Embed Size (px)
Citation preview

SELF-ASSESSMENT
Answer sheets are bound into the Journal for US, Canadian, and life members of the American Academyof Dermatology. Additional answer sheets may be obtained by contacting the Member Resource Centerof the American Academy of Dermatology by calling toll-free (866) 503-SKIN (7546), by calling (847)240-1280 (for international members), or by e-mailing [email protected]
Self-Assessment examination of the AmericanAcademy of Dermatology*
Identification No. 805-211
Learning objectives: At the conclusion of this self-assessment learning activity, physician participants shouldbe able to assess their own diagnostic and patient management skills with respect to those of theircolleagues in their field, use the results of the self-assessment to help determine personal learning needsthat can be addressed through subsequent CME involvement, and enhance their ability to comply with therequirements for certification in the specialty of dermatology.
Instructions for Category I CME credit appear in the front advertising section. See last page of Contents forpage number.
Instructions: In answering each question, refer to the specific directions provided. Because it is oftennecessary to provide information in questions occurring later in a series that give away answers to earlierquestions, please answer the questions in each series in sequence. ( J Am Acad Dermatol 2005;53:925-30.)
Tumor of the eyelid
Ashley Jones, BS, and Hobart W. Walling, MD, PhDIowa City, Iowa
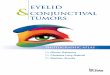
A 64-year-old white woman presented with a slow-growing, tender, draining nodule of 2 years’ durationin her left upper eyelid, initially treated as a chalazion,but with no improvement. On examination, a 6-mm,firm, yellow, mamillated papule with an induratedbase was noted on the left upper lid margin (Fig 1).There was no peripheral adenopathy. A biopsy wasperformed for histopathology (Figs 2 and 3).
1. The most likely diagnosis is (Choose single bestresponse.)a. basal cell carcinomab. sebaceous cell carcinomac. Merkel cell carcinoma
*The Self-Assessment and recertification Education Task Force
of the American Academy of Dermatology is led by Mary C.
Spellman, MD.
J AM ACAD DERMATOL
d. squamous cell carcinomae. syringoma
2. What is the most common malignancy of theeyelid? (Choose single best response.)a. Sebaceous cell carcinomab. Melanomac. Basal cell carcinomad. Squamous cell carcinomae. Merkel call carcinoma
3. Which of the following glands are NOT associ-atedwith theeyelid? (Choose single best response.)a. Krause’s glandsb. Moll’s glandsc. Glands of Zeisd. Meibomian glandse. Bartholin’s glands
4. Lymphatic drainage of the eyelids is by the(Choose single best response.)a. preauricular and postauricular nodesb. postauricular and submandibular nodes
NOVEMBER 2005 925

J AM ACAD DERMATOL
NOVEMBER 2005
926 Self-Assessment examination
c. submandibular and submental nodesd. preauricular and submandibular nodese. submental and preauricular nodes
5. In performing operation on the lower eyelid,which branch of the trigeminal nerve is atgreatest risk of injury? (Choose single bestresponse.)a. Infratrochlearb. Infraorbitalc. Supratrochleard. Lacrimale. Mental
6. What is the most common site of sebaceouscarcinoma? (Choose single best response.)a. Earb. Trunkc. Eyelidd. Extremitiese. Genitalia
7. What syndrome is characterized by the pres-ence of sebaceous carcinoma and internalmalignancies? (Choose single best response.)a. Gardner’s syndromeb. Muir-Torre syndromec. Cowden syndromed. Peutz-Jeghers syndromee. Birt-Hogg-Dube syndrome
8. What is the internal malignancy most com-monly associated with sebaceous carcinoma?(Choose single best response.)a. Lungb. Colorectalc. Breastd. Urogenitale. Stomach
9. What is the primary modality for treating seba-ceous carcinoma? (Choose single best response.)a. Chemotherapyb. Radiationc. Operationd. Exenteratione. Intralesional methotrexate
10. The histologic differential diagnosis of seba-ceous carcinoma is least likely to include (Choosesingle best response.)a. clear cell basal cell carcinomab. trichilemmal carcinomac. Merkel cell carcinomad. metastatic clear cell carcinoma from a visceral
primary tumore. verrucous carcinoma
11. Sebaceous carcinoma is most likely to stainpositively for what immunohistochemical stain?(Choose single best response.)a. S-100b. Carcinoembryonic antigenc. Epidermal membrane antigend. Gross cystic disease fluid protein-15e. Vimentin
12. Which of the following is true regarding mor-tality? (Choose single best response.)a. Squamous cell carcinoma [ melanoma [
sebaceous cell carcinoma[ basal cell carci-noma
b. Sebaceous cell carcinoma [ melanoma [squamous cell carcinoma[ basal cell carci-noma

J AM ACAD DERMATOL
VOLUME 53, NUMBER 5
Self-Assessment examination 927
c. Melanoma[sebaceouscell carcinoma[squa-mous cell carcinoma[basal cell carcinoma
d. Melanoma [ squamous cell carcinoma [sebaceous cell carcinoma[ basal cell carci-noma
e. All have approximately the same mortality
13. A full-thickness defect involving 50% of thelower eyelid is best repaired by (Choose singlebest response.)a. granulation/secondary intentionb. primary lid margin repairc. primary lid margin repair and a Tenzel flapd. tarsoconjunctival advancement flape. paramedial forehead flap
DiscussionSebaceous carcinoma is a rare malignancy that
typically originates in the tarsal meibomian glands,or less commonly in the glands of Zeis or carunclesof the eyelids. It is more prevalent in the uppereyelid than the lower eyelid, possibly because of thegreater number of meibomian glands in this region.Eyelid sebaceous cell carcinoma is often clinicallymisdiagnosed as other periocular diseases, such asrecurrent chalazion, blepharitis, tarsitis, and con-junctivitis. Extraocular sebaceous cell carcinomaaccounts for approximately 25% of reported cases.The prognosis of sebaceous carcinoma is guardedin part because of its tendency to metastasizeearly and in part as a result of common delays indiagnosis.
Sebaceous carcinoma is the fourth most commoneyelid malignancy after basal cell carcinoma, squa-mous cell carcinoma, and melanoma. It accountsfor 1.0% to 5.5% of malignant eyelid tumors. Riskfactors include ionizing radiation, age older than50 years, and Asian descent.
The diagnosis of sebaceous carcinoma is con-firmed histopathologically. Microscopically, seba-ceous carcinoma typically reveals neoplastic cellsin well-circumscribed lobules. Within the lobulestwo types of cells are present, those with foamycytoplasm and those with eosinophilic cytoplasm.Both populations demonstrate atypia and frequentmitoses. Other less common cytologic patterns in-clude comedocarcinoma, papillary, and mixed. Redoil O or Sudan IV stains enhance the characteristicfoamy, lipid-laden cells. Immunohistochemistry maybe used to distinguish the tumor from histologicmimickers, including balloon cell melanoma, clearcell basal or squamous cell carcinoma, trichilemmalcarcinoma, or metastatic clear cell carcinoma.Sebaceous carcinoma typically stains positively withepithelial membrane antigen. In addition to the
meibomian glands of the eyelids, sebaceous glandsare also found at the vermilion lip (Fordyce glands)and areola (Montgomery’s glands).
Sebaceous carcinoma treatment is appropriatelytreated by surgical excision, preferably Mohs micro-graphic surgery, or local excision with a 5- to 6-mmmargin. The recurrence rate with Mohs micrographicsurgery is lower than with wide local excision; 11%and 32%, respectively. Nerve injury is a commoncomplication; the infratrochlear, supratrochlear, su-praorbital, and lacrimal nerves are branches of thetrigeminal nerve found above the palpebral fissure.Surgical defects involving the lid margin are oftenrepaired by oculoplastic surgeons. For defects in-volving less than 25% of the lid, primary repair isoften possible. Defects involving 50% of the lid arebest repaired with a Tenzel flap (myocutaneousadvancement flap with canthotomy). Defects involv-ing 75% or more of the lid may be repaired witha Hughes procedure (a tarsoconjunctival advance-ment flap). In patients who decline or cannot toleratesurgical intervention, radiation is considered a palli-ativemeasure. Extensive bulbar conjunctivae or orbitinvolvement is often treated by exenteration.
Mortality of sebaceous cell carcinoma has beenreported between 9% and 22%. Clinicopathologicfeatures associated with high mortality includelesions larger than 10 mm, pagetoid invasion,multicentric origin, highly infiltrative pattern, vascu-lar of lymphatic invasion, orbital invasion, upperand lower lid involvement, and symptoms for morethan 6 months. In addition, orbital invasion, metas-tases to regional lymph nodes, and vascular orlymphatic invasion usually occur in the context ofmoderate to minimal differentiation and a highlyinfiltrative pattern. Metastases are usually to regionallymph nodes (the lateral third of the eyelids drain tothe preauricular nodes and the medial two thirdsdrain to the submandibular nodes), but distantmetastases can occur.
For this series, the recommended choices are asfollows: 1, b; 2, c; 3, a; 4, d; 5, d; 6, c; 7, b; 8, b; 9, c; 10,c; 11, c; 12, c; 13, c.
BIBLIOGRAPHY
Ansai S. A histochemical and immunohistochemical study of
extraocular sebaceous carcinoma. Histopathology 1993;22:
127-33.
Nelson BR, Hamlet KR, Gillard M, Railan D, Johnson TM. Sebaceous
carcinoma. J Am Acad Dermatol 1995;33:1-15.
Spencer JM, Nossa R, Tse DT, Sequeira M. Sebaceous carcinoma of
the eyelid treated with Mohs micrographic surgery. J Am Acad
Dermatol 2001;44:1004-9.
Zurcher M, Hintschich C, Garner A, Bunce C, Collin JRO. Sebaceous
carcinoma of the eyelid: a clinicopathological study. Br J
Ophthalmol 1998;82:1049-55.