Embed Size (px)
Citation preview

Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) Biu LGA CMAM Program.
Borno State, Northern Nigeria. Nov-Dec 2014
Ifeanyi Maduanusi, Chika Obinwa, Francis Ogum, Zulai Abdulmalik, and Janet Adeoye
ACF-International

2
ACKNOWLEDGEMENTS
The ACF Coverage Team appreciates Borno State Primary Health Care Development Agency (BSPHCDA) Maiduguri for giving authorization to
conduct the assessment in Biu LGA. The Chairman BSPHCDA, and Jibrin Bukar (Director Human resource BSPHCDA) received the Coverage
Team and were very supportive throughout the exercise. Ladi Ezike, the State Nutrition Officer, gave the Team the routine monitoring data,
and acted as the link between the State and ACF Coverage Team. Mallam Iliya, acting PHC Coordinator and Aisha Abubakar the Nutrition Focal
Person (NFP) Biu LGA provided the team with client records, list of villages in Biu LGA, and other useful program information.
The effort of Peter Magoh the ACF security manager who coordinated security assessment and daily security procedure while the team was
in the field is highly appreciated. Abubakar Chiroma Kawu, Program Support Officer, provided logistics and administrative support to the entire
team in the field.
Ifeanyi Maduanusi (ACF CMAM Coverage Deputy Program Manager) led the assessment and provided technical support during the
implementation. The ACF Coverage Officers –Chika, Zulai, Janet and Francis– supervised the field enumerators and data collection and were
instrumental in compiling the SQUEAC report. Diego Macias of ACF-UK reviewed the report, while Sophie Woodhead of the Coverage
Monitoring Network (CMN) gave useful insights in compilation and validation of this SQUEAC report.
The enumerators who collected the field data despite the security challenges are appreciated. All stakeholders who gave useful information
regarding the CMAM Program in Biu LGA are highly appreciated.
This assessment was completed through the generous support of Children Investment Fund Foundation (CIFF).

3
Table of Contents
1. EXECUTIVE SUMMARY ................................................................................................................................................................................................ 6
2. INTRODUCTION .......................................................................................................................................................................................................... 7
3. OBJECTIVES ................................................................................................................................................................................................................. 8
4. METHODOLOGY .......................................................................................................................................................................................................... 9
5. DESCRIPTION OF FIELD ACTIVITIES ............................................................................................................................................................................ 11
6. RESULTS AND FINDINGS ........................................................................................................................................................................................... 12
6.1. QUANTITATIVE DATA (ROUTINE MONITORING DATA AND BENEFICIARY RECORDS). ................................................................................................................. 12 6.1.3 PROGRAM EXITS......................................................................................................................................................................................................... 13 6.1.4 MUAC AT ADMISSION ............................................................................................................................................................................................... 14 6.1.5 LENGTH OF STAY FROM ADMISSION TO RECOVERY ............................................................................................................................................................ 15 6.1.6 NUMBER OF VISITS BEFORE DEFAULT .............................................................................................................................................................................. 17 6.1.7 CONCLUSION OF THE ROUTINE MONITORING (OTP CARDS) ANALYSIS .................................................................................................................................. 17 6.2 STAGE 1: QUALITATIVE DATA ....................................................................................................................................................................................... 18 6.2.1 QUALITATIVE SAMPLING FRAMEWORK ........................................................................................................................................................................... 18 6.2.2 KNOWLEDGE ABOUT MALNUTRITION ............................................................................................................................................................................. 18 6.2.3 HEALTH SEEKING BEHAVIOR IN COMMUNITIES ................................................................................................................................................................. 18 6.2.4 AWARENESS OF THE CMAM PROGRAM IN COMMUNITIES AND COMMUNITY MOBILIZATION ................................................................................................... 19 6.2.5 COMMUNITY VOLUNTEER ACTIVITIES ............................................................................................................................................................................. 19 6.2.6 RUTF SUPPLY AND AVAILABILITY .................................................................................................................................................................................. 19 6.2.7 ROUTINE DRUGS ........................................................................................................................................................................................................ 19 6.2.8 HEALTH WORKERS ACTIVITIES AND TRAINING .................................................................................................................................................................. 20 6.3 DATA TRIANGULATION ................................................................................................................................................................................................ 20 6.4 CONCEPT MAP ........................................................................................................................................................................................................... 22 6.5 STAGE 2: SMALL AREA SURVEY AND SMALL STUDY. ......................................................................................................................................................... 22 6.5.1 SMALL AREA SURVEY .................................................................................................................................................................................................. 22 6.5.2 SAMPLING METHODOLOGY .......................................................................................................................................................................................... 22 6.5.2.1 CASE DEFINITION ....................................................................................................................................................................................................... 22 6.5.2.2 RESULT OF SMALL AREA SURVEY................................................................................................................................................................................... 23 6.5.2 SMALL STUDY ON DEFAULTERS ..................................................................................................................................................................................... 24 6.5.3 CONCLUSION OF SMALL AREA SURVEY AND SMALL STUDY ................................................................................................................................................ 25 6.6 DEVELOPING THE PRIOR............................................................................................................................................................................................... 26 6.6.1 HISTOGRAM OF BELIEF. ............................................................................................................................................................................................... 26 6.6.2 CONCEPT MAP .......................................................................................................................................................................................................... 26 6.6.3 UN-WEIGHTED BARRIERS AND BOOSTERS ........................................................................................................................................................................ 26 6.6.4 WEIGHTED BARRIERS AND BOOSTERS. ............................................................................................................................................................................ 27 6.6.5 TRIANGULATION OF PRIOR ........................................................................................................................................................................................... 28 6.6 DISCUSSION .............................................................................................................................................................................................................. 28 6.7 RECOMMENDATIONS .................................................................................................................................................................................................. 29
7.0 ANNEXURE ........................................................................................................................................................................................................... 31
7.1 ANNEX1: SCHEDULE OF IMPLEMENTED ACTIVITIES IN DAMATURU SQUEAC. ....................................................................................................................... 31 7.2 ANNEX 2: CONCEPT MAPS ........................................................................................................................................................................................... 33 7.3 ANNEX 3: ACTIVE AND ADAPTIVE CASE FINDING PROCEDURE. ............................................................................................................................................ 34 7.5 ANNEX 4: SEASONAL CALENDAR OF EVENTS IN BIU LGA ................................................................................................................................................... 35

4
List of figures
FIGURE 1: MAP OF BORNO STATE SHOWING THE CONSTITUENT LGAS .......................................................................................................................................................... 7 FIGURE 2: SOCIAL MAP OF BIU LGA SHOWING THE 11 POLITICAL WARDS ..................................................................................................................................................... 8 FIGURE 3: ADMISSION TREND OF BIU LGA CMAM PROGRAM .................................................................................................................................................................. 12 FIGURE 4: EXIT TRENDS FOR BIU LGA CMAM PROGRAM-NOVEMBER 2013 TO OCTOBER 2014 .................................................................................................................... 13 FIGURE 5: ADMISSION MUAC FOR BIU LGA CMAM PROGRAM............................................................................................................................................................... 14 FIGURE 6: SAMPLES OF ADMISSIONS ABOVE 115MM BY HEALTH FACILITIES. CROSS-REFERENCING WITH EDEMA. ................................................................................................ 15 FIGURE 7: LENGTH OF STAY IN PROGRAM BEFORE RECOVERY ..................................................................................................................................................................... 15 FIGURE 8: DISTRIBUTION OF THE MUAC OF CHILDREN DISCHARGED AS ‘RECOVERED’ .................................................................................................................................... 16 FIGURE 9: REASONS FOR NOT ATTENDING THE CMAM PROGRAM-SMALL AREA SURVEY ................................................................................................................................. 24 FIGURE 10: ILLUSTRATION OF TRIANGULATION OF PRIOR .......................................................................................................................................................................... 28 FIGURE 11: CONCEPT MAP SHOWING THE RELATIONSHIP BETWEEN FACTORS AFFECTING CMAM PROGRAM AND COVERAGE ................................................................................. 33
List of tables
TABLE 1 SUMMARY OF EXTRACTED BENEFICIARY INFORMATION AT A GLANCE –MAY TO NOVEMBER 2014. ....................................................................................................... 12 TABLE 2 SOURCES AND METHODS USED TO GET INFORMATION IN THE BBQ ................................................................................................................................................. 20 TABLE 3: BARRIERS, BOOSTERS & QUESTIONS FINDINGS AND SOURCES OF INFORMATION................................................................................................................................. 21 TABLE 4: SIMPLIFIED LOT QUALITY ASSURANCE CLASSIFICATION OF SMALL AREA SURVEY RESULTS ..................................................................................................................... 23 TABLE 5: WEIGHTED BARRIERS AND BOOSTERS OF BIU LGA CMAM PROGRAM ........................................................................................................................................... 27 TABLE 6: PROPOSED RECOMMENDATIONS AND PROCESSES AFTER THE CONCLUSION OF THE ASSESSMENT ........................................................................................................... 29

5
ABBREVIATIONS
ACF Actin Contre La Faim/Action Against Hunger International
BSPHCDA Borno State Primary Health Care Development Agency
CIFF Children Investment Fund Foundation
CMAM Community Management of Acute Malnutrition
CV Community Volunteer
ECHO European Commission Humanitarian Aid
FMOH Federal Ministry of Health
HF Health Facility
IEC Information Education and Communication
LGA Local Government Area
NFP Nutrition Focal Person
NHIS National Health Insurance Scheme
INGO International Non-governmental Organization
MDG Millennium Development Goals
OTP Outpatient Therapeutic Program
PHC Primary Health Care
RUTF Ready to Use Therapeutic Food
SAM Severe Acute Malnutrition
SLEAC Simplified Lot quality assurance sampling Evaluation of Access and Coverage
SNO State Nutrition Officer
SMART Standardized Monitoring Assessment of relief and Transitions
SMOH State Ministry of Health
SQUEAC Semi Quantitative Evaluation of Access and Coverage
VI Valid International

6
1. Executive summary
In October 2010, Biu LGA of Borno State commenced the implementation of Community-based Management of Acute Malnutrition
(CMAM) in four HFs1. These CMAM health facilities (HF) receive technical support primarily from UNICEF through the ‘D’ Field
Office Bauchi, and also from the BSPHCDA. In March 2014, a HF (Yawi) was selected for scale-up of CMAM services in Biu local
government area. Since the inception of the CMAM program in Biu LGA in 2010, SQUEAC assessment had not been conducted to
assess the program. Nevertheless, a recent SLEAC assessment2 by Valid International (VI) in 11 States of Northern Nigeria, showed
that CMAM services in Biu LGA had a low classification3 of coverage. Only nine children out of 61 SAM cases found in Biu LGA were
in-program. The coverage classification was lower than the average estimate for Borno state (31.4% [95% CI 23.2% - 39.6%]. This
is one of the reasons why Biu LGA was chosen for a SQUEAC assessment, and also, to further identify in detail the barriers and
boosters that influence access to the CMAM program, identify the spatial pattern of coverage, recommend lasting solutions to the
barriers identified, and build capacity of the LGA and SMoH staff on the SQUEAC methodology.
The beneficiary records covering a six month period (May – November 2014) were collected from the HFs and extracted into a
database for detailed analyses. The following indicators were analyzed: level of MUAC at admission, length-of-stay from admission
to recovery, number of visits before default, distribution of defaulters according to their exit MUAC, distribution of recovered cases
according to their exit MUAC, and time-to-travel from home to CMAM HFs. On the other hand, the routine program data was
obtained from the State Nutrition Officer over a one-year period (November 2013 to October 2014). This data was extracted to
analyze the trends of admission and performance indicators. After the analysis of routine program data and client records from
May 2014 to November 2014, qualitative information was sought from 6 villages4 in four out of the five CMAM sites5 in Biu LGA.
Different sources and methods were used to obtain the qualitative information. All the findings were analyzed into barriers and
boosters, and triangulated by source and method.
The barriers identified during the assessment include: insecurity as a major challenge to access in half of Biu LGA; health workers
had only been trained once since the inception of the program in 2011; stock-out of RUTF due to insecurity and a poor
logistic/supply chain management from the State and LGA stores; stock-out of routine drugs; poor health seeking behavior in some
communities; lack of motivation of community volunteers; consumption of RUTF by healthy siblings and adults; lack of volunteers
in some of Biu’s health facilities; poor case finding and defaulter tracing; poor community mobilization and sensitization; poor
integration with other child health programs; and lack of support and funding by the local government area.
Conversely, the boosters found include: good opinion about the program in communities, passive referrals from non-CMAM HFs,
peer-to-peer referrals from communities, good awareness of the program in communities, supply of free drugs by MDGs6 and
NHIS in some CMAM HFs, and good attitude of HWs towards caregivers.
A spatial pattern of coverage within Biu LGA was hypothesized and tested. Homogenous high coverage was found within political
wards, since both near and far villages were identified with high levels of coverage. The same applied to villages in wards where
there is no insecurity. Consequently, Insecurity was envisaged to be contributing to heterogeneity and variability of coverage levels
1These include; Biu MCH, Gunda, Mandaragirau, and Miringa. 2Chrissy B., Bina S., Safari B., Ernest G., Lio F. & Moussa S.; Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage (SLEAC) Survey of Community-based Management of Acute Malnutrition program; Northern States of Nigeria-(Sokoto, Kebbi, Zamfara, Kano, Katsina, Gombe, Jigawa, Bauchi, Adamawa, Yobe, Borno). Valid International. February 2014 3The SLEAC used a three-class classifier with 20% and 50% as the thresholds; ≤20% is low; >20% to ≤50% is moderate coverage while >50% 4 Villages visited include ; filingiji, hema, dugja, tum, maina hari, yamekurmi, 5The five CMAM HFs include; Biu MCH, Gunda, Mandaragirau, Miringa and Yawi were visited. 6 Millennium Development Goals project attached to the Presidency, Federal Republic of Nigeria.

7
in Biu LGA. However, small area survey could not be fully conducted in areas with insecurity, and therefore such assumption could
not be tested.
The headline coverage estimate for the LGA could not be arrived at because of insecurity in half of Biu LGA, which prevented the
team from conducting a wide area survey necessary for final coverage estimation (see methodology below), as well as a part of
the small area survey during the previous phase. The conducting team had no guarantees about their safety and that of the
enumerators collaborating in the assessment.
Recommendations: refresher training for HWs, supportive supervision of CMAM HFs, recruitment and refresher training for CVs,
strengthening of supply chain of RUTF and routine drugs, amongst other recommendations were proffered.
2. Introduction Borno State was created in 1976 with Maiduguri as its capital. It is located at the North-East of Nigeria, with 27 Local Government Areas (LGAs). Borno borders three countries —the Republic of Niger to the North, Republic of Chad to the Northeast and Cameroon to the East—, while it borders the Nigerian States of Adamawa and Gombe to the South, and Yobe to the West. Borno State has a population of 4,151,193 people according to the 2006 census.
Biu LGA is a southern local government area (see Figure 1), with Biu town as its administrative headquarter. Biu is situated about 188 kilometers Southwest of Maiduguri, the state capital. The LGA has eleven political wards: Buratai, Dugja, Galdimare, Garubula, Gur, Mandaragireu, Miringa, Silumthla, Yawi and Zarawuyaku. Biu town was once the capital of Biu kingdom and now it also serves as the capital of Biu emirate. It has seven traditional districts: Biu east, Biu west, Buratai, Gunda, Garubula, Mandaragiru and Miringa. The major ethnic groups in the LGA are Pabur/Bura, Tera, Marghi, Mina, Hausa and Fulani. The major occupations within the LGA is crop farming, cattle rearing, and trading.
Figure 1: Map of Borno State showing the constituent LGAs

8
Figure 2: Social Map of Biu LGA showing the 11 political wards
The implementation of the CMAM program in Biu LGA commenced in October 2010 in four HFs where the program is integrated with other health services. In May 2014, one HF was added to the existing four to provide CMAM services. The program utilizes health workers working under the Biu LGA PHC department, and is supervised by the NFP and LGA Primary Health Care Coordinator. The NFP supervises the CMAM health facilities, collates and sends the report to the State Nutrition Officer, who works under the supervision of the Director Primary Health Care. The State Nutrition Officer (SNO) also serves as the link to the UNICEF Nutrition Specialist ‘D’ Field Office, and the Nutrition Division of the Federal Ministry of Health.
A recent SLEAC study conducted early 2014 by Valid International classified Biu with low levels of coverage (nine SAM cases were
covered by the CMAM program out of 61 SAM cases found in the LGA). The LGA was chosen for a SQUEAC assessment to
understand in detail the positive (booster) and negative (barrier) factors affecting the program, amongst other objectives outlined
below.
3. Objectives The following are the specific objectives of the SQUEAC assessment:
1. To investigate and identify the barriers and boosters to access and coverage of the CMAM program. 2. To determine the spatial pattern of coverage in Biu LGA. 3. To estimate the headline program coverage in Biu LGA. 4. To proffer recommendations to improve the CMAM program. 5. To build the capacity of SMoH and LGA staff to conduct a SQUEAC assessment.

9
4. Methodology
The SQUEAC methodology expects to serve as an adaptive and changing tool, capable of adjusting some of its aspects to concrete
realities and different circumstances. Here follows the outline of the methodological elements of the research.
Stage 1
Quantitative data:
Routine program data was obtained and used to plot indicators such as new admissions over time, trends of recovery, defaulters,
and death rates. Then, the beneficiary information was extracted from the OTP cards into a database and analyzed into various
plots including MUAC measurement at admission; length of stay from admission to recovery; number of visits before default;
distribution MUAC measurements among defaulting cases, distribution of MUAC measurement at recovery, and time-to-travel
from home to CMAM health facilities.
The derived plots were critically observed and some factors that might be affecting access and coverage were identified for further
investigation using qualitative tools.
Qualitative data
Interviews were conducted using varying methods to collect qualitative data about the program. The information obtained were
analyzed using the Barriers, Boosters and Questions (BBQ) tool.
Barriers, boosters and questions (BBQ): The BBQ tool was used to capture the positive and negative factors that were interpreted
to be affecting the program coverage from both the quantitative and qualitative data analyses.
Triangulation: The barriers and boosters identified from the qualitative and quantitative information were triangulated by sources
and methods. Questions were raised where the information was not very clear, and further evidence were gathered to answer the
questions raised. Information was collected as much as possible, until no new evidence was forthcoming around a certain
theme/topic. This process is referred as sampling to redundancy.
Concept map: Illustration of the link between factors that affect the program were summarized in a concept map shown in annex
of this report.
Stage 2 data
A small area survey and small study were conducted to investigate the spatial pattern of coverage and factors that may be affecting
coverage.
Small Area Survey
The small area survey data was analyzed using simplified lot quality assurance technique (LQAS) to test a hypothesis about a
concrete barrier affecting coverage. Such barrier was defined by the conducting team according to the observations of the previous
stage. This was done by examining the number of Severe Acute Malnutrition (SAM) cases found (n) and the SAM cases covered in
the program. The threshold value (d) was used to determine if the coverage was classified as satisfactory or not. Another value
(p) was used to denote a standard used as a measure of coverage7.
7 SPHERE standards has recommended minimum coverage for Therapeutic programs in rural, urban, and camp settlements. These thresholds are 50%, 70% and 90% coverage for TFP program run in the contexts of rural, urban and camp areas respectively.

10
The value of (p) used was 50%, which is an acceptable threshold of coverage for rural areas.
The formula for deriving (d) = ⌊𝑛 × 𝑝1⌋ = ⌊𝑛 ×50
100⌋ =
𝑛
2
If the number of covered cases exceeded value (d), then the coverage was classified as being satisfactory. However, if the number
of covered cases found did not exceed value (d), then the coverage was classified as being unsatisfactory. The combination of the
(n) and (d) was used as the sampling plan.
The reasons for coverage failure obtained from the small area survey were plotted in figure 9.
Small Study
A small study was conducted to investigate the reasons for high rate of default observed from the analyses of the extracted
beneficiary information.
Stage 3 data
The prior: The prior mode for the program was estimated by triangulating the estimates from the following:
Belief histogram
Weighted barriers and boosters
Un-weighted barriers and boosters
Calculation of the total positive and total negative factors illustrated in the concept map.
The prior was established in a beta prior distribution with prior shaping parameters and plotted on Bayes calculator. The beta prior
distribution expresses the findings of stage 1 and 2 in similar ways to the likelihood survey as described below. The Bayes calculator
also suggested a sample size at 10% precision.
The likelihood survey: as a central part of the final stage, the SQUEAC foresees the conduction of a Wide Area Survey. For this, a
sample size of SAM cases to be found is calculated using statistical formulas derived from the prior (see previous stages). A number
of villages to be visited is equally deducted from a statistical formula. The conducting team is deployed across these villages and
finds as many SAM cases as possible.
The data obtained from the likelihood survey is then organized into the parameters tabulated in the table below and the likelihood
results expressed as a percentage.
Parameters Values
Current cases in the program x
Current SAM cases not in the program y
Total current SAM cases (n) 𝒙 + 𝒚
Likelihood 𝒍𝒊𝒌𝒆𝒍𝒊𝒉𝒐𝒐𝒅 =(𝒙)
(𝒙 + 𝒚)
The prior and likelihood are then combined (also referred as conjugate analysis8) to arrive at the posterior -final program coverage in any SQUEAC investigation.
8 A conjugate analysis requires that the prior and the likelihood are expressed in similar ways.

11
However, the likelihood survey was not conducted due to insecurity in half of Biu LGA. It was decided to avoid deploying the team
into most villages, so enough information for determining the likelihood could not be have been obtained.
5. Description of field activities
SQUEAC planning, training and implementation
A letter from the Federal Ministry of Health (FMOH) introducing ACF Coverage Team to Bornu State Primary Health Care
Development Agency (BSPHCDA) was delivered through the State Nutrition Officer. The Coverage Team arrived in Gombe9 from
where they proceeded to Maiduguri, Borno State capital, on the 16th of November 2014 to meet with the SNO and the Director of
the BSPHCDA. Authorization to conduct the assessment was obtained from the State.
A total of 696 OTP cards of beneficiaries that exited the program from May 2014 to November 2014 from the existing 5 CMAM
HFs was pulled together into a database. Advert for enumerators and recruitment was done; enumerators were sourced from Biu
LGA. A two days theoretical training for successful enumerators and LGA staff, and one day field training were conducted from
24th to 26th November 2014. Three CMAM sites10 and 6 communities were visited to gather qualitative information. Analyses of
information obtained from the field and update of BBQ were done in Gombe. After small area survey and small study, field activities
could not continue, as the team could not conduct wide area survey in half of the LGA due to insecurity. This included five out of
eleven political wards of Biu LGA that are affected by the insurgency.
The enumerators and LGA staff and the coverage team held a participatory recommendation session in Gombe on the 15thof
December 2014, to develop a way forward towards improving the CMAM program in Biu LGA.
9Gombe State capital is where the coverage team resided during Biu SQUEAC. The town is about 128 kilometers from Biu LGA. 10Biu MCH, Miringa and Yawi HF, the remaining two facilities could not be accessed due to insecurity.

12
6. Results and findings
The results obtained from data analysis are presented and summarized below.
6.1. Quantitative data (routine monitoring data and beneficiary records).
The routine program data (performance indicators), beneficiary information and anecdotal program information were analyzed.
The data extracted from the beneficiary records that exited the program from May 2014 to November 2014 are summarized in
Table 1 below:
6.1.2 Admission trends
Figure 3: Admission trend of Biu LGA CMAM program
From November 2013 to December 2013, admissions dropped to zero, reportedly due to stock-out of RUTF at the State, LGA and
health facilities. As RUTF was made available, admissions were observed to rise steadily. However, admissions from January and
OTP Site Exit records Dead Defaulter Non-recovered Recovered
Biu MCH 252 0 120 1 128
Gunda 178 0 69 0 109
Madaragirau 71 0 31 0 38
Miringa 129 0 48 0 81
Yawi 66 1 7 3 55
Total 696 1 275 4 411
Proportion 100% 0.14% 39.5% 0.57% 59.05%
Table 1 Summary of extracted beneficiary information at a glance –May to November 2014.

13
until April 2014 were low compared to the period May–August 2014. This was majorly due to the availability of food in households
during January to March after good harvesting by the end of the previous year. Consequently, when the planting season
commences in May, continuing through July, household food reserves are usually depleted. May to August coincides with the peak
of hunger in Biu LGA. On its side, the rainy season peaks during June and July, and malaria and diarrhea are usually reported during
this season. The increased admission from May to August could thus be attributed to high incidence of malnutrition due to hunger
and poorly treated malaria and diarrhea. The sharp decline in the number of children admitted in September 2014 could be due
to stock-out of RUTF at the LGA and HFs.
6.1.3 Program exits
The trend of exit of the routine performance data was plotted and smoothened with spans of median and average of three months
(M3A3).
Figure 4: Exit trends for Biu LGA CMAM program-November 2013 to October 2014
The recovery rate was observed to be below SPHERE standard (>75%) during almost the whole period, except January and February
2014. On the other hand, defaulters were minimal in November 2013 and until February 2014. Insurgency and rumor of impending
attacks by insurgents were reported to have contributed to the decrease in recovery rate in March – June 2014, as many

14
beneficiaries defaulted during this period. Though the performance indicators improved from July – October 2014, both remained
below SPHERE standard until October 2014. Only the death rate was below the acceptable standard.
6.1.4 MUAC at Admission
Figure 5: Admission MUAC for Biu LGA CMAM program
The median MUAC at admission was found to be 109 mm. This showed that beneficiaries are admitted into the program relatively
early. A relatively early admission indicates good health seeking behavior, and good referrals from communities. However, pockets
of beneficiaries were noticed to have been admitted into the program at a later moment, when cases have deteriorated. This could
indicate poor health seeking behavior and low active case finding in areas where such clients are coming from. Some children were
also observed to have been admitted into the program with MUAC > 115mm. These were triangulated with edema cases at
admission with MUAC >115, and presented in figure 6 below.

15
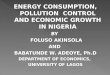
Figure 6: Samples of admissions above 115mm by health facilities. Cross-referencing with Edema.
What the previous graph indicates is that not all cases that were admitted with a MUAC value superior to 115mm presented
Edemas. In other words, there are some persistent problems of wrong admission where kids that do not suffer from edemas and
whose MUAC value is above 115mm are nonetheless admitted.
6.1.5 Length of stay from admission to recovery
Figure 7: Length of Stay in program before recovery
4
0
2
8
6
4
9
2
0
2
4
6
8
10
12
Biu Gunda Mandaragirau Miringa Yawi
M UA C O N A D M I S S I O N ≥ 1 1 5
Oedema cases with MUAC ≥ 115 Total wrong Admissions

16
The analyzed data unveiled a median length of stay (LOS) of 7 weeks. This is considered as being a positive value, unveiling a
relatively well performing program where SAM children are identified on time, come timely to their weekly visits and regain weight
according to expectations.
Simultaneously, some beneficiaries were noted to have been in the program for more than 12 weeks or even more. These were
majorly hidden defaulters, who were not classified as defaulters by the health workers despite having unattended the program for
more than three weeks11. Furthermore, the MUAC value at exit for the beneficiaries who were classified as recovered by the health
workers were also analyzed and shown below in Figure 8. It was suspected that the HWs did not adhere to discharge criteria
according to the National CMAM Guideline, as many children were discharged as recovered while their MUAC was still below 125
mm.
Figure 8: Distribution of the MUAC of children discharged as ‘recovered’
The situation depicted by the graph above is one in which a huge majority of discharged cases are effectively cured (with regards to their
MUAC value of 125mm or above). A smaller proportion is nevertheless discharged with MUAC values below that threshold (15%), although
above the admission level of 115mm, which indicates that the have shown some improvement during the program and are likely to be hidden
defaulters. A negligible share (1%) of cases were discharged below even the admission criteria. These may be non-respondent cases.
11 Hidden defaulters are children who missed a certain number of weekly visits to the OTP and therefore did not receive CMAM services as expected. However, some of this cases do come back to the OTP at some point and fulfil the programme until they are cured. This partly explains longer lengths of stay in the program.

17
6.1.6 Number of visits before default
Figure 9: Plot of number of visits before default
Most of the beneficiaries leaving the program before completion were noticed to be early defaulters. The median number of weeks
SAM children stayed in the program before default was found to be 4 weeks. Early defaulters are likely to be SAM cases12.
Therefore, the MUAC values at default were analyzed and presented in Figure 10 below. The results cross-check and confirm what
the median number of visits before defaulting already suggested: above 50% of identified defaulters leave the program before
reaching MUAC 115mm, and only 13% leave after having reached 125mm, which implies that only one in eight defaulters can be
expected to have successfully cured during the program.
Figure 10: Distribution of Defaulter’s MUAC on exit
6.1.7 Conclusion of the routine monitoring (OTP cards) analysis
The quantitative data analyses gave indications that referral activities, health seeking behavior, adherence to National CMAM
guideline by HWs and general attitudes toward defaulting unveil a certain complexity. There are good indicators of performance,
such as a comparatively high rate of correct discharges and good average length of stay in the program. These are combined with
12Defaulters that have had below 4 visits are likely to be current cases of SAM. Refer to SQUEAC/SLEAC technical manual.

18
stronger challenges, such as the level of defaulting and stock-out of RUTF, which both needed to be investigated further using
qualitative methods.
6.2 Stage 1: Qualitative data
6.2.1 Qualitative sampling Framework
Interviews of different stakeholders in Biu LGA were conducted to gather qualitative information about the CMAM program.
Varying methods were used, while the information obtained was used to complement the quantitative results. The information
was systematized into barriers and boosters, and the evidences were triangulated by sources and methods. As a result of
insurgency in the LGA, only three CMAM sites were visited. In each of the sites, at least four caregivers (randomly chosen), health
workers, and community volunteers were interviewed. Six communities were visited to collect additional information about the
program from community members. These communities were purposively selected based on the distance (far or near) to CMAM
HFs.
At least, one community leader, one religious leader, teacher, provision shop seller, patent medicine vendor, majalisa (community
age-group social gathering in tea places and shades), Okada rider, youth leader, traditional birth attendant (TBA) and traditional
healer were interviewed in each of the communities visited.
The information gathered were discussed in line with the following sub-topics
6.2.2 Knowledge about Malnutrition
From the responses gathered, it was noted that some symptoms of malnutrition are well known in the communities. However,
the causes of these symptoms are not always clearly understood. The local terms for malnutrition are mostly in Bura Language.
Bzirsisi or Hal refers to wasting in children, and is linked to the spiritual realm. This is also similar to Bwilikur which is seen as an
infliction from evil spirits. Sabal or Kishiwili was reported to be malnutrition arising from the child feeding on contaminated breast
milk believed to flow if the lactating mother has intercourse. Kunjiji is described as malnutrition resulting from not eating sufficient
food. Kichiku was the term used to refer to Kwashiorkor. Tamowa (Hausa word) for malnutrition, while Rasil (Hausa word) refers
to malnutrition as a result of poor hygiene. These indicated community members’ perception about malnutrition.
6.2.3 Health Seeking behavior in communities
During the SQUEAC investigation it was found that inhabitants from the majority of communities in Biu LGA visit health facilities
when children fall ill. However, in some communities some respondents said they still visit traditional healers within and outside
the LGA for treatment13. Additionally, some caregivers reported to have visited either a patent-medicine-vendor or a traditional
healer first, but when the child did not recover, they came to the CMAM HF to access treatment. Therefore, health seeking behavior
in the communities are mixed. This confirms the information in Figure 5 and Session 6.1.4.
13In Tum community the community leader and TBA said community members visit traditional healers; In Dugja community the chemist said malnourished children are brought to him for treatment.

19
6.2.4 Awareness of the CMAM program in communities and community mobilization
The interviews conducted revealed that community members are aware of the CMAM services in Biu LGA. However, sensitization
and mobilization were reported to have been conducted only at the inception of the program within the host communities of the
CMAM HFs. Awareness about the program is mostly explained by community members who have noticed beneficiaries accessing
CMAM services and assimilate and share information about the program. Many community members were able to recall the names
of some beneficiaries from their communities who had accessed CMAM treatment. Nevertheless, most interviewees reported
that nobody had come to tell them about the program in their communities. Only the PMV and religious leader from Filin Jirgi
community reported they heard about the program from a CV.
6.2.5 Community volunteer activities
At the inception of the program in 2010, twenty-five community volunteers (CVs) were selected and trained for case-finding in
each of the CMAM HFs. Most of the CVs were reported to have stopped working since 2011 because they were no longer given
incentives by the State or LGA. This led to some health attendants volunteering themselves to work at the health facility as CVs14,
yet they only conduct active case finding in the community where they are residing. The few CVs in Yawi, and Miringa health
facilities also reported that they do not trace defaulters in other communities due to insecurity. Nevertheless, only health workers
confirmed that community volunteers go for active case finding and defaulter tracing. No caregiver interviewed mentioned being
referred by a community volunteer, all were referred by either their peers in the community or by a health worker in a non-CMAM
health facility.
6.2.6 RUTF Supply and availability
The supply of RUTF in Biu LGA was observed to be affected mostly by insurgency. The transportation of RUTF from Maiduguri (the State capital) to Biu LGA (which initially covers a distance of about 188 km), has been lengthened to about 500 km. This was because insurgents attacked and destroyed the Bridge linking Maiduguri to Biu LGA thereby making the journey to be possible only by passing through Gombe and Yobe States. RUTF stock-out was noticed as a strong barrier to good quality service delivery. During stock-outs, caregivers do not access CMAM services because they were not given weekly RUTF ration. On the other hand, fund required to transport RUTF from LGA store to CMAM HFs was not usually provided by the LGA. Therefore HWs resorted to charging fees ranging from N20 - N50 on the beneficiaries weekly to transport RUTF from the LGA to the HFs.
6.2.7 Routine drugs
The LGA was saddled with the responsibility of providing routine drugs to the CMAM HFs since the program commenced in Biu LGA. However, it was evident that routine drugs were not always available. According to the HWs and CVs, there has been stock out of routine drugs since January 2014. Nevertheless, the acting PHC Director and NFP hinted that the stock-out of routine drugs does not affect all CMAM HFs. Some HFs are supported by the MDG and NHIS where they are given free drugs. Notwithstanding, some of the line drugs for CMAM beneficiaries in those that are supported by the NHIS and MDG project are not available, therefore, the beneficiaries are advised to buy the drugs from patent-medicine-vendors in the community.
14 Biu OTP

20
6.2.8 Health Workers activities and training
One or two health workers were found present in each of the CMAM HFs15 visited despite the fact each health facility have at least
four health workers trained on CMAM. From the information gathered it was evident that since the inception of the program
(October 2010) the health workers had been trained only twice, one at the beginning and the last one in October 2011. There was
a scale up of one additional CMAM site16 in March 2014. After the implementation of the CMAM site, no refresher training has
been given to the health workers. Lack of refresher training and on site monitoring from time to time could explain low adherence
to CMAM protocol, as some beneficiaries were admitted into the program with MUAC >115 without edema and discharged with
MUAC <115 —according to the information obtained from the beneficiary cards.
It was also evident that there is a cordial relationship between HWs and CVs. Also, the HWs were seen to have good attitudes
towards caregivers; however, some caregivers complained that HWs give preferential treatment to their relatives. Caregivers also
complained that HWs are not available to provide CMAM services on immunization campaign days. This indicated poor integration
with other child health programs in HFs. Nevertheless, referrals from non-CMAM HFs were evident.
6.3 Data triangulation
The qualitative and quantitative information obtained was analyzed into barriers and boosters, and was triangulated using varying
sources and methods used to obtain such information. The barriers and boosters identified, and the sources and methods used to
obtain such information during the investigation are tabulated in in the tables 3 and 4 below.
CODE SOURCE METHOD CODE
1 Health worker Semi structure interview/ In-depth interview A, D
2 Care-giver Semi structure interview/ In-depth interview A,D
3 Health facility Observation B
4 CVs Semi structure interview/ In-depth interview A,D
5 NFP In-depth interview D
6 PHC Director Biu In-depth interview D
7 Community leader Semi structure interview/ In-depth interview A,D
8 Religious leader Semi structure interview/ In-depth interview A,D
9 Majalisa Informal group discussion C
10 Patent medicine dealer Semi structure interview/ In-depth interview A,D
11 Provision shop owner Semi structure interview/ In-depth interview A,D
12 TBA Semi structure interview/ In-depth interview A,D
13 Okada rider Semi structure interview/ In-depth interview A,D
14 Teacher Semi structure interview/ In-depth interview A,D
15 CHEW Semi structure interview A
16 Health attendants Semi structure interview A
17 Traditional healer In-depth interview D
18 Youth leader In-depth interview D
Table 2 Sources and methods used to get information in the BBQ
15 Yawi, Biu and Miringa health facilities were visited on their OTP days 28th Nov 2014, 1st Dec 2014 and 4th Dec 2014 respectively. At Biu MCH, only one
health worker was present instead of four (one of the health worker lost her relative and the other health worker was absent while the fourth health worker
is involved with the SQUEAC activities) and two were present at yawi (the person in charge was involved in MCH week and the four health worker is in
school) while Miringa CMAM site had four health workers present. 16 Yawi OTP

21
Table 3: barriers, boosters & questions findings and sources of information
S/N BOOSTERS SOURCES BARRIERS SOURCES
1 Passive referral and peer-to-peer referral 1A,2A Lack of refresher training for Health workers on CMAM (training was conducted once since the inception of the program in October 2010)
1A,5D
2 Good opinion about the CMAM program 1A,2A,4A,8A,9C,11A,12A,13A,15A,14A,7A,16A,4D,1A
Stock out of RUTF due to insecurity, poor logistic/ supply chain management from the State to LGA, and from LGA to CMAM HFs. (Sept – October 2013, and September 2014)
1A,3B,4A,16A,1D,4D
3 Community leader and HWs contribute money to transport RUTF from the LGA to Yawi HF.
1A,1D Stock out of routine drugs (Yawi HF). 1A,1D
4 Good collaboration between HWs and CVs 1A,4A,16A, Poor health seeking behavior in some communities
2A,4A,9C,12A,13A,16A,17D,18D
5 Good health seeking behavior in some communities
7A,8A,9C,10A,11A,13A,15A
CVs are not motivated due to lack of incentive 4A, 16A, 1D, 4D
6 Good awareness of the CMAM program in communities
7A,8A,9C,10A,11A,12A,13A14A,15A
Consumption of RUTF by healthy siblings and adults
11A,9C
7 Health workers are friendly towards caregivers 3B, 4D CVs are not present in Biu health facility 5D,16A
8 MDG17/NHIS18 supply free drugs for under five children in some HF which run CMAM.(Biu, Miringa, Gunda and Mandaragirau)
4D,6D poor active case finding and defaulter tracing in the LGA
1A,16A,4D
9 HWs give preference to relatives instead (Biu, Mirinda and Yawi CMAM HFs)
16A,2A
10 Poor community mobilization and sensitization 7A,8A,9C,10A,11A,12A,13A,14A,15A, 11D, 14D, 17D, 18D
11 Lack of shade and sits at CMAM sites 2A,1D,4D,3B
12 Beneficiaries pay for drugs and for transportation of RUTF up to N50 (Miringa CMAM HF)
1D
13 Insecurity in half of the BIU LGA decreasing access to CMAM services and increasing defaulter rates
5D,1A,4A,4D,6D
14 Lack of proper integration with other health programs, especially immunization; HWs do not attend to CMAM beneficiaries on immunization campaign days
5D, 6D
15 Lack of support and funding by the LGA due to change in leadership every six month.
5D, 6D
16 Poor supportive supervision of CMAM HFs due to insecurity in Biu
5D, 6D
17 Millennium Development Goals 18 National Health Insurance Scheme

22
6.4 Concept map
The coverage team drew a concept map to illustrate the relationship existing between the barriers and boosters obtained from
the field. Epigram software-version 1.1019 was used to draw the concept maps presented in the annex 2.
6.5 Stage 2: Small Area Survey and Small Study.
At the completion of stage 1, the major factors that may be affecting coverage in Biu LGA based on the result of analysis of
information gathered were identified. Three factors identified include:
1. Location and accessibility of CMAM Sites
2. Insecurity in communities
3. Defaulting
A hypothesis was formulated and small area survey conducted around each of the factors above, except defaulting. Defaulting was
investigated further using small study.
6.5.1 Small Area Survey
Hypothesis 1: Distance does not play a significant factor in explaining levels of coverage across the intervention area.
According to information obtained during the gathering of qualitative data, distance from each village to the health facility
offering CMAM programs is not determinant for defaulting. It is thus expected for coverage to be homogeneous in near and
far communities within wards hosting the CMAM program in Biu LGA. Coverage in any village will be above 50%20.
Hypothesis 2: Conversely, insecurity has been identified as a major cause of disruption in the provision of CMAM services. It
is expected for coverage within political wards of the LGA where there is no insecurity to be greater than 50%; and in political
wards with insecurity, coverage is expected to range below 50%.
6.5.2 Sampling methodology
Hypothesis 1 was tested by choosing three communities considered to be near, and three more considered to be far within political
wards hosting CMAM services (two communities for each ward). The second hypothesis was tested by selecting three communities
in both the secure and insecure wards. A small area survey was conducted in each of the selected communities to test the
formulated hypothesis. Active and adaptive case-finding was conducted in the communities during the small area survey.
6.5.2.1 Case Definition
Severe Acute Malnutrition (SAM case) was defined as Children (6-59) months, with MUAC <115mm and or bilateral pitting oedema.
19Epigram software was developed by Mark Myatt and is available on www.brixtonhealth.com 20This is based on the 2-standards, 3-classifications setting of coverage. According to this, less than 20% is classified as being low coverage; 20% to 50% as moderate; and greater than 50% as high. This is especially applicable to rural areas.

23
SAM case covered: Refers to a SAM case identified as defined above and is currently enrolled in a CMAM site or Stabilization Centre
(SC). The status is verified when beneficiary shows the investigator the RUTF packets and/or ration Card.
SAM case not covered: Refers to a SAM case who is not currently enrolled in a CMAM program or the SC.
Recovering case: A child (6-59) months old, with MUAC above 115mm and who is enrolled in a CMAM program at the time of the
investigation. This case is verified when beneficiary shows the investigator the RUTF packets and/or ration Card.
6.5.2.2 Result of Small Area Survey
The results of small area survey are presented in the table 5 below.
Table 4: Simplified Lot Quality Assurance classification of small area survey results
Coverage Wards Location Total
SAM
(𝒙)
Decision rule
𝒅 =𝒙 × 𝟓𝟎
𝟏𝟎𝟎
Covered(C) Not covered
(NC)
Recovering case (RC)
Hypothesis
Near communities
(< 5 km from
CMAM HFs)
Zarawuyaku Kogu 0 d = 0 0 0 0
Tabura
Tsahuyam
0 0 0 0
Yawi Kubura 0 0 0 0
Far communities
(> 5 km from
CMAM HFs)
Miringa Maina Hari 5 d = 3 4 1 2
Zarawuyaku Hema 1 1 0 0
Yawi Gura 0 0 0 0
Secured Wards
MIringa Abuja 4
d = 5
4 0 6
Yawi Yawi 1 1 0 0
Zarawuyaku Mbulamel 5 2 3 0
Insecure Wards
Buratai Dora21
Gur Yaulari22
Mandaragirau Barkiyalwa23
21 Could not be accessed due to insecurity. 22 Could not be accessed due to insecurity. 23 Could not be accessed due to insecurity.

24
Figure 9: Reasons for not attending the CMAM program-Small area survey
Interpretation of the results
Hypothesis 1: In near communities, not a single SAM case was found. The team also did not find any recovering case. There is thus no way of classifying any coverage whatsoever. In distant communities, six SAM cases were found. According to this, the decision rule calculated equals 3, and since five SAM cases were found as covered by the program, coverage can be classified as high (five is greater than the decision rule [3]). Hypothesis 2: The number of SAM cases found in communities in political wards without insecurity was 10, which implies that the 50% decision
rule calculated equals five SAM cases. The number of SAM cases covered by the program was seven. Therefore, coverage in wards
without insecurity was classified as being acceptable at above 50% (because seven is greater than 5).
However, the communities in insecure wards could not be visited due to fear of attack by insurgents, so the hypothesis as a whole
could not be confirmed.
6.5.2 Small Study on Defaulters
A small study was done to investigate the reasons for the high default in the CMAM program. A sample of OTP cards for defaulting cases was
made and the conducting team tracked back the cases in their communities so they could have the chance to meet the caregiver. The result
are tabulated below:

25
S/No Age (month)
Location MUAC on Admission
Exit MUAC
Findings Present MUAC (mm)
Action taken
1 22 Biu 112 113 Caregiver stopped attending due to fear of insurgent attack
110 Referred to OTP
2 6 Biu 99 110 Caregiver stopped coming because she did not receive RUTF ration at the CMAM HFs for 2 weeks.
105 Referred to OTP
3 8 Biu 108 118 Dead
4 Biu 106 118 Relocated due to insecurity Nil Nil
5 12 Biu 105 110 Relocated due to insecurity Nil Nil
6 12 Biu 105 105 Relocated due to insecurity Nil nil
7 12 Biu 100 100 Dead Nil Nil
8 8 Biu 108 118 Dead Nil nil
9 18 Biu 113 113 Dead Nil nil
10 24 Bera 112 120 Caregiver defaulted because she thought child has recovered.
112 Referred to OTP
11 15 Bera 104 104 Caregiver stopped attending because she thought her child has recovered.
125 Recovered
12 24 Bera 102 120 Caregiver defaulted because she thought child has recovered.
145 Recovered
13 6 Bera 90 90 Relocated due to insecurity. Nil nil
14 36 Bera 113 113 Dead Nil nil
15 24 Bera 108 108 Relocated due to insecurity Nil nil
16 6 Bera 105 118 Relocated due to insecurity Nil nil
Table 8: Description of defaulters and reasons for defaulting during Small Study on Defaulters.
As observable in the table, a significant amount of defaulting children has been relocated because of insurgency. These cases have
thus abandoned the program for reasons external to service delivery and/or lack of awareness. Other examples of the survey do
suggest, however, that lack of awareness is still a present challenge that has a direct impact on defaulting levels.
6.5.3 Conclusion of Small Area Survey and Small Study The LQAS classification for hypothesis 1 indicated homogeneous coverage above 50% in both near and far communities within wards hosting the CMAM HFs. Nevertheless, the result for hypothesis 2 is inconclusive as communities in insecure wards could not be accessed. Regarding defaulters, it could be seen that most of children were relocated with their due to insecurity. Or else, caregivers cited fear of attack by insurgents as the reason for default.

26
6.6 Developing the prior.
6.6.1 Histogram of Belief.
A histogram of beliefs was constructed with members of the conducting team discussing and reaching consensus on what the most likely level of coverage could be in Biu LGA. Each individual estimated a concrete value on the basis of its perceptions and the information gathered during the previous stages. This was used to construct a histogram of belief of the coverage team. The central tendency of the histogram on the coverage of beliefs was set at 38 per cent with a minimum at 20 per cent and maximum at 60 per cent.
Prior 1: Histogram of belief = 38 per cent
6.6.2 Concept Map
The Coverage team drew a concept map based on the barriers and boosters obtained in the field.
The concept map had a total number of 18 barriers and 14 boosters. The total number of each is calculated by a predetermined
value (in this case, five), which results in the weight of barriers and boosters all together. Since they should represent negative
values, the overall weight of barriers is deducted from 100 (the maximum possible value for coverage). The result is added to the
overall weight of boosters (in this case, 70) and the result is divided by two (see details below).
Prior calculated from concept map Team
𝑐𝑜𝑛𝑡𝑟𝑖𝑏𝑢𝑡𝑖𝑜𝑛 𝑜𝑓 𝑏𝑎𝑟𝑟𝑖𝑒𝑟𝑠 = 18 × 5 = 90
𝑐𝑜𝑛𝑡𝑟𝑖𝑏𝑢𝑡𝑖𝑜𝑛 𝑜𝑓 𝑏𝑜𝑜𝑠𝑡𝑒𝑟𝑠 = 14 × 5 =70
𝑝𝑟𝑖𝑜𝑟 𝑒𝑠𝑡𝑖𝑚𝑎𝑡𝑖𝑜𝑛 =(70 + (100 − 90)
2= 40%
Prior 2: Estimated from Concept map = 40%
6.6.3 Un-weighted barriers and boosters
Following the same path, all boosters and barriers identified by the group are put into the same list. They each receive the same
value (in this case, 6) and the same calculation takes place. The barriers and boosters were consolidated and scored, the maximum
score was scaled so that neither the sum of positive scores nor the sum of the negative scores can exceed 100%. Thus:
𝑀𝑎𝑥𝑖𝑚𝑢𝑚 𝑠𝑐𝑜𝑟𝑒 =100
16= ⌊6.25⌋ = 6
To calculate the contribution of barriers and boosters to coverage:
𝑐𝑜𝑛𝑡𝑟𝑖𝑏𝑢𝑡𝑖𝑜𝑛 𝑜𝑓 𝑏𝑎𝑟𝑟𝑖𝑒𝑟𝑠 = 16 × 6 = 96
𝑐𝑜𝑛𝑡𝑟𝑖𝑏𝑢𝑡𝑖𝑜𝑛 𝑜𝑓 𝑏𝑜𝑜𝑠𝑡𝑒𝑟𝑠 = 11 × 6 = 66
𝑝𝑟𝑖𝑜𝑟 𝑒𝑠𝑡𝑖𝑚𝑎𝑡𝑖𝑜𝑛=66 + (100−96)/2 = 70/2 = 35

27
Prior 3: Prior estimated from un-weighted barriers and boosters = 35%
6.6.4 Weighted barriers and boosters.
The coverage team discussed and weighted each of the barriers and boosters with regards to their perception on the contribution
of each barrier or booster to the coverage of the CMAM program in Biu LGA. To reach on a score, team members discussed
extensively before finally agreeing upon a score. The highest possible score assigned to a barrier or booster was 7 while 1 was the
lowest score.
The table below shows that the weight assigned by the teams and average/final score given to the barriers and boosters.
Table 5: Weighted barriers and boosters of Biu LGA CMAM Program
S/N BOOSTERS
SCORE
BARRIERS
SCORE
1 Passive referral and peer-to-peer referral 7 Lack of refresher training for Health workers on CMAM (training was conducted once since the inception of the program in October 2010)
4
2 Good opinion about the CMAM program 7 Stock out of RUTF due to insecurity, poor logistic/ supply chain management from the State to LGA, and from LGA to CMAM HFs. (Sept – October 2013, and September 2014)
2
3 Community leader and HWs contribute money to transport RUTF from the LGA to Yawi HF.
3 Stock out of routine drugs (Yawi HF). 6
4 Good collaboration between HWs and CVs 1 Poor health seeking behavior in some communities 7
5 Good health seeking behavior in some communities 5 CVs are not motivated due to lack of incentive 7
6 Good awareness of the CMAM program in communities 5 Consumption of RUTF by healthy siblings and adults 1
7 Health workers are friendly towards caregivers 7 CVs are not present in Biu health facility 7
8 MDG24/NHIS25 supply free drugs for under five children in some HF which run CMAM.(Biu, Miringa, Gunda and Mandaragirau)
7 poor active case finding and defaulter tracing in the LGA 7
9 HWs give preference to relatives instead (Biu, Mirinda and Yawi CMAM HFs)
5
10 Poor community mobilization and sensitization 5
11 Lack of shade and sits at CMAM sites 2
12 Beneficiaries pay for drugs and for transportation of RUTF #50 (Miringa CMAM HF)
1
13 Insecurity in half of the BIU LGA decreasing access to CMAM services and increasing defaulter rates
7
14 Lack of proper integration with other health programs, especially immunization; HWs do not attend to CMAM beneficiaries on immunization campaign days
3
15 Lack of support and funding by the LGA due to change in leadership every six month.
1
16 Poor supportive supervision of CMAM HFs due to insecurity in Biu
2
Total 42 Total 67
Overall values for barriers and boosters are calculated following the same proceeding than in previous components of the prior.
Therefore:
24 Millennium Development Goals 25 National Health Insurance Scheme

28
𝑝𝑟𝑖𝑜𝑟 𝑒𝑠𝑡𝑖𝑚𝑎𝑡𝑖𝑜𝑛 =(42 + (100 − 67)
2= 37
Prior 4: Prior estimate from weighted barriers and boosters = 37%
6.6.5 Triangulation of Prior
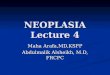
The Prior estimate26 was then calculated by triangulation of all the prior components obtained from various methods. It is
illustrated by figure 10 below.
Prior mode = (38+40+37+35)/4 = 37.5%
Prior mode = 37.5%
Figure 10: Illustration of triangulation of prior
6.6 Discussion
The CMAM program in Biu LGA was noted to be affected mostly by insecurity due to Boko Haram insurgency, which in turn has a
deep impact on accessibility of services and people’s mobility. A likelihood survey could not be integrated into the Biu SQUEAC
assessment due to insecurity in half of the LGA. Thus, the coverage estimate for the LGA could not be arrived at. Many of the
26 The average of the “coverages” is a credible value of the mode of the prior. It is also referred as the mode of the probability density of the coverage.
Belief histogram
38%
Weighted Barriers
&Booster
37%
Un-weighted Barriers
and Booster
35%
Concept Map
40%
PRIOR
37.5%

29
barriers identified in stage 1 were linked to the insecurity in the LGA. However, coverage within the secure wards of the LGA was
believed to be above 50%, as resulted from stage 2.
The prior itself cannot be presented as an estimation of coverage. It responds to the perceptions and understandings of the
conductive team, but its strength is supposed to be checked against the results of a wide area survey —which could not take place
under the present situation.
Nonetheless, the conducting team identified many other barriers during the first stage of the research that can have strong impact
on the levels of coverage and on the performance of the program itself. Poor sensitization and insufficient activities of community
mobilization are probably linked to insecurity and lack of accessibility, but they are also very likely to be important barriers to
access on their own. Interviews and group discussions with beneficiaries and other actors confirmed that barriers such as poor
case finding, little training and retraining of community volunteers, and insufficient activities of sensitization and follow-up of
defaulting cases also have an important explanatory role on the levels of default —which have not been below the SPHERE
standard for over six months.
6.7 Recommendations
In order to improve the Biu LGA CMAM program, a debriefing and participatory recommendation session took place between the
enumerators and LGA staff. The recommendations proffered are tabulated as follows.
Table 6: Proposed recommendations and processes after the conclusion of the assessment
THEME/TOPIC PROCESS VERIFICATION RESPONSIBLE PARTY
EXPECTATION
1 Refresher training and reorientation of HWs on CMAM
Selection of HWs for training on CMAM. Conduct training for HWs
Comprehensive list of HWs trained on CMAM. Training modules developed
SMoH/ UNICEF
Sufficient health worker trained on CMAM at all CMAM site Adherence to National CMAM protocols.
2 Communization Mobilization and Sensitization. Awareness
Complete list of all the villages in all Wards stratified by the OTPs under Biu LGA. Schedule meeting with gatekeepers (community leaders, TBA, Traditional healer, patent medicine dealer, Religious leaders Women group) of all targeted community to enlighten them on how the program works. Key messages, IEC materials
Meetings with traditional leaders and religious leaders. Minute of meeting Minute of meeting and list of participates
SMoH through SNO, State Health Educator, LGA PHC, and NFP
Decentralized Community mobilization and sensitization in all the villages in the LGA. Enhance Knowledge on how the program works. Decrease in consumption of RUTF by healthy siblings and adults Decrease in number of defaulters as the beneficiaries understand how the program works.

30
Community town hall meeting to enlighten them on how the program works. Sensitization talks using town criers. Talk shows. Jingles on the need for a good pathway to health
Samples of Talk shows, Jingles. Pictorial aids and IEC materials used for sensitization on good pathway to health seeking behavior
The targeted communities follow a good pathway to health/good health seeking behavior.
3 Routine drugs Advocacy to LGA chairman for ownership, Create a budget line for purchase of routine drugs
Stock of drugs in OTP used for CMAM treatment.
SNO, LGA PHC coordinator and NFP
4 Supply chain management of RUTF
Advocacy to LGA chairman for ownership. Budget from source. Schedule of transportation .
Presence of RUTF at all times at OTP
SNO, LGA PHC coordinator and NFP
5 Improved community volunteer activities
Recruitment/selection of willing community members for indoctrination as CVs into the Biu CMAM program Training of CVs on how to measure MUAC. Training of CVs on the importance of active case finding and defaulters tracing.
List of participate and modules used for training
SNO, LGA PHC coordinator and NFP with funding from UNICEF
Sufficient CVs trained on proper measurement of MUAC tape. Increase in active case finding and defaulter tracing. Increase in referrals of SAM cases by CVs Adherence to National CMAM protocols.
6 Supportive supervision. Create an LGA work plan on supervision. Integration of LGA supervision with the State Conduct joint supportive supervision
Work plan developed Number of CMAM HFs supported quarterly Number of joint supportive supervision held
LGA PHC coordinator, LGA M&E Officer, NFP SMoH (SNO and State M&E Officer)

31
7.0 Annexure
7.1 Annex1: Schedule of implemented activities in Damaturu SQUEAC.
Date Activity/Villages visited HF Sources of information
15/11/2014 SQUEAC team travel from Abuja to Gombe, Gombe
state
16/11/2014 SQUEAC team travel from Gombe, Gombe state to
Maiduguri Borno State
17/11/2014 Preliminary meeting with Director Primary Health
Care, Agency and State Nutrition Officer
18/11/2014 19/11/2014 20/11/2014 21/11/2014
Data extraction Biu HF, Gunda HF, Mandaragirau HF, Miringa HF, Yawi HF
OTP cards
24/11/2014 25/11/2014
SQUEAC training
Visit to Nutrition & Rehabilitation Center, Song,
conduct practical on MUAC standardization and
qualitative information gathering.
De Grand Apartment, Gombe.
20 Enumerators, Nutrition Focal
Person and PHC coordinator Biu
LGA
28/11/2014 Yawi HF,
Near community (hema) <3km to OTP,
Far community (filin jilgi) <9km to OTP
Yawi HF 2 religious leader
2 community leader
2 Majalisa (25 to 50 years)
2 patent medicine dealer
2 traditional birth attendance
2 Teacher
2 provision store dealer
4 health workers
4 community volunteers
6 care-givers
01/12/2014
Biu HF,
Near community (Bayan tsha) <3km to OTP,
Far community (Tum) <10km to OTP
Biu HF
2 religious leader
2 community leader
2 Majalisa (25 to 50 years)
2 patent medicine dealer
2 TBA
2 Teacher
2 provision store dealer
4 health workers
4 community volunteers
4 care-givers
CHEW

32
02/12/2014
Update BBQ Conduct in-depth interview on program staff: , NFP & Acting Director Primary Health care development Agency Biu LGA
Program Staff
okada
NFP and Acting DPHCDA Biu LGA
04/12/2014 Miringa HF,
Near community (maina hari) <3km to OTP,
Far community () <15km to OTP
Miringa HF 2 religious leader
2 community leader
2 Majalisa (25 to 60 years)
1 patent medicine dealer
2 traditional birth attendance
1 traditional healer
2 Teacher
2 provision store dealer
4 health workers
4 community volunteers
4 care-givers
05/12/2014 Update BBQ Conduct in-depth interview on program staff: , NFP & Acting Director Primary Health care development Agency Biu LGA
Program Staff
06/12/2014 Defaulters tracing Biu HF Coverage team
08/12/2014 09/12/2014 10/12/2014 11/12/2014 12/12/2014
Communities visited: maina hari, hema, kogu, tabura, tsahuyam, yawi,yawi Fulani, gura, yawulari, mbulamel,
Catchment area to the following CMAM site; Miringa and Biu HF
Small area survey
13/12/2014 Drawing of concept map
Weighed BBQ Coverage team
15/12/2014 Technical report writing
16/12/2014 Coverage team travel back to Abuja

33
7.2 Annex 2: Concept maps Figure 11: Concept map showing the relationship between factors affecting CMAM program and coverage
COVERAGE
Early Admission
Good collaboration between HWs & CVs
Good health seeking behaviour
MDGs/NHIS supply free drugs to CMAM site
Good community mobilization & sensitization
Double ration of RUTF
Community leader contributes in transportation of RUTF to HF
HWs friendly to caregivers
Active case findingShort LOS
Passive referral
Good Opinion
Peer to Peer referral
Good awareness
No refresher training for HWs
Lack of community mobilization
Lack of shades, benches & mats
Poor logistics
Incured charges for transportation of RUTF
Consumption of RUTF by adults
Non adherance to CMAM protocol
CVs clamouring for incentives Insecurity
Stockout of Routine drugs
Poor health seeking behavoiur
Stockout of RUTF
Defaulter
Lack of CVs
HWs given preference to relatives in services
increases
leads toleads to
increases
leads to
leads to
Access
limits
inhibits
leads to
leads to
leads to
promotes
results
promotes
encourages
increases
leads to
encourages
increases
leads to
reduces
stops
increases
leads to
leads to
Lack of support & funding by LGA
No proper integration with other health programs
associated with
limits
leads to
hinders
No supportive supervision
leads to
leads to

34
7.3 Annex 3: Active and adaptive case finding procedure27.
27 Local terms of malnutrition used are from Damaturu LGA in Yobe state, Northern Nigeria.
Check the child is aged between 6 and 59 months
Explain the purpose of the survey to the parents and what you will do
Measure the MUAC of the child
Check for the Oedema sign
Visit the community gathering place first and seek permission to visit the village.
Request the village leader to provide a key informant of choice.
Ask the key informant the case finding question ‘can you show us child who is under-five years and is ‘Tamowa, Datti, rana
(wasting, skiny or drying-up), iska (possession by evil spirit), tsunburarre (Hausa)-‘shrinking and or dryness’ &Ciwon yunwa
(Hausa word for hunger). Bajul (Fulani word foroedema), and tuhundi- Fulani words for different types of malnutrition.
Kadawu (Kanuri word for wasting), Kumberi (oedema), Kinna (hunger),
”
Go to the first house where a potential case may be found
Does the child have bilateral Oedema or is the MUAC < 115mm?
Not a Current SAM case
Is the child in OTP?
Ask to see sachet of RUTF and health card
Current SAM case
Is the child in OTP?
Ask to see sachet of RUTF and health card
Current SAM case not in the program
1. Fill out the tally sheet 2. Apply questionnaire 3. Refer the child to
CMAM program site 4. Thank the caregiver
5. Ask case finding question
Current SAM case in the program
1. Fill out the tally sheet
2. Thank the caregiver
3. Ask case finding question
RecoveringSAM case
1. Fill out the tally sheet 2. Thank the caregiver
3. Ask case finding question
Normal child, No history of SAM
1. Not included in the study.
2. Thank the caregiver
3. Ask case finding question
Use additional sources or other key informants to inform and improve the search
Always ask parents of the SAM children identified whether they know of other cases
Continue until no new cases are indicated by any source or all leads point to previously identified cases

35
7.5 Annex 4: Seasonal Calendar of events in Biu LGA