Embed Size (px)
Citation preview

BritishJournal ofOphthalmology 1994; 78: 875-880
PERSPECTIVE
Selective cell death in glaucoma: does it really occur?
J E Morgan
Glaucoma is associated with retinal ganglion cell death andconsequent deterioration in visual field. However, the asso-ciation between these events is not straightforward since asubstantial proportion of the ganglion cell population may belost before visual field defects can be detected using conven-tional perimetric methods.'2 Clinically, ganglion cell lossmanifests as optic disc cupping and defects in the nerve fibrelayer3 before the onset ofvisual field changes. In recent years anumber of studies have suggested that some ganglion cellsmay have a greater susceptibility to the damaging effects ofglaucoma and this idea has become central to a number ofstrategies designed to detect the earliest changes in thisdisease. Such ideas rest on the fact that the retinal ganglionpopulation is not homogeneous. It comprises cell groups withdifferent physiological and anatomical properties that enablethe complex parallel visual analysis thought to occur in theprimate.47 Cells can be divided broadly into those of theparasol type that comprise the M visual pathway and those ofthe midget type that comprise the P pathway. For simplicity,in this review, I will refer to the respective retinal ganglioncells as M or P cells.8 M cells form approximately 10% of theretinal ganglion cell population, have high luminance andcontrast sensitivity, large receptive fields, and lack spectralselectivity. P cells have lower luminance sensitivity, smallerreceptive fields, and do show spectral sensitivity."'Anatomically, at any retinal eccentricity M cells have largercell soma, axons, and dendritic fields than the P cells andproject almost exclusively to the magnocellular laminae ofthelateral geniculate nucleus. P cells project to the more dorsalparvocellular laminae.' It has been reported that cells with alarger soma and axon diameter may be selectively damagedearly in glaucoma12-15 raising the exciting prospect thatpsychophysical tests that are sensitive to and specific for theproperties of M cells may be able to detect the 'silent' celldeath occurring in the early phase of the disease. 6 17The hypothesis that ganglion cell death is selective in early
glaucoma is attractive and has become widely accepted in theophthalmic community. Large cells are more susceptible toglaucomatous damage than small cells and, since cell sizecorrelates with type, it follows that this indicates a selectivevulnerability of cells of a particular physiological class (theMcells). There are two important aspects to this hypothesis.Firstly, that glaucomatous cell damage is selective for cell sizeand, secondly, that it is selective for cell type. The evidence infavour of cell size related change is persuasive though thereare some caveats that should be considered when reviewingthe data. The effects that would be expected on particular celltypes are more complicated and require close analysis in thelight of recent anatomical and psychophysical data. I willconsider both of these aspects in turn.The earliest anatomical indications of selective loss came
from the analysis of optic nerve axon counts in both thehuman and monkey that showed, in glaucomatous subjects,loss of axons with diameters greater than the mean whencompared with normal optic nerves.'2 13 Corresponding losswas also seen in the ganglion cell layer in flat mounted retinal
preparations2 148 where, away from the fovea, cell sizehistograms indicated a reduction in the number of cells at theupper end of the cell diameter range. A similar effect wassubsequently observed in tissue taken from the macular zoneand examined in the transverse plane."9 It seemed reasonableto assume that these changes in the axon and cell diameterdistributions would be reflected as a change in the proportionof the types of remaining ganglion cells.The first aspect ofthese cell size distributions to consider is
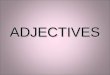
whether they result from a mechanism of cell death that isinfluenced by cell size. Taken on its own, this point isimportant since it has implications for the mechanism of celldeath in glaucoma.20 There are a number of possible explana-tions for the published distributions that have been consid-ered. Cell shrinkage, for example, has been considered as amechanism to account for the cell size distributions'4 and it isinstructive to consider the arguments concerning this mech-anism. Cell shrinkage, in its simplest form could occur non-selectively throughout the entire ganglion cell distribution. Ifall cells underwent the same percentage shrinkage the absoluteeffect of this change would be greater for the larger cells. It isconceivable, therefore, that this may generate cell sizedistributions in which larger cells appear to have beenselectively affected. In Figure 1 the size frequencies for ahypothetical cell population have been plotted whose meansize and standard deviation approximate that in the monkeymodel. The cell distribution is Gaussian and as such is anoversimplification ofactual distributions. In Figure IA all thecells from which this distribution has been derived under-went 5% cell shrinkage. The frequency distribution for thispopulation was then replotted and, to model the effect of celldeath, the number of cells in each bin reduced by 20% (apercentage cell death value for which cell distributions havebeen published'4). The decrease in the height on the glau-comatous distribution is obvious but there does not, at firstglance, appear to have been selective death of the larger cells.However, if the number of remaining cells in the shrunkendistribution is plotted on the same graph, it can be seen thatthis effect is quite marked for the larger cells. An importantargument against cell shrinkage is that this might in the earlystages be reflected in a left shift in the cell population. Such ashift has not been seen to occur in the macaque monkeymodel though there is a suggestion that it occurs in some ofthe cell size distributions in the human (see Quigley et al2figures 7, 8, and 11). Figure lB shows the sort of left shift thatmight be expected with a higher degree of cell death wherecells have undergone 10% shrinkage and 20% cell death. Thepercentage cell death at each cell size is also superimposed onthis plot and quite clearly there is a strong trend for cell loss asa function ofcell size. The third graph (Figure IC) shows howthis left shift may be hidden where the proportion of celldeath in relation to cell shrinkage is increased. In this plot thetendency for cell loss to increase with cell size is marked andthere appears to be little tendency for the distribution to shiftbeyond the lower limits of the normal distribution. Theimportant point to stress about these models is that they do
875
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.11.875 on 1 N
ovember 1994. D
ownloaded from

Morgan
A
* 0U.
5 7 9 11 13 15 17Cell size (,um)
19 21
.
.
9 ;1 13 15 17 19 21 23Cell size (,um)
.
..maE .
* * E
5 7 9 11 13 15 17 19 21 23 25 27C
Cell size (gim)
-60 L
Figure I (A) Hypothetical cell size distributions approximating those seenin the human and monkey. Broken line shows the normal cell sizedistribution. Continuous line shows the cell size distribution when cells in thenormal population all undergo 5% cell shrinkage and 20% cell death.
*Indicate the percentage cell death as a function ofcell size. The continuousstraight line shows the best straight line fit to these points. (B) Cell sizedistribution for a cell population that has undergone 10% shrinkage and 20%cell death. Conventions asfor (A). (C) Cell size distribution for a cellpopulation that has undergone 15% cell shrinkage and 50% cell death.Conventions as for (A).
not require selective action of either cell death or cellshrinkage as a function of cell size.The methods used to quantify the ganglion cell population
raise further problems for the interpretation of cell sizedistribution data. Ganglion cells in both the human andmonkey examples were identified on the basis of Nisslstains'34 in which ganglion cell distinction from amacrinecells requires some subjective judgment. The distinctionbetween these cell types may be more difficult in glau-comatous eyes where one is dealing with a diseased cellpopulation and the criteria that are used in normal subjectsmay not be applicable. In any primate study, ganglion cellidentification, particularly of the smaller cells, is confoundedby the presence of displaced amacrine cells in the ganglioncell layer as well as the displacement ofsome ganglion cells inthe amacrine cell layer.9 The published amacrine cell sizedistribution'4 suggests that overlap between retinal ganglionand amacrine cells soma size may be slight. Recent evidence,however, points also to the presence of some amacrine cellpopulations whose size overlaps extensively with that ofretinal ganglion cells.2' Details of the retinal eccentricities ofall the sampled areas are also essential for accurate interpreta-tion of cell soma size data, but these are missing in several ofthe published figures where cell populations have beenpooled on the basis of percentage cell death. Given the widevariation in cellular morphology with respect to eccen-tricity,22 this may have significant effects on the shape ofa cellsize distribution.As yet, there is no evidence that cell shrinkage occurs in
7glaucomatous damage and the foregoing discussions areentirely theoretical. Cell shrinkage has been observed as aprelude to cell death and can be a manifestation of apop-tosis." Recent work suggests that apoptosis occurs in themonkey glaucoma model25 but also that it is a rapid process,unlikely to generate large populations of shrinking cells. Cellshrinkage and atrophy have been widely studied in develop-ment6 and in models oftransneuronal degeneration.27 Signifi-cantly, cell shrinkage can occur in retinal ganglion cells intransneuronal degeneration with the preservation of thedendritic characteristics that differentiate cell type.27 Fromthe models of shrinkage and death presented in the previoussection, the degree of shrinkage would not have to be thatgreat to generate cell size distributions suggesting the occur-rence of selective cell death.The axon and cell size distribution histograms on which the
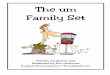
conclusions ofselective cell loss are based must be interpretedwith even more caution when considering whether cell deathis selective for particular cell types. A decrease in the numberofcells in a particular part ofthe cell size distribution does nottranslate simply into selective loss ofone particular cell class.In Figures 2 and 3 the mean and standard deviation of theMand P class ganglion cells have been represented graphicallyand include the subset of larger P cells that are thought torepresent the blue (ON) ganglion cells.28 In both cases there isconsiderable overlap of all three cell groups. In terms of size,the blue (ON) cell distribution in the monkey lies betweenthose for the M and P cells. Selective cell damage would, inthis species, correlate well with the finding that short wavesensitivity loss can be an early predictor of glaucomatousdamage.2930 However, this explanation is less convincing inthe human where the size distribution of blue (ON) cells andP cell population shows greater overlap. Of course theassumption in this argument is that retinal ganglion cell deathis the only mechanism by which a particular physiologicalpathway may manifest dysfunction and result in psycho-physical defects. Reliable conclusions about the effects onvarious cell classes can only be made when the relevant cellshave been unequivocally identified on the basis of theirdendritic and soma characteristics.
In an attempt to clarify these issues, Dandona et al'5
100
80
60
40
20
C',
0-
0a)u
-20
-40
B
0
0X
Cl)CA)0
0
c100
80
60
40
20
-20
-40
876
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.11.875 on 1 N
ovember 1994. D
ownloaded from

Selective cell death in glaucoma: does it really occur?
120
100
L-
a)-0
E
C3
80
60
40
20S
0
1 5 9 13 17
Cell size (,rrFigure 2 Cell size distributions based on knownstandard deviation for ganglion cells comprising tmonkey (from Dacey"). S denotes the cells involvsystem. The relative contributions to the entire gabeen estimated at 80% forP cells ofwhich 8%, aand 10% forM cells. There appears to be less ovepopulations in the monkey compared with the hun
studied the anterograde labelling of renormal and glaucomatous monkeys.project almost exclusively to the magcellular laminae ofthe lateral geniculateselective damage to these populationsdecrease in labelling at these laminae.'glaucomatous monkeys the density creduced in the magnocellular layersstrong argument for selective loss of tHowever, this result can be explaine(invoke mechanisms of selective cellbetween the density of anterograde labretinal ganglion cell population is comacids are often used in such studies an
density of innervation of a particular pbased on the densities of silver grain decell, the amount of tritiated amino ac:
gradely to the LGN will be determinumber of axons projecting to that paiby the area and the density of the terntion.32 33 Anterograde tracing studies hinformation about terminal arbors but (
ing ideas about the parent cell populatiterminal area of a retinal ganglion cc
shrinkage and retraction before cell
120
100 _
80
E
c 60
40 _
20
5 9 13 17
Cell size (grr
Figure 3 Cell size distributions based on knownstandard deviation for ganglion cells comprising t)human (from Dacey28). S denotes the cells involve,system. These distributions do not reflect possible spopulations. The size ofeach distribution reflects teach cell type to the entire retinal ganglion cell popwould comprise approximately 80% ofthe populaiwould comprise, at most 6% ofthe P population.overlap between all cell class size distributions.
Monkey decrease in anterograde labelling in the geniculate laminae.Although the affected geniculate laminae would be lessdensely labelled than unaffected areas, it does not necessarilyfollow (at least in the early stages of glaucoma) that thisreflects greater cell death among the cells giving rise to thoseaxons. Consideration of the probable innervation densities ofthe primate LGN suggests possible alternative interpretationof anterograde labelling data. The ratio of P to M ganglioncells in the primate retina is approximately 8:1 compared with4:1 for that of the P to M laminar volumes.35" Not sur-
M prisingly, this disparity is reflected in the different terminalarborisation patterns for the two ganglion cell classes.3' P cell
21 25 29 33 terminal (axonal) fields are cylinder-like with an averageI) width of 40 ,tm whereas M terminal field are much larger and
i values of the mean and more spherical with mean diameters of 125 [tm. If all arbors inrhe P andM svstems in the the LGN underwent the same percentage shrinkage then, ined in the bluei(ON) centre absolute terms, the effect would be greater for the projectionnmglion cell populations have to the magnocellular laminae generating a disparity in thertmost, would be S cells,erlap between the S and P density of innervation of the M and P laminae.,nan. Recent anatomical studies of the human LGN also suggest
that cell death may be selective.37 Postmortem analysis of celldensities in the geniculate laminae of glaucomatous patients
tinal ganglion cells in has revealed a significantly lower cell density in the magno-Since M and P cells cellular laminae, but not parvocellular laminae, when com-nocellular and parvo- pared with normal subjects. The authors conclude that by
- nucleus (LGN)93' any comparison with the parvocellular laminae the cells in the3 should manifest as a magnocellular layers have been selectively lost in glaucoma.The finding that in the Unfortunately, such conclusions are flawed when made)f labelling was more without reference to the volume of the remaining laminae.was interpreted as a Anterograde degeneration certainly results in cell loss in thehe M cell population. geniculate nucleus but it can also cause a reduction in laminard without the need to volumes. Quantitative analysis in the adult macaque monkeydeath. The relation following enucleation353" has shown that shrinkage can occur
)el in the LGN and the in denervated laminae to a greater extent than cell death withiplex. Tritiated amino a consequent increase in cell density. The lower density in theId some idea about the magnocellular lamina of the glaucomatous LGN is the resultart of the brain can be of cell death but the statement that this is selective relies onposition.32 For a single the evidence that less cell death has occurred in the parvo-id transported antero- cellular laminae. At first glance, the lack of any change in theined not only by the parvocellular laminae seems to support this view. However, itrt of the LGN but also is also what would have been expected if laminar shrinkageminal axonal arborisa- had kept pace with cell death, thereby maintaining a 'normal'ave provided valuable cell density. Indeed, it is difficult to believe that thecan give quite mislead- unchanged cell density in the parvocellular layer reflects aion.' For example, the relatively undamaged parvocellular cell population in view ofA1l axon may undergo the marked glaucomatous damage in some of the subjectsdeath resulting in a studied. Once again, the interpretation of apparently
straightforward anatomical data is fraught with difficulties.Human Ifwe are to understand the pattern ofganglion cell death inglaucoma, unequivocal identification and characterisation of
P cell populations must be achieved. In the monkey glaucomamodel where retinal ganglion cells have been labelled withhorseradish peroxidase (HRP) injected into the optic tractand LGN, preliminary reports suggest that selective ganglioncell death does not occur.39 However, any interpretation ofthese data must reflect the fact that the disruption of axonaltransport mechanisms in glaucoma may introduce samplingbias. If, for example, transport mechanisms in larger cells
M were selectively affected then this might, artefactually,suggest greater death among this cell population. With regard
21 25 29 33to cell type, a promising approach has been to address some
21 property such as neurofibrillar structure that appears tocorrelate with cell type.4" Recent work in which neurofila-
values of the mean and ment proteins were labelled immunologically suggests thathe P andM systemsin the these cells may be selectively vulnerable in the monkey model!din the blue (ON) centrekew in any ofthe cell of glaucoma.4' However, the correlation between neuro-the contribution made by fibrillar staining and cell type is somewhat indirect and itution Thuells P0%.Scells should be noted that non-M cell types also stain positively for~tion, M cells 10%. 5 cells
Note the considerable neurofibrils (though less dramatically4'). Work in otherspecies has to be compared with caution with the macaque
877
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.11.875 on 1 N
ovember 1994. D
ownloaded from

878
monkey and human models. In the cat, where cells belongingto the larger a ganglion cell class are easily distinguished onthe basis of HRP staining42 the smaller (B) cells appear to bemore susceptible to raised intraocular pressure.43 a Cells wererelatively well preserved, even in areas of severe cell loss and,significantly, underwent cell soma and dendritic tree shrink-age. However, it should be noted that the cells in this studywere subjected to relatively short periods of extremely highintraocular pressure and this may result in changes that areunrepresentative of those occurring in chronic glaucoma.Interestingly, direct external pressure to the intraorbital opticnerve in the cat results in selective degeneration of the largerY type axons.4
In spite of these difficulties with the interpretation of theanatomical evidence for selective cell death, many psycho-physical studies have produced results that seem to be in itsfavour. For example, in the monkey model, low spatialfrequency losses can be demonstrated using the patternelectroretinograph and visual evoked potentials45 and, in thehuman, motion detection thresholds are raised.'617 Thesedeficits are to be expected iftheM pathway is affected early inglaucoma. However, the conclusion that they are selectiveimplies that, at a given stage in the disease process theproperties of the P cells are affected to a lesser extent. Thedemonstration that pathways are differentially affectedrequires the employment of tests that have comparablespecificity and sensitivity for the properties of the P and Mpathways. This problem is epitomised in the paper bySilverman et al,'6 where the M pathway function wasmeasured with a random dot display and the P pathwayfunction using the Pelli-Robson chart; it is not at all clearwhether these techniques allow an unbiased assessment oftherelative damage to the M and P pathways." If the twopathways are assessed using the common criterion of spatialfrequency' 80% of patients have high spatial frequencyattentuation (with 60% of these having attenuation also at thelower spatial frequencies). High spatial frequency loss tendedto be seen in those cases with mild visual field loss whereas thelower spatial frequencies are involved in more advanceddisease (see also Sample et al 47). The results from a number ofrecent studies that short wavelength (chromatic) sensitivity isdecreased early in glaucoma and ocular hypertension48 under-mine the strength of the argument for selective visualfunction loss early in glaucoma. Chromatic selectivity is aproperty of the parvocellular pathway449 50 with the magno-cellular system having a broad band response to light ofdiffering wavelengths. The implication therefore is that theparvocellular system sustains damage early in glaucoma. Itdoes not follow that this damage is any greater than that in themagnocellular system. Indeed, electrophysiological studiesin glaucomatous monkeys are consistent with similar damageto the two pathways since the reduction in the frequency withwhich M and P cells are encountered is reduced to the sameextent in their respective laminae.5" Results from single testscan be misleading. When ocular hypertensive or earlyglaucoma patients are followed it has been found that defectsin both blue/yellow and temporal modulation occurred con-currently and preceded defects in white on white perimetry,52arguing against cell loss that is specific for cells ofeither theMor P pathway.Given the problems with the interpretation of the anatomi-
cal data, the concept of selective cell death requires clarifica-tion. Any doubts about selective cell death with regard to celltype can only be laid to rest on the basis of anatomical studiesin which ganglion cells have been unequivocally identifiedand classified using retrograde tracers (see Zamber et al 39) atechnique that could also dispel any theories regarding cellshrinkage. It must be stressed that the current data areconsistent with both the non-selective and selective modelsand I have not attempted to discuss which may be the more
important. It is conceivable that both patterns of cell loss mayoccur in different parts of the retina at different times."3 Theprecise mechanisms remain unclear and further work isrequired if we are to understand the mode of ganglion celldeath in glaucoma and develop tests that are sensitive andspecific for the earliest changes in this disease.
Ray Guillery, John Sparrow, Ian Thompson, and Michael Miller made valuablecomments on an earlier version of the manuscript.
J E MORGANDepartment of Ophthalmology and
Visual Science,Yale University School of Medicine,330 Cedar Street, PO Box 208061,New Haven, Connecticut 06520-8061,USA
1 Quigley HA, Addicks EM, Green WR. Optic nerve damage in humanglaucoma: III. Quantitative correlation of nerve fiber loss and visual fielddefect in glaucoma, ischaemic neuropathy, disc edema, and toxic neuro-pathy. Arch Ophthalmol 1982; 100: 135-46.
2 Quigley HA, Dunkelburger GR, Green WR. Studies of retinal ganglion cellatrophy correlated with automated perimetry in human eyes with glaucoma.AmJ Ophthalmol 1989; 107: 453-64.
3 Sommer A, Katz J, Quigley HA, Miller NR, Robin AL, Richter RC, et al.Clinical detectable nerve fibre atrophy precedes the onset of glaucomatousfield loss. Arch Ophthalmol 1991; 109: 77-83.
4 Livingstone MS, Hubel DH. Psychophysical evidence for separate channels forthe perception of form, color, movement and depth. J Neurosci 1987; 7:3416-68.
5 Leventhal AG, Rodieck RW, Dreher B. Retinal ganglion cell classes in theold world monkey: morphology and central projections. Science 1981; 213:1139-42.
6 Derrington A, Lennie P. Spatial and temporal contrast sensitivities ofneuronesin lateral geniculate nucleus of macaque.J Physiol 1984; 357: 219-40.
7 Derrington AM, Krauskopf J, Lennie P. Chromatic mechanisms in lateralgeniculate nucleus of macaque.J Physiol 1984; 357: 241-65.
8 Shapley R, Perry H. Cat and monkey retinal ganglion cells and their visualfunctional roles. Trends Neurosci 1986; 9: 229.
9 Perry VH, Oehler R, Cowey A. Retinal ganglion cells that project to the dorsallateral ganglion nucleus in the macaque monkey. Neuroscience 1984; 12:1101.
10 Kaplan E, Lee BB, Shapley RM. New views of primate retinal function. In:Osbourne NN, Chader GJ, eds. Progress in retinal research. Vol 9. Oxford:Pergamon, 1990: 273-336.
11 Merigan WH, Mansell JHR. How parallel are the primate visual pathways?Annu Rev Neurosci 1993; 16: 369-402.
12 Quigley HA, Sanchez RM, Dunkelberger GR, L'Hernault NL, Baginski TA.Chronic glaucoma selectively damages large optic nerve fibers. InvestOphthalmol Vis Sci 1987; 28: 913-20.
13 Quigley HA. Chronic human glaucoma causing selectively greater loss of largeoptic nerve fibres. Ophthalmology 1988; 95: 357-63.
14 Glovinsky Y, Quigley HA, Dunkelburger GR. Retinal ganglion cell loss is sizedependent in experimental glaucoma. Invest Ophthalmol Vis Sci 1991; 32:484-91.
15 Dandona L, Hendrickson A, Quigley HA. Selective effects of experimentalglaucoma on axonal transport by retinal ganglion cells to the dorsal lateralgeniculate nucleus. Invest Ophihalmol VisSci 1991; 32: 1593-9.
16 Silverman SE, Trick GL, Hart WM. Motion perception is abnormal in primaryopen angle glaucoma and ocular hypertension. Invest Ophthalmol Vis Sci1990; 31: 722-9.
17 Fitzke FW, Poinoosawmy D, Ernst W, Hitchings RA. Peripheral displacementthresholds in normals, ocular hypertensives and glaucoma. In: Greve EL,Heijl A, eds. Seventh international visualfield symposium. Dordrecht: MartinusNijhof/DrW Junk, 1987: 447-52.
18 Asai T, Katsumori N, Mizokami K. [Retinal ganglion cell damage in humanglaucoma. 2. Studies on damage pattern]. Nippon Ganka Gakkai Zasshi 1987;91: 1204-13.
19 Glovinsky Y, Quigley HA, Pease ME. Foveal ganglion cell loss is sizedependent in experimental glaucoma. Invest Ophthalmol Vis Sci 1993; 34:395-400.
20 Yablonski ME, Asamoto A. Hypothesis concerning the pathophysiology ofoptic nerve damage in open angle glaucoma. J Glaucoma 1993; 2: 119-27.
21 Dacey DM, Brace S. A coupled network for parasol but not midget ganglioncells in the primate retina. Vis Neurosci 1992; 9: 279-90.
22 Silviera LCL, Perry VH. The topography of magnocellular projecting cells (M-ganglion cells) in the primate retina. Neuroscience 1991; 40: 217-37.
23 Kerr JFR, Wyllie AH, Currie AR. Apoptosis: a basic biological phenomenonwith wide ranging implications in tissue kinetics. BrJ3 Cancer 1972; 26: 239-57.
24 Wyllie AH, Kerr JFR, Currie AR. Cell death: the significance of apoptosis. IntRev Cytol 1980; 68: 251-306.
25 Quigley HA, Nickells RW, Zack DJ, Kerrigan LA, Thibault DJ, Pease ME.Ganglion cell death in glaucoma occurs by apoptosis. Invest Ophthalmol VisSci (Suppl) 1994; 35: 2083.
26 Sloper JJ. Competition and cooperation in visual development. Eye 1993; 7:319-31.
27 Payne BR, Pearson H, Cornwell P. Transneuronal degeneration of beta retinalganglion cells in the cat. Proc Roy Soc LondB 1984; 222: 15-32.
28 Dacey DM. Morphology of a small-field bistratified ganglion cell type in themacaque and human retina. J Neurosci 1993; 10: 1081-98.
29 Sample PA, Taylor JD, Martinez GA, Lusky M, Weinreb RN. Short-wavelength color visual fields in glaucoma suspects at risk. Amj Ophthalmol1993; 115: 225-33.
30 Johnson CA, Adams AJ, Casson EJ, Brandt JD. Blue-on-yellow perimetry canpredict the development of glaucomatous visual field loss. Arch Ophthalmol1993;111: 645-50.
Morgan
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.11.875 on 1 N
ovember 1994. D
ownloaded from

Selective cell death in glaucoma: does it really occur?
31 Michael CR. Retinal afferent arborization patterns, dendritic field orientationand the segregation of function in the lateral geniculate nucleus of themonkey. Proc Natl Acad Sci 1988; 85: 4914-8.
32 Cowan WM, Gottlieb DI, Hendrickson AE, Price JL, Woolsey TA. Theautoradiographic demonstration of axonal connections in the central nervoussystem. Brain Res 1972; 37: 21-51.
33 Hendrickson AE. Electron microscopic distribution of axoplasmic transport.JCompNeurol 1972; 144: 381-98.
34 Thompson ID, Morgan JE, Henderson Z. The effects ofmonocular enucleationon ganglion cell number and terminal distribution in the ferret's retinalpathway. EurJ Neurosci 1993; 5: 357-67.
35 Matthews MR, Cowan WM, Powell TPS. Transneuronal cell degeneration inthe lateral geniculate nucleus of the macaque monkey. J Anat 1960; 94:145-69.
36 Le Gros Clark WE. The laminar organisation and cell content of the lateralgeniculate body in the monkey. JAnat 1941; 75: 419-33.
37 Chaturvedi N, Hedley-Whyte ET, Dreyer EB. Lateral geniculate nucleus inglaucoma. AmJ7 Ophthalmol 1993; 116: 182-8.
38 Matthews MR. Further observations on transneuronal degeneration in thelateral geniculate nucleus of the macaque monkey. J Anat 1964; 98: 255-63.
39 Zamber RW, Mills RP, Koontz MA, Phillips JO, Hendrickson AE. Ganglioncell loss in laser-induced primate glaucoma. Invest Ophthalmol Vis Sci(Suppl): 1988; 29: 421.
40 Silveira LCL, Perry VH. The topography ofmagnocellular projecting ganglioncells (M-ganglion cells) in the primate retina. Neuroscience 1991; 40: 217-37.
41 Vickers JC, Schummer R, Podos S, Wang RF, Morrison JH. Selectivevulnerability of neuroschemically coded subpopulations of retinal neurons ina monkey model of glaucoma. Invest Ophthalmol Vis Sci (Suppl) 1994; 35:2083.
42 Illing RB, Wassle H. The retinal projection to the thalamus in the cat: a
quantitative investigation and comparison with the retinal pathway. J CompNeurol 1981; 202: 265-85.
43 Grehn F, Eysel UT. Patterns of retinal ganglion cell loss after acute elevation ofintraocular pressure in the cat. Chib IntJ Ophthalmol 1986; 5: 17-26.
44 Burke W, Cottee LJ, Garvey J, Kumarasinghe R, Kyriacou C. Selectivedegeneration of optic nerve fibres in the cat produced by a pressure block. JPhysiol 1986; 376: 461-76.
45 Marx MS, Podos SM, Bodis-Woliner I. Signs of early damage in glaucomatousmonkey eyes: low spatial frequency losses in the pattern ERG and VEP. ExpEye Res 1988; 46: 173-84.
46 Ross JE, Bron AJ, Clarke DD. Contrast sensitivity and visual disability inchronic simple glaucoma. BrJ Ophthalmol 1984; 68: 821-7.
47 Sample PA, Juang PS, Weinreb RN. Isolating the effects ofprimary open-angleglaucoma on the contrast sensitivity function. Am3J Ophthalmol 1991; 112:308-16.
48 Heron G, Adams AJ, Husted R. Central visual fields for short wavelengthsensitive pathways in glaucoma and ocular hypertension. Invest OphthalmolVisSci 1988; 29: 64-72.
49 Merigan WH. Chromatic and achromatic vision in macaques: role of the Ppathway. J Neurosci 1989; 9: 776-83.
50 Rodieck RW. Which cells code for color. In: Valberg A, Lee BB, eds. Frompigments to perception. v. NATO ASI series. New York: Plenum Press, 1991;83-93.
51 Smith III EL, Harwerth RS, Chino YM, Ridder WH, Crawford MLJ.Neurophysiological alterations produced by elevated intraocular pressure.Optom Vis Sci 1989; 66: 64.
52 Casson EJ, Johnson CA, Shapiro L. Longitudinal comparison of temporalmodulation perimetry with white on white and blue on yellow perimetry inocular hypertension and early glaucoma. J Opt Soc Am 1993; 10: 1792-806.
53 Shapley R. Retinal ganglion cell function. In: Varma R, Spaeth G, eds. Theopticnerve in glaucoma. Philadelphia: Lippincott, 1993: 27-35.
Commentary
The review by Morgan considers evidence from our labora-tory that chronic human glaucoma and experimental glau-coma in monkeys cause a more rapid loss of larger retinalganglion cells. This work has now been confirmed in chronicglaucoma tissues by three other research groups (his refer-ences 18, 37, 41). The evidence includes measurements ofganglion cell body size by three different histological tech-niques, measures ofaxon diameter, and quantitative patternsof axonal transport and trans-synaptic effects in the lateralgeniculate body (LGN). Morgan suggests alternative expla-nations for our data. However, each of the possible explana-tions that he considers have been adequately discussed in ourprevious publications. I am grateful to the editor ofthe BritishJournal ofOphthalmology for allowing me to comment.Morgan invokes cell shrinkage to explain selective large cell
loss, pointing out that we considered this 'as a mechanism toaccount for the cell size distributions'. We did discuss butdismissed shrinkage as an explanation, since it is an implaus-ible event that does not fit the data. Only with a contrivedmatch of shrinkage in all ganglion cells to cell loss is itpossible to model our data to simulate no selective effect. Inaddition, the amount of putative shrinkage has to differ withvarious degrees in cell loss in exactly the correct proportion,or the result does not match observed data. Why would theamount of shrinkage change as percentage cell loss increases?Furthermore, we have recently reported that cell death byapoptosis occurs in glaucomatous ganglion cells (his reference25), but this is 'unlikely to generate large populations ofshrinking cells' - in fact, the number of cells dying at anypoint in time by apoptosis is very small, since it occurs sorapidly. Hence, shrinkage as a confounder is not only'entirely theoretical', it is unsupported by data on primaryganglion cell degeneration.Morgan suggests that we confused amacrine cells for
ganglion cells, citing 'subjective judgment'. I have studiedinner retinal anatomy for over 20 years and this researchincluded quantitative studies of cell size and cytology inmasked tissues of glaucoma, optic nerve transection, andnormal specimens. While no experiment is perfectly objec-tive, our reported ganglion cell body data do not include cellsof the same size or morphology as amacrines that normally
reside in the ganglion cell layer. The numerical data todemonstrate this have been published.Morgan has interpreted our LGN data to imply that
anterograde axonal transport is a poor indicator of cell bodyhealth. We found a selectively greater, statistically significantdecrease in axonal transport to magnocellular layers com-pared with that to parvocellular layers. His shrinkage argu-ment cannot explain the data, since we controlled theobservations by comparing LGN transport from the experi-mental glaucoma eye with those from control and acuteglaucoma eyes. His presentation therefore, on the ratio ofcells, laminar volumes, and arborisation patterns cannotexplain the data. Either there was less transport by larger cellsor the terminal arborisations of large cells were drasticallyaltered compared with smaller cells. Both conclusions arecompatible with a selectively greater susceptibility to chronicexperimental glaucoma among the magnocellular projectingcells. Furthermore, the topography of transport decreaseshows it to be greatest in LGN areas corresponding with themid retina, sparing the macular and nasal peripheral projec-tion zones. The damage pattern is exactly what would beexpected from the loss ofganglion cells in the upper and loweroptic nerve (from the arcuate retina) and supports therelevance of anterograde transport decrease to glaucomatousdamage.Among the possible explanations for our findings and those
of others, it is most likely that larger ganglion cells areselectively susceptible to injury. Morgan seems to suggestthat other possibilities have not been considered. This is farfrom the case, as can be seen from reading the discussionsections ofour work.Our group and others continue to study the details of
glaucoma damage to ganglion cells, particularly effects on themany cells that are not M cells. M cells are thought tocomprise only 10% of all primate ganglion cells. If glaucomacauses loss of one third or one half of the optic nerve, theclinical findings are still mild. But, many of the cells that aredead at this stage must be non-M types. We have recentlyreported central ganglion cell damage in glaucoma that maybe relevant to blue-yellow sensitivity loss.As to the implications of larger ganglion cell loss for
879
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.11.875 on 1 N
ovember 1994. D
ownloaded from


![Wendell Crenshaw Technologies - Hack.lu 2016 (base transceiver station) [Usually located at cell tower] MS (Mobile Station) Um (air) interface Layers of the GSM Um interface Connection](https://img.pdfslide.us/doc/110x75/5ae4a8a97f8b9a87048b8bd9/wendell-crenshaw-technologies-hacklu-2016-base-transceiver-station-usually.jpg)