Embed Size (px)
Citation preview

Case Report
Self-Management of Nocturnal Respiratory Insufficiency with aPortable Ventilator "Pneu-PAC" by an Amyotrophic
Lateral Sclerosis Patient
Kiyoshi HOSHINO, Arihiko KURODA, Yutaka MlZUSHIMA,
Toshihiko MORIKAGEand Saburo YANO
A 76-year-old man with amyotrophic lateral sclerosis was admitted to our hospital because of progressiveexertional dyspnea (PaCO2=68.5 torr, PaO2=62.5 torr). He was put on mechanical ventilation, and
thereafter sleep apnea of a central type was recognized. After improvement of general conditions, a portableventilator "Pneu-PAC" was used for the self-management of nocturnal respiratory insufficiency. A portableventilator might be of clinical benefit for the managementof a patient with neuromuscular disorder whoseactivities of daily living are still functional.
Key words: Neuromuscular disease, Sleep apnea, Managementof respiratory insufficiency
The "Pneu-PAC"is a portable ventilator usuallyused for emergency resuscitation. Wereport hereina case of amyotrophic lateral sclerosis (ALS)presenting with exertional dyspnea as a primarycomplaint, in which the Pneu-PAC device was usefulfor the self-management of nocturnal respiratoryinsufficiency.
CASE REPORT
A 76-year-old manwas admitted to our hospitalon November 29, 1988 for a detailed examinationof exertional dyspnea, loss of body wt, and a highlevel of serum creatine phosphokinase (CPK).Arterial blood gas analysis on admission revealedhypercapnia (PaCO2=49 torr, PaO2=80 torr).
Spirometry showed a restrictive ventilatory defect(<7oFVC=59.2%, FEV1>0% =82.4%). Chest roent-genogram showed no abnormal findings. Physicalexamination revealed atrophy of the chest muscles,but no abnormality was detected by electromyo-graphic (EMG) or neurological examinations.
Laboratory data suggested mild hypothyroidism,and a thyroid biopsy revealed features of chronicthyroiditis (Table 1). The high level of serum CPK(268 IU/1) returned to normal soon after admission.He was clinically diagnosed as having chronicthyroiditis and thyroid myopathy. He was dis-
charged on December29, and treated as an out-patient with Levothyroxine sodium (Thyradin S).However, his condition progressively deterioratedand he was hospitalized again on June 23, 1989. Hecomplained of a 13.5 kg wt loss in the previous 8months (ht 159 cm, wt 46.5 kg). Pulse rate was
84/min with normal rhythm, blood pressure 125/70mmHg, and respiration rate was 32/min andshallow. Arterial blood gas levels were PaCO2 68.5torr, PaO2 62.5 torr. Atrophy of the chest muscleswas marked. As shown in Table 2, deep tendonreflexes were brisk, and some pathological reflexeswere positive, but no sensory disturbance could beobserved. General muscle weakness was minimal.Bulbar paralysis was not evident. The EMGfindings
From The First Department of Internal Medicine, Toyama Medical and Pharmaceutical University, ToyamaReceived for publication February 23, 1990; Accepted for publication October 25, 1990Reprint requests should be addressed to Kiyoshi Hoshino, MD,The First Department of Internal Medicine,
Toyama Medical and Pharmaceutical University, 2630 Sugitani, Toyama 930-01, Japan
260 Jpn J Med Vol 30, No 3 (May, June 1991)

Pneu-PAC for Respiratory Insufficiency
Table 1. Laboratory data on first admission
R B C 4 2 9 x l O 4 / m m 3 T h y r o i d t e s t 4 0 2
H b 1 3 .2 g / d l M ic r o s o m e te s t 3 2 O 2
P I 1 8 . 4 x l O 4 / m m 3 T S H 7 . 1 m c V / m l
W B C 5 7 x l O 2 / m m 3 T 3 R S U 2 5 .6 %
C R P 0 . 3 m g / d l 1 4 0 n g / d l
E S R 2 7 m m / h 7 . 7 m c g / d l
f - T , 2 . 8 p g / m l
T -P 7 . 1 g / d l f- T 4 0 .8 n g / d l
G O T 2 2 K U
G P T 1 4 K U
L D H 1 8 9 IU / 1 U r in a ly s i s : o c c u lt b l o o d ( + )
A l -P 6 . 2 K A U E C G : n o r m a l
C P K
N a
2 6 8 IU / 1
1 4 4 m E q / 1T h y r o id e c h o g r a m
K 4 . 6 m E q / 1 C h r o n ic th y r o i d it is s u s p .
a 1 0 6 m E q / 1 T h y r o i d b i o p s y
C a 9 . 6 m E q / 1 C h r o n ic th y r o i d it is
p 3 . 9 m E q / 1
B U N 1 7 m g / d l E le c t r o m y o g r a m : n o r m a l
C r 0 . 9 m g / d l M o t o r n e r v e c o n d u c t i o n v e l o c i t y : n o r m a l
L u n g fu n c t io n A B G 's
F V C 1. 8 2 1 p H 7 . 3 7 8
F E V l. 0 1. 5 0 1 P C O o 4 9 t o r r
% F V C 5 9 . 2 % P O 2 8 0 t o r r
F E V , 8 2 . 4 % H C O , 2 8 . 2 m E q / 1
B E 2 . 4 m E q / 1
Table 2. Neurological findings on second admission
Bulbar signs
Speech disturbance (± ) Cerebellar ataxia (-)Dysphagia ( ± ) Extra-pyramidal sign (-)Tongue atrophy ( ± ) Bladder-rectum disturbance (-)
Upper motor neuron signs Ophthalmoplegia (-)Deep tendon reflex (t ) Grip strength: R=20kg, L=20kg
Pathological reflex (+ ) Gait disturbance (-)Lowermotor neuronsigns Autonomicnerve disturbance (-)
Muscle atrophy (+ ) Electromyogram: Neurogenic changes (+ )Fasciculation (+ ) Intercostal muscle biopsy:
Neurogenic atrophy
Pathological reflexesHoffman R/L (-)/(-)
Wartenberg R/L (-)/( + )Babinski R/L (+)/(±)
Chaddock R/L ( + )/(-)Clonus R/L ( + )/(-)
Plantar R/L (-)/(-)
Jpn J Med Vol 30, No 3 (May, June 1991) 261

Hoshino et al
indicated that the pattern of muscle atrophy wasneurogenic, and biopsy of the intercostal musclesalso demonstrated features of neurogenic atrophy.These data supported a diagnosis of ALS.
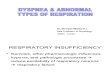
Laboratory data showed a high level of serum CPKand a low level of free T4 (Table 3).He was initially treated with Doxapram, and hisarterial blood gases improved (Fig. 1). On June 29,the ventilatory response test was performed withCHEMOTEST 531 (NEC San'ei Instrument Ltd.,Japan) (1, 2), and markedly depressed ventilatoryresponses to hypercapnia and to hypoxia weredemonstrated (Fig. 2). In isocapnic condition the ex-piratory volume/min (Vg) did not increase inresponse to progressive hypoxia (Ave), and innormoxic condition the VE did not increase in
response to progressive hypercapnia (Sve). A few
days thereafter, the PaCO2 increased to over 80
torr, and his dyspnea became severe. On July 6, atracheostomy was carried out, followed by assistedventilation with a Bennett 7200a ventilator. Underthe management of pressure support ventilation, thealarm warning of an over 20 s apnea was frequentlysounded during the night. In a sleep apnea studywith a thermistor and chest-band, apnea over 10 swas recorded 58 times/night, and he was diagnosedas having sleep apnea of a central type. Accordingly,he was put on controlled ventilation during only thenight. Following this regimen, his general conditionsteadily improved to the extent that he could walkaround the ward in the day. He was then taught touse a Pneu-PACto manage his nocturnal respiratoryinsufficiency by himself, and he became skillful athandling the device (Fig. 3). But he refused to have
Table 3. Laboratory data on second admission
R B C 4 0 4 x 1 0 4/ m m 3 T h y ro id test 2 0 2
H b 1 2. 0 g /d l M icr o so m e te st 3 20 2
P I 16 .5 x lO V m m 3 T S H 0 . 8 m c V / m l
W B C I
4 7. 9 x lO 2/ m m 3 T 3-R S U 2 6 .9 %
C R P 0 . 3 m g / d l f-T , 2 .6 p g / m l
E S R 1 5 m m / h f-T 4 1 .0 n g / d l
T -P 6. 3 g / d l R A H A < 4 0 x
G O T 2 2 K U A N A < 2 0 x
G P T 2 0 K U A n t i - D N A A b 8 0 x
A l-P 5 . 0 K A U A n t i - E N A A b
L D H 1 49 IU / 1 E N A < 4 0 x
C P K 34 9 IU / 1 R N A s e r e s i s t a n t < 4 0 x
N a 1 4 3 m E q / 1 C H s n 4 2 U / m l
K 4 .9 m E q / 1
c ¥ 1 0 0 m E q / 1 U rin a ly sis n o rm a l
C a 8 .9 m E q / 1 E C G n o rm a l
p 4. 1 m E q / 1
B U N 2 0 mg / d l
C r 0 .9 m g /d l
L u n g fu n ctio n
F V C 1. 0 2 1 A B G 's
F E V i.o 0.82 1 P H 7 .3 2 3
% F V C 3 1. 5 % P a C O ? 6 8 .5 to rr
F E V l.0-7o 8 0 .3 % P a O , 6 2 .5 to rr
H C O 3 3 5 . 8 m E q / 1
V T 33 2 .2 m l B E 7 . 7 m E q / 1
v E 9 .9 7 I/ ml
R R 3 0 /m in V en tilato ry resp o n se te st
v o 9 2 8 9 . 5 m l /m i n h y p erc a p n ic d riv e : n o re sp o n se
v c o , 2 4 1 . 6 m l/ m i n hy po x ic d r iv e: lo w r es po n se
R Q 0. 8 3
262 Jpn J Med Vol 30, No 3 (May, June 1991)

Pneu-PAC for Respiratory Insufficiency
June 23,'89 July 6 August 14 August 28
Admission Tracheostomy
Oo x a pr am _____________________________________ Treatment 1 I j Pressure Support Ventilation Control Ventilation Pneu PAC __ (n'ght on|y) (night only) nasal 1l/min 02 Tl FCfeiSl /W350m,N /W400m.\
\ RR12 / \ RR19 J
torr
PaO2 90- y V^^ y
Jla
S0J70-1\ / \ \j^
6o- \ / \'
50- ^ ' a.^
40- I / s> ^ ^-~ - ^
Fig. 1. Clinical course.
50-1 (A) 50-
40- 40-
| 3D- AVe=1 30- SVe=-°'W
.£ 20- 20'
io- t..' å «.à"*.>.*/. t. io-
-' :'' .. ..- .. - *-H ^-
o L, , , ,-_t , o I-, t , ,40 80 120 160 200 240 40 50 60 70
50-1 (B) 50-
Sve=0.8240- 40-
-S Ave= 58
g. 2o- y 20- >^r10- \r.... . 10- -t-^H-^^^V
OH . 1 1 1 1 0' å à" 1
40 80 120 160 200 240 40 50 60 70
PETO2 (TORR) PETCO2 (TORR)
Fig. 2. Ventilatory responses to hypoxia and hypercapnia (A) thiscase, (B) normal control. Ave, parameter of ventilatory response to theisocapnic progressive hypoxia; Sve, parameter of ventilatory responseto the normoxic progressive hypercapnia; PetO2> end-tidal O2pressure;
PETCO2, end-tidal CO2 pressure. Ave was obtained by hyperbolicregression analysis and Sve by linear regression analysis.
PETOV2e- 32' VE = Sve(PETCO2- C) + B
Jpn J Med Vol 30, No 3 (May, June 1991) 263

Hoshino et al
Fig. 3A. Pneu-PAC ventilator. Fig. 3B. The patient managing his ventilationwith Pneu-PAC.
home respiratory care because of the strong fear ofunexpected troubles at home. On November14,1989, he was transferred to another hospital. Mean-
while, his respiratory condition improved to theextent which he could manage to live without theuse of Pneu-PAC even at night in hospital.
DISCUSSION
Respiratory failure is a commonfeature of ALSin the end-stage of the disease (3). ALS with exer-tional dyspnea as an initial symptomis not common
(4-10). Therefore cases with no bulbar signs aresometimes mis-diagnosed as chronic obstructive
pulmonary disease (COPD)or pulmonary emboli.This case had chronic thyroiditis (Hashimoto's
disease), therefore on the first admission, it was mis-interpreted that his symptoms might be derived fromthe thyroid myopathy. ALSaccompanying auto-immunedisease such as Hashimoto's disease alsoseems very rare.This patient was successfully weaned from theventilator during the day time, but mechanical
ventilation was required during the night because ofsleep apnea. In the report of Sivak and Streib (8)on the long-term managementof respiratory failurein ALS, two out of six patients received night-timeventilation. However, no detailed explanation wasincluded. Haward et al (ll) reported 3 cases withsleep apnea and 4 cases with nocturnal hypoventila-tion in 14 cases with motor neuron disease. Noctur-nal respiratory insufficiency might occur frequentlyin ALS patients. Thorpy et al (12) reported the im-
portance of managing nocturnal respiratory in-
sufficiency in a case of non-obstructive hypoventila-tion associated with diaphragmatic paralysis. Theyspeculated that daytime alveolar hypoventilationmight be sleep-induced, possibly due to anaccumulation of bicarbonate resulting in a reduc-tion of respiratory center sensitivity. In the presentcase, significant improvements in symptoms anddaytime blood gasses were also observed bychanging the pressure support ventilation to the con-trolled ventilation during the night. The reasonswhy nocturnal respiratory insufficiency is oftenassociated with ALS have not been made clear.Probably, this is due to the fact that respiratorymuscles responsible for non-voluntary respirationmay be more severely affected than those responsiblefor voluntary respiration. Accumulation and evalua-tion of neuropathological studies are necessary.
The Pneu-PAC (Pneupac Ltd., England) is a
volume-cycled, positive pressure ventilator mainlyused for resuscitation and ambulance service (13,14). The performance characteristics of Pneu-PACare as follows: frequency, ll.5-31 cycles/min; tidalvolume, 230-1,370 ml; minute volume, 6.5-15.7 1;inspiration time, 0.32-2.0 (s); expiration time,1.6-3.2 (s), and inspiration flow rate, 40 1/min.
This device consists of two units, the control moduleand the patient valve (Fig. 3A). The control moduleis light (1.3 kg) and compact (182x 94x60 mm) forpatients to carry and store at their bedside, and alsostrong enough to withstand being knocked over ordropped. It is easy to operate because it has onlyone switch to adjust the respiratory rate and tidal
volume. However, it has some disadvantages for
264 Jpn J Med Vol 30, No 3 (May, June 1991)

Pneu-PAC for Respiratory Insufficiency
long-term use. 1) It has no adaptator for humidifica-tion, thus dry air enters the airway directly. 2)
Respiratory rate and tidal volume are fixed at cer-tain magnitudes, therefore patients maynot be ableto regulate the device for their optimumrespiratorycomfort. 3) It is a gas-powered ventilator, so that
large volumes of gas or an air compressor is re-quired. Regarding the first point, this could be over-come by the use of a Thermovent (Portex Ltd.,
England) and frequent nebulization during thedaytime.
This portable ventilator is easy to operate evenfor aged persons. Therefore, this device may beapplicable for homerespiratory care in patients withneuromuscular diseases with a functional active dailylife. In particular, this device may be useful forpatients who wish to stay at homefor a short period.Another merit of this device is that one can avoidthe long-term use of muchmoreexpensive non-portable ventilators. The cheaper portable ventilatorshould be of great help for hospitals that can notafford to have additional non-portable ventilators.Recently, some improvements have been made onthis model, and a new model with an alarm systemis currently available. A portable ventilator could
be of clinical benefit for the management of
respiratory insufficiency in certain patients.
REFERENCES
1) Asahi T, Ohgaku S, Sawa T, Morioka H, Yano S.Evaluation of the respiratory responses in diabetics bythe ventilatory response test (CHEMOTEST). DiabeticRes Clin Pract 5: S441, 1988.
2) Nishimura M, Miyamoto K, Suzuki A, et al. Ventilatoryand heart rate responses to hypoxia and hypercapnia
in patients with diabetes mellitus. Thorax 44: 251 , 1989.Sivak ED, Gipson WT, Hanson MR. Long-term
managementof respiratory failure in amyotrophiclateral sclerosis. Ann Neurol 12: 18, 1982.Miller RD, Mulder DW, Fowler WS, Olsen AM. Exer-tional dyspnea: Primary complaint in unusual cases of
progressive muscular atrophy and amyotrophic lateralsclerosis. Ann Intern Med 46: 119, 1957.Goldstein RL, Hyde RW, Laoham LW, Gazioglu K,
dePapp ZG. Peripheral neuropathy presenting withrespiratory insufficiency as the primary complaint. Am
J Med 56: 443, 1974.
FrommGB, Wisdom PJ, Block AJ. Amyotrophiclateral sclerosis presenting with respiratory failure. Chest
71: 612, 1977.
Parhad IM, Clark AW, Barron KD, Staunton SB.Diaphragmatic paralysis in motor neuron disease.Neurology 28: 18, 1978.
Sivak ED, Streib EW.Management of hypoventilationin motor neuron disease presenting with respiratory in-
sufficiency. Ann Neurol 7; 188, 1980.Daras M, Spiro AJ, Swerdlow M. Respiratory failurein amyotrophic lateral sclerosis. NY State J Med 84:
570, 1984.
Meyrignac C, Poirier J, Degos JD. Amyotrophic lateralsclerosis with respiratory insufficiency as the primary
complaint. Eur Neurol 24: 115, 1985.Haward RS, Wiles CM, Loh L. Respiratory complica-
tions and their managementin motor neuron disease.Brain 122: 1155, 1989.Thorpy MJ, Schmidt-Nowara WW, Pollak CP,
Weizman ED. Sleep-induced non-obstructive hypo-ventilation associated with diaphragmatic paralysis. Ann
Neurol 12: 308, 1982.
Adams AP, Henville JD. A new generation ofanaesthetic ventilators. The Pneupac and Penlon A-P.
Anaesthesia 32: 34, 1977.
Harber T, Lucas BGB. Instruments and techniques. Anevaluation of somemechanical resuscitators for use in
the ambulance service. Ann R Coll Surg Engl 62: 291,1980.
Jpn J Med Vol 30, No 3 (May, June 1991) 265





![[Product Monograph Template - Standard] - Roche … and Packaging section of the product monograph Severe respiratory insufficiency ... Sleep apnea syndrome Myasthenia gravis](https://img.pdfslide.us/doc/110x75/5ae5e3e07f8b9acc268c9f1c/product-monograph-template-standard-roche-and-packaging-section-of-the.jpg)