Embed Size (px)
Citation preview

Cancer Genetics and Cytogenetics 126 (2001) 139–146
0165-4608/01/$ – see front matter © 2001 Elsevier Science Inc. All rights reserved.PII: S0165-4608(00)00406-4
Segmental amplification of 11q23 region identified by flourescence in situ hybridization in four patients with myeloid disorders: a review
K.S. Reddy
a,
*, L. Parsons
a
, L. Mak
a
, P. Dighe
b
, T. Saphner
c
, M.K. Crow
d
, M. Scott
e
a
Quest Diagnostics Inc., Nichols Institute, Cytogenetics Department, 33608 Ortega Highway, San Juan Capistrano, CA 92690-6130, USA
b
Stockton Hematology Oncology Medical Group, Stockton, CA, USA
c
Green Bay Oncology Ltd., Green Bay, WI, USA
d
Diagnostic Clinic of Houston, Houston, TX, USA
e
Indian River Memorial Hospital, Vero Beach, FL, USA
Received 28 July 2000; received in revised form 6 October 2000; accepted 10 October 2000
Abstract
Four cases with a segmental amplification of 11q23 region were detected by FISH. The amplifica-tion was either contiguous amplification on chromosome 11, or multiple markers involving the11q23 region. The markers were derivative chromosomes, or isochromosomes. Amplification of11q23 region was associated with complex karyotypes at the time of diagnosis or following treat-ment in secondary leukemias. Three were AML cases belonging to either AML-M5a or AML-1subtypes and one was a myeloproliferative disorder. These cases were resistant to treatment. Con-ventional cytogenetic analysis and fluorescence in situ hybridization (FISH) studies using MLL, 11painting, or 11 centromere probes ascertained the segmental amplification. Since the patients didnot respond to treatment the amplification of gene or genes that map to 11q23 may be responsiblefor the unfavorable prognosis. Hence, this type of amplifications could have clinical significance.
© 2001 Elsevier Science Inc. All rights reserved.
1. Introduction
Genomic amplification of oncogenes has been observedfrequently in solid tumors and is less common in hematogicalmalignancies. The amplifications manifest as double minutes(dmin) or homogeneously staining regions (HSR). The esti-mated incidence of cytogenetically detectable gene amplifi-
cation in AML is
z
1% [1]. FISH/molecular investigation ofsuch amplifications have been limited. In AML, the ampli-cons have most frequently been C-MYC [2,3]. MLL
2
dminand
2
HSR in AML have been reported recently [4–6].In this article, the focus is on patients with myeloid dis-
orders and 4–9 copies of the 11q23-segment encompassingMLL. The amplifications of 11q23 segment are either onchromosome 11, i.e., intrachromosomal or on another chro-mosome, i.e., interchromosomal [1,5,7–10].
Tanaka et al. [1], identified a segmental jumping translo-cation containing the CD3-MLL region as a new form ofgene amplification in a treatment related leukemia with a
complex karyotype. The leukemia was of French-American-British (FAB) M1 morphologic subtype and occurred follow-ing 5-fluorouracil chemotherapy for the management ofbreast tumor. This patient had 4 copies of CD3-MLL region.Felix et al. [7] studied a treatment related acute myeloid leu-kemia (t-AML) case with a complex karyotype. FISH analy-sis showed multiple copies of the MLL gene. A genomic re-gion including CD3
e
, MLL and a segment of band 11q24was unrearranged and amplified by Southern-blot analysis.Cuthbert et al. [9] described a jumping translocation of 11q23with MLL gene rearrangement and interstitial telomeric se-quences. A marker with interspersed chromosome 9 and 11regions and also involving chromosome 19 was reported byAllen et al. [8]. In one AML-M4 patient, Avet-Loiseau et al.[5] found a complex karyotype with multiple MLL signals ona ring and marker chromosomes post breast cancer treatmentfor 5 years. A second patient had de novo AML-M1 andmarker chromosomes with multiple MLL signals. Both pa-tients were refractory to treatment. Size variable ring chromo-somes in a AML-M4 and AML-M5a case and a homoge-nously staining region with MLL amplification in a AML-M6case was reported by Streubel et al. [6]. Reddy et al. [10] de-scribed a chromosome 11 with 2–3 copies of 11q23-MLL re-
* Corresponding author. Tel.: 949-728-4334; fax: 949-728-4979.
E-mail address
: [email protected] (K.S. Reddy).

140
K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
gion. In this paper, we present four cases with multiple copiesof 11q23-MLL segment resulting from direct duplication ormultiple copies of a derivative chromosome involving 11q23.Case 1 has been previously published [10].
Partial tandem duplication of the MLL gene has been ob-served in
z
5% of AML patients with normal cytogenetics[11–13]. However, MLL gene duplications are regularlygenerated by homologous ALU recombination in a smallnumber of hematopoietic cells of most healthy donors.These data suggests that MLL gene duplications are not im-plicated in the malignant transformation in AML, or alter-nately only a few cells acquire additional oncogenic muta-tions necessary to establish the malignant phenotype [14].
Second cancers occur in
z
7% of survivors of a primarymalignancy [15]. Leukemias are the major second cancerthat result from chemotherapy [16–18]. The two majorforms of treatment related leukemias are those with chro-mosome 5 and 7 monosomies induced by alkylating agentsand those with MLL gene translocations and other translo-cations related to topoisomerase II inhibitors [7].
2. Clinical history
2.1. Case 1
A 66-year-old Caucasian male was diagnosed with my-eloproliferative disorder (MPD) 10 years ago. The thrombo-cytosis was treated with hydroxyurea for 1 1/2 years. In1994 and 1997, the patient was again prescribed hydrox-yurea and was given frequent blood transfusions. The RT-PCR was negative for BCR/ABL fusion transcript. Re-cently, he developed a persistent cough. Chest X-rayshowed bilateral interstitial pulmonary infiltrates. The blasts(68%) were consistent with acute myeloid leukemia and fa-vored the subclass M5a. Flow cytometry studies supportedthis diagnosis. The presence of trilineage dysplasia raisedthe possibility of treatment-related acute myeloid leukemia.
2.2. Case 2
An 82-year-old woman presented with progressive pancy-topenia. Sixteen years ago she had right radical mastectomy
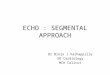
Fig. 1. Case 1. (A): A G-banded karyotype from an abnormal clone showing ?add(11)(arrow ↑ ) and two markers. (B1): Two copies of MLL probe was foundon the add(11) (arrow) and 2 markers also had MLL signals (arrowhead). (B2): The DAPI-converted G-banded chromosomes showing the add(11)(q23)(arrow) and two markers (arrowhead). (B3): The 11-paint hybridized to the add(11) (arrow) and the markers end to end (arrowhead). (B4): The DAPI-con-verted G-banded chromosomes showing the add(11) (arrow) and markers (arrowhead). (B5): Three copies of the MLL probe was found to be present on theadd(11) (arrow). (B6): The DAPI-converted G-banded chromosomes showing the add(11)(q23) (arrow). (B7): Sequential FISH with chromosome 11-paintprobe hybridized to both add(11) end to end (arrow).

K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
141
with axillary dissection finding of
,
1 cm infiltrating lobularcarcinoma for which treatment was declined. Four years later,she had a left radical mastectomy with axillary dissection for a2.5 cm infiltrating ductal carcinoma. Three lymph nodes werepositive. She received 6 courses of CMF chemotherapy withIV cyclophosphamide and Tamoxifen for 1 year. A year ago,she had painless vaginal bleeding and had hysterectomy, bilat-eral salpingo-oophorectomy because of a malignant Mullerianmixed tumor. The patient underwent external beam radiother-apy to the pelvis. A diffuse large B-cell lymphoma presentedas a right hilar mass in the lung. She had partial remission ofher lung disease after CHOP chemotherapy four times withdose reduction. The significant pancytopenia that ensued re-quired erythropoietin and G-CSF, growth factor support. After4 weeks of treatment, she achieved partial remission and re-ceived weekly rituximab (monoclonal antibody directedagainst CD20) 375 mg/M
2
. Because of progressive pancy-topenia flow cytometry and cytogenetics studies on a bonemarrow biopsy, was performed and found to be consistentwith acute myeloid leukemia probably of FAB subclass M1.The patient was in hospice care and had received chronictransfusions. Four months later the patient passed away.
2.3. Case 3
A 78-year-old woman presented with gingivitis of the ante-rior mouth, fever, chills and decreased appetite. She has had ahistory of a hysterectomy and a bilateral salpingo-oophorec-tomy for an abnormal PAP smear. The CBC showed mildanemia with a hemoglobin of 8–9 gm/dl and platelets 41
3
10
9
/L. The smear had 100% blasts, presumably of myelocyticorigin. In flow cytometry studies, the majority of the cellswere positive for HLA-DR, CD13, CD33, CD34 and cyto-plasmic myeloperoxidase and was compatible with myelo-blasts of the M1 FAB subclassification. Following treatmentwith idarubacin and infusion ARA-C, she went into partial re-mission and lived for 6 months following AML diagnosis.
2.4. Case 4
An 86-year-old white male was admitted because of sud-den onset of hemoptysis. He had a respiratory infection forseveral weeks and was running a slight temperature. Earlier,he was diagnosed with myeloproliferative disorder in 1994and was treated with hydroxyurea to control his platelet count.He was noted recently to have some immature white cells and
Fig. 2. Case 2. (A): A GTG karyotype showing the of markers (arrow ↑ ). (B1): Each marker has two MLL signals (arrow). (B2): The DAPI-convertedG-banded chromosomes showing markers (arrow). (B3): The markers painted end to end with whole painting 11 probe (arrow). (B4): The DAPI- convertedG-banded chromosomes showing the markers (arrow). (B5): Sequential FISH using 11 centromere probe hybridized to the markers. (B6): The DAPI-con-verted G-banded chromosomes showing the markers (arrow).

142
K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
Fig. 3. Case 3. (A): A GTG banded karyotype showing the der(22)t(11;22) (arrow ↑) (B1): The derivative, der(22)t(11;22) had a MLL signal (arrow). (B2):The DAPI- converted G-banded chromosomes showing der(22) (arrow).
was investigated for leukemic transformation. A week afterthe cytogenetic study the patient passed away. He had low-grade transitional cell carcinoma in 1981 and was under sur-veillance cytoscopies. A pilonidal cysts was removed. A rightcarpal tunnel release was also performed. He had a benignprostatic hyperthrophy and hypothyoidism. One brother andsister died of lung cancer at 41 years and 81 years of age.
3. Material and methods
Unstimulated bone marrow cultures were harvested after24 and 48 hours. The slides were GTG-banded.
Fluorescence in situ hybridization (FISH) was performedusing coatasome-11, MLL, or D11Z1 probes (Ventana Inc.,Gaithesburg, MD, USA). The MLL probe used detectsabout 80% of the rearrangements except those that occur inthe 3
9
of the MLL gene. The GTG analyzed slides wereused for FISH. The slides were denatured at 70
8
C for 2 min.After overnight hybridization at 37
8
C in a humid chamber,the slides were washed in 2
3
SSC (MLL), 1
3
SSC(Coatasome 11), or 0.25
3
SSC (D11Z1) at 72
8
C for 5 min.
4. Cytogenetics and FISH results
4.1. Case 1
Twenty cells were analyzed from the GTG bandedslides. A normal and two related abnormal clones were ob-served. The karyotype was 45
z
47,X,
2
Y[9],add(1)(p35) [9],
2
10[11],?add(11)(q23)[15],del(17)(p13)[9],add(17)(p11)[4],
2
20[4],
1
mar1[11],
1
mar2[9][cp15] (Table 1)/89,XXYY,?add(11)(q23)
3
2,
2
10,
2
12,
2
16[2]/46,XY[3] (Fig. 1A).By FISH, either 2–3 copies of the MLL gene were found onthe add(11)(q23) and a single copy on the markers (Fig. 1B1and 1B4). The total number of MLL signals was 5 or 6.
4.2. Case 2
Seventeen GTG banded metaphases were analyzed andfound to have an abnormal clone with multiple abnormali-ties that included a derivative 11 and an isochromosome for11q21qter region. The karyotype was 47,XX,der(5)t(5;7)(q13;q11.2),
2
7,der(11)add(11)(p13)del(11)(q14),
2
13,
2
17,
1
r,
1
3mar[cp13]/ 46,XX[4] (Fig. 2A). The abnormalclone was found predominantly in the B-cell culture. Each

K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
143
marker was found to have two MLL signals (Fig. 2B1).The wcp11 painted the markers uniformly from end to end(Fig. 2B3). The 11 centromere probe (D11Z1) also hybrid-ized to the marker (Fig. 2B5). By FISH, the marker wasshown to be a derivative isochromosome 11, i.e., der(11)i(11)(q23qter). The total number of MLL signals was 7.Two each on the three copies of isochromosome 11 andone from the normal 11.
4.3. Case 3
GTG analysis of 20 metaphases found an aberrant clonein 19 cells and one normal cell. The karyotype was46,XX,
2
5,der(7;17)(p10;q10),del(8)(p21),t(11;22) (q23;q13),
2
13,add(16)(p11.2),der(16)t(13;16)(q14;q22),
2
18,add(20)(p13),
1
der(22)t(11;22)(q23;q13)
3
3,
1
r[cp19]/46,XX[1](Fig. 3A). FISH was performed and the der(22) was found tohave the MLL signal (Fig. 3B1) and the der(11)t(11;22) lackedthe MLL signal. The total number of MLL signals was 4.
4.4. Case 4.
GTG analysis of 20 metaphases found an aberrant clonein 5 cells. The karyotype was 48,XY,
1
11,
1
11,der(11)t(11;
11)(p11.2;q14)x2[5]/46,XY[15] (Fig. 4A) FISH was per-formed and the der(11) was found to have two MLL signals(Fig. 4B1). The total number of MLL signals was 6.
5. Discussion
The cases in this study were compared to other reportedcases with 11q23–MLL segmental rearrangements (Table 2)[1,5–10]. The segmental rearrangements included duplicationand triplication of 11q23 region on chromosome 11 or asmarkers involving this region. Eight were males and 5 werefemale. Their ages ranged from 2–86 years. Eight were pri-mary myeloid disorder cases, 5 were secondary acute myeloidleukemia following treatment with 5-fluorouracil for breastcancer; vincristine, actinomycin D, ifosfamide, cyclophospha-mide, etopside, doxorubicin, carboplatinum treatment for em-bryonal rhabdomyosarcoma; hydroxyurea for myeloprolifera-tive disorder and CMF chemotherapy with IV Cytoxan andTamoxifen for breast cancer and CHOP chemotherapy forB-cell lymphoma. The treatment related acute myeloid leuke-mia were AML-M1, AML-M4, AML-M5, and AML-5a. Theduration between primary malignancy and secondary leuke-
Fig. 4. Case 4. (A): GTG banded karyotype showing the der(11)t(11;11) (arrow ↑ ). (B1): The derivative, der(11) with two MLL signals (arrow). (B2): TheDAPI-converted G-banded chromosomes showing der(11) (arrow).

144
K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
mia ranged from 2–10 years. Survival after the secondary leu-kemia ranged from 2 days to 4 months. Apart from monosomy5 and 7 which are associated with treatment related leukemia,duplication of 11q23–MLL region may be yet another therapyrelated abnormality to be considered in the future.
The intrachromosomal change in this study included seg-mental duplication or triplication of 11q23 region. A roughestimate of the incidence of 11q23 segmental amplificationsis 4/690 (0.57%) in myeloid disorder cases. Interestingly, incase 1, MLL region amplification increased from 2 copies to3 copies in a sideline. This suggests that the region is dy-namic and probably subject to duplication by unequal cross-ing over. In cases 2 to 4 the multiplication of the derivativechromosome with 11q23 segment, suggests a growth advan-tage to these cells and hence their selective retention.
In our experience, the segmental duplications and theirvarious manifestations were hard to detect using G-bandingalone. Multiple copies of marker chromosomes and deriva-tive chromosomes also required FISH studies to confirm thechromosomal origin. The role of 11q23 amplifications in leu-kemogenesis may involve over expression of either MLLand/or other genes that map to this region. Therefore, in mye-loid disorders possible 11q23 rearrangements should be eval-uated using FISH/molecular studies to detect 11q23–MLLamplification and this may identify cases that are probably re-sistant to treatment and have an unfavorable prognosis.
References
[1] Tanaka K, Arif M, Eguchi M, Kyo T, Dohy H, Kamada N. Frequentjumping translocations of chromosomal segments involving ABL on-cogene alone or in combination with CD3-MLL genes in secondaryleukemias. Blood 1997;89:596–600.
[2] Li YP. Double minutes in acute myeloid leukemia. Int J Cancer 1983;32:955–9.
[3] Mohamed AN, Macoska JA, Kallioniemi A, Kallioniemi OP, Wald-man F, Ratanatharathorn V, Wolman SR. Extrachromosomal gene am-plification in acute myeloid leukemia: characterization by metaphaseanalysis, comparative in situ hybridization, and semi-quantitative PCR.Genes Chromosom Cancer 1993;8:185–9.
[4] Ariyama Y, Fukuda Y, Okuno Y, Seto M, Date K, Abe T, NakamuraY, Inazawa J. Amplification on double minute chromosomes and par-tial tandem duplication of the MLL gene in leukemic cells of a patientwith acute myelogenous leukemia. Genes Chromosomes Cancer1998;23:267–72.
[5] Avet-Loiseau H, Gordon C, Li J-Y, Daviet A, Mellerin M-P, TalmantP, Harousseau J-L, Bataille R. Amplification of the 11q23 in acutemyeloid leukemia. Genes Chromosom Cancer 1999;26:166–70.
[6] Streubel B, Valent P, Jager U, Edelhauser M, Wandt H, Wagner T,Buchner t, lechner K, Fonatsch C. Amplification of the MLL gene ondouble minutes, a homogenously staining region, and ring chromo-somes in five patients with acute myeloid leukemia or myelodysplas-tic syndrome. Genes Chromosom Cancer 2000;27:380–6.
[7] Felix CA, Megonigal MD, Chervinsky DS, Leonard DGB, TsuchidaN, Kakati S, Block AMW, Fisher J, Grossi M, Salhany KI, Jani-SaitSN, Aplan PD. Association of germline p53 mutation with MLL seg-mental jumping translocation in treatment-related leukemia. Blood1998;91:4451–6.
[8] Allen RJ, Smith SD, Moldwin RL, Lu MM, Giordno L, Vignon C,Beau MM, Rowley JD, Zeleznik-Le N. Establishment and character-ization of a megakaryoblast cell line with amplification of MLL. Leu-kemia 1998;12:1119–27.
[9] Cuthbert G, McCullough S, Finney R, Breese G, Brown N. Jumpingtranslocation at 11q23 with MLL gene rearrangement and interstitialtelomeric sequences. Genes Chromosom Cancer 1999;24:295–8.
[10] Reddy KS, Parsons L, Wang S, Mak L, Dighe P, Yu TL. An AML-5apatient with segmental 11q23-MLL region identified using FISH.Can Genet Cytogenet 2000;118:48–51.
[11] Schnittger S, Kinkelin U, Schoch C, Heinecke A, Hasse D, HaferlachT, Buchner T, Wormann B, Hiddemann W, Griesinger F. Screeningfor MLL tandem duplication in 387 unselected patients with AMLidentify a prognostically unfavourable subset of AML. Leukemia2000;14:796–804.
[12] Caligiuri MA, Strout MP, Lawrence D, Arthur DC, Baer MR, Yu F,Knuutila S, Mrozek K, Oberkircher AR, Marcucci G, de la ChapelleA, Elonen E E, Block AW, Rao PN, Herzig GP, Powell BL, Ruutu T,Schiffer CA, Bloomfield CD. Rearrangement of ALL1 (MLL) inacute myeloid leukemia with normal cytogenetics. Cancer Res 1998;58:55–9.
[13] Yu M, Honoki K, Andersen J, Paietta E, Nam DK, Yunis JJ. MLLtandem duplication and multiple splicing in adult acute myeloid leu-kemia with normal karyotype. Leukemia 1996;10:774–80.
[14] Strout MP, Marcucci G, Bloomfield CD, Caligiuri MA. The partialtandem duplication of ALL1 (MLL) is consistently generated by Alu-mediated homologous recombination in acute myeloid leukemia.Proc Natl Acad Sci 1998;95:2390–5.
Table 1G-banding and FISH results
Sl # Age/Sex G-band Karyotype FISH
1 66/M 45
z
47,X,
2
Y[9],add(1)(p35)[9],
2
10,?add(11)(q23)[15],del(17)(p13)[9],add(17)(p11)[4],
2
20[4],mar1[11],mar
3
2[9][cp15]/89,XXYY,?add(11)(q23)
3
2,
2
10,
2
12,
2
16[2]/46,XY[3]
ish add(11)(q23)(wcp11
1
,MLL
11
or MLL
111
),mar(wcp11
1
,MLL
1
)
2 82/F 47,XX,der(5)t(5;7)(q13;q11.2),
2
7, der(11) add(11)(p13)del(11)(q14),13,
2
17,
1
r,
1
3mar
3
[cp13]/46,XX[4] predominantly in B-cell culture
mar. ish der(11)i(11)(qter
→
21::q13
→
q10::q10
→
q13::q21
→
qter) (wcp11
1
,D11Z1
1
,MLL
11
)
3
33 78/F 46,XX,
2
5,der(7;17)(p10;q10),del(8)(p21),t(11;22)(q23;q13),
2
13,add(16)(p11.2),der(16)t(13;16)(q14;q22),
2
18,add(20)(p13),
1
der(22)t(11;22)(q23;q13)
3
3,
1
r[cp19]/46,XX[1]
ish der(22)t(11;22)(MLL
1
)
3
3
4 86/M 48,XY,
1
11,
1
11,der(11)t(11;11)(p11.2;q14)
3
2[5]/46,XY[15]ish der(11)t(11;11)(MLL
11
)
3
2

K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
145
Tab
le 2
Sum
mar
y of
rep
orte
d ca
ses
with
seg
men
tal a
mpl
ific
atio
n of
11q
23 r
egio
n
Ref
.#
Sex/
Age
Prim
ary
Mal
igna
ncy
Tre
atm
ent
Dur
atio
n (y
rs)
Seco
ndar
yM
alig
nanc
ySu
rviv
altim
e (m
o)K
aryo
type
Tan
aka
(199
7)[1
]F/
63B
reas
t5-
FU7.
3A
ML
-M1
2.3
46,X
X,d
up(1
)(q2
5q44
),de
l(4)
(q25
q28)
,del
(5)(
q13q
31),
i(11
)(q1
0),d
er(1
2)t(
11;1
2)
(q23
;p12
),de
l(13
)(q1
2q14
),
2
14,
2
17,a
dd(1
9)(q
13),
der(
19)t
(?;?
11;1
9)(?
;q13
;q13
.4)
[27]
. nuc
ish
9q34
(AB
L
3
2
2
5), i
sh i(
11)(
CD
3
2
,ML
L
11
),de
r(12
) (C
D3
2
,ML
L
1)
Felix
(19
98)
[2]
M/2
Em
bryo
nal
rhab
dom
yo-
sarc
oma
Vin
, Act
-D, I
F,
ES,
DR
, CP
2A
ML
-M5
— (D
ead)
45,X
Y,d
er(5
)t(5
;11)
(5pt
er→
5q12
::11q
23→
11qt
er),
der
(11)
(pte
r→q1
2::q
24→
q12:
:q13
→qt
er),
217
.ish
der(
5)(M
LL
1,C
D31
,C11
q7q2
41),
der(
11)(
mul
tiple
co
pies
of
ML
L,C
D31
,C11
q7q2
41)
Alle
n (1
998)
[3]
M/6
8A
ML
-M1
343
,X,2
Y,a
dd(5
)(q1
3),d
ic(5
;9)(
p15;
p13)
,27,
1de
r(9)
t(9;
19)(
q11;
q11)
,dic
(9;?
;16;
?)
(9qt
er→
9p13
::?::1
6p11
→16
q22:
:?),
211
,116
,dic
(16;
21)(
q11;
p12)
,der
(17)
t(7;
17)
(p14
;p12
),2
19,2
19.
Cut
hber
t (19
99)
[4]
M/7
4A
ML
-M5a
——
2 da
ys46
,XY
,add
(11)
(q23
). is
h tr
p(11
)(q2
3) (
wcp
111
,ML
L1
11
)A
vet-
Loi
seau
(1
999)
[5]
F/53
Bre
ast c
ance
rFU
, ER
, CP
5A
ML
-M4
— d
ead
44,X
X,a
dd(3
)(p2
5),2
5,de
l(11
)(q1
3),2
15,2
16,d
el(1
7)(p
11),
218
,1r,
1m
ar1,
1z2
min
[16]
/43,
idem
,2r,
der(
3)t(
3;?)
(q27
;?),
add(
8)(p
12),
29,
1m
ar2[
7].is
h r(
ML
L
mul
tiple
sig
nals
), m
ar (
ML
L m
ultip
le s
igna
ls).
[6]
M/6
3A
ML
-M6
346
,XY
,add
(5)(
q12)
,27,
add(
11)(
q23)
,213
,add
(17)
(q22
), 1
2mar
[7].
ish
mar
(ML
L
mul
tiple
sig
nals
)St
reub
el (
2000
)[7
]M
/54
MD
S1
47,X
Y,t(
9;11
;22)
(p24
;q23
;q11
.1),
216
,1r3
2[10
]/46
, ide
m,2
Y[1
4] .
ish
r(11
) (w
cp11
1,M
LL
mul
tiple
sig
nals
)[8
]F/
67A
ML
-M5a
650
z52
,XX
,der
(5)t
(5;9
)(q2
2;q2
2)de
l(5)
(q22
q33)
,der
(8)(
qter
→pt
er::q
22→
q24:
:p1
1.2→
qter
),de
l(9)
(q22
),di
c(11
;13)
(11q
ter→
q23.
3::q
23.1
→11
q10:
:13p
12
→13
qter
),di
c(11
;13)
(11p
ter→
q10:
:q23
.3→
q23.
1::1
3p12
→13
qter
)113
,12z
4r.
ish
r(w
cp11
1,M
LL
mul
tiple
cop
ies)
[9]
M/6
3A
ML
-M6
246
,XY
,r(5
),ad
d(7)
(q22
),di
c(10
;11)
(p11
;q11
),de
r(15
)t(1
0;hs
r;15
)(p1
1;;p
12)/
44,
idem
,25/
46,id
em,1
8. I
sh d
er(1
5)(h
sr)(
wcp
111
,ML
L m
ultip
le s
igna
ls)
Red
dy (
2000
)[1
0]M
/66
Mye
lopr
olif
erat
ive
diso
rder
(M
PD)
HU
10A
ML
-M5a
1 w
eek
46z
47,X
,2Y
,add
(1)(
p35)
,210
,? a
dd(1
1)(q
23),
del(
17)
(p13
),1
mar
32
[cp9
]. is
h du
p (1
1)(q
23qt
er)(
ML
L1
1, w
cp11
1),d
el(1
7)(p
13)(
p532
),mar
32(
ML
L1
, wcp
111
)/ 46
,XY
,add
(11)
(q23
), a
dd(1
7)(p
11),
220
[4].
ish
dup
(11)
(q23
qter
)(M
LL
11
, w
cp11
1)/
452
46,X
Y, 2
10,a
dd(1
1)(q
23),
1m
ar[2
]. is
h du
p (1
1)(q
23qt
er) (
ML
L1
1,
wcp
111
), m
ar(M
LL
1,w
cp11
1)/
89,X
XY
Y,?
add(
11)(
q23)
32,
210
,212
,216
[2].
is
h tr
p (1
1)(q
23qt
er)(
ML
L1
11
,wcp
111
),du
p(11
)(q2
3qte
r)(M
LL
11
,wcp
1)/
46,X
Y[3
].Pr
esen
t[1
1]F/
82B
reas
t can
cer,
Lym
phom
aC
MF,
CX
, T
X, C
HO
P3
AM
L-M
14
47,X
X,d
er(5
)t(5
;7)(
q13;
q11.
2),2
7,de
r(11
)add
(11)
(p13
)del
(11)
(p14
),2
13,2
17,
1r,
1m
ar3
3[cp
13].
mar
ish
der(
11)i
(11)
(q21
qter
)(M
LL
11
, wcp
111
, D11
Z11
)/46
,XX
[4]
pred
omin
antly
in B
-cel
l cul
ture
[12]
F/78
AM
L-M
1Id
arub
acin
A
RA
-C6
part
ial
rem
issi
on46
,XX
,25,
der(
7;17
)(p1
0;q1
0),d
el(8
)(p2
1),t(
11;2
2)(q
23;q
13),
213
,add
(16)
(p11
.2),
de
r(16
)t(1
3;16
)(q1
4;q2
2),2
18,a
dd(2
0)(p
13),
1de
r(22
)t(1
1;22
)332
4,1
r[19
]. is
h de
r(22
)t(1
1;22
)(M
LL
1)3
3/46
,XX
[1]
[13]
M/8
6M
yelo
prol
ifer
ativ
e di
sord
erH
U6
MPD
One
-w
eek
48,X
Y,1
11,1
11,d
er(1
1)t(
11;1
1)(p
11.2
;q14
)32[
5]/4
6,X
Y[1
5]. i
sh d
er(1
1)t(
11;1
1)
(ML
L1
1)3
2
Abb
revi
atio
ns:
FU, f
luor
oura
cil;
Vin
, vin
cris
tine;
Act
-D, a
ctin
omyc
in D
; IF
, Ifo
sfam
ide;
ES,
eto
psid
e; D
R, d
oxor
ubic
in;
CP,
car
bopl
atin
um;
ER
, Epi
rubi
cin;
CP,
Cyc
loph
osph
amid
e; H
U, h
ydro
xyur
ea;
CM
F, c
ombi
natio
n ch
emot
hera
phy
for
brea
st c
ance
r hi
gh d
ose
cycl
opho
spha
mid
e, m
etho
trex
ate
and
FU a
nd C
X, C
ytox
an; T
X, T
amox
ifen
; CH
OP,
com
bina
tion
chem
othe
rapy
for
chr
onic
lym
phoc
ytic
leuk
e-m
ia in
clud
ing
cycl
opho
spha
mid
e, d
oxor
ubic
in, v
incr
istin
e an
d pr
edni
sone
; AM
L, a
cute
mye
loid
leuk
emia
with
the
subc
lass
M1,
M5,
M5a
.

146 K.S. Reddy et al. / Cancer Genetics and Cytogenetics 126 (2001) 139–146
[15] Flannery JT, Boice JD Jr., Devesa SS, Kleinerman RA, Curtis RE,Fraumeni JF Jr. Natl Cancer Inst Monogr 1995;68:13–24.
[16] Donaldson SS, Hancock SL. Second cancers after Hodgkin’s diseasein childhood. N Engl J Med 1997;334:792–3.
[17] Wolden SL, Lamborn Kl, Cleary SF, Tate DJ, Donalson SS. Second
cancers following pediatric Hodgkin’s disease. J Clin Oncol 1998;16:536–44.
[18] Travis LB, Curtis RE, Boice JD Jr., Platz CE, Hankey BF, FraumeniJF Jr., (1996). Second malignant neoplasms among long-term survi-vors of ovarian cancer. Cancer Res 1996;56:1564–70.