Embed Size (px)
Citation preview

GLAUCOMA
Sectoral variations of iridocorneal angle width and iris volumein Chinese Singaporeans: a swept-source optical coherencetomography study
Tin A. Tun & Mani Baskaran & Shamira A. Perera &
Anita S. Chan & Ching-Yu Cheng & Hla M. Htoon &
Lisandro M. Sakata & Carol Y. Cheung & Tin Aung
Received: 22 December 2013 /Revised: 18 March 2014 /Accepted: 7 April 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractPurpose To assess variations in the iridocorneal angle widthand iris volume in Chinese subjects using swept-source opti-cal coherence tomography (SS-OCT).Methods Consecutive subjects, aged 40–80 years, with noprevious ophthalmic problems were recruited from apopulation-based study of Chinese Singaporeans. All subjectsunderwent 360° SS-OCT (SS-1000 CASIA, TomeyCorporation, Nagoya, Japan) angle imaging and gonioscopyin one randomly selected eye in the dark. For each eye, 16frames (11.25° apart) were selected for analysis from 128cross-sectional images, and measurements of the trabeculariris space area 750 μm from the scleral spur (TISA750) andiris volume were made for each image. The measurementsfrom four consecutive frames were further averaged as a
sector of 45°. Sector-wise angle width and quadrant-wise irisvolume were analyzed.Results Two hundred and twelve subjects (90 with closed-angles) were examined. The majority of the subjects werefemale (70.7 %) with mean age 61 (±8.9) years. The TISA750(mm2) of superior [0.101 (0.09)], inferior [0.105 (0.09)],superior–nasal [0.111 (0.09)] and superior–temporal [0.117(0.09)] sectors were smaller compared with other sectors(P<0.05). The nasal iris volume (mm3) was the smallestcompared with other quadrants for the entire cohort [nasal8.18 (1.2)<inferior 9.13 (1.3)<temporal 9.16 (1.2)<superior9.33 (1.3), P<0.001], as well as for open- and closed-anglegroups.Conclusions The irido-corneal angle was narrower in thesuperior, inferior, superior–nasal and superior–temporal sec-tors compared with other sectors. Iris volume in the nasalquadrant was the smallest compared with the other quadrants.
Keywords Angle width . Iris volume . Swept-source opticalcoherence tomography . Angle closure
Introduction
Primary angle-closure glaucoma (PACG) is a highly prevalentform of glaucoma in Asia [1]. The current reference methodfor assessing angle closure is clinical gonioscopy; however, itssubjective and semi-quantitative nature has directed interesttowards alternative methods of angle assessment [2]. Objec-tive and quantitative angle assessment by ultrasoundbiomicroscopy (UBM) or anterior segment optical coherencetomography (AS-OCT) have allowed assessment of a range ofnew angle parameters [3–6]. Studies using AS-OCT haveconfirmed the importance of shallow anterior chamber depth,smaller anterior chamber width, a thicker and anteriorly
T. A. Tun :M. Baskaran : S. A. Perera :A. S. Chan :H. M. Htoon :C. Y. Cheung : T. Aung (*)Singapore Eye Research Institute and Singapore National EyeCentre, 11 Third Hospital Avenue, Singapore 168751, Singaporee-mail: [email protected]
M. Baskaran : C. Y. Cheung : T. AungYong Loo Lin School ofMedicine, National University of Singapore,Singapore, Singapore
M. Baskaran : C.<Y. Cheng :H. M. Htoon : C. Y. Cheung : T. AungDuke–NUS Graduate Medical School, National University ofSingapore, Singapore, Singapore
A. S. ChanDepartment of Pathology, Singapore General Hospital, Singapore,Singapore
C.<Y. ChengSaw Swee Hock School of Public Health, National University ofSingapore, Singapore, Singapore
L. M. SakataFederal University of Parana, Curitiba, Brazil
Graefes Arch Clin Exp OphthalmolDOI 10.1007/s00417-014-2636-0

located lens as risk factors for angle closure [7–9]. Morerecently, iris parameters such as increased iris thickness, cur-vature, area, and volume have also been found to be associatedwith angle closure [3–5].
Studies on AS-OCT have focused on description of isolat-ed single sector summary measures of angle parameters in theeye. However, it is well-known that angle parameters varybetween sectors; for example, it has been suggested thatangles are narrower superiorly than inferiorly. In theory, sec-toral variation in angle width and iris profile can be assessedwith time-domain (TD) AS-OCT by rotating the orientation ofthe scan lines. However, due to low sampling speed, thesescans are limited to at most four simultaneous cross-sections.This precludes imaging the whole circumference of an eye indetail. A circumferential evaluation of the angle and irisprofile with its crypts, surface undulations, and a varyingthickness would be more analogous to clinical gonioscopy,and may deliver insights into the pathophysiology of angleclosure, glossed over by more limited isolated meridionalscanning protocols. Further, the iris volume measured bySSOCT may be more accurate than by ASOCT becauseSSOCT iris volume calculation is based on the informationfrom more cross-sectional scans compared to the single-scaninformation with ASOCT.
Swept-source OCT [10] (SS-OCT, CASIA SS-1000,Tomey Corporation, Nagoya, Japan) is a new form of AS-OCT that uses 1,310 nmwavelength (as with the TDAS-OCTsystem), to deliver 30,000 A-scans per second with an axialresolution of less than 10 μm. One unique advantage over TDAS-OCT is its anterior segment 360° scan protocol, whichtakes 2.4 s to capture 128 cross sectional slices; one every 1.4°[11]. It has a low variability of angle assessment and goodvisibility of the scleral spur in all quadrants [12, 13].
The aim of this study was to describe the variations in theiridocorneal angle width and iris volume across the entirecircumference of the anterior segment of the eye, using SS-OCT in subjects recruited from a population-based study.
Methods
This was a sub-study of the Singapore Chinese Eye Study(SCES), a population-based cross-sectional study of 3,300ethnic Chinese, aged 40 to 80 years, residing in Singapore.The details of recruitment and study design of the SCES havebeen described [14]. Written informed consent was obtainedfrom all participants. The study had the approval of the insti-tutional review board of the Singapore Eye Research Institute,and adhered to the tenets of the Declaration of Helsinki.
Consecutive participants were recruited and subjected tothe following examinations: measurement of visual acuity,dark-room SS-OCT anterior segment imaging, slit-lampbiomicroscopy, Goldmann applanation tonometry, and dark-
room gonioscopy on the same day. Subjects with a history ofintraocular surgery or penetrating trauma or those with anycorneal abnormalities that would preclude gonioscopy or im-aging were excluded from the study. Subjects who had laseriridotomy or iridoplasty were also excluded.
Gonioscopy
A single masked examiner with glaucoma fellowship training(MB) performed dark room gonioscopy with a Sussman four-mirror lens (Ocular instruments Inc., Bellevue, WA, USA) inall cases. The angle in each quadrant was graded using themodified Shaffer grading system, based on the anatomicalstructures observed (grade 0=no angle structures, grade 1=Schwalbe’s line, grade 2=anterior trabecular meshwork, grade3=posterior trabecular meshwork or scleral spur, grade 4=visible ciliary body band). A quadrant was considered“closed” if the posterior trabecular meshwork could not beseen in the primary position without indentation (modifiedShaffer grade 0, 1 or 2). Angle closure was defined in an eyewith two or more closed quadrants [15].
Anterior chamber angle imaging
One randomly-selected eye was imaged using the 3D-angleanalysis scan protocol of the SS-OCTunder standardized darkroom conditions before any contact procedures. Seated sub-jects were examined in the primary gaze position whilstdirected towards an internal fixation light. The operatoropened both lids, avoiding inadvertent pressure on the globeduring scanning. Each scan took 2.4 s and provided 128 crosssections of the anterior segment of each eye. Each image wasaveraged automatically from three consecutive scans by thealgorithm native to the CASIA system.
Image analysis
A single masked observer (TAT) used the 360° SS-OCTviewer (version 5.0, Tomey, Nagoya, Japan) to mark thelocation of the scleral spur and the algorithm calculated allthe parameters automatically. The scleral spur was defined asthe inward protrusion of the sclera where a change in curva-ture of the corneo-scleral interface was noted [16]. Attemptswere made to substitute the images, which had poor scleralspur visibility, with the nearest scans with better visibility.However, the images were excluded from calculation if thescleral spur could not be identified.
Sixteen out of 128 frames (32 anterior chamber angles,11.25° increments) were chosen automatically by the analysisprotocol. The trabecular-iris space area at 750 μm (TISA750)from the scleral spur of four consecutive ‘angles’ of theparticular sector (45º) were averaged and compared betweensuperior, superior–nasal, nasal, inferior–nasal, inferior,
Graefes Arch Clin Exp Ophthalmol
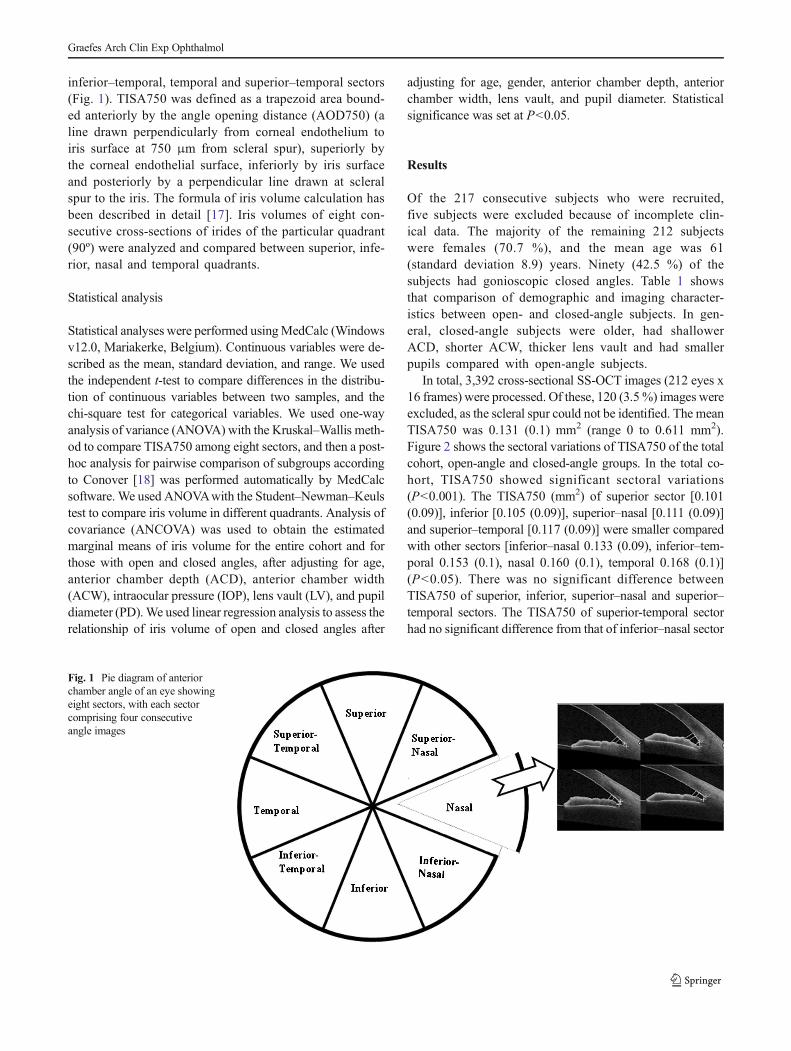
inferior–temporal, temporal and superior–temporal sectors(Fig. 1). TISA750 was defined as a trapezoid area bound-ed anteriorly by the angle opening distance (AOD750) (aline drawn perpendicularly from corneal endothelium toiris surface at 750 μm from scleral spur), superiorly bythe corneal endothelial surface, inferiorly by iris surfaceand posteriorly by a perpendicular line drawn at scleralspur to the iris. The formula of iris volume calculation hasbeen described in detail [17]. Iris volumes of eight con-secutive cross-sections of irides of the particular quadrant(90º) were analyzed and compared between superior, infe-rior, nasal and temporal quadrants.
Statistical analysis
Statistical analyses were performed usingMedCalc (Windowsv12.0, Mariakerke, Belgium). Continuous variables were de-scribed as the mean, standard deviation, and range. We usedthe independent t-test to compare differences in the distribu-tion of continuous variables between two samples, and thechi-square test for categorical variables. We used one-wayanalysis of variance (ANOVA) with the Kruskal–Wallis meth-od to compare TISA750 among eight sectors, and then a post-hoc analysis for pairwise comparison of subgroups accordingto Conover [18] was performed automatically by MedCalcsoftware. We used ANOVAwith the Student–Newman–Keulstest to compare iris volume in different quadrants. Analysis ofcovariance (ANCOVA) was used to obtain the estimatedmarginal means of iris volume for the entire cohort and forthose with open and closed angles, after adjusting for age,anterior chamber depth (ACD), anterior chamber width(ACW), intraocular pressure (IOP), lens vault (LV), and pupildiameter (PD).We used linear regression analysis to assess therelationship of iris volume of open and closed angles after
adjusting for age, gender, anterior chamber depth, anteriorchamber width, lens vault, and pupil diameter. Statisticalsignificance was set at P<0.05.
Results
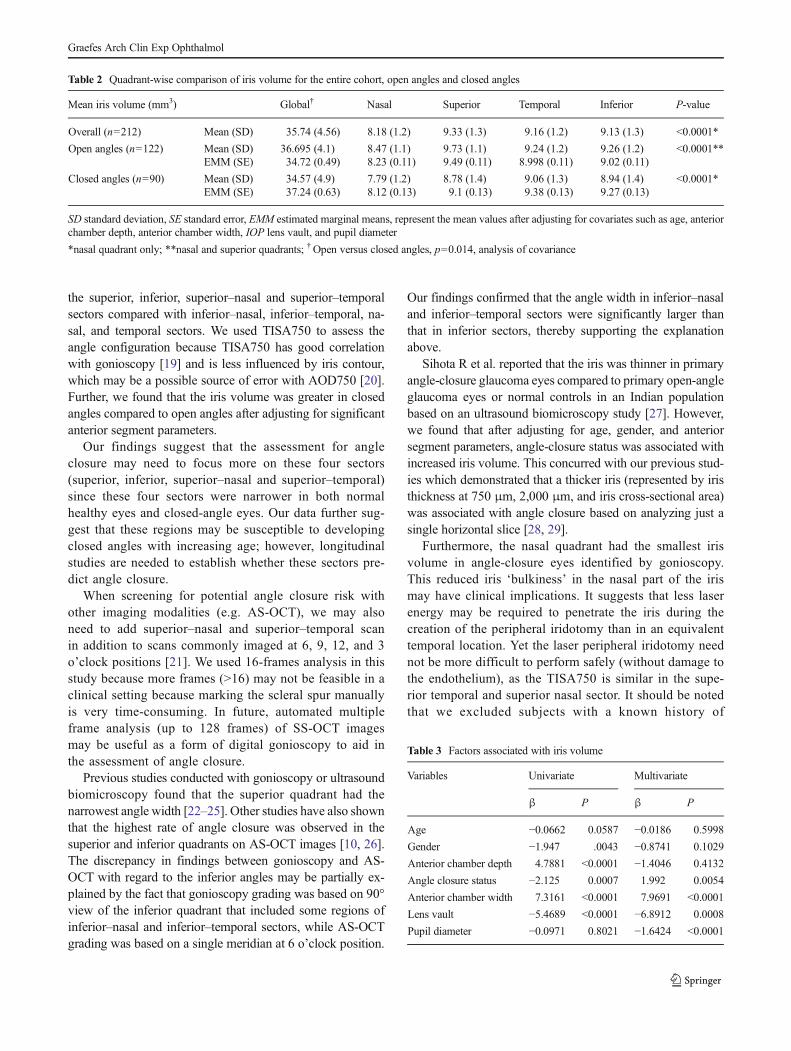
Of the 217 consecutive subjects who were recruited,five subjects were excluded because of incomplete clin-ical data. The majority of the remaining 212 subjectswere females (70.7 %), and the mean age was 61(standard deviation 8.9) years. Ninety (42.5 %) of thesubjects had gonioscopic closed angles. Table 1 showsthat comparison of demographic and imaging character-istics between open- and closed-angle subjects. In gen-eral, closed-angle subjects were older, had shallowerACD, shorter ACW, thicker lens vault and had smallerpupils compared with open-angle subjects.
In total, 3,392 cross-sectional SS-OCT images (212 eyes x16 frames) were processed. Of these, 120 (3.5%) images wereexcluded, as the scleral spur could not be identified. The meanTISA750 was 0.131 (0.1) mm2 (range 0 to 0.611 mm2).Figure 2 shows the sectoral variations of TISA750 of the totalcohort, open-angle and closed-angle groups. In the total co-hort, TISA750 showed significant sectoral variations(P<0.001). The TISA750 (mm2) of superior sector [0.101(0.09)], inferior [0.105 (0.09)], superior–nasal [0.111 (0.09)]and superior–temporal [0.117 (0.09)] were smaller comparedwith other sectors [inferior–nasal 0.133 (0.09), inferior–tem-poral 0.153 (0.1), nasal 0.160 (0.1), temporal 0.168 (0.1)](P<0.05). There was no significant difference betweenTISA750 of superior, inferior, superior–nasal and superior–temporal sectors. The TISA750 of superior-temporal sectorhad no significant difference from that of inferior–nasal sector
Fig. 1 Pie diagram of anteriorchamber angle of an eye showingeight sectors, with each sectorcomprising four consecutiveangle images
Graefes Arch Clin Exp Ophthalmol
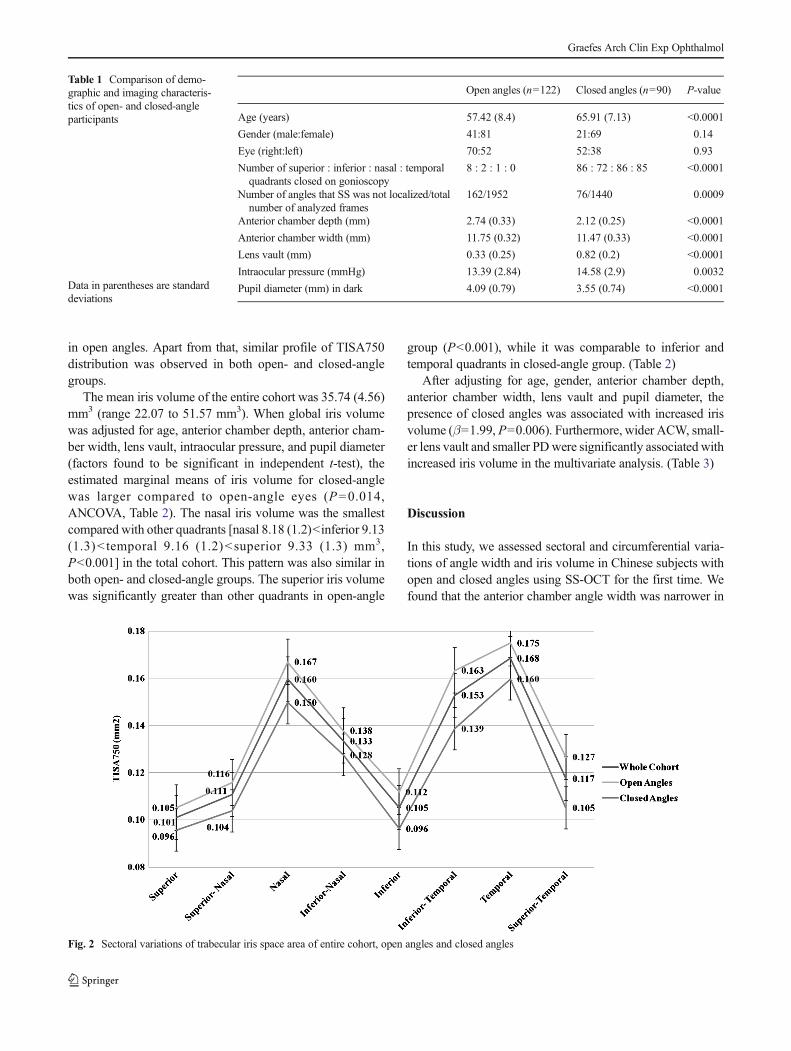
in open angles. Apart from that, similar profile of TISA750distribution was observed in both open- and closed-anglegroups.
The mean iris volume of the entire cohort was 35.74 (4.56)mm3 (range 22.07 to 51.57 mm3). When global iris volumewas adjusted for age, anterior chamber depth, anterior cham-ber width, lens vault, intraocular pressure, and pupil diameter(factors found to be significant in independent t-test), theestimated marginal means of iris volume for closed-anglewas larger compared to open-angle eyes (P=0.014,ANCOVA, Table 2). The nasal iris volume was the smallestcompared with other quadrants [nasal 8.18 (1.2)<inferior 9.13(1.3)< temporal 9.16 (1.2)<superior 9.33 (1.3) mm3,P<0.001] in the total cohort. This pattern was also similar inboth open- and closed-angle groups. The superior iris volumewas significantly greater than other quadrants in open-angle
group (P<0.001), while it was comparable to inferior andtemporal quadrants in closed-angle group. (Table 2)
After adjusting for age, gender, anterior chamber depth,anterior chamber width, lens vault and pupil diameter, thepresence of closed angles was associated with increased irisvolume (β=1.99, P=0.006). Furthermore, wider ACW, small-er lens vault and smaller PDwere significantly associated withincreased iris volume in the multivariate analysis. (Table 3)
Discussion
In this study, we assessed sectoral and circumferential varia-tions of angle width and iris volume in Chinese subjects withopen and closed angles using SS-OCT for the first time. Wefound that the anterior chamber angle width was narrower in
Table 1 Comparison of demo-graphic and imaging characteris-tics of open- and closed-angleparticipants
Data in parentheses are standarddeviations
Open angles (n=122) Closed angles (n=90) P-value
Age (years) 57.42 (8.4) 65.91 (7.13) <0.0001
Gender (male:female) 41:81 21:69 0.14
Eye (right:left) 70:52 52:38 0.93
Number of superior : inferior : nasal : temporalquadrants closed on gonioscopy
8 : 2 : 1 : 0 86 : 72 : 86 : 85 <0.0001
Number of angles that SS was not localized/totalnumber of analyzed frames
162/1952 76/1440 0.0009
Anterior chamber depth (mm) 2.74 (0.33) 2.12 (0.25) <0.0001
Anterior chamber width (mm) 11.75 (0.32) 11.47 (0.33) <0.0001
Lens vault (mm) 0.33 (0.25) 0.82 (0.2) <0.0001
Intraocular pressure (mmHg) 13.39 (2.84) 14.58 (2.9) 0.0032
Pupil diameter (mm) in dark 4.09 (0.79) 3.55 (0.74) <0.0001
Fig. 2 Sectoral variations of trabecular iris space area of entire cohort, open angles and closed angles
Graefes Arch Clin Exp Ophthalmol
the superior, inferior, superior–nasal and superior–temporalsectors compared with inferior–nasal, inferior–temporal, na-sal, and temporal sectors. We used TISA750 to assess theangle configuration because TISA750 has good correlationwith gonioscopy [19] and is less influenced by iris contour,which may be a possible source of error with AOD750 [20].Further, we found that the iris volume was greater in closedangles compared to open angles after adjusting for significantanterior segment parameters.
Our findings suggest that the assessment for angleclosure may need to focus more on these four sectors(superior, inferior, superior–nasal and superior–temporal)since these four sectors were narrower in both normalhealthy eyes and closed-angle eyes. Our data further sug-gest that these regions may be susceptible to developingclosed angles with increasing age; however, longitudinalstudies are needed to establish whether these sectors pre-dict angle closure.
When screening for potential angle closure risk withother imaging modalities (e.g. AS-OCT), we may alsoneed to add superior–nasal and superior–temporal scanin addition to scans commonly imaged at 6, 9, 12, and 3o’clock positions [21]. We used 16-frames analysis in thisstudy because more frames (>16) may not be feasible in aclinical setting because marking the scleral spur manuallyis very time-consuming. In future, automated multipleframe analysis (up to 128 frames) of SS-OCT imagesmay be useful as a form of digital gonioscopy to aid inthe assessment of angle closure.
Previous studies conducted with gonioscopy or ultrasoundbiomicroscopy found that the superior quadrant had thenarrowest angle width [22–25]. Other studies have also shownthat the highest rate of angle closure was observed in thesuperior and inferior quadrants on AS-OCT images [10, 26].The discrepancy in findings between gonioscopy and AS-OCT with regard to the inferior angles may be partially ex-plained by the fact that gonioscopy grading was based on 90°view of the inferior quadrant that included some regions ofinferior–nasal and inferior–temporal sectors, while AS-OCTgrading was based on a single meridian at 6 o’clock position.
Our findings confirmed that the angle width in inferior–nasaland inferior–temporal sectors were significantly larger thanthat in inferior sectors, thereby supporting the explanationabove.
Sihota R et al. reported that the iris was thinner in primaryangle-closure glaucoma eyes compared to primary open-angleglaucoma eyes or normal controls in an Indian populationbased on an ultrasound biomicroscopy study [27]. However,we found that after adjusting for age, gender, and anteriorsegment parameters, angle-closure status was associated withincreased iris volume. This concurred with our previous stud-ies which demonstrated that a thicker iris (represented by iristhickness at 750 μm, 2,000 μm, and iris cross-sectional area)was associated with angle closure based on analyzing just asingle horizontal slice [28, 29].
Furthermore, the nasal quadrant had the smallest irisvolume in angle-closure eyes identified by gonioscopy.This reduced iris ‘bulkiness’ in the nasal part of the irismay have clinical implications. It suggests that less laserenergy may be required to penetrate the iris during thecreation of the peripheral iridotomy than in an equivalenttemporal location. Yet the laser peripheral iridotomy neednot be more difficult to perform safely (without damage tothe endothelium), as the TISA750 is similar in the supe-rior temporal and superior nasal sector. It should be notedthat we excluded subjects with a known history of
Table 2 Quadrant-wise comparison of iris volume for the entire cohort, open angles and closed angles
Mean iris volume (mm3) Global† Nasal Superior Temporal Inferior P-value
Overall (n=212) Mean (SD) 35.74 (4.56) 8.18 (1.2) 9.33 (1.3) 9.16 (1.2) 9.13 (1.3) <0.0001*
Open angles (n=122) Mean (SD) 36.695 (4.1) 8.47 (1.1) 9.73 (1.1) 9.24 (1.2) 9.26 (1.2) <0.0001**EMM (SE) 34.72 (0.49) 8.23 (0.11) 9.49 (0.11) 8.998 (0.11) 9.02 (0.11)
Closed angles (n=90) Mean (SD) 34.57 (4.9) 7.79 (1.2) 8.78 (1.4) 9.06 (1.3) 8.94 (1.4) <0.0001*EMM (SE) 37.24 (0.63) 8.12 (0.13) 9.1 (0.13) 9.38 (0.13) 9.27 (0.13)
SD standard deviation, SE standard error, EMM estimated marginal means, represent the mean values after adjusting for covariates such as age, anteriorchamber depth, anterior chamber width, IOP lens vault, and pupil diameter
*nasal quadrant only; **nasal and superior quadrants; †Open versus closed angles, p=0.014, analysis of covariance
Table 3 Factors associated with iris volume
Variables Univariate Multivariate
β P β P
Age −0.0662 0.0587 −0.0186 0.5998
Gender −1.947 .0043 −0.8741 0.1029
Anterior chamber depth 4.7881 <0.0001 −1.4046 0.4132
Angle closure status −2.125 0.0007 1.992 0.0054
Anterior chamber width 7.3161 <0.0001 7.9691 <0.0001
Lens vault −5.4689 <0.0001 −6.8912 0.0008
Pupil diameter −0.0971 0.8021 −1.6424 <0.0001
Graefes Arch Clin Exp Ophthalmol

glaucoma or those with iridotomy or iridoplasty to avoidthe consequence of ischemic iris atrophy, reduced irismobility, or the effect of laser therapy on the iris.
There are some limitations to our study. This study popu-lation was Chinese and findings may be different in otherracial groups. However, Chinese persons are at high risk ofangle-closure glaucoma. The image acquisition proved diffi-culties at times, due to movement of the globe or eyelidsespecially those with small eyes. There may have been sys-tematic bias, as we used a single observer for gonioscopy aswell as a single grader for image analysis.
In summary, we describe the sectoral variations of anglewidth and iris volume in the Chinese population using SS-OCT. The narrowest angle width was observed in the superior,inferior, superior–nasal and superior–temporal sectors com-pared with others. The iris volume of the nasal quadrant wasthe smallest compared with other quadrants. These sectorsmay be at highest risk of angle closure, and could be the focusof future screening strategies.
Grant support The study was supported by a Translational ClinicalResearch Partnership grant from the Biomedical Research Council(BMRC), Singapore (Grant No. 10/1/35/19/674) and National MedicalResearch Council.
References
1. Foster PJ, Johnson GJ (2001) Glaucoma in China: how big is theproblem? Br J Ophthalmol 85(11):1277–1282, Review
2. Friedman DS, He M (2008) Anterior chamber angle assessmenttechniques. Surv Ophthalmol 53(3):250–273
3. Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS (1991) Clinical useof ultrasound biomicroscopy. Ophthalmology 98(3):287–295
4. Pavlin CJ, Harasiewicz K, Foster FS (1992) Ultrasoundbiomicroscopy of anterior segment structures in normal andglaucomatous eyes. Am J Ophthalmol 113(4):381–389
5. Leung CK, Yung WH, Yiu CK et al (2006) Novel approach foranterior chamber angle analysis: anterior chamber angle detectionwith edge measurement and identification algorithm (ACADEMIA).Arch Ophthalmol 124(10):1395–1401
6. Dorairaj S, Liebmann JM, Ritch R (2007) Quantitative evaluation ofanterior segment parameters in the era of imaging. Trans AmOphthalmol Soc 105:99–108, discussion 108–10. Review
7. Lowe RF (1970) Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyesand eyes with primary angle-closure glaucoma. Br J Ophthalmol54(3):161–169
8. Nongpiur ME, Sakata LM, Friedman DS et al (2010) Novel associ-ation of smaller anterior chamber width with angle closure inSingaporeans. Ophthalmology 117(10):1967–1973
9. Nongpiur ME, He M, Amerasinghe N et al (2011) Lens vault,thickness, and position in Chinese subjects with angle closure.Ophthalmology 118(3):474–479
10. Leung CK,WeinrebRN (2011)Anterior chamber angle imagingwithoptical coherence tomography. Eye (Lond) 25(3):261–267
11. Baskaran M, Ho SW, Tun TA et al (2013) Assessment of circumfer-ential angle-closure by the iris-trabecular contact index with swept-source optical coherence tomography. Ophthalmology 120(11):2226–2231
12. Liu S, Yu M, Ye C, Lam DS, Leung CK (2011) Anterior chamberangle imaging with swept-source optical coherence tomography: aninvestigation on variability of angle measurement. Invest OphthalmolVis Sci 52(12):8598–8603
13. Tun TA, Baskaran M, Zheng C et al (2013) Assessment of trabecularmeshwork width using swept source optical coherence tomography.Graefes Arch Clin Exp Ophthalmol 251(6):1587–1592
14. Lavanya R, Jeganathan VS, Zheng Yet al (2009)Methodology of theSingapore Indian Chinese Cohort (SICC) Eye Study: quantifyingethnic variations in the epidemiology of eye diseases in Asians.Ophthalmic Epidemiol 16(6):325–336
15. SEAGIG guidelines (2008) Gonioscopy. Asia pacific glaucomaguidelines. Scientific Communications Int, Hong Kong, http://www.apglaucomasociety.org/toc/APGG2_fullversionNMview.pdf.Accessed July 3, 2013
16. Ho SW, Baskaran M, Zheng C et al (2013) Swept source opticalcoherence tomography measurement of the iris-trabecular contact(ITC) index: a new parameter for angle closure. Graefes Arch ClinExp Ophthalmol 251(4):1205–1211
17. Mak H, Xu G, Leung CK (2013) Imaging the iris with swept-source optical coherence tomography: relationship between irisvolume and primary angle closure. Ophthalmology 120(12):2517–2524
18. Conover WJ (1999) Practical nonparametric statistics, 3rd edn. JohnWiley & Sons, New York
19. Radhakrishnan S, Goldsmith J, Huang D et al (2005) Comparison ofoptical coherence tomography and ultrasound biomicroscopy fordetection of narrow anterior chamber angles. Arch Ophthalmol123(8):1053–1059
20. Radhakrishnan S, Huang D, Smith SD (2005) Optical coherencetomography imaging of the anterior chamber angle. OphthalmolClin N Am 18(3):375–381, vi. Review
21. Khor WB, Sakata LM, Friedman DS et al (2010) Evaluation ofscanning protocols for imaging the anterior chamber angle withanterior segment-optical coherence tomography. J Glaucoma 19(6):365–368
22. He M, Foster PJ, Ge J et al (2006) Gonioscopy in adult Chinese: theLiwan Eye Study. Invest Ophthalmol Vis Sci 47(11):4772–4779
23. Kunimatsu S, Tomidokoro A, Mishima K et al (2005) Prevalence ofappositional angle closure determined by ultrasonic biomicroscopy ineyes with shallow anterior chambers. Ophthalmology 112(3):407–412
24. Phillips CI (1956) Closed-angle glaucoma; significance of sectoralvariations in angle depth. Br J Ophthalmol 40(3):136–143
25. Phillips CI (1956) Sectoral distribution of goniosynechiae. Br JOphthalmol 40(3):129–135
26. Sakata LM, Lavanya R, Friedman DS et al (2008) Comparison ofgonioscopy and anterior segment ocular coherence tomography indetecting angle closure in different quadrants of the anterior chamberangle. Ophthalmology 115(5):769–774
27. Sihota R, Dada T, Gupta R, Lakshminarayan P, Pandey RM (2005)Ultrasound biomicroscopy in the subtypes of primary angle closureglaucoma. J Glaucoma 14(5):387–391
28. Wang BS, Narayanaswamy A, Amerasinghe N et al (2011) Increasediris thickness and association with primary angle closure glaucoma.Br J Ophthalmol 95(1):46–50
29. Wang B, Sakata LM, Friedman DS et al (2010) Quantitative irisparameters and association with narrow angles. Ophthalmology117(1):11–17
Graefes Arch Clin Exp Ophthalmol