-
Pharmaceuticals sector
Inexpensive drugs from India to transform the global drug
industrytrend toward biosimilars
Analysts
Ryoichi UrushiharaMotoya KohtaniKaran AhujaSaion
MukherjeeAvinash Ghalke
(Japan)(Japan)(Japan)(India)(India)
US/European majors procuring cheap drugs in bulk from
IndiaAntibody biosimilars poised for widespread global useSigns of
shift back from antibody therapeutics to small molecule drugs
21 June 2010Please read the important disclosures and analyst pp
certifications on. 105-108. gl
-
Nomura 1
Inexpensive drugs likely to become widespread throughout the
world:
Healthcare reforms in the US mean that in all the major
industrialized nations, the state now has overall control of
medical insurance. With industrialized economies growing at less
than 2% a year, ways will have to be found to curtail healthcare
spending now that it is partly or wholly the responsibility of the
state. The volume of pharmaceuticals consumed is rising by about 7%
a year as the world's population becomes older. As such, drug
prices will have to fall more than 5% a year to prevent a squeeze
on government finances. We therefore think the uptake of
inexpensive drugs will become necessary globally.
Generic versions of antibody drugs: Indian generic drugmakers
are attempting to cut manufacturing costs to the bone via lower
personnel costs and streamlined production processes for drug
materials. We estimate that production costs for low molecular
weight drugs are less than 20% of costs in Japan. The Indian
authorities already have approved a biosimilar for Rituxan, an
antibody treatment for cancer. Although it is priced at only a 50%
discount to the branded drug, very low production costs mean that
the Rituxan biosimilar appears to command a gross margin of more
than 80%. Antibody treatment with branded drugs costs several
million yen per annum. We think biosimilars will establish
themselves rapidly in industrialized nations as they will help to
reduce costs for both patients and governments.
Partnerships between Western and Indian drugmakers: Major
drugmakers in Europe and the US have been pursuing partnerships
with Indian generic drugmakers since 2008 in order to secure
supplies of inexpensive pharmaceuticals. Their aim is to generate
stable earnings by supplying inexpensive drugs for the treatment of
chronic conditions on global markets. This has given rise to a
well-balanced business model, with the high-risk, high-return
business of developing drugs for unmet medical needssuch as
anticancer drugs and treatments for central nervous system
disorderscomplemented with inexpensive drugs sourced from
India.
Indian companies riding the wave of expansion in biosimilar
industry: Among Indian drugmakers, we find Dr Reddys Laboratories
[DRRD IN] (Buy; INR1,423.45, 17 June close) to be of the most
interest. Dr Reddy's has been expanding its US operations, as well
as supplying active pharmaceutical ingredients (APIs) for generics
and partnering with GlaxoSmithKline [GSK LN] (Neutral; GBp1,215) to
market drugs in emerging economies. Our next recommendation is
Jubilant Organosys [JOL IN] (Buy; INR348.65), which has alliances
with Eli Lilly [LLY US] (No rating; $34.39) and other overseas drug
majors under which it provides not only R&D but also
manufacturing support.
Pharmaceuticals sector
Inexpensive drugs from India to transform the global
pharmaceutical industrytrend toward biosimilars In this report,
partially based on research carried out in India, we make the case
that biosimilar antibody drugs (generic versions of
biotherapeutics) will become widespread in industrialized nations
by 2015, for the following two reasons. First, we think conditions
are right for medical authorities in Japan, the US and Europe to
start approving biosimilars, including antibody biosimilars.
Second, biosimilars can now be manufactured inexpensively.
Regulatory and technological obstacles to the release of
biosimilars are now diminishing. We think biosimilars will make
rapid inroads if guidelines for their approval are established in
Europe, Japan, and the United States. Industrialized nations are
likely to approve inexpensive yet effective biosimilars in order to
rein in growth in healthcare spending caused by the ageing of their
societies. Biosimilars of antibody drugs have already been approved
in India. US and European generic drugmakers have been stepping up
partnerships with Indian companies to produce biosimilars, and
branded drugmakers are now following suit. We think inexpensive
drugs from India will transformthe contours of the global
pharmaceutical industry.
21 June 2010 Japanese full report: 21 Jun
Report no. 10-236 Analysts Ryoichi Urushihara +81-3-5255-1785
[email protected] Motoya Kohtani +81-3-5255-1640
[email protected] Karan Ahuja [email protected]
Financial & Economic Research Center Nomura Securities, Tokyo
Saion Mukherjee +91-22-4037-4184 [email protected] Nomura
Financial Advisory and Securities (India) Avinash Ghalke
+91-22-405-32046 [email protected] Nomura Structured
Finance Services, India Please read the important disclosures and
analyst certifications on pp. 105108. gl
Nomura Securities Co Ltd, Tokyo Japanese Equity Research
(continued over)
-
Nomura Japanese Equity Research
2 Pharmaceuticals sector
Japanese drugmakers establishing themselves in India: Japanese
drugmakers have been slow to adapt to the global shift toward
cheaper drugs. In the context of this report, we therefore focus on
Daiichi Sankyo [4568] (Buy; 1,607, 18 June close), which has
acquired Indias Ranbaxy Laboratories [RBXY IN] (Reduce; INR442.70,
17 June close) with a view to building a presence in emerging
markets, and Eisai [4523] (Buy; 2,982), which has a manufacturing
plant in India. In doing so, both are taking steps to curb
production costs. We also highlight JCR Pharmaceuticals [4552] (No
rating; 1,264), which has already released an erythropoietin (EPO)
biosimilar in Japan. Nipro [8086] (Neutral; 1,718) too is
developing an EPO biosimilar for the domestic market, and we think
both companies bear close monitoring. Also noteworthy is Fuji
Pharma [4554] (No rating; 1,725), for its granulocyte-colony
stimulating factor (G-CSF).
1. Summary: we look for sustained global demand for inexpensive
drugs............. 5 2. Indian pharmaceutical
industry.........................................................................
20
(1) Dr Reddys Laboratories [DRRD IN] (Buy; INR1,423.45) (Saion
Mukherjee) .....................30 (2) Lupin Laboratories [LPC IN]
(Buy; INR1,879.90) (Saion
Mukherjee)..................................31 (3) Glenmark
Pharmaceuticals [GNP IN] (Buy; INR271.80) (Saion
Mukherjee).......................32 (4) Sun Pharmaceutical
Industries [SUNP IN] (Neutral; INR1,698.75) (Saion
Mukherjee).........................33 (5) GlaxoSmithKline
Pharmaceuticals [GLXO IN] (Neutral; INR2,096.70) (Saion Mukherjee)
....................34 (6) Cipla [CIPLA IN] (Reduce; INR334.65)
(Saion
Mukherjee).................................................35 (7)
Ranbaxy Laboratories [RBXY IN] (Reduce; INR442.70) (Saion
Mukherjee) ......................36 (8) Jubilant Organosys [JOL IN]
(Buy; INR348.65) (Saion Mukherjee)
....................................37
3. Antibody biosimilars destined to take hold around the
world........................... 38
Shimadzu [7701] (Buy) (Motoya
Kohtani).................................................................................71
Nipro [8086] (Neutral) (Motoya
Kohtani)...................................................................................73
4. Japan: government promoting generics
........................................................... 75
Kyowa Hakko Kirin [4151] (Buy) (Ryoichi
Urushihara)..............................................................85
Eisai [4523] (Buy) (Ryoichi Urushihara)
....................................................................................88
Nichi-Iko Pharmaceutical [4541] (Buy) (Ryoichi Urushihara)
....................................................90 JCR
Pharmaceuticals [4552] (No rating) (Motoya
Kohtani)......................................................92
Towa Pharmaceutical [4553] (Buy) (Ryoichi Urushihara)
.........................................................94 Fuji
Pharma [4554] (No rating) (Ryoichi Urushihara)
................................................................96
Sawai Pharmaceutical [4555] (No rating) (Ryoichi
Urushihara)................................................98
Daiichi Sankyo [4568] (Buy) (Ryoichi Urushihara)
..................................................................100
Contents
continued from front cover
-
Nomura Japanese Equity Research
Pharmaceuticals sector 3
-
Nomura Japanese Equity Research
4 Pharmaceuticals sector
Companies mentioned in this report
Code/ticker Company Rating Share price Ticker Company Rating
Share price 2269 Meiji Holdings Buy 3,705 SVLS IN Suven Life
Sciences Limited No rating INR31.35 3101 Toyobo Neutral 159 TRP IN
Torrent Pharmaceuticals Limited No rating INR557.20 4151 Kyowa
Hakko Kirin Buy 847 WANB IN Wanbury Limited No rating INR77.35 4502
Takeda Pharmaceutical Neutral 3,895 WPL IN Wockhardt Limited No
rating INR136.20 4503 Astellas Pharma Neutral 3,015 ZTL IN Zenotech
Laboratories Ltd. No rating INR113.80 4506 Dainippon Sumitomo
Pharma Buy 709 ABT US Abbott Laboratories No rating US$48.63 4507
Shionogi Neutral 1,690 ALXN US Alexion Pharmaceuticals, Inc. No
rating US$54.22 4508 Mitsubishi Tanabe Pharma Buy 1,319 AGN US
Allergan Inc. No rating US$61.45 4514 Aska Pharmaceutical No rating
643 AMGN US Amgen Inc. No rating US$55.44 4519 Chugai
Pharmaceutical Buy 1,633 ARQL US ArQule Inc. No rating US$5.22 4523
Eisai Buy 2,982 BAX US Baxter International Inc. No rating US$42.58
4528 Ono Pharmaceutical Neutral 3,610 BIIB US Biogen Idec Inc. No
rating US$49.01 4530 Hisamitsu Pharmaceutical Buy 3,335 BMY US
Bristol-Myers Squibb Company No rating US$25.86 4534 Mochida
Pharmaceutical No rating 848 CPD US Caraco Pharmaceutical
Laboratories, Ltd. No rating US$4.43 4535 Taisho Pharmaceutical
Neutral 1,749 ELN US Elan Corporation, plc, No rating US$4.95 4536
Santen Pharmaceutical Neutral 2,989 LLY US Eli Lilly & Co. No
rating US$34.39 4540 Tsumura Buy 2,666 ENDP US Endo Pharmaceuticals
Holdings No rating US$21.89 4541 Nichi-Iko Pharmaceutical Buy 3,330
FRX US Forest Laboratories Inc. No rating US$27.30 4552 JCR
Pharmaceuticals No rating 1,264 GENZ US Genzyme Corporation No
rating US$51.43 4553 Towa Pharmaceutical Buy 5,860 GILD US Gilead
Sciences, Inc. No rating US$35.97 4554 Fuji Pharma No rating 1,725
HSP US Hospira, Inc. No rating US$56.18 4555 Sawai Pharmaceutical
No rating 8,290 JNJ US Johnson & Johnson No rating US$59.18
4568 Daiichi Sankyo Buy 1,607 MRK US Merck & Co. Inc. No rating
US$35.86 4569 Kyorin Buy 1,255 MYL US Mylan No rating US$18.36 5201
Asahi Glass Buy 936 PDLI US PDL BioPharma, Inc. No rating US$5.62
7701 Shimadzu Buy 708 PFE US Pfizer No rating US$15.47 8086 Nipro
Neutral 1,718 REGN US Regeneron Pharmaceuticals, Inc. No rating
US$26.55 ARBP IN Aurobindo Pharma Limited No rating INR851.55 SIAL
US Sigma-Aldrich Corporation No rating US$53.38 BIOS IN Biocon
Limited No rating INR310.65 TEVA US Teva Pharmaceutical Industries
No rating US$54.22 CDH IN Cadila Healthcare Ltd. No rating
INR630.20 WPI US Watson Pharmaceuticals Inc. No rating US$44.26
CIPLA IN Cipla Ltd. Reduce INR334.65 AZN LN AstraZeneca PLC Reduce
GBp3,082 DISH IN Dishman Pharmacuticals & Chemicals Ltd. No
rating INR205.60 GSK LN GlaxoSmithKline plc Neutral GBp1,215 DIVI
IN Divi's Laboratories Ltd No rating INR770.05 NOVN VX Novartis AG
Buy CHF54.40 DRRD IN Dr. Reddy's Laboratories Ltd. Buy INR1,423.45
ROG VX Roche Neutral CHF158.90 GLXO IN GlaxoSmithKline
Pharmaceuticals Ltd. Neutral INR2,096.70 LONN VX Lonza Group Ltd.
No rating CHF77.40 GNP IN Glenmark Pharmaceuticals Limited Buy
INR271.80 BAS GR BASF Neutral 46.64 JOL IN Jubilant Organosys
Limited, Buy INR348.65 BAYN GY Bayer AG Neutral 48.665 JPO IN
Jupiter Bioscience Limited No rating INR83.30 BIM FP bioMerieux sa
No rating 83.90 LPC IN Lupin Limited. Buy INR1,879.90 SAN FP
Sanofi-Aventis Neutral 51.11 NTCPH IN Natco Pharma Limited No
rating INR168.35 SAZ GY Stada Arzneimittel AG No rating 29.60 OPTC
IN Opto Circuits India Limited No rating INR228.05 UCB BB UCB S.A.
Neutral 26.96 OCP IN Orchid Chemicals & Pharmaceuticals Ltd. No
rating INR154.55 YM CN YM Biosciemces No rating C$1.27 PFIZ IN
Pfizer Limited, India No rating INR1,101.05 GEN DC Genmab A/S No
rating DKK51.30 PIHC IN Piramal Healthcare Limited No rating
INR488.55 NOVOB DC Novo Nordisk A/S Reduce DKK488.70 PLSL IN
Piramal Lifescience No rating INR137.80 NZYMB DC Novozymes A/S No
rating DKK688.50 RBXY IN Ranbaxy Laboratories Limited Reduce
INR442.70 068270 KS Celltrion No rating KRW21,200 STR IN Strides
Arcolab Limited No rating INR389.45 068875 KS LG Life Sceineces Ltd
No rating KRW22,250 SUNP IN Sun Pharmaceutical Industries Ltd.
Neutral INR1,698.75 Note: Share prices as of 18 June close for
Japanese stocks, 17 June close for other stocks. Source: Nomura
-
Nomura Japanese Equity Research
Pharmaceuticals sector 5
1. Summary: we look for sustained global demand for inexpensive
drugs (1) Conclusion: antibody therapeutic biosimilars likely to
find a global market We recently visited 21 companies1, including
Indian generic drug makers, to gauge the current status of the
generic drug market. We toured manufacturing plants of four makers:
Aurobindo, Eisai, Ranbaxy, and Strides Arcolab. We discovered the
main focus of Indian generic drug makers is expanding scale merits
as much as possible to reduce manufacturing costs, thereby
facilitating the supply of a wide range of low-cost drugs.
Typically, a generic drug refers to the generic version of a
small molecule drug that has a molecular weight below 300. Indian
generic makers have started expanding into generic biologicals
(biosimilars). Biologicals are pharmaceuticals that use biological
substances as the active ingredient and products like growth
hormone and anemia treatment EPO. They are typically classified as
either protein drugs, which have a molecular weight of
10,00030,000, or antibody therapeutics, which have a molecular
weight of 150,000 (Exhibit 1-1). Biosimilars is the term for
generic versions of biopharmaceuticals. Unlike small molecule drugs
that are chemically synthesized, biosimilars are produced through
fermentation and thus are not completely identical to the original
drug. Instead, they are mostly similar, which is why the term
biosimilar was coined. Dr. Reddys Laboratories currently markets a
biosimilar of antibody therapeutic Rituxan (cancer treatment) under
the trade name Reditux. Sold at half the price of brand drugs, the
branded drug maker lowered its price as well. Conventional stock
market wisdom is that antibody therapeutic biosimilars will not be
commercialized, but we believe several will be marketed in Europe
and the US by 2015 (see Chapter 2). Moreover, we expect the pricing
to be significantly lower than for the original drugs.
Investors belief that it would be difficult to commercialize
antibody therapeutic biosimilars is based on two factors: (1)
regulatory guidelines do not currently exist and (2) manufacturing
costs are high. First, regulatory authorities in Japan, Europe, and
the US have not yet announced approval guidelines for antibody
therapeutic biosimilars. Accordingly, market watchers do not think
generic makers are willing to commit substantial resources to
development without knowing the requirements. Our research,
however, suggests generic companies have not been idly sitting on
the sidelines waiting for the regulatory authorities, but instead
are engaging them in ongoing consultations prior to the
establishment of guidelines. In effect, the regulatory authorities
are formulating guidelines with input from the generic drug
companies.
1 The 21 companies we visited are Alkem Laboratories, Aurobindo
Pharma [ARBP IN], Biocon [BIOS IN], Cadila Healthcare [CDH IN], Dr.
Reddys Laboratories [DRRD IN], Eisai Pharmaceuticals India Private,
GlaxoSmithKline Pharmaceuticals [GLXO IN], Glenmark Pharmaceuticals
[GNP IN], GVK Biosciences Private, Intas Biopharmaceuticals,
Jubilant Organosys [JOL IN], Jupiter Bioscience [JPO IN], Lupin
[LPC IN], Matrix Laboratories, Natco Pharma [NTCPH IN], Opto
Circuits India [OPTC IN], Ranbaxy Laboratories [RBXY IN], Strides
Arcolab [STR IN], Sun Pharmaceutical Industries [SUNP IN], Torrent
Pharmaceuticals [TRP IN], and Wanbury [WANB IN].
India-based generic drug makers are low-cost producers
Commercialization of antibody therapeutic biosimilars
Consultations ongoing prior to establishment of guidelines
-
Nomura Japanese Equity Research
6 Pharmaceuticals sector
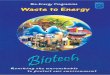
1-1. Drug categories including biologicals
Biological drugs Category (1) Small molecule drug (2) Protein
drug (3) Antibody therapeutic Molecular weight 100300 10,00030,000
About 150,000 Formulation Tablet, capsule, liquid formulation
Liquid formulation, freeze-dried Administration Oral, injection
Injection
Blopress Antihypertensives Insulin Antidiabetes drugs Remicade
Antirheumatism drug Lipitor Cholesterol-lowering drug Growth
hormone Dwarfism treatment Rituxan Anticancer Example drugs Aricept
Alzheimers disease EPO preparation Anemia drug Avastin
Anticancer
Manufacturing Chemical synthesis/partial fermentation
Fermentation/partial chemical synthesis Fermentation Clinical
trials Simple comparison Similar to those required for new drugs
Europe Proof of bioequivalence Development guidelines for
individual products Japan Proof of bioequivalence Development
guidelines for individual products (more stringent than Europe?) US
Proof of bioequivalence Simple review? Complete data similar to new
drugs?
(3) Antibody drug(fermentation)
(1) Sm all m olecule drug(chemical synthesis)
(2) Protein drug(fermentation)
Source: Nomura
Second, it is becoming increasingly possible to reduce
manufacturing costs. Biosimilars are produced through fermentation
using E. coli, yeast, and mammalian cells. Consequently,
manufacturing costs are exceptionally high because initial
investments, including fermentation tanks, can exceed 10bn.
However, technological advances have led to significant
improvements in production, with yields of the target substance
having risen from 20mg/liter in the 1980s, to 5g/liter more
recently. We estimate the current manufacturing cost for a
biosimilar at several thousand yen per gram. This is significantly
lower than the cost of branded antibody therapeutics, and we
therefore see ample scope for low-cost biosimilars.
The generic drug market has not expanded merely on the back of
greater supply, but has also benefited from increasing demand. The
business model for generic drug makers differs from that of branded
drug makers, which aggressively conduct marketing activities to
sell their drugs. We think the environment is positive for growth
of biosimilars as demand is there for suppliers as well as
users.
Inexpensive drugs are in demand throughout the world. Developed
markets need them to contain rising healthcare expenditures while
emerging markets require them to support the health of their
citizens amid economic expansion. Following the US healthcare
reform, all major developed markets now have health insurance
managed by government. Since medical expenditures are a major
component of the national budget, increases in healthcare spending
need to be kept in line with economic growth. Against the backdrop
of developed countries increasingly facing difficulties in
financing their high healthcare expenditures, low-cost
Manufacturing costs can be reduced
Business climate is conducive to suppliers and users
Universal health insurance spurs demand
-
Nomura Japanese Equity Research
Pharmaceuticals sector 7
biosimilars would be welcomed to replace expensive antibody
therapeutics, annual costs for which can run several million yen
per patient. Our review of data related to JCR Pharmaceuticals
[4552] EPO biosimilar (epoietin alpha BS Injection JCR), a
treatment for anemia, suggests the Ministry of Health, Labour and
Welfare (MHLW) is inclined to approve biosimilars. Approval of a
generic drug typically requires proof of bioequivalence, but
approval was granted in the case of epoietin alpha BS Injection JCR
based on proving equivalent efficacy. In fact the approval process
appears to have been surprisingly easy.
According to biopharmaceutical manufacturer Lonza Group [LONN
VX], biologicals going off patent in 200815 have a global market
value of US$59bn while generic drug maker Teva [TEVA US] estimates
patent expiries in 201620 are worth another US$23bn. Combined, this
represents a potential market for biosimilars by 2020 of around
US$80bn. Major patent expiries begin from 2012 and we estimate the
potential market for biosimilars will increase by around US$10bn
each year from that point. We further assume biosimilars will
capture about 50% of that market potential, thereby reducing global
pharmaceutical expenditures of 50trn by 500bn. The US market
accounts for about 80% of biological sales, and we therefore expect
biosimilars to reduce US pharmaceutical expenditures of 30trn by
about 400bn, representing an annual reduction of 1.3% on
pharmaceutical spending. Various measures to cut pharmaceutical
costs were adopted as part of the US healthcare reform and we think
these will slow pharmaceutical market growth to 5%.
Commercialization of biosimilars could further contribute to
reducing pharmaceutical expenditures.
Major US and European pharmaceutical manufacturers began forming
alliances with Indian generic drug makers from 2008. Initially, the
alliances centered on the supply of bulk for small molecule drugs
and consignment manufacturing, but more recent partnerships have
targeted biosimilars. India is already a source of low-cost drugs,
and tapping the Indian generic drug makers to become global
suppliers of low-cost drugs for chronic diseases could provide the
branded drug makers with a stable profit stream. Branded drug
companies, meanwhile, have been turning their attention to
high-risk, high-return drugs that address unmet medical needs like
oncology and central nervous system (CNS) diseases. Stable profits
generated by the drugs for chronic diseases could be used to fund
development of new drugs, thereby creating a well-balanced business
model (Exhibit 1-2).
1-2. Changing business structure of major US and European
pharmaceutical manufacturers
Previousmodel
Risk
Return
Combining results in
rebalancing
Unmet medical needs
Cheap drugs
Risk
Return
medium-risk, medium-return
high-risk, high-return
Low-risk, low-return
Cash f low source
Supports R&D
Source: Nomura
Antibody therapeutic biosimilars would help hold back rising
pharmaceutical expenditures
Indian companies key suppliers
-
Nomura Japanese Equity Research
8 Pharmaceuticals sector
Our top pick among Indian generic makers is Dr. Reddys
Laboratories. In addition to expanding its US business, the company
is a generic drug bulk supplier and is expanding into emerging
markets through an alliance with GlaxoSmithKline [GSK LN]. Next, we
like Jubilant Organosys, which has formed partnerships with major
branded drug makers like Eli Lilly [LLY US] and is providing both
R&D and manufacturing support.
Japanese companies are late in adapting to the structural
changes in the global market. Standouts are Daiichi Sankyo [4568],
which acquired Ranbaxy Laboratories and is expanding into emerging
markets, and Eisai, which is taking advantage of Vizaqs Indian
plant to sharply lower manufacturing costs of Alzheimers disease
treatment Aricept. In the biosimilar field, JCR Pharmaceuticals has
already commercialized an EPO (anemia drug) biosimilar while Nipro
[8086] is on track to become the second company to do so. EPO is an
essential drug for dialysis patients, who are increasing in number
by 10,000 every year, and there is a strong need for cheaper
alternatives. Mochida Pharmaceutical [4534] and Fuji Pharma [4554]
are jointly developing a granulocyte-colony stimulating factor
(G-CSF) biosimilar for the treatment of neutropenia while Shimadzu
[7701] is developing analysis equipment for biosimilar sugar
chains.
(2) Aging population drives up healthcare expenditures and
pharmaceutical costs Use of pharmaceuticals is expanding on the
back of demographic trendsie, the aging populations and higher
incidence of disease among the elderlyand will likely drive up
pharmaceutical costs. The rise is not limited to pharmaceutical
costs but also applies to total healthcare expenditures, which
include medical procedures. We used Japan as a model, because it is
at the vanguard of these demographic trends, and analyzed factors
that boosted healthcare expenditures in the past (Exhibit 1-3). We
concluded that the increase in the number of elderly over the age
of 65 was the single greatest factor boosting healthcare
expenditures. Japans government has attempted to lower healthcare
expenditures per capita through periodic medical fee revisions, but
total healthcare expenditures have continued to rise as the impact
of the growing population exceeded savings from healthcare cost
containment policies. In the past 15 years, the elderly population
has increased at an annual rate of 3.7%. The growth rate will
decline to 2.8% during 200510, 1.2% for 201015, and 0.3% for
201520, according to the National Institute of Population and
Social Security Researchs Future Population Projections for Japan.
If government policies to cut healthcare expenditures for the
elderly were maintained at 200005 levels, expenditures would not
stop increasing until 201015.
1-3. Healthcare expenditures for elderly linked to population
growth: analysis of growth factors (%)
National healthcare expenditures Healthcare expenditures for
elderly CY Total Per capita Population Total Per capita Population
GDP
Social security costs
9095 4.00 3.68 0.31 5.80 1.60 4.14 1.96 6.51 9500 1.70 1.48 0.22
3.87 0.05 3.81 0.26 3.83 0005 0.97 0.83 0.14 2.21 -0.92 3.17 -0.04
2.36 0510E - - -0.30 - - 2.80 - - 1015E - - -0.40 - - 1.20 - -
1520E - - -0.60 - - 0.30 - - Note: Data from 2005 are compiled from
National Institute of Population and Social Security Researchs
Future Population Projections for Japan (December 2006). Source:
Nomura
Investment points for key Indian companies
Investment points for key Japanese companies
Aging population is driving up healthcare expenditures
-
Nomura Japanese Equity Research
Pharmaceuticals sector 9
The incidence of disease rises with age, and thus it is easy to
imagine rising healthcare cost per capita. In analyzing Japanese
demographic trends, we confirmed that longer life spans translated
into higher per capita healthcare costs (Exhibit 1-4). Although
Japan is the leader in the aging population, the trend will become
increasingly pronounced next in Europe and then the US.
Accordingly, Europe and the US will likely next experience sharply
expanding healthcare expenditures. Even France and Spain, which
have had relatively lax policies on healthcare expenditures
compared to other European countries, enacted full-scale
cost-containment initiatives from May 2010. The US just passed
healthcare reform and will have to aggressively implement
cost-cutting measures. It is generally believed that the goal of
social security is to promote and maintain the health of the
citizenry. However, maintaining health of the elderly would drive
up healthcare costs, thereby impeding economic expansion, and
ultimately proving counter-productive. We expect to see an
increased focus on curbing pharmaceutical costs.
1-4. Healthcare costs rose sharply in line with increase in life
span
Age
Healthcare costs
Increased costs
Advancement of aging
Source: Nomura, based on data from Professor Ogawa et al at
Nihon University
(3) Inexpensive drugs needed for all fields Given the structural
changes underway worldwide, we see little prospect of growth for
pharmaceutical markets in developed countries. The major countries
have universal health insurance systems similar to Japans and
therefore a large portion of the cost for pharmaceuticals is borne
by national coffers. Substantial economic growth is unlikely in the
developed countries, and thus healthcare cost-containment measures
will probably be necessary. Consequently, pharmaceutical
expendituresa subset of overall healthcare expendituresare unlikely
to expand, and we expect net zero growth in developed
countries.
Aging populations are boosting the volume of drug use in
developed countries, but the size of pharmaceutical markets is
being regulated because of strained national finances. It is
therefore essential to bring down unit drug costs. We conclude that
downward pressure on unit prices for drugs will continue so long as
this demographic trend persists.
Major developed countries advancing healthcare cost containment
policies
Zero growth for pharmaceutical markets in developed
countries
Pharmaceutical prices need to decline
-
Nomura Japanese Equity Research
10 Pharmaceuticals sector
A natural result of aging populations will likely be an increase
in patients suffering from cancer, CNS diseases like Alzheimers
disease, and immune disorders like rheumatoid arthritis. However,
given that there are few truly effective treatments for these
diseases at present, there is substantial potential demand. In the
case of Alzheimers disease, assuming it manifests at age 65,
treatment would likely continue for 10 years at most. If a more
effective treatment emerged, priority would be on concurrent use
with existing drugs to improve efficacy. We expect the market for
drugs addressing unmet medical needs to continue expanding.
In contrast, existing treatments for chronic diseases like
hypertension, hyperlipidemia, and diabetes are already highly
effective. Therefore, the market need is not for new drugs but
rather cheaper ones. Assuming diabetes manifests at age 40,
pharmaceutical treatment would likely continue for 35 years based
on Japans life expectancy. In addition, patients of chronic
diseases often suffer from additional circulatory diseaseseg, about
half of hyperlipidemia patients also have hypertension. The need
for cheaper drugs is substantial given the high volume of demand
and the long period of treatment. Caduet, a pill that combines
amlodin (hypertension drug) and atorvastatin (hyperlipidemia
treatment), was marketed domestically in July 2009 targeting
patients that suffer from both diseases.
We assume pharmaceuticals will overall be nearly a zero-sum
market, but expect sales for drugs targeting unmet medical needs to
expand while sales of chronic disease treatments contract. It would
be difficult to restrict expansion in pharmaceutical volume usage,
leading to a drop in unit prices. Accordingly, we think generics
will become the drug of first choice. In fact, US prescriptions for
cholesterol-lowering drug Lipitor have continued to decline prior
to the patent expiry and there has been a similar trend for
diabetes drug Actos. Even if a new drug for chronic diseases is
commercialized, it has to compete with generic versions of similar
drugs. Accordingly, new drug sales are unlikely to expand on the
scale at which they did in the past.
1-5. Market for drugs treating unmet medical needs likely to
expand while generics likely to become drug of choice for chronic
diseases
Current FutureMarket s ize not expected to grow
Generic drugs
Immune diseasetreatments
Others Anticancer agents
CNS drugsGenerics
HypertensivesAntidiabetics
Cholestero l-loweringdrugs
Others
Source: Nomura
Low-cost drugs in developed markets are crucial to maintaining
health in emerging markets. Makers that supply low-cost drugs to
emerging markets are contributing to their economic expansion as
the health and well being of workers in emerging markets is crucial
to the continued economic success. This is similar to Japan during
its economic expansion in the 1960s and 1970s. As the economy
expands, per capita GDP rises and so does healthcare expenditures
per capita (Exhibits 1-6, 1-7). The use of generic drugs could lead
to a shift to the same brand drugs used in Europe and the US.
Changing structure of drug use (1): expanding market for drugs
that address unmet medical needs
Changing structure of drug use (2): generic drugs will likely be
first-choice treatment for chronic diseases
Market share rules are changing
Inexpensive drugs widely used even in emerging markets
-
Nomura Japanese Equity Research
Pharmaceuticals sector 11
1-6. Expanding pharmaceuticals in emerging markets
Em erging m arkets w ill outgrow developed markets"Annual
pharmaceutical sales in emerging markets is expected to reach
$400bn by 2020,
equivalent to current sales in the US and the f ive major
European markets combined."
Turkey: $52bn
Korea: $66bnMexico: $60bnRussia: $38bnBrazil: $60bnIndia:
$40bn
China: $82bn
Emergingmarkets
$55bn
2006 2020 (see note) (CY)
Assuming2% grow th
per yearUS$364.18bn
Eur 5$162.3bn
Eur 5$123bn
US$276bn
Note: Extrapolations from 2006 to 2020 based on IMS projection
and % of 2006 sales. Source: IMS MIDAS 2006 sales data, Total
Pharmaceutical Market
1-7. Healthcare expenditures rise in tandem with economic
growth
0
1,000
2,000
3,000
4,000
0 10,000 20,000 30,000 40,000 50,000
Turkey
Mexico
Brazil
IndiaChina
Spain Italy
Germany
UK
US
Japan
8,000
7,000
Per capita GDP ($)
Per capita healthcare expenditures ($)
France
Russia
Source: Nomura
(4) US/European branded drug makers change business model At
their 2008 annual meetings, Pfizer [PFE US] and Merck [MRK US] both
announced plans to expand into the generic drug business, including
biosimilars, marking a substantial change in their business models.
Thereafter, US and European branded drug makers formed alliances
with Indian generic drug makers, in an effort to develop a business
structure that supports low-cost drugs. The flurry of major patent
expiries in the 2000s that depressed earnings prompted the business
model change. The branded drug makers attempted to sustain profit
growth
Turning point from 2008
-
Nomura Japanese Equity Research
12 Pharmaceuticals sector
through external measures such as M&A but were unable to
offset the negative impact of successive major patent expiries.
The US and European pharmaceutical manufacturers new business
model centered on a necessary shift from the previous medium-risk,
medium-return model to one focused on high risk and high return
that targeted drugs to treat unmet medical needs. The strategy was
unsuccessful because of repeated delays to new drug approvals. As a
result, the branded drug makers needed a business that could
generate stable cash flow. Supplying low-cost drugs to emerging
markets and the generic drug business became the necessary stable
cash cow businesses. The low-risk, low-return generic drug business
generated stable cash flow to fund R&D for the high-risk,
high-return new drug business. The combination of the low-risk,
low-return stable businesses and high-risk, high-return new drugs
businesses resulted in a net overall medium-risk, medium-return
model, basically unchanged from before (Exhibit 1-2). Even now, US
and European pharmaceutical majors are aggressively forming
partnerships with Indian generic drug makers (Exhibit 1-8).
1-8. Alliances between Indian makers and US/European branded
drug majors
Main company Partner company Type Details Dr. Reddys Partnership
Development and marketing of specific drugs in emerging markets
Daiichi Sankyo Partnership Joint marketing of hypertensive
Olmesartan Eisai Partnership Production, distribution, marketing of
antiulcer drug Parit
GSK India
Astellas Partnership Exclusive rights to antifungal Maycamine in
Indian market Shantha Biotechnics Acquisition Vaccine business
Sanofi Aventis Glenmark Partnership Development and marketing of
chronic pain treatment Aurobindo Partnership Licensing out of solid
dosage business
Pfizer India Johnson & Johnson Sale Four healthcare
products
Abbott Zydus Cadila Partnership Marketing of 24 Abbott products
in 15 emerging markets Biocon Partnership Biologicals Forest
Partnership Development, distribution, and marketing of
hypertensive Bystolic Mylan Natco Partnership Global supply of
copaxone Bayer Acquisition Bayers French generic drug business
Taisho Acquisition Japanese generic drug maker Pfizer Acquisition
Pfizers Italian generic drug business Kowa Partnership Joint
venture with Kowa Shinyaku Aventis Partnership Marketing copaxone
in North America Lundbeck Partnership Developing copaxone in Europe
Lonza Partnership Development, production, and marketing of
biologicals UCB Partnership Joint marketing of ProAirRHFA inhalant
in US Abbott Partnership Licensing of TriCor
Teva
Hospira Sale Global rights to G-CSF biosimilar Source:
Nomura
(5) Indian generic drug makers targeting biosimilars Indian
generic drug makers market branded generics domestically and
standard generics in Europe and the US. Branded drug makers have
formed alliances with Indian generic drug makers on the back of the
performance of their US/European businesses. The branded
pharmaceutical majors are changing their business model by having
Indian makers produce and supply drugs globally. Indian generic
makers have ramped up production to generate scale merits, thereby
providing cheaper drugs. One line in Aurobindos state-of-the-art
plant can produce 700mn tablets monthly (8.4bn annually). If the
plant site were fully utilized, annual production would reach 126bn
tablets. In comparison, Japanese major generic drug maker Sawai
Pharmaceutical [4555] produced a total of only 4.2bn tablets in
10/3 and its medium-term business plan calls for boosting this to
6bn by 12/3.
Overall risk-return balance of branded drug makers has not
changed
Supplying drugs to US/European pharmaceutical manufacturers
-
Nomura Japanese Equity Research
Pharmaceuticals sector 13
Given the limited disclosure by companies, we estimated the
Indian generic drug makers manufacturing costs by using publicly
available information. In Japan, we used Towa Pharmaceutical [4553]
and Sawai Pharmaceuticals Schedule of Cost of Goods Manufactured.
We base our figures for Indian generic makers on feedback from
management interviews. We concluded that manufacturing costs of
Indian generic drug makers were one-seventh those of Japanese
makers. Specifically, wages were one-tenth, material costs were
one-fifth, and business expenses were one-twentieth. Materials
represent the largest cost factor and there appears to be scope for
additional reductions by the Indian makers. The cost of receptacles
is significantly higher in Japan. For example, glass vials used for
injectable drugs in Japan are much more expensive owing to higher
domestic standards. Tablet packaging is also much cheaper in India,
as Japanese tablets use a backing comprised of several aluminum
sheet layers compared to only a single layer in India. This
accounts for only a few yen but substantially bolsters the profit
margins of Indian generic drug makers. Our initial impression
following company interviews was that the Indian makers
manufacturing costs were one-fifth those of the Japanese generic
drug makers, but our estimates suggests these are even lower. We
based our sales estimates for Indian makers on the drug price
listing (Current Index of Medical Specialties) and sales were about
one-tenth those of the Japanese counterparts.
1-9. Indian makers manufacturing costs are substantially
lower
Japanese companies
Towa Pharmaceutical Sawai
Pharmaceutical Average Indian
companies Change
% Sales 100.0 100.0 100.0 10.0 90 Cost of manufacturing 50.0
60.0 55.0 8.2 85 Labor expenses 11.5 8.4 10.0 1.0 90 Raw material
costs 29.0 37.2 33.1 6.6 80 Other expenses 10.0 14.4 12.2 0.6 95
Gross profits 50.0 40.0 45.0 1.8 96 Source: Nomura
The drugs referenced above are small molecule drugs with
molecular weights of around 300, but Indian generic drug makers
have expanded their efforts to include follow-on biologics or
biosimilars. There are two categories of biosimilars: protein drugs
with molecular weights of around 10,00030,000 and antibody
therapeutics with a molecular weight of around 150,000. The Indian
generic makers are targeting both categories. We cover details in
chapter 2, but the European regulatory authorities have released
review guidelines for biosimilars and already approved a protein
drug biosimilar. No antibody therapeutic biosimilar has been
approved yet. In India, Dr. Reddys Laboratories launched a
biosimilar of anticancer agent Rituxan under the name of Reditux in
April 2007 and posted 2009 sales of INR199mn (US$4mn, +29% y-y).
Although not a biosimilar, Biocons BIOMAb EGFR (generic name:
nimotuzumab) was marketed from July 2006. BIOMAb EGFR was
originally discovered by YM Biosciences [YM CN] and is already
commercialized in Cuba for the treatment of head and neck cancer.
Daiichi Sankyo is currently conducting domestic Phase 2 clinical
trials.
The business model adopted by Indian generic makers, with its
focus on establishing a value chain, is superior to that of its
Japanese counterparts. The biggest difference is that Indian
generic makers have a vertically integrated business model and
manufacture their own pharmaceutical bulk. In contrast, Japanese
makers are geared for small-lot diversified production and are
unable to manufacture pharmaceutical bulk in-house. We think Indian
generic drug makers are far better positioned to reduce
manufacturing costs on the back of
Indian manufacturing costs are one-seventh those of Japan
Entry into biosimilar market
Indian generic makers have superior business model
-
Nomura Japanese Equity Research
14 Pharmaceuticals sector
scale merits. Indian generic makers also stand out for their
success in concurrently operating domestic and overseas (Europe and
the US) businesses.
1-10. Japanese generic makers: unable to apply vertically
integrated business model
Type Branded drug Generics Company origin Japan/US/Europe India
Japan Region Japan/US/Europe India Overseas Japan Overseas R&D
~ { { x Bulk production { { { x x Formulation { { { { x Marketing ~
{ { { x Source: Nomura
Indian generic drug makers are advancing into development of
brand drugs, but we are skeptical of their prospects of
successfully making the shift to innovators because (1) they lack
sufficient financial clout and (2) the commercial value of drug
candidates is limited. We think the issue of finances could be
resolved eventually but not in the near future, given that it costs
at least about 50bn (US$500mn) to develop a brand name drug. The
annual R&D budget for most major generic drug makers stands at
about 10bn (US$100mn), making it exceedingly difficult to develop a
drug in the US (the worlds biggest market). Moreover, even if
development were successful, marketing costs in the US and Europe
would likely run at least 20bn (US$200mn). Japanese branded drug
makers started marketing new drugs in the US from the late 1990s
and formed marketing alliances with US partners to minimize sales
promotion costs. Despite this, they ran deficits of around 10bn for
the first several years. A loss of this level would wipe out all
term profits of the Indian generic drug makers. We conclude it will
be some time before return on invested capital will improve
sufficiently. As for the commercial value of branded drug
candidates, the main problem we see is that the candidates have the
same mechanism of action as drugs from 10 years ago, making
differentiation difficult. In India and Europe, many of the generic
drug makers are developing diabetes drugs like peroxisome
proliferator-activated receptor (PPAR) inhibitors, for which there
are concerns over potential liver damage, and dipeptidyl
peptidase-4 (DPP-4) inhibitors, for which large-scale clinical
trials are required because circulatory-related side effects have
been confirmed. The Food and Drug Administration (FDA) issued
stringent review guidelines for diabetes drugs in December 2008
that required additional Phase 3 clinical trials even for Takeda
Pharmaceuticals [4502] SYR-322, which had demonstrated exceedingly
high safety results in animal studies. Considering global trends,
we think the production of generic drugs for US and European
companies will be a successful business model for the Indian
generic drug makers, but are skeptical regarding the profit
potential of them marketing branded drugs in India and Europe.
Expansion into branded drug business would be difficult
-
Nomura Japanese Equity Research
Pharmaceuticals sector 15
1-11. Drug pipelines of Indian generic drug companies Company
Molecule name Indication Target Clinical trial phase
Crofelemer (inlicensed) Antidiarrhoeal CTFR inhibitor Phase 3
GRC 3886 (oglemilast) Asthma, COPD PDE IV inhibitor Phase 2 GRC
8200 (melogliptin) Diabetes mellitus (Type II) DPP IV inhibitor
Phase 2 GRC 4039 (revamilat) Rheumatoid arthritis, MS inhibitor PDE
IV Phase 1 GRC 10693 Neuropathic pain, osteoarthritis CB-2 Phase 1
GRC 500 MS, inflammatory diseases VLA-2 antagonist Phase 1 GRC
15300 Osteoarthritic pain, neuropathic pain, and skin disorders
TRPV3 antagonist Preclinical GBR 600 Antiplatelet, adjunct to
PCI/acute coronary syndrome Von Willebrand factor Preclinical
Glenmark
GRC 6211 Osteoarthritic pain, neuropathic pain, and urinary
incontinence TRPV 1 antagonist Phase 1
ZYH1 Dyslipidemia PPAR alpha:gamma Phase 3 ZYO1 Obesity,
diabetes CB-1 antagonist Phase 1 ZYI1 Pain Multi-modal Phase 2 ZYH2
Diabetes PPAR alpha:gamma Phase 1 ZYH7 Dyslipidemia PPAR alpha
Phase 1 ZYT1 Dyslipidemia Undisclosed Phase 1
Zydus Cadila
ZYD1 Dyslipidemia GLP-1 Phase 1 Oral insulin Diabetes - Phase 2
Anti-CD6 Oncology/inflammation/autoimmune - Phase 3 Targeted
immunoconjugates Oncology - Discovery Anti-CD20 Oncology -
Preclinical Peptide hybrid Diabetes - Discovery Anti-EGFR Oncology
- Market Biosimilar MAbs Oncology/immunology - Preclinical Insulin
analogs - lispro, aspart Diabetes - Preclinical Rh-insulin,
glargine Diabetes - Market
Biocon
GCSF, EPO Oncology - Market Reditux Non-Hodkins lymphoma
Monoclonal antibody Market DRF 2593 (balaglitazone) Metabolic
disorders (partnership with Rheoscience) - Phase 3 DRL 17822
Metabolic disorders/CVS (partnership with Argenta) - Phase 1 Dr
Reddy's
Several compounds Respiratory disorders (dyslipidemia and
atherosclerosis) - Phase 1 Ranbaxy P. falciparum combination
Malaria - Phase 3
LLL 2011 (amigra) Antimigraine, herbal - Phase 3 LL 4218
(desoside-P) Antipsoriasis - Phase 2 LL 3858 (sudoterb) Anti-TB -
Phase 2 LL 3348 (sesoris) Antipsoriasis, herbal - Phase 2
Unspecified Type II diabetes - Preclinical
Lupin
Unspecified Rheumatoid arthritis - Preclinical P276 - CDKs Head
& neck cancer, multiple myeloma - Phase 2 P276 - gemcitabine
combination Pancreatic cancer - Phase 1 P276 - tadiation
combination Head & neck cancer - Phase 1 P1446 - CDKs
Unspecified - Phase 1 NPB-001-05-Bcr-Abl Chronic myeloid leukemia -
Phase 2 NPS31807 - TNF alpha Rheumatoid arthritis and psoriasis -
Phase 2 P979 - TNF alpha Inflammation - Preclinical P1736-non-PPAR
gamma Diabetes and metabolic disorders - Phase 1 P1201 - Lilly
Diabetes and metabolic disorders - Phase 1 P2202 - Lilly Diabetes
and metabolic disorders - Phase 1
Piramal Lifesciences
NPH30907 Dermaphytotypes - Phase 2 Source: Nomura
(6) Japanese generic drug makers limited to domestic market
Japanese regulatory authorities, keen to reduce pharmaceutical
costs, have been promoting use of cheaper generic drugs. The MHLW
has set a generic drug ratio (volume basis) target of 30% by FY12,
which would require a 1.5-fold increase in the market from the 2009
ratio of 20%, or annual average growth of 14%. This would translate
into additional sales of more than 20bn and would largely be
dependent on sharp increases in production by the three generic
drug majors. These three companies control a market share of about
50%, and thus achieving the government target based solely on
increased sales by them would require nearly a doubling in
production. However, production capacity is limited to 1.5x current
levels, thereby putting the government target for all purposes
beyond reach. If production were boosted on par with the current
maximum capacity, we estimate that it would result in a generic
drug ratio
Government FY12 target of 30% generic drug ratio seems
unrealistic
-
Nomura Japanese Equity Research
16 Pharmaceuticals sector
of 25%. The government is likely to revise its generic drug
ratio target to 25% in the near future, citing the aforementioned
points.
New incentives were adopted to further promote the use of
generic drugs. Under the previous system, pharmacies were awarded a
40 incentive for each prescription that included at least one
generic drug. To be eligible for the generic drug dispensing
premium, pharmacies had to maintain a generic dispensing ratio of
30% or higher on a prescription basis. Effective from April 2010,
the eligibility requirement for the generic drug-dispensing premium
was changed to a three-tier system based on the volume of drugs
dispensed rather than the number of prescriptions. When the generic
drug dispensing ratio exceeds 20%, 25%, and 30%, the respective
premium is 60, 130, and 170. The generic drug makers sales growth
in April and May substantially exceeded the industry average,
suggesting that government stimulatory measures were
successful.
Japanese generic makers rely almost completely on the domestic
market, in contrast to Indian generic drug makers, which have
successfully expanded abroad. The low diffusion rate of generic
drugs in Japan was one factor responsible for the significantly
weaker profit bases of generic drug makers relative to their Indian
counterparts, and a factor that prevented them from expanding
overseas. We are optimistic on the growth prospects of the domestic
generic drug makers but expect cash flow to be primarily channeled
into investment to boost production capacity.
In contrast, overseas companies have successively expanded into
the Japan market (Exhibit 1-12), although sales have fallen short
of initial expectations in most cases. One reason for the limited
success of foreign generic drug makers in Japan is the difficulty
in competing with the exceedingly high quality of Japanese
products. This same high quality is likely responsible for Japanese
generic drug makers low profitability. We think a much more
attractive business model would be the generic drug bulk business,
which commonly maintains operating margins of around 30%.
1-12. New entrants to Japanese generic drug market: foreign and
nonpharmaceutical companies
Date Company Partner company Details
Jan Novartis (Switzerland) Sandoz (Germany) Nippon Hexal Sandoz
parent company, Novartis, acquired Hexal. Marketed Japans first
generic recombinant biopharmaceutical in Sep 2009; aims to launch
more than 10 new generic drugs annually
Mar Hospira (US) Taiyo Yakuhin Established Japanese corporation
and partnered with Taiyo Yakuhin to develop injectable generics
2006
Apr Orchid Chemicals & Pharmaceuticals (India) - Established
Japanese corporation
Apr Zydus (India) Nippon Universal Pharmaceutical (renamed Zydus
Pharma Japan in June 2010)
Zydus established Japanese corporation in Sep 2006 and acquired
Nippon Universal Pharmaceutical in April 2007 2007
Oct Lupin (India) Kyowa Pharmaceutical Industry Lupin acquired
Kyowa Pharmaceutical Industry
Feb Mylan (US) Merck Mylan acquired Mercks generic drug
business, including operations in Japan Torrent (India) -
Established Japanese corporation (stopped operation Apr 2008)
2008
Apr Ranbaxy (India) Daiichi Sankyo (acquirer) Daiichi Sankyo
acquired Ranbaxy, making it a subsidiary; collaborating in
development
Jan Teva (Israel) Kowa Established joint venture (Teva
established Japanese corporation in 2005), sales start from 2010
Apr Actavis (Iceland) Aska Pharmaceutical Established joint
venture
GlaxoSmithKline (UK) JCR Pharmaceuticals Concluded comprehensive
alliance for biosimilars; GSK became JCR Pharmaceuticals top
shareholder from Mar 2010 2009
Dec Pfizer (US) - Inaugurated Japanese corporation specialty
organization, sales targeted from 2011
Jan PharmaForce (US) Daiichi Sankyo Daiichi Sankyo subsidiary,
Luitpold Pharmaceuticals, acquired injectable generic maker
PharmaForce (Ohio) 2010
May Sanofi Aventis (France) Nichi-Iko Pharmaceutical Established
joint venture, joint development of biosimilars Source: Nomura
April 2010 incentives to dispensing pharmacies is proving
effective
Japanese generic makers almost completely dependent on domestic
market
Overseas competitors continue to enter domestic market
-
Nomura Japanese Equity Research
Pharmaceuticals sector 17
We think generic drugs will eventually replace long-term listed
drugs. Policies to expand the domestic generic drug market have
focused on boosting demand instead of supply. Currently, the
preferred cheaper alternative of physicians and patients is
long-term listed drugs instead of generics. Sanofi-Aventis [SAN FP]
recently announced an alliance with Nichi-Iko Pharmaceutical [4541]
that not only expands the generic drug business but also transfers
marketing of long-term listed drugs in Japan. The government focus
over the near to medium term will likely remain on promoting use of
generic drugs; however, over the longer term, we expect the
emphasis to shift to reducing long-term listed drug prices.
Accordingly, we think long-term listed drugs will be the key to
generic drug makers continued sustainability. When we queried top
management of generic drug companies as to whether branded drug
makers would be more likely to transfer marketing of long-term
listed drugs to domestic or foreign generic drug makers, most
replied that domestic drug makers would be the preferred
distributor. We think branded drug makers are likely to
increasingly transfer production and marketing of low-price,
long-term listed drugs.
1-13. Reorganization of long-term listed drug business
Majorpharma
Branded drug
Long-term listed drug
Medium-tierpharma
GE
GE subsidiary
GEMajor
pharmaMedium-tier
pharma
Note: GE = generic drugs Source: Nomura
The high level of quality required for drugs in Japan makes it
unlikely that generic drugs manufactured by Indian companies will
make substantial inroads in Japan. On the flip side, if
high-quality drugs could be made very inexpensively, they could
easily be sold worldwide. This combination of high quality and low
cost applied to biosimilars could mark the path of sharp growth for
the Japanese generic drug makers. Mass production and supply of the
worlds highest-quality biosimilar bulk to Europe and the US would
be an attractive business model for any Japanese drug maker. We
think a promising business model would be for European/US
biosimilars to be introduced to Japan, with Japanese generic drug
makers being in charge of production.
(7) A return to small molecule drug business model over the long
term Major Japanese companies are focusing on the development of
antibody drugs, but their European and US counterparts have been
changing their areas of development with a view to business
expansion beyond antibody therapeutics. A typical example of this
can be found in the 2007 annual report of Genentech (acquired by
Roche [ROG VX] in 2009). The CEO at the time, Arthur D. Levinson,
PhD, said that the company was developing small molecule drugs
as
Focus on long-term listed drugs
Global suppliers of generic drug bulk
Development of small molecule drugs is gathering momentum
again
-
Nomura Japanese Equity Research
18 Pharmaceuticals sector
its development approach to anticancer agents. Even those
companies that have specialized in antibody drugs had set their
sights on developing small molecule drugs, which suppress the
communications system involved in cell growth. Antibody drugs are
effective but cannot be made more inexpensively than small molecule
drugs with lower costs, and moreover cannot be formulated as oral
drugs. We think development of small molecule drugs, which can
easily be made inexpensively and as oral formulations, will gain
momentum as it becomes clearer how the drugs work inside
organisms.
Previously, small molecule drugs targeted receptors serving as
barriers between the cell interior and exterior. It was easy to get
results with these drugs by opening and closing the receptors,
which serve as barriers, and since the receptors are located on the
cell surface, it was easy to find new receptors that could be
targeted by drug development. It is now easy to detect small
amounts of proteins, making it possible to target drug development
efforts on cells internal communication systems, which represent
the downstream function in cell growth. Specifically, Novartiss
[NOVN VX] Affinitor is a new type of anti-cancer agent. The drug
impedes the action of mTOR, which has a central role in cell
growth, and is highly effective in renal cancer, for which there
was previously a lack of effective treatments. Another drug we
would highlight in this context is ArQules [ARQL US] ARQ 197 (c-MET
inhibitor), which is currently in the development stage. Daiichi
Sankyo has signed a joint development agreement with ArQule for
overseas markets, while Kyowa Hakko Kirin [4151] is in charge of
development in Japan.
1-14. Development of small molecule anticancer agents attacking
from within the cell is proceeding apace
Active sites to date
Cell growth, infiltration, transfer, and apoptosis
prevention
Pho
spro
ylat
ion
cas
cade
Grb2SOS
STAT SRC
kina
se
III
III
mTOP
P
AKTP
P
kina
se
I
IIIII
P Pp11 p85
PI3K
EGF EGF
Pho
spro
ylat
ion
cas
cade
RAS RAS
MAP PP
RAFP
P
MEKP
P
Receptor-typetyrosine kinase
Nonreceptor typetyrosine kinase
Nonreceptor typetyrosine kinase
(1) PI3K pathway (2) MAPK pathway
1. Receptors2. Receptor-type tyrosine kinase
3. Nonreceptor type tyrosine kinase
IV IV
GDP GTP
Active sites from now on
Source: Nomura
Now that drug development previously at the research lab stage
has reached the market, companies need business strategies to take
them beyond antibody therapeutics. We think there will be more
examples of strategies where conditions previously treated with
antibody drugs are covered by small molecules that are cheaper but
have the same results. Although the examples below are not of
changes from antibody drugs to oral ones, they do show shifts from
injected drugs to oral drugs. For multiple sclerosis, we think the
oral Gilenia will take over from injected interferon beta as the
main treatment. Aside from requiring injections, interferon
The shift from receptor to intracellular action
Turning to a business model that looks ahead
-
Nomura Japanese Equity Research
Pharmaceuticals sector 19
beta also costs several million yen per year. Gilenia, however,
can be taken orally without significant disruption to daily life
and it costs only some tens of thousands of yen. The new drug is
still in the approval process in the US, but on 10 June an FDA
advisory panel recommended approval, making it likely that the drug
could reach the US market by end-2010. It is unusual for companies
to shift their focus from one antibody drug to another antibody
drug, as with the switch from Remicade (antirheumatic) to Simponi
(antirheumatic) in the strategy adopted by Johnson & Johnson
[JNJ US].
Turning our attention to the different models in advanced
countries and emerging countries, we think small molecule drugs
will rapidly expand in advanced countries while antibody
biosimilars become more widespread. In emerging countries,
meanwhile, generics are likely to be used increasingly for
currently mainstream receptor-type small molecule drugs, while in
antibody therapeutics, biosimilars become more widespread and the
original branded drug market shows no growth. Longer term, we think
intracellular small molecule drugs will penetrate the market as
branded drugs in tandem with the development of emerging economies.
However, the companies supplying these drugs are likely to be
European and US branded drug manufacturers, rather than their
Indian or Chinese counterparts.
1-15. A return to small molecule drugs over the long term
(1) Small molecule drugs(Receptor-type)
(2) Antibody therapeutics
(3) Small molecule drugs(intracellular-type)
Sales
(1)
(2)(3)
10 15 20 25
Sales
(CY)
Advanced countries Emerging countries
Generics (1)'
Biosimilars (2)'
Branded drugs (3)
10 15 20 25 (CY)10 15 20 25
(CY)
Sales
Source: Nomura
-
Nomura Japanese Equity Research
20 Pharmaceuticals sector
2. Indian pharmaceutical industry The Indian pharmaceutical
industry is currently going through a transitional phase in which
it is being transformed from a supplier of inexpensive generic
drugs globally into a hub for adding immense value to new drug
R&D. Our analysis broadly highlights two key factors that have
modified the rules of the game for the Indian pharmaceutical
industry. These factors are:
Intellectual property rights
Evolving business models
(1) Intellectual property rights in India The Indian Patents Act
of 1970 made pharmaceutical product innovations unpatentable in
India and granted patents to production processes. This allowed
Indian drug companies to reverse engineer molecules to produce
generic versions of patented drugs. While this weakened
intellectual property right (IPR) protection in the country, the
Indian pharmaceutical industry flourished and rapidly increased its
global footprint.
Patents (Amendment) Act, 2005
The Indian Patents Act of 1970 was amended in 2005 in order to
align Indian IPRs with the WTOs TRIPS Agreement and product patents
were reintroduced. The major changes included the following:
Retrospective effect of the patent regime: The patent regime was
introduced with retrospect effect from 1995, ie, any new drugs
patented after 1995 would receive protection. However, generic
entry was made possible for drugs for which patent applications had
been filed but patents had not yet been granted over 19952005.
Furthermore, companies manufacturing these drugs were allowed to
continue their manufacture even after the granting of the patent,
with a reasonable royalty payment to the patentee.
Minor innovations made not patentable: More importantly,
according to the Indian Patents Act, patentability scope is limited
because minor innovations are not patentable. Minor innovations are
defined under the following categories: salts, esthers, ethers,
polymorphs, metabolites, pure form, particle size, isomers,
mixtures of isomers, complexes, combinations, and other derivatives
of known substances. Unless they differ significantly in properties
with regard to efficiency, these products will not be granted
patents.
Pre-grant opposition and post-grant opposition: India has a
distinct pre-grant and post-grant opposition process in place
primarily to empower the patent office, reduce the incidence of
patent litigation, and discourage evergreening and filing of minor
innovations. According to the act, pre-grant oppositions have to be
initiated within six months of publication of the patent
application. A post-grant opposition has to be initiated within a
year of the date of publication of the patent grant.
We believe that in India, the scope of patentability definition
is a bigger hurdle, rather than regulatory support or the interests
of big pharmaceutical companies, in realizing the potential of
patented drugs. In fact, a majority of the pre-grant and post-grant
oppositions for pharmaceutical products fall in the category of
secondary/minor innovations. Note that unlike revocation
proceedings, pre-grant opposition filings are relatively
inexpensive and take place with the patent office. In addition, any
party/person can file a pre-grant opposition.
Indian pharmaceutical industry is in transitional phase
currently
Process patents weakened intellectual property rights in
India
Patent law amended to align with WTOs TRIPS Agreement
-
Nomura Japanese Equity Research
Pharmaceuticals sector 21
Pre-grant opposition
Some of the pre-grant opposition filers among Indian companies
include Ranbaxy, Cipla [CIPLA IN], USV, and Torrent
Pharmaceuticals. Furthermore, various patient groups and
nongovernmental organizations (NGOs) have also been among pre-grant
opposition filers, primarily in the categories of HIV- and
oncology-related drugs. Some instances of pre-grant oppositions
include: (1) AstraZenecas [AZN LN] patent application for
omeprazole and one of its enantiomers was rejected following a
pre-grant application by Torrent Pharmaceuticals; (2) Novartiss
application for an invention pertaining to crystalline ascomycin
derivatives was rejected (opposition filed by Ranbaxy) because
there was no inventive step in preparing the crystalline form from
the amorphous form; and (3) in Boehringer Ingelheims application
for powder medicament for inhalation, comprising tiotropium salt
and salmeterol xinafoate, the controller general of patents,
designs, and trademarks (controller) rejected opposition grounds of
combination without any synergistic effects. However, the
controller rejected the patent application on the grounds of no
enhancement in efficiency compared with earlier known inhalable
powder formulations containing the same active ingredients. The
opposition was filed by Cipla.
Indias 2005 Patents (Amendment) Act was a game-changer in an
industry that had prospered under protection provided by the
erstwhile Patent Act. Post-2005, Indian companies were compelled to
rethink, realign, and remodel their businesses in order to compete
in the new regulatory framework. One direct effect of the new law
was an increase in R&D spending by the Indian generic drug
companies, which increased from a paltry average of about 2% of
sales in the 1990s to almost 7% in 2010. Although this increase may
not seem large enough at first glance, it underlines a clear shift
in the overall strategy of Indian pharmaceutical companies as they
learned that innovation was the way forward. Many companies, such
as Piramal Healthcare [PIHC IN] and Sun Pharma, separated their
R&D from their generics divisions in order to create a clear
bifurcation between the two businesses. This dual strategy model
was perhaps the first step in the transformation process that the
Indian pharmaceutical industry is currently undergoing.
(2) Evolving business models Domestic market focus
The Indian pharmaceutical market is pegged at roughly $8bn,
having grown at more than 10% a year over the last decade. The
domestic market is likely to grow at 1214% a year for next few
years on account of three main factors. The first is increased
healthcare spending by the government. Currently, the Indian
governments spending on healthcare is around 3.5% of its overall
spending, compared with roughly 10% in other emerging markets. The
second is higher penetration of health insurance. Currently,
healthcare insurance accounts for about 5% of national healthcare
spending. The third factor likely to propel market growth is
greater awareness among the Indian population of quality healthcare
and an increase in income levels for the population in general.
With rapid growth seen in the domestic market, Indian companies
such Cipla, Mankind, and Alkem and multinational companies such as
Glaxo, Abbott Laboratories [ABT US], Pfizer, etc have developed
clear domestic strategies and established themselves as leading
players in this space.
Indian companies benefitted from the 1970 change in the patent
law that did not recognize product patents. They established
themselves as dominant players in absence of the multinational
companies. Following the change in the patent law in 2005,
multinationals have come back, but domestic companies continue to
dominate because of (1) low pricing of drugs, with affordability
key for the Indian population, (2) wider distribution reach
compared with the global players, and (3) the introduction of new
products in the market. With an eye to catering to every segment of
the market, multinational players that stayed in the country
following the
Pre-grant oppositions have been filed by Indian companies,
multinational companies, and NGOs
Companies have increased their R&D spending
Domestic market offers big opportunity
Competition from multinational companies
-
Nomura Japanese Equity Research
22 Pharmaceuticals sector
patent law change in 1970 have been more successful in capturing
growth in the domestic drug market. These players are now looking
at introducing products from their parent pipelines in the domestic
market. GlaxoSmithKline is among the global leaders in the vaccine
segment, with nearly a 33% share in emerging markets. It has one of
the widest ranges of vaccines in its pipeline among the big
pharmaceutical companies in India. It has introduced vaccines like
Rotarix and Cervarix in the domestic market and expects to launch
two more vaccines (Synflorix and Infanrix Hexa) and three oncology
products in India over the next 1218 months.
Various multinationals have also paid high premiums to acquire
leading Indian companies in order to get a taste of the domestic
market growth. While the acquisition of Ranbaxy at an EV/sales
ratio of 3.7x (or $4.6bn) by Daiichi Sankyo was a harbinger of the
future, the recent acquisition of Piramal Healthcares domestic
business for a premium EV/sales ratio of more than 8.2x ($3.7bn)
only underlines the importance of being present in the growing
Indian drug market.
The saturation of urban markets has led companies in India to
focus on deriving growth from the rural segment of the market. We
estimate that the size of the Indian market will more than to $20bn
by 2015 and that the size of the rural market will increase to
around 44% of the total. We project that almost half of total
growth until 2015 will come from the rural market, compared with
30% from metropolitan areas and 25% from Class I geographies. The
government is also aiming to improve healthcare services for the
rural masses and public spending is likely to quadruple from $1.5bn
to $6bn.
The strategies that companies adopt for urban and rural markets
can be very different. While the former relies on competitors
aiming to capture fragments of specialty segments, the latter
focuses on aggressive price cutting, promoting healthcare
awareness, and deploying a large sales force. Companies like
Mankind Pharma have been able to establish extensive rural networks
and have aggressively promoted low-cost medicine in these areas,
thereby inducing competitors to cut their prices as well. Some
multinationals have forayed into the rural market as well. Novartis
and Sanofi-Aventis are mentoring doctors and educating patients in
rural areas in an attempt to capitalize on the rural growth story.
Sanofi-Aventis also plans to launch drugs commonly used as
antiinfectivrs, cough and cold medications, and pain management
drugs. These drugs would be sourced from leading contract
manufacturing companies in the country and would lead to the
lowering of drug prices, thereby making them more affordable for
the rural population of India.
During the eighties and early nineties, active pharmaceutical
ingredients (APIs) were the bastion of Indian pharmaceutical
companies. However, stiff competition over the years from Chinese
imports has resulted in a significant price decline, thereby making
API production unattractive. Most Indian companies that we have
talked to view the API market as a lukewarm opportunity and they
currently produce APIs primarily for internal consumption and
backward integration. The exceptions to this rule are companies
that produce niche APIs, such as Wanbury and Jubilant Organosys.
These companies enter the market only for those APIs where they can
be market leaders around the world. Wanbury has a 30% share in the
world market for metformin while Jubilant maintains market
leadership in carbamazepine, oxcarbamazepine, and lamotrigine.
As per Eisai India, the production of Aricept (donepezil)
involves the use of a unique API that other generic makers cannot
use. In order to source this API, the company had to invest a
significant amount of time in training a local vendor so as to
increase the quality of the API and bring it up to the mark. The
company projects that by sourcing this unique API from the local
vendor, they will able to cut production costs by almost 50%.
However, according to some leading Indian companies, the average
cost of producing one generic pill is not going fall drastically
below INR0.5 (1) (Exhibit 2-1).
Acquisition of Indian companies at high premiums
Targeting bottom of pyramid
Companies need to adopt different strategies for rural
markets
Cutthroat competition from Chinese APIs
Cost of production has bottomed out
-
Nomura Japanese Equity Research
Pharmaceuticals sector 23
2-1. Domestic market business models
Domestic market
Indian companies
Low pricing strategy
Focus on small cities & rural markets
Large sales forces
Little or no product differentiation
Low entry barriers
Branded drugs w ith an India-centric pricing strategy
Focus on large cities and mass market products
Inlicensed products from parent; low R&D spending
Product differentiation
Acquisitions of domestic companies
Multinationals
Source: Nomura
Regulated and semiregulated market focus
As noted, the passage of the Indian Patents Act of 1970 resulted
in the end of product patents because it recognized only process
patents. Indian pharmaceutical companies could therefore legally
produce patented drugs through reverse engineering and sell
inexpensive copies of these leading branded drugs in India. Over
the next few years, Indian companies championed process engineering
and started exporting inexpensive drugs to unregulated markets (for
example, Ranbaxys Nigerian JV in 1977, Malaysian JV in 1983, and
Thai JV in 1987). By the end of the 1980s, India had become a
leading bulk drug exporter in the international market.
Indian pharmaceutical companies made large forays into the US
market after the passing of the Hatch-Waxman Act of 1984. The act
allowed generics companies to apply for Abbreviated New Drug
Applications (ANDAs) by simply proving bioequivalence and without
having to carry out clinical trials. By filing ANDAs and
First-to-Files, these companies challenged the existing patent of
the innovator through the Para IV clause of the act. This clause
allowed companies to challenge the innovators patent by claiming
that the patent was invalid or that it would not be infringed by
the generic drug. If the challenge was successful, the generics
company was provided with 180 days of exclusive marketing rights to
the drug and this often resulted in immense profitability as the
generic drug was marketed at a 1020% discount to the branded
drug.
Protective patent laws helped establish firm foundation
Hatch-Waxman Act provided further growth impetus
-
Nomura Japanese Equity Research
24 Pharmaceuticals sector
In the 1980s, Indian companies started at the low end of the
value chain by producing bulk drugs and vanilla generics and
exporting them to the US and other international markets. By the
1990s, the production strategy eventually shifted to finished
formulations and branded generics as the companies created
front-end marketing presences in regulated markets and leveraged
their production capabilities back in India.
The generics companies also set up their own subsidiaries in
foreign markets and some large Indian companies actively pursued
inorganic growth through the acquisition of smaller generics
companies and API manufacturers in regulated markets. The pursuit
of economies of scale gave the companies the opportunity to enter
new markets by growing their businesses. The companies also
invested heavily in creating world class production facilities in
India as the total number of US FDA-approved manufacturing plants
increased from one in 1988 to 125 in 2010, the largest number of
plants outside the US. Seeing this rapid increase in the number of
approved manufacturing plants, the US FDA also set up offices in
India (in New Delhi and Mumbai).
The interest of Indian pharmaceutical companies in Germany was
perhaps triggered by Ranbaxys acquisition of Bayers [BAYN GY]
generics business (Basics) back in 2000. When Germany revamped its
Reference Pricing Policy 2004, Indian drugmakers sensed another
huge opportunity for generics and adopted an aggressive expansion
strategy in the market. Between 2005 and 2008, Indian companies
such as Dr Reddys, Torrent Pharmaceuticals, Wockhardt [WPL IN],
etc, acquired six companies in total. However, the acquisitions did
not reap the intended rewards because drug prices fell owing to
tender-based pricing systems and other government policies.
Currently, Germany remains an unattractive market for Indian
pharmaceutical companies, much like the Netherlands and the UK.
Most Indian companies have stated that the remaining profitable
markets of the EU are France, Italy, and Spain. However, recent
austerity measures proposed by the governments in these countries
may play spoil-sport for the Indian companies.
Other markets, such as Brazil, Mexico, South Africa, the CIS,
and Eastern Europe, have also provided instrumental growth
opportunities for Indian companies. Demand for generics in these
semiregulated markets has led to the establishment of manufacturing
facilities, marketing capabilities, and distribution networks by
Indian companies in these territories (Exhibit 2-2).
Examples of companies in regulated and semiregulated markets are
Ranbaxy, Lupin, Dr Reddys, Sun Pharma, Zydus Cadila, Torrent
Pharmaceuticals, etc.
2-2. International market business model
Regulated & semiregulated markets
Branded and vanilla generics, bulk drugs
Front-end marketing capabilities
ANDAs, FTFs, and Para IV challenges
Acquisitions and partnerships
Source: Nomura
Moving up value chain
Aggressive expansion through acquisitions and increase in
production capacity
Germany strategy did not work effectively
Exploiting opportunities globally
-
Nomura Japanese Equity Research
Pharmaceuticals sector 25
Collaborative strategies
The innovators among drugmakers are witnessing a decline in
R&D productivity and facing stiff hurdles in terms of
sustaining earnings growth because some of the key products in
their portfolios face patent expiration. Lower success in drug
development implies that sales lost from patent expiry will not be
replenished by new product launches. In an effort to control costs
and improve productivity, the innovators are looking at options to
outsource drug discovery and development. Some Indian companies
have offered to collaborate with innovator drugmakers, rather than
file patent litigations against them.
The Indian contract research industry is worth less than $500mn,
implying less than a 2% share of the pharmaceutical R&D
outsourcing market. India presents advantages with respect to cost,
patient population, skill sets, and the like. As per an industry
estimate, by outsourcing R&D to India, the innovator
pharmaceutical companies could save up to 60% of overall R&D
expenses. These savings can be realized across all stages of the
drug discovery process, from research biology to clinical
development. However, our estimates indicate that the largest
savings can be achieved in the area of research chemistry and
clinical development.
Indian contract research companies are gaining traction and have
established credibility, as evidenced by various deals struck by
Indian companies with major pharmaceutical makers. Jubilant
Organosys currently has partnerships with Eli Lilly, AstraZeneca,
and Endo Pharmaceuticals Holdings [ENDP US] to work on
collaborative research. Meanwhile, Biocon has opened a dedicated
R&D center in Bengaluru for Bristol-Myers Squibb [BMY US] as
per a deal struck by the two companies. The R&D center employs
400 scientists who are dedicated exclusively to carrying out
clinical studies. In 2007, GVK Biosciences struck a deal with Wyeth
(now Pfizer) and opened a dedicated contract research center for
the American company. The involvement of Indian companies is now
not limited to a fee-based model as it has evolved into a
collaborative model for drug discovery.
Collaboration is not restricted to research services but also
extends to manufacturing services. It includes supply of APIs,
intermediates, and finished dosage forms. We expect outsourcing
penetration to increase, in the cases of both APIs/intermediates
and formulations, as the drug majors focus on drug discovery and
sales and marketing. We believe that the outsourcing industry can
record growth of 1015% per annum over the next five years, with the
potential for outsourcing penetration to double during the period.
We see more deals and partnerships being struck in the near future
as the innovator companies look at tapping into Indias outsourcing
strengths.
Another strategy that has become popular within the
collaborative framework is that of Indian generics companies
creating separate entities for branded and generic drugs. This
strategy helps create a clear distinction between the two
businesses because the mindsets required to run the two can be very
different. The branded drug arm usually works on discovering new
chemical entities (NCEs) and carrying out clinical trials up till
Phase 1. Because of limited financial capabilities, the companies
aim to partner with innovator drugmakers and outlicense the
molecule for upfront fees, royalty fees, and various milestone
payments upon successfully bringing the new molecules to Phase 1.
The innovator drug company usually retains the marketing rights for
the regulated markets while the Indian company gets the marketing
and distribution rights for emerging markets (Exhibit 2-3).
A recent example of this model is a Glenmark-Sanofi-Aventis deal
signed in May 2010, whereby Glenmark outlicensed the development
and commercialization rights of its painkiller molecule GRC 15300
to Sanofi-Aventis for an upfront payment of $20mn and milestone
payments that could reach a total of $325mn. Other leading
companies in this space include Jubilant Organosys, Piramal
Healthcare, Divi's Laboratories [DIVI IN], Dishman Pharmaceuticals
& Chemicals [DISH IN], Suven Life Sciences [SVLS IN], etc.
Major drugmakers are becoming more cost effective
Capitalizing on Indias soft skills strengths
Striking deals and gaining credibility globally
Drug discovery through different model: collaboration with
global majors
Drug discovery through different model: bifurcation and
outlicensing discoveries
Mutually beneficial partnerships
-
Nomura Japanese Equity Research
26 Pharmaceuticals sector
2-3. Collaborative strategy business model
Collaborative strategy
Collaborative drug discovery research
Initial stage clinical trials
Contract manufacturing
Outlicensing partnerships; upfront fees and royalties
Source: Nomura
2-4. Drug pipelines of Indian generic drug companies Company
Molecule name Indication Target Clinical trial phase
Crofelemer (inlicensed) Antidiarrhoeal CTFR inhibitor Phase 3
GRC 3886 (oglemilast) Asthma, COPD PDE IV inhibitor Phase 2 GRC
8200 (melogliptin) Diabetes mellitus (Type II) DPP IV inhibitor
Phase 2 GRC 4039 (revamilat) Rheumatoid arthritis, MS inhibitor PDE
IV Phase 1 GRC 10693 Neuropathic pain, osteoarthritis CB-2 Phase 1
GRC 500 MS, inflammatory diseases VLA-2 antagonist Phase 1 GRC
15300 Osteoarthritic pain, neuropathic pain, and skin disorders
TRPV3 antagonist Preclinical GBR 600 Antiplatelet, adjunct to
PCI/acute coronary syndrome Von Willebrand factor Preclinical
Glenmark
GRC 6211 Osteoarthritic pain, neuropathic pain, and urinary
incontinence TRPV 1 antagonist Phase 1
ZYH1 Dyslipidemia PPAR alpha:gamma Phase 3 ZYO1 Obesity,
diabetes CB-1 antagonist Phase 1 ZYI1 Pain Multi-modal Phase 2 ZYH2
Diabetes PPAR alpha:gamma Phase 1 ZYH7 Dyslipidemia PPAR alpha
Phase 1 ZYT1 Dyslipidemia Undisclosed Phase 1
Zydus Cadila
ZYD1 Dyslipidemia GLP-1 Phase 1 Oral insulin Diabetes - Phase 2
Anti-CD6 Oncology/inflammation/autoimmune - Phase 3 Targeted
immunoconjugates Oncology - Discovery Anti-CD20 Oncology -
Preclinical Peptide hybrid Diabetes - Discovery Anti-EGFR Oncology
- Market Biosimilar MAbs Oncology/immunology - Preclinical Insulin
analogs - lispro, aspart Diabetes - Preclinical Rh-insulin,
glargine Diabetes - Market
Biocon
GCSF, EPO Oncology - Market Reditux Non-Hodkins lymphoma
Monoclonal antibody Market DRF 2593 (balaglitazone) Metabolic
disorders (partnership with Rheoscience) - Phase 3 DRL 17822
Metabolic disorders/CVS (partnership with Argenta) - Phase 1 Dr
Reddy's
Several compounds Respiratory disorders (dyslipidemia and
atherosclerosis) - Phase 1 Ranbaxy P. falciparum combination
Malaria - Phase 3
LLL 2011 (amigra) Antimigraine, herbal - Phase 3 LL 4218
(desoside-P) Antipsoriasis - Phase 2 LL 3858 (sudoterb) Anti-TB -
Phase 2 LL 3348 (sesoris) Antipsoriasis, herbal - Phase 2
Unspecified Type II diabetes - Preclinical
Lupin
Unspecified Rheumatoid arthritis - Preclinical P276 - CDKs Head
& neck cancer, multiple myeloma - Phase 2 P276 - gemcitabine
combination Pancreatic cancer - Phase 1 P276 - tadiation
combination Head & neck cancer - Phase 1 P1446 - CDKs
Unspecified - Phase 1 NPB-001-05-Bcr-Abl Chronic myeloid leukemia -
Phase 2 NPS31807 - TNF alpha Rheumatoid arthritis and psoriasis -
Phase 2 P979 - TNF alpha Inflammation - Preclinical P1736-non-PPAR
gamma Diabetes and metabolic disorders - Phase 1 P1201 - Lilly
Diabetes and metabolic disorders - Phase 1 P2202 - Lilly Diabetes
and metabolic disorders - Phase 1
Piramal Lifesciences
NPH30907 Dermaphytotypes - Phase 2 Source: Nomura, based on
company data
-
Nomura Japanese Equity Research
Pharmaceuticals sector 27
Productivity analysis
We analyzed the value-added generated over the last seven to 10
years by three Indian companies, namely, Aurobindo, Ranbaxy, and
Torrent Pharmaceuticals. The following details were observed:
Aurobindo invested heavily in increasing capacity in 03/3, as
its gross block increased almost 3x that year, from INR2.21bn to
INR6.60bn. The increase in capacity was done mainly at
manufacturing plants in China and India. The company is now poised
to meet future production demands following the increase in its
capacity.
R