Embed Size (px)
Citation preview

Seda%on – Part Deux Sarah Ahn DDS
SBH Pediatric Den1stry
Sedation • Controlled, pharmacologically induced, minimally depressed
level of consciousness that retains the patient’s ability to maintain a patent airway independently and continuously and respond appropriately to physical and/or verbal commands
• Objectives: – Control behavior/movement to allow treatment – Control anxiety, fear – Amnesia
Sedation • Oral, intravenous, nasal routes • Examples of drugs used: Midazolam, Chloral Hydrate, Demerol • Documentation:
– Informed consent – Pre- and Post-op instructions – Pre-op health evaluation
• Claims of allergy to sedation meds – literature does not support
– Time-based records • Name(s)/dosages/administration routes of drugs (including LA) • HR, RR, O2 saturation, level of consciousness/responsiveness, BP
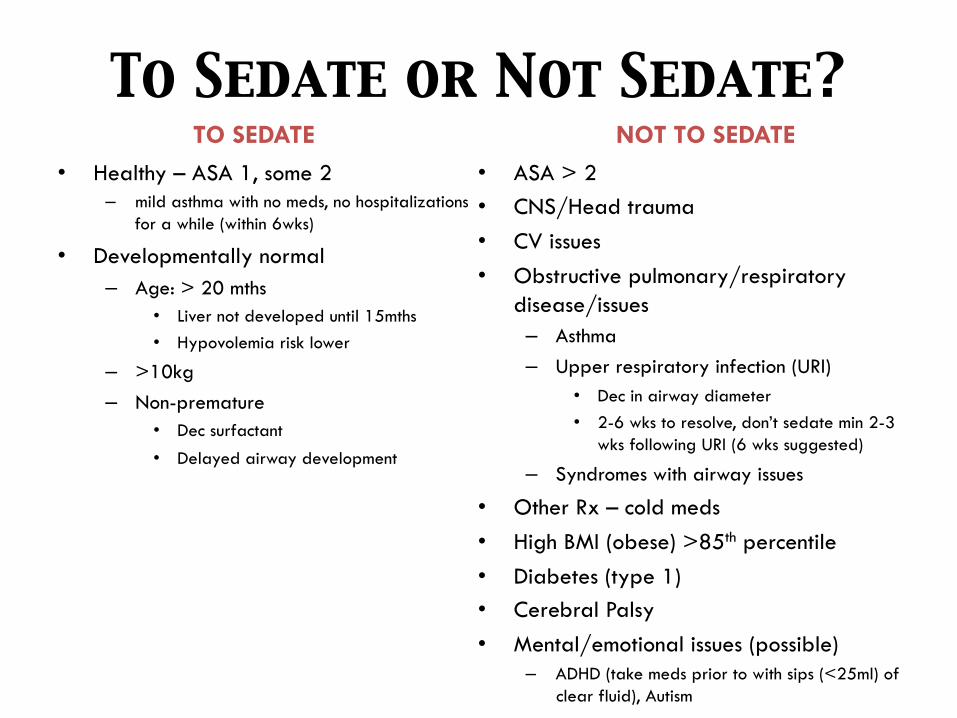
To Sedate or Not Sedate? • Healthy – ASA 1, some 2
– mild asthma with no meds, no hospitalizations for a while (within 6wks)
• Developmentally normal – Age: > 20 mths
• Liver not developed until 15mths • Hypovolemia risk lower
– >10kg – Non-premature
• Dec surfactant
• Delayed airway development
• ASA > 2 • CNS/Head trauma • CV issues • Obstructive pulmonary/respiratory
disease/issues – Asthma – Upper respiratory infection (URI)
• Dec in airway diameter • 2-6 wks to resolve, don’t sedate min 2-3
wks following URI (6 wks suggested)
– Syndromes with airway issues
• Other Rx – cold meds • High BMI (obese) >85th percentile • Diabetes (type 1) • Cerebral Palsy • Mental/emotional issues (possible)
– ADHD (take meds prior to with sips (<25ml) of clear fluid), Autism
TO SEDATE NOT TO SEDATE
To Drug Before Sedation Tx? • Procedural sedation must not be administered without direct
supervision by trained medical personnel – Liability issues
• Meds (e.g., Benadryl) the night before sedation? – Not effective in helping with sedation if young child

THE DRUGS
Local Anesthetics!
• Cross blood-brain barrier • When combined with sedation, LA dosages must be adjusted
and decreased to prevent overdose – Calculate the mg/carpules that you can use prior to tx
• Limits how much tx you can provide
– Exception: 4% Septocaine with epi – Lidocaine metabolites may produce sedation
• So instead of 4.4mg/kg, use 4mg/kg – Mepivacaine is very potent – so avoid in kids – RULE OF THUMB FOR MAX DOSAGE: 4mg/kg
Local Anesthetics!
• When giving LA injections in your patient’s mouth, avoid injecting posterior to the 2M due to the risk of hitting the venous plexus – Best to inject between the 1M and 2M
• Topical anesthesia: compounded topicals (2 types of anes) – Associated with deaths – EMLA: emulsion of lidocaine 2.5% and prilocaine 2.5% (1:1 ratio)
• OraVerse – Useless if overdose
• In fact since it causes vasodilation, it will lead to an increase in systemic LA à lead to increased toxicity
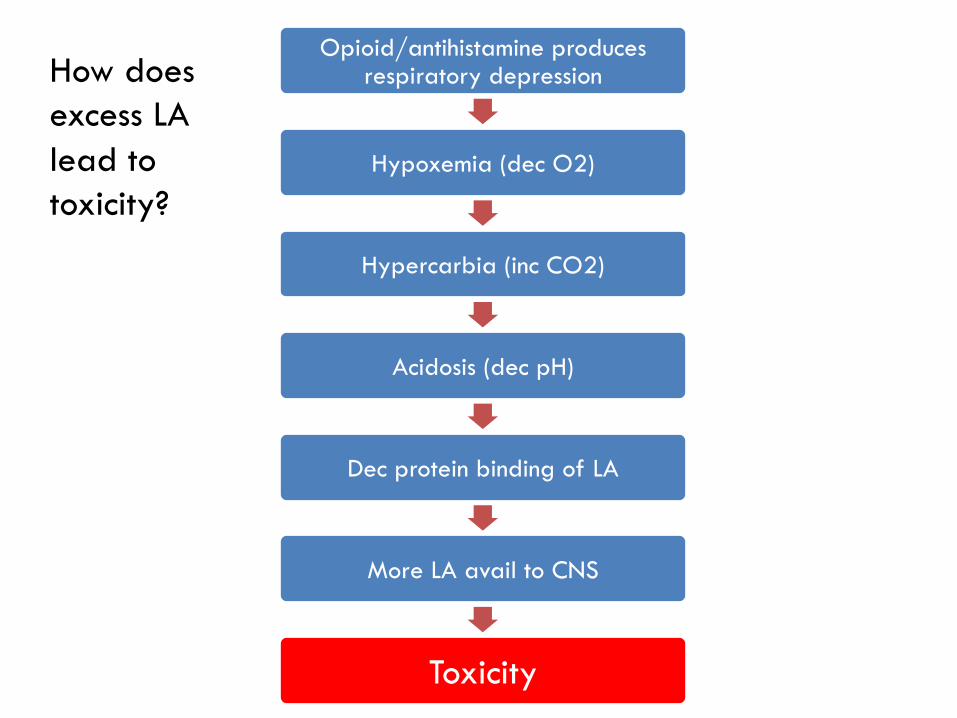
Opioid/antihistamine produces respiratory depression
Hypoxemia (dec O2)
Hypercarbia (inc CO2)
Acidosis (dec pH)
Dec protein binding of LA
More LA avail to CNS
Toxicity
How does excess LA lead to toxicity?
Nitrous Oxide (N2O)
• Deepens sedation slightly without adversely affecting resp • Aids in “settling” patient
– Increase N2O (70%) during more unsettling periods (e.g., LA, RDI) – Wait 5-10mins for desired effect – Dec to 40-50% after settling
• Potentiation of other sedation meds? – Caution with Mep as both are nauseating
• Supplemental O2
SEDATIVE-HYPNOTICS
Three classes: • Anti-anxiety benzodiazepines - Diazepam, Midazolam • Non-barbiturates - Chloral Hydrate • Barbiturates - Pentobarbital
Choral Hydrate (CH)
• Non-barbiturate sedative-hypnotic • CNS depression with min CV/resp depression • Gastric irritation • May result in hypotonic tongue – airway! • Onset: 30-60mins, peak 60mins, duration 5 hrs • Working time: up to 60mins • Dose: 25-50mg/kg orally; 1gm max
– Lower dosage if in combo with other Rx
• Converted to alcohol via liver • No reversal agent • No longer mass produced in liquid form in the US
(Pharmaceutical Associates Inc) as of April 2012 – Avail as capsules; must be compounded into liquid form by pharmacists
Meperidine (Demerol)�• Narcotic • Sedation, analgesia • CNS, CV, Respiratory depression; hypotension • Histamine release à avoid submucosal, IM, IV
– Use Fentanyl
• Oral or parental (even submucosal) • Dosage: 1-2mg/kg; max 50mg • Onset: 30mins, peak 1-2 hrs; duration 2-4 hrs • Working time: 60mins • Reversal agent: Naloxone
– 0.01 mg/kg (slow reversal) – 0.1mg/kg (fast reversal; for severe resp depression; rec by PALS) – IV, sublingual – Excess can cause pulmonary edema
Hydroxyzine (Vistaril, Atarax)
• Antihistamine • CNS depression – anxiolytic • Analgesia • 1-2 mg/kg orally; max 50mg • Onset 15-30mins, 2-4 hrs duration • Working time: 30-45mins • Used with CH or Mep
Diazepam (Valium)�• Benzodiazepine • Anxiolytic, sedative hypnotic, anticonvulsant, mild anterograde
amnesia • Min CV, resp depression • Better with older pts; rare with young kids • Dosages: 1mg/yr of age or 0.2-0.3mg/kg
– 2-5mg (2-5yo), 5-10mg (6-10yo), 10-15mg (11-20yo)
• Onset 45-60mins, peak 60mins • Working time: 30-90mins • Reversal: Flumazenil (0.1mg/kg)
– Submucosal, IM, intranasal, IV (fastest) – 2-3mins – Excess can cause seizures
Midazolam (Versed)
• Benzodiazepine • More reliable/profound amnesia than Diazepam • 3-4x more potent than Diazepam • Dosages:
– Oral: 0.25mg to 1.0mg/kg (avg: 0.5mg/kg); max 15mg (20mg if older child)
– Submucosal: 0.2-0.3mg/kg – Intra-nasal (with atomizer; faster onset): 0.2-0.3mg/kg
• Onset: 5mins (usually 15mins) • Working time: 20-30mins
Midazolam (Versed)
• Combined use with N2O – Sometimes N2O may not help in settling pt à don’t wait and just start
working
• Respiratory depression – usually seen if >0.75mg/kg dosages, IV route or rapid administration (submucosal)
• Reversal: Flumazenil (0.1mg/kg) – Submucosal, IM, intranasal, IV (fastest) – 2-3mins – Excess can cause seizures – Watch for re-sedation
Ketamine
• Can give orally • General anes rx à GA credentials • Hypersalivation
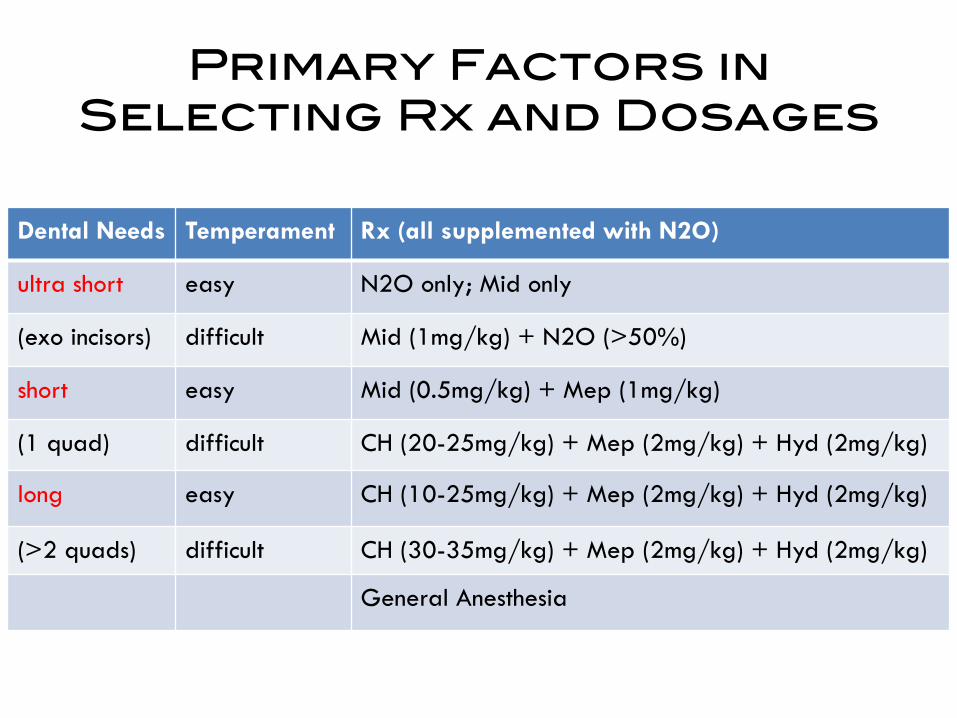
Primary Factors in !Selecting Rx and Dosages!
Dental Needs Temperament Rx (all supplemented with N2O)
ultra short easy N2O only; Mid only
(exo incisors) difficult Mid (1mg/kg) + N2O (>50%)
short easy Mid (0.5mg/kg) + Mep (1mg/kg)
(1 quad) difficult CH (20-25mg/kg) + Mep (2mg/kg) + Hyd (2mg/kg)
long easy CH (10-25mg/kg) + Mep (2mg/kg) + Hyd (2mg/kg)
(>2 quads) difficult CH (30-35mg/kg) + Mep (2mg/kg) + Hyd (2mg/kg)
General Anesthesia
One Lump or Two (or Three)?
• Single Rx: – Minimize adverse effects – Decrease likelihood of drug dosing error(s)
• Combos of Rx: – Potentiate/summate drug effects – Complement or expand rx classes or effects (e.g., analgesic
with sedative) – Increase working time
Most Frequently Used Drugs and Combos
• Midazolam • Diazepam • Triple combo (CH+Hyd+Mep) • CH+Hyd • Triple combo (Mid+Hyd+Mep)
Which Combo Would You Like?
• Mild Sedation Combo: – Midazolam + Hydroxyzine
• Indicated for mild-mid fearful child who is potentially cooperative • 0.5mg/kg Mid + 1-2mg/kg Hyd • Onset: 10-20mins • Working time: 30-45mins • Less crying than mid alone • Possible inc working time • Can’t reverse Hyd
• Moderate to Deep Combos: – CH combos -- Triple cocktails
• High CH (50mg/kg) + Mep (1mg/kg) + Hyd (1-2mg/kg) • Low CH (10-25mg/kg) + Mep (2mg/kg) + Hyd (2mg/kg)
– Higher CH – deeper sedation – Higher Mep – more analgesia
• Ideally want to use capnograph • Working time longer than 40mins • Settling with N2O highly recommended • Airway! Laryngospasm risk • Only Mep is reversible
– CH combos -- Doubles: • CH (20-40mg/kg) + Hyd (1-2mg/kg)
– Onset: 20mins, working time: 1-1.5hrs
• Moderate to Deep Combos: – Midazolam Combos:
• Mid (0.5-1mg/kg) + Hyd (25mg/kg) + Mep (1mg/kg) • Two reversible agents used • Shorter duration of onset (than CH) – 25-30mins • Quicker recovery • Possible increase in amnesia? • Wilson finds it not as effective at CH combos • There is literature to support
– Note: Diazepam (0.2mg/kg) + Hyd + Mep à no literature yet
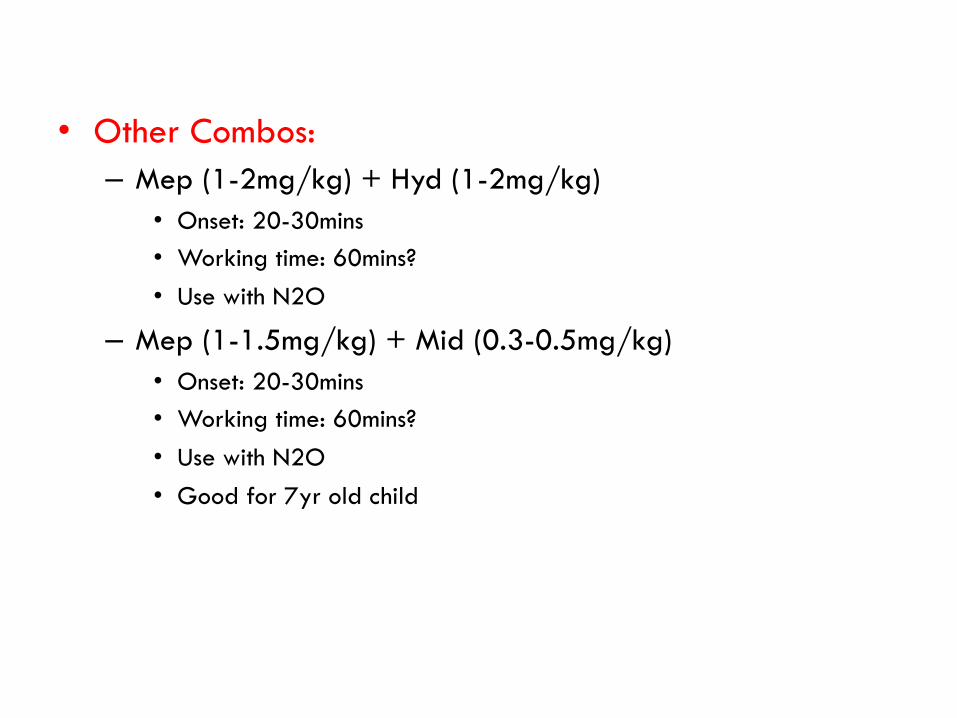
• Other Combos: – Mep (1-2mg/kg) + Hyd (1-2mg/kg)
• Onset: 20-30mins • Working time: 60mins? • Use with N2O
– Mep (1-1.5mg/kg) + Mid (0.3-0.5mg/kg) • Onset: 20-30mins • Working time: 60mins? • Use with N2O • Good for 7yr old child
What If I Can Only Use 2 Drugs?
• If limited to two drugs, 3-6 yr old child – Midaz + Mep – Mep + Hyd (Benadryl)
IV Sedation
• Rx: – Midazolam is the idea drug – Meperidine not ideal but will provide analgesia – Fentanyl is common
IV Sedation
• Advantages: – Predictable and precise – 100% bioavailable – Titratable – Rapid onset – Emergency Rx access – Reversible
• Disadvantages: – Requires highest level of
monitoring – Supplies – cost – Significant training
required • Starting IV • Montefiore, UCLA, USC
– Different state permit may be involved
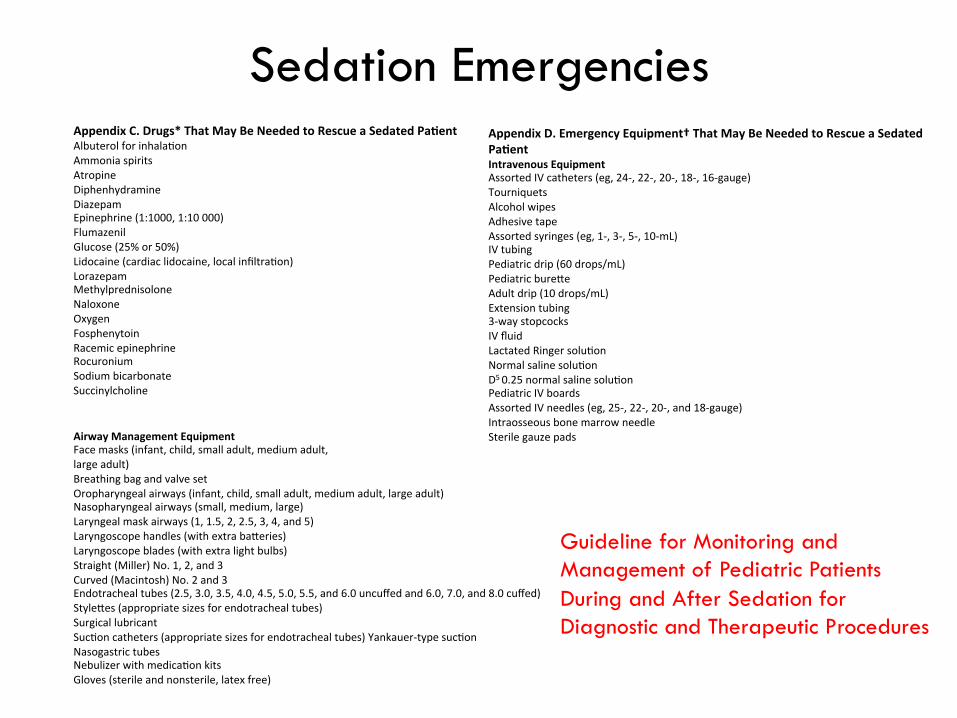
Appendix C. Drugs* That May Be Needed to Rescue a Sedated Pa%ent Albuterol for inhala1on Ammonia spirits Atropine Diphenhydramine Diazepam Epinephrine (1:1000, 1:10 000) Flumazenil Glucose (25% or 50%) Lidocaine (cardiac lidocaine, local infiltra1on) Lorazepam Methylprednisolone Naloxone Oxygen Fosphenytoin Racemic epinephrine Rocuronium Sodium bicarbonate Succinylcholine
Appendix D. Emergency Equipment† That May Be Needed to Rescue a Sedated Pa%ent Intravenous Equipment Assorted IV catheters (eg, 24-‐, 22-‐, 20-‐, 18-‐, 16-‐gauge) Tourniquets Alcohol wipes Adhesive tape Assorted syringes (eg, 1-‐, 3-‐, 5-‐, 10-‐mL) IV tubing Pediatric drip (60 drops/mL) Pediatric bure\e Adult drip (10 drops/mL) Extension tubing 3-‐way stopcocks IV fluid Lactated Ringer solu1on Normal saline solu1on D5 0.25 normal saline solu1on Pediatric IV boards Assorted IV needles (eg, 25-‐, 22-‐, 20-‐, and 18-‐gauge) Intraosseous bone marrow needle Sterile gauze pads
Sedation Emergencies
Airway Management Equipment Face masks (infant, child, small adult, medium adult, large adult) Breathing bag and valve set Oropharyngeal airways (infant, child, small adult, medium adult, large adult) Nasopharyngeal airways (small, medium, large) Laryngeal mask airways (1, 1.5, 2, 2.5, 3, 4, and 5) Laryngoscope handles (with extra ba\eries) Laryngoscope blades (with extra light bulbs) Straight (Miller) No. 1, 2, and 3 Curved (Macintosh) No. 2 and 3 Endotracheal tubes (2.5, 3.0, 3.5, 4.0, 4.5, 5.0, 5.5, and 6.0 uncuffed and 6.0, 7.0, and 8.0 cuffed) Style\es (appropriate sizes for endotracheal tubes) Surgical lubricant Suc1on catheters (appropriate sizes for endotracheal tubes) Yankauer-‐type suc1on Nasogastric tubes Nebulizer with medica1on kits Gloves (sterile and nonsterile, latex free)
Guideline for Monitoring and Management of Pediatric Patients During and After Sedation for Diagnostic and Therapeutic Procedures
Emergencies
So…The Future �
• Due to demands of parents and child-rearing practices, sedation will become more common or in demand
• IV sedation will become more popular • Dental anesthesia will have an increasingly important role • Be aware of the state’s regulations with sedations
– Personnel – Monitoring
• Follow AAPD guidelines – Monitoring personnel
– Crash cart requirements