Embed Size (px)
Citation preview
Seizures in the Seizures in the Emergency Emergency DepartmentDepartment
MOHAMD MIKATI MDMOHAMD MIKATI MDDirector, Adult and Pediatric Epilepsy Director, Adult and Pediatric Epilepsy Program, Professor and Chairman, Program, Professor and Chairman, Department of Pediatrics, American Department of Pediatrics, American University of Beirut University of Beirut

OUTLINEOUTLINE
REVIEW OF AVAILABLE REVIEW OF AVAILABLE PROTOCOLS FOR THERAPYPROTOCOLS FOR THERAPY
REVIEW OF GUIDELINES FOR REVIEW OF GUIDELINES FOR INVESTIGATIONS INVESTIGATIONS
REVIEW OF CLASS I AND II REVIEW OF CLASS I AND II COMPARATIVE EFFICACY STUDIESCOMPARATIVE EFFICACY STUDIES
CONTORVERSIES AND CONTORVERSIES AND CONCLUSIONSCONCLUSIONS

REVIEW OF AVAILABLE REVIEW OF AVAILABLE PROTOCOLS FOR THERAPYPROTOCOLS FOR THERAPY

Treatment of Paediatric Generalized Treatment of Paediatric Generalized Convulsive Status Epilepticus Convulsive Status Epilepticus
(Canadian Guidelines)(Canadian Guidelines)Position, airway, suction available secretions,
100% oxygen Verify adequacy of breathing and circulation
Commence intravenous access with normal saline.
Rapid glucose determination Diazepam 0.3mg/kg or Lorazepam 0.1 mg/kg
intravenously with an infusion rate of <2mg/min
Repeat Diazepam 0.3 mg/kg or Lorazepam 0.1 mg/kg intravenously up to 3 times
Phenytoin 20 mg/kg IV. Infusion rate of 1 mg/kg/min
Phenobarbital 20 mg/kg IV. Infusion rate of 1 mg/kg/min
The elapsed seizure time is now approximately 45 minutes. Depending on the resources
available, further intervention will be needed in consultation with a pediatric intensivist,
anaesthetist, neurologist.
Administer 1g/kg of 25% dextrose if hypoglycemia (4ml/kg) Diazepam 0.5mg/kg or paraldehyde 0.3 ml/kg may be given rectally if no IV access
Transfer to intensive care unit for further treatmentEmergency Paediatrics Section, Canadian Paediatric Society. Paediatrics & Child Health 1996; 1(2): 151-155
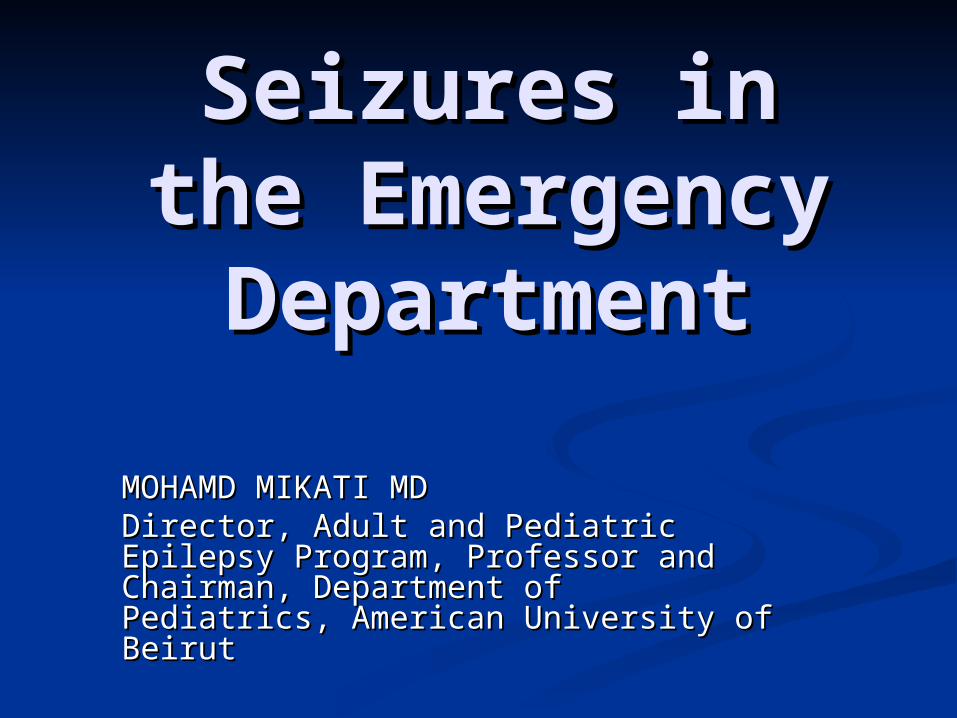
Management of Convulsive Status Epilepticus Management of Convulsive Status Epilepticus in Children (Baystate) in Children (Baystate)
Child presents with seizure activity
Protect Airway Ensure Respiration
Monitor Vital Signs with Cardiac and O2 Saturation Monitors
Administer O2 Start IV*
ABCs
Brief History from Family or Witnesses Neuro Exam
Hx PE
Lorazepam 0.05-0.15 mg/kg IV slow push
(Max 4 mg,)(may repeal x 1 after 20 minutes)
Point-of-Care: GlucoseConsider sending blood for: Ca++, Glucose BUN, Cr CBC w/diff Tox. And AC levels Blood Culture Electrolytes
Lab**
Respiratory depression may occur-be prepared to manage airway and support respiration.Midazolam ***
0.2mg/kg Intranasally or IM
*Administer D5%/NS IV at 2/3 maintenance rate.
**Lumbar Puncture is indicated if meningitis is suspected.
***Intranasal or IM Midazolam, 0.2mg/kg, has been used successfully to terminate CSE. Consider as an option if unable to achieve IV access.
Jackson et al., 2002. Baystate Health System

Phenytoin 18-20 mg/kg IV @ 1 mg/kg/min (Max 50mg/min) OR Phenobarbital **** 20mg/kg IV @
25-50 mg/min. See Text re history of allergy to either agent.
Load #1
Have seizures
Terminated?
EKG Monitoring (dysrhythmias or hypotension may occur have atropine available) RespiratoryDepression may occur-be prepared to manage airway airway and support respiration.
Phenytoin 5-10 mg/kg IV @ 1 mg/kg/min (Max 50mg/min) OR Phenobarbital **** 5-10 mg/kg IV
@ 25-50 mg/min
Have seizures
Terminated?
Check phenytoin level 30 min post loading dose
Phenytoin 5-10 mg/kg/day IV or PO in divided doses.
(Max 300-400 mg/day)Administer q8h age<6yrs,
q12h age>=6yrs
Maintenance
Yes
Load #2
Midazolam 0.2 mg/kg slow IV push, followed by 0.045-0.6 mg/kg/hr continuous infusion. Adjust based on clinical response.
No
Yes
Have seizures
Terminated?
Yes
No
Refractory CSE Next slide
****Maximum dose of phenobarbital is 40 mg/kg or 1 gram, whichever is greater, within 24 hours.
About fosphenytoin: Fosphenytoin is recommended in reference to phenytoin when venous access may be difficult to establish or precarious.
Jackson et al., 2002. Baystate Health System
About Time: Status Epilepticus is defined as prolonged seizures that last over 30 minutes, or recurrent epileptic seizures during which the patient does not regain consciousness within a 30-minute period. Since most seizures terminate spontaneously within a few minutes, seizures that persist for more than 5 to 7 minutes should probably be treated as CSE.
Management of Convulsive Status Epilepticus in Management of Convulsive Status Epilepticus in Children (Baystate) Children (Baystate)

To be managed by pediatric To be managed by pediatric intensivist/pediatric intensivist/pediatric anesthesiologist/pediatric neurologist teamanesthesiologist/pediatric neurologist team
Continuous EEG monitoringContinuous EEG monitoring Vital signs monitoringVital signs monitoring OO2 saturation monitoring saturation monitoring IntubateIntubate Paralyze patientParalyze patient Hemodynamic monitoring if indicatedHemodynamic monitoring if indicated Consider further diagnostic studies if Consider further diagnostic studies if
appropriate, e.g.,CTappropriate, e.g.,CT
Management of Convulsive Status Epilepticus Management of Convulsive Status Epilepticus in Children (Baystate) in Children (Baystate)
Jackson et al., 2002. Baystate Health System

Options include:Options include:• Continue Midazolam InfusionContinue Midazolam Infusion• PropofolPropofol 1-2 mg/kg. May repeat in 5 minutes, followed by 1-15 mg/kg/hr1-2 mg/kg. May repeat in 5 minutes, followed by 1-15 mg/kg/hr Adjust dose based upon EEG monitoring resultsAdjust dose based upon EEG monitoring results Check EEG hourly once patient has achieved a stable responseCheck EEG hourly once patient has achieved a stable response Primary end-point is suppression of EEG spikes, secondary end-point is Primary end-point is suppression of EEG spikes, secondary end-point is
burst suppressionburst suppression• PentobarbitalPentobarbital 3-15 mg/kg IV over 1 hr, followed by 0.5-5 mg/kg/hr to suppress all 3-15 mg/kg IV over 1 hr, followed by 0.5-5 mg/kg/hr to suppress all
epileptiform activity as above. (Cardiovascular toxicity can be life-epileptiform activity as above. (Cardiovascular toxicity can be life-threatening, and weakness post infusion can delay weaning from threatening, and weakness post infusion can delay weaning from ventilatory support).ventilatory support).
• DepaconDepacon 15-20 mg/kg IV load followed by 15 mg/kg/day IV in 4 doses (q 6hr). 15-20 mg/kg IV load followed by 15 mg/kg/day IV in 4 doses (q 6hr).
Monitor CBC, platelets, liver function. Avoid in patients with suspected Monitor CBC, platelets, liver function. Avoid in patients with suspected mitochondrial dysfunction or liver disease.mitochondrial dysfunction or liver disease.
• PyridoxinePyridoxine Trial in an infant or toddler may be warrantedTrial in an infant or toddler may be warranted
Management of Convulsive Status Epilepticus Management of Convulsive Status Epilepticus in Children (Baystate) in Children (Baystate)
Jackson et al., 2002. Baystate Health System

• Continue maintenance doses of phenytoin, Continue maintenance doses of phenytoin, tracking serum levels to determine optimum tracking serum levels to determine optimum dosesdoses
• Use intravenous fluids and low-dose dopamine Use intravenous fluids and low-dose dopamine to treat hypotensionto treat hypotension
• Decrease dosage of propofol if there are any Decrease dosage of propofol if there are any signs of cardiovascular compromise. signs of cardiovascular compromise. Rhabdomyolysis is a risk after 12-18 hours of Rhabdomyolysis is a risk after 12-18 hours of propofol administrationpropofol administration
• Taper infusion at 12 hours to observe for further Taper infusion at 12 hours to observe for further seizure activity. If seizures recur, reinstate seizure activity. If seizures recur, reinstate infusion in intervals of at least 12 hours.infusion in intervals of at least 12 hours.
Management of Convulsive Status Management of Convulsive Status Epilepticus in Children (Baystate)Epilepticus in Children (Baystate)
Jackson et al., 2002. Baystate Health System
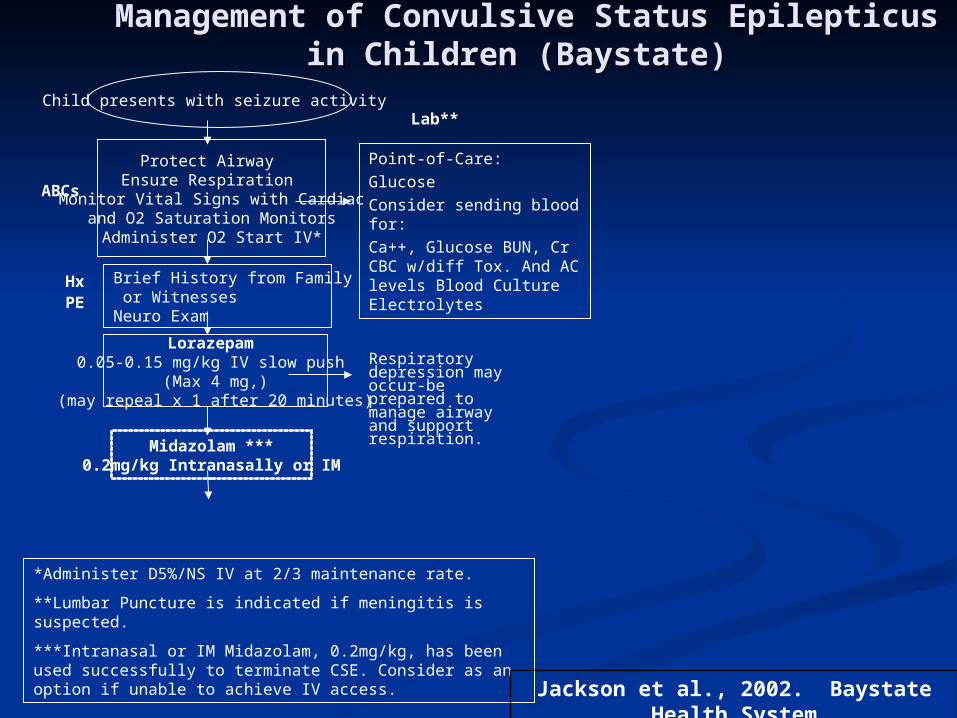
The NICE Consensus Protocol for The NICE Consensus Protocol for Treating Status Epilepticus in ChildrenTreating Status Epilepticus in Children
Airway Breathing Circulation Airway Breathing Circulation
Give high flow oxygenGive high flow oxygen
Measure blood glucose Measure blood glucose
Confirm epileptic seizureConfirm epileptic seizure
Immediate IV access Immediate IV access No IV accessNo IV access
1.1. Lorazepam 0.1 mg/kg IV Lorazepam 0.1 mg/kg IV 1. Diazepam 0.5 mg/kg PR1. Diazepam 0.5 mg/kg PR
(give over 30-60 seconds)(give over 30-60 seconds)
Seizure continuing at 10 minutes IV ACCESS Seizure Seizure continuing at 10 minutes IV ACCESS Seizure continuing at 10 minutes continuing at 10 minutes
2.2. Lorazepam 0.1 mg/kg IVLorazepam 0.1 mg/kg IV 2. Paraldehyde 0.4 ml/kg PR2. Paraldehyde 0.4 ml/kg PR
(give over 30-60 seconds)(give over 30-60 seconds) (give with the same (give with the same volume of olive oil)volume of olive oil)
Seizure continuing at 10 minutes Seizure continuing at 10 minutes Seizure Seizure continuing at 10 minutes continuing at 10 minutes
Call for senior helpCall for senior help
3.3. Protocol for treating status epilepticus in adults and Children, NICE, December 2003
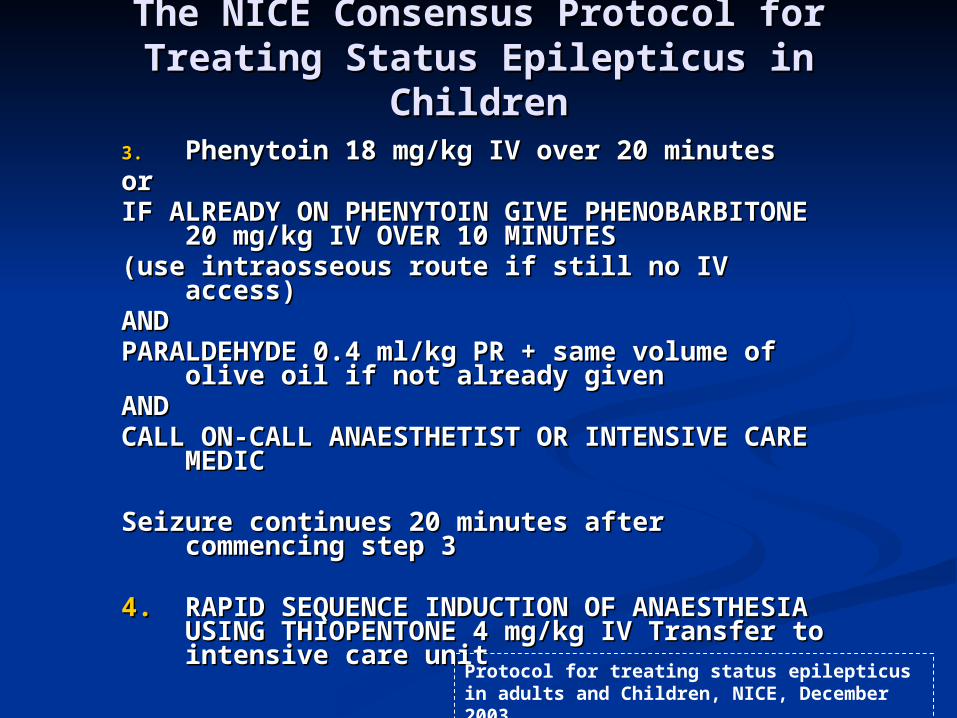
3.3. Phenytoin 18 mg/kg IV over 20 minutes Phenytoin 18 mg/kg IV over 20 minutes or or IF ALREADY ON PHENYTOIN GIVE IF ALREADY ON PHENYTOIN GIVE
PHENOBARBITONE 20 mg/kg IV OVER 10 PHENOBARBITONE 20 mg/kg IV OVER 10 MINUTESMINUTES
(use intraosseous route if still no IV access)(use intraosseous route if still no IV access)AND AND PARALDEHYDE 0.4 ml/kg PR + same volume of PARALDEHYDE 0.4 ml/kg PR + same volume of
olive oil if not already given olive oil if not already given AND AND CALL ON-CALL ANAESTHETIST OR CALL ON-CALL ANAESTHETIST OR
INTENSIVE CARE MEDICINTENSIVE CARE MEDIC
Seizure continues 20 minutes after Seizure continues 20 minutes after commencing step 3commencing step 3
4.4. RAPID SEQUENCE INDUCTION OF RAPID SEQUENCE INDUCTION OF ANAESTHESIA USING THIOPENTONE 4 ANAESTHESIA USING THIOPENTONE 4 mg/kg IV Transfer to intensive care unit mg/kg IV Transfer to intensive care unit
Protocol for treating status epilepticus in adults and Children, NICE, December 2003
The NICE Consensus Protocol for The NICE Consensus Protocol for Treating Status Epilepticus in ChildrenTreating Status Epilepticus in Children

REVIEW OF GUIDELINES FOR REVIEW OF GUIDELINES FOR INVESTIGATIONS INVESTIGATIONS

Laboratory studies
In Class I and II studies, results of laboratory studies usually did not contribute to diagnosis or management. Occasional single patients had hyponatremia or hypocalcemic, and in one ClassII study one had a positive cocaine screen.
An exception to the small number of abnormal
laboratory findings in the absence of specific suggestive features is in the under 6 month age group. Hyponatremia (<125 mM/L) was found to be associated with seizures in 70% of 47 infants younger than 6 months in a Class II study.
Hirtz et al., 2000. Neurology 55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children

EEGEEG
10 Class I studies demonstrated the utility of the 10 Class I studies demonstrated the utility of the EEG in prognostications, for example 54% of EEG in prognostications, for example 54% of children with an abnormal EEG had a children with an abnormal EEG had a recurrencerecurrence compared with 25% of 165 children compared with 25% of 165 children with a normal EEG (p < 0.001). with a normal EEG (p < 0.001).
EEG was also useful for diagnosis of the event, EEG was also useful for diagnosis of the event, and for identification of the and for identification of the epilepsy epilepsy syndromesyndrome. .
A Class I study published in 1998 in children and A Class I study published in 1998 in children and adults concluded that an EEG obtained adults concluded that an EEG obtained within within 24 hours24 hours of a seizure was more likely to contain of a seizure was more likely to contain epileptiform abnormalities than one done later epileptiform abnormalities than one done later (51% versus 34%). (51% versus 34%).
Hirtz et al., 2000. Neurology 55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children
CTCT
In Class I and II studies, only a small In Class I and II studies, only a small percentage of children (0 to 7%) percentage of children (0 to 7%) had lesions on CT that altered or had lesions on CT that altered or influenced management.influenced management. The yield The yield of abnormality on CT when the of abnormality on CT when the neurologic examination and EEG neurologic examination and EEG were normal was 5 to 10%.were normal was 5 to 10%. MRI MRI scanning was preferable to CTscanning was preferable to CT in in children following nonfebrile seizures. children following nonfebrile seizures.
Hirtz et al., 2000. Neurology 55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children

MRIMRIThere was one Class I report regarding MRI in There was one Class I report regarding MRI in children presenting with a first seizure and children presenting with a first seizure and another Class I report of newly diagnosed epilepsy another Class I report of newly diagnosed epilepsy in children. Four (2%) had lesions seen on MRI or in children. Four (2%) had lesions seen on MRI or CT (two brain tumors, two neurocysticercosis) CT (two brain tumors, two neurocysticercosis) that potentially altered management.. 19 (33%) that potentially altered management.. 19 (33%) MRI scans were abnormal,MRI scans were abnormal, but but none of the none of the children required [immediate] intervention children required [immediate] intervention on the basis of the MRI findings.on the basis of the MRI findings. In another In another the Class I study, 86% had neuroimaging, and the Class I study, 86% had neuroimaging, and none had abnormalities influencing immediate none had abnormalities influencing immediate treatment or management decisions. A third Class treatment or management decisions. A third Class I study reported that 3/43 children had an I study reported that 3/43 children had an abnormal MRI, one showing hippocampal sclerosis abnormal MRI, one showing hippocampal sclerosis and two showing single gray matter heterotopic and two showing single gray matter heterotopic nodules Two Class II six Class III reports showed nodules Two Class II six Class III reports showed similar findings.similar findings.
. . Hirtz et al., 2000. Neurology
55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children

Laboratory testsLaboratory tests should be ordered based on should be ordered based on individual clinical circumstances (option)individual clinical circumstances (option)
Toxicology screeningToxicology screening should be considered should be considered across the entire pediatric age group across the entire pediatric age group (option)(option)
Lumbar punctureLumbar puncture is of limited value an and is of limited value an and should be primarily used if there is concern should be primarily used if there is concern about meningitis or encephalitis (option)about meningitis or encephalitis (option)
EEGEEG is recommended as part of the is recommended as part of the evaluation (standard)evaluation (standard)
Hirtz et al., 2000. Neurology 55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children

If a neuroimaging study is obtained If a neuroimaging study is obtained MRI MRI is the preferredis the preferred modality (guideline) modality (guideline)
Emergent neuroimagingEmergent neuroimaging should be should be performed in a child of any age with performed in a child of any age with Todd’s paresisTodd’s paresis or post ictal or post ictal depressiondepression not quickly resolving (option)not quickly resolving (option)
Nonurgent imagingNonurgent imaging studies with MRI studies with MRI should be seriously considered in any should be seriously considered in any child with neurologic child with neurologic abnormalitiesabnormalities and with and with partial seizurespartial seizures (option) (option)
Hirtz et al., 2000. Neurology 55: 616-623
Practice Parameter: Evaluating Practice Parameter: Evaluating a First Nonfebrile Seizure in a First Nonfebrile Seizure in
Children Children
REVIEW OF CLASS I AND II REVIEW OF CLASS I AND II COMPARATIVE EFFICACY STUDIESCOMPARATIVE EFFICACY STUDIES

Therapy of Status: Comparative Therapy of Status: Comparative EfficacyEfficacy
89
76
0
20
40
60
80
100
Lorazepam Diazepam
Eff
icac
y (%
)
Reference: Leppik et al.1983, JAMA. 249: 1452-1454

Therapy of Status: Therapy of Status: Comparative EfficacyComparative Efficacy
Pro
port
ion
of
Pati
en
ts
in S
tatu
s E
pil
ep
ticu
s
0.0
0.2
0.4
0.6
0.8
1.0
0 10 20 30 40 50 60
Minutes
Placebo
Diazepam
Lorazepam
Alldredge et al., 2001. N Engl J Med, 345(9):631-637

Therapy of Status: Comparative Therapy of Status: Comparative EfficacyEfficacy
9
5
15
5.5
0
2
4
6
8
10
12
14
16
Cumulativeconvulsive time
Response latency
Diazepam+phenytoin
Phenobarbital
Tim
e in
min
ute
s
•Reference: Shaner et al.1988, Neurology. 38: 202-207.
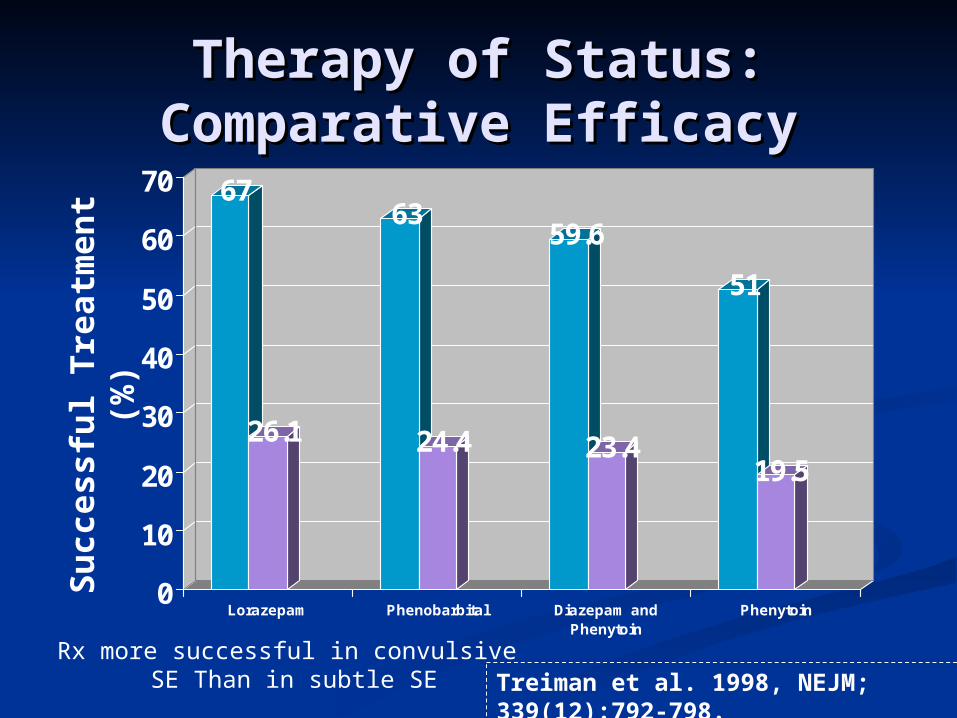
Treiman et al. 1998, NEJM; 339(12):792-798.
Therapy of Status: Therapy of Status: Comparative EfficacyComparative Efficacy
67
26.1
63
24.4
59.6
23.4
51
19.5
0
10
20
30
40
50
60
70
Lorazepam Phenobarbital Diazepam andPhenytoin
Phenytoin
Su
ccess
ful
Tre
atm
en
t (%
)
Rx more successful in convulsive SE Than in subtle SE

Therapy of Neonatal Status Therapy of Neonatal Status Epilepticus: Comparative Efficacy Epilepticus: Comparative Efficacy
43 45
0
20
40
60
80
100
Phenobarbital Phenytoin
•Reference: Painter et al.1999, N Engl J Med. 341: 485-489.
Eff
ica
cy
(%
)
Stages of Status EpilepticusStages of Status Epilepticus
1.1. Discrete seizures with interictal slowingDiscrete seizures with interictal slowing2.2. Waxing and waning of ictal dischargesWaxing and waning of ictal discharges3.3. Continuous ictal dischargesContinuous ictal discharges4.4. Continuous ictal discharges Continuous ictal discharges
punctuated by flat periodspunctuated by flat periods5.5. Periodic epileptiform discharges on Periodic epileptiform discharges on
a flat backgrounda flat backgroundThese last two stages correspond to These last two stages correspond to refractory status epileptics which refractory status epileptics which may may difficult to detectdifficult to detect (subtle (subtle seizures) seizures) difficult to treatdifficult to treat, and is , and is associated with associated with long term sequelilong term sequeli..
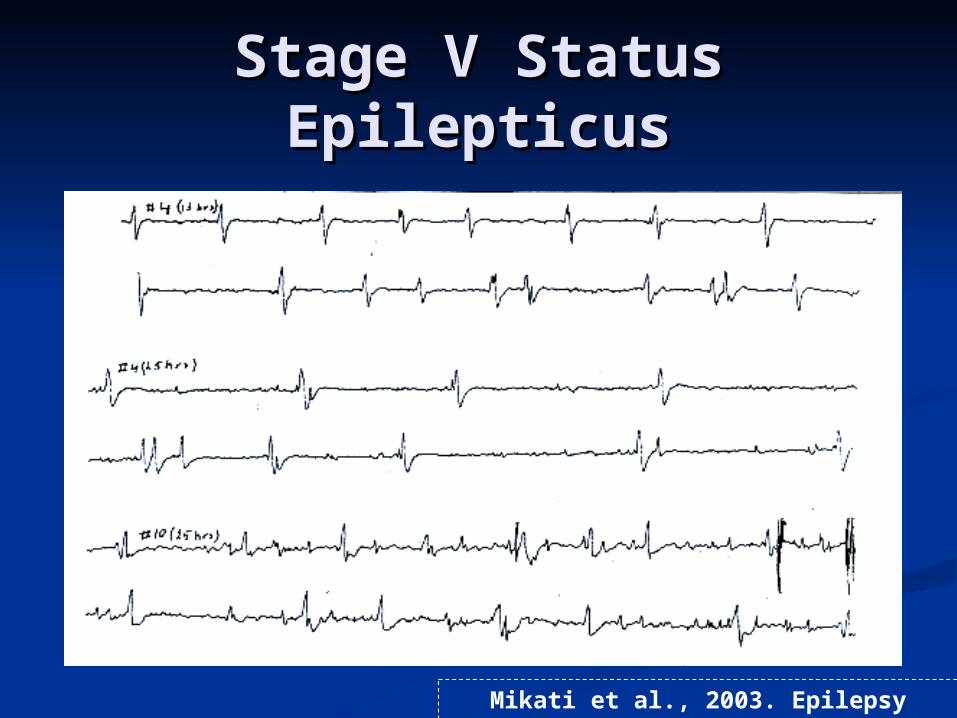
Stage V Status Stage V Status EpilepticusEpilepticus
Mikati et al., 2003. Epilepsy research, 55:9-19

Apoptosis after Status Apoptosis after Status EpilepticusEpilepticus
(Kainic Acid Model)(Kainic Acid Model)
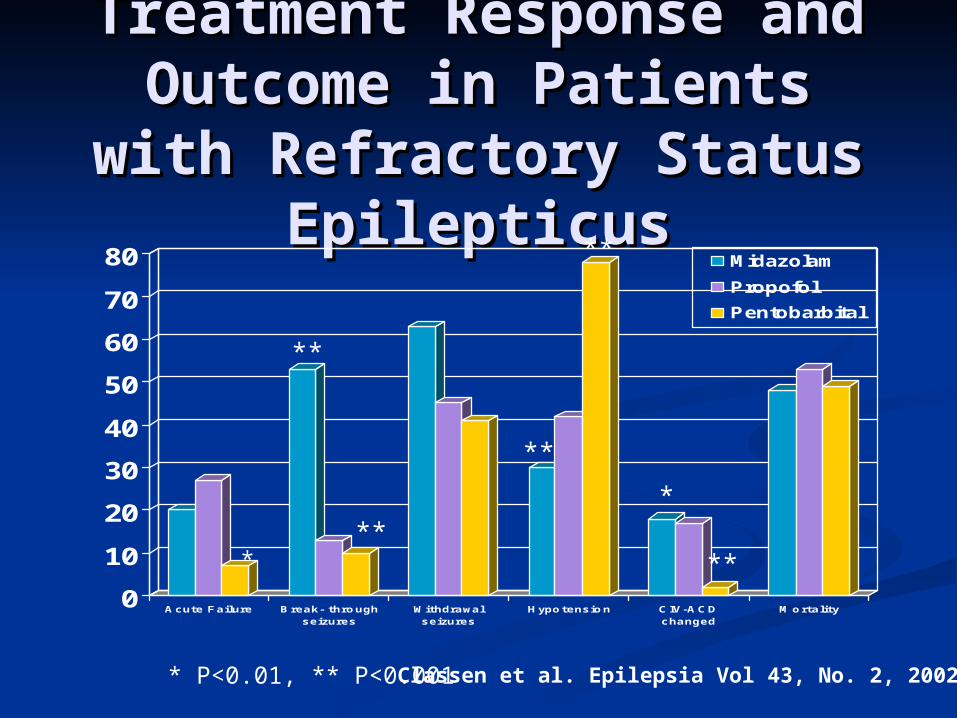
Treatment Response Treatment Response and Outcome in and Outcome in
Patients with Patients with Refractory Status Refractory Status
EpilepticusEpilepticus
0
10
20
30
40
50
60
70
80
Acute Failure Break- throughseizures
Withdrawalseizures
Hypotension CIV-ACDchanged
Mortality
Midazolam
Propofol
Pentobarbital
***
**
**
**
*
**
* P<0.01, ** P<0.001 Classen et al. Epilepsia Vol 43, No. 2, 2002

Treatment Response in Treatment Response in Refractory Status Epilepticus Refractory Status Epilepticus According to Goal of Seizure According to Goal of Seizure Control Vs. EEG Background Control Vs. EEG Background
SuppressionSuppression
0
10
20
30
40
50
60
70
80
Acute Failure BREAK THRU SZS WITHDRAWAL SZ HYPOTENSION RX CHANGED MORTALITY
SZ SUPPRESSION
EEG SUPPRESSION
**
**
** P<0.01 Classen et al. Epilepsia Vol 43, No. 2, 2002

Conclusions and Conclusions and RemarksRemarks
There are There are effective initial therapieseffective initial therapies for for status epilepticus, but what are the status epilepticus, but what are the most most effectiveeffective initial therapy medications initial therapy medications (consider the benzodiazepines, (consider the benzodiazepines, the the newer optionsnewer options, intravenous valproate, , intravenous valproate, and possibly levetiracetam), what do we and possibly levetiracetam), what do we do in the absence of more controlled do in the absence of more controlled studies.studies.
What is the optimal approach to stage IV What is the optimal approach to stage IV and V and V refractory statusrefractory status, knowing that , knowing that most medications are not very effective?most medications are not very effective?

Conclusions and Conclusions and RemarksRemarks
Is there a role for Is there a role for neuroprotective agentsneuroprotective agents and strategies in the treatment of status?and strategies in the treatment of status?
What do we do about What do we do about neonatal statusneonatal status, do , do we treat EEG seizures like we do clinical we treat EEG seizures like we do clinical seizures?seizures?
At present the key in the management is At present the key in the management is recognition of status as a recognition of status as a medical medical emergencyemergency, the application of a , the application of a justifiable justifiable institutional protocolinstitutional protocol, and , and individualizationindividualization of therapy. of therapy.