimental animals. It is worth notithat while these criteria
have been repeatedly employed dental research, the third criterion
was abandoned by Koin 188426 when he could not induce cholera using
Vibrcholera in animal model systems. The recognition of
tcarrier-state led to the relaxation of the second criterion
1890.27In recent years, periodontal research workers have etended
Koch's postulates somewhat to include criteria association,
elimination, animal pathogenicity, host rsponses, and formation of
virulence factors. The criteriof association requires that the
suspected pathogenic specibe more frequently detected and at higher
levels in casthan in controls. For example, the species should be
highin actively progressing sites than in healthy sites,
non-prgressing sites, or sites showing improvement.
Longitudinassessment might also show an increase in the species
prito or concomitant with measured disease progression.
Tfundamental basis of elimination studies is that
treatmeadministered to subjects with a given form of disease
shouinfluence both the clinical status of the disease and m embeof
the associated microbiota. It is reasonable to expect thsuccessful
therapy will diminish the level of a pathogen anhalt disease
progression. Failure to eliminate or diminithe level of the
pathogen ultimately might lead to furthprogression at that site or
in that subject.Testing of pathogenicity in animal model systems
cotinues to be used to further support (or refute) possibpathogens.
In spite of concerns with animal model syt e m ~ , ' ~hey can
provide additional evidence of roles fcertain species in di ~e as
e~ $- ~Ond will be particularly usefin defining virulence factors
for di ~ e a s e .~ ' he host rsponse has also been employed in
attempting to discrimnate periodontal pathogens. Most notable has
been thassociation of antibody response to A. actinomycetemcomitans
as a marker demonstrating the relationship of thspecies with
localized juvenile period on ti ti^.^^.^^ It is fethat a
periodontal pathogen which causes destructive perodontal disease
often will elicit an elevated immunologicresponse, either locally
or systemically. In certain circumstances, it is conceivable that
the pathogen may diminisaspects of the host response. Finally, the
ability of certaispecies to produce virulence factors has been used
to suport possible roles of such species in periodontal diseaseThe
production of unique biochemical determinants bpathogens may be
important in disease and an indicator othe potent ia l of the
species to cont r ibute to d iseasprogression.Currently Suspected
PathogensTables 1, 2 and 3 are excerpted from a previously
publisheworkI8 and list some of the currently suspected
pathogen
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
4/10
Volume 63Number 4 SOCRANSKY. IIAFFAIEE 325Table 1. Data That
Suggest Actinobacillus actinomyceterncomitans asa Possible
Etiologic Agent of Destructive Periodontal Diseases(adapted from
18)Criterion FindingsAssociation Elevated in lesions of juvenile
periodontitisUnusual in health or gingivitis subjectsElevated in
some periodontitis lesions
Elevated in active juvenile periodontitis lesionsDetected in
prospective studiesDetected in apical area of pocket or in tissues
ofUP lesions
Elimination Elimination resulted in successfu l therapyRecurrent
lesions harbored speciesHost response Elevated serum antibody in
juvenile periodontitisElevated local antibody in juvenile
periodontitisVirulence factors Leukotoxin, collagenase, endotoxin,
epitheliotoxin,fibroblast inhibitory factor, bone
resorptioninducing factorAnimal studies Induce disease in
gnotobiotic rat
Table 2. Data That Suggest Porphyromonas gingivalis as a
PossibleEtiologic Agent of Destructive Periodontal Diseases
(adapted from18)Criterion FindingsAssociation Elevated in lesio ns
of periodontitisUnusual in health or gingivitis subjectsPresent on
crevicular epithelial cellsElimination Elimination or suppress ion
resulted in successfu ltherapyRecurrent lesions harbored
speciesHost response Elevated serum antibody in
periodontitisElevated local antibody response in
periodontitisVirulence factors Collagenase, trypsin-like activity,
fibrinolysin, otherproteases, phospholipase a,
phosphatases,endotoxin, H,S, NH,, fatty acids, and factors
whichadversely affect polymorphonuclear leukocytesAnimal studies
Important role in experimen tal mixed infectionsStudies in monkeys
and dogs
Table 3. Data That Suggest Additional Species as Possible
EtiologicAgents of Destructive Periodontal Diseases (adapted from
18)Host Virulence AnimalSpecies Association Elimination Response
Factors Studies
P. intennediaF. nucleatumB. forsythusC. rectusE. corrodensP.
microsSelenomonas sp.Eubacterium sp .(E. brachyE. nodatumE.
timidum)Spirochetes*Indicates relative number of publications.
and the nature of some of the data which support their
role.Documentation of the findings is provided in that paper.
-- -PATHOGENS SPECIES
IMPA IREDNEUTROPHILS
A acltn~mycefemcomrrans Aciinomyces spB iorsyrhus C
ochraceaINADEQUATE OR E cor iodcns S tnriisUNREGULATED F oucleafum
S sangurs 1IMMUNOLOGICAL P micros V parvulaRESPONSE P gingrvalisLPS
RESPONSIVENESS P irreiined,a
AIDS C recfusDIABETES Selenomonas spSMOKING Eubacferiiini
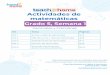
spSoiiochcfcsDRUGSFigure 2. Diagrammatic representation of 3 groups
of factors which de-
termine whether active periodontal disease w ill occur in a su
bject or at asite.The evidence for these species differs and it is
highly prob-able that some of these species will be removed from
thelist and others added. Currently, more data are available
tosupport the pathogenic roles of A. actinomyceterncomitansand P.
gingivalis than are available for other suspectedperiodontal
pathogens.Evolving ConceptsThe foregoing discussion indicated the
level of complexitythat has been encountered in the search for the
etiologicagents of destructive periodontal diseases. In spite of
thiscomplexity, a number of species have been suggested whichmay be
pathogens of these diseases. However, it is clearthat while
presence of pathogens is necessary for diseaseactivity to take
place, it is not sufficient. If the presence ofpathogens were
sufficient, then detection of the pathogenwould be synonymous with
detection of disease activitymaking diagnostic tests and their
interpretation quite sim-ple. Clearly, other factors play a role in
the initiation, pro-gression, and remission of destructive
periodontal diseases.Figure 2 is a diagrammatic representation of
three groupsof factors which determine whether active periodontal
dis-ease will occur in a subject or at a site. First, the host
mustbe susceptible to the pathogens or disease will not occur.Some
of the factors which have been suggested to increasesusceptibility
of periodontal subjects include impaired neu-trophils, inadequate
or unregulated host immunologic re-sponse, differences in LPS
responsiveness, AIDS, diabetes,tobacco, and drug use. Some of these
factors will be dis-cussed in greater detail by Drs. Genco and Page
and willnot be elaborated further here. The second essential
factorfor disease initiation and progression is the presence of
oneor more pathogens of the right clonal type in sufficientnumbers
to cause disease. A number of suspected pathogensare listed in
Figure 2 which were derived from Tables 1 to3. The role of
"beneficial species" (to the host) in theprogression of disease is
less obvious. As will be discussedbelow, high levels of beneficial
species, even in the pres-ence of pathogens, may have a marked
effect on diseaseinitiation and progression. Finally, the local
periodontal en-vironment may have a profound effect on the
expression ofvirulence factors by resident pathogens influencing
disease.
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
5/10
326 CURRENT CONCEPTS OF BACTERIAL ETIOLOGYEXTENT OF DISEASE
0 l o 6 L ~ ~ L - U n-r;i_n 1 LL- 7-C) l o 5 - ~- WIDESPREADC
,A
HEALTHY
1 1 3 3 3 1MAXILLA MANDIBLE
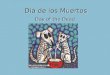
Figure 3. Diagram demonstrating the distribution of A.
actinomycetem-comitans serorype b in two healthy subjects and two
subjects each withlocalized and widespread disea se. In this
figure, sites with prior attach -ment loss > 3 mm are indicated
by boxes and bacterial levels by thecircles. Empty spaces represent
no disease and no infection (there wereno missing samples in 6
subjects). The numbers below each panel indicatequadrant (1,2,3,4)
and tooth (1-7, i. e. central incisor to second m olar)from which
mesial samples were taken. (Adapted rom 34).
The Role of Disease SusceptibilityIn ongoing studies of
periodontal disease at Forsyth DentalCenter, su bjects with
destructive periodontal diseases havebeen evaluated longitudinally
using clinical, microbiologi-cal, and immunological
parameter^.^^,^' Briefly, 67 sub-jects with prior evidence of
destructive periodontal diseaseswere monitored every 2 months for
pocket depth, attach-ment level, subgingival temperature, bleeding
on probing,suppuration, redness, and plaque. A subject was
consideredto be active if he or she exhibited one or more sites
withattachment loss > 2.5 mm in a Zmonth period. In addition,the
levels of 14 subgingival species were determined insubgingival
plaque samples taken from the mesial aspect ofeach tooth in each
subject at each visit using a "colony-lift" method and DNA probes."
Ten suspected pathogens:A. actinomycetemcomitans serotypes a and b,
Bacteroidesforsythus, Fusobacterium nucleatum ss vincentii,
Pepto-streptococcus micros, P. gingivalis, Prevotella intermed
iahomology groups I and 11, Streptococcus intermedius, andCamp
ylobacter rectus (formerly Wolinella recta) and foursuspected
beneficial species: Capnocytophaga ochracea,Streptococcus sanguis I
and 11, and Veillonella pawula wereenumerated. The results of this
prospective study confirmedthe role of certain suspected
periodontal pathogens.35One of the most interesting findings from
this type ofinvestigation was the demonstration that microbial
speciesare not evenly distributed from subject to subject or
fromsite to site in the same subject. Figures 3 and 4 indicate
thedistribution and levels of P. gingivalis and A.
actinomy-cetemcomitans serotype b in two healthy, two
minimallydiseased, and two widespread disease subjects. A
actinomy-cetemcomitans serotype b was found less frequently
inwidespread disease subjects than in subjects with
localizeddisease (Fig. 3). In the example shown, one
widespreaddisease subject (MA) did not harbor the organism at
anysampled site, while one of the localized disease subjects(CD )
harbored the species in 12 sites. Interestingly, one of
J PeriodontApril 1992 (SupplemenEXTENT OF DISEA
I I I: I t 6 t i 4 11 12 1 1 21 2 2 2 3 2 % 21 2 5 2 7 3 7 3 C
3131 1 1 3 2 11 4) 6 2 4 3 r < : / 5 r :
MAXILLA MANDIBLE
5sWIDESPREAD
MA
MTLOCALIZED
CD
DOHEALTHY
AM
Figure 4. Diagram demonstrating the distribution of P .
gingivalis in healthy subjects and 2 subjects each with localized
and widespread disease. F or details regarding the composition of
the diagram see F igure 3(Adapted rom 34).
the healthy subjects harbored the species in four sites, albeat
low levels. Figure 4 provides examples of different patterns of
colonization by P. ging.valis. While this speciewas not detected in
any sampled site in one healthy (AMand one localized disease
subject (CD), it was found ihigh numbers in 23 of 28 sites in one
of the subjects witwidespread disease (MA). Although many subjects
harbored this species, the number of sites colonized and thpattern
of colonization were different. The lack of homogeneity of
distribution of a given species is important noonly in
understanding disease initiation and progression, buin designing
sampling procedures for diagnostic tests.While monitoring these
subjects longitudinally, it became apparent that subjects with
widespread disease exhibited more sites showing new attachment loss
than subjectwith fewer affected sites at baseline. The relationship
between prior extent of disease and new disease progressionhas been
repor ted in other ~tudies .~~-~Ohis observatiomight have been due
to the presence of higher levels of thesuspected pathogens in the
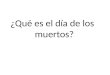
widespread disease subjects. Totest this hypothesis, the mean p
ercentages of the total cultivable microbiota for each species in
subjects with differenlevels of periodontal destruction at baseline
were computed(Fig. 5 ) . Percentages of suspected pathogens were
highesin subjects with localized destruction and lowest in
thewidespread disease subjects. Such findings could be explained in
a number of ways. First, the pathogens of themore widespread forms
of disease may not have been amongthe test species. Second, the
pathogens m ay have been correct but not of a virulent clonal type.
Third, the pathogensmay have been of a virulent clonal type, but
the presenceof beneficial species (to the host) or unfavorable
environmental conditions precluded disease in the localized
diseaseindividuals. Finally, and most relevant to this section,
wasthe possibility that the hosts differed in their threshold
sus-ceptibility to given pathogenic species. This last
hypothesiswas supported by the observation that lower threshold
percent of sites colonized by suspected pathogens including,C.
rectus, P. intermedia I , P. gingivalis, and A.
actinomycetemcomitans serotypes a and b were needed to produceodds
ratios > 4 for disease progression in subjects with
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
6/10
Volume 63Number 4 SOCRANSKY, HAFFAJEE 32716
MEAN %TOTAL
CULTIVABLEFLORA
12
A, actinomi/cetemcomitans aF, nucleatum ss.vlncentl1
16MEAN %TOTAL
CULTIVABLEFLORA
12
A. acti,nomycetemcomi,tans58 A, act~nomycetemcom~tansF,
nucleatum ss.vlncentl1
4 P, intermedia IP. intermedia II
0LOCALIZED WIDESPREADINTERMEDIATE
Figure 5. Stacked bar chart of the mean levels of the 10
suspected pathogen s detected using DN A probes insubjects with
localized (< 16 % of sites with attachment loss > 3mm at
baseline), intermediate (16% to 44%affected sites) and widespread j
> 44% affected sites) periodontal destruction. The mean for each
species wascomputed by averaging the levels oftha t species for
each subject and then averaging the means for all subjectswithin
the localized, interm ediate, or widespread disease groups. The
shading of the bars is used for o rientationpurposes only.
widespread baseline attachment 10~s.~'ubjects who exhib-ited
both widespread disease and high levels of suspectedpathogens
exhibited mo re active sites than subjects in otherg r o ~ p s . ~
'Bacterial InteractionsPeriodontal pathogens do not exist in dental
plaque in iso-lation. Indeed this has been one of the most
confusing as-pects of research in this area. Undoubtedly, the
otherorganisms in the pocket affect the ability of pathogens
tocause disease progression. In certain situations, the pres-ence
of one species could facilitate the colonization of an-other
pathogenic species or act synergistically with thatspecies to cause
disease. A lternatively, a bacterial speciescould be beneficial to
the ho st acting to prevent or minimizetissue damage.
During the course of enumerating subgingival species inplaque
samples using a "colony-lift" method, it was notedthat a number of
colonies produced areas of P hemolysison blood agar plates. These
colonies included strains ofActinomyces naeslundii, Actinomyces
odontolytcus, Acti-nomyces israelii, A. viscosus, Streptococcus
pyogenes,Streptococcus constellatus, Prevotella melaninogenica,
andPrevotella denticola (unpublished results). The remarkablystrong
relationship between the presence of p hemolyticspecies in a
subject or at a site and the levels of "black-pigmented
Bacteroides" species is of interest to the presentdiscussion. For
examp le, mean coun ts of "black-pigmented
Bacteroides" species (P. intermedia I, P. intermedia 11,and P.
gingivalis) at sites where P hemolytic species werenot detected
were 0.90 -+ 0.20 (95% C1, n = 1758) and2.73 + 0.38 (n = 1035) at
sites where P hemolytic specieswere detected (unpublished data).
While there are a numberof interpretations of this observation,
perhaps the simplestis that the p hemolytic species cause damage to
red bloodcells or other host tissue cells and foster the
colonizationof the suspected periodontal pathogens. These in turn
mightlead to tissue damage. (One alternative explanation is
that"black-pigmented Bacteroides" species result from
tissuedamage.)Bacterial interactions can also be beneficial to the
host.For example, a species could affect disease progression ina
number of ways: 1) by "passively" occupyin g a nichewhich might
otherwise be colonized by a pathogen; 2) byactively limiting a
pathogen's ability to adhere to appro-priate tissue surfaces; 3) by
adversely affecting the vitalityor growth of a pathogen; 4) by
affecting the ability of apathogen to produce virulence factors; or
' 5) by degradingvirulence factors produced by the pathogen. One
well-doc-umented example of a bacterial interaction which is bene-f
ic ia l to the hos t is the e ffec t of S. sanguis o n
A.actinomycetemcomitans. S. sanguis pro duces H,O,, wh icheither
directly or by host enzyme amplification kills A.
ac-tinomycetem~omitans.~~*~~nother example of a relation-ship which
may be beneficial to the host is provided inFigure 6 where the
levels P. gingivalis and C. ochracea in
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
7/10
328 CURRENT CONCEPTS OF BACTERIAL ETIOLOGYJ PerioA~ r i l 992
(Su~~
INACTIVE ACTIVEMEAN% lo j7-T= 0.08 + 0 . 7 ~ y = 1.78 - 0 . 4
~P. gingivalis r = 0.72 r = -0.23
0 5 10 0 5 10MEAN % C. ochracea
Figure 6. Scatter plots of the mean % of C . ochracea (x-axis)
and mean% P . gingivalis (y-axis) n subjects subset on the basis of
showing (active)or not showing (inactive) I or more sites with
attachment loss > 2.5 mmin 2 months. Each circle represents the
mean values for one subject.(Adapted from 41).
active and inactive subjects are presented. W hen high leve lsof
P. gingivalis were found in subjects with high levels ofC.
ochracea, the risk of new attachment loss in subjectswas
diminished. In contrast, subjects with high levels of P.gingivalis
and low levels of C. ochracea tended to exhibitdisease
progression.Ano ther exam ple of the role of "beneficia l" spec ies
wa sobserved in preliminary results from an ongoing treatmentstudy
at Forsyth. Sub jects were treated by Widman flapsurgery and
scaling together with one of the four followingsystemic agents:
tetracycline, augmentin, ibuprofen, or pla-cebo. Subjects receiving
the adjunctive antibiotic therapyshowed a higher percentage of
sites with attachment levelgain and higher levels of the suspected
beneficial speciesC. ochracea and S. sanguis I1 post-therapy than
subjects inthe other two groups. Although this study is far from
com-plete, the early results indicated that successful therapy
maybe dependent not only on the reduction or elimination
ofpathogens, but on subsequent colonization of high levels
of"beneficial" species (unpublished data).The Concept of Virulent
Clonal Types of PathogensThe concept of bacteria playing important
roles in destruc-tive periodontal diseases was reintroduced in the
1950s whenit was suggested that plaque control was essential in
thetreatment of periodontal patients. This finding gave rise tothe
non-specif ic p laque hypothesi~ .~~ater studies, as in-dicated
above, suggested that all organisms in plaque maynot be equally
capable of causing destructive periodontaldiseases and thus the
concept of specificity in destructiveperiodontal disease
re-emerged. In recent years, infectiousdisease workers in medicine
have indicated that not all clonaltypes of a pathogenic species are
virulent for man. Forexam ple six of 104 clonal types of
Haemophilus influenzaeappear to be virulent, w hile two of 15
clonal types of Hae-mophilus influenzae biogroup aegyptius have
been shownto be associated with Brazilian purpuric It seemslikely
that here might be multiple clonal types of periodon-tal pathogens,
some of which are virulent and others ofwhich are not. This is an
attractive hypothesis in that it
might explain observations such as the presence of "pogens" in
healthy sites or subjects and the return of "pogens" to
successfully treated sites. In order to supporhypothesis, it will
be necessary to demonstrate: 1) that are multiple clonal types
within a pathogenic speciethat these clonal types differ in
pathogenicity; and 3)som e clonal types are associated with health
and othersdisease. There are a number of ways in which investigcan
distinguish clonal types. Among these are the exnation of
multi-locus enzyme patterns and of ribotypeindividual strains.48
The latter approach has been useexamine ribotypes of P. [email protected]
and C. rectus (unlished data). Preliminary data from these studies
havdicated that there are multiple clonal types in each of
tspecies. The second requirement, differences in pathnicity for
different clonal types, has not yet been elished. However, it has
been shown that there are sdifferences in the pathogenicity of P.
gingivalis isolatanimal test systems.19-21~23-25hese differences
may blated to clonal type, but this has not been determined.final
test, the comparison of clonal types isolated from cand controls,
has not been initiated as yet; however, testing will be of enormous
interest.Transmission of Virulence FactorsThe possibility of the
transfer of genetic information cofor virulence properties from o
ne strain or species to anodeserves consideration. Imagine, if you
will, a pathowith virtually all the genetic factors needed to cause
disbut lacking in a single key element. For exam ple, the smight be
lacking an essential adhesin, toxin, or hemolyConceivably, this
strain might acquire the genetic inmation needed to produce this
factor from other cellthat or other species in that environment.
There is prdence for this concept in that transfer of virulence
facby medically-important bacteria have been shown as as the
transfer of antibiotic resistance. Indeed, bactphage-related
virulence has been ascribed to strains
oactinomycetemcomitans.49~50ntibiotic resistance has transferred
from P. denticola to P. i n t e rmed i ~ .~~hesence of an essential
extra-chromosomal element mighplain failure of a putative pathogen
to cause disease manner analogous to differences in clonal types as
cussed above.The Importance of Regulation by the
LocalEnvironmentConsider for a m oment the possibility that a
virulent cltype of a pathogenic species colonizes a site in
seemisufficient numbers to cause disease in a susceptible and yet
disease does not occur. The possibility that "beficial" species
have ameliorated this process has beencussed above. However, there
might be other explanatfor this phenomenon. Until recently, w e and
perhaps othad the view that a cell of a virulent pathogenic
specontinuously produced its virulence factors. Recent w
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
8/10
Volume 63Number 4 SOCRANSKY.HAFFAlEEin other fields suggest that
this may not be the case. It hasbeen shown that strains of many
pathogenic species "turn-on" or "turn -off" production of virulence
factors depend-ing on the n atu re of th eir e n v i r ~ n m e n t
. ~ ~ ~ ' ~ ~ ~ 'pparentlythe species "senses" its environm ent and
a regulating geneaffects a global network of genes which
simultaneously turnon or off production of multiple virulence
factors." Tem -perature, iron concentration, osmolarity, magnesium,
andcalcium all have been shown to be environmental factorswhich
influence the production of virulence factor^.^^^'^^^"It has been
shown that production of virulence factors bysuspected periodontal
pathogens can be influenced by en-vironment. For example,
expression of certain cell mem-brane proteins and pathogenicity in
animal model systemsby P. gingivalis is influenced by the level of
iron or heminin the medium in which the strain is g r ~ w n . ' ~ -
' ~emper-ature has been shown to differ from subgingival site
tosubgingival site in the same oral cavity and in
differentsubject^.'^ In addition, higher subgingival temperature
ap-pears to confer higher risk of new attachment loss and
in-fluence (or be influenced by) the levels of certain subgingivals
p e ~ i e s . ~ ~ , ~ "t is tempting to speculate that subgingival
tem -perature or other environmental factors might influence
theexpression of virulence factors by virulent clonal types
ofpathogens and turn these quiescent subgingival residentsinto
vehicles of destruction. Thus, a change in environmentresulting
from a local traumatic incident such as food impac-tion might
result in a local inflammation and an alteration inthe environment
which induces the production of virulencefactors by a resident
pathogen in that site. Although the datarelating environment to
pathogenicity are limited, the conceptis so attractive that it
warrants further investigation.DISCUSSIONThe material presented
above attempts to describe some ofthe changing concepts in the
etiology of destructive peri-odontal diseases. These changes are
driven, in part, bydiscrepancies between microbial and clinical
status and, inpart, by parallel recognitions in infectious disease
micro-biology. Infection does not mean instantaneous disease.
Evenagents as lethal as the HIV virus can persist in individualsfor
months to years before clinical manifestations are ob-served.
Infection by a species does not necessarily meanthat disease is
imminent. The carrier state of quite patho-genic species such as
Salmonella typhi provide examplesof this phenomenon. All strains of
a pathogenic species arenot pathogenic. A test of the presence of
Escherichia coliin the human intestinal tract would probably reveal
the pres-ence of this species in most individuals. However,
mostindividuals do not get diarrhea associated with this
speciesbecause only a subset of E. coli strains are
entero-toxigenic.Thus, lag phase, host susceptibility, and clonal
type canaffect interpretation of diagnostic tests.
I t would be simple and convenient if one could take asample of
plaque and detect a pathogen and know imme-diately that this was
the cause, or about to be the cause, of
disease at that site. The foregoing discussion should wus that
this may not be the case. The outcome, diseinitiation or
progression, is a resultant of the interplay tween a large number
of factors. The presence of a paogenic species is necessary, but
not sufficient for diseto take place. In order that disease result
from this pathgen, 1) it must be of a virulent clonal type; 2) it
mpossess the chromosomal and extra-chromosomal genefactors to
initiate disease; 3) the host must be susceptito this pathogen; 4)
the pathogen must be in numbers sficient to exceed the threshold
for that host; 5) it must located at the right place; 6) other
bacterial species mfoster, or at least not inhibit, the process;
and 7) the loenvironment must be one which is conducive to the
exprsion of the species' virulence properties. With this list mind
it is not surprising that disease activity, at least thwhich causes
major destruction, appears to be a somewhuncommon event. Assuming
that all factors are in order an episode of active disease to take
place, the episode itsmarkedly changes the equation leading to a
massive loresponse by the host, shifts in the other oral
microorgaisms, and establishment of a new equilibrium.The foregoing
discussion highlights both the complexof the problem and the fact
that investigators have sharened the focus of their search. If one
had asked "Whcauses periodontal disease?" 150 years ago, a likely
answmight have been "God only knows." Over time, the sponses to
that question might have shifted to "accumlations of bacteria" or
"specific bacterial spec ies 7' and,the above discussion were
correct, to "specific bacteria the right clonal type with the
essential genetic elementssufficient numbers for that host with
appropriate additionspecies in the right environm ent." Such
progression deonstrates both the evolution of the concepts and the
iproved focus of investigation. In turn, improvement in focshould
lead to improvement in potential diagnostic tesFor example, a
diagnostic test might not seek a species, ba specific clonal type
of a species or a critical element that species such as the gene
for toxin production in thecoli example cited above. In addition,
diagnostic tests fbacteria would probably not exist in isolation,
but in combination with other diagnostic tests of host
susceptibiliand/or status of the local environment. Given
sharpenunderstanding of the biologic basis of disease, it may
surmised that combinations of diagnostic tests will be usefin
determining not only the pathogens of disease, but ttherapies best
suited for control.AcknowledgmentsThis work was supported in part
by research grants D04881 and DE-02847 from the National Institute
of DentResearch.REFERENCES1. Koch R. Die aetiologie der
tuberculose. Berliner Klinische W ochschn'ft 1882;19:221-230.
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
9/10
330 CURRENT CONCEPTS OF BACTERIAL ETIOLOGYJ PeriodontolApri l
1992 (Su ~ole me nt)
2. Koch R. Kritische Besprechung der gegen die Bedeutung der
Tub-erkeilbazillen gerichteten Publikationen. Deutsche
MedizinischeWochenschrift 1883;9: 137-141.
3. Fraser DW, Tsai T, Orenstein W, et al. Legionnaires' disease
I:Description of an epidemic of pneumonia. New England J
Med1977;297:1189-1197.
4. McDade JE, Shepard CC, Fraser DW, et al. Legionnaires'
disease:Isolation of a bacterium and demonstration of its role in
other respi-ratory diseases. New England J Med
1977;297:1197-1203.5. Socransky SS, Haffajee AD, Listgarten MA.
Microliiology (plaque).In: Grant DA, Stern IB, Listgarten MA, eds.
Periodontics, 6th ed.St. Louis: C.V. Mosby: 1987:147-197.
6. Listgarten MA, Socransky SS . Ultrastructural characteristics
of a spi-rochete in lesions of acute necrotizing ulcerative
gingivostomatitis(Vincent's infection). Arch Oral Biol
1964;9:95-96.
7. Listgarten MA. Electron microscopic observations of the
bacterialflora of acute necrotizing ulcerative gingivitis. J
Periodontol1965;36:328-339.
8 . Jordan HV, Keyes PH. Aerobic, Gram-positive, filamentous
bacteriaas etiologic agents of experimental periodontal disease in
hamsters.Arch Oral Biol 1964;9:401-414.
9. Newman MG, Socransky SS. Predominant cultivable microbiota
inperiodontosis. J Periodont Res 1977; 12: 12 c1 28 .
10. Slots J. The predominant cultivable organisms in juvenile
periodon-titis. Scand J Dent Res 1976;84:1-10.
11. Newman MG, Socransky SS, Savitt ED, Propas DA, Crawford
A.Studies of the microbiology of per iodontosis . J
Periodontol1976;47:373-379.
12. Slots J. The predominant cultivable microflora of advanced
peri-odontitis. Scand J Dent Res 1977;85:114-121.
13. Spiegel CA, Hayduk SE, Minah GE, Kryolap GN.
Black-pigmentedBacteroides from clinically characterized
periodontal sites. J Perio-dont Res 1979; 14:376-382.
14. Tanner ACR, Haffer C, Bratthall GT, Visconti RA, Socransky
SS.A study of the bacteria associated with advancing periodontal
diseasein man. J Clin Periodontol 1979:6:278-307.
15. White D, Mayrand D. Association of oral Bacteroide.~with
gingivitisand adult periodontitis. J Periodont Res
1981;16:259-265.
16. Zambon JJ, Reynolds HS, Slots J. Black-pigmented Bacteroides
spp.in the human oral cavity. Infect lmmun 1981;32:198-203.
17. Socransky SS, H affajee AD , Sm ith GLF, Dzink JL.
Difficu!ties en-countered in the search for the etiologic agents of
destructive peri-odontal diseases. J Clin Periodontol
1987;14:588-593.
18. Socransky SS, Haffajee AD. Microbiological risk factors for
destruc-tive periodontal diseases, In: Bader JD, ed. Risk
Assessment in Den-tistry. Chapel Hill: University of North Carolina
Dental Ecology;1990:79-90.
19. Grenier D, Mayrand D. Selected characteristics of pathogenic
andnonpathogenic strains of Bacteroides gingivalis. J Clin
Microbiol1987;25:738-740.
20. Van Steenbergen TJ, Delemarre FG, Namavar F, De Graaff J.
Dif-ferences in virulence within the species Bacteroides
gingivalis. An-tonie Van Leeuwenhoek 1987;53:233-244.21. McKee AS,
McDermid AS, Wait R, Baskerville A, Marsh PD . Iso-lation of
colonial variants of Bacteroides gingivalis W50 with a re-duced
virulence. J Med Microbiol 1988;27:59-64.
22. Marsh PD, McKee AS, McDermid AS, Dowsett AB.
Ultrastructureand enzyme activities of a virulent and an avirulent
variant of Bac-teroides gingivalis W50. Fems Microbiol Let
1989;50:181-185.
23. Neiders ME, Chen PB, Suido H, Reynolds HS, Zambon JJ.
Heter-ogeneity of virulence amon g strains of Bacteroides gingiv
alis. J Per-iodont Res 1989;24:192-198.
24. Shah HN, Seddon SV, Gharbia SE. Studies on the virulence
prop-erties and metabolism and pleiotropic mutants of Porphyromonas
gin-givalis (Bacieroides gingivalis) W50. Oral Microbiol
lrnmunol1989;4:19-23.
25. Smalley JW, Birss AJ, Kay HM , McKee AS, Marsh PD. The
distri-
bution of trypsin-like enzyme activity in cultures of a virulent
and anavirulent strain of Bacteroides gingiv alis W50. Oral
Microbiol Im-munol 1989;4: 178-181.
26. Koch R. Erste Konferenz zur Eroterung der Cholerafrage.
BerlinerKlinische Wochenschrift 1884;30:20-49.
27. Carter KC. Essays of Robert Koch. New York: Greenwood
Press;1987; xviii-xix.
28. Kornman KS , Holt SC, Robertson PB. The microbiology of
ligature-induced periodontitis in the cynomologus monkey. J
Periodont Res1981;16:363-371.
29. Kornman KS, Siegrist B, Soskolne WA, Nuki K. The
predominantcultivable subgingival flora of beagle dogs following
ligature place-ment and metronidazole therapy. J Periodont Res
1981;16:251-258.
30. Holt SC, Ebersole J, Felton J. Brunsvold M, Kornman KS.
Implan-tation of Bacteroides gingivalis in nonhuman primates
initiates pro-gression of periodontitis. Science
1988;239:55-57.
31. Socransky SS, Haffajee AD. Microbial mechanisms in the
pathogen-esis of destructive periodontal diseases: A critical
assessment. J Per-iodont Res; 1991;26: 195-212.
32. Ebersole JL, Taubman MA, Smith DJ, Genco RJ, Frey DE.
Humanimmune responses to oral microorganisms. I. Association of
localizedjuvenile periodontitis (LJP) with serum antibody responses
to Acti-nobacillus actinomycetemcomitans. Clin Exper Immunol
1982;47:43-3L .
33. Ebersole JL, Taubman MA, Smith DJ, Hammond BF, Frey DE.Human
immune responses to oral microorganisms. 11. Serum
antibodyresponses to antigens from Actinobacillus
actinomycetemcomitans andthe correlation with localized juvenile
periodontitis. J Clin Immunol1983;3:321-331.
34. Haffajee AD, Socransky SS, Smith C, Dibart S. The use of
DNAprobes to examine the distribution of subgingival species in
subjectswith different levels of periodontal destruction. J Clin
Periodontol1992;19:84-91.
35. Haffajee AD, Socransky SS , Smith C, Dibart S. Relation of
baselinemicrobial parameters to future periodontal attachment loss.
J ClinPeriodontol 1991 18:744-750.
36. Gunaratnam M, Smith GLF , Socransky SS, Smith CM, H affajee
AD.Enumeration of subgingival species on primary isolation plates
usingcolony lifts. Oral Microbiol Immunol 1992;7:14-18.
37. Albandar JM , Rise J, Gjermo P, Johansen JR. Radiographic
quanti-fication of alveolar bone level changes. A 2-year
longitudinal studyin man. J Clin Periodontol 1986;13:195-200.
38. Axelsson P, Lindhe J. Effect of controlled oral hygiene
procedureson caries and periodontal disease in adults. J Clin
~eriodon to l1978;5:133-151.
39. Haffajee AD, Socransky SS, Dzink JL, Taubman MA, EbersoleJL.
Clinical, microbiological and immunological features of sub-jects
with refractory periodontal diseases. J Clin
Periodontol1988;15:390-398.
40. Haffajee AD, S ocransky SS, Lindhe J, Kent RL, Okamoto H,
Yoney-ama T. Clinical risk indicators for periodontal attachment
loss. J ClinPeriodontol 1991; 8: 1 17-1 25.
41. Haffajee AD, Socransky SS, Smith C, Dibart S. Microbial risk
in-dicators for periodontal attachment loss. J Periodont Res
1991;26:292-296.
42. Hillman JD, Socransky SS, Shivers M. The relationships
betweenstreptococcal species and periodontopathic bacteria in human
dentalplaque. Arch Oral Biol 1985;30:791-795.
43. Hillman JD, Socransky SS. The theory and application of
bacterialinterference to oral diseases. In: Myers HM, ed. New
Biotechnologyin Oral Research. Basel: Karger; 1989: 1-17.
44. Loesche WJ. Chemotherapy of dental plaque infections. Oral
Sci Rev1976;9:65-107.
45. Brenner DJ, Mayer LW, Carlone GM, et al. Biochemical,
genetic,and epidemiologic characterization of Haemophilus
influenzae bio-group aegyptius (Haemophilus aegyptius) strains
associated with Bra-zilian purpuric fever. J Clin Microbiol
1988;26:1524-1534.
-
7/27/2019 Senador @JoseRafaelS deposit proyecto de ley que
declara el da 25 de septiembre de cada ao como "Da de l
10/10
Volume 63Number 4 SOCRANSKY, AFFAJEE 3346. Musser JM, K roll JS,
Moxon ER, Selander RK. Evolutionary geneticsof the encapsulated
strains of Haemo philus influenzae. Proc Natl Acad
Sci (USA) 1988;85:7758-7762.47. Finlay BB, Falkow S. Common
themes in microbial pathogenicity.Microbiol Rev 1989;53:210-230.48.
Eisenstein BI. New molecular techniques for microbial
epidemiologyand the diagno sis of infectious diseases. JInfect Dis
1990;161:595402.49. Preus HR, Olsen I, Namork E. Association
between bacteriophage-
infected Actinobacillus actinomycetemcomitans and rapid
periodontaldestruction.J Clin Periodontol 1987;14:245-247.50. Preus
HR, Olsen I, Namork E. The presence of phage-infected
Ac-tinobacillus actinomycetemcomitans in localized juvenile p
eriodon titispatients. J Clin Periodontol 1987;14:605409.
51. Guiney DG, Bouic K. Detection of conjug al transfer systems
in oral,black-pigmented Bacteroides spp. J Bactenol
1990;172:495497.
52. Maurelli AT. T emp erature regulation of virulence genes in
pathog enicbacteria: a general strategy for human pathogens?
Microbial Patho-genesis 1989; 7:l-10.53. Miller JF, Mek alanos JJ,
Falkow SF . Coordina te regulation and sen-sory transduction in the
control of bacterial virulence. Science
1989;243:91&922.
54. McKee AS, McDermid AS, Baskewille A, Dowsett AB, EllwooDC.
Effect of hemin on the physiology and virulence of
Bacteroidegingivalis W50. Infect Immun 1986;52:349-355.
55. Barua PK, Dyer DW , Neiders ME. Effect of iron limitation on
Bacteroides [email protected]. Oral Microb iol Immu nol 1990;5:263-268.56.
Bramanti TE, Holt SC. Iron-regulated outer membrane proteins in
thperiodontopathic bacterium, Bacteroides gingivalis. Biochem
BiophyRes Comm 1990;166: 1146-1 154.
57. Haffajee AD, S ocransky SS, G oodson JM. S ubgingival
temperaturI Relation to baseline clinical parameters. J Clin
Periodonto1992;19:00-00.
58. Haffajee AD, S ocransky SS, Goodson JM. Su bgingival
temperaturI1 Relation to future periodontal attachment loss. J Clin
Pt:riodonto1992; in press.59. Haffajee AD, Socransky SS, Smith C,
Dibart S, Goodson JM
Subgingival temperature. 111 Relation to micro bial co unt s. J
Clin Periodontol 1992; in press.
Send reprint requests to: Dr. S.S. Socransky, Forsyth Dental
Cente140 The Fenway, Boston, MA 02115.