Embed Size (px)
Citation preview

GITAM DENTAL COLLEGE & HOSPITAL
DEPARTMENT OF Oral & Maxillofacial Surgery
SEMINAR ON
Neurological disorders Of Maxillofacial region
Presented By: Dr. Satyajit Sahu
II MDS
TRIGEMINAL NERVE - ANATOMY, LESIONS AND TREATMENT
INTRODUCTION

NEURO ANATOMY
NEURONS
Functional Anatomy
Physiology of Nerve Conduction
THE TRIGEMINAL NERVE (COURSE)
INTRODUCTION
INTRACRANIAL COURSE
EXTRACRANIAL COURSE
Opthalmic Nerve
Maxillary Nerve
Mandibular Nerve
PAIN PATHWAYS
NERVE INJURIES
Types of Nerve injuries
Histopathology of Nerve Injuries
Repair of Nerve Injuries
Suturing Techniques
Nerve Transplantation
POST TRAUMATIC PAIN SYNDROMES
Anesthesia Dolorosa
Causalgia
Phantom Facial Pain
LESIONS OF THE TRIGEMINAL NERVE
Central
Oeripheral

TRIGEMINAL NEURALGIA
Introduction
Diagnosis
Clinical Features
Differental Diagnosis
Pathogenesis
Treatment
Medical
Surgical
POST HERPETIC NEURALGIA
HEADACHE
MIGRAINE
MIGRANEOUS NEURALGIA
A TYPICAL FACIAL NEURALGIA
MYOFASCIAL PAIN DYSFUNCTION
CONNECTIVE TISSUE NEUROPATHIES
TOXIC AND NUTRITIONAL NEUROPATHIES
TUMORS OF NERVE TISSUE ORIGIN
BENIGN TUMOR
Traumatic Neuroma
Neuro Fibroma
Neurilemmoma
MALIGNANT TUMORS
Neuro Fibro Sarcoma

TRIGEMINAL NERVE
ANATOMY
INTRODUCTION
NEURO ANATOMY
Divisions of the Nervous System
a) Central Nervous System, made up of the brain and spinal cord.
b) The Peripheral Nervous system, consisting of the Peripheral nerves and the
ganglia associated with them
The Brain consists of (i) Cerebrum - Comprising two large cerebral
hemispheres.
(ii) The Cerebellum
(iii) The Midbrain
(iv) The Pons
(v) The medulla oblongata.
The midbrain, pons and medulla form the brain stem. The medulla is continuous below, with the spinal cord. Peripheral nerves attached to the brain are called cranial nerves. And those attached to the spinal cord are called spinal nerves. The nerves supplying the visver, along with the parts of the brain and spinal cord related to them, contitute the autonomic nerves system. The autonomic nerve systems is subdivided in to two major parts - The Sympathetic Nervous System.
- The Para Sympathetic Nervous System.
TISSUES CONSTITUTING THE NERVOUS SYSTEM
The nervous systems is made up predominantly of tissue that has the special property of being able to conduct impulses rapidly from one part of the body to another. The specialized cells that consitute the functional units

of the nervous system are called Neurons. Neuron Tissue, composed of neurons and Neuroglia, is richly supplied with blood.
Neurons:- (The Structural and functional unit of nervous system)
Neurons are excitable cells, Specialized for the reception, integration, transformation and transmission of coded information.
It has got a cell body (the nerve cell) a mass of specializes Cytoplasm with a diploid nuleus and an excitable membrance, from which project one or more neurites. These are branching, cytoplasmic processes, enclosed by excitable plasma membrane. Neurans are classified us unipolar, bipolar or mutlipolar according to the number of extension. Most neurites conduct towards the number of extension. Most neurites, conduct towards or directly influence the nerve cell as dendrites, only one conducts away from it, the axon.
Neurons (Definition)
Neurons is the structural and functional unit of the nervous system and consists of a nerve cell body and its processes.
Functional Anatomy
A neuron contains (1) a nerve cell body
(ii) The processes - two kinds
(a) Dendrite (b) Axon.
All neurons contain one and only one axon. But dentrite may be absent, one or many.
Axon carries impluses away from nerve cell body and Dendrite brings impulse from a distance.
Nerve cell body contains (i) Nucleus
(ii) Nissl bodies
(iii) Mitochondria
(iv) Golgi apoparatus
(v) Neurofibrils
The processes of Neurons

(I0 Dendrites (2) Axon
A nerve fiber may be myelinated or non myelinated.
Myelinated Nerve Fiber:-
The axon, shown at regular intervals an apparently constricted are called the nodes of ranvier. At the node of Ramvier, there is no myelin Sheath, and the neurilemma is in direct contact with axis cylinder. The portion in between the two successive nodes and internodes, gives the appearance (of myelinated nerve fiber) of a bamboo stick.
The myelin Sheath is made up of lipid materials, Great majority of nerve fibers in our body are myelinated nerves. Each internode contains one nuclius of schwann, which lies between the neurilemma, and myelin sheath.
Non Myelinated Nerves:-
There is no myelin sheath, the diameter of these nerves are very small, and there is no node of ranvier.
Importance of Myelin Sheath
Propagation of Action Potential is very fast in myelinated n erve fiber and slow in non myelinated one. This is because of the Saltatory conduction which is possible only in a myelinated nerve fiber.
Physiology of Nerve Conduction :-
The two basic properties of nerve fiber are
(i) Excitability and (ii) Conductvity
Excitability
When a nerve fiber is stimulated adequately the fiber is excited Threshold intensity of stimulus is the minimum strength of stimulus which can cause excitation.
Action Potential
When a threshold stimulus is applied to a nerve fiber, the fiber develops an AP which propagates onwards without any reduction in the amplitude until it reaches the end of the fiber.
(i ) The AP shows, all or none phenomenon.

That is, once the nerve fiber recives threshold strength stimulus, it develops, an AP. If the strength of stimulus is increased, there is no augumentation of the aplitude of AP.
(ii) When the AP propogates, there is no dimnution of the amplitude of it
(iii) Stimulation:- A single threshold stimulus fails to produce AP, but if a second stimulus is applied sufficiently quickly after the first one, the two stimuli are summated and an excitation results.
Refractory Period:-
When a nerve fibre is producing an AP, the fiber becomes refractory to a second stimulus. The first phase of this refractor period is called, absolute refractory period. (During a later phase, only a very strong stimulus can produce a response, this phase is called relative refractory period).
Conductivity:-
Propagation of AP:-
In non mylinated - a spot of the nerve fiber depolarized first. Because of the fact that the nerve membrane is both excitable and resistant, potential drop across the membrane develops in neighbouring point.
Saltatory Conduction:- In myelinated nerve.
Here entry of Na+ or exit of K+ can occur only at the nodes of Ranvier and not in any other points, As a result, sharp drop of membrane potential can occur only at the nodes of Ranvier, consequently the impluse appears to jump from node to node. This makes the velocity of the condiction in the myelinated fibers much higher than their non-myelinated counter parts.
THE TRIGEMINAL NERVE
Intrduction:- This is the largest cranial nerve, and is the sesory supply to the face, the greater part of the scalp, the teeth, the oral and nasal cavities, and motor supply to the masticatory and some other muscles. It also contains proprioceptive nerve fibers from the masticatory and probably the extra-ocular muscles.
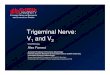
It has three divisions
(i) Ophthalmic

(ii) Maxillary
(iii) Mandibular.
The trigeminal nerve emerges from the ventral surface of pons, near its upper border, as a large sensory and a small motorroot, the latter lying anteromedial to the former.
Fiber in the sensory root are mainly axons of cells in the trigeminal ganglion (Semilunar) which occupies a recese in the dura mater covering the trigeminal impression near the apex of the petrous temporal bone. The ganglion liess at a depth of 4.5-5Cm. from the lateral surface of the head of the posterior end of Zygomatic arch. Medial to it are the internal carotid artery and the post. part of the cavernous sinus, inferior are the motor-root of the nerve, the greater petrosal nerve, the apex of the petrous temporal bone and the foramen lacerum. It receives filaments from the internal carotid sympathetic plexus and supplies twigs to the tentorium cerebelli.
The neurites of unipolar cells in the trigeminal ganglion divide into perpheral and central branches, the former being grouped to form the ophthalmic and maxillary nerve and the sensory part of the mandibular. The central branches constitute the fibers of the sensory root, leaving the ganglion's cancave margin to run posteromedially under the superior petrosal sinus and tentorium cerebell to enter the pons. Some fibers from proprioceptor endings in the masticatory muscles traverse the ganglion uninterruptedly to pass to the mesencephalic nucleus of the trigeminal.
On entering the pons, the fibers of the sensory root run dorsomedially towards the Principal sensory nucleus situated at this level. Before reaching the nucleus about 50% of the fibers deivide into ascending and descending branches, the others ascending or descending without division. The descending fibers, predomintly myelinated or non myelinated, form the spinal tract of the trigeminal nerve which reaches the upper cervical spinal cords, as it descends, terminals and collaterals are given off to synapse with neurons in the spinal trigeminal nucleus. Which contain small and intermediate neurons and is continuous with the substantia gelationsa of the spinal cord. The tract embraces the nucleus droso laterally, in the lower medulla oblongata it is superficial and lies under the tub erculum Cinerum. The fibers which synapse in the nucleus are concerned mostly with pain and thermal sensibility.

The spinal trigeminal nucleus divided into three levels the nucleus oralis (most rostral, adjoining the principal sensory nucleus). The Nucleus interpolaris, The nucleus Caudalis.
They differ in structure and to some extent in their connection. All levels receive afferents from the whole trigeminal sensory field.
Some ascending trigeminal fibers, heavily myelinated, synapse around the small neurons in the principal sensory nucleus, which lies lateral to the motor nucleus and medial to the cerebellar peduncle, It is continuous inferiorly with the spinal nucleus and is concerned with tactile stimulus.
Other ascending fibers enter the mesencephalic nucleus, a column of unipolar cells, whose perpheral branches convery proprioceptive impulses from the masticatory muscles. It is also stated that similar impulses reach it from the teeth and from the facial and occular muscles.
CONNECTIONS
Most fibers arising in the trigeminal sensory nuclei cross the midline to ascend in the trigeminal leminscus to the thalamic nuclius centralis posterior medialis relaying to the cortical post centralgyrus. Some, however, ascend to the nucleus of the ipsilateral thalamus. Collateral branches of primary and secondary afferent trigeminal neurons reach may other central region, such as the cranial nerve nuclei, the reticular formation, cerebellum, tectum, subthalamus, hypothalamus etc.
The motor nucleus of trigeminal nerve is avoid, with large multipolar cells interspersed with smaller multipolar cells. It lies in the upper pons medial to the principal sensory nucleus, separated from it by fibers of the trigeminal nerve.
Extra Cranial Course:
THE OPHTHALMIC NERVE
The opthalmic nerve the superior and the smallest trigeminal division, is wholly sensory. It supplies the eyeball, lacrimal gland and conjunctiva, part of the nasal mucosa and the skin of the nose, eyelids, forehead and part of the scalp. It arises from the antero medial end of the trigeminal ganglion on a flat band, about 2.5cm. long, passing forwards in the cavernous sinus in its lateral wall, below the occulomotor and trochlear nerves, just before

entering the orbit by the superior orbital fissure it divides into the lacrimal, frontal and nasociliary branches.
The ophthalmic nerve is joined by filaments from the internal carotid sympathetic plexus and communicates with the occulomotor trochliear and abducent nerves, thus forming routes by which proprioceptive fibers in these nerves may possibly enter the trigeminal. It has a recurrent meningeal branch (Tentorial nerve), which arises below and adheres to the trochlear nerve an ais distributed in the tentorium cerebelli.
THE LACRIMAL NERVE
he smallest of the main ophthalmic branches, sometimes receivesup filament from the trochlear nerve. The lacrimal nerve enters the orbit through the lateral part of the superior orbital fissure and runs along the upper border of the rectus lateralis with the lacrimal artery, recieving a twig from the zygomatico temporal branch of the maxillary nerve. Which contain lacrimal secroto motor fibers, entering the lacrimal gland, it supplies the adjoining conjunctiva. It then pierces the orbital septum and ends in the upper eyelid, joining filaments of the facial nerve.
The Frontal Nerve
The largest branch of the ophthalmic division, enters the orbit by the superior orbital fissure, and proceeds between the levator palpetrae superior is and the periosteum, dividing about midway between the apex and base of the orbit into a small supratrochlear and a large supraorbital branch.
The supratrochlear runs antero medially, passing bove the trochlea, and supplies a descending filament to the infratrochlear branch of the nasociliary nerve. It then emerges between the trochlea and the supraorbital foraman, curving upon the forehead close to the bone with the supratrochlear artery and supplying the conjunctiva and the skin of the upper eyelid. It then ascends beneath the corrugator and frontal belly of occipito frontalis dividing into branches which pierce these muscles to supply the skin of the lower forehead near the midline.
The Supraorbital nerve proceeds between the levator palpebrae superions and the orbital roof and traverse the supraorbital notch or foramen, supplying palpebral fiaments to the upper eyelid and conjunctiva. It ascends on the forehead with the supraorbital artery, dividing into smaller medial and a lateral branch, which supply the skin of the scalp as far upto the lambdoid suture. These branches are at first deep to the frontal belly of occipito

frontalis, the medial branch perferates it, while lateral pierces the epicramial aponeurosis. The main neve and both branches supply small rami to the mucosa of the frontal sinus and to the peri/cranium. Some enter the sinus by foramina in the floor of the supraorbital notch.
The Nasociliary Nerve
Intermediate in size between frontal and lacrimal, deeply placed in the orbit, enters between the two rami of the occulomotor nerve. It crosses the optic nerve with the ophthalmic artery and runs obliquely below the rectus superior and obliqus superior to the medial orbital wall. Here as the anterior ethmoidal nerve, it travers the anterior ethmoidal formen and canal, enters the cranial cavity and runs forwards in a groove on the upper surface of the cribriform plate beneath the dura mater. It descends through aslit lateral to the crista galli into the nasal cavity, where it occupies a groove on the surface of the nasal bone. It supplies two internal nasal branches, a medial to the anterior septal mucosa and a lateral to the anterior part of the lateral nasal wall. It emerges, as the external nasal nerve, at the lower border of the nasal bone, descending under the transverse part of the nasal is to supply the skin of the nasal ala, apex and vestibule.
The nasociliary nerve connects with the ciliary ganglion and has long ciliary, infratrochlear and posterior ethmoidal branches.
Two or three long ciliary nerves branch from the nasociliary as it crosses the optic nerve. They accompany the short ciliary nerves to piece the sclera near the attachment of the optic nerve. Running forwards between sclera and choroid, they supply the ciliary body, iris and cornea and usually contain the sympathetic fibers of the dilator pupillae, these being postganglionic fibers from neurons in the superior cervical ganglion.
The infratrochlear nerve branches from the nasociliary near the anterior ethmodial foramen, running forwards along the medial orbital wall above the rectus medialis it is joined, near the trochlea, supplying the skin of the eyelids and the side of the nose above the medial canthus, the conjunctiva, lacrimal sac and lacrimal caruncle. The posterior ethmoidal nerve leaves the orbit by the posterior ethmoidal foramen and supplies the ethmoidal and sphenoidal sinuses.
THE MAXILLARY NERVE
The maxillary nerve the intermediate division of the trigeminal, is wholly sensory, it leaves the trigeminal ganglion between the ophthalmic

and mandibular divisions as a flat plexiform band which passes horizontally forwards, low in the lateral wall of the cavernous sinus, to traverse the foramen rotundum, where it becomes more cylindrical and compact. Crossing the upper part of the pterygopalatine fossa, it incline intrally on the posterior surface of the orbital process of the palatine bone and on the upper part of the posterior surface of the maxilla and enters the orbit throught the infrarbital fissure, as the infraorbital nerve. Traversing the infraorbital groove and canal inn he orbital in the orbital floor, it appears on the face through the infraorbital foramen, under the cover of the levator labii superi cs, and divides, in to branche cwhich distribute to the nasal ala and lower eyelid and to the skin and mucous membrane of theu·heek and upper lip, these ramiFaommunicatres with the facial nerve.
Since the mouth is regarded as having evolved from a pair of fused visceral clefts, the maxillary nerve can be described as pretrematic and mandibular nerve as the post trematic branch of the trigeminal nerve. The branches of the maxillary nerve can be devided into four groups corresponding to their origine.
In the cranial Cavity - Meningeal
In the pterygopalatine fossa - Ganglionic, Zygomatic, Posterior
superior alveolar,
In the infraorbital canal - Middle superior, alveolar, anterior
superior alveolar.
On the face - Palpebral, Nasal , superior labial.
The Meningeal Nerve:-
Leaves the maxillary nerve near t he foraman rotundum, it receives a rami from the internal carotid sympathetic plexus and accompanies the frontal branch of the middle meningeal artery to supply the dura mater in the middle cranial fosa. Its anterior twigs just reach the anterior fossa.
Two Ganglionic Branches:- Connect the maxillary nerve to the pterygopalatine (sphenopalatine) ganglion situated just below it in the pterygopalatine fosa. They contain lacrimal screto moto fibers and

sensory fibers from the orbital periosteum and mucosa of the nose, palate and pharynx.
The Zygomatic Nerve:- Starts in the pterygopalatine fossa, enters the orbit throuight the inferior orbital fissure, runs along its lateral wall and divides into two branches, Zygomatico Temporal and Zygomatic Facial.
The Zygomatico facial traverse the inferolateral angle of the orbit, emerging in the face through foramen, in the Zgomatic bone, perforating the orbicularis oculi, it supply the skin on the prominence of the cheek. It forms a plexus with zygomatic branches of the facial nerve and palpebral branches of the maxillary nel e.
The Superio. Alveolar nerves:- Arises from the maxillary nerve in the pterygopalatine fossa or in the infraorbitaobproove (canal)¸ They are the posterior, middle and anterior superior alveolar nerve.
The Posterior superior alveolar nerve leaves the maxillary in the pteygopalatine fossa and runs antero-inferiorly to pierce the infratemporal surface of the maxilla, descending under the mucosa of the maxillary sinus after supplying the sinus the nerve divides into small branches which link up d the molar part of the superior dental plexus supplying twigs to th molar teeth. It also supplies a branch to the uppergum an1313the adjoining part of the cheek.
The Middle Superior Alveolar Nerve:- It arises from the infraorbital nerve as it runs in the infrorbital groove and run down and forwards in the lateral wall of the maxillary sinus. Like the posterior, it ends in small branches which link up with the superior dental plexus, supplying small rami to the upper premolar teeth.
The Anterior Superior Alveolar Nerve:- Leaves the latee l side of the infraorbital nerve near the mid point of its canal and traverses the canalis sinuosus in the anterior wall of thy maxillary sinus. Curving first under the infraorb ital foramen, it passes medially towards the nose, turns downwards, and divides into branches supplying the incisor and canine teeth. It assists in the formation of superior dental plexus and gives off a nasal branch, which passes through a minute canal in the lateral wall of the inferior meatus to supply the mucuous membrane of the anterior area of the lateral wall and the floor of the nassal cavity, communicating with the nasal branches of the pterygopalatine ganglion. Fin ally it emerges near the root of the anterior nasal spine to supply the adjoining part of the nasal septum.

The Palpebral Branches:- Ascend deep to the orbicularies oculi, piercing the muscle to supply the skin in the lower eyelid and joins with the facial and zygomatics facial nerves near the lateral canthus.
Nasal Branches:- Supply the skin of the side of the nose and of the movable part of the nasal septum, joining the external nasal branches of the anterior ethmodial nerve.
Superior Labial branches:- Descend behind the levator labii superioris, to supply the skin of the anterior part of the cheek, upper lip, oral mucosa and labial glands, and are joined by branches from the facial nerve to form the infraorbital plexus.
THE PTERYGO PALATINE GANGLION
The largest of the peripheral parasympathetic ganglia, is placed deeply in the pterygo palatine fossa, near the sphenopalatine foramen and anterior of the pterygoid canal, and lies just below the maxillary nerves as it crosses the fossa. Though connected functionally with the facial nerve, it is closely related to the maxillary nerve in position.
Its motor or parasympathetic root is the nerve of the pterygoid canal. Entering the ganglion poseriorly, its fibers arise from a special lacrimatory nucleus in the lower pons, emerging in the sensory root of the facial nerve to run in its greater petrosal branch unites with the deep petrosal nerves to form the nerve of the pterygoid canal. These preganglionic fibers relay in the pterygopalatine ganglion, the postganglionic fibers following a complicated course to their destimation, leaving the ganglion in one of its branches, they join the maxillary nerve and pass into its zygomatic branch and then into the zygomatico temporal nerve, leaving it in its communicating ramus to reach the lacrimal nerve. Thus they supply secretomotor fibers to the gland. Secretomotor fib ers for the palatine, pharyngeal and nasal glands are also believed to follow a similar route to the ganglion, where they are relayed, the postganglionic fibers running in the palatine and nasal branches.
The branches which appear to arise from the pterygopalatine ganglion are largely derived from the maxillary nerve and though intimately related to the ganglion, do note synapse in it. They include the orbital, nasal and the pharyngeal branches.
The orbital branches are two or three fine rami which enter the orbit by the inferior orbital fissure and are distributed to the periosteum and orbitalis muscle. Some fibers traverse the posterior ethmoidal foramen to supply the

sphenoidal and ethmoidal sinuses. The fibers supplying the orbitalis are from the sympathetic root.
The palatine nerves are distributed to the roof of the mouth, the softpalate, tonsil and nasal mucosa. The greater palatine nerves descends through the greater palatine foramen, runs forwards in a groove on the inferior surface of the bony palate almost to the incisor teeth and supplies the gums and the mucosa and glands of the osseous palate. It also communicates with the terminal filaments of the nasopalatine nerves. In the greater palatine canal it supplies the posterior inferior nasal branches, which emerges through the perpendicular plate of the palatine bone and ramify over the inferior nasal concha and the w3alls of the middle and inferior meatuses, as its exit from the canal the palatine branches are distributed to both surfaces of the soft palate. The lesser palatine nerves descend through the greater palatine canal, energe through the lessor palatine foramen and give branches to the uvula, tonsil and soft palate. Fibers conveying taste impulses from the palate probably pass via the palatine nerves to the pterygopalatine ganglion and through it to the nerve of the pterygoid canal and greater petrosal nerve to the facial ganglion.
Nasal branches enter the nasal cavities through the sphenopalatine foramen, forming the lateral and medial groups.
(1) About six lateral posterior superior nasal nerves innervates the mucosa of the posterior part of the superior and middle nasal conchae and the lining of the posterior ethmoidal sinuss.
(2) Two or three medial posterior superior nasal nerves cross the nasal roof below the opening of the sphenoidal sinus to supply the mucosa of the posterior part of the roof and of the nasal septum.
The largest of these nerves is the nasopalatine nerve, which runs antero-inferiorly on the nasal septum in a groove on the vomer. It descends to the roof of the mouth through the incisive fossa in the anterior hard palate.
The nasopalatine nerves supply a few filaments to the nasal septum and end by supplying the mucosa of the anterior part of the hard palate, there communicating with the anterior palatine nerves.
THE MANDIBULAR NERVE
The mandibular nerve supplies the teeth and gums of the mandible, the skin in the temporal region, part of the auricle, the lower lip, the lower part of the face and muscles of mastication, it also supplis the mucosa of the

anterior, presulcal part of the tongue and the oral floor., The largest trigeminal division, it has a large, sensory root which proceeds from the lateral part of the trigeminal ganglion to emerge almost at once from the foramen ovale and a small motor root which passes under the ganglion to unite with sensory root just beyond the foramen ovale, where the nerve passes between the tensor veli palatini (medial) and the lateral pterygoid. Just beyond this junction a meningeal branch and the nerve to the medial pterygoid leave the nerve's medial side. It then divides into small anterior and posterior trunk. As it descends from the foramen ovale, the nerve is about 4cm from th surface and a little anterior to the neck of the mandible.
The Meningeal Branches (nervus - Spinosus):- Re enters the cranium through the foramen spinosum with the middle meningeal artery, dividing the anterior and posterior branches which accompany the main division of the artery and supply the dura mater in the middle cranial fossa and to a lesser extent in the anterior fossa and calvarium the posterior also supplies the mucous lining of the mastoid air cells while the anterior communicates with the meningeal branch of the maxillary nerve. The nerves spinosus also contain sympathetic postganglionic fibers from the middle meningeal plexus.
The nerve to the medial pterygoid:- is a slender ramus entering the deep aspect of its muscle, supplying one or two filaments which pass through the otic ganglion without interrupting to supply the tensor tympani and tensor veli palatini.
The Anterior Trunk:- It gives rise to (1) the sensory buccal nerve and (2) motor branches, Masseterice, deep temporal and lateral pterygoid nerves.
The Buccal Nerve :- Proceeds between the two parts of the lateral pterygoid, descending beneath or through the lower part of the temporalis and deep to the mandible and masseter, it emerges from under the cover of the mandibular ramus and masseter anteriorly and unites with the buccal branches of the facial nerve. It supplies the lateral pterygoid while passing through it and may give of the anterior deep temporal nerves. It suppliers the skin over the anterior part of the buccinator and the mucous membraine lining its inner surface together with the posterior part of the buccal gingival surface.
The Masseteric Nerve:- Passes laterally, above the lateral pterygoid anterior to the TMJ and posterior to the tendon of the temporalis, it cross the

posterior part of the mandibular incisive with the masseteric artery, ramifies on and enters the masseter's deep surface and also supplies the joint.
The deep temporal nerves:- Usually an anterior and posterior, pass above the lateral pterygoid to enter the deep surface of the temporalis. The small posterior nerve is posterior in the temporal fossa, sometimes arising in common with the masseteric nerve, it ascends over the upper head of the lateral pterygoid.
The nerve to the lateral pterygoid:- enters the deep surface of the muscle. It may arise seperately from the anterior division of the mandibular, or with the bucal nerve.
The Posterior Trunk:- The posterior and larger, mandibular trunk is mainly sensory but recives a few filaments from the motor root. It divides into auriculo temporal, lingual and inferior alveolar nerves.
The Auriculo Temporal Nerves:- Usually has two roots, encircling the middle meningeal artery. It runs back under the lateral pterygoid on the surface of the tensor veli palatini to pass between the sphenomandibular ligament and the neck of the mandible and then laterally behind the TMJ inrelation with the upperm part of the parotid gland. Emerging from behind the joint, it ascends posterior to the superficial temporal vessels, over the posterior root of the zygoma, and divides into superficial temporal branches.
It communicate with the facial nerve and otic ganglion. The rami of the facial nerve, usually two, pass antero laterally behind the neck of the mandible to join the facial nerve at the posterior border of the masseter. Filaments from the oricganglion join the roots of the auriculo temporal nerve closed to their origin.
The branches of auriculo temporal nerve are the anterior auricular, branches to the external acoustic meatus, articular, parotid and superficial temporal. Usually two anterior auricular branches supply the skin of the tragus and sometimes a small part of the adjoining helix. The two branches of the external acoustic meatus pass between the osseous and cartilaginous parts of the meatus to supply the skin of the meatus, the upper sents a twig to the tympanic membraine. The articulr branches are one or two filaments which enter the posterior part of the TMJ. The parotid branches convey secretomotor fibers to the gland, preganglionic fibers come from the glossopharyngeal nerve by its sympanic branch, travelling via the lessor petrosal nerve to the otic ganglion, where postganglionic fibers pass to the auriculotemporal nerve to reach the gland. Vasoomotor fibers to the blood

vessels of the parotid gland are from the sympathetic root of the otic ganglion. The superficial temporal branches accompany the superficial temporal artery and its terminal branches supplying the skin in the temporal region and connecting with the facial and zygomatico temporal nerves.
The lingual nerve:-Is sensory to the mucousa of the persulcal part of the tongue, the floor of the mouth and the mandibular gingivae. It arises from the posterior trunk of the mandibular nerve and at first runs between the tensor Veli palatini and the lateral pterygoid, where it is joined by chorda tympani branch of the facial nerve and often by the branch of the inferior alveolar nerve. Emerging from the cover of the lateral pterygoid it proceeds down and forwards between the mandibular ramus and the medial pterygoid, lying anterior and slightly deep to the inferior alveolar nerve. It them passes below the mandibular attachment of the superior pharyngeal constrictor and lies against the medial surface of the mandible near the roots of the third molar tooth, where it is covered only the gingival mucosa, here it can be passed against the bone by a finger placed inside the mouth, It leaves the gingiva and passes into the side of the tongue, where it crosses the styloglossus and runs on the lateral surface of the hyoglossus and deep to the mylohoid, above the deep part of the submandibular gland and its duct. It proceeds forwards on the side of the tongue, lateral to the hyoglossus and gemioglossus, and divids into terminal branches which lie directly under the lingual mucosa. In the latter part of its course the nerve is near the submandibular duct, it passes downwards and forwards lateral to the duct, winds beolw it and then ascends forwards medial to it.
In addition to receiving the chorda tympani and a branch from the inferior alveolar nerve, the lingual nerve is connected to the submandibular ganglion by two or three branches and, at the anterior margine of the hyoglossus it forms connecting loops with twigs of the hypoglossal nerve.
Branches of the lingual nerve supply the mucosa of the oral floor, lingual aspects of the gingivae and the mucosa of the presulcal part of the tongue, being overlapped slightly by the lingual fibers of the glossopharyngeal nerve, terminal filaments join t the lingual apex with twigs of the hypoglossal nerve. It also carries postganglionic fibers from the submandibular ganglion to the sublingual and anterior lingual glands.
The Inferior Alveolar Nerve:-
It descends medial to the lateral pterygoid and then, at its lower border, passes between the spheno mandibular ligament and the mandibular ramus

to enter through the mandibular foramen into the mandibular canal, in this, it runs below the teeth, to the mental foramen, where it emeges to divide into incisive and mental branches. Below the lateral pterygoid it is accompnied by the inferior alveolar artery.
Dissection and radiography show that with in most mandibles the inferior dental nerve is plexiform and does not occupy a single canal. It is joined directly, or through plexiform branches, by rami entering the bone as parts of neuro vascular bundles derived from attached muscles such as the masseter. Such accessory dental nerves ramify in a plane lateral to the molar tooth, there common occurence accounts for incomplete anaesthesia by inferior dental nerve block.
The mylohyoid nerve leaves just before the inferior alveolar nerve enters the mandibular foramen. It pierces the spheno mandibular ligament, descends in a groove as the medial surface of the ramus of the mandible and, passing below the mylohyoid line, reaches the inferior surface of the mylohyoid, supplyng it and the anterior belly of digastric.
Branches to the molar and premolar teeth supply the adjoining gingiva also. Before they enter the dental roots they communicate and form an inferior dental plexus. The incisive nerve is often described as continuing on inthe bone to supply the canine and incisor teeth. The canine teeth may be supplied from the incisor plexus or from the plexus innervating the premolaras.
The mental nerve, emerging from its foramen, divides beneath the depressor anguli oris into three. A branch descending to the skin of the chin and two ascending to the skin and mucosa of the lower lip, these communicates freely with the facial nerve (Mandibular branch)
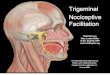
PAIN PATHWAYS
The trigeminal nerve, is the principal sensory nerve of the head region. Any stimulus in the area of the trigeminal nerve is first received by both myelinated and non myelinated fibers and conducted as an impulse along the afferent fibers of the ophthalmic, maxillary and mandibular branches into the semilunar or gasserion ganglion. From the ganglion the impulse is mediated by the sensory root of the nerve into the pons. Here the sensory root either ends directly in the main sensory nucleus or bifurcates into scending and descending fibers. The ascending fibers conveys general tactile sensibility, whereas the descending fibers conveys pain and temperature. Thus the pain impulse descends from the pons by the spinal

tract fibers of the trigeminal nerve, through the medulla, down to about the level of the second cervical segment, where the tract terminates. The mandibular, maxillary and ophthalmic branches terminate in the nucleus in that order.
Axons of the secondary neurons emerge from the spinal nucleus, cross the midline, and ascend to join with fibers of mesencephalic nucleus form the trigeminal lemniscus, or spinothalmic tracts, of the trigeminal nerve. These tracts continue upwards and terminate in the posteroventral nucleus of the thalamus. Some fibers of the lateral spinothalamic tract caus a general stimulation of the reticular formation that increases the patients awareness of and reaction to pain.
The pain impulse, on reaching the posteroventral nucleus of the thalamus, is mediated by secondary connecting neuron that project from the posteroventral thalamus to the posterocentral convolutions of the cerebral cortex.
Although the fifth crainal nerve is the main sensory nerve of the head, the seventh, ninth and tenth carinal nerves and the second and third cervical nerves play a minor part in the mediation of pain from this area.
NERVE INJURIES
In injuries of the facial skeleton and facial soft tissues, various cranial nerves are involved. Trigeminal nerve is most frequently involved.
Incidence:-
90% incidence of inf. alveolar nerve injury found with fractures of the mandibular body and 100% incidence of infraorbital nerve injury with zygomatico maxillary complex fractures. Elective mandibular third molar surgery accounts for most common injuries to inf. alveolar nerve and lingual nerve. Long buccal nerve injury can occur while raising the buccal flap for third molar exposure, mandibular osteotomy and vestibulo plasty. Removal or exposure of impacted cuspids and supernumerary teeth from the palate can lead to naso palatine neuropathy.
Inferior alveolar neuropathy following sagittal mandibular osteotomy and following osteotomy for mandibular augumentation has got 50% to 90% incidence. Mental nerve paraesthesia is usual with skin graft vestibulo plasty. The sensory neuropathies associated with reconstructive and preprosthetic surgeries are more severe as they are performed in older age populations and have less favourable regenerative response.

Nerve injuries are classified according to the degree of nerve injury as neurapraxia, Axonotmesis, Neurotmesis.
Neurapraxia:- Neurapraxia, usually the result of compression, is the simplest form of nerve damage. Only the narrow sheath is locally dmaged in a limited region. After an edematous phase, there can be disintergration and resorption of the myelin sheath, but without deeper damage involving the axons. There fore, the result is only a temporary interruption of conduction, with the continuity of the axial cylinder remaining completely intact. As soon as the cause of the damage is removed, function is restored. The regeneration phase depends on the time required for regeneration of the myelin sheaths. If the damage continues, however, complete disintegration of the myelin sheath rsults, and the axons themselves may become involved, sometimes, because of an ischemic disturbances of the blood supply. Since neurapraxia proceeds without significant morphologic damage, of course it does not require surgical intervention, fun ction returns spontaneously.
Axonotmesis:- Axonotmesis is characterized by destructions of axons and myelin sheaths, while connective tissue structures remain intact. The chief cause of axonotmesis is prolinged compression of the nerve or localized ischemic damage. As the continuity of the nerve is not interrupted in axonotmesis, degenerative and regenerative processes can proceed in an ideal fashion after interruption of the nerve fibers.
First, the axons and maroow sheath in the distal segment fall victim to wallerian degeneration, they disintegrate, and their fragments are decomposed by the Schwann cells and by entering macrophages. At the same time, the schwnn cells proliferate within the basal membrane, they multiply and are organized into band like chains, the Hanke-Bungner bands. The degeneration in the Central nerve segment proceeds, as a rule, only as far as the next, proximally located Ranviers node. It may go even further if extensive trauma is present. Regeneration of the nerve fibers can proceed only from the center. That is from the proximal stump. Usually, several axones except from the ends of the axial cylinder, they use the Hanke-Bungner bands prepared by the Schwann cells as a path and follow them to the end organ. The Schwann cells cause a new myelin sheath to form around the axone, whose sheath segments, however, are shorter than those of the intact nerve. The nerve fibers regenerate by 0.25 to 3mm per day, their regenerative capacity remains intact over a period of years.
Neurotmesis:- Here, the nerve with its nerve fibers is completely severed. The wallarian degeneration proceeds in the distal segment in the same way

as in axono tmesis. Here, also the result is complete degeneration of the axial cylinders and myelin sheath. Nutrition to the remaining slements of the distal nerve is preserved, after interruption of the longitudinal vessels, by way of collateral vessels in the vicinity, so that the connective tissue covering survives. Here, also reinnervation proceeds by way of the axons arising from the proximal stumps, the axons, however, must first find their way through the injury site into the distal nerve. But this is possible only in the ideal case in which the fascicles are approximated precisely and the newly formed axone do not have to overcome any obstacle before penetrating the peripheral nerve segment. This is the reason for the central problem in reconstructive surgery of nerve injuries. The surgical procedures must ensure that the regenerating axons can penetrate into the peripheral nerve stump without hindrance and must remove all factors that interfere with this process.
Histopathology of Nerve Injury:-
Degeneration and regeneration of Neurons:-
When the axon of a neuron is cut across a series of degenerative changes are seen in the axon distal to the injury, in the axon proximal to the injury and in the cell body.
The changes in the part of the axon distal to the ijury are referred to as anterograde degeneration or wallerian degeneration. They take place in the entire length of this part of the axon. A few hours after injury the axon becomes swollen and irregular in shape, and in a few days it breaks up into small fragments. It also uundergoes chemical changes. The schwann cells increase in size and mutiply in number. They act as macrophages and remove remnants of the axon and of myelin. At the same time schwann cells produce a large series of membranes that help to form numerous tubes Later these tubes play a vital role in regeneration of nerve fibers.
Degenerative changes in the neuron proximal to the injury are referred to as retrograde degeneration. These changes take place in the cell body and in the axon proximal to the injury.
The cell body of the injured neuron undergoes series of changes that constitute the phenomenon of chromatolysis. The cell body enlarges to become spherical, the nucleus moves from the centre to the periphery, the nissl sustances dissolves away. The reactions is more severe when the injury to the axon is near the cell body.

Some times the changes resulting from axonal injury are not confined to the injured neurons, but extend to other neurons with which the injured neuron, synapses. This phenomenon is referred as trans neuronal degeneration.
Changes in the proximal part of the axon are confined to a short segment near the site of injury. If the injury is harp and clean the effects extend only upto one or two nodes of Ranvier proximal to the injury. If the injury is severe enough longer segment of axon may be affected. The changes in the affected part ar exactly the same s for the distal part of the axon. They are soon followed by active growth at the tip of the surviving part of the axon. This causes the terminal part of the axon to swell up. If then gives off a number of branches. These branches grow into the connective tissue at the site of injury, in an effort to reach the distal cut end of the nerve. The schwann cells of the distal part of the nerve proliferate to form a series of tubes. When one of the regenerating axonal branches succeds in reaching such a tube, it enters it and then grows rapidly within it. The tube serves as a guide to the growing fiber. Axonal branches that fail to reach one of the tubes degenerate. The axon terminal growing through the schwann cell tube ultimately reaches and establishes. contact with an appropriate peripheral end argan.
REPAIR OF NERVE INJURIES
Principles of Nerve Anastomosis:-
Suture Technique:-Direct Suture Anastomosis of nerves is indicated when neuromesis type injury is known to have occured. Immediate repair of total nerves and sheath injuries is most effective if the field is free of foreign material and there is no infection and when the nerve endings can be approximated passively without significant tension. Tension of greater than 25gms is excessive and stretching of more than 8% of the nerve length will reduce the intrinic venule flow.
Delayed nerve anastomosis can also be successful but delay for more than 2 months will permit the ingrowth of significant fibrous tissue, neuroma formation and reduction of 50% off normal epineural sheath diameter.
In the standard technique for nerve anastomosis the meso neurium is released, and the nerve is freed for atleast 5mm. on either side of the injury site in order to observe for secondary injuries and debris and to aid in tension free repair. Bleeding should be controlled with bipolar microcoagulator, traumatic suctioning or retraction of neuro vascular trunks

should be avoided. The anatomic features of the cut nerve ends are identified to enable a proper realignment, of fascicles. Any excess fascicular protoplasum or irregular epineurium are trimmed.
For monofasciular nerves such as the inferior alveolar nerve and lingual, epinural rpair is simplest and effective. For nerves with more than one fascicle such as the infraorbital and mental, perineural suturing is necessary to match up correct proximal and distal branches.
The actual suturing is accomplished with 9-0 or 10-0 nylon material. It sutures have been overtightened, there will be a lateral bulging of fascicular contents, requiring either trimming or resuture.
The Cause of Failure of macroscopic suturing or epinural suturing:-
I) Even with a fresh cut, the cut surfce of a nerve remains smoothdue to the ends neurl pressure and the retraction of the perineuriam, the exan tend to bulg out from the perinural tubes of individual fascicles.
II) It is difficult to achieve exact adaptation of correspoding fasciles by means of epineural sutures, even slightest twisting of the nerve stumps leads to incomplete aproximation of identical fasciles or to their gliding past one another
Perineural Suturing:-
The use of surgical microscope makes possible atraumatic handling of the nerve stumps, exact evaluation of the cut surfaces of the nerve, and adaptation of the smaller unit of the nerve stumps (the fascicles).
After removal of the epineurium, single larger fascicles can be isolated and it is possible to resect the nerve substance bulging from the perineural tubes without shortening the perineurium and thus to avoid repeated bulging out of aditional axon masses. The fascicles stumps which are smooth now, are joined by one or two interrupted sutures. This procedure there fore referred to as perineural inter fascicular nerve suture. (Millesi - etal 1972, Sammi and Willebrand 1970).
Proliferation of Connective tissue at the suture site:-
This is the greatest danger in nerve anastomosis as it prevents the growth of the axon into the distal nerve stump and which can lead to formation of scar.
Factors leading to scar formation are

i) Tissue trauma
ii) Type and amount of suture material and
iii) Inter position of blood between the nerve stumps (due to bleeding
from the vessels of the nerve endings)
Prevention:- I) To prevent tissue trauma - keep the sutures free of tension. If it is not possible, in a nerve injury, to achieve a tension free approximation by mobilization of the nerve endings, proximally and distally, then only the inter position of a nerve transplant can lead to tension free briding of the defect.
Atraumatic dissection shlould be done, operating under surgical microscope makes this possible. The types of suture material can also affect connective tissue proliferation, similar to a foreign body reaction. There for the anastomosis should be performed with suture material of good tissue compatibility. Monofilament nylon I0/0 or II/0 is particularly suitable.
To avoid such foreign body reaction to the suture material, synthetic adhesives are tried (Using fibrin clot).
Inter position of coagulated blood between the nerve stumps can lead to severe connective tissue proliferation at the suture site. Using Bipolar coagulation careful coagulation of small vessels can be done without trauma to the fascicles.
NERVE TRANSPLANTATION (NERVE GRAFTING)
Nerve grafting is indicated in cases of acute neuro-tmesis where I) reanastomosis can not be accomplished without tension.
2) Neurotmesis and axonotmesis have resulted in pain and poor return of sensitivity.
3) There is evidence of symptomatic neuroma.
Two primary graft donor nerves are suitable
1) Sural nerve branch of the peroneal nerve
2) Great Auricular nerve.
The sural nerve is compatible with the inferior alveolar nerve and segments of great auricular nerve can be adapted to infrai\orbital and mental

nerve branches and less sensory deficit can be produced by removing only a portion of the great auricular.
A clean vertical sectioning is then made proximal and distal to the diseased nerve region. Excess exoplasm that exudes from the cut fascicles should be trimmed flush with the epineural or perineural sheath in preparation for the graft.
The graft is brought to place with a single 9-0 or 10-0 traction suture placed first through the roximal nerve stump, then through the graft. A second suture is then given by rotating the nerve 120 to 180o. The first traction suture of the distal repair should be placed first through the distal nerve stump rather than through the graft, to avoid excessive pull on the proximal repair. Overtightening of sutures avoided otherwise lateral bulging and neuroma formation will occur.
POST TRAUMATIC PAIN SYNDROMES
Anesthesia Dolorosa:-
It is a constant, boring, penetrating pain experienced in the center of a distribution of numbness. Seen mainly in patients who underwent nerve root rhizotomies. The site of pathology possibily in the higher thalamic and cortical levels.
CAUSALGIA:- It is a deep aching or burning that spreach out from the injure zone and beyond natural boundaries. These pain neither paroxysmal or nor triggered, although attacks are brought on by mild pain or touch stimulation of the region, by drying of tissue or by environmental stimuli such as loud noises. The affected tisues sweat excessively bcome warm or cold and will show degenerative trophic changes. All the symptoms are intensified by emotional stress. The specific mechanisum of causaligia may be the artificial synapsing of efferent sympathetic fibers with somatic sensory fibers within neuromas that have formed at the site of original nerve injury. Usually cured by identifying and excising neuromas.
Phantom facial pain:-
Patients who have undergone excision of a body part often experience a sense of awarness of the missing part called the phantom penomenon. Paroxysms of 10 minutes duration felt as stabbing, with extreme itching or deep burning and pressure of the missing part. May get triggered by tactile stimulation.

Complaints can be anticipated from patients who have undergone glossectomy and mandibulectomy operation for cancer control. Complaints of toothache and of phantom teeth in dental extraction sites, especially when the teeth have been chronically symptamatic before removal are not unusual.
After amputation of a body part, about half the associated neurons die, and the regenerated fibers of the stump are small, poorly myelinated and slow conducting. Stimulation of these stumps may have the effect of activating an imbalanced gate control machanisum in the brain stem and inappropriate sensory phenomena such as phantom pain.
Carbamazapine therapy is successful sometimes. Supportive care and reassurance is often adquate because phantom pain diminish with time.
LESIONS OF THE TRIGEMINAL NERVE
Peripheral Lesions:-
The nerve may be involved between the pons and the trigeminal ganglion in granulomatous meningitis or it may be compressed by a tumour or an aneurysm.
In the tigeminal ganglion it may be compressed by a tumour of the ganglion itself, or by a meningiona or acoustic neuroma arising in its neighbourhood or damaged by a basal skull fracture involving the middle fossa. Inflammation of the ganglion occurs in trigeminal herpes zoster.
Its upper two divisions may be damaged by lesions in the cavernous sinus or its first division bylesion in the superior orbital fissure, more peripherally still its division and major branches may be as a result of fracture of the facial bones.
When the nerve is involved between the pons and the ganglion, all the three divisions are likely to be affected. Lesions of the motor root cause weakness and wasting of muscles of mastication on the affected side. Wasting of temperalis and masseter leads to hollowing above and below the zygoma, and when patient clenches his teeth, palpation reveals that contraction of these muscles is less vigrous that on the normal side. When the mouth is opend, the jaw deviates to the paralysed sided as a result of the unantagonized action of the opposite lateral pterygoid.
Central Lesions:-

The central connection of trigeminal nerve may be involved in lesions, especially tumors, syringobulbia, and vascular lesions. Affcting pons, medulla and the upper cervical cord. A plaque of demyelination may occur at the point of entry of the sensory root into the brainstem in multiple sclerosis leading to trigeminal neuralgia or unilateral facial sensory loss. The motor nucleus can be affected by a lesion in the lateral pontine tegmentum.
Neuropathic Keratitis:-
It is change in the cornia which may follow any lesion of the fifth nerve if cornial analgesia results. It was often seen in the past after alcoholic injection of the trigeminal ganglion. It is due to the recurrent trauma to the insensitive cornea. The corneal surface becomes hazya, If unchecked, loss of surface epithelium, ulceration, and secondfary infection may develop.
TRIGEMINAL NEURALGIA AND RELATED DISORDERS
Introduction:-
Trigeminal neuralgia is probably the most excruciating of all of the disorders of facial pain. As the painful peroxysms of trigeminal neuralgia are often triggered by chewing and swallowing, patients a re often unable to eat and may become severaly cachetic as a result. Not only are the attacks of trigeminal euralgia agonizingly painful, they are also refractory to all conventional analgesic drugs. Even opiates are effectove only when given in high doses. Fortunately, we now have a number of effective medical and surgical therapies for this disorder, all of which are fairly specific for trigeminal neuralgia. Consequently, successful treatmnt of this malady depends on accurate diagnosis.
Diagnosis:- Subjective symptoms are the outstanding features of trigeminal Neuralgia. 90% of neuraligic diagnosis depends on the patients history. This is certainly true for orofacial pain in general and tigeminal euralgia in particular.
High essential to obtain as accurate and detailed information as possible regarding the frequency, duration, site, radiation nd quality of pain and whether there is any precipitating or aggravating factor is there.
The diagnostic evaluation of patients with orofacial pain is completed by performing a complete neurologic and dental examination and obtaining magnetic resonance imaging (MRI) of head, as well as specific laboratory tests indicated by the history and physical examination and E.M.G.

Clinical Characteristic or Trigeminal Neuralgia:-
Symptoms:- Trigeminal neuralgia is characterized by recurring paroxysms of sharp, stabbing, burning or electricx shock like pain in the distribution of one or more branches of the trigeminal nerve. The second and third divisions are affected much more frequently than the first division and the right side of face is more likely to be involved than the left side. The attacks only last a few seconds to a few minutes, and patients are pain free in between attacks.
A characteristic feature of trigeminal neuralgia is the presence of trigger points on the face or in the mouth. These are likely to set off an attack if touched. Most trigger points are in the centre part of the face, around the nose and lips. Light touch and vibration are the most effective triggering stimuli. Thus, washing the face, shaving or a light breeze hitting the face commonly precipitates the painful peroxysms of trigeminal neuralgia. Some patients even become dangerously emaciated and dehydrated because an attack ensues esch time they try to eat or drink.
Natural History:-
Age:- Trigeminal neuralgia usually starts in middle or late life but may occur at any age.
Sex:- Women are affected somewhat more than men.
There is an association between multiple sclerosis and trigeminal neuralgia, with a 1 to 8 percent incidence of multiple sclerosis in patients suffering from trigeminal neuralgia.
There is an occasional familial incidence. Most patients with trigeminal neuralgia will have exacerbation and remissions with an overall progressive increase in severity as time goes by. Eventually there will be frequent attacks occuring every day.
Diagnosis of trigeminal neuralgia is made on the basis of its characteristic symptoms in a patient whose neurological examination is essential normal and who has a negatice MRI study.
Differential Diagnosis:-
Trigeminal neuralgia must be differentiated from other types of face pain such as atypical odontalgia, postherpetic neuralgia, glossopharyngeal neuralgia temporal arteritis, cluser headache, TMJ dysfunction, myofascial

pain, atypical facial neuralgia, costents syndrome, migraine, referred pain, or simple toothache.
Atypical odontalgia is characterized by dull, aching, throbbing or burning pain which is more or less continuous and is triggered by mechanical stimulation of one of the teeth. It is relieved by sympathetic blocks.
Post herpetic nuralgia usually affects the first division of the trigeminal nerve and is precded by a vesicular eruption. The pain is described as a chronic buring feeling.
Cluster headaches cause a burning, boring, piercing or tearing pain lasting minutes to hours and are often triggered by the ingestion of alcohol.
Temporal arterits causes chronic aching over the affected artery, and there is marked tenderness on palpation of this artery.
TMJ dysfunction is an overdiagnosed entity but does occur in some patients. This individuals complains of aching pain that is triggered and exacerbated by jaw movement and that lasts for days, weeks or months.
Myofascial pain simularly presents as an aching pain lasting few days, weeks, or months but is triggered by palpation of triger points in the effected muscle.
Consten's syndrome may reasomble trigeminal neuralgia. In consten's Syndrome pain radiating into the lower jaw and temple on chewing is present. But is provoked by chewing only and no other trigger it is usually due to TMJ arthrosis and dental malocclusion and may be relieved by building up the bite.
Referred Pain may be seen in frontal and maxillary sinusitis, malignant diseases, glaucoma of the eye, Dental caries, Peri apical abscess, unerupted wisdom teeth, and in Angina of effert.
PATHOGENESIS OR TRIGEMINAL NEURALGIA
Aetiology:-
Various postulations are put forward as etiology
- Comprssion of the Sensory root by an artery
- In Patients with ipsilateral or contralateral tumors in the posterior foss traction on the sensory root is postulated (Hamby 1947)

- Tractions upon the sensory root of the nerve, not only due to tumour but also due to hydrocephalus (Tuker, fleming, Taylor and Schutz 1978) or to basilar anueurysm or compression of the nerve trunk in posterior fossa by a vertebrobasilar arterial system (Puhinelli and Rottenberg 1977)
Non specific inflammation of the ganglion and dental malocclusion (Carney 1967) and ischemia have all been postulated as the cause. But this is often a disease without a specific pathology.
- Epidemological risk factors (age, rce, smoking and drinking habits) have been postulated as being of significance in relation to whether the upper or lower face is involved (Rothman and Beck man 1974).
Two major Schools of thought regarding the etiology and pathogenesis of trigeminal neuralgia.
i) A Peripheral cause of this disorder
ii) A Central Mechanism.
The surgical treatment of trigeminal neuralgia has been mainly based on the notion of a peripheral cause, such as compression of the trigeminal nerve or roots by vascular, neoplastic or inflammatory lesions.
On the other hand, effective medical theraphy has developed as a consequence of Trousseau's Suggestion that the attacks of pain are due to paroxysmal activity in the trigeminal nuclei in the brain stem.
Clinical Data:-
There have been many reports that compression or stretching of the trigeminal roots by aberrant arteries, vascular malformation of slow-growing tumors causes trigeminal neuralgia.
Inflamatory changes in the trigeminal nerves have also been proposed as the etiologic agent in the trigeminal neuralgia (Harris)..
The notion that a central mechanism is involved in the painful paroxysm of trigeminal neuralgia is supported by a number of th clinical features of this disorder. There is measurable latent period between the onset of the stimulus to the trigger point and the onset of attack of trigeminal neuralgia. The attacks are more readily evoked by stimulating low-threshold mechano receptive afferants. Finally, the pain of trigeminal

neuralgia radiates outside the stimulated area and may be felt in entirely different division of trigeminal nerve than the location of the trigger point.
Experimental Data:-
- Focal demyelination of trigeminal roots in experimental animals leads to the generation of abnormal impulses in the demyelinated areas.
- The application of epileptogenic agents to the spinal trigeminal nucleus caused over reaction to tactile stimulation of the Ipsilateral face.
Experimental studies interpreted that trigeminal dysfunction elicited depends on the degree of damage inflicted. Mild injuries caused only transient increases in euronal activity, where as severe injuries lead to continuous high frequency neuron firing, resulting dysesthesias. Lesions some where in between these two extremes result in intermittent paroxysmal neuronal discharges that are perceived on the agonizing attacks of trigeminal neuralgia.
The fact that the drugs effective, in the treatment of trigeminal neuralgia all facilitate segmental inhabition of the trigeminal complex. Also suggest that a failure of this inhibitry mechanism may be involved in these pathogenisis of trigeminal neuralgia.
Dr.Gerhard.H.Fromm suggested that both central and peripheral mechanism plays a role.
He suggested the most likely explanation that chronic irritation of trigeminal afferent fibers results in a continuing impairment of segmental inhibition in the trigeminal complex as well as increased activity in the primary afferent fibers due to ectopic action potentials. As a consequence of such a combination of increased afferent input and impaired segmental inhibition, tactile stimulation of the face leads to hyperactivity and eventually paroxysmal discharges of flow-threshold mechano receptive and wide dynamic range neurons in the trigeminal nuclei. The transmission of such paroxysmal activity by trigeminolthalamic wide-dynamic range neurons result in the perception of the flashes of pain that characterize the attacks of trigeminal neuralgia.
It appears, therefore, that both schools of thought regarding the cause of trigeminal neuralgia nerve partly correct and that trigeminal neuralgia can be considered to have a peripheral etiology but a central pathogenesis.
CHRONIC IRRITATION OF TRIGEMINAL NERVE

ECTOPIC ACTION FAILURE OF POTENTIAL SEGMENTAL
INHABITATION
PAROXYSMAL DISCHARGE OF INTERNEURONS IN TRIGEMINAL NUCLEUS
FIRING OF NOCICEPTIVETRIGEMINO THALAMIC NEURONS
ATTACK OF TICK DOULOUREXINCREASED AFFERENT ACTIVITY + INCREASED SEGMENTAL
INHIBITION
PARAOXYSMAL DISCHARGES IN THETRIGEMINAL NUCLEUS
(From - Fromm G.H., Terrence CF, Maroon JCTrigeminal neuralgia - Current concepts regarding etiology andpathogenesis 1984 )
TREATMENT OF TRIGEMINAL NEURALGIA
Various treatment modalites have been tried in the past
1) Borsook etal (1939) I.V. Injection thiamine hydrochloride supplement by oral
intake of vit. B. ( 10 to 100 mgm.)
2) Trichlorethylene inhalation (specific action on sensory nerve ending of T.N)
Loomis (1937)
3) Alcohal or phenol injection to gasserion ganglion (hami 1937)
4) Division of the spinal tract of the nerve in the medulla Sjoqvist 1937.
5) Retrogasserian rhizotomy - temporal approach above the zygoma - recommended by Frazier (1925).
6) Radio frequency thermo coagulation (Sengupta and Stunden 1977).

Treatment:- (Recent) MedicalSurgical
MEDICAL TREATMENT
The Medical treatment should be the primary approach and that surgical intervention should be reserved for those patients who become refractory to, or can not tolerate, the currently available medication.
Before 1941, the medical treatment of trigeminal neuralgia consist only of a wide variety of nostrum. Truly effective medical therapy really started with the discovery of the ability of carbamazaepine to prevent the attacks of trigeminal neuralgia. The more recent discovery that baclofen is also effective, and has a strong synergistic action with carbamazepine and pheytoin, has greatly expanded the therapeutic aramamentarium.
Phenytoin:-
Main use as an adjunctive drug to baclofen and who can not tolerate carbamazepine.
Dose - 300 to 400 mg/day in two divided doses.
Side Effects - Drowiseness, diziness, diplopia and ataxia.
carbamazepine:-
The effectiveness of carbamazepine in the treatment of trigeminal neuralgin have been cnfirmed by a number of controlled trials. (Blom's study). It has led to the sugestion that carbamazepine can be employed as a diagnostic test, for trigeminal neuralgia.
The starting dose of Carbamazepine for the treatment of trigeminal neuralgia is 100 to 200 mgm twice a day. This does is increased by 200 mgm. every other day until the patient free or side effect occurs. The usual maintenanace dose is 600 to 1200 mg/day. The half life of carbamazapine is 30 to 50 hours when patients first start on this drug. but drops to 8 to 12 hours after a few weeks. Many patients therefore require 3 times a day regimen for best results and some may even need to take in four divided doses.
Side Effects:- Most commonly drowsiness, dizziness, unsteadiness nausea and anorexia.

Rarely causes oplastic anemia, leukopenia and thrombocytopenia and has also induced congestive heart failure rarely.
Baclofen:-
Baclofen resembles carbamazepine and phenytoin in facilitating segmental inhibition and depressing excitatory transmission in the spinal trigeminal nucleus, suggesting that this drug should also be used in the treatment of trigeminal neuralgias. Open trials have further substantiated the effectiveness of Baclofen in trigeminal neuralgia.
The starting dose of baclofen is 5 to 10 Mgm three times a day. This dose is increased by 10 mg every other day until the patient is pain free or side effects occur. The usual maintenanace dose is 50 to 60 mgm per day.
Side Effects:- not hve carbamazapine's potential for life threatening side effects. But it can cause drowsiness, dizziness and G.I.T. distress.
The most important precaution to observe in treating patients with baclofen is never to stop this medication abruptly after long term administration, as halucinations or seizures can occur. A new drug chlorphenerin carbamate is also used.
RECOMMENDED TREATMENT FOR TRIGEMINAL NEURALGIA
In view of its greater safely, treatment of trigeminal neuralgia should start with baclofen, even though it may not be quite as effective as carbamazepine.
Carbamazapine is the next choice if baclofen is ineffective or causes unacceptable side effects. One should always taper the medication gradually after the patient has been free of attacks.
Owing to the progressive increase in the severity of trigeminal neuralgia, eventually neither baclofen nor carbamazapine may be able to control the painful attacks. The combination of baclofen an d carbamazepine is much more effective than either drug alone, So should be tried in those patients who do not respond to monotherapy.
The combination of baclofen and phenytoia is also used where patients can not tolerate carbamazepine.
Those patients who become refractory to all these medication will require neurosurgical intervention.

SURGICAL MANAGEMENT
Micro vascular decompression and radio frequency or glycerol gangliolysis and rhizotomy are currently the procedures of choice. Micro vascular decompression offers the advantages of attacking the presumed etiology of trigeminal neuralgia, preserving the trigeminal nerve and produring longer lasting relief in most patients. Radio frequency or glycerol gangliolysis and rhizotomy avoid the risks of craniectomy, entail minimal morbidity and essentially no mortality, are much less empensive and can be repeated easily.
In younger healthy patients the chances of long term relief of pain with microvascular decompression would be an important consideration, whereas the minor operative procedures would be preferable in older patients with significant medical problems. It should be kept in mind that no surgical procedure has yet been developed that is 100 percent successful and that even microvascular decompression does not "Cure" trigeminal neuralgia.
Patients will often respond to another trial of medical therapy when their trigeminal neuralgia recurs after surgical intervention. Baclofen, Carbomazepine and phenytoin should there fore be tried once more at that point.
I) Peripheral Denervation:-
The specific objective of peripheral neurectomy are to eliminate as much as possible of the affected nerve branch and also to attempt to block its regeneration. Therefore, after the nerve has been exposed and before it is cut, dissection should be carried distally into the terminal tissues as far as possible. Proximally the maximum amount of nerve tissue should be avuled by rolling the nerve around a hemostat. Finally the nerve foramen should be obliterated with sterile wooden pegs, amalgam or bone plugs to block further nerve regeneration.
In the third trigeminal division, inferior alveolar nerve and lingual nerves are commonly resected. The lingual nerve can most easily be exposed at the inner surface of mandible in the third molar region by making a vertical incision along the internal oblique ridge. This same incision can be used to approach and cut the inferior alveolar nerve at the mandibular foramen.
Extraoral approach to inferior alveolar nerve resection is simpler and has the advantage of avoiding damage to the lingual nerve and permitting

direct obliteration of the mandibular canal. In this procedure, a 1cm. incision is made at the inferior border of the mandible in the antegonial notch region. Dissection is carried directly to the bone, and, by use of a nasal speculum to retract the masseter, the outline of the mandibular canal can be seen with the aid of intraoral transillumination. The lateral bony plate of the canal is removed, the nerve is avulsed and the canal is finally obliterated. When this procedure has been combined with mental nerve resection, the entire intra mandibular length of the inferior alveolar nerve can be removed intact.
For infraorbital neurectomy intraoral approach is used. Both the superior labial and lateral nasal branches of the nerve dissected free, and then the infraorbital foramen can be clearly visualized. After avulsion, canal obliteration done.
Branches of the first trigeminal division, including the supraorbital, frontal and supratrochlear nerves, may be exposed through an incision in the midportion of the eyebrow. Care should be taken to avoid damaging the lacrimal gland in the lateral roof of the orbit.
Peripheral neurectomies are minor operation that may be performed comfertably with local anaesthesia.
Radio Frequency Thermogangliolysis:-
Done at the level of trigeminal ganglion and sensory root, when applied to peripheral nerves, have the effect of selectively destroying small nerve fibers at the same time retaining the large nerve fibers. So preserves the normal tactile sensation of the patient.
In the Radio Frequency thermogangliolysis technique a 22-gauge needle, insulated except at its tip, is inserted through the skin of the cheek, passed medial to the mandibular ramus and through the foramen ovale to come to rest at the vental aspect of the trigeminal ganglion in Meckel's cavity. One or two thermal lesions of 60o to 70o are made for 30 seconds each. Results of these lesions have been very good. With a high rate of pain control, minimal complications.
Radio Frequency Thermo Neurolysis:-
In these techniques the same basic approach is used as discribed previously except that the lesions can be made in the outpatient setting, G.A.

is not required, there are no risks of dangering vital intratranial structures, and lesions can be repeated more early if necessary.
Cryosurgery:-
Controlled freezing of peripheral sensory nerve has been used successfully to suppress neuralgia form pain. Cryosurgical lesions are made at tempreature lower than 50oC by directly exposing the epineeurim for 15 to 60 seconds and repeating 3 to 4 times. Pain relief can be expected to last 2 weeks to a year, depending on the cause of the pain and on the extent of the freeze.
Cryoneurolysis depends on an ice crystalization of intracellular fluids and dissolution of the axon plasm membrane. This produces axon degeneration but preserve the connective tissue sheaths when done proparly. If the lesion is not controlled, occlusion of perineurial vessels will produce local ischemia and result in paresthesias.
Osseous Curettage (Rather procedure)
Surgical bony decortication with added topical and systemic antibiotic has been advocated for the management of Trigeminal Neuralgia and atypical neuralgia.
Retrogasserian Rhizotomy:-
In this oeration the trigeminal sensory root fibers are sectioned between the ganglion and the point of root entry into the pons. A complete permanent degeneration of the nerve cell bodies results from this lesion. Incomplete lesioning or the action of aberrant sensory fibers in the motor trigeminal root may lead to recurence. The resulting profound numbness occassionally leads to anesthesia dolorosa as well as recurrent herpes zoster, corneal ulceration and other troiphic tissue changes. For these reasons this procedure now rarely done to control trigeminal neuralgia and have been replaced by the Radio Frequency thermal lesions and an even more promising operation, Microsurgical root decompression.
Micro Vascular Nerve Root Decompression:-
Dandy was the first to suggest that vascular compression of th Vth nerve near the pons might be an etiologic cause for trigeminal Neuralgia and later Janetta considered Tigeminal Neuralgia due to vascular compression of Trigeminal Nerveroot entry zone in the pons and developed Microvascular decumpression operation. Janetta has advocated a posterior fossa approach

to decompress the neurovascular anomalies by placing alloplastic materials between the vassels and roots. 85% success rate has been seen. Mortality less than 5% . This operation reserved for healthior patients with long life expectancies.
Complication:-
- Hematoma (Intracerebral)
- Infarction of brainstem
- Status epilepticus
- Postoperative Hearing lose
- Fusion of the middle ear.
Balloon Compression Rhizolysis:-
Balloon inserted to Meckel's cave and inflated and thus decompression produced.
Tractotomy:- The primary desending tracts of trigeminal, as well as eighth, ninth and tenth nerve sensory fibers may be interrupted by lesions placed 4mm. below the obex in the medulla.
It is especially indicated when pain is bilateral or when many cranial nerves are involved. Meduallary tractotomy has a higher mortality rate than rhizotomy and recurrence rate is high.
Tractotomy also done at the level of the pons or midbrain to control maxillofacial pains such as post herpetic neuralgia.
Thalamotomy and Cortical Leukotomy Procedures:-
Selective lesions in the thalamus and cortex are the only known surgical treatment for most varities of central pain such as phantom pain, thalamic syndrom, post herpetic neuralgia. Lesions of the posterior medial thalamus are made by radio frequency electrodes that are left implanted for a period of time.
Cortical leukotomy consists of white matter lesions of the frontal lobes nd has the interesting result of decreasing the suffering or emotional component of pain without causing any significant change in the perception thres holdes.

An important danger with leukotomy procedures is the potential to induce significant personality defects and loss of "Social Senses". So done only as a last resor.
Misallaneous Therapies:-
Use of electrical stimulation of the gasserian ganglion was proposed by Meyersin in 1980 and consists of chronic implantation of an electrode in the gasserion ganglion.
POST HERPETIC NEURALGIA
Post herpetic neuralgia (PHN) is a common caus of severe neuropathic pain, especially in the elderly.
Origin:- PHN is a consequence of herpes zoster (HZ), which is caused by reactivation of the varicella Zoster virus, usually contracted in childhood. On intial exposure, varicella zoster causes varicella, in which the virus disseminates hematogenously from the neasopharynx to the skin and mucous membranes. Later in the cause of the illness, the virus presumably enters sensory nerve fibers and its transported to trigeminal, geniculate and dorsal root gan glia, where it comes to be dormant for many years. The declining immus surveillance accompanying advancing age or an immuno compromised state causes the virus to re-erupt in the sensory ganglion. This results in a segmental hemorrhagic inflammatory reaction in the skin, mucous membrain etc. This disorder is often very painful and constitutes herpes zoster. Usually pain subsides, but if persists or recurs with healing, referred to as PHN.
- Females are more prone to PHN
- Older age group more affected
Treatment:-
Post herpectc pain persists for 1 month or longer duration and in most diminishes with time.
For prevention of PHN systemic Steriods usually 60 Mg. of predmisone tapered over 10 to 14 days.
- Amantadine is used in patients for whom steriods are contra indicated (100mgm twice daily for a month)
For established PHN - Amitriptyline can be given in low doses (10mgm.)

Surgical Treatment:- Trigeminal tractotomy has reported success (Hitchcock and Schvarz).
HEADACHE
Migraine:-
True migraine headaches are debilitating pains that throb and ache unilaterally in the temporal region. Women are affected twice than men. Familial tendency is there. Occurs before the age of 16 Years.
The attack lasts mnutes, hours or for fewdays. Migraine may be caused by excess vasodilation of the extra cranial vessels.
Treatment is entirely medical.
In milder cases aspirin is enough. In severe forms ergotamine tartarate is used.
Periodic migranious neuralgia:-
Also known as cluster headache.
Its clinical features are intermediate between trigeminal neuralgia and migraine headache. The pain is burning or aching begins deep within the midface and then migrates unilaterally to the forehead, temple and then to the lower face.
Hereditary factors and emotional factors seems to play a role in this disorder. There is no known trigger points, althoug alcohol intake precipitate attacks.
This disorder is a result of an arterial dilation as in migraine headache, but in periodic migranious neuralgia the point of neuropathology is some where along the course of the greater petrosal nerve.
Diganosis and pain relief can be aided by local anaesthetic block of the spheno palatine ganglion through the greater palatine foramen.
Ergotamine usually gives good relief to patients with this disorder.
Atypical Facial Neuralgia:-
In 1927, Temple Fay described atypical facial neuralgia as a vascular syndrome of dull aching, throbbing, situated deep in the eye and malar regions.

Atypical facial neuralgia is characterized by burning, boring, throbbing pain appearing in attacks of 20 to 90 minutes duration. There is no explosive quality or tactile triggering characteristic of classic neuralgias.
Ergotamine 150mgm. 3 times a day is effective in managing many cases. More recently, propranolol 60 to 120 mgm daily has proven to be effective and sfe prophylactic therapy for many patients.
More recently this sydrome has been effectively managed with relaxation therapies and biofeedback techniques.
Myofacial Pain Dysfunction:-
Caused by muscle spasm in the masticatory apparatus. In their acute form, these spasms poduces trismus, deviation of the mandible to the affected side, inability to occlude the teeth, and sharp pain brought on by clenching. The pain felt over TMJ or above the gonial angle and some times over the zygoma, temporal, submandibular or occipital region.
The acute syndrome often follows trauma such as subluxation or dislocation of mandible and radical changes in the chewing patterns, but the most important factor is emotional stress.
Joine clicking and jerky mandibular movements are common. The myofacial pain syndrome must be differenciated from true osteoarthritis, migranious neuralgia, maxillary sinusitis and referred pain.
Treatment of the acute phase of myofacial pain by (I) Supportive therapy with analgesics, tranquilizers and muscle relaxants and physiotherapy such as local moist heat. (II) Disengagement of the masticatory apparatus by consciously avoiding stressful clenching and by using temporary occlusal splints. The need for rest and psychological counselling should be stressed.
Connective tissue neuropathies:-
Trigeminal neuropathies been linked with major collagen disorders, including SIE, Sjogren's syndrome, rheumatoid arthritis, Sclerodrma, Polyarteritis nodosa and diabetes mellitus.
Pathogenesis in these disorders are believed to be due to Vasculitis occus in the nutrient vessels of peripheral nerves, causing ischemia and microinfarcts to the nerve segments.

The disease state most commonly associated with neuropathies of all types is diabetic mellitus.
Toxic andn Nutritional Neuropathies:-
In conditions of nutritional deprivation, the nerve cell metabolism may be disterbed that it no longer maintain its perpheral processes, and wallerian degeneration results and are characterized by numbness and paresthesias in the more distal portion of nerve.
Deficiencies of Vitamin B1 (Thiamin) cause beriberi and result in nerve deafness and a patchy trigeminal paresthesia. In pellagra (Vit. B2 def.) also trigeminal sensory neuropathy seen.
In pernicious anemia neuropathy is caused by incomplete absorption of Vit. B12 by the small intestine.
Heavy metal intoxication produces necrosis in the trigeminl sensory ganglia. The metals most frequently associated with maxillofacial neuropathies have been mercury, lead, cadmium, bissmuth and arsenic.
Finally, trigeminal sensory neuropathies have linked with a number of well known therapeutic drugs, including penicillins, cortisone, isoniazid and mitrofurantoin.
TUMORS OF NERVE TISSUE ORIGIN
BENIGN TUMORS:
Traumatic Neuroma (Amputation Neuroma):-
Not a true neoplasm, but an exuberant ttempt at repair of a damaged nerve trunk. A hyper plasia of nerve fibers and their supporting tissues.
Occurs due to accidental or purposeful sectioning of a nerve or may be incidentl to difficult extraction.
Repair of a damaged nerve begins with proliferation of the axis cylindes, the cells of the neurilemmal sheaths and the endoneurium. Regeneration is facilitated by the persistence of the neurilemmal tubes, since new fibers proliferate through them and schwann cells multiply around them.
Reinnervation occurs under the bproliferating proximal ends meet some obstructions such as scar tissue, in which case the nerve continues to

proliferate into an unorganized bulbous or nodular mass of nerve fibers and schwann cells in varying proportions. This constitute a traumatic neuroma.
Treated by sugical axcision of the nodule along with a small proximal portion of the involved nerve.
Neuro Fibroma:-
The Neuro Fibroma is a tumer of the nerve tissue origin. It is most frequently involves the skin or oral mucosa and does not differ from the disseminated or multiple form of the disease, known as neuro fibromatosis or Von Recklinghausen's disease.
They are uncommon in the mouth and present as soft pedunculted swellings of the cheek, tongue or palate, or as sessile masses on the gingiva. Deepar lesions produce a fusiform swelling often soft and lobulated in the substance of cheek, tongue or palate and may be mistaken for a lipoma. Brown patches ( Cafe - au - lait) will be present on the skin in von-reckling hausen's disease. Lesions arising from the Inferior alveolar nerve will enlarge the bony canal or even create a significant intra-osseous radiolucency.
Plexiform neurofibromatosis affect the head and neck region. Here the whole plexus of nerves is thickned producing a marked deformity due to the soft redundant mass. Histologically there is proliferation of schwann cells.
Treatment:- Excision. Incomplete removal lead to recurrence. Sarcomatoms transformation can occur leading to a poor prognosis.
Neurilemmoma (Schwannoma)
Is a common tumor derived from schwann cells. C/F - is a slow growing lesion. They are usually painless unless they are causing pressure on adjacent nerves. The preseting symptom of the majority of patients is only the peence of a tumor mass. In all instances the tumor is encapsulated. Treatment is by surgical excision. The neurolemmoma does not undergo malignant transformation.
Malignant Tumors:-
Neuro fibro Sarcoma (Malignant Schwannoma)
Very rare

Sarcomatous transformation in neuro fibromatosis occurs more in the deep seated lesions rather than in the superificial ones.
C/F - Found to occur in the 3rd to 6th decades, no sexpredilection. The lips, gingiva, palate and buccal mucosa have been the site of involvement.
In the central tumors, the mandible or mandibular nerve affected than the maxilla.
Treatment:- Treated by Surgory and radiation. High recurrence rate due to the tendancy of the tumor to grow along the involved nerve, making total excision difficult.
CONCLUSION
In summary, the exprience of pain is the most common problem in maxillofacial neuro pathology and should be viewed s more than a predictable specific sensation or a warning sign of a disease. The diagnosis of maxillofacial neurological problems depends on an orderly process of
i) Interpreting the symptoms and signs of altered neurophysiology ii) determining the anatomical localization of the disease process iii) understanding the basic pathological processes that exist and iv) identifying the etiological or precipitating factors.
Treatment of these problem is a challange to practioners from many discipline and effective action depend on a team approach. However, the oral and maxillo facial surgeon is in a position to make a strong contribution in this field because of his extensive knowledge of maxillo facial symptomatology anatom y, physiology and pathology.

REFERENCES
1. GRAY'S ANATOMY2. MANUAL OF ANATOMY - CUNNIGHAM3. HUMAN NEUROANATOMY - INDER BIR SINGH4. ANATOMY AND PHISIOLOGY - MILLER5. HUMAN PHYSIOLOGY - SARADA SUBRAMNIAM6. TEXT BOOK OF MEDICAL PHYSIOLOGY - GUYTON7. CONCISE MEDICAL PHYSIOLOGY - SUJIT .K. CHAUDHARI8. TEXT BOOKS OF SURGERY - BAILERY AND LOVE9. TEXT BOOK OF SURGERY - SABISTON10. ORAL AND MAXILLOFACIAL TRUMATOLOGY - SCHILLI AND
KRUGER11. DISEASES OF THE NERVOUS SYSTEM - BRAIN'S SIR JOHN WALTON10. CURRENT ADVANCES IN ORAL AND MAXILLOFACIAL
SURGERY WILLIAM, B. IRBY. DAVID W. SHELTON13. ORAL AND MAXILLOFACIAL SURGERY - GUSTAV .O. KRUGER14. AN ATLAS OF HEAD AND NECK SURGERY - LOR15. TEXT BOOK OF NEUROSURGERY - ROGER.N . ROSENBERG16. ORAL PATHOLOGY - SCHAFER17. ORAL PATHOLOGY - THOMA AND GOLDMAN18. TEXT BOOK OF PHARMACOLOGY - SATOSKAR19. TEXT BOOK OF MEDICINE - DAVIDSON20. MINOR ORAL SURGERY - KILLEY AND KAY21. LOCAL ANAESTHESIA - MONHEIM'S22. NEUROLOGY CLINICS - MAY 198923. NEUROLOGY CLINICS - FEB.99024. AMERICAL JOURNAL OF ORAL AND MAXILLOFACIAL SURGERY OCT
1982

25. AMERICAL JOURNAL OF ORAL AND MAXILLOFACIAL SURGERY FEB. 1982.