Embed Size (px)
Citation preview

Seminar in Palliative CareSeptember 26 – October 02, 2010
Salzburg, Austria
in Collaboration with
The EPEC-O Curriculum is produced by the EPECTM Project with major funding provided by NCI, with supplemental funding provided by the Lance Armstrong Foundation.
Education in Palliative and End-of-life Care - Oncology
The
ProjectEPEC-O
TM
DeliriumDelirium
Frank D. Ferris, Frank D. Ferris, MD, FAAHPMMD, FAAHPM
Institute for Palliative MedicineInstitute for Palliative Medicineat San Diego Hospiceat San Diego Hospice
University of California San DiegoUniversity of California San Diego
University of TorontoUniversity of Toronto
Scott A. Irwin, MD, PhDDirector, Psychiatry Programs
Rosene D. Pirrello, RPhDirector, Pharmacy
Jeremy M. Hirst, MDAssistant Director, Psychiatry
Gary T. Buckholz, MDDirector, Fellowship Program
Frank D. ferris, MD, FAAHPMDirector, International Programs © 2010
The Butcher, Baker, and Candlestick Maker The Butcher, Baker, and Candlestick Maker Return: Interdisciplinary Goal-Based Return: Interdisciplinary Goal-Based
Approaches to DeliriumApproaches to DeliriumRecognition, Work-Up, and ManagementRecognition, Work-Up, and Management
Key Topics…Key Topics…
Definition
Prevalence &consequences
Many causes
Under recognition
Assessment Common language
History & exam
Tools
Differential diagnoses
Goals of care
Diagnostic workup
……Key TopicsKey Topics
Management
Non–pharmacological
Pharmacological
Reversible
Irreversible
Terminal
Delirium Is... Delirium Is...
Change in mental status, impaired Attention
Orientation
Cognition
Consciousness
Reality
Behavior
American Psychiatric Association. (2000) Diagnostic and statistical manual of mental disorders. 943
. . . Delirium Is. . . Delirium Is
Develops quickly
May fluctuate
Underlying medical etiology
NOT dementia
American Psychiatric Association. (2000) Diagnostic and statistical manual of mental disorders. 943.
Associated changesAssociated changes
Day-night reversal
Emotional states
Non-specific neurological abnormalities
Decline in functional ability
TypesTypes
Hyperactive
Associated behavioral disturbances
Hallucinations
Delusional beliefs
Hypoactive
Quiet
Mistaken for depression or fatigue
Mixed – waxing and waning
Delirium is Highly Prevalent Delirium is Highly Prevalent and has and has
Serious Consequences… Serious Consequences…
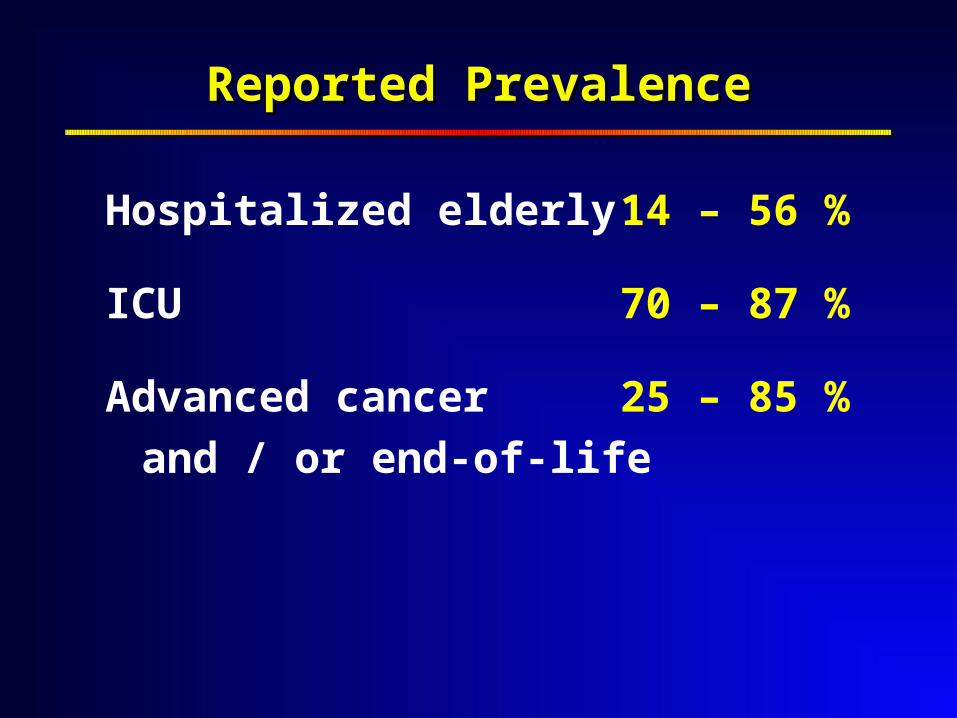
Reported PrevalenceReported Prevalence
Hospitalized elderly 14 – 56 %
ICU 70 – 87 %
Advanced cancer 25 – 85 %
and / or end-of-life
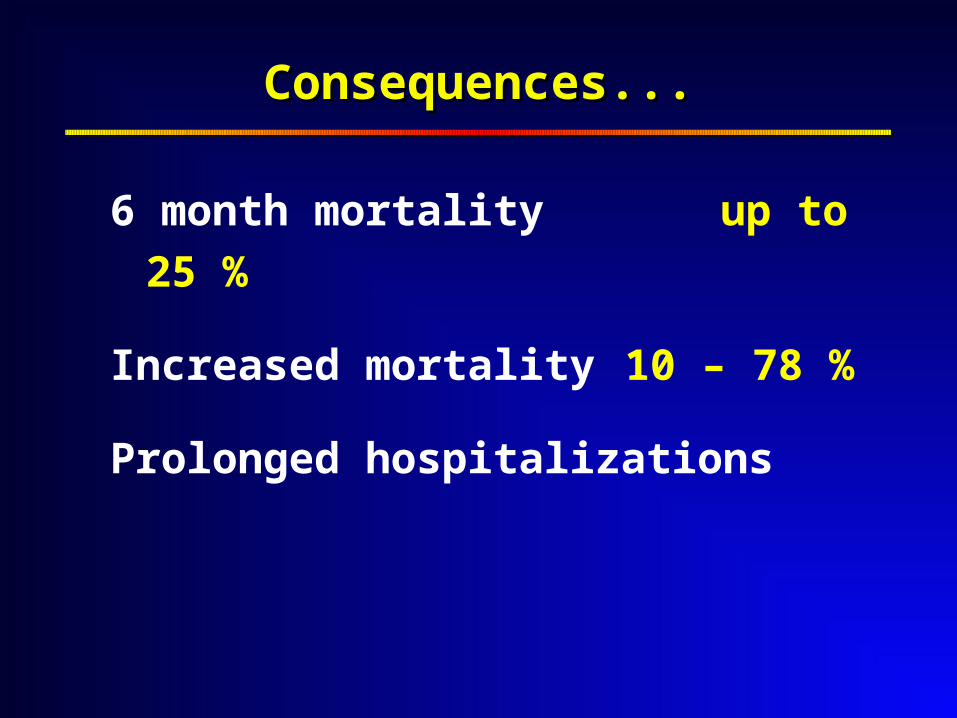
Consequences...Consequences...
6 month mortality up to 25 %
Increased mortality 10 – 78 %
Prolonged hospitalizations
……Consequences...Consequences...
Stress, discomfort,
reduced quality of life
Patients, nurses, family members
Even if hypoactive
Namba M, et al. (2007) Palliat Med 21: 587
Morita T, et al. (2007) J Pain Symptom Manage 34: 579
Cohen, MZ, et al. (2009) J Palliat Care 25:164
Bruera, E, et al. (2009) Cancer 15:2004
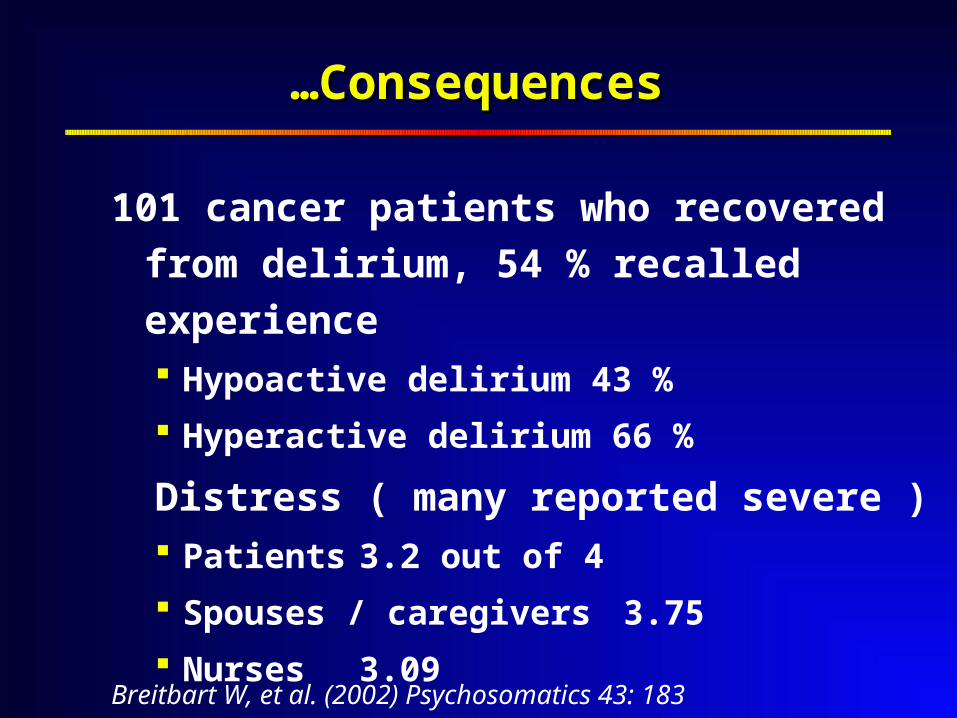
101 cancer patients who recovered from
delirium, 54 % recalled experience Hypoactive delirium 43 %
Hyperactive delirium 66 %
Distress ( many reported severe ) Patients 3.2 out of 4
Spouses / caregivers 3.75
Nurses 3.09
……ConsequencesConsequences
Breitbart W, et al. (2002) Psychosomatics 43: 183
Video – Hypoactive DeliriumVideo – Hypoactive Delirium
Key pointsKey points
1. Pathophysiology
2. Assessment
3. Management
Delirium has Delirium has Many, Many Causes…Many, Many Causes…
Many are Discoverable Many are Discoverable and Reversible…and Reversible…
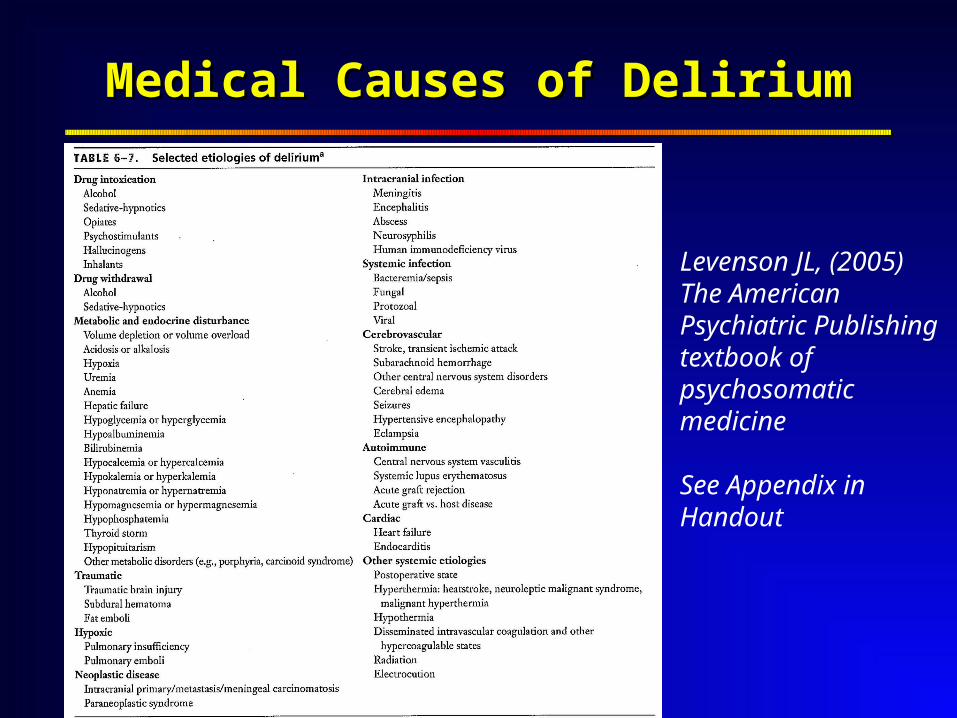
Medical Causes of DeliriumMedical Causes of Delirium
Levenson JL, (2005) The American Psychiatric Publishing textbook of psychosomatic medicine
See Appendix in Handout
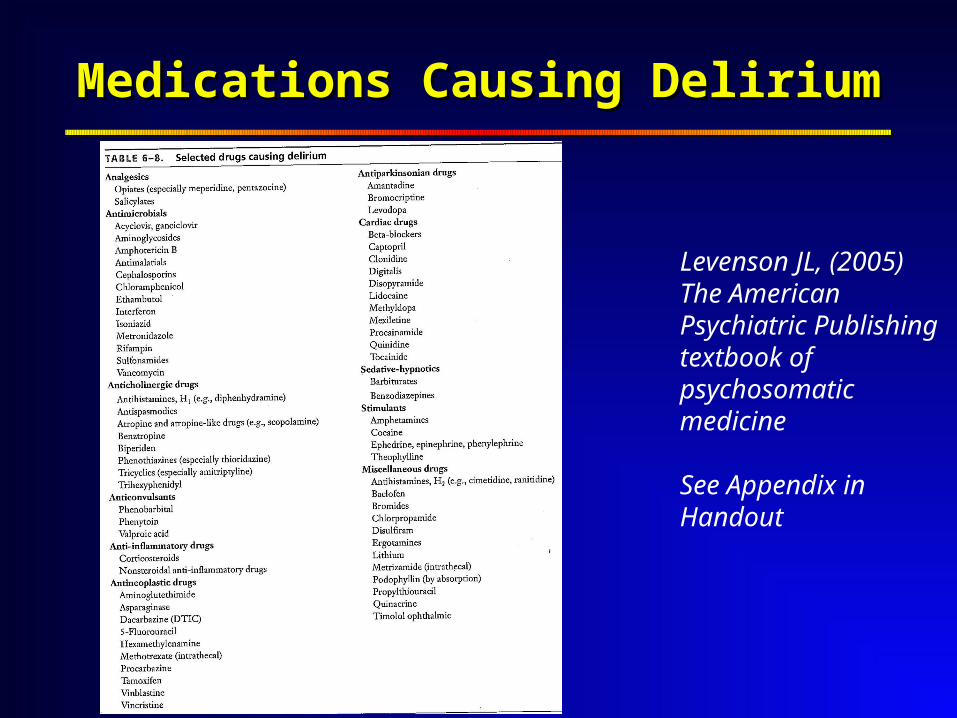
Medications Causing DeliriumMedications Causing Delirium
Levenson JL, (2005) The American Psychiatric Publishing textbook of psychosomatic medicine
See Appendix in Handout
Most Common Causes…Most Common Causes…
Fluid imbalance
Infections
Hepatic / renalfailure
Hypoxia
Hematological disturbance
Medications Anticholinergics Benzodiazepines Opioids Steroids
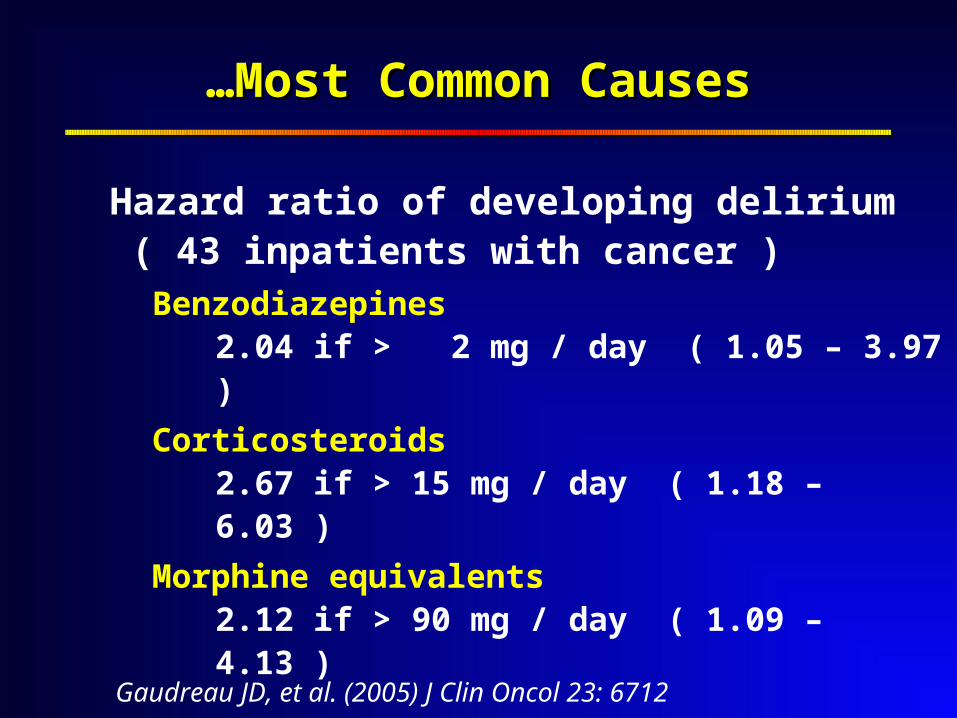
……Most Common CausesMost Common Causes
Hazard ratio of developing delirium( 43 inpatients with cancer )
Benzodiazepines 2.04 if > 2 mg / day ( 1.05 – 3.97 )
Corticosteroids 2.67 if > 15 mg / day ( 1.18 – 6.03 )
Morphine equivalents2.12 if > 90 mg / day ( 1.09 – 4.13 )
Gaudreau JD, et al. (2005) J Clin Oncol 23: 6712
Many Causes are Treatable...Many Causes are Treatable...
237 hospice inpatients with cancer 213 ( 90 % ) had 245 episodes of
delirium
Causes found in
93 of the 153 who had a workup
Multi-factorial in > 50 %
Complete remission in 20 %
Morita T, et al. (2001) J Pain Symptom Manage 22: 997
……Many Causes are TreatableMany Causes are Treatable
104 inpatients with advanced cancer
receiving palliative care 71 had 94 episodes of delirium
Reversible in 50 %
Lawlor PG, et al. (2000) Arch Intern Med 160: 786
Delirium is Delirium is Under–Recognized… Under–Recognized…
Often UnderOften Under––Recognized...Recognized...
2716 hospice patients
Delirium recognized in only
17.8 % of home care patients
28.3 % of inpatients
Irwin SA, et al. (2008) Palliative and Supportive Care 6: 159
……Often UnderOften Under––RecognizedRecognized
107 end-stage cancer inpatients
Delirium recognition rate : 44.9 %
20.5 % of hypoactive cases
Fang CK, et al. (2008) Jpn J Clin Oncol 38: 56
Complex presentation
Inconsistent language
Hypoactive sub-type
Thought to be normal part
of end-of-life
Why UnderWhy Under––Recognized ? Recognized ?
Careful Assessment & Careful Assessment & Communication of Findings Communication of Findings
is Key to Successful is Key to Successful Management of Delirium…Management of Delirium…
Common Language Common Language is Essential…is Essential…
AssessmentAssessment
Clinical history, physical examination, observations over time
Mental status exam
Review of medication use
Thorough medical and laboratory work-up to elucidate underlying cause
HistoryHistory
Context of the patient
Symptoms
Quality
Severity
Temporal profile
Effect of treatments
Assessment Tools…Assessment Tools…
“ Gold Standard ”
Experienced clinician
DSM-IV criteria
Three types of standardized tools
1. Screening
2. Diagnosis
3. Symptom severity
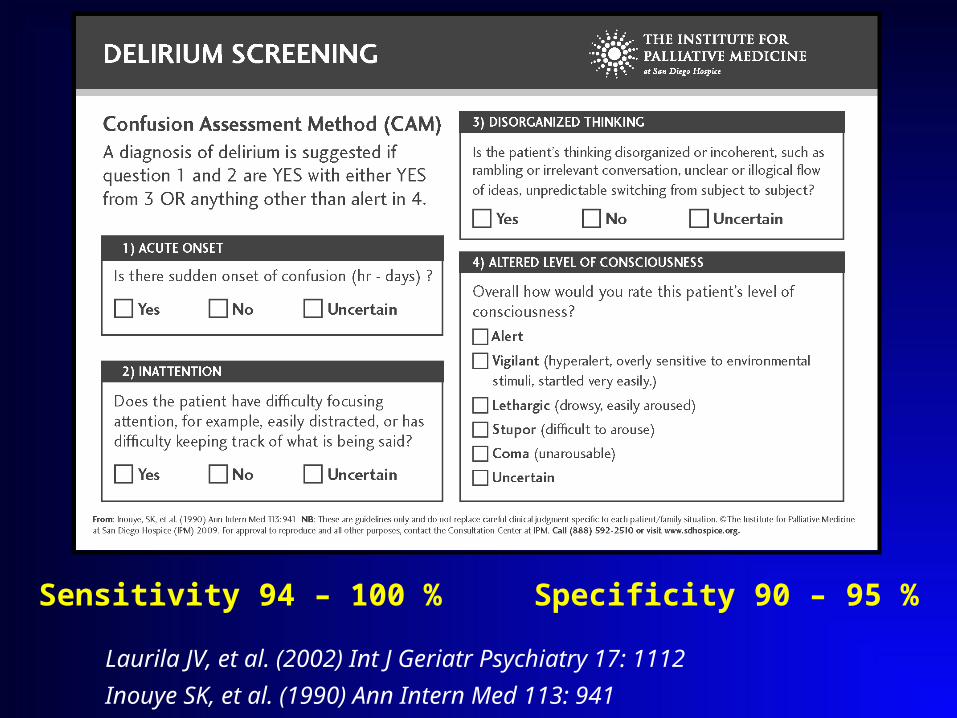
Sensitivity 94 – 100 % Specificity 90 – 95 %
Laurila JV, et al. (2002) Int J Geriatr Psychiatry 17: 1112
Inouye SK, et al. (1990) Ann Intern Med 113: 941
Differential DiagnosesDifferential Diagnosesto Consider…to Consider…
American Psychiatric Association. (2000) Diagnostic and statistical manual of mental disorders. 943
Differentiate Delirium FromDifferentiate Delirium From
Dementia
Depression
Anxiety
Akathisia
Psychotic disorders
Personality disorders
Developmental disorders
DementiaDementia
Slow decline in brain function Slow decline in brain function
> expected with normal aging> expected with normal aging
May have May have
Problems with memory, attention, Problems with memory, attention,
language, emotions, & problem solvinglanguage, emotions, & problem solving
Confusion, hallucinations, delusionsConfusion, hallucinations, delusions
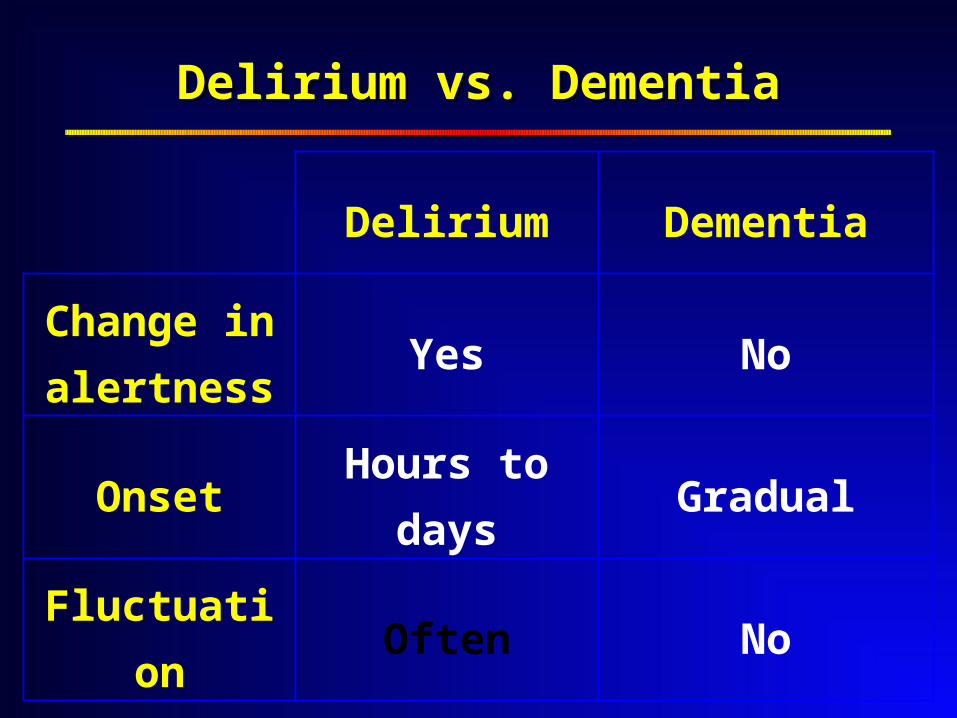
Delirium vs. DementiaDelirium vs. Dementia
Delirium Dementia
Change in
alertnessYes No
OnsetHours to
daysGradual
Fluctuatio
nOften No
DepressionDepression
Symptom, episode, recurrent disorderSymptom, episode, recurrent disorder
Major depression Major depression
Several symptomsSeveral symptoms
> 2 weeks duration> 2 weeks duration
Impaired functionImpaired function
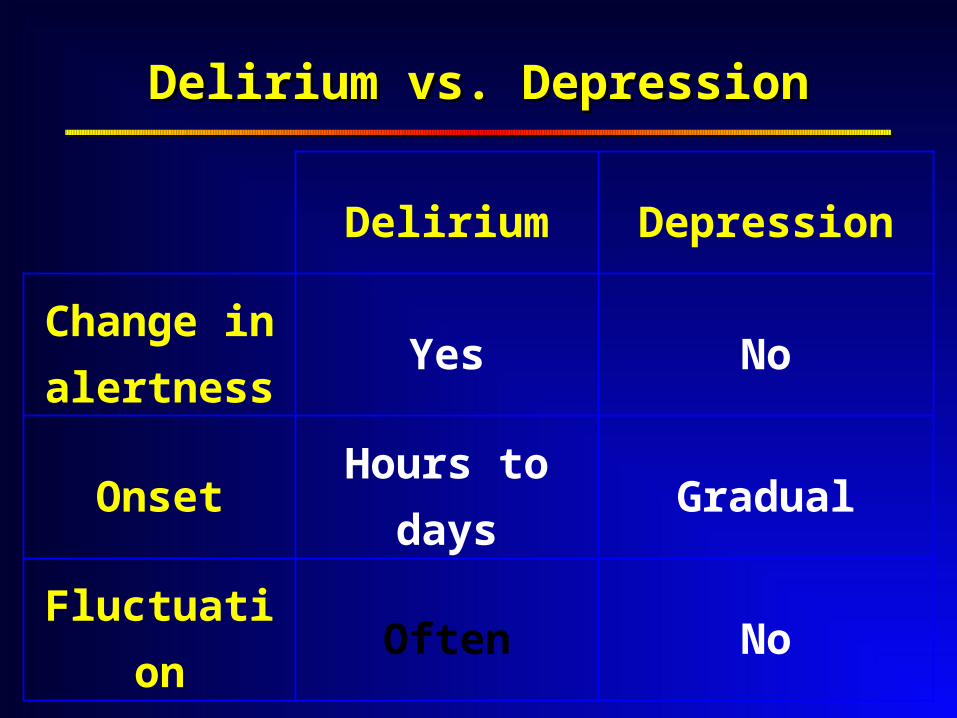
Delirium vs. DepressionDelirium vs. Depression
Delirium Depression
Change in
alertnessYes No
OnsetHours to
daysGradual
Fluctuatio
nOften No
Potential Reversibility Potential Reversibility of Delirium of Delirium
Guides Work-up & Guides Work-up & Management…Management…
Potential Reversibility of DeliriumPotential Reversibility of Delirium
Potentially ReversiblePotentially Reversible
IrreversibleIrreversible
Patient is dying ( terminal delirium )Patient is dying ( terminal delirium )
Goals of careGoals of care
Work–up / reversal unsuccessfulWork–up / reversal unsuccessful
Goals of CareGoals of Care
Initial patient & family goalsInitial patient & family goals
Goals can changeGoals can change
Goals after diagnosisGoals after diagnosis
Diagnostic work-up vs. palliateDiagnostic work-up vs. palliate
Goals after work-upGoals after work-up
Reverse vs. palliate vs. irreversibleReverse vs. palliate vs. irreversible
Diagnostic Work-up May IncludeDiagnostic Work-up May Include
Chemistry
Hematology
Endocrine
Vitamin levels
Cardiac
Infection
Toxicology
Imaging
DeliriumDelirium Management… Management…
Management Strategies…Management Strategies…
Ensure safetyEnsure safety
Address environmentAddress environment
Manage based on Manage based on
potential reversibility & goals of carepotential reversibility & goals of care
Adapted from APA Practice Guidelines 2004
American Psychiatric Association. (1999) Am J Psychiatry 156: 1Cook IA. (2004) Available online at: http://wwwpsychorg/psych_pract/treatg/pg/prac_guidecfm
……Management Strategies…Management Strategies…
ReverseReverse
Treat underlying causesTreat underlying causes
RelieveRelieve
Non-pharmacologicalNon-pharmacological
PharmacologicalPharmacological
Consult psychiatryConsult psychiatry
……Management StrategiesManagement Strategies
TreatmentTreatment
BenefitsBenefits
RisksRisks
BurdensBurdens
Time-limited therapeutic trialsTime-limited therapeutic trials

Always Use Always Use Non-pharmacological Non-pharmacological
Treatments…Treatments…
Non-Pharmacological Non-Pharmacological Treatments Can AddressTreatments Can Address
Disordered thinkingDisordered thinking
DisorientationDisorientation
Sleep Sleep
disturbancedisturbance
ImmobilityImmobility
Risk of falls / injuryRisk of falls / injury
Sensory deprivationSensory deprivation
DehydrationDehydration
Environmental factorsEnvironmental factors
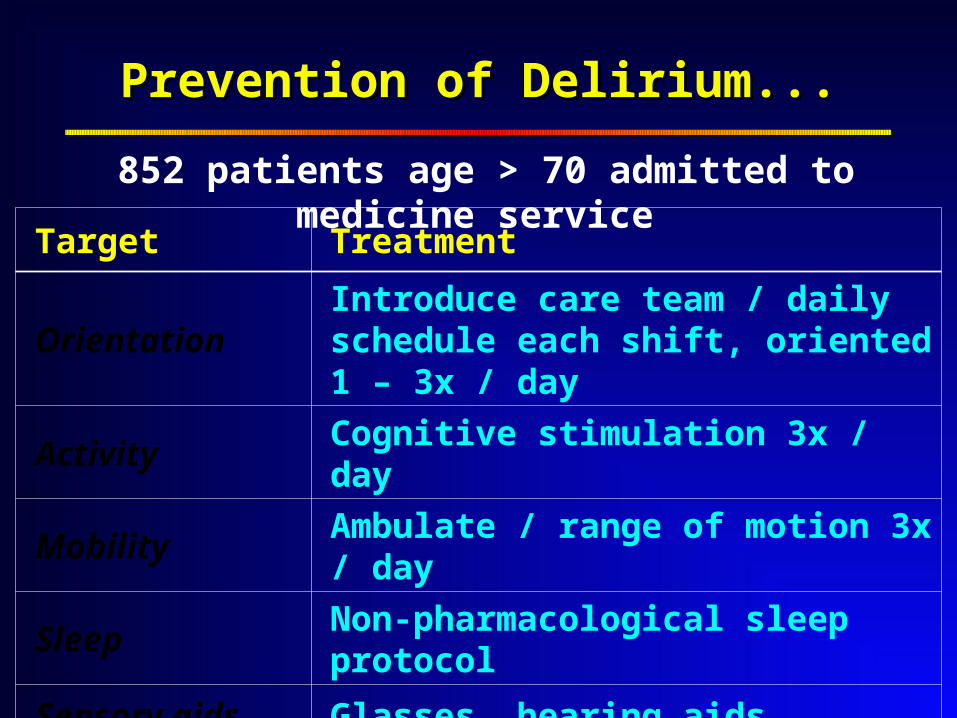
Prevention of Delirium...Prevention of Delirium...
Target Treatment
OrientationIntroduce care team / daily schedule each shift, oriented 1 – 3x / day
Activity Cognitive stimulation 3x / day
Mobility Ambulate / range of motion 3x / day
Sleep Non-pharmacological sleep protocol
Sensory aids Glasses, hearing aids
Dehydration Rehydrate as needed
852 patients age > 70 admitted to medicine service
……Prevention of DeliriumPrevention of Delirium
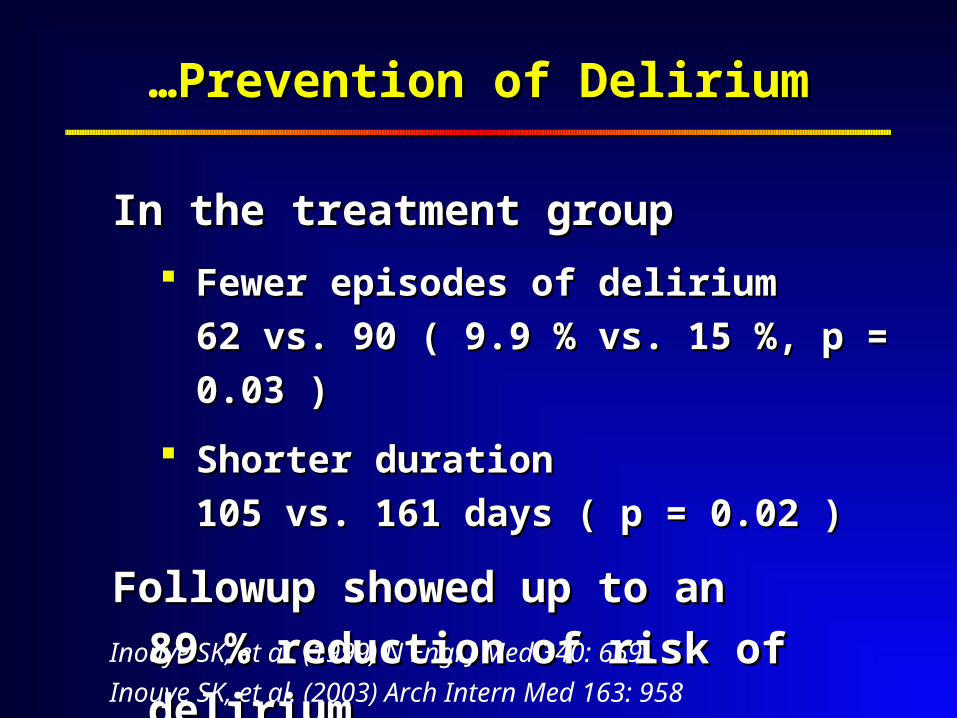
In the treatment groupIn the treatment group
Fewer episodes of deliriumFewer episodes of delirium
62 vs. 90 ( 9.9 % vs. 15 %, p = 0.03 )62 vs. 90 ( 9.9 % vs. 15 %, p = 0.03 )
Shorter duration Shorter duration
105 vs. 161 days ( p = 0.02 )105 vs. 161 days ( p = 0.02 )
Followup showed up to an Followup showed up to an
89 % reduction of risk of delirium89 % reduction of risk of deliriumInouye SK, et al. (1999) N Engl J Med 340: 669
Inouye SK, et al. (2003) Arch Intern Med 163: 958

Use Pharmacological Use Pharmacological Treatments when Treatments when
Appropriate…Appropriate…
& Appropriately…& Appropriately…
Pharmacological Management Pharmacological Management
No No medication is FDA approved for the medication is FDA approved for the
treatment of deliriumtreatment of delirium
NoNo published double-blind, randomized, published double-blind, randomized,
placebo controlled trialsplacebo controlled trials
NoNo consensus among oncologists, consensus among oncologists,
geriatricians, psychiatrists, or geriatricians, psychiatrists, or
palliative medicine specialistspalliative medicine specialists
Agar M, et al. (2008) Palliat Med 22: 633
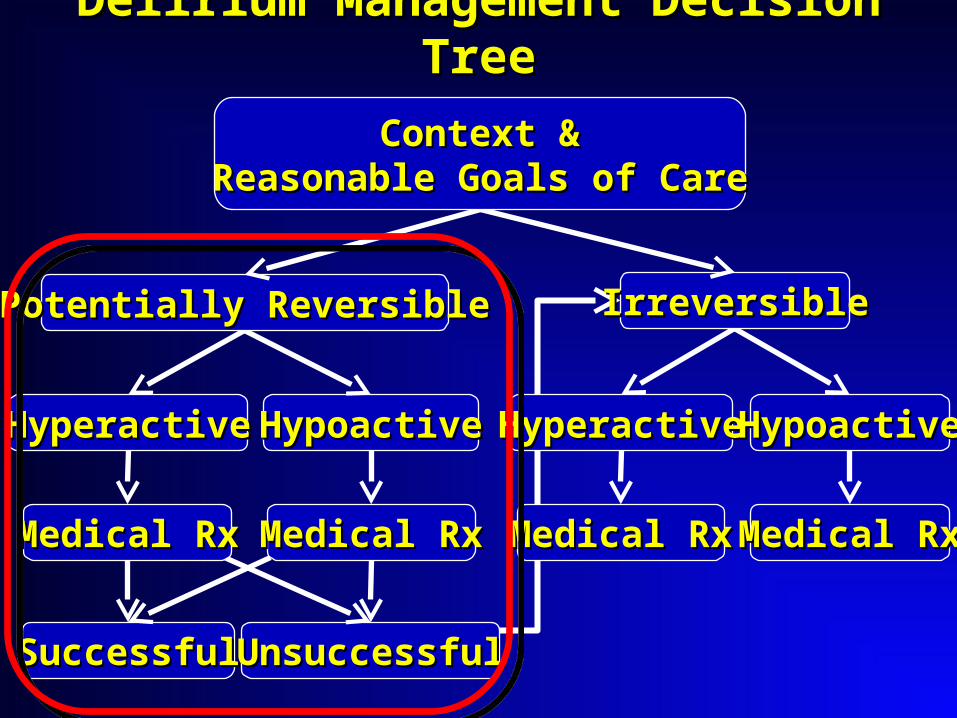
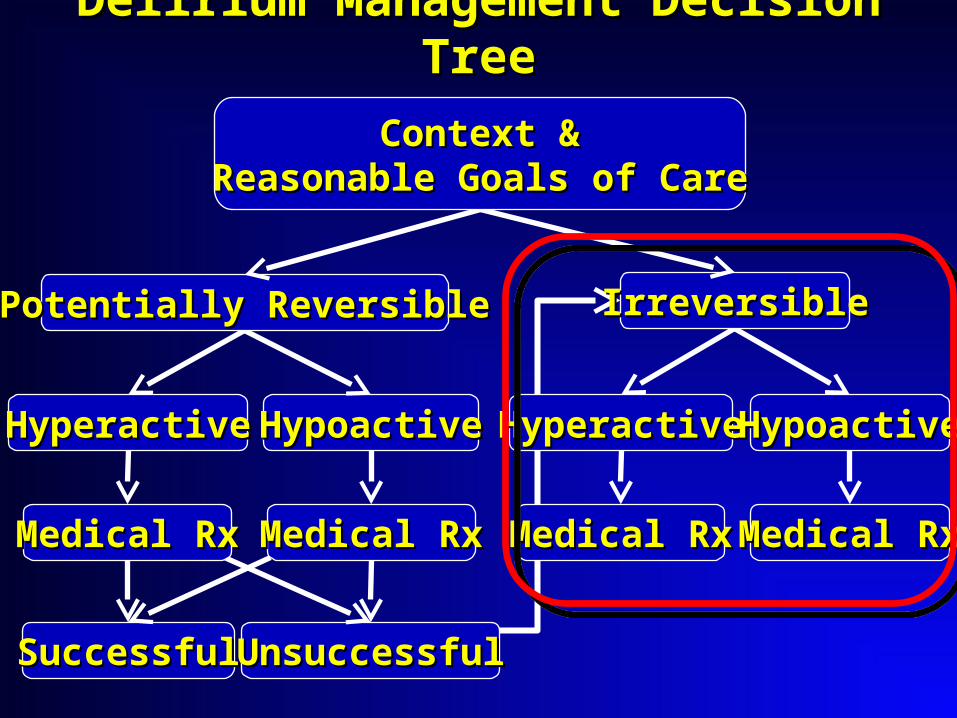
HyperactiveHyperactive HypoactiveHypoactive
SuccessfulSuccessful
HyperactiveHyperactive
Medical RxMedical Rx
HypoactiveHypoactive
Medical RxMedical Rx
UnsuccessfulUnsuccessful
Delirium Management Decision TreeDelirium Management Decision Tree
Medical RxMedical Rx Medical RxMedical Rx
Potentially ReversiblePotentially Reversible IrreversibleIrreversible
Context Context &&Reasonable Goals of CareReasonable Goals of Care
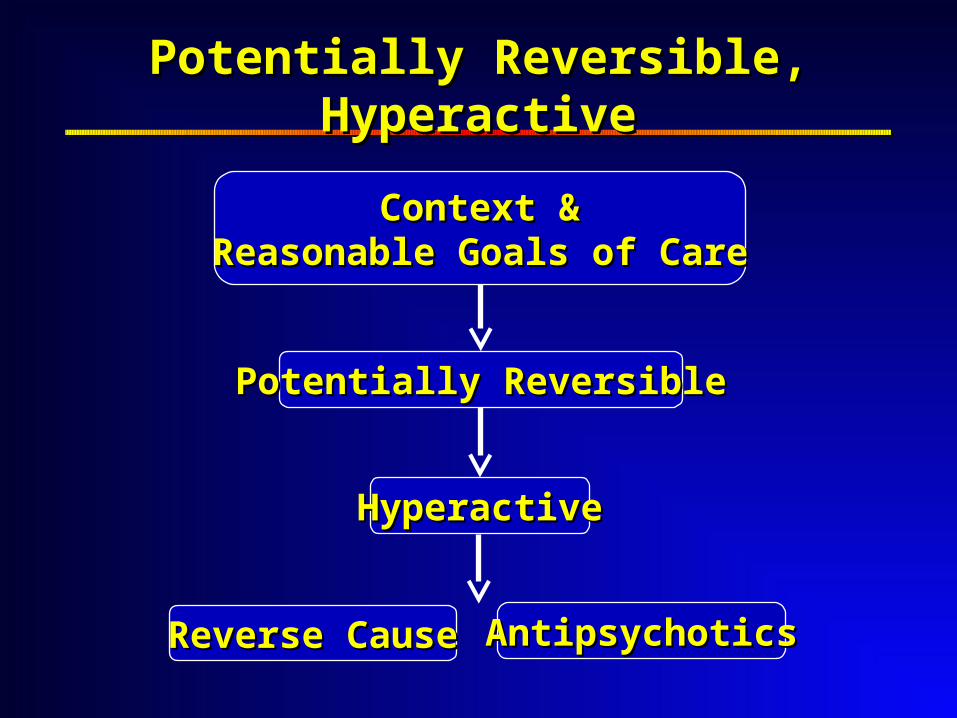
HyperactiveHyperactive
Potentially ReversiblePotentially Reversible
Potentially Reversible, HyperactivePotentially Reversible, Hyperactive
AntipsychoticsAntipsychoticsReverse CauseReverse Cause
Context Context &&Reasonable Goals of CareReasonable Goals of Care
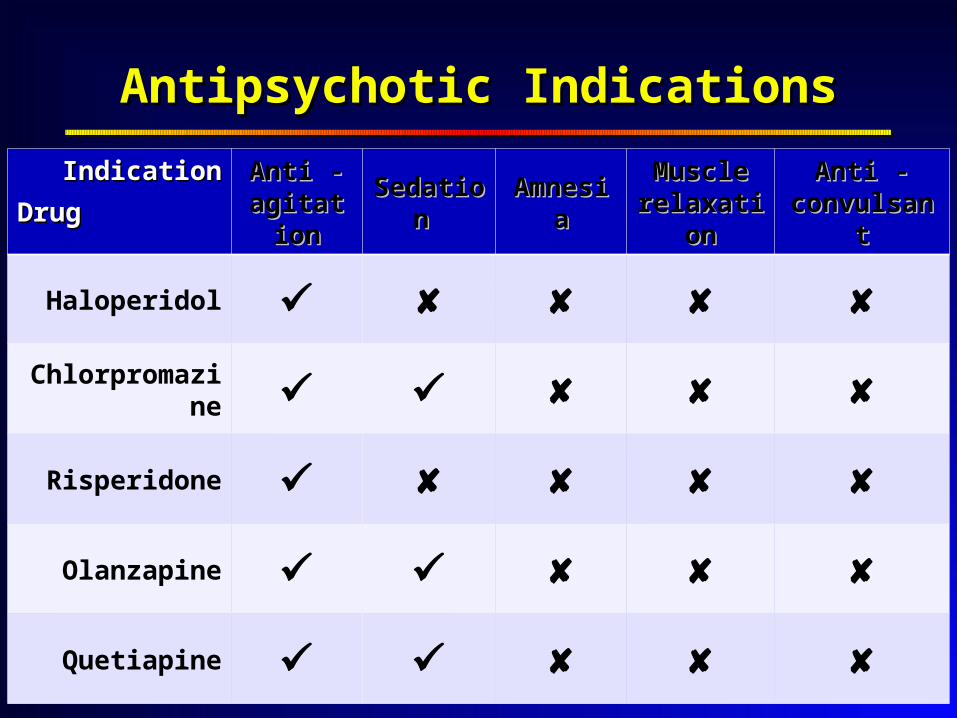
IndicationIndication
DrugDrugAnti - Anti -
agitationagitation Sedation Sedation AmnesiaAmnesia Muscle Muscle relaxationrelaxation
Anti - Anti - convulsantconvulsant
Haloperidol
Chlorpromazine
Risperidone
Olanzapine
Quetiapine
Antipsychotic IndicationsAntipsychotic Indications
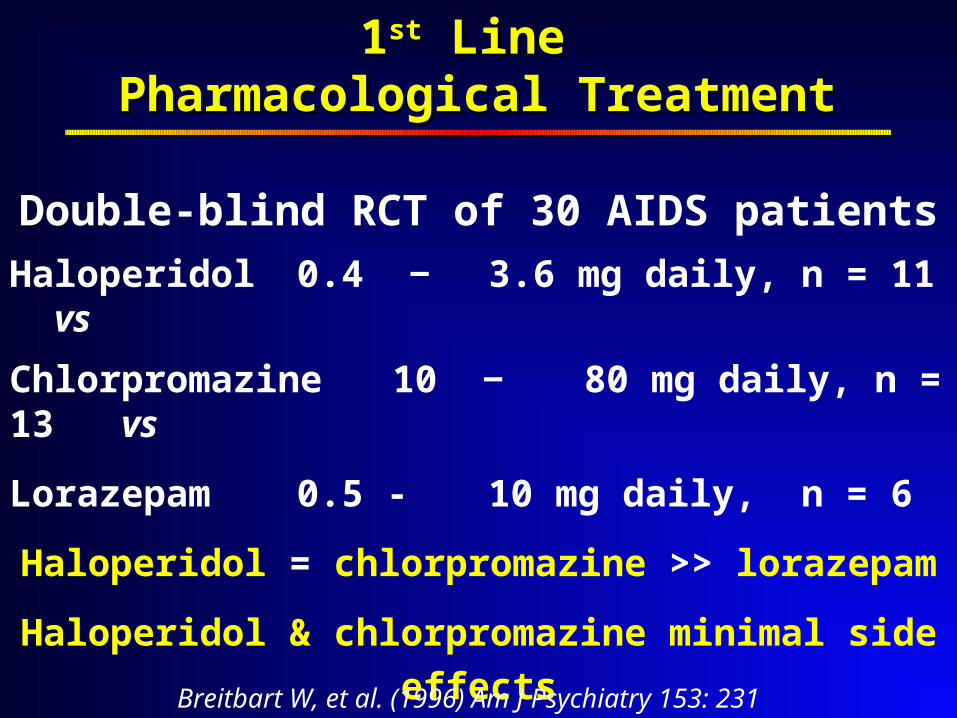
11stst Line Line Pharmacological TreatmentPharmacological Treatment
Double-blind RCT of 30 AIDS patients
Haloperidol 0.4 ‒ 3.6 mg daily, n = 11 vs
Chlorpromazine 10 ‒ 80 mg daily, n = 13 vs
Lorazepam 0.5 - 10 mg daily, n = 6
Haloperidol = chlorpromazine >> lorazepam
Haloperidol & chlorpromazine minimal side effects
Lorazepam stopped early due to adverse events
Breitbart W, et al. (1996) Am J Psychiatry 153: 231
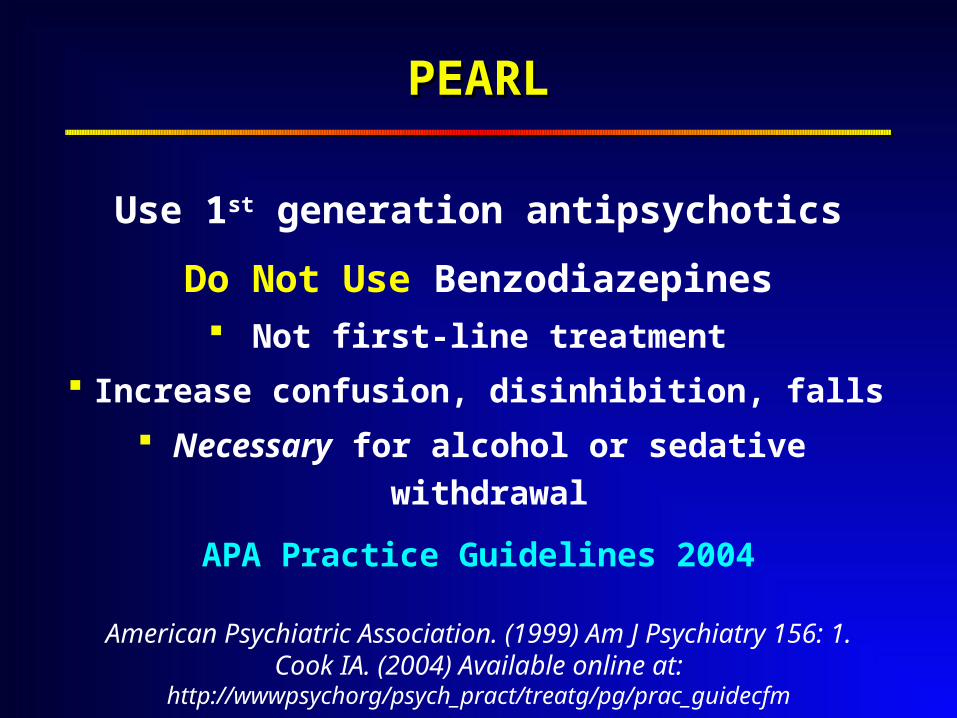
PEARLPEARL
Use 1st generation antipsychotics
Do Not Use Benzodiazepines Not first-line treatment
Increase confusion, disinhibition, falls
Necessary for alcohol or sedative withdrawal
APA Practice Guidelines 2004
American Psychiatric Association. (1999) Am J Psychiatry 156: 1.Cook IA. (2004) Available online at:
http://wwwpsychorg/psych_pract/treatg/pg/prac_guidecfm
Application of Application of Pharmacological Principles Pharmacological Principles
Improves Management…Improves Management…

Pla
sma
Co
nce
ntr
atio
n
0 Half-life ( t1/2 ) Time
PO / PR 60 min
SC / IM 30 min
Cmax
t1/2 24 hrs
Anti-psychotic Pharmacokinetic Guidelines
Cmax
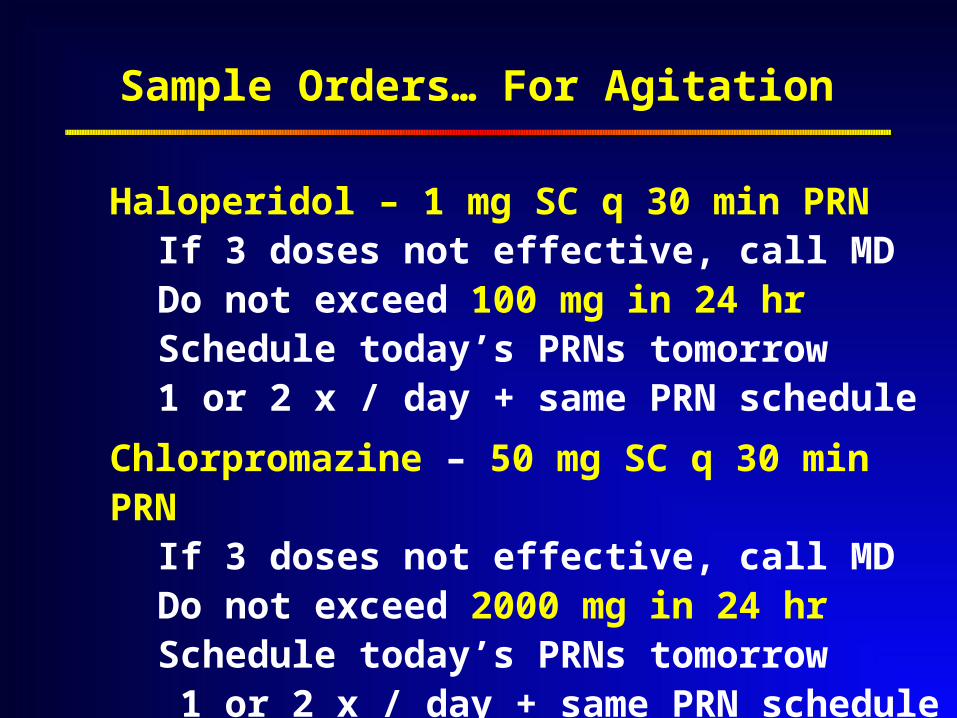
Sample Orders… For Agitation
Haloperidol – 1 mg SC q 30 min PRNIf 3 doses not effective, call MDDo not exceed 100 mg in 24 hrSchedule today’s PRNs tomorrow1 or 2 x / day + same PRN schedule
Chlorpromazine – 50 mg SC q 30 min PRNIf 3 doses not effective, call MDDo not exceed 2000 mg in 24 hrSchedule today’s PRNs tomorrow 1 or 2 x / day + same PRN schedule
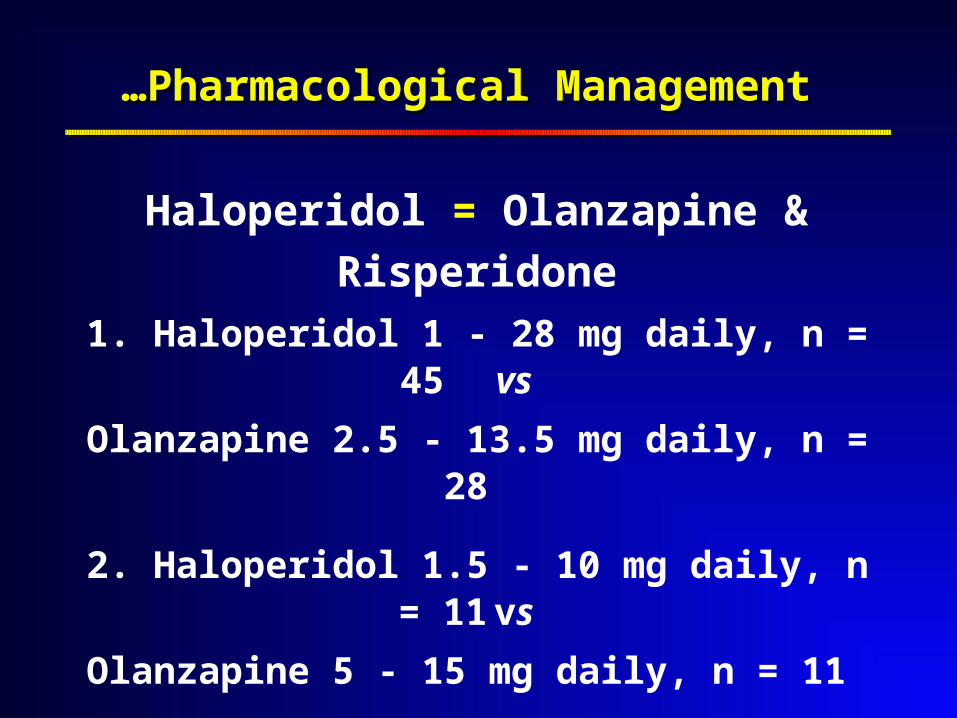
……Pharmacological Management Pharmacological Management
Haloperidol = Olanzapine & Risperidone
1. Haloperidol 1 - 28 mg daily, n = 45 vs
Olanzapine 2.5 - 13.5 mg daily, n = 28
2. Haloperidol 1.5 - 10 mg daily, n = 11 vs
Olanzapine 5 - 15 mg daily, n = 11
3. Haloperidol 1 - 3 mg daily, n = 12 vs
Risperidone 0.5 - 2 mg daily, n = 12
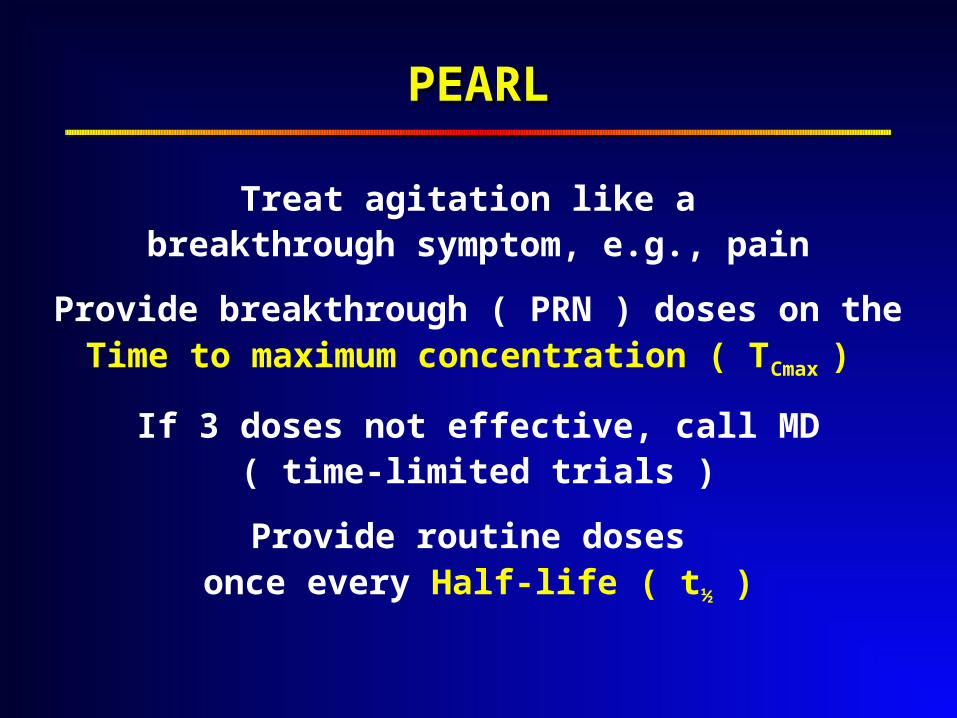
PEARLPEARL
Treat agitation like a breakthrough symptom, e.g., pain
Provide breakthrough ( PRN ) doses on theTime to maximum concentration ( TCmax )
If 3 doses not effective, call MD( time-limited trials )
Provide routine doses once every Half-life ( t½ )
Management ofManagement ofSevere Agitation…Severe Agitation…
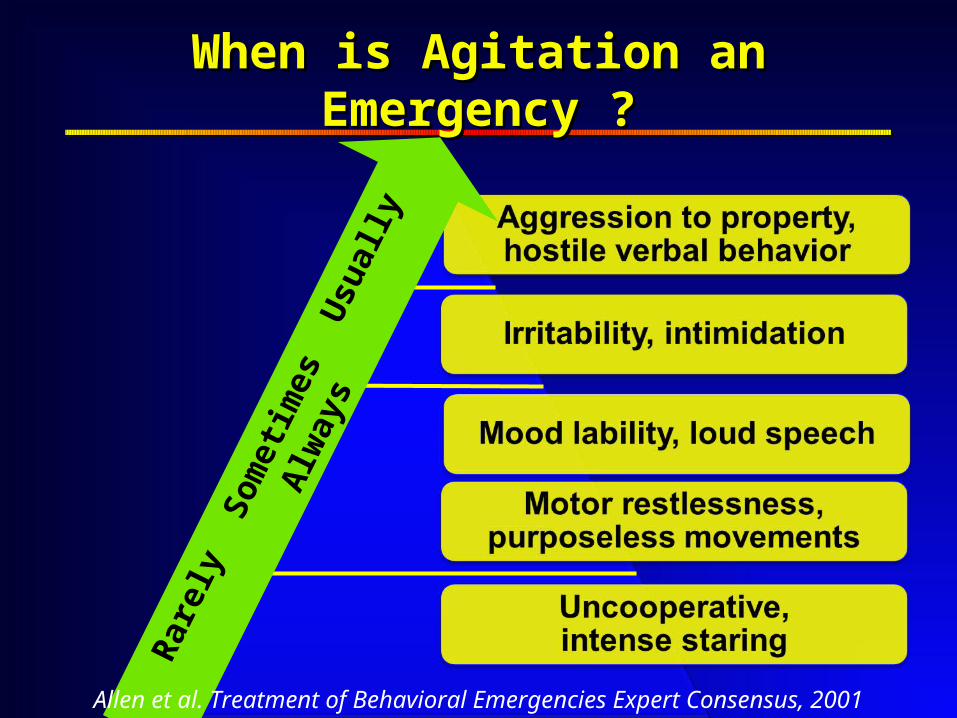
When is Agitation an Emergency ?When is Agitation an Emergency ?
Rar
ely
Som
etim
es U
sual
ly A
lway
s
Allen et al. Treatment of Behavioral Emergencies Expert Consensus, 2001
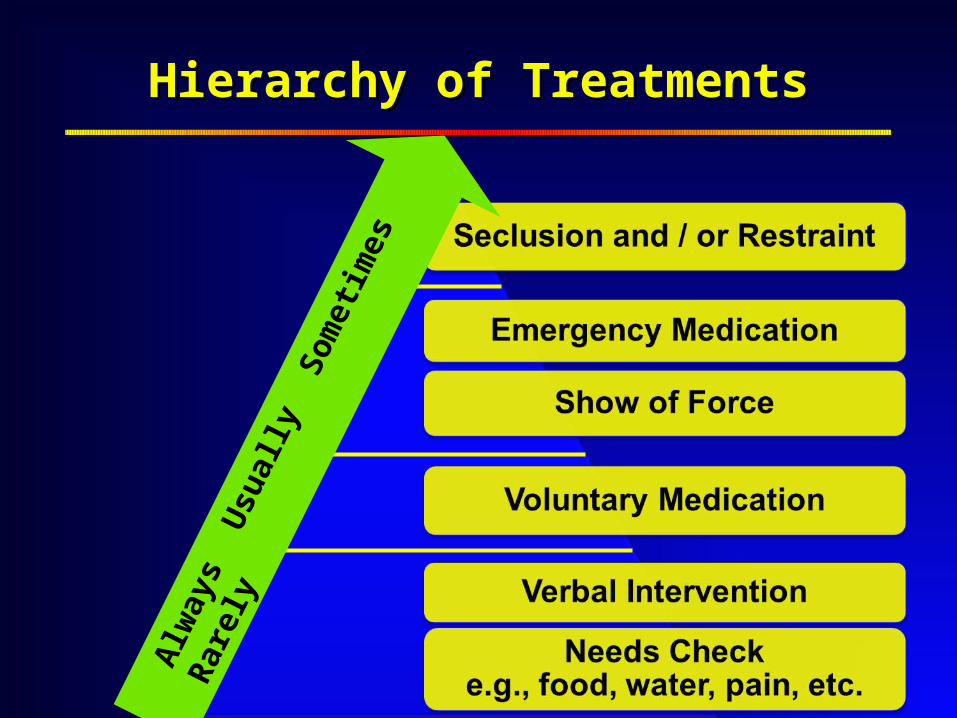
Hierarchy of TreatmentsHierarchy of Treatments
Alw
ays
Usu
ally
Som
etim
es R
arel
y
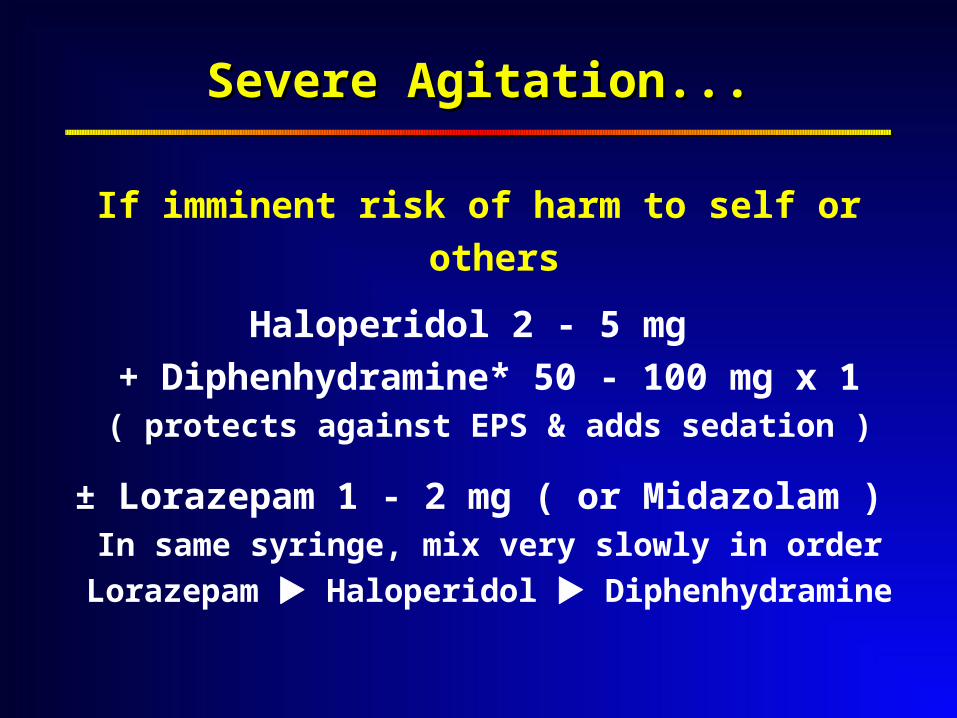
Severe Agitation...Severe Agitation...
If imminent risk of harm to self or others
Haloperidol 2 - 5 mg
+ Diphenhydramine* 50 - 100 mg x 1( protects against EPS & adds sedation )
± Lorazepam 1 - 2 mg ( or Midazolam )In same syringe, mix very slowly in order
Lorazepam Haloperidol Diphenhydramine
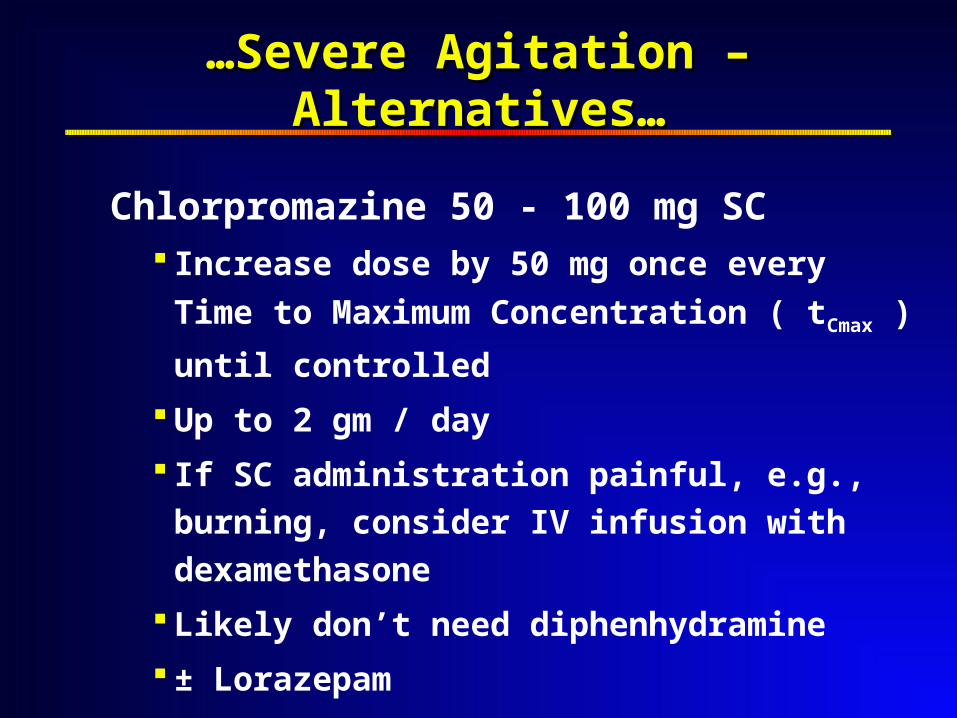
……Severe Agitation – Alternatives…Severe Agitation – Alternatives…
Chlorpromazine 50 - 100 mg SC Increase dose by 50 mg once every
Time to Maximum Concentration ( tCmax )
until controlled
Up to 2 gm / day
If SC administration painful, e.g., burning,
consider IV infusion with dexamethasone
Likely don’t need diphenhydramine
± Lorazepam
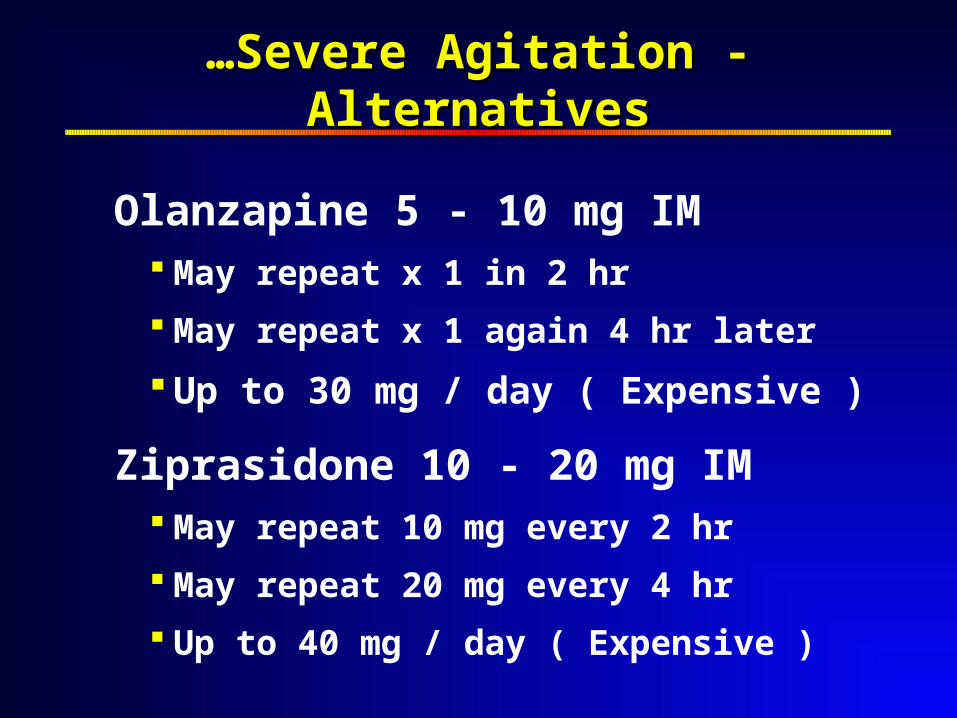
……Severe Agitation - AlternativesSevere Agitation - Alternatives
Olanzapine 5 - 10 mg IM May repeat x 1 in 2 hr
May repeat x 1 again 4 hr later
Up to 30 mg / day ( Expensive )
Ziprasidone 10 - 20 mg IM May repeat 10 mg every 2 hr
May repeat 20 mg every 4 hr
Up to 40 mg / day ( Expensive )
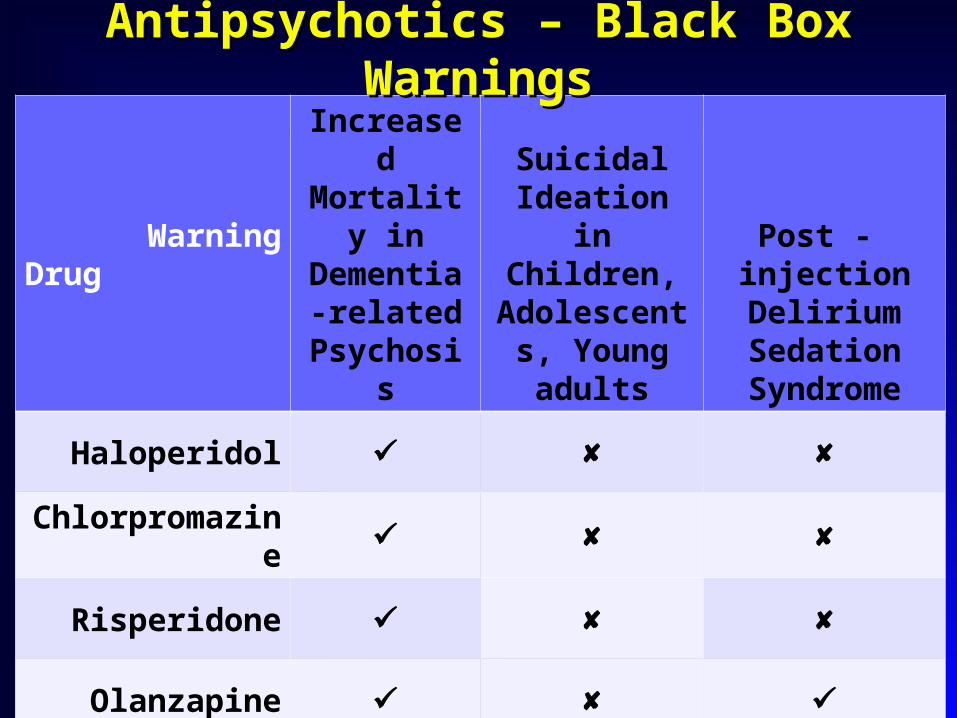
WarningDrug
Increased Mortality
in Dementia-
related Psychosis
Suicidal Ideation in Children,
Adolescents, Young adults
Post - injection Delirium Sedation
Syndrome
Haloperidol
Chlorpromazine
Risperidone
Olanzapine
Quetiapine
Antipsychotics – Black Box WarningsAntipsychotics – Black Box Warnings
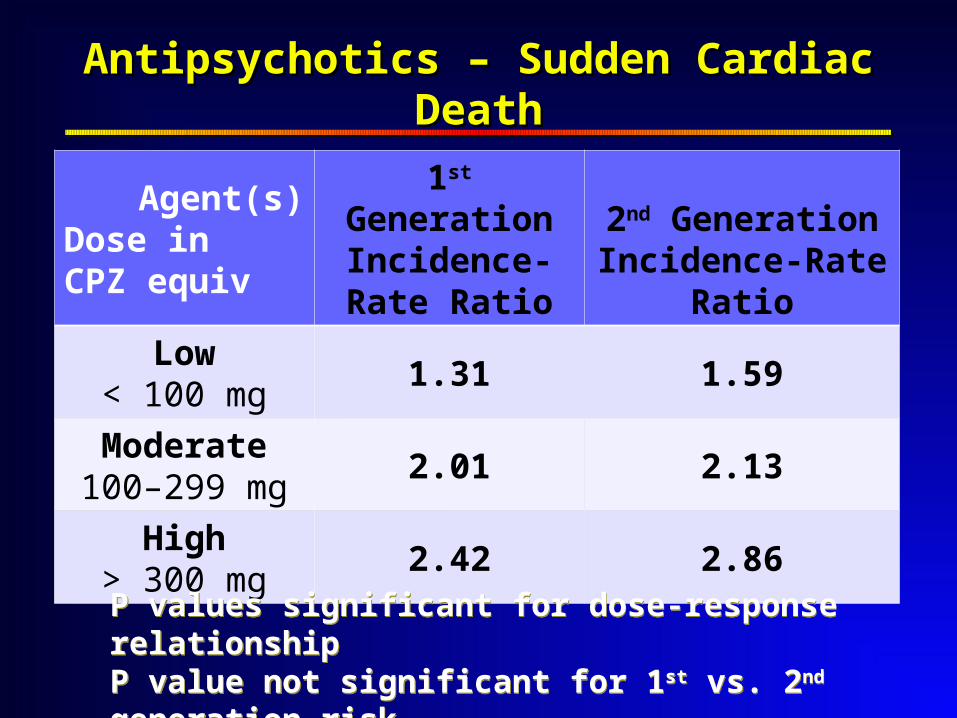
Agent(s)Dose in CPZ equiv
1st GenerationIncidence-Rate
Ratio
2nd GenerationIncidence-Rate
Ratio
Low< 100 mg
1.31 1.59
Moderate100–299 mg
2.01 2.13
High> 300 mg
2.42 2.86
Antipsychotics – Sudden Cardiac DeathAntipsychotics – Sudden Cardiac Death
P values significant for dose-response relationshipP value not significant for 1st vs. 2nd generation risk
NEJM 2009; 360 : 225 - 35
P values significant for dose-response relationshipP value not significant for 1st vs. 2nd generation risk
NEJM 2009; 360 : 225 - 35
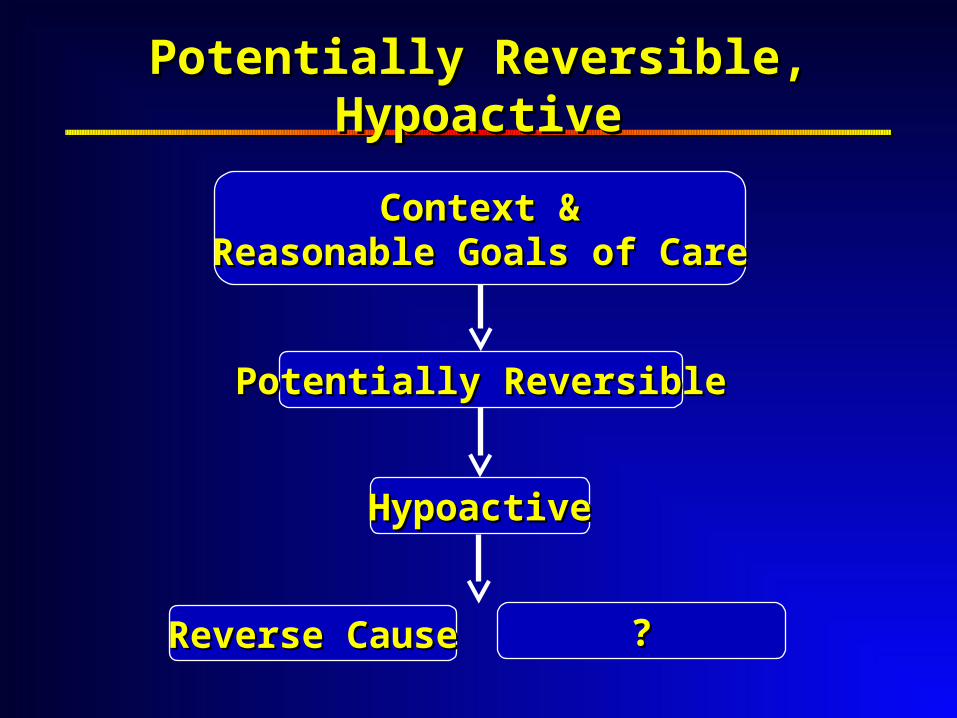
HypoactiveHypoactive
Potentially ReversiblePotentially Reversible
Potentially Reversible, HypoactivePotentially Reversible, Hypoactive
??Reverse CauseReverse Cause
Context Context &&Reasonable Goals of CareReasonable Goals of Care
HyperactiveHyperactive HypoactiveHypoactive
SuccessfulSuccessful
HyperactiveHyperactive
Medical RxMedical Rx
HypoactiveHypoactive
Medical RxMedical Rx
UnsuccessfulUnsuccessful
Delirium Management Decision TreeDelirium Management Decision Tree
Medical RxMedical Rx Medical RxMedical Rx
Potentially ReversiblePotentially Reversible IrreversibleIrreversible
Context Context &&Reasonable Goals of CareReasonable Goals of Care
Terminal DeliriumTerminal Delirium
Delirium during dying process
Prospective, irreversible
Altered level of consciousness
Tachycardia
Abnormal breathing patterns
Loss of swallow / gag
Oral / tracheal secretions
Loss of sphincter control
Oliguria / anuria
Cyanosis
Peripheral cooling
Venous pooling / mottling
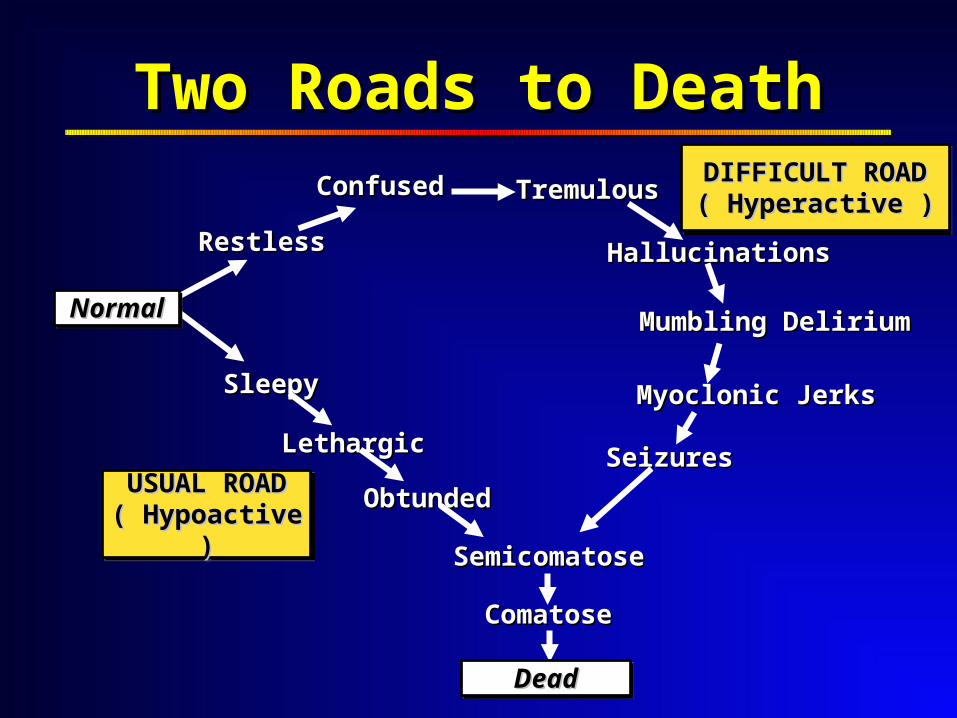
Two Roads to DeathTwo Roads to Death
RestlessRestless
ConfusedConfused TremulousTremulous
HallucinationsHallucinations
Mumbling DeliriumMumbling Delirium
Myoclonic JerksMyoclonic JerksSleepySleepy
LethargicLethargic
ObtundedObtunded
SemicomatoseSemicomatose
ComatoseComatose
SeizuresSeizures
USUAL ROADUSUAL ROAD( Hypoactive )( Hypoactive )USUAL ROADUSUAL ROAD( Hypoactive )( Hypoactive )
DIFFICULT ROADDIFFICULT ROAD( Hyperactive )( Hyperactive )
DIFFICULT ROADDIFFICULT ROAD( Hyperactive )( Hyperactive )
NormalNormalNormalNormal
DeadDeadDeadDead
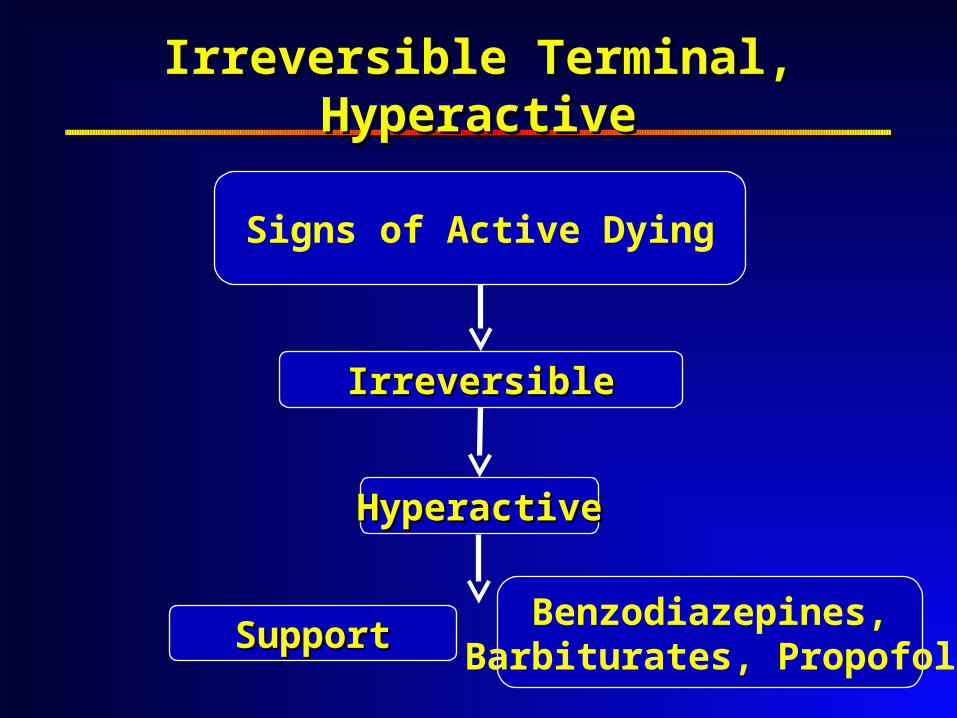
HyperactiveHyperactive
IrreversibleIrreversible
Irreversible Terminal, HyperactiveIrreversible Terminal, Hyperactive
Benzodiazepines,Barbiturates, PropofolSupportSupport
Signs of Active Dying
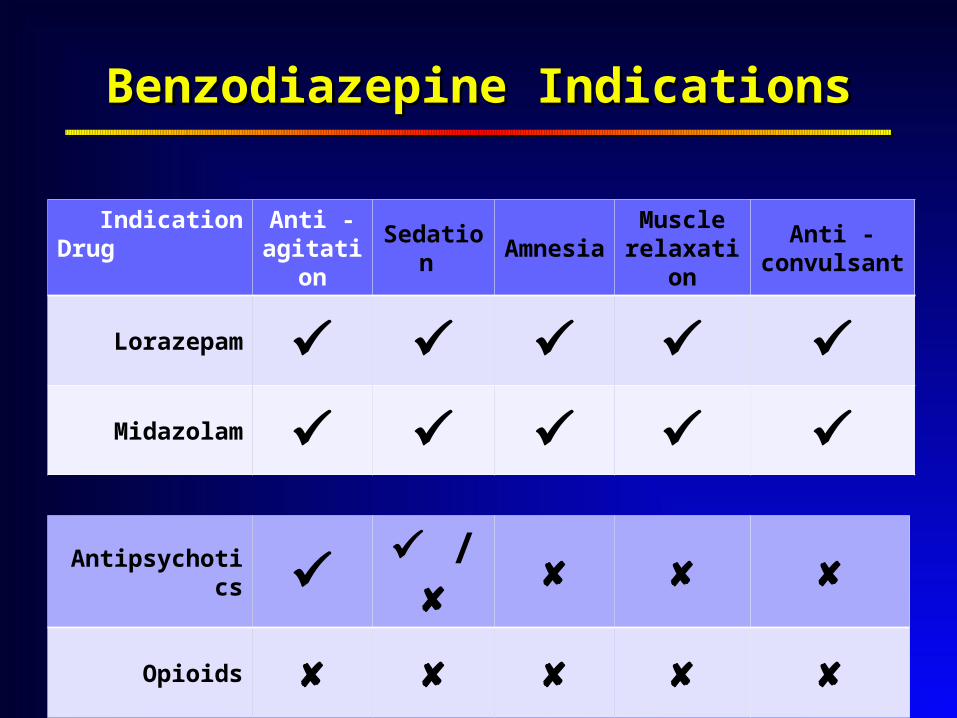
IndicationDrug
Anti - agitation
Sedation AmnesiaMuscle
relaxationAnti -
convulsant
Lorazepam Midazolam
Benzodiazepine IndicationsBenzodiazepine Indications
Antipsychotics /
Opioids
Sample Orders to Control Agitation…
Lorazepam PO / Buccal Mucosa
Starting dose = 1 mg PO / Buccal q 1 h PRN
If 3 doses not effective, call MD
Up to 40 mg in 24 hr
Schedule today’s PRNs tomorrow q 8 h +
PRN doses q 1 h
…Sample Orders to Control Agitation…
Midazolam SC
Loading dose = 0.2 mg / kg
then 0.1 mg / kg q 30 min x 2 PRN
Maintenance dose / hr =
25 % total dose to sedate
Consider alternative if need > 10 mg / hr
…Sample Orders to Control Agitation…
Propofol IV
Starting dose = 1 mg / kg / hr
Increase by 0.5 mg / kg / hr increments
every 15 – 30 min PRN
Maximum for EOL = 6 mg / kg / hr
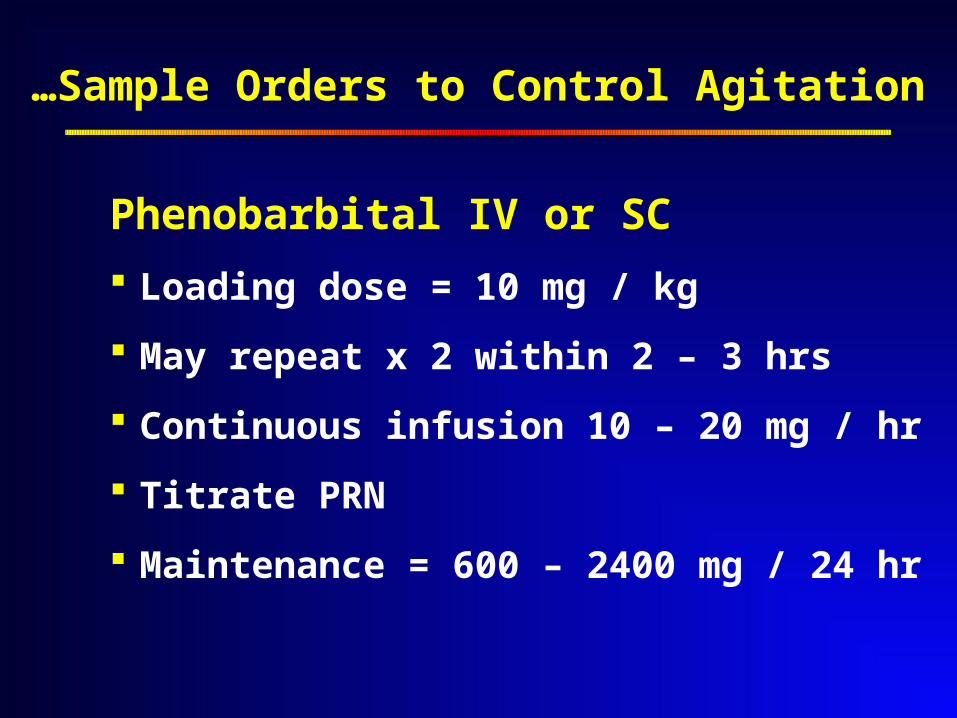
…Sample Orders to Control Agitation
Phenobarbital IV or SC
Loading dose = 10 mg / kg
May repeat x 2 within 2 – 3 hrs
Continuous infusion 10 – 20 mg / hr
Titrate PRN
Maintenance = 600 – 2400 mg / 24 hr
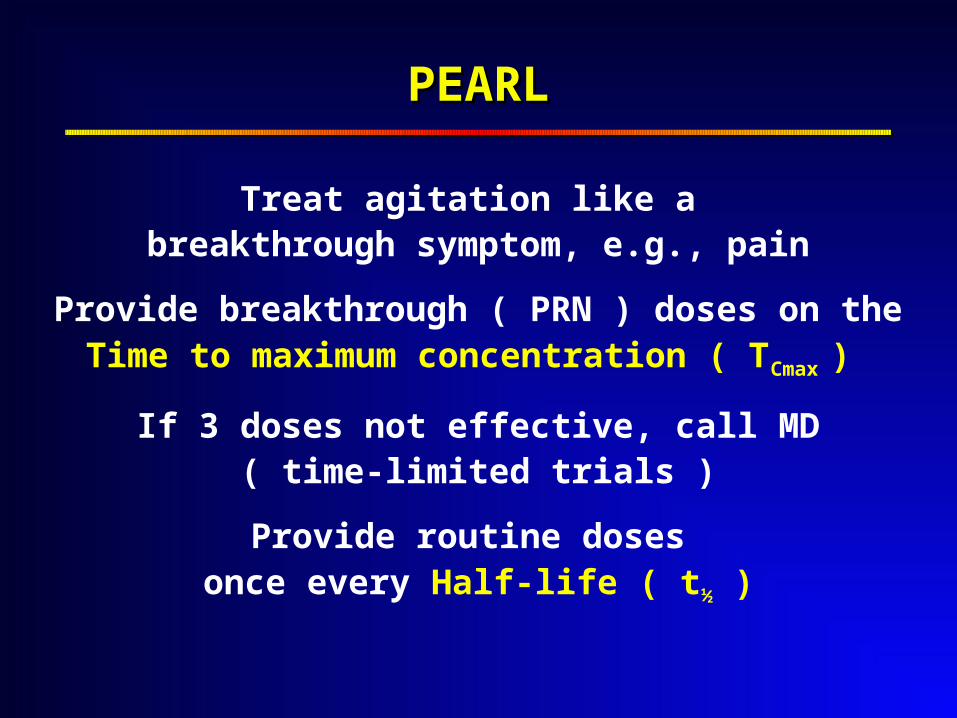
PEARLPEARL
Treat agitation like a breakthrough symptom, e.g., pain
Provide breakthrough ( PRN ) doses on theTime to maximum concentration ( TCmax )
If 3 doses not effective, call MD( time-limited trials )
Provide routine doses once every Half-life ( t½ )
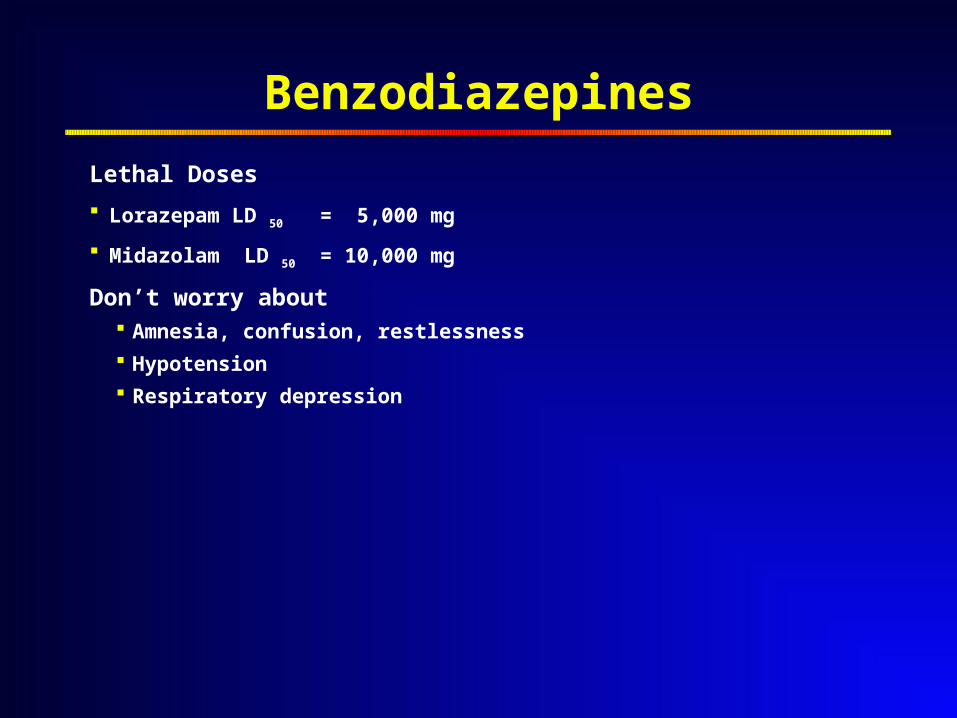
Benzodiazepines
Lethal Doses
Lorazepam LD 50 = 5,000 mg
Midazolam LD 50 = 10,000 mg
Don’t worry about Amnesia, confusion, restlessness
Hypotension
Respiratory depression
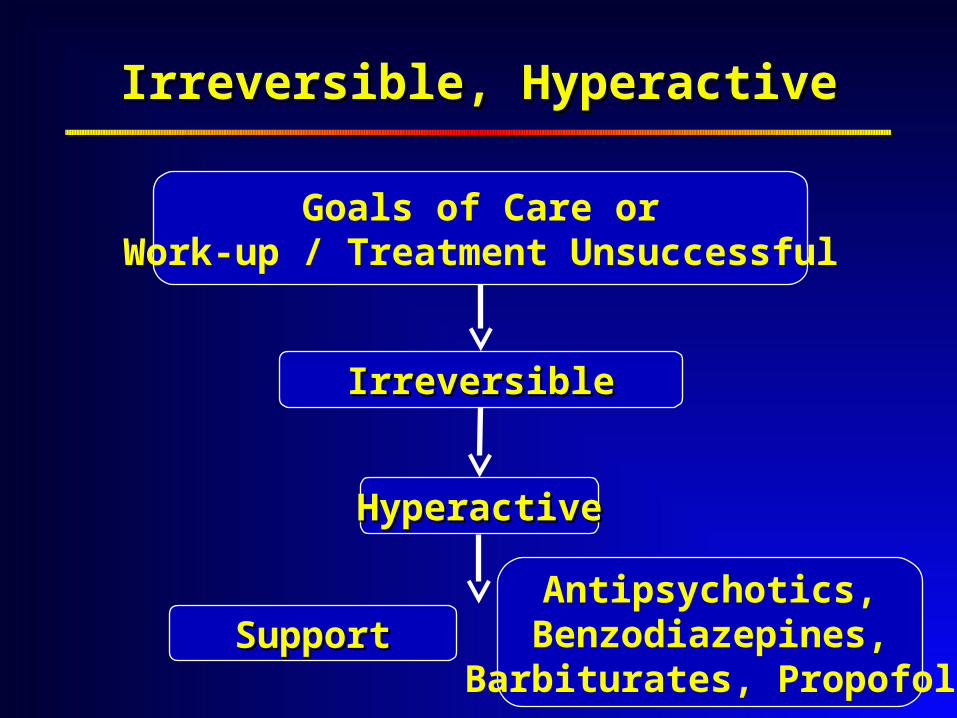
HyperactiveHyperactive
IrreversibleIrreversible
Irreversible, HyperactiveIrreversible, Hyperactive
Antipsychotics,Benzodiazepines,
Barbiturates, PropofolSupportSupport
Goals of Care orWork-up / Treatment Unsuccessful
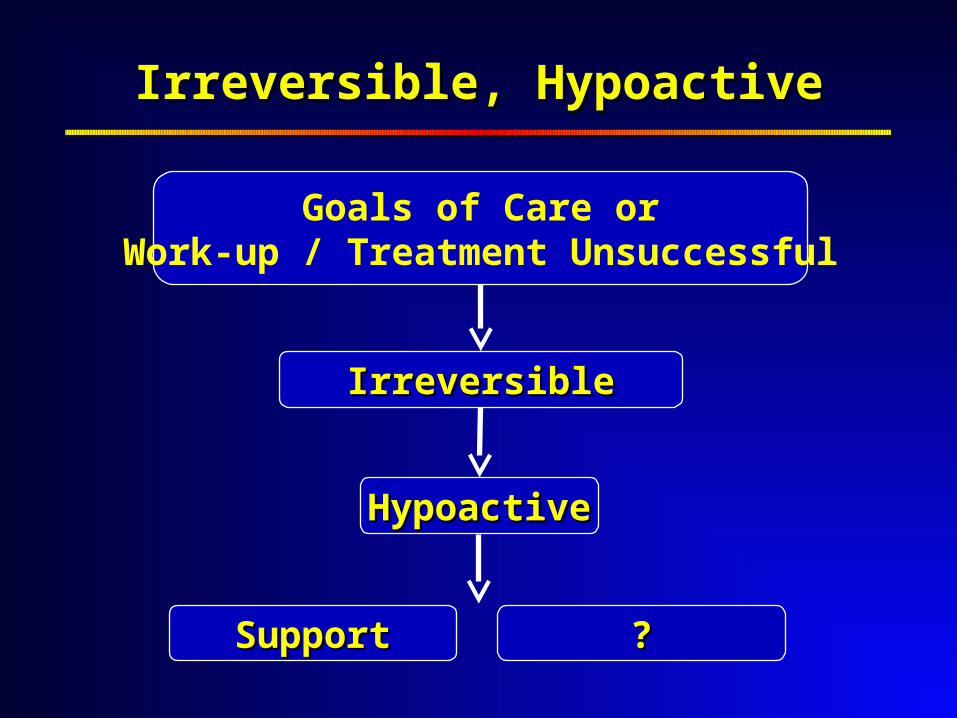
HypoactiveHypoactive
IrreversibleIrreversible
Irreversible, HypoactiveIrreversible, Hypoactive
SupportSupport
Goals of Care orWork-up / Treatment Unsuccessful
??
Mental Health Experts Can HelpMental Health Experts Can Help
Diagnoses often complex
Clinicians unfamiliar with
non-pharmacological treatments
Clinicians often uncomfortable with
pharmacological treatments,
especially off-label use
Develop new treatments
Key Topics…Key Topics…
Definition
Prevalence &consequences
Many causes
Under recognition
Assessment Common language
History & exam
Tools
Differential diagnoses
Goals of care
Diagnostic workup
……Key TopicsKey Topics
Management
Non–pharmacological
Pharmacological
Reversible
Irreversible
Terminal
SummarySummary
Cases can be complex
Clinicians often unfamiliar
with all possible treatments
Complex cases stressful