Embed Size (px)
Citation preview

CompassPoint Nonprofit Serviceswww.compasspoint.org
Funded by
The California Wellness Foundation
Community Clinics Initiative (A joint project of Tides and The California Endowment)
October, 2003
ByJeanne Peters, M.N.A.,Principal Investigator
Catalina Ruiz-Healy and Kara Vassily, Research Associates
A Profile of CommunityClinic and Health CenterLeadership in California
A Study Commissioned bythe Regional & State ClinicAssociations of California
Securing the Safety Net

Contents
I Acknowledgements
II Executive Summary
III Introduction and Background to the Study
IV Methodology and Sample Clinic Demographics
V Findings: Clinic CEOs
A. Characteristics
B. Career Paths to CEO
C. Salaries
D. Job Rewards and Challenges
E. Tenure and Post-CEO Career Paths
VI Findings: Clinic Consortia/Association CEOs
VII Calls to Action
A. Clinic and Consortia CEOs
B. Boards of Directors
C. Associations and Technical Assistance Providers
D. Funders
VIII Conclusion
Appendixes
A. Survey Instrument
B. List of Participants
C. Succession Planning Bibliography
D. About CompassPoint Nonprofit Services
Inside Front Cover

1© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
I
AcknowledgementsThis study’s Advisory Committee played a numberof key roles to ensure the success of the project.Committee Members advised the CompassPointresearch team on the overall research questionsand design of the survey instrument. They alsovolunteered considerable amounts of their time toencourage CEO participation across the State andprovide editorial feedback on the final report.
CompassPoint gratefully acknowledges theMembers of the Advisory Committee:
Yvonne Bice, Executive DirectorCentral Valley Network
Debra Farmer, President/CEOWestside Family Health Center
John Gressman, President/CEOSan Francisco Community Clinic Consortium
Kathy Lim Ko, Program DirectorCommunity Clinics Initiative
Marty Lynch, CEOLifelong Medical Group
Mary Murphy, Executive DirectorDarin M. Camarena Health Center
Margie Fites Seigle, CEOCalifornia Family Health Council
CompassPoint and Members of the AdvisoryCommittee thank the funders of this project:
The California Wellness Foundation
The Community Clinics Initiative (A joint project
of Tides and The California Endowment)
CompassPoint and Members of the AdvisoryCommittee acknowledge the regional andstatewide associations of California.
Consortia NameAlameda Health ConsortiumAlliance for Rural Community HealthCalifornia Family Health CouncilCalifornia Primary Care AssociationCentral Valley Health NetworkCoalition of Orange County Community ClinicsCommunity Clinic Association of Los AngelesCountyCommunity Clinic Consortium Of Contra CostaCommunity Health PartnershipCouncil of Community ClinicsNorth Coast Clinics NetworkNorthern Sierra Rural Health NetworkPlanned Parenthood Affiliates of CaliforniaRedwood Community Health CoalitionSan Francisco Community Clinic ConsortiumShasta Consortium of Community Health Centers
Web Sitewww.chcn-eb.orgwww.ruralcommunityhealth.orgwww.cfhc.orgwww.cpca.orgwww.cvhnclinics.orgwww.forhealthoc.orgwww.ccalac.orgwww.clinicconsortium.orgwww.chpscc.orgwww.ccc-sd.orgwww.northcoastclinics.orgwww.nsrhn.orgwww.ppacca.orgwww.rchc.netwww.sfccc.orgwww.shastaconsortium.org
Finally, we thank the more than 100 individualCEOs who gave of their time to complete oursurvey, attend a focus group, or provide aninterview. We hope that this report reflectsaccurately and meaningfully the enormous rewardsand challenges of the work that they do providingthe health care safety net for California’s low-income and uninsured residents.
2 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
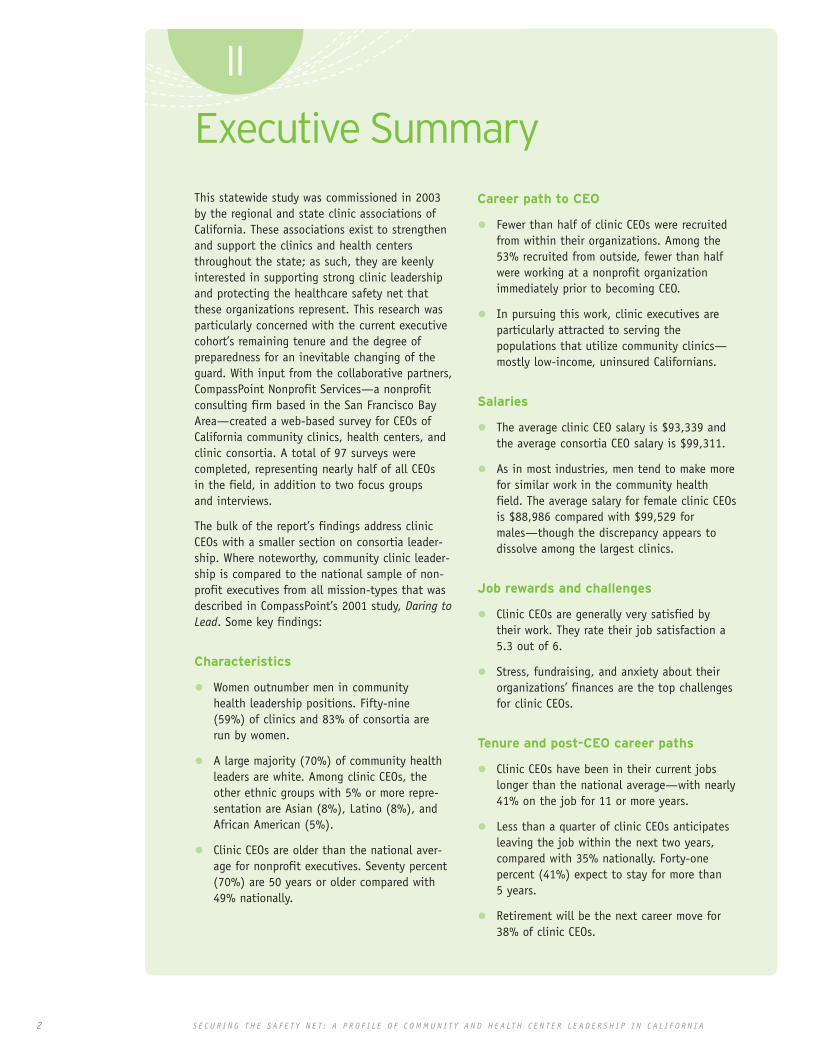
This statewide study was commissioned in 2003by the regional and state clinic associations ofCalifornia. These associations exist to strengthenand support the clinics and health centersthroughout the state; as such, they are keenlyinterested in supporting strong clinic leadershipand protecting the healthcare safety net thatthese organizations represent. This research wasparticularly concerned with the current executivecohort’s remaining tenure and the degree ofpreparedness for an inevitable changing of theguard. With input from the collaborative partners,CompassPoint Nonprofit Services—a nonprofitconsulting firm based in the San Francisco BayArea—created a web-based survey for CEOs ofCalifornia community clinics, health centers, andclinic consortia. A total of 97 surveys werecompleted, representing nearly half of all CEOsin the field, in addition to two focus groupsand interviews.
The bulk of the report’s findings address clinicCEOs with a smaller section on consortia leader-ship. Where noteworthy, community clinic leader-ship is compared to the national sample of non-profit executives from all mission-types that wasdescribed in CompassPoint’s 2001 study, Daring toLead. Some key findings:
Characteristics
• Women outnumber men in communityhealth leadership positions. Fifty-nine(59%) of clinics and 83% of consortia arerun by women.
• A large majority (70%) of community healthleaders are white. Among clinic CEOs, theother ethnic groups with 5% or more repre-sentation are Asian (8%), Latino (8%), andAfrican American (5%).
• Clinic CEOs are older than the national aver-age for nonprofit executives. Seventy percent(70%) are 50 years or older compared with49% nationally.
Career path to CEO
• Fewer than half of clinic CEOs were recruitedfrom within their organizations. Among the53% recruited from outside, fewer than halfwere working at a nonprofit organizationimmediately prior to becoming CEO.
• In pursuing this work, clinic executives areparticularly attracted to serving thepopulations that utilize community clinics—mostly low-income, uninsured Californians.
Salaries
• The average clinic CEO salary is $93,339 andthe average consortia CEO salary is $99,311.
• As in most industries, men tend to make morefor similar work in the community healthfield. The average salary for female clinic CEOsis $88,986 compared with $99,529 formales—though the discrepancy appears todissolve among the largest clinics.
Job rewards and challenges
• Clinic CEOs are generally very satisfied bytheir work. They rate their job satisfaction a5.3 out of 6.
• Stress, fundraising, and anxiety about theirorganizations’ finances are the top challengesfor clinic CEOs.
Tenure and post-CEO career paths
• Clinic CEOs have been in their current jobslonger than the national average—with nearly41% on the job for 11 or more years.
• Less than a quarter of clinic CEOs anticipatesleaving the job within the next two years,compared with 35% nationally. Forty-onepercent (41%) expect to stay for more than5 years.
• Retirement will be the next career move for38% of clinic CEOs.
Executive Summary
II

3© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
• Only 8% of clinic CEOs anticipates theirnext career move to be as CEO of anothernonprofit clinic.
• Half of clinic CEOs have identified one or morepersons as a potential successor.
Boards and other sources of supportand training:
• Clinic CEOs perceive their boards to be mosteffective at mission advocacy and least effec-tive at fundraising.
• CEOs at smaller clinics perceive their boardsto be less effective in key governance areasthan CEOs at larger clinics do.
• Clinic CEOs rely heavily on their managementteams and peers as sources of support andinformation.
Summary of Calls to Action
CEOs
• Recognize succession planning as a necessaryaspect of organizational leadership.
• Develop future leaders.
• Insist on and model a sustainable approach toorganizational leadership.
Clinic Boards of Directors
• Recognize succession planning as a funda-mental aspect of organizational governance.
• Take responsibility for board education anddevelopment.
Associations and Consortia
• Build awareness among members about theemerging field of executive leadership services.
• Consider board and organizational structurechanges to mitigate competition and conflictamong members.
Funders
• Fund realistic infrastructure costs.
• Fund executive access to leadership services.
The overall impression is of a deeply committedcadre of healthcare leaders—many of whomplayed founding roles in the community healthmovement in the 1960s and 1970s. In a contextof increasing need for their services and ever-changing political and funding priorities, theyhave to face what they commonly refer to asthe “graying of the sector.” That is, the fieldwill have to focus its attention on the transi-tion of a core group of its founding leaders. Ofcourse those who aren’t leaving any time soonalso need attention; the data suggest a numberof opportunities to better support them. Thisreport concludes with a series of Calls toAction—ways that CEOs, boards of directors,associations, and funders can help ensure thatquality leadership is cultivated and retained.
In this report, we use the terms “clinic” and “healthcenter” interchangeably knowing that some organizationsprefer one or the other. Although a variety of titles areused for the senior staff position at community clinics andhealth centers—sometimes president or executive director,for example—the term “CEO” is the most widely used, so itis the term we use throughout the report.
A WORD ON TERMINOLOGY:

4 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
Across the State of California there are
nearly 200 community clinics, health
centers, and free clinics with some 500
clinic locations. Each year, these health
centers and clinics provide health care
services to more than 1 million patients:
the uninsured, under-insured, and
patients using government programs to
pay for their health care. The clinics and health centers have been the backbone of thehealth care safety net—providing neighborhoodbased, culturally and linguistically appropriatemedical services for people of all ages and back-grounds. Over the past 30+ years, many clinicleaders have been pioneers in forging this healthcare delivery system to assure that all Califor-nians have access to care in their communities.
Supporting the community clinics are clinic-gov-erned networks created over the last 25 years tohelp them expand access to care, join forces tofacilitate their service delivery, and provide lead-ership in health policy at the local, state, andfederal levels. Today, there are 13 networks andthree statewide organizations that meet regular-ly to develop statewide strategy around thechanging needs of the clinics and their patients.
This statewide study was inspired byCompassPoint’s 2001 report, Daring to Lead:Nonprofit Executive Directors and Their WorkExperience—a national study of 1,100 nonprofitexecutives from all organizational sizes andmissions. The collaborative responsible forfunding and guiding this project determinedthat Daring to Lead raised important questionsabout leadership in the community clinics andhealth centers in California. Clinic and networkleadership recognize that a generation ofcommunity health center founders and long-time leaders is rapidly approaching retirementage and that fostering new leadership willbecome a clear priority in the near term.
The report concludes with a series of Calls toAction for CEOs, boards, associations, andfunders and is intended to be a spark fordialogue among the stakeholders invested inpreserving and strengthening the communityhealth safety net.
III
Introduction andBackground to the Study

5© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
Primary data for this study was collected
through a 50-question web-based
survey and from two focus groups held
in Northern and Southern California.
SurveyIn February 2003 a letter signed by Jan Masaoka,Debra Farmer, and Yvonne Bice was sent by U.S.mail to a list of 185 clinic and consortia CEOs.The Community Clinics Initiative provided themailing list to CompassPoint. The letter invitedCEOs to take the 50-question web-based survey.After an initial round of responses, the research-ers sent a reminder email to non-respondents;additionally, Advisory Committee membersencouraged participation through their peer net-works. Ultimately, 97 CEOs completed the onlinesurvey: 82 from clinics and health centers, and 15from consortia. This represents a 52% responserate. The surveys were anonymous and respon-dents are quoted without attribution throughoutthis report. Please see Appendix B for a completelist of participating organizations. Appendix A isa full copy of the online survey instrument.
The survey sample includes clinics of all budget,staff, and client population sizes from all acrossCalifornia. Following are the key demographics of thesample‘s 82 clinics (consortia are not included here).
Because many clinic corporations have more thanone site, the categories in Figure 1 are difficult toapply consistently. Seventeen percent (17%) ofrespondents chose a combination of location typesin responding to the question of primary location.
Figures 2, 3, and 4 are indicators of clinic size:operating budget, number of paid staff, and num-ber of unduplicated patients per year. In order tosurface any management differences inherent inrunning a smaller community clinic, we lookedcarefully at how clinics were distributed acrossthese three variables. Interestingly, the number ofunduplicated patients seen per year is the leastreliable indicator of overall clinic size; that is,some clinics that see fewer than 5,000 patientsper year nonetheless have operating budgets ofmore than $1 million and paid staffs of more than25 people. A cohort of “small clinic” respondents
FIGURE 1 Clinic Respondents by Main Office Location Type
Location No. of respondents % of respondentsUrban 40 49.4Sub-urban 4 5.1Rural 16 20.3Frontier 7 8.9Some combination of above 14 16.5
82 100%
FIGURE 2 Clinic Respondents by Operating Budget Size
Budget No. of respondents % of respondents< $1 million 10 12.2$1 – 2.99 million 21 25.6$3 – 4.99 million 12 14.6$5 – 9.99 million 16 19.5$10 – 19.99 million 16 19.5$20 million and above 7 8.6
82 100%
FIGURE 3 Clinic Respondents by Paid Staff Size
Paid staff No. of respondents % of respondents0 - 25 17 20.726 - 50 15 18.351 - 99 18 22.0100 - 299 25 30.5300 and above 7 8.5
82 100%
FIGURE 4 Clinic Respondents by No. of Unduplicated Clients Per Year
Clients No. of respondents % of respondents< 5,000 19 23.25,000 – 9,999 15 18.310,000 – 29,999 30 36.630,000 – 49,999 8 9.850,000 and above 9 12.1
81 100%
FIGURE 5 Clinics by Year Founded
Year founded No. of respondents % of respondents< 1960s 3 3.81960s 10 12.81970s 45 55.61980s 8 9.91990s to present 15 18.5
81 100%
Methodology + Clinic Demographics
IV
6 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
was identified as having both of the followingcharacteristics: paid staff of fewer than 25 peopleand unduplicated patients per year of fewer than10,000. There are 14 respondents in this group—10 of whom have operating budgets of less than$1 million (the remaining four are all under $3million). Where noteworthy throughout the clinicCEO findings, we distinguish between this cohortof 14 small clinics and the other 68 respondents.
Focus Groups and InterviewsThe CompassPoint research team conducted twoone-and-a-half hour focus groups for clinic CEOsas well as interviews with 2 executives who wereunable to attend the groups. The line ofquestioning followed the survey instrument, withparticular emphasis on job challenges, rewards,and succession issues. The focus groups wereaudio taped and a number of focus group/interview participants are quoted withoutattribution in this report.
Paula Cohen, Mendocino Coast Clinics, Fort Bragg
Orvin Henson, Indian Health Council, PaumaValley
George Provencher, Consolidated Tribal Health,Redwood Valley
Jim Ruiz, United Health Centers, Parlier
Steve Schilling, Clinica Sierra Vista, Bakersfield
Mary Szecsey, West County Health Centers,Guerneville
Kuldip Thusu, Alta Familia Health Clinic, Dinuba
Carl Coan, Eisner Pediatric and Family MedialCenter, Los Angeles
Debra Farmer, Westside Family Health Center,Santa Monica
Jann Hamilton Lee, South Bay Family HealthCenter, Los Angeles
Margie Martinez, CHAP, Pasadena
Kazue Shibata, Asian Pacific Healthcare Venture,Los Angeles
Gay Kaplan, Curry Senior Center, San Francisco
Nance Rosencranz, Marin Community Clinic, Marin

7© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
CEO Characteristics
Gender Overall, there are more female CEOsthan male. Of the 81 clinic CEOs who providedtheir gender, 33 (41%) are male and 48 (59%)female. There are equal or nearly equal numbers ofwomen and men in 4 out of 6 clinic budget cate-gories. It is among clinics in the $1-5 millionrange where women significantly outnumber men;among these 33 clinics, there were 23 female and9 male CEOs1. This trend of equal representationamong the smallest and largest organizationsvaries dramatically from the national sample ofnonprofits in which 69% of the smallest nonprofitsare run by women and 59% of the largest are runby men.
Age A large majority of clinic executives are 50years old or older. Compared with the national sam-ple, clinic executives are significantly more likely tobe in their 50s and 60s. Whereas 51% of nonprofitexecutive directors are less than 50 years old, just30% of clinic CEOs are in this age group. Clearly,the baby boom population played a founding lead-ership role in building the community health move-ment and can be described as the first “seniorclass” of the community clinic sector. This raisesconcerns about the readiness of the next wave ofleadership; we address these issues in Section E,beginning on page 12.
Race/ethnicity The majority of clinic andhealth center CEOs are European/white, with 70%of the sample in this category. An open-ended sur-vey question about diversity yielded a range ofresponses from CEOs. A number of respondentsmentioned specifically the dearth of AfricanAmerican executives among California’s communityclinics and health centers; they make up 5% of thecurrent leadership cohort. Some respondentsargued that race and ethnicity ought not to be asignificant factor in identifying clinic leadership—noting that the difficulty of the job requires com-petency first and foremost; this respondent’s com-ment captures this sentiment: “As we serve diversepopulations, it is nice if people of color are inmanagement positions, but only if they are compe-tent and capable of doing the job.” Others arguedthat diversity should be cultivated intentionallybecause it is aligned with the community healthmission. As one CEO wrote, “Diversity is critical as
Findings: Clinic CEOs
V
A
FIGURE 6 Gender of Executive Directors by Budget Size
FIGURE 7 Age of Clinic CEOs Compared with Nonprofits Generally
FIGURE 8 Race/Ethnicity of Clinic CEOs2
1 One respondent inthis budget categorydid not providehis/her gender.
2 The 7.7% “Other” inFigure 9 includesrespondents whoidentified as NativeAmerican, MiddleEastern, and “other.”
“Unfortunately right now it's oftena choice between hiring someonebecause they are the appropriateminority or hiring someone who isnot, but has the appropriate level ofskills to take the clinic where it needsto go. Good minority candidates arein high demand — as they should be —but there aren't enough qualifiedminority candidates to go around.”
80
60
40
20
0
60
40
20
0
$10-19.99million
ClinicsNonprofits
Perc
ent
of C
EOs
Perc
ent
of C
EOs
$20+million
< $1million
<40 years old 40-49 years old 50-59 years old 60+ years old
AfricanAmerican5.1%
Other 7.7%
AsianAmerican7.7%
Latino 9%
$1-2.99million
$3-4.99million
$5-9.99million
50
4.918
25.6
33
52.2
37
18.312
50 50 50
67
29
67
29
75
25
50 50
WomenMen
White70.5%
8 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
it relates to social justice and thepopulations we serve. Self determi-nation is extremely important.”Several respondents questionedwhether the pipeline of candidatesis itself diverse enough:“Professional and academic institu-tions are failing to produce racial-ly/ethnically diverse graduates whoknow about the nonprofit world,community needs, and professionalapproaches or solutions.”
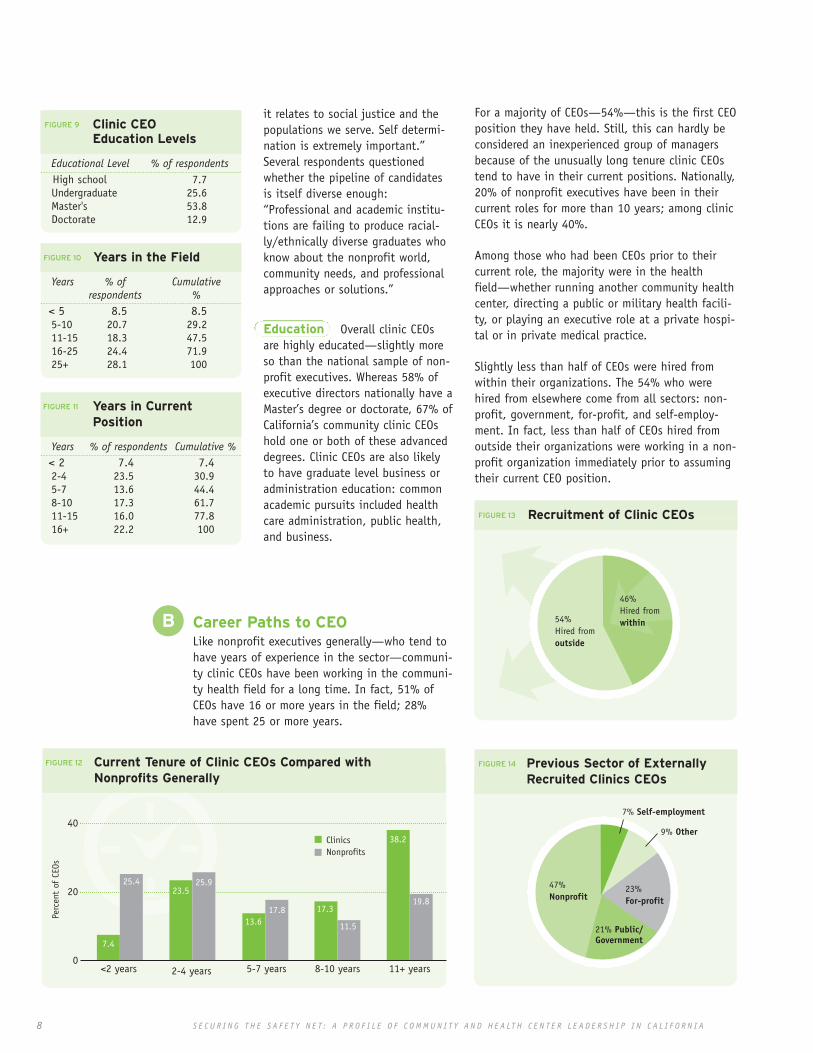
Education Overall clinic CEOsare highly educated—slightly moreso than the national sample of non-profit executives. Whereas 58% ofexecutive directors nationally have aMaster’s degree or doctorate, 67% ofCalifornia’s community clinic CEOshold one or both of these advanceddegrees. Clinic CEOs are also likelyto have graduate level business oradministration education: commonacademic pursuits included healthcare administration, public health,and business.
\
For a majority of CEOs—54%—this is the first CEOposition they have held. Still, this can hardly beconsidered an inexperienced group of managersbecause of the unusually long tenure clinic CEOstend to have in their current positions. Nationally,20% of nonprofit executives have been in theircurrent roles for more than 10 years; among clinicCEOs it is nearly 40%.
Among those who had been CEOs prior to theircurrent role, the majority were in the healthfield—whether running another community healthcenter, directing a public or military health facili-ty, or playing an executive role at a private hospi-tal or in private medical practice.
Slightly less than half of CEOs were hired fromwithin their organizations. The 54% who werehired from elsewhere come from all sectors: non-profit, government, for-profit, and self-employ-ment. In fact, less than half of CEOs hired fromoutside their organizations were working in a non-profit organization immediately prior to assumingtheir current CEO position.
FIGURE 13 Recruitment of Clinic CEOs
FIGURE 14 Previous Sector of Externally Recruited Clinics CEOs
FIGURE 12 Current Tenure of Clinic CEOs Compared with Nonprofits Generally
Career Paths to CEOLike nonprofit executives generally—who tend tohave years of experience in the sector—communi-ty clinic CEOs have been working in the communi-ty health field for a long time. In fact, 51% ofCEOs have 16 or more years in the field; 28%have spent 25 or more years.
B
FIGURE 9 Clinic CEO Education Levels
Educational Level % of respondentsHigh school 7.7Undergraduate 25.6Master's 53.8Doctorate 12.9
FIGURE 10 Years in the Field
Years % of Cumulative respondents %
< 5 8.5 8.55-10 20.7 29.211-15 18.3 47.516-25 24.4 71.925+ 28.1 100
FIGURE 11 Years in Current Position
Years % of respondents Cumulative %< 2 7.4 7.42-4 23.5 30.95-7 13.6 44.48-10 17.3 61.711-15 16.0 77.816+ 22.2 100
40
20
0
ClinicsNonprofits
Perc
ent
of C
EOs
<2 years 2-4 years 5-7 years 8-10 years 11+ years
7.4
25.423.5
25.9
13.617.8 17.3
11.5
38.2
19.8
54%Hired fromoutside
21% Public/Government
23% For-profit
7% Self-employment
9% Other
47% Nonprofit
46%Hired fromwithin

9© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
+$
Overwhelmingly respondents took their currentjobs because of the mission of their organizations.Like nonprofit executives generally, money—in theform of salary or benefits—is not reported as acritical factor. After mission, the CEOs’ own pro-fessional development was the next most impor-tant factor in their decision to take the job.
People working in the community clinic field viewthe mission of their organizations as multi-faceted—inclusive of not only health care deliveryobjectives, but also of advocacy for the servicepopulation of low-income children, families andseniors, as well as health policy and broader socialjustice. Clinic CEOs tended to rate each of thesefactors as important motivators that attractedthem to this work. Rating the aspects of missionon a scale of 1 to 6, with 6 meaning “extremelyattractive,” CEOs appear to be especially motivat-ed by working with the populations that utilizetheir clinics. This was the only aspect of missionthat received no 1, 2, or 3 scores at all; 79%rated “service population” a 6 out of 6.
Salaries
As part of the healthcare industry, the CEOs ofCalifornia’s community clinics and health centersare paid slightly more in each budget categorythan national averages for nonprofit executivessector-wide. Primarily because clinics and healthcenters tend to have larger operating budgets thatother types of nonprofits, the mean3 salary forCalifornia’s clinic executives is $93,339 comparedwith $57,332 for nonprofits generally. Still, CEOsat the smallest clinics and health centers tend tomake much less than the average. There was awide range in salary among CEOs in the small clin-ics cohort—from $25,000 to $130,000, with amean of $64,579.
FIGURE 17 Clinic CEO Salaries
Low $25,000
High $230,000
Median $94,500
5% Trimmed Mean $93,339
Interestingly, the gender disparity across agencysizes that was evident in the national sample ofnonprofit executives is less pronounced amongcommunity health CEOs. That is, there are not
FIGURE 15 Factors in Taking Clinic CEOs Positions
FIGURE 16 Percentage of 1 – 6 Ratings, Aspects of Clinic Mission that Attract CEOs
C
FIGURE 18 Average CEO Salaries by Clinic Budget Size
3 Throughout the report we are using the 5% trimmed mean, which is a mean calculated afterthe top and bottom 5% of scores (outliers) are eliminated
160,00
120,000
80,000
40,000
0
80
60
40
20
0
6
5
4
3
2
1
1
2
3
4
5
6
2.4
Sala
ry
<$1 million
1-2.99 million
3-4.99 million
5-9.99 million
10-99.99 million
20+ million
$58,856
$75,456$82,204
$101,719
$122,222
$140,476
Policy
Prof Devmnt
AgencyMission
KnewStaff/Board
AgencyReput
Salary Benefits
Social Justice Care Delivery Service Population
7.3
13.4
15.9
17.1
43.9
2.5
2.5
9.9
9.9
9.9
19.8
65.4
0.0
0.0
0.0
3.7
17.3
79.0
198
55.6
0.0 1.2
3.7
3.2
3.6
2.62.6
5.8
4.4
10 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
ss
$Job Rewards and Challenges
Given the clear passion for the community healthmission evident in their reasons for taking theirjobs, it is not surprising that CEOs reported beingvery satisfied overall with their work. Rating theirsatisfaction on a scale of 1 to 6, with 6 meaning“extremely satisfied,” respondents gave a remark-ably high mean answer of 5.3 out of 6. Whenasked what they like most about the work, CEOstalked frequently about serving their client popu-lations, about the opportunity to lead and pro-vide vision and inspiration for staff, and thechance to work with others who are equally com-mitted to community health. CEOs also mentionedthe diversity of tasks they take on as a positiveaspect of the work.
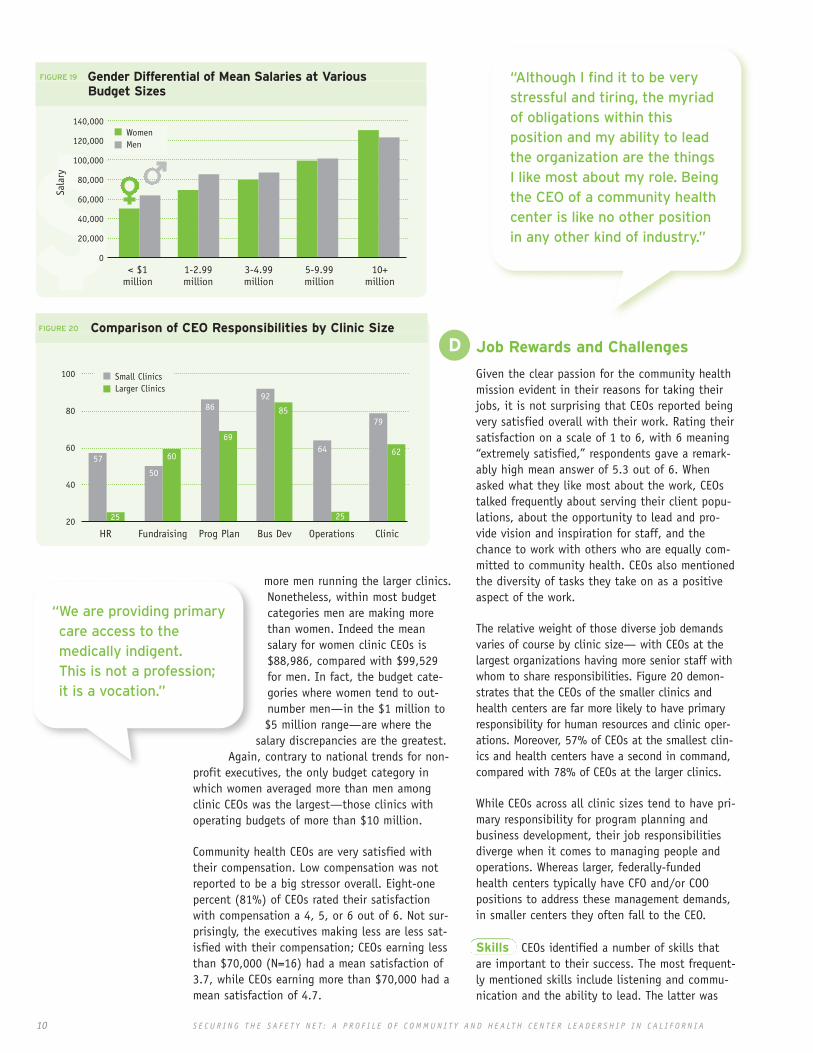
The relative weight of those diverse job demandsvaries of course by clinic size— with CEOs at thelargest organizations having more senior staff withwhom to share responsibilities. Figure 20 demon-strates that the CEOs of the smaller clinics andhealth centers are far more likely to have primaryresponsibility for human resources and clinic oper-ations. Moreover, 57% of CEOs at the smallest clin-ics and health centers have a second in command,compared with 78% of CEOs at the larger clinics.
While CEOs across all clinic sizes tend to have pri-mary responsibility for program planning andbusiness development, their job responsibilitiesdiverge when it comes to managing people andoperations. Whereas larger, federally-fundedhealth centers typically have CFO and/or COOpositions to address these management demands,in smaller centers they often fall to the CEO.
Skills CEOs identified a number of skills thatare important to their success. The most frequent-ly mentioned skills include listening and commu-nication and the ability to lead. The latter was
“Although I find it to be verystressful and tiring, the myriadof obligations within thisposition and my ability to leadthe organization are the thingsI like most about my role. Beingthe CEO of a community healthcenter is like no other positionin any other kind of industry.”
more men running the larger clinics.Nonetheless, within most budgetcategories men are making morethan women. Indeed the meansalary for women clinic CEOs is$88,986, compared with $99,529for men. In fact, the budget cate-gories where women tend to out-number men—in the $1 million to$5 million range—are where the
salary discrepancies are the greatest.Again, contrary to national trends for non-
profit executives, the only budget category inwhich women averaged more than men amongclinic CEOs was the largest—those clinics withoperating budgets of more than $10 million.
Community health CEOs are very satisfied withtheir compensation. Low compensation was notreported to be a big stressor overall. Eight-onepercent (81%) of CEOs rated their satisfactionwith compensation a 4, 5, or 6 out of 6. Not sur-prisingly, the executives making less are less sat-isfied with their compensation; CEOs earning lessthan $70,000 (N=16) had a mean satisfaction of3.7, while CEOs earning more than $70,000 had amean satisfaction of 4.7.
FIGURE 19 Gender Differential of Mean Salaries at Various Budget Sizes
FIGURE 20 Comparison of CEO Responsibilities by Clinic Size
“We are providing primarycare access to themedically indigent.This is not a profession; it is a vocation.”
D100
80
60
40
20
140,000
120,000
100,000
80,000
60,000
40,000
20,000
0< $1
million
Sala
ry
1-2.99million
3-4.99million
5-9.99million
10+million
HR
57
25
Fundraising
50
60
86
69
92
85
64
25
79
62
Prog Plan Bus Dev Operations Clinic
WomenMen
Small ClinicsLarger Clinics
11© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
><variously described as “strategic vision,”“holding the big picture,” and “keeping futuregoals in focus while dealing with day to day chal-lenges.” Many CEOs also referenced their businessand financial skills, which is not unexpectedgiven the funding complexities they deal withregularly and the graduate level business andadministration training that many clinic execu-tives have. Political skills and advocacy —whether in reference to their own staff andboards or to the broader community health land-scape—was mentioned by a number of respon-dents as well. Finally, some respondents refer-enced their own clinical background as importantto their executive effectives; indeed, a smallnumber of CEOs maintain a clinical practice.
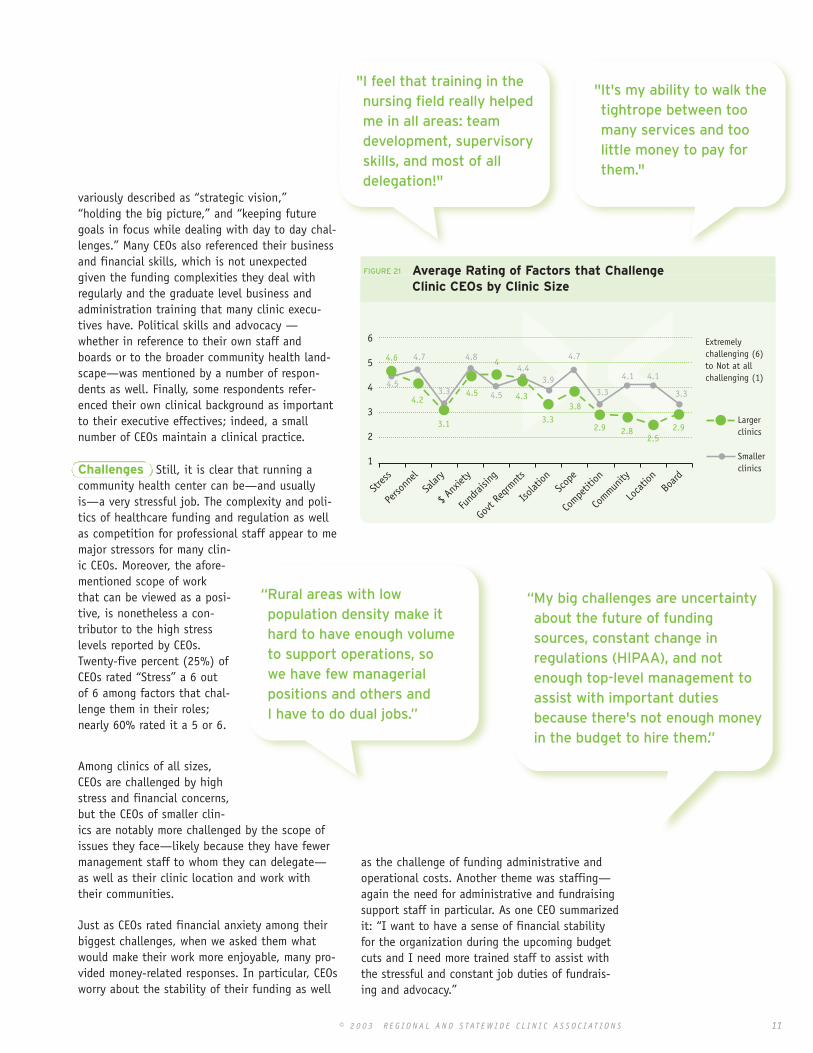
Challenges Still, it is clear that running acommunity health center can be—and usuallyis—a very stressful job. The complexity and poli-tics of healthcare funding and regulation as wellas competition for professional staff appear to memajor stressors for many clin-ic CEOs. Moreover, the afore-mentioned scope of workthat can be viewed as a posi-tive, is nonetheless a con-tributor to the high stresslevels reported by CEOs.Twenty-five percent (25%) ofCEOs rated “Stress” a 6 outof 6 among factors that chal-lenge them in their roles;nearly 60% rated it a 5 or 6.
Among clinics of all sizes,CEOs are challenged by highstress and financial concerns,but the CEOs of smaller clin-ics are notably more challenged by the scope ofissues they face—likely because they have fewermanagement staff to whom they can delegate—as well as their clinic location and work withtheir communities.
Just as CEOs rated financial anxiety among theirbiggest challenges, when we asked them whatwould make their work more enjoyable, many pro-vided money-related responses. In particular, CEOsworry about the stability of their funding as well
"I feel that training in thenursing field really helpedme in all areas: teamdevelopment, supervisoryskills, and most of alldelegation!"
"It's my ability to walk thetightrope between toomany services and toolittle money to pay forthem."
“Rural areas with lowpopulation density make ithard to have enough volumeto support operations, sowe have few managerialpositions and others andI have to do dual jobs.”
FIGURE 21 Average Rating of Factors that Challenge Clinic CEOs by Clinic Size
as the challenge of funding administrative andoperational costs. Another theme was staffing—again the need for administrative and fundraisingsupport staff in particular. As one CEO summarizedit: “I want to have a sense of financial stabilityfor the organization during the upcoming budgetcuts and I need more trained staff to assist withthe stressful and constant job duties of fundrais-ing and advocacy.”
Extremelychallenging (6)to Not at allchallenging (1)
Largerclinics
Smallerclinics
6
5
4
3
2
1
Stres
s
Perso
nnel
Salar
y
$ Anx
iety
Fund
raisin
g
Isolat
ionSc
ope
Compe
tition
Commun
ity
Loca
tion
Board
Govt
Reqrm
nts
4.6
4.2
3.1
4.54.5
4.7
3.3
4.8
4.5
4.44
4.3
3.9
4.7
4.1 4.1
3.3 3.3
3.33.8
2.9 2.92.82.5
“My big challenges are uncertaintyabout the future of fundingsources, constant change inregulations (HIPAA), and notenough top-level management toassist with important dutiesbecause there's not enough moneyin the budget to hire them.”

12 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
FIGURE 24 Predicted Next Jobs for Clinic CEOs
Tenure and Post-ED Career Paths
A primary objective of this research was tounderstand the anticipated career paths ofcurrent clinic leaders. How long can we expectthem to stay in their jobs? Will they stay in thecommunity health field when they leave theircurrent positions? Equally important, what arethey doing to develop and ensure a smoothtransition to their successors?
Given how long many community health CEOshave been in their current roles, it is remarkablethat more than 40% expect to be in their currentjobs for another 6 years or more. And whereasnationally 35% of nonprofit executives anticipat-ed leaving their jobs within the next 2 years, just22% of clinic CEOs have the same expectation.
One inevitable factor in leadership retention isretirement. With the age data showing that 70%of current executives are in their fifties or older,many plan to retire out of their current roles.Indeed when offered a range of potential nextsteps, “retirement” was chosen by 38% ofrespondents, making it the most frequentresponse. Sixty-four percent (64%) of respondentsin their 60s or older plan to retire out of theircurrent positions. Still, 60% of this older cohortplans to be in their current job for at leastanother 3 to 5 years.
Next Jobs Where will the CEOs who aren’tplanning to retire go next in their careers? Figure24 demonstrates that similar to nonprofit execu-tives generally, clinics leaders are not likely torun a clinic again. Instead, they have interest inphilanthropy, consulting, or other personal goalssuch as returning to school or private practice(captured in “Other” in Figure 23).
FIGURE 22 Anticipated Length of Stay in Current CEO Position
E
“In small clinics, there's not anobvious feeder role for the CEOposition. We just recently addedthe COO role here and we are a$5.5 million clinic. I am leavingand we have gone outside foran Interim and will for the newCEO as well.”
> 5 years
3-5 years
1-2 years
<1 year
41%
37%
15%
7%
FIGURE 23 Next Career Move for for Clinic CEOs
52%Identifiedpotentialsuccessor
48%Have notidentifiedpotentialsuccessor
8% Nonprofit clinic
4% Nonprofit (non-clinic)
6% Govt
3% For-profit
9% Philanthropy
16%Consulting
16%Other
FIGURE 24 CEO Identification of Potential Successors
38%Retiring

13© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
Roughly half of current CEOs have identified oneor more people with the potential to take theirjob when they leave or retire. Among these, mostare looking to internal staff; 82% of these poten-tial successors are within the organization. ChiefFinancial Officers, Chief Operating Officers, MedicalDirectors, and Deputy Directors (or the equivalentto these titles) were the most frequently identi-fied probable successors.
However, a critical finding of this research is atendency for ambivalence among communityhealth leaders about succession planning general-ly—and in some cases about the next wave ofleaders specifically. The fact that many currentexecutives played founding roles in the communi-ty health movement no doubt contributes to thisambivalence. As one outgoing CEO said, “There’sonly one generation of pioneers.”
Study participants readily acknowledged the“graying of the sector,” but few had specificstrategies in mind for their own successfultransition. There is the sense in listening to manyclinic CEOs talk that this field—as opposed to anyone CEO—has a kind of collective “founder’ssyndrome.” When used to describe an individual,“founder’s syndrome” refers to such deepownership of an organization that it is difficultfor her/him to imagine anyone else ever takingover adequately. Not necessarily arrogance, thismind-set has more to do with a lack of boundarybetween the leader’s personal investment and theorganization’s viability in its own right. In this
case, the very long tenure of most CEOs—alongwith founders’ attachment to the communityhealth center movement they helped to build—iscertainly a key factor. For example, one executiveagreed that succession planning is important butwondered how to do it given the fact that manyon his staff and board have been involved withthe organization for 20+ years. There simply isn’tthe institutional knowledge or memory of whatleadership transition looks like in cases like his.Moreover the emerging recognition in thenonprofit sector that succession planning isinclusive of a number of skills beyond choosingan ideal successor when one is ready to resign—from cultivating leaders, to sharing knowledgeand key organizational relationships, to insistingon a sustainable workload for senior staff and theCEO—is not yet widely evident in the way clinicleaders talk about succession. While thesetrends were not ubiquitous, their prevalence wasnoteworthy and has implications for successfuland proactive transition planning.
A related issue is the percep-tion by today’s clinic execu-tives of the next wave ofleadership. A number of par-ticipants referenced how dif-ferently the next generationviews the work. In additionto not having been part ofthe founding movement, thenext generation wants a bal-anced life—something thatwas not part of the equationfor most founders. Somerespondents questioned theyounger generation’s depthof commitment to the com-munity health center mis-sion. Others acknowledgedthat older clinic leadershipat times has difficulty relat-ing to the young staff whoare potential successors.
“I have a strategic plan formy organization, but notfor myself. PersonallyI don't believe insuccession planning.”
What this data suggests is that the field of com-munity health can expect just 8% of the currentcohort of executives to be available for future CEOopenings. Thus many of the future CEO positionopenings will likely be filled by current membersof senior clinic staff. This begs the question ofwhether CEOs are actively cultivating these poten-tial future leaders.
“Our generation's concernabout the next cohort ofclinic leaders may beabout the social justiceaspect of the work. Dothe incoming interns havethe burning righteousindignation to sustainthem through thechallenges they'll face?”

14 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
death in my immediate family, not one Boardmember sent me a message of condolence.” Butthe majority of CEOs described their boards assources of personal support—many alluding tostrong relationships whose boundaries and roledefinitions have become clearer over time. Manyalso used emotional terms to describe the rela-tionship: “trusting,” “respectful,” “compassion-ate,” and “a shoulder to cry on.” Frequently, CEOsattributed the success of their board relationshipto the board’s willingness to let them run theorganization on a day-to-day basis: “They do notmicromanage, but advise wisely and keep direc-tion of mission and policy.”
An important factor in community health CEO-Board relations is the federal funding requirementfor consumer board participation. As in otherparts of the nonprofit sector, CEOs who are man-aging up to consumer boards have to address avariety of board training and communicationissues. Executives in the midst of transitioningtheir boards from traditional nonprofit composi-
“My board members have accepted the needto develop into a more functioninggoverning body of a nonprofit agency, andtheir development process is very conduciveto my own development as the CEO.
FIGURE 25 Perceived Effectiveness of CEO/Board Partnership by Clinic Size
Boards of Directors
Like nonprofit executives generally, clinic CEOstell a somewhat mixed story about the success oftheir board/staff partnership. When asked to ratehow effectively their boards team up with them in5 key areas (see figure 25 below), CEOs gave fairlyhigh ratings to everything except fundraising.CEOs viewed board members as most effective part-ners in advocating for the organization’s mission.
However, the CEOs of larger organizations per-ceive their boards to be more effective than doCEOs in smaller clinics and health centers. In thekey governance areas of strategic planning andfinance for instance, the cohort of CEOs fromsmaller clinics rated board effectiveness a fullpoint lower or more than their colleagues fromlarger clinics and health centers.
A minority of CEOs complained about boards thatoffer little or no professional guidance, engagetoo much in the minutia of clinic management,and/or are not a source of personal support orinspiration. In a powerful reminder that CEOsneed more than oversight from their bosses, onerespondent noted: “When I had an unexpected
F
From VeryEffective (6)to Not at allEffective (1)
Largerclinics
Smallerclinics
6
5
4
3
2
1
Community PR Fundraising Strateiccplanning
Finances Missionadvocacy
3.83.4
3.33.5
4.3
4.2
3.0
4.2 4.54.7
“We have just instituted a consumermajority [on our board]. We haven'tdone all the training we want to doyet, but I am already seeing theirtendency to want to get involved inclinic operations. We are going touse an Advisory Council structureas a place for consumers to gothrough first and learn.”

15© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
From VeryImportant (6)to NotImportant (1)
6
5
4
3
2
1
4.54.6
4.4
2.9
4.0
5.0
4.3
Prof p
eers
Prof A
ssns
Mgmnt
cours
es
Worksh
p & co
nf
Netw
orks
CPCA RC
C
tion to the consumer representation face a peri-od of mutual adjustment that can be an addi-tional stressor for the CEO. One CEO noted,“Finding board members who meet the require-ments of funding sources (like being representa-tive of our patient populations) while bringingexpertise to the board, is very challenging.”
Finally, the same issue of long tenure andfounder orientation seen among CEOs appears tobe present on many clinic and health centerboards. A number of survey respondents pointedto the many years of service of their currentboard members as a factor in their deeprelationship. Though the survey did not addressthe issue directly, one is left with theimpression that some clinics—presumably thosenot required to comply with federal Section 330mandated governance rules—are not making useof board term limits as a means of infusingtheir organizations with new expertise or vision.As one focus group member commented abouther clinic: “The organization had outgrown theboard and is now reconfiguring itself. And it’svery difficult!”
Sources of Training & Support
We asked CEOs to rate the importance to themin their CEO role of a variety of sources of bothsupport and training. As Figures 26 and 27below demonstrate, CEOs use both informal andformal networks to learn and sustainthemselves—with their senior staff and fellowCEOs being particularly crucial. Formal sourcesCPCA and RCC had slightly higher ratings asproviders of training than of support.
Several respondents noted specifically the lackof clinic executive training available. The ideaof a targeted executive academy of some sortwas discussed by members of one of the focusgroups. Another survey respondent lamented:“One of my challenges is not having formaltraining on how to be an effective CEO.Although some of the learning can only happenon the job, the balance of formal trainingversus on-the-job training is off, which createsan environment for unnecessary mistakes andre-inventing of the wheel.” Arguing for learningfrom peers who’ve had success, one CEOconcluded provocatively: “A business/medicaleducation is vastly overrated as qualification forexecutives and sometimes gets in the way ofseeing the big picture.”
FIGURE 27 Current Sources of TRAINING for Clinic CEOs
“The board was part of thefree clinic model; theywanted the hippie days.They didn't have a grasp ofwhere the organization hadgone, although they hadapproved every new contractthat came along.“
G
FIGURE 26 Current Sources of SUPPORT for Clinic CEOs
From VeryImportant (6)to NotImportant (1)
6
5
4
3
2
1
4.3
4.13.8
4.44.64.6
5.5
1.8
3.4
Mgmnt
team
Spon
sor/p
artne
r
Peer
netw
ork
Mento
ring
Exec
coac
hing
Board
Netw
orks
CPCA RC
C

16 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
Though not the primary focus of this research, theclinic-governed consortia and associations4 acrossthe state are a crucial element of the safety-net—advocating regionally and statewide for patientsand services, fighting for adequate clinic funding,and offering support and training to health centerstaff and executives. Thus the CEOs of the state’s21 such associations were also part of our study’starget; 15 responded to the web-based survey.A condensed summary of findings follows.
The personal characteristics of consortia CEOs aresimilar to those of clinic leadership though themembers of this cohort are less likely to be intheir 60s. Eighty-three percent (83%) are womenand 61% are in their 50s. Seventy-eight percent(78%) are white—with one CEO identifying ineach of these race/ethnicity categories: AfricanAmerican, Asian/Pacific Islander, Latino, andOther. Most consortia CEOs—61%—have a Master’sdegree, but none reported having a doctorate.
Like clinic CEOs, association executives haveworked in the community health field for manyyears—more than 50% for 16 years or more. Two-thirds have been CEOs before, all but one in pub-lic or nonprofit health settings. Forty percent(40%) of association CEOs ascended to the posi-tion from within the organization from among thepositions of CFO, board member, policy staff, andconsultant. Nearly three-quarters of associationexecutives have been in their current position for5 or more years.
FIGURE 29 Years in Current Position
Years % of respondents Cumulative %< 2 13.3 13.32-4 13.3 26.75-7 33.4 60.08-10 20.0 80.011+ 20.0 100.0
Consortia executives have very similar motivationsin taking their roles as clinic CEOs—emphasizingmission and professional development over salaryand benefits. They are equally similar in identify-ing health center patient populations as the mostcompelling aspect of the mission.
Association executive salaries range from $45,000to $164,000 with a mean of $100,941. Respon-dents are quite satisfied with their compensation;87% rated their satisfaction as a 5 or 6 on a six-point scale. They are equally satisfied with theirwork; 87% rated their overall satisfaction withtheir jobs as a 5 or 6 on a six-point scale. Indescribing why they like their work, associationexecutives talk about impacting a system of careand successful advocacy on behalf of member clin-ics. Among the skills they identify as responsiblefor their success: communication, vision and lead-ership, and political savvy.
Consortia executives report being as stressed astheir clinic peers; 67% rated stress a 5 or 6 out of6. Asked to rate a list of potential stressors, theyexpress slightly less concern about agencyfinances and slightly more about their boards ofdirectors than clinic executives do.
Consortia/Association CEO Findings
VI
“One of my most importantskills is political instinct:I am responsible for healthpolicy advocacy in a veryconservative region.”
4 A variety of names for clinic membership groups are used throughout the state including: consortia, associations, councils, networks, and part-nerships. We refer to these as consortia and/or associations throughout the report. Please see Appendix B for a list of participants.
FIGURE 28 Age of Consortia/Association CEOs
61%50-59years old
28%40-49years old
11%<40years old

17© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
54%3-5 years
33%5+ years
13%1-2 years
Surveys and interviews with both associationexecutives and health center CEOs suggest that achallenge facing this health care system is theengagement and functioning of associationboards of directors. While this is not new infor-mation, the opportunity for executives to speakanonymously yielded honest feedback about theinherent challenges of collaboration as well asthe member clinic-association CEO dynamic.Among the issues raised: competition amongboard members, lack of engagement by boardmembers, and the potential for power strugglebetween association CEOs and board members.As one association CEO explained, “Members havea strong conflict of interest. We are now lookingat governance issues and hope that the board canbe restructured to address these conflicts.”Another challenge identified is the mixture ofsmall and large clinics in any one association,which can lead to conflict over priorities andperceptions of disrespect.
The majority of association executives expect tobe in their current jobs for 3-5 more years, while33% expect to stay for 6 or more years. Nonereported that she/he would be leaving withinone year.
FIGURE 30 Average Rating of Factors that Challenge Association CEOs
“What I like most is movingthe clinic system forward-implementing new collaborativeand integrated services thatimprove care, decrease costs,and improve the financialperformance of health centers.”
“It’s kind of hard for the ED of a consortium toanswer to the EDs of its member clinics. Thestructure can be awkward. As board membersour roles get confused. Advocating for ourown agencies, especially in the case of fundsto be distributed through the consortium, canbe an uncomfortable conversation.”
“It is challenging to build consensus andmaintain a level of fairness among colleagueswho are operating from different frames ofreference, such as very large clinics who havea different set of needs and priorities than wewho are still struggling to survive.”
FIGURE 31 Years Executives Expect to Stayin Current Position
Extremelychallenging (6)to Not at allchallenging (1)
5
4
3
2
1
4.5
2.9
1.8
44.2
3.7
3 32.7 2.6 2.6
3.6
Stres
s
Perso
nnel
Salar
y
$ Anx
iety
Fund
raisin
g
Isolat
ionSc
ope
Compe
tition
Commun
ity
Loca
tion
Board
Govt
Reqrm
nts

18 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
The findings suggest a number of
potential responses for key stakehold-
ers in California’s community health
center network. With guidance from our
Advisory Committee, we propose the
following next steps for clinic CEOs,
clinic boards of directors, associations
and consortia, and funders.
RECOMMENDATIONS FOR
Clinic CEOs
Recognize succession planningas a necessary aspect oforganizational leadership.
The findings of this researchconfirm what manysuspected about the agingof the community healthcenter leadership cadre.But more importantly theyalso surface a lack ofplanning for thatimpending turnover. Whilesuccession planning isalso the responsibility ofa board of directors (seesubsequent Calls to Actiontargeted to boards), aportion of theresponsibility falls toincumbent executives.
Proactive consideration ofcareer goals and their timing, promoting thereadiness of the organization and its managers tofunction well in their absence, and regulardialogue with the board of directors on thesubject of succession are all appropriate ongoingsteps for CEOs regardless of their age. The key isto move beyond thinking of succession planningas something one undertakes once she hasdecided to retire; instead recognize it as anapproach to leadership that is ongoing. Workingfrom the perspective that the organization will berun by a number of successors over time gives a
new level of priority to developing leaders withinand outside of the clinic, to insisting oncompetitive compensation and a sustainableworkload for the CEO and other managers—inshort, creating a job that somebody else wouldwant and at which somebody would have areasonable chance for success.
Develop future leaders.
Another component of effective organizationalleadership is active development of potential suc-cessors—whether for one’s own job or for futureleadership needs of the field. Given that most cur-rent clinic CEOs do not expect to take another clin-ic CEO position, it’s today’s medical directors,COOs, and other senior management team membersthat will likely be the next class of clinic leader-ship. It’s critical that CEOs identify and intention-ally provide these staff with professional develop-ment opportunities, access to key organizationalrelationships, and encouragement to consider along-term management track. This is not to sug-gest that one person on staff should be obviouslysingled out, but instead that CEOs should inten-tionally build the capacity of their managementteams.5 Being mindful of developing leaders ofcolor also appears warranted; respondents notedthe under-representation of African American lead-ers in community clinic leadership and the overalltendency for health center CEOs to be white.
Model a sustainable approachto leadership.
Some CEOs expressed ambivalence about the nextgeneration of clinic leadership—questioningwhether they had the commitment and drive thatthe founding cohort displayed. While a lack of com-mitment is damaging to any organization, so too isextremely high stress, crisis-oriented management.By maintaining their own work/life balance, CEOsnot only provide better leadership, they alsodemonstrate to potential successors that the job isdo-able. On the other hand, executives that demandthat the next generation of managers work like theythemselves worked in the early days of the clinic
Calls to Action
VII
5 “?eparting? Arriving?Surviving and Thriving:Lessons for Executives.”Adams, Tom. The NonprofitQuarterly, Volume 9, Issue4, page 7.
A
“Your investment inconsciously andcontinuously groomingnew leadership ensuresthere is a diverse pool ofpotential executives readyto serve your community.”
Tom AdamsAnnie E. Casey Executive Leadership and Transition and Capacity Building Project

19© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
movement, are in danger of pushing talent out ofthe pool just as it’s most needed. Long-term CEOscan consider a paid sabbatical program to allow forrejuvenation as well as professional developmentfor the management team in the CEOs absence.
RECOMMENDATIONS TO
Clinic Boards of Directors
Recognize succession planningas a fundamental aspect oforganizational governance.
One of the primary responsibilities of aboard of directors is to hire, evaluate theperformance of, and replace when necessarythe organization’s chief executive. While inpractice nonprofit organizations vary widely in thestrength and assertiveness of their boards, thedegree of retirement and other kinds of turnoverthat clinic boards face in the coming yearsmandates that they become versed in the basictenets of succession planning. The board ofdirectors is the agent during succession: if asearch firm is hired, the board is the client; if aninterim executive is needed during a prolongedsearch, the board must find him or her, and so on.Moreover, the board must know enough about theexecutive job to determine the best successor. It’sthe board executive committee’s responsibility tobe in regular dialogue—typically during annualperformance evaluation—with the CEO about hercareer plans and the degree to which she isdeveloping future leaders.
Take responsibility for boardeducation and development.
Recognizing that a high functioning board willlower the stress level of the CEO, board leadershipshould identify where theirs boards needs skills-building and secure appropriate training. If boardmembers are uncomfortable asking for money,they make seek a development training; if mostcannot read health center financial statements,they can ask the center’s CPA to do an annualcustom training for the board. For new boardmembers and/or consumer board members, this is
Bespecially important. Making the transition from aprevious relationship to the organization—andrespecting the boundaries between managementand governance—are essential to strong gover-nance and an effective board-CEO relationship.
RECOMMENDATIONS TO
Associations and Consortia
Build awareness among membersabout the emerging field ofexecutive leadership services.
Clinic CEOs need exposure to the emerging fieldof executive leadership services. There is a grow-ing realization in the nonprofit sector that payingattention to leadership is critical to the sustain-ability of organizations. Given this report’s find-ings on the age of community health CEOs as wellas how unlikely current CEOs are to take anotherexecutive position, it’s critical that the field learnthe concepts and begin to promote the value ofintentional executive transition planning. Throughmembership meetings and conferences, associa-tions can introduce this thinking and serve aschannels of information about services availableto CEOs locally and regionally.
Consider board and organizationalstructure changes to mitigatecompetition and conflict amongmembers.
It appears that some associations are strugglingto make their founding governance structures andsystems continue to work despite the changingneeds of member clinics. Participants in this studyraised issues of conflicts of interest, discordbetween member clinics of various sizes, and thechallenge of the association executive-clinic exec-utive relationship. What each association may
C
“Nothing has greater impact onthe outcome than a board'sleadership skills in exploiting themoment of leadership turnoverfor its myriad opportunities.”
Tim WolfredDirector, Executive Transitions, CompassPoint

20 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
need to consider now is a strategic planningprocess that addresses the question, “What are thecurrent goals of our affiliation?” And from this,“Which governance and organizational structureswill best meet the member clinic needs?” Part ofthis strategic thinking should be consideration ofwhat role the associations are best suited to play:service organizations or trade associations?
RECOMMENDATIONS TO
Funders
Fund realistic infrastructure costs.
Much of the financial anxiety described by partici-pants in this study stems from the full costs of
their services not beingpaid— whether by gov-ernmental or non-gov-ernmental sources.Moreover, CEOs facechanging funding priori-ties and budget cuts tiedto the current adminis-tration and the fledglingeconomy. When askedwhat would make theirwork more enjoyable,many CEOs talked aboutinfrastructure: facilities,technology, supportstaff, and operations. Asone frustrated CEO putit: “We need to educate
all the organizations wedeal with that there is an administrative cost toeverything we do. No one wants to pay foradministration!” While infrastructure costs mayseem less appealing to funders seeking demon-strable patient impact, in fact sufficient infra-structure is essential to organizational effective-ness as well as retention of high-performing staff.Some respondents in this study talked about dou-bling up administrative roles in one person orgoing without key positions, which are clearpaths to eventual staff burnout and/or lowerquality work.
Fund executive access toleadership services.
Philanthropy is beginning to recognize the valueof investing in executives—both as a means ofimproving organizational performance and ofsector retention of our most experienced talentpool. In California, the leadership of TheCalifornia Wellness Foundation and the DurfeeFoundation (Los Angeles) in establishing paidexecutive sabbatical programs is a prime example.Launched this year, the Wellness Foundation’ssabbatical program6—which is targeted tononprofit health executives throughoutCalifornia—had 91 applicants for 6 awards!Clearly there is ample room for additionalphilanthropy-sponsored sabbatical programs.
Less expensive but highly impactful is executivecoaching. Long established in the for-profit sec-tor, coaching is beginning to take hold as animportant tool for executive burnout preventionand leadership skills development in the nonprofitsector. A recent evaluation by Harder+Company ofthe Executive Coaching Project7 in the SanFrancisco Bay Area concluded, “EDs reported sta-tistically significant improvement in the clarity oftheir vision for the organization, as well as staffand Board alignment with the mission.” Coachingalso had positive impacts on executives’ levels ofconfidence and ability to balance the demands oftheir personal and professional lives. The stresslevels indicated by this research suggest thatcoaching could be of enormous use in the com-munity clinic field.
Especially important is providing support to long-time executives who are approaching transition—aswell as the boards of directors who will have toidentify their successors. The arena of executivesuccession planning has developed rapidly over thelast 5 years and now includes training for execu-tives who are contemplating resignation/retirement,interim executive placement, consulting to theboard during transition, and executive placementservices. Financially strapped clinics may not havethe resources to direct to this effort, so the leader-ship of philanthropy in encouraging and fundingthis work is crucial.
6 This program is adminis-tered by CompassPointNonprofit Services.
7 This was a joint projectof CompassPoint, MarinNexus, and ResourceCenter for Nonprofits atthe Volunteer CenterSonoma County.
D
“A big stressor is the changes inclinic financing. In the old days,if you added a $100,000 doctorto your staff in order to expand,those new costs would becovered. Not anymore. Whilethat doctor is getting up tospeed, the clinic has to coverthose costs in some other way.Medi-cal doesn't pay forexpansion any longer.”
21© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
ConclusionThe heroism of clinic, health center, and association leadership is evi-dent throughout these findings. Their passionate commitment to themillions of uninsured and under-insured residents of California is whatinspires them to work long hours, struggle to find adequate funding,and advocate politically for those with little power in Sacramento orWashington D.C. The system of hundreds of clinics and health centersacross the state that this cohort of founding leaders has built is aremarkable model that is even more critical today than it was 30 yearsago. The regional and statewide associations commissioned this reportto inspire dialogue about how best to ensure its future.
One way to do this is to is to invest in clinic, health center, and associ-ation leadership. These CEOs and board members are faced with toughdecisions and arduous political battles on behalf of their patients. Thisreport’s findings suggest that the next several years are the right timefor the clinic and health centers across California to focus on develop-ing the next class of leaders, building the savvy of the boards that willguide them, and strengthening the networks that leverage their individ-ual strengths into regional and statewide forces protecting California’shealthcare safety net.

22 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
California Community ClinicsExecutive Director/CEO Leadership Survey
PLEASE TELL US ABOUT YOUR CAREER PATH
1) How many total years have you worked in community clinics (in anycapacity)?
a. Less than 5 years b. 5 - 10 years c. 11 - 15 years d. 16 - 25 years e. More than 25 years
2) For how many years have you been in your current ExecutiveDirector/CEO position?
#______Years
3) Have you previously held an Executive/CEO position?a. Yes b. No
4) If YES, Please list number of years and field of service for each posi-tion
a. As a Nonprofit ED (e.g. human service)b. As a Government Executive (e.g. public health)c. As a For-profit Executive (e.g. for-profit hospital)
5) Were you working or volunteering at your current agency before youbecame the Executive Director/CEO?
a. Yes b. No
6) If YES, for how long?#______Years
7) If YES, what was your role in your current agency immediately prior tobecoming Executive Director/CEO?
a. Associate Director d. Director of Finance/Administration b. Development Director e. Board Member c. Medical Director f. Other (please specify)
If you selected other please specify:___________________
8) If NO, in which sector were you working immediately prior tobecoming Executive Director/CEO?
a. Nonprofit b. Public/Government c. For profit d. Self-employed e. Other (please specify)
If you selected other please specify:____________________
9) On a scale of 1 - 6, how important were each of the following factorsin your decision to take your current job as Executive Director/CEO?
My professional development Not At All - 1 2 3 4 5 6 - Very MuchThe organization’s mission Not At All - 1 2 3 4 5 6 - Very MuchThe salary Not At All - 1 2 3 4 5 6 - Very MuchThe benefits (e.g. healthcare, retirement plan, etc) Not At All - 1 2 3 4 5 6 - Very MuchStaff and/or board members I knew at the agency Not At All - 1 2 3 4 5 6 - Very MuchThe perceived financial and/or programmatic strength of the agencyNot At All - 1 2 3 4 5 6 - Very Much
10) On a scale of 1 - 6, how much did each of the following aspects of acommunity clinic’s mission attract you to your current job as ExecutiveDirector/CEO?
The public policy and advocacy aspect of the mission Not At All - 1 2 3 4 5 6 - Very MuchThe social justice aspect of the mission Not At All - 1 2 3 4 5 6 - Very MuchThe health care delivery aspect of the mission Not At All - 1 2 3 4 5 6 - Very MuchThe service to under-served populations aspect of the mission Not At All - 1 2 3 4 5 6 - Very Much
PLEASE TELL US ABOUT YOUR CURRENT EXECUTIVE DIRECTOR/CEO POSITION
11) What is your current annual salary (excluding benefits and other non-monetary compensation)?
$_________________
12) On a scale of 1 - 6, how satisfied are you with your total compensa-tion package?
1 - Not Satisfied 2 3 4 5 6 – Very Satisfied
13) On a scale of 1 - 6, how satisfied are you overall with your currentjob as Executive Director/CEO?
1 - Not Satisfied 2 3 4 5 6 – Very Satisfied
14) Which three (3) of your skills are most responsible for your successas Executive Director/CEO?
Skill 1______________________________________________________________Skill 2______________________________________________________________Skill 3_____________________________________________________________
15) How much longer do you imagine that you’ll stay in your current posi-tion as Executive Director/CEO?
a. Less than 1 yearb. 1 - 2 years c. 3 - 5 years d. More than 5 years
16) What do you like most about your job as Medical Director/CEO?
17) To what degree are these factors challenging to you in your role?High stress Not A Challenge – 1 2 3 4 5 6 - Very ChallengingPersonnel Issues Not A Challenge –1 2 3 4 5 6 - Very ChallengingLow compensation Not A Challenge –1 2 3 4 5 6 - Very ChallengingAnxiety about agency’s finances Not A Challenge –1 2 3 4 5 6 - Very ChallengingFundraising Not A Challenge –1 2 3 4 5 6 - Very ChallengingDealing with government funding and/or program requirements Not A Challenge –1 2 3 4 5 6 - Very Challenging“Feeling “”lonely at the top””/isolation “
APPENDIX A
Survey Instrument

23© 2 0 0 3 R E G I O N A L A N D S TAT E W I D E C L I N I C A S S O C I AT I O N S
Not A Challenge –1 2 3 4 5 6 - Very ChallengingScope and variety of issues and responsibilities Not A Challenge –1 2 3 4 5 6 - Very ChallengingDealing with real or perceived competition Not A Challenge –1 2 3 4 5 6 - Very ChallengingWorking with the community Not A Challenge –1 2 3 4 5 6 - Very ChallengingClinic(s) geographic location Not A Challenge –1 2 3 4 5 6 - Very ChallengingRelationship with board Not A Challenge –1 2 3 4 5 6 - Very Challenging
18) Please list any other factors that are very challenging to you inyour role:
19) Have you identified one or more persons with the potential to bethe future Executive Director/CEO of your organization?
a. Yes b. No
20) If YES, what is/are their title(s) or position(s)?
21) If YES, are they internal or external to your organization?a. Internal b. External
22) What are you most likely to do upon leaving your current position?a. Retire b. A for-profit position c. Another non-profit clinic d. A philanthropy position e. Another non-profit (non-clinic) f. Consulting g. A government position h. Other (please specify) i. If you selected other please specify:
23) What one or two things would make your work more enjoyable?
PLEASE TELL US ABOUT YOUR NONPROFIT ORGANIZATION
24) Your clinic or consortium/association name?
25) City of your organization’s main office/site?
26) If you are a community clinic (not a consortium or association)which of the following describe the service area(s) of your organization.
a. Urban b. Sub-urban c. Rural d. Frontier e. Some combination of the abovef. NA - we are not a community clinic g. Other (please specify)
If you selected other please specify:
27) If you are a consortium or association (not a community clinic)which of the following describes your geographic scope.
a. Regional b. State-wide c. NA - we are not a consortium or association d. Other (please specify)
If you selected other please specify:
28) In what year was your organization founded?
29) How many paid full-time and part-time staff does your organiza-tion employ?
30) What is the annual operating budget of your organization?a. Less than $500,000 e. $5 million - $9,999,999b. $500,000 - $999,999 f. $10 million - $19,999,999c. $1 million - $2,999,999 g. $20,000,000 or mored. $3 million - $4,999,999
31) If your organization serves clients directly, what number of undu-plicated patients does your clinic serve in one year?
a. Less than 5,000 e. 50,000 - 99,999b. 5,000 - 9,999 f. 100,000 - 199,999c. 10,000 - 29,999 g. 200,000 or mored. 30,000 - 49,999 h. NA, We Don’t Serve Clients Directly
32) For each of these executive functions check the proper column tomean that you are primarily responsible for it OR that others on yourstaff have primary responsibility.
a. Human resources management: __My Responsibility __Others Responsibilityb. Fundraising: __My Responsibility __Others Responsibilityc. Program planning:__My Responsibility __Others Responsibilityd. Business development: __My Responsibility __Others Responsibilitye. Operations:__My Responsibility __Others Responsibilityf. Clinic leadership: __My Responsibility __Others Responsibility
33) Do you have a Management Team?a. Yes b. No
34) If YES, please list the management team’s titles:
35) If YES, how frequently do you meet with your entire managementteam?
a. Weekly b. Monthly c. Quarterly d. Semi-annually e. Annually
36) If YES, is the management team authorized to make decisions inyour absence?
a. Yes b. No
APPENDIX A
Survey Instrument (continued)
24 S E C U R I N G T H E S A F E T Y N E T : A P R O F I L E O F C O M M U N I T Y A N D H E A LT H C E N T E R L E A D E R S H I P I N C A L I F O R N I A
37) Do you have a 2nd in Command?a. Yes b. No
38) If YES, what is the 2nd in Command’s title?
PLEASE TELL US ABOUT YOUR TRAINING AND SUPPORT NETWORK
39) On a scale of 1 - 6, how important is each of these sources of train-ing to you in your ongoing development as an Executive Director/CEO?
Professional peers Not Important At All – 1 2 3 4 5 6 - Very ImportantProfessional associations Not Important At All – 1 2 3 4 5 6 - Very ImportantCollege-based management course work Not Important At All – 1 2 3 4 5 6 - Very ImportantTopical workshops and conferences Not Important At All – 1 2 3 4 5 6 - Very ImportantNetworks, such as: “National Association of Community Health Centers “Not Important At All – 1 2 3 4 5 6 - Very ImportantCalifornia Primary Care Association Not Important At All – 1 2 3 4 5 6 - Very ImportantRegional Clinic Consortium Not Important At All – 1 2 3 4 5 6 - Very Important
40) On a scale of 1 - 6, how important is each of these sources of supportto you in your ongoing development as an Executive Director/CEO?
My management team/staff Not Important At All – 1 2 3 4 5 6 - Very ImportantMy spouse/partner Not Important At All – 1 2 3 4 5 6 - Very Important Clinic peers Not Important At All – 1 2 3 4 5 6 - Very ImportantMy mentor(s) Not Important At All – 1 2 3 4 5 6 - Very ImportantMy executive coach Not Important At All – 1 2 3 4 5 6 - Very ImportantMy board members Not Important At All – 1 2 3 4 5 6 - Very ImportantNetworks, such as: “National Association of Community Health Centers “Not Important At All – 1 2 3 4 5 6 - Very ImportantCalifornia Primary Care Association Not Important At All – 1 2 3 4 5 6 - Very ImportantRegional Clinic ConsortiumNot Important At All – 1 2 3 4 5 6 - Very Important
41) List any other sources of training and/or support to you:
42) On a scale of 1 - 6, how effectively does your Board of Directorsteam up with you in the following areas?
Community/public relations Not At All – 1 2 3 4 5 6 - Very MuchFundraising Not At All – 1 2 3 4 5 6 - Very MuchStrategic planning Not At All – 1 2 3 4 5 6 - Very MuchFinancial oversight and budgeting Not At All – 1 2 3 4 5 6 - Very MuchAdvocacy for the agency’s mission Not At All – 1 2 3 4 5 6 - Very Much
43) In what ways is your Board of Directors a source of personal sup-port to you as Executive Director/CEO, if at all?
44) What are your thoughts on issues of diversity (race, gender,class, sexual orientation, etc) among community clinic executiveleadership?
PLEASE TELL US ABOUT YOURSELF
45) What is your age?
46) What is your gender?a. Male b. Female c. Transgender d. Other
47) What is your race/ethnicity?a. African American b. Asian/Pacific Islander c. Latino/a d. Middle Eastern e. Native American f. White/Anglo g. Other (please specify)
48) What is your sexual orientation? (optional)a. Heterosexual b. Gay/Lesbian c. Bisexual d. Other
49) What is the highest level of formal education that you have com-pleted?
a. High school b. Undergraduate c. Master’s
50) What was your degree in?
THANK YOU VERY MUCH FOR YOUR TIME!
APPENDIX A
Survey Instrument (continued)

South of Market Health CenterSt. Anthony Free Medical ClinicSt. John’s Well Child and Family CenterThe Children’s Clinic Serving Children and Their FamiliesThe EffortTiburcio Vasquez Health Center, Inc.Tri-City Health CenterTulare Community Health ClinicValley Community ClinicVenice Family ClinicVista Community ClinicWarner Mt. Indian HealthWest County Health CentersWestern Sierra Medical ClinicWestside Family Health CenterWomen’s Community Clinic
Consortia and AssociationsRedwood Community Health CoalitionSan Francisco Community Clinic ConsortiumCalifornia Family Health CouncilShasta Consortium of Community Health CentersCouncil of Community ClinicsCentral Valley Health NetworkCoalition of Orange County Community ClinicsCommunity Clinic Consortium of Contra CostaAlameda Health ConsortiumNorthern Sierra Rural Health NetworkCommunity Clinic Association of Los Angeles CountyNorth Coast Clinics NetworkCommunity Health PartnershipPlanned Parenthood Affiliates of CACA Rural Indian Health Board, Inc.
Clinics and Health CentersAlliance Medical CenterAnderson Valley Health CenterAsian Americans for Community InvolvementAsian Health Services, Inc.Bill Moore Community Health ClinicBrookside Community Health CenterCASA de SALUD Family Health ClinicChinatown Service Center Family Health ClinicClinica Msr. Oscar A. RomeroClinica Sierra VistaCoastal Health AllianceCommuniCare Health CentersCommunity Care Health CentersCommunity Health Alliance of PasadenaCommunity Health Partnership of Santa Clara
CountyCommunity Medical Centers, Inc.Copper Towers Family Medical Center Inc.Darin M. Camarena Health Centers, Inc.Del Norte Clinics, incEast Valley Community Health CenterEconomic Opportunity Commission, Inc.Eisner Ped. & Family M.C.Golden Valley Health CentersHaight Ashbury Free ClinicsHaight Ashbury Free Clinics Inc.Hill Country Community Clinic, Inc.Indian Health Center of Santa Clara ValleyIndian Health Council, Inc.Inland Behavioral and Health Services, IncKCEOC Family Health CenterKorean Health, Education, Information &
Research Center
APPENDIX B
Survey Respondents
APPENDIX C
CEO Succession Bibliography
La Maestra Family Clinic, Inc.Laguna Beach Community ClinicLassen Indian Health CenterLifeLong Medical CareLivingston Medical GroupLong Valley Health CenterMendocino Coast ClinicsMendocino Community Health ClinicMountain Health & Community ServicesMountain Valleys Health CentersNative American Health CenterNeighborhood HealthcareNHSINorth of Market Sr. Center (now Curry Senior
Center)Northeast Valley Health CorporationNortheastern Rural Health ClinicsOur Saviour Center/Cleaver ClinicPlanned ParenthoodPlanned Parenthood Mar MonteRedding Rancheria Indian Health ClinicRedwood coast Medical ServicesRedwood Community Health CoalitionRoseland Children’s Health CenterSalud Para La Gente, Inc.San Francisco Free ClinicSanta Barbara Neighborhood ClinicsSanta Cruz Women’s Health CenterS an Diego Community ClinicSequoia Community Health Foundation, Inc.Share Our Selves Free Medical/Dental ClinicShasta Community Health CenterSiskiyou Family Healthcare
“Daring to Lead: Nonprofit Executive Directors and Their Work Experience,” Jeanne Peters and Timothy Wolfred.CompassPoint Nonprofit Services, 2001. (415) 541-9000, www.compasspoint.org
“Finding and Retaining Your Next Chief Executive: Making the Transition Work,” Thomas N. Gilmore. Governance SeriesBooklet, BoardSource, 1993. (202) 452-6262, www.boardsource.org
“Following the Leader: A Guide for Planning Founding Director Transition,” Emily Redington and Donn Vickers. TheAcademy for Leadership & Governance, 2001. (614) 228-7444
“Hiring the Chief Executive: A Practical Guide to the Search and Selection Process,” Sheila Albert. BoardSource, 2000.(202)452-6262, www.boardsource.org
“Leadership Transitions,” The Nonprofit Quarterly, Volume 9, Issue 4, Winter 2002
“Managing Executive Transitions: A Handbook for Nonprofit Organizations,” Neighborhood Reinvestment Corporation,1999. (202)220-0300, www.nw.org
Managing Transitions: Making the Most of Change, William Bridges. Perseus Publishing. 1991. (617) 252-5000,www.perseuspublishing.com
“Managing Turnover at the Top: Charities seek to transform the loss of a leader into an opportunity,” The Chronicle ofPhilanthropy, Volume 11, June 3, 1999. www.philanthropy.com
Inside Back Cover

About CompassPointNonprofit Services
With offices in San Francisco and San José,CompassPoint Nonprofit Services is one of thenation’s leading consulting and training firmsserving nonprofit organizations. Through its 39staff and hundreds of volunteer professionals,CompassPoint provides management consultingand training to nonprofits in fundraising,technology utilization, strategic planning,nonprofit finance, executive transitions, boardsof directors, strategic internet presence, andother topics. Last year CompassPoint conductedmore than 600 workshops for Bay Areanonprofits, and consulted to more than 300nonprofit organizations. In addition toworkshops and consulting, CompassPointconducts several research projects each year,and publishes two free electronic newsletters—Food for Thought and the Board Café.CompassPoint’s mission is to increase theeffectiveness and impact of people working andvolunteering in the nonprofit sector.
CompassPoint Nonprofit Services
San Francisco706 Mission Street, 5th FloorSan Francisco, CA 94103415.541.9000415.541.7708 fx
Silicon Valley1922 The Alameda, Suite 212San José, CA 95126408.248.9505408.248.9504 fx
© 2003 Regional Associations of Californiavia: Family Health Council, Inc.All rights reserved. No portion of this material may be reproduced without prior written permission.
A free, downloadable version of this report is available at www.compasspoint.org.